nhsimprovement-cancer cancer stratifiedpathwaysofcare · p r ima yce/ o un t p a lit v ec r d...
TRANSCRIPT

NHSNHS Improvement
Cancer
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
Stratified pathways of care...from concept to innovationExecutive Summary
NHS Improvement - Cancer
March 2012
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 1

Pathway to Improvement:Survivorship 15/3/12 16:00 Page 2

NHS Improvement is working in partnership withpatients, clinical teams, the Department of Health(DH) and voluntary organisations to improve theeffectiveness and quality of service delivery forthose living with and beyond cancer. TheNational Cancer Survivorship Initiative (NCSI) wasset up as a recommendation in the Cancer ReformStrategy (2007), and the importance of the workreinforced through Improving Outcomes; aStrategy for Cancer (2011).
The current traditional approach to managingpatients following initial treatment is based on amedical (illness) model where patients can be infollow-up for two to five years or more followingcompletion of initial treatment. This isunsustainable for two key reasons:
• Incidence and prevalence of cancer continuesto increase thereby putting pressure onavailable resources
• The current arrangement are not meeting allof the needs of those living with and beyondcancer.
The focus for NHS Improvement is to work withclinical teams supporting patients following initialtreatment for breast, colorectal, lung or prostatecancer, to redesign the pathway of care andstratify patients into an appropriate level of care.
Introduction
Stratified pathways of care... from concept to innovation
3Introduction
For breast colorectal and prostate cancers theemphasis has been on supporting patients to getback to living their lives following initial treatmentfor cancer with remote monitoring replacingroutine follow up where appropriate. For lungcancer it was about managing active andadvanced disease through proactive rather thanreactive management with the focus onimproving quality of life.
This work has been supported by the DH cancerteam, NCSI project teams, Macmillan CancerSupport, and specialty specific charities such asbreast cancer care, beating bowel cancer and theprostate cancer charity.
Evaluation of the testing is on-going and it will beearly in 2013 before we see the whether thestratified model of care and associated supporthas improved patient experience and reportedoutcomes of care. However, the economicbenefits of reducing outpatient follow up on boththe NHS and individual patients is evidencedthrough the reduction in the projected outpatientactivity compared to the traditional model.
However, to realise the full potential of thisredesigned model of care, commissioners need tofocus not on activity but on providing theresources through a bundle of care to support
patients to self-manage. This will include supportto enable patients to return to living their livesand a robust monitoring solution to detect relapseor recurrence over time. Service providers need toensure that they have systems in place for timelyaccess should patients experience difficulty andwork with commissioners to ensure they have theright people with the right skills in the right placeto support patients to self-manage.
Commissioners and providers should embrace thiswork and proactively support the shift from thetraditional activity based medical model to a safeand effective stratified model that meets patients’needs whether they are being professionallymanaged or are being supported to self-manage.
This is a summary report of this year’s workand a more comprehensive report can befound on our website at:www.improvement.nhs.uk/cancer
Gilmour FrewDirector - NHS Improvement
www.improvement.nhs.uk/cancer/survivorship
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 3

1
2
4
5
3
STRATIFIED PATHWAY OF CARE: BREAST
4 Stratified Pathway of Care: Breast
www.improvement.nhs.uk/cancer/survivorship
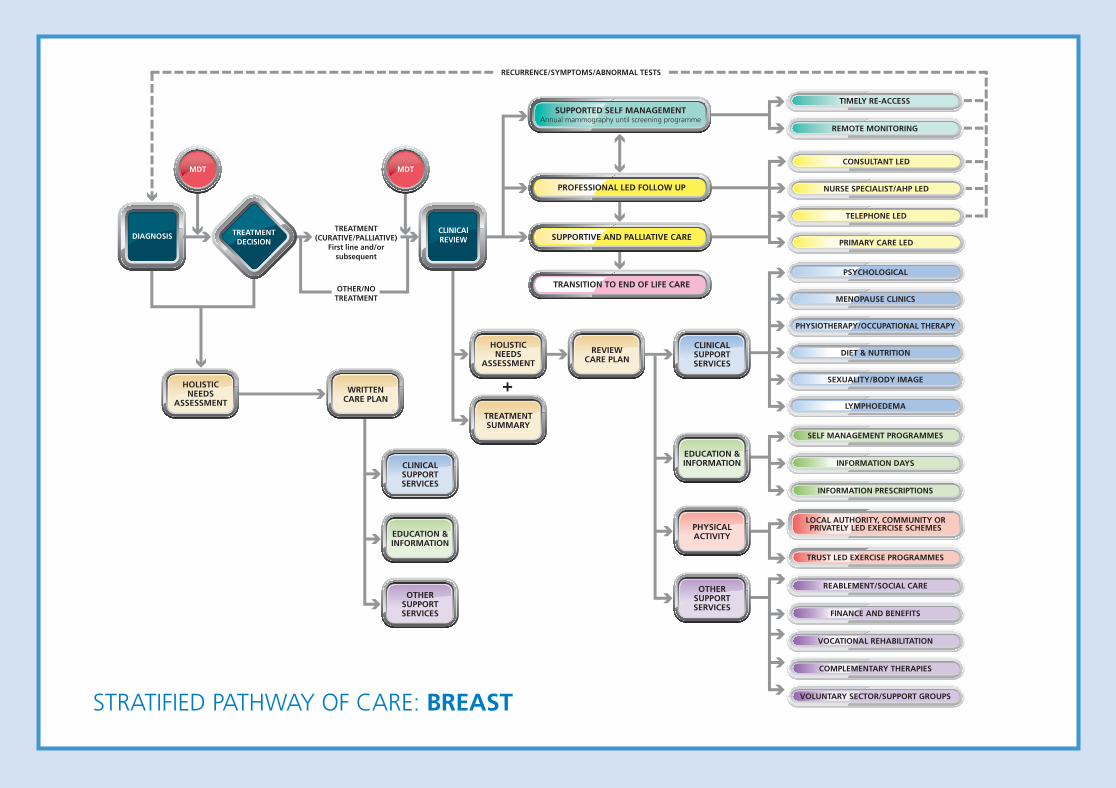
Background and contextThe traditional model of follow up has been tooffer annual mammography and outpatientreviews over a period of three to five years.
