nhs scotland nmahp ehealth network learning workshop …• continued roll out of trakcare for all...
TRANSCRIPT

NHS Scotland NMAHP eHealth Network
Learning Workshop 8th June 2016
#eNMAHP

Welcome
Today's Programme Prizes/Draw Rules
Evaluation Survey QR #eNMAHP
Reflections : How Far Have We Come?
Lesley Holdsworth
Hugh Masters
Tracy MacInnes

Eunice Muir

National Services Scotland
Tina Watson

We’re a national NHS Board operating right at the heart of NHSScotland. Through our services we provide invaluable
support and advice. A role we also extend to the wider public sector
Tina Watson, Transfusion Practitioner
National Services Scotland



NHS Ayrshire and Arran
Karen Lauder

NHS Ayrshire & Arran This year’s key eHealth issues for us




What’s gone well and why?
• Mobile working pilot
• Improved reporting functionality
• Starting meaningful conversations in H&SCP

What happened next?

Our top three priorities going forward
• 1. Infrastructure to support mobile working
• 2. Devices to support mobile working
• 3. Progressing Integration
What we need from the network?
• Support to encourage Boards to take strategic approach to infrastructure


Greater Glasgow and Clyde
Michelle Wardrop

Greater Glasgow & Clyde


E HEALTH
• Rationalise the number of systems across GGC and consolidate around 3 cornerstone applications
• Clinical Portal
• Universal GP it services through EMIS
• Reduction of Patient Management Systems from 20 -1 using TRAKCARE,
• improved information provision to managers and clinicians using Micro strategy

Clinical e Health Team
1 wte Medical e health consultant
0.8 wte AHP ehealth leads
2.0 wte ehealth Project nurses


Nursing
• Nursing documentation is moving towards developing EPR that will follow the patient through their pathway regardless of specialty
• Huge process of streamlining documentation so that it is patient centred fast and efficient and also meets the need of nursing standards

AHPs
• All AHPs within GGC will be using a PAS system in the form of TRAKCARE or EMIS by the end of 2016
• All AHPs with some exceptions will be using an EPR by the end of 2016.
• All will have access to Microstrategy for reporting to inform work force planning locally and to inform the Operational Measures

GGC
• Clinical portal from GGC to Lanarkshire data sharing pilot project happening now.
• GGC data set shared with West Dunbartonshire Council and vice versa
• GGC sharing data with Glasgow City Council
• AHP - Development in SCS of digital platform by OT services.
• Annonymised data sharing in TOMs project between SLT in GGC and RCSLT to inform outcome measures

Health & Social Care
Information Strategy
Pieter van de Graaf
SG eHealth & Health and Social Care Analysis Divisions
NHS National Information Leads Group
“Improve how health system information is used
to drive quality improvement“
“..greater use of big
data and technological responses,
underpinned by a public health data and
technology strategy”
“The NHS collects a huge
array of information and this
valuable resource can be put
to use by creating the
concept of a learning care
system”

Current Issues:
• competing demands for management information and
business intelligence, professional decision support,
and data for national reporting and research
• lack of coordinated leadership on information
priorities
• lack of feed-back of higher-level outputs and outcomes
to local decision making
• duplication of data capture and analysis with a need
for an improved shared services approach in some
areas.

Information Strategy – Draft Vision
“As a citizen of Scotland, I have access to the
information I need to help improve my health and
wellbeing. I expect my health and social care
information to be shared securely with the service staff
that need to see it, and that data will be used
appropriately to help plan services, enable research &
innovation and ultimately improve outcomes for
everyone.”

Learning Care System Approach
• Joint decision making between the citizen and the multi-disciplinary
care team
• Use of integrated health and social care information for decision
making from a diverse range of sources
• Integration with information beyond traditional care data, such as
genomic, environmental and socio-economic information
• Aggregating and using information beyond the context of an
individual citizen
• Consistent feed-back loops ensuring that each decision at each level
is informed by the outcomes from earlier actions

Targeting Improvements
Use
Capture
Store/
Manage
Interrogate/ Analyse
Visualise/ Contextualise
Identifying outcomes
Coding
Matching
Customisation
Decision support
Information
Data
Knowledge

Discussion Points
• What are the key issues in practice in relation to
information for NMAHPs?
• Where should improvements be targeted and how could
the NMAHP network help?
• What are relevant examples of good practice we could
share amongst and beyond NMAHPs?

Lynne Douