nicola barnstaple programme manager. key challenges in scotland increasing cancer incidence –...
TRANSCRIPT

Nicola Barnstaple
Programme Manager

Key challenges in Scotland• Increasing cancer incidence – predicted 35,000
cases per year in 2020• Ageing population -proportion of over-75s up
25% by 2023• Impact of health inequality - mortality rates from
cancer in the 10% most deprived areas are around 1.5 times those in the 10% least deprived areas
• Survival for some cancer types is lower in Scotland than in other European countries

Scotland: age-standardised incidence and mortality rates (EASRs), by SIMD 2009 deprivation quintile

Scotland: age-standardised cancer incidence and mortality rates (EASRs), by SIMD 2009 deprivation quintile
5=Least deprived
4 3 2 1=Most deprived
-
100.0
200.0
300.0
400.0
500.0
600.0 All cancersIncidence Mortality
EA
SR
5=Least deprived
4 3 2 1=Most deprived
-
10.0
20.0
30.0
40.0
50.0
60.0
70.0
ColorectalIncidence Mortality
EA
SR
5=Least deprived
4 3 2 1=Most deprived
-
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0 BreastIncidence Mortality
EA
SR
5=Least deprived
4 3 2 1=Most deprived
-
20.0
40.0
60.0
80.0
100.0
120.0 LungIncidence Mortality
EA
SR

Cancer staging by deprivation2010/2011 (baseline)
Stage 1 Stage 2 Stage 3 Stage 4 Not known
1=most deprived 19.8% 21.4% 19.3% 30.2% 9.3%
2 21.8% 24.1% 18.6% 26.4% 9.2%
3 22.6% 26.1% 18.0% 23.7% 9.6%
4 25.0% 27.5% 16.2% 22.9% 8.3%
5=least deprived 27.2% 28.0% 15.6% 21.1% 8.0%
2011/2012
Stage 1 Stage 2 Stage 3 Stage 4 Not known
1=most deprived 20.3% 22.1% 18.6% 30.9% 8.1%
2 23.0% 23.6% 18.8% 27.0% 7.6%
3 23.5% 25.9% 17.5% 25.6% 7.4%
4 26.9% 26.7% 16.5% 23.1% 6.9%
5=least deprived 27.5% 27.1% 16.4% 21.8% 7.1%

Key challenges• Increasing cancer incidence – predicted
35,000 cases per year in 2020• Ageing population -proportion of over-75s
up 25% by 2023• Impact of health inequality - mortality rates
from cancer in the 10% most deprived areas are around 1.5 times those in the 10% least deprived areas
• Survival for some cancer types is lower in Scotland than in other European countries






0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Stomach Colon Rectum Lung Skin Melanoma
Type of cancer / Country
Rel
ativ
e su
rviv
al (
%)
Five-year age-adjusted relative survival (%) with 95% confidence intervals for adults diagnosed during 2000-2007, by selected country and cancer site/type

Five-year age-adjusted relative survival (%) with 95% confidence intervals for adults diagnosed during 2000-2007, by selected country and cancer site/type
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Denm
ark
Finland
Norw
ay
UK,England
UK, Scotland
Breast (Woman) Ovary Prostate Kidney Non-Hodgkin lymphoma
Type of cancer / Country
Rel
ativ
e su
rviv
al (
%)
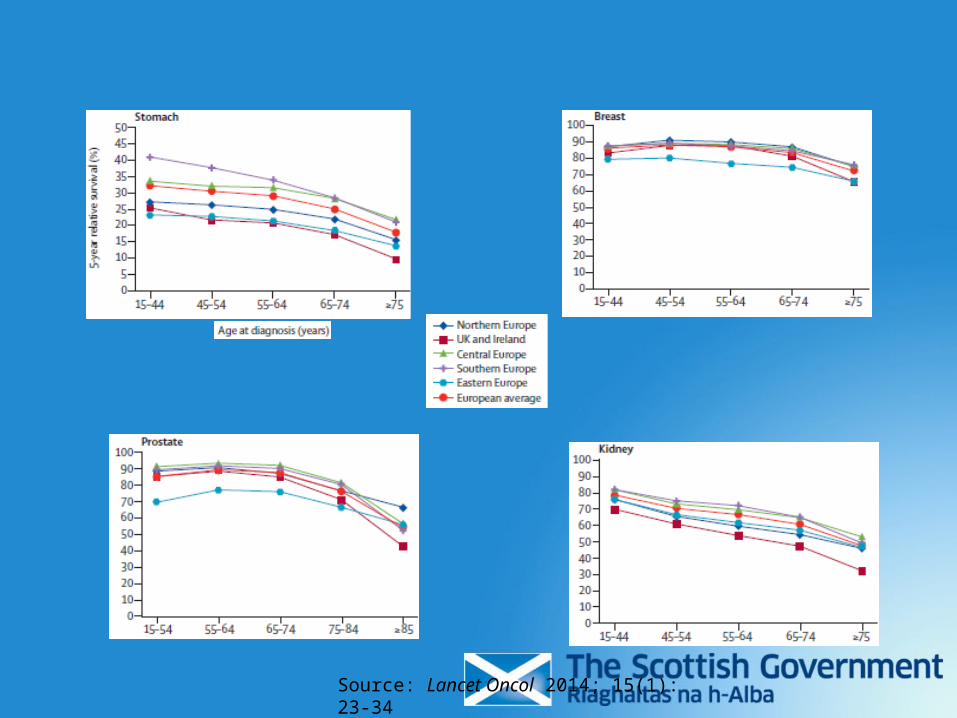
Source: Lancet Oncol 2014; 15(1): 23-34