Data has shown that recurrences are morecommonly picked up by the patient betweenappointments or following mammogram scansrather than an outpatient consultation.
Increased demand has led to overbooked clinicswith insufficient discussion time for those who stillhave complex emotional and psychosocial needsafter their treatment has ended.
Five teams have tested stratified pathways offollow up care. An expected 70% of breastpatients were predicted to be suitable for asupported self management pathway.
The duration of follow up had already started toreduce in some Trusts. All were keen improveinformation, education and support services forpatients.
What we did?Baseline data was gathered and and the currentpathways were mapped.
The baseline patient experience survey found themain issues for breast cancer patients were:• Fatigue• Fear of recurrence• Signs and symptoms of recurrence.
Breast specific or generic cancer education eventswere held in most organisations with the focus oninformation, overcoming the above issues andrebuilding lives.
All teams established links with communityschemes with particular focus on physical activity.Several teams have provided oncology awarenesstraining for leisure centre staff.
All teams have introduced holistic needsassessment at the end of treatment where afuture care plan is agreed.
All sites have separated the annualmammography test from the outpatient visitwith results sent by post.
What we found• Self managed follow up is safe, acceptable andoften welcomed by patients
• Self management was suitable for around 77%patients treated with curative intent within oneyear of diagnosis as long as patient has a reviewof needs at end of treatment and continuedopen access to the specialist team
• Only two pathway options were required;supported self management and professionallyled follow up
• Mammography screening can be separated fromthe outpatient visit. Some reporting processesoffer scope for further development
• Information events are cost effective and offervalue to patients. Take up rates were dependantupon how and who invited them and perceivedimportance
• Access to physical activity and other supportservices have been welcomed
• Resources may need to shift from medical tonursing budgets to support additional holisticneeds assessments and educational initiatives
• The stratified pathway model needs to bereinforced at new staff induction.
I thought I was the only one who felt like me. This group(Moving On) has increased my confidence and given me apositive direction.“
”Patient
1 Hull and East Yorkshire HospitalsNHS Trust
2 Ipswich Hospital NHS Trust
3 North Bristol Hospital NHS Trust
4 Hillingdon Hospital NHS Trust
5 Brighton and Sussex UniversityHospitals NHS Trust
Survivorship Test Sites -Breast 2011/12
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 4
RECURRENCE/SYMPTOMS/ABNORMAL TESTS
TELEPHONE LED
PRIMARY CARE LED
MENOPAUSE CLINICS
PSYCHOLOGICAL
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
PHYSICALACTIVITY
REVIEWCARE PLAN
PHYSIOTHERAPY/OCCUPATIONAL THERAPY
DIET & NUTRITION
SEXUALITY/BODY IMAGE
LYMPHOEDEMA
SELF MANAGEMENT PROGRAMMES
INFORMATION DAYS
INFORMATION PRESCRIPTIONS
DIAGNOSISCLINICAlREVIEW
HOLISTICNEEDS
ASSESSMENT
WRITTENCARE PLAN
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
OTHERSUPPORTSERVICES
HOLISTICNEEDS
ASSESSMENT
TREATMENTSUMMARY
OTHERSUPPORTSERVICES
SUPPORTIVE AND PALLIATIVE CARE
TRANSITION TO END OF LIFE CARE
PROFESSIONAL LED FOLLOW UP
MDT MDT
TIMELY RE-ACCESS
REMOTE MONITORING
CONSULTANT LED
NURSE SPECIALIST/AHP LED
TRUST LED EXERCISE PROGRAMMES
REABLEMENT/SOCIAL CARE
FINANCE AND BENEFITS
VOCATIONAL REHABILITATION
COMPLEMENTARY THERAPIES
VOLUNTARY SECTOR/SUPPORT GROUPS
TREATMENT(CURATIVE/PALLIATIVE)
First line and/orsubsequent
OTHER/NOTREATMENT
TREATMENTDECISION
LOCAL AUTHORITY, COMMUNITY ORPRIVATELY LED EXERCISE SCHEMES
+
SUPPORTED SELF MANAGEMENTAnnual mammography until screening programme
STRATIFIED PATHWAY OF CARE: BREAST
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 5
1
23
STRATIFIED PATHWAY OF CARE: COLORECTAL
6 Stratified Pathway of Care: Colorectal
www.improvement.nhs.uk/cancer/survivorship
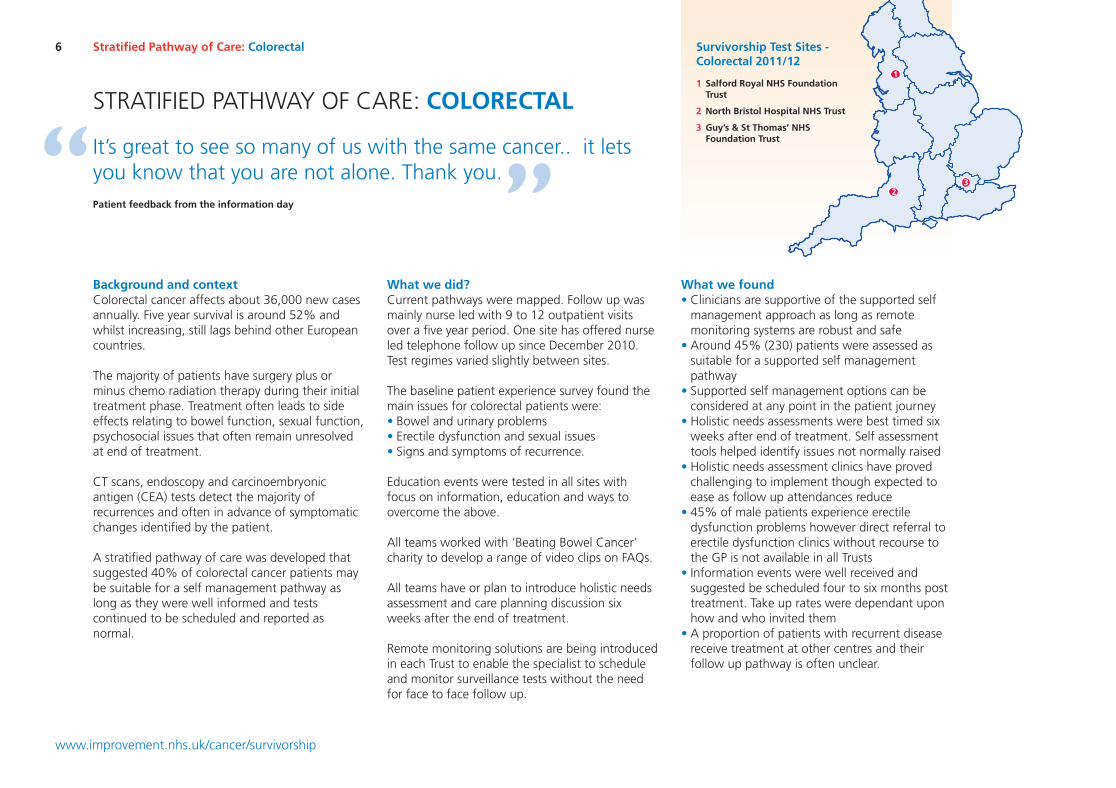
Background and contextColorectal cancer affects about 36,000 new casesannually. Five year survival is around 52% andwhilst increasing, still lags behind other Europeancountries.
The majority of patients have surgery plus orminus chemo radiation therapy during their initialtreatment phase. Treatment often leads to sideeffects relating to bowel function, sexual function,psychosocial issues that often remain unresolvedat end of treatment.
CT scans, endoscopy and carcinoembryonicantigen (CEA) tests detect the majority ofrecurrences and often in advance of symptomaticchanges identified by the patient.
A stratified pathway of care was developed thatsuggested 40% of colorectal cancer patients maybe suitable for a self management pathway aslong as they were well informed and testscontinued to be scheduled and reported asnormal.
What we did?Current pathways were mapped. Follow up wasmainly nurse led with 9 to 12 outpatient visitsover a five year period. One site has offered nurseled telephone follow up since December 2010.Test regimes varied slightly between sites.
The baseline patient experience survey found themain issues for colorectal patients were:• Bowel and urinary problems• Erectile dysfunction and sexual issues• Signs and symptoms of recurrence.
Education events were tested in all sites withfocus on information, education and ways toovercome the above.
All teams worked with ‘Beating Bowel Cancer’charity to develop a range of video clips on FAQs.
All teams have or plan to introduce holistic needsassessment and care planning discussion sixweeks after the end of treatment.
Remote monitoring solutions are being introducedin each Trust to enable the specialist to scheduleand monitor surveillance tests without the needfor face to face follow up.
What we found• Clinicians are supportive of the supported selfmanagement approach as long as remotemonitoring systems are robust and safe
• Around 45% (230) patients were assessed assuitable for a supported self managementpathway
• Supported self management options can beconsidered at any point in the patient journey
• Holistic needs assessments were best timed sixweeks after end of treatment. Self assessmenttools helped identify issues not normally raised
• Holistic needs assessment clinics have provedchallenging to implement though expected toease as follow up attendances reduce
• 45% of male patients experience erectiledysfunction problems however direct referral toerectile dysfunction clinics without recourse tothe GP is not available in all Trusts
• Information events were well received andsuggested be scheduled four to six months posttreatment. Take up rates were dependant uponhow and who invited them
• A proportion of patients with recurrent diseasereceive treatment at other centres and theirfollow up pathway is often unclear.