Colorectal cancer diagnosed 1995-99. Five year relative survival vs survival conditional on surviving at least one year
0
10
20
30
40
50
60
70
80
5-year Relative survival Conditional survival
% s
urv
ivin
g Denmark
England
Scotland
Finland
Norway
Sweden



So what is the explanation for this apparent excess of early mortality?
•Unfavourable stage distribution due to delays and/or tumour biology?
and/or
•Poor general health/lifestyle factors laid down over decades?


Source: Lancet Oncol 2014; 15(1): 2-3



Source: BMJ 2010; 341: c5133

Eurocare 5 findings
• Survival from major epithelial cancers seems to be lower in Scotland (and the UK) compared to all of the Nordic countries except Denmark
• The excess risk of death seems to occur early on and is more apparent in oldest age groups
• Some evidence suggests that, on average, UK patients may be presenting with more advanced disease at diagnosis
• But we don’t know for sure whether this is due to later presentation, later referral, delays in diagnosis or staging, or more aggressive disease
• We know that lifestyle factors can influence survival, but we don’t really know to what extent, if any, this contributes to European survival variations
• The reasons for reported survival differences seem most likely to be multifactorial

Cancer: approx 6% total NHS spend
Cancer services: estimated activity and costs: Scotland 2007/08
Acute Services episodes
Geriatric long stay episodes
Out patient services
Pharmaceutical items dispensed
GMS visits
Activity 188,141 517 144,624 1,153,614 195,363
Cost £390M £8.5M £25M £46M £6.3M

Costs
• Projected 65% increase in costs of treating cancer by 2021
• For colon cancer: treatment in Stage 1 costs £3131 and treatment in stage 4 costs £12519


DCE HEAT Target
• to achieve a 25% increase in the proportion of breast, colorectal and lung cancers (combined) diagnosed at stage 1 by December 2015 when compared to the 2010 and 2011 (combined) baseline (23% → 29%).

Social Marketing

Primary Care
• Review of Scottish Referral Guidelines for Suspected Cancer
• New sGMS contract initiative for bowel screening
• Primary Care education sessions• Improvements in e-Health, eRAT• Development of practice profiles for
cancer

Evaluation – key points
• Data on cancer diagnoses not yet available• 4.7% increase in cancers diagnosed at Stage I (2012/13 compared to
baseline)• Priming Campaign - just under half (48%) of all respondents feel more
confident about approaching their GP with signs or symptoms which could possibly be cancer
• Breast Campaign – 50% increase in attendances at GP for breast symptoms• Bowel Campaign- increases in requests for replacement kits and calls to
screening helpline, increase in screening programme participation (56.1% from 54.9%)
• Lung Campaign - Significant improvement in relation to key campaign message of importance of getting cough checked
• Other measures of success – emergency admissions, ICBP, TCT, other studies

DCE Next Steps
• Consolidation• Breast Screening Campaign• Updated bowel and lung cancer
campaigns• Interim Evaluation• Consideration of new tumour groups

Early diagnosis is important
• relations with patients and families• RCGP/Patient Safety Agency report• best chance for long-term survival. • still well enough to tolerate disease modifying
treatments • emergency diagnoses don’t do as well• more time to manage symptoms• allows more to join clinical trials

Scottish Cancer Taskforce
• DCE• Treatment capacity• TCAT• QPI
Acknowledgements
EUROCARE-5 slides mostly reproduced from the Lancet Oncology papers
Data are also now available to download from the EUROCARE website: http://www.eurocare.it/