It’s great to see so many of us with the same cancer.. it letsyou know that you are not alone. Thank you.“ ”Patient feedback from the information day
1 Salford Royal NHS FoundationTrust
2 North Bristol Hospital NHS Trust
3 Guy’s & St Thomas’ NHSFoundation Trust
Survivorship Test Sites -Colorectal 2011/12
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 6
RECURRENCE/SYMPTOMS/ABNORMAL TESTS
TELEPHONE LED
PRIMARY CARE LED
CONTINENCE/STOMA
PSYCHOLOGICAL
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
PHYSICALACTIVITY
REVIEWCARE PLAN
PHYSIOTHERAPY/OCCUPATIONAL THERAPY
DIET & NUTRITION
ERECTILE DYSFUNCTION/SEXUALITY
LYMPHOEDEMA
SELF MANAGEMENT PROGRAMMES
INFORMATION DAYS
INFORMATION PRESCRIPTIONS
DIAGNOSISCLINICAlREVIEW
NEEDSASSESSMENT
WRITTENCARE PLAN
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
OTHERSUPPORTSERVICES
NEEDSASSESSMENT
TREATMENTSUMMARY
OTHERSUPPORTSERVICES
SUPPORTIVE AND PALLIATIVE CARE
TRANSITION TO END OF LIFE CARE
PROFESSIONAL LED FOLLOW UP
MDT MDT
TIMELY RE-ACCESS
REMOTE MONITORING
CONSULTANT LED
NURSE SPECIALIST LED
TRUST LED EXERCISE PROGRAMMES
REABLEMENT/SOCIAL CARE
FINANCE AND BENEFITS
VOCATIONAL REHABILITATION
COMPLEMENTARY THERAPIES
VOLUNTARY SECTOR/SUPPORT GROUPS
CURATIVETREATMENT
First line and/or subsequent
PALLIATIVETREATMENT
TREATMENTDECISION
LOCAL AUTHORITY, COMMUNITY ORPRIVATELY LED EXERCISE SCHEMES
+
SUPPORTED SELF MANAGEMENTCEA, CT scans, colonoscopy per local protocol
STRATIFIED PATHWAY OF CARE: COLORECTAL
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 7

1
2
STRATIFIED PATHWAY OF CARE: LUNG
8 Stratified Pathway of Care: Lung
www.improvement.nhs.uk/cancer/survivorship
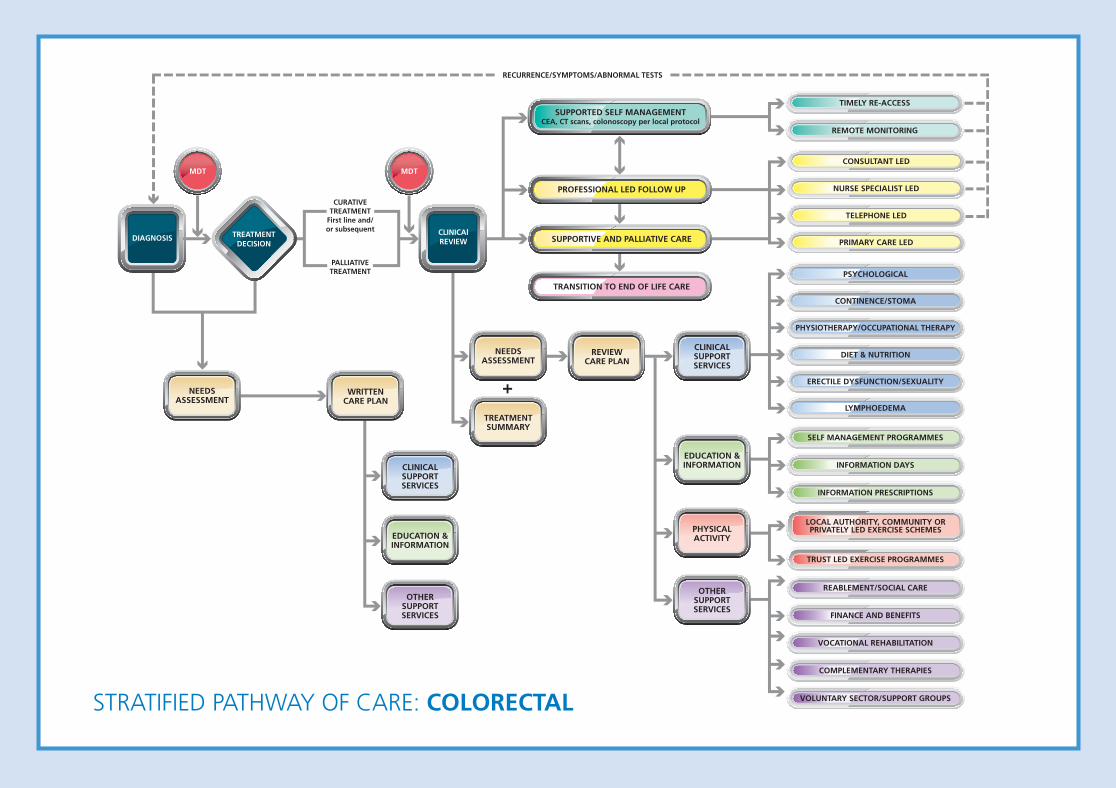
Background and contextLung cancer is the commonest cause of cancerdeaths in the UK (22% of all cancer deaths).Patients often present late in the course of theirdisease with around 70% having advanced orincurable disease at presentation. About 38% ofpatients are first diagnosed following anemergency admission.
Lung cancer patients are highly symptomaticoften with significant health needs. Manyexperience difficulties with breathing, fatigue,anxiety and depression along with poor appetiteand nutritional needs.
Two teams in Hull and Brighton were invited totest the degree to which risk stratified pathwayscould be applied in lung cancer with focus onproviding a more proactive rather than reactivemanagement approach and on improving qualityof life. It had been suggested that 15% ofpatients may be suitable for a self managedpathway.
The use of needs assessments, care plans andtreatment summaries were already embedded inpractice on both sites.
What we did?In Brighton, a pilot health and wellbeing clinic wasestablished to address the most frequent needs ofpatients: anorexia and weight loss, breathlessnessand fatigue and financial and benefits issues.
Also in Brighton, for patients not on activetreatment yet remaining under specialist care, apre clinic telephone assessment was implementedone week prior to the outpatient appointment. Asimilar flexible approach to appointments exists inHull, with patients added to or removed as needschange.
Criteria have been defined that may predict theneed for complex, supported or self managedcare – analysis is ongoing. In Hull, a set ofpragmatic criteria were developed to support thetransfer of immediate care responsibility to thecommunity teams
In Hull, nurse led end of treatment review clinicswere established building on the needsassessment carried out at diagnosis.
What we foundAll patients require some form of professional ledcare but several can self manage for periods ofthe pathway and can be supported by telephoneassessment during this period.
In Hull, 33% of patients seen in the nurse led posttreatment clinic, met the criteria for dischargeunder the care of the community team. This clinicwas best timed four to six weeks after end oftreatment.
Offering tailored care packages can impact onemergency admission rates and unnecessaryattendances at hospital clinics without causingharm:• Both sites recorded 6% to 8% reductions inunplanned admissions. In Hull, there were 34fewer admissions over eight months in 2011compared to 2010
• Brighton recorded a 25% reduction in bed days• In Brighton, around 20% to 25% of clinicappointments were cancelled and rescheduledas a result of the pre clinic telephone calls. 18%of appointments were arranged at patient orprofessional request avoiding and emergencyadmission.
Holistic care plans, educational resources andwell-being clinics allow patients to have a greaterunderstanding of their condition, provide a greatersense of control and merit future investment.
Implementing tailored packages of care requiresconsiderable administrative support which shouldbe accounted of in the commissioning of services.
I was very impressed with the kindness and consideration givento me by all members of the team from the doctors and nursesdown to the tea man.“
”Patient
1 Hull and East Yorkshire HospitalsNHS Trust
2 Brighton and Sussex UniversityHospitals NHS Trust
Survivorship Test Sites -Lung 2011/12
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 8
HOSPICE LED
NUTRITIONALCLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
REVIEWCARE PLAN
DISTRICT NURSING
COPING/PSYCHOLOGICAL
HOME OXYGEN SERVICES
INFORMATION PRESCRIPTIONS
DIAGNOSISCLINICAlREVIEW
NEEDSASSESSMENT
WRITTENCARE PLAN
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
OTHERSUPPORTSERVICES
NEEDSASSESSMENT
TREATMENTSUMMARY
OTHERSUPPORTSERVICES
SUPPORTIVE AND PALLIATIVE CARE
PROFESSIONAL LED
END OF LIFE CARE
MDT
CLINICAL NURSE SPECIALIST LED
TELEPHONE LED
REABLEMENT/SOCIAL CARE
FINANCE AND BENEFITS
LEGAL ADVICE
COMPLEMENTARY THERAPIES
VOLUNTARY SECTOR/SUPPORT GROUPS
CURATIVE TREATMENT
PALLIATIVE TREATMENT
SUPPORTIVE CARE
TREATMENTDECISION
+
SPECIALIST PALLIATIVE CARE LED
CONSULTANT LED (RESPIRATORY,ONCOLOGY, THORACIC)
PRIMARY CARE/COMMUNITYPALLIATIVE CARE LED
OCCUPATIONAL THERAPY/WHEELCHAIR SERVICES
PHYSIOTHERAPY/BREATHLESSNESS CLINICS
RECURRENCE/SYMPTOMS
STRATIFIED PATHWAY OF CARE: LUNG
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 9
1
2
34
STRATIFIED PATHWAY OF CARE: PROSTATE
10 Stratified Pathway of Care: Prostate
www.improvement.nhs.uk/cancer/survivorship
Background and contextThe incidence and prevalence of prostate cancer isincreasing and the service is struggling to copewith the demand. The traditional model is tooutpatient follow up, or when the condition isdeemed stable and two years out of initialtreatment to discharge the patient to primarycare. There are a few urology clinical teams whomanage their patients remotely through PSAtesting with the database being clinicallymanaged by a CNS supported by a urologyconsultant.
A consensus meeting and further discussions wereheld to identify potential levels of care, keypathway components and the potential split ofpatients into the different levels of care. Withinthe test sites the current follow up attendancesranged from 8 to10 over a five year periodthough we know that PSA monitoring for manypatients continues for life.
The emphasis was on recovery following initialtreatment, preparing patients to self-manage withsupport, which includes on-going monitoring ofPSA and timely access should problems occur.
What we did?Four urology clinical teams participated in thetesting of the risk stratified model of care.Baseline information was obtained from the testsites such as current pathway and patient flows. Abaseline Ipsos MORI patient survey showed thatthe key areas for improvement were:• Better information on signs and symptoms tolook out for; 40% did not have all theinformation they needed)
• Better management of erectile dysfunction;44% of those with a problem continue to haveproblems
• Better continence management; of the 55%who had continence problems following initialtreatment, in 20% they continued to have aproblem.
It was interesting that 80% of patients felt fairlyor very confident in managing their own health.Risk stratification into three levels of care weretested and test sites were asked to include anindividual assessment, including a self-assessmenttriage tool for patients post treatment, a summarytreatment record for the patient and GP/primarycare team, and a hand held record where keycontacts, outcomes of interactions and tests couldbe recorded.
What we found• During the testing it became apparent that forprostate cancer there were a number of managementpathways which through the leadership of theNational Clinical Advisor were distilled down into twolevels of care following stratification; supportedself-managed or professionally managed
• Supported self-management is a safe and acceptedalternative to outpatient follow up where a robustremote management solution is in place
• From the testing, between 28% and 44% werestratified to self-management but it was felt asconfidence in remote monitoring became establishedthe number stratified to this level of care wouldincrease
• Needs assessment informs the conversation aboutwhat matters to the individual patient
• Specific needs around erectile function and continencecontinue to be an area of concern which can havephysical, social and psychological consequences forpatients and their families if unresolved
• Information and education help inform patients andthe conversation can be supplemented throughMacmillan and the Prostate Cancer Charitypublications
• On-going evaluation is required to collect the evidencethat the interventions and support provided is makinga real difference to patient experience and outcomesof care.
It’s much better on both sides as it saves time for everyoneand we don’t have to keep coming up to the hospital.“ ”Patient
1 Ipswich Hospital NHS Trust
2 Luton and Dunstable HospitalNHS Foundation Trust
3 North Bristol Hospital NHS Trust
4 Hillingdon Hospital NHS Trust
Survivorship Test Sites -Prostate 2011/12
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 10
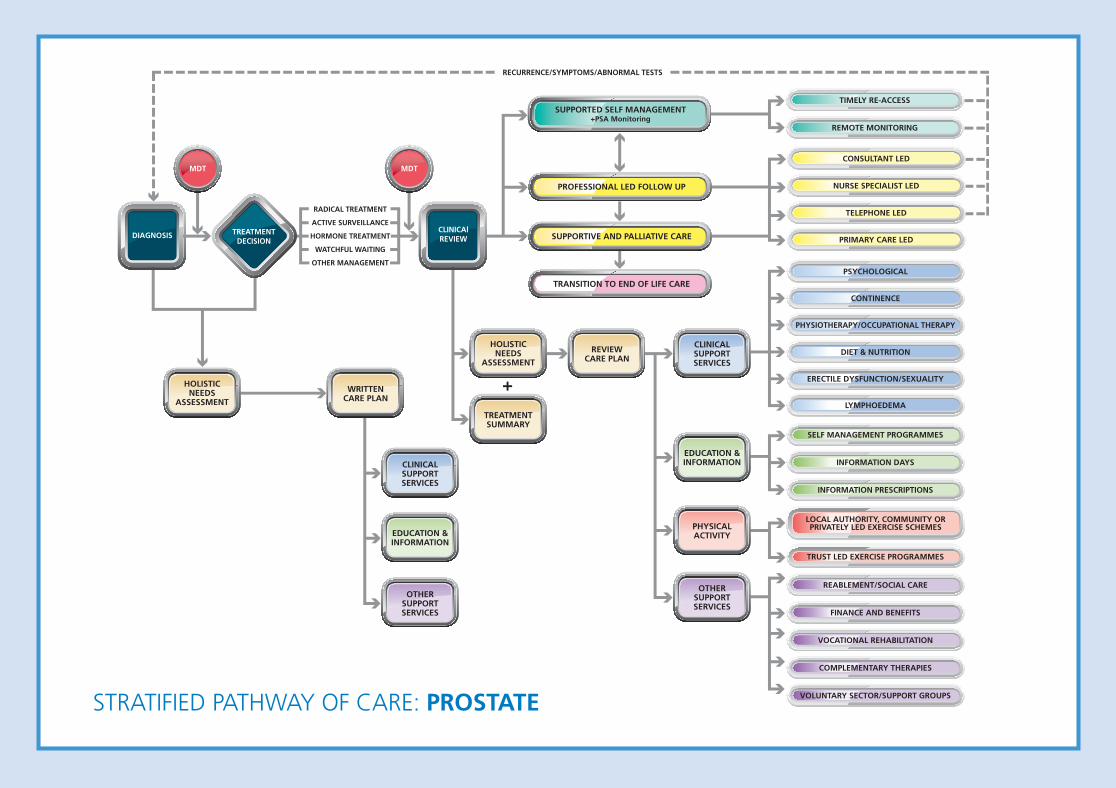
RECURRENCE/SYMPTOMS/ABNORMAL TESTS
TELEPHONE LED
PRIMARY CARE LED
CONTINENCE
PSYCHOLOGICAL
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
PHYSICALACTIVITY
REVIEWCARE PLAN
PHYSIOTHERAPY/OCCUPATIONAL THERAPY
DIET & NUTRITION
ERECTILE DYSFUNCTION/SEXUALITY
LYMPHOEDEMA
SELF MANAGEMENT PROGRAMMES
INFORMATION DAYS
INFORMATION PRESCRIPTIONS
DIAGNOSISCLINICAlREVIEW
HOLISTICNEEDS
ASSESSMENT
WRITTENCARE PLAN
CLINICALSUPPORTSERVICES
EDUCATION &INFORMATION
OTHERSUPPORTSERVICES
HOLISTICNEEDS
ASSESSMENT
TREATMENTSUMMARY
OTHERSUPPORTSERVICES
SUPPORTIVE AND PALLIATIVE CARE
TRANSITION TO END OF LIFE CARE
PROFESSIONAL LED FOLLOW UP
MDT MDT
TIMELY RE-ACCESS
REMOTE MONITORING
CONSULTANT LED
NURSE SPECIALIST LED
TRUST LED EXERCISE PROGRAMMES
REABLEMENT/SOCIAL CARE
FINANCE AND BENEFITS
VOCATIONAL REHABILITATION
COMPLEMENTARY THERAPIES
VOLUNTARY SECTOR/SUPPORT GROUPS
RADICAL TREATMENT
ACTIVE SURVEILLANCE
HORMONE TREATMENT
WATCHFUL WAITING
OTHER MANAGEMENT
TREATMENTDECISION
LOCAL AUTHORITY, COMMUNITY ORPRIVATELY LED EXERCISE SCHEMES
+
SUPPORTED SELF MANAGEMENT+PSA Monitoring
STRATIFIED PATHWAY OF CARE: PROSTATE
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 11
STRATIFIED PATHWAY OF CARE: REMOTE MONITORING
12 Stratified Pathway of Care: Remote Monitoring
www.improvement.nhs.uk/cancer/survivorship
Background and contextRemote monitoring in this context describes theway specialist cancer teams can monitor largenumbers of patients in the community withoutthe need for face-to-face follow up. Remotemonitoring is a key enabler for patients stratifiedto a self management pathway.
All patients enrolled for remote monitoring willhave been assessed for suitability, have theinformation and support they need with openaccess back into the service if required.
Good examples of remote monitoring exist inEngland, however, adoption and spread has beenhampered by lack of IT development resources,constrained IT architecture, lack of full MDTsupport or concerns around financial instabilityfrom reduced outpatient activity.
All participating teams were asked to test aremote monitoring solution/s for patientsstratified to a self management pathway. Thesecould be in house systems or the NHSImprovement sponsored solution.
Several breast teams had established systems inplace for ongoing mammogram monitoring usingeither local radiology or parallel national breastscreening systems.
What we did?NHS Improvement sponsored the development of aremote monitoring solution capable of interfacingwith local IT systems to support prostate cancer(PSA monitoring) and colorectal cancer (CEA, CTscans and endoscopy procedures). Systemrequirements included the ability to schedule andmonitor tests, issue standard result letters, triggerdefaults and record all outcomes.
The modules became available in summer 2011,however, few organisations were able to progressimplementation at that time due to existingworkload commitments.
Two colorectal teams opted to develop in housesolutions and these are expected to go live April2012. The IT functionality developed at Guys and StThomas’ enables use across several tumour groups.
Two organisations required formal business caseapproval to proceed. Two additional associate sitesat St Georges, London and the Royal UnitedHospital Bath were also recruited to test theprostate cancer module.
Systems for mammography surveillance provedstraightforward. Most patients are referred at thepost surgery MDT meeting for ongoingmammograms (as per NICE guidelines) withresults sent by post.
What we found• IT resources need to be identified at the start of theproject and time scheduled into IT work plans forimplementation and testing before go live.
• Stratified pathways of care can be introduced inadvance of the remote monitoring solution beingmade available
• Clinical leads and their teams need to ensure thatgovernance arrangements, such as standardoperation procedures, are in place to support thesystem
• Resources required to support implementationshould include general project management time,plus approximately 20 days IT resource over aminimum period of three months
• Teams should meet with commissioners early inproject to allay concerns about shifting activity toprimary care. Any impact on phlebotomy services isexpected to be minimal
• Savings associated with reduced outpatient activityneed to be off set against the cost (people and kit) tosupport remote monitoring. In Bath, the prostateservice requires one CNS session per week to supportabout 700 patients
• Remote monitoring solutions for prostate andcolorectal cancers have taken longer thanexpected to implement.
There was sceptism that patients would accept ‘self care’, imagining that these patients wouldvalue regular surveillance. When the rationale was properly explained it becomes obvious thatthe opposite was the case and most patients were delighted to accept the logic of the scheme.“
”Consultant Oncologist
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 12

STRATIFIED PATHWAY OF CARE: CARE COORDINATION
Background and contextCare coordination is the seamless experience ofcare which encompasses information andcommunication between patients, their carers andproviders, and between those providing servicesacross the individual patient pathway. It istherefore a function to ensure that as far aspossible those who will be working in partnershipwith patients have access to appropriateinformation (with the patients consent) to providean effective service.
The key areas of care coordination addressedduring this phase have been:
• Assessment and care planning includingtreatment summaries
• Information, education and advice• Self-management and timely re-access• Working across care sectors and organisations.
What we did?Our aim was to create a cultural shift from thepatient being clinically managed to beingsupported through a recovery phase to increasetheir confidence to be able to self-manage theirown health with support through monitoring andtimely access should problems occur.
To facilitate this cultural shift clinical teamswere offered:• Assessment tool training• Motivational interview training.
The sites tested different methods of informationdelivery to meet the learning needs of theindividual patients. This included informationdays, health and wellbeing clinics, survivorshipcourses, one to one sessions, and informationprescriptions.
The care plan resulted from a needs assessmentand sites tested various assessment tools includingself-assessment to focus the conversation on theneeds of the individual. As an outcome from theassessment patients would be referred orsignposted to support services that could supportmeeting their needs.
The treatment summary provided a useful tool forpatients and GP’s to understand the disease stage,what treatment the patient received, amanagement plan and what to look out for in thefuture. This was either part of the care plan or aseparate document.
Hand held records were developed or modified inseveral of the sites to include the treatmentsummary, key information and contacts shouldthe individual need advice or support.
What we found• Clinicians may need additional skills to managethe transition in moving patients from a medicalto a self-management model of care
• Assessment and care planning is timeconsuming and needs to be focussed on theconversation and what makes a real differenceto the individual patient
• Information is power, and the confidence thisgives the individual in knowing about theirdisease and what to look out for and takecontrol of their own health is critical to enableself-management
• Care coordination requires professionals acrossall sectors to communicate effectively to providea consistent service and to respond to needsproactively where appropriately thereby avertingcrisis intervention.
13Stratified Pathway of Care: Care Coordination
www.improvement.nhs.uk/cancer/survivorship
The most surprising and pleasing thing about this project was discovering what facilities alreadyexisted in the community and that by exploring these and networking with providers we couldgreatly enhance our service simply by being aware of existing services and using them properly.“
”Healthcare Professional
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 13

ACKNOWLEDGEMENTS
14 Stratified Pathway of Care: Remote Monitoring
www.improvement.nhs.uk/cancer/survivorship
We are grateful for the enthusiasm andcommitment of all the test site teams to thiswork over the past year. You have all embracedthe changes with determination and resolveand the scale of what has been achieved insuch a short timescale has been commendable.We will continue to develop and learn fromyour experience and trust you will be theambassadors for change in your organisationand beyond in the future.
Our thanks go to Adam Glaser our NationalClinical Lead and the four National ClinicalAdvisors; Mick Peake, John Griffith, DorothyGoddard and Roger Kocklebergh for theirclinical leadership during this phase of testing.
Our special appreciation to Noeline Young,NCSI Project Manager, and to colleagues fromMacmillan Cancer Support, Breast Cancer Care,Beating Bowel Cancer and the Prostate CancerCharity for their advice and support over thepast year.
Finally, our thanks to the IT development teamat North Bristol NHS Trust and John McFarlaneat Royal United Hospital Bath for their supportin the development of a remote monitoringsolution.
Through your work we now have a wealth ofexperience knowledge and skills to take thisagenda forward and continue to improve thequality and effectiveness of services for thoseliving with and beyond their diagnosis ofcancer.
Thank you all again for your contribution.
NHS Improvement -Adult Survivorship Team
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 14
I hold a firm belief that both medical and psychological care go hand in hand insupporting patients through their personal journey of cancer. The project hasallowed the focus to shift away from the medical model to a more holisticapproach for all patients. It has helped me to think outside the box in helpingpatients feel more empowered both physically and emotionally.
Cancer Nurse Specialist
“
”
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 15

NHS Improvement3rd Floor | St John’s House | East Street | Leicester | LE1 6NBTelephone: 0116 222 5184 | Fax: 0116 222 5101
www.improvement.nhs.uk
NHS ImprovementNHS Improvement’s strength and expertise lies in practical service improvement. It has over a decade ofexperience in clinical patient pathway redesign in cancer, diagnostics, heart, lung and stroke anddemonstrates some of the most leading edge improvement work in England which supports improvedpatient experience and outcomes.
Working closely with the Department of Health, trusts, clinical networks, other health sector partners,
professional bodies and charities, over the past year it has tested, implemented, sustained and spread
quantifiable improvements with over 250 sites across the country as well as providing an improvement
tool to over 1,500 GP practices.
Delivering tomorrow’simprovement agendafor the NHS
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
NHSNHS Improvement
Pathway to Improvement:Survivorship 15/3/12 16:00 Page 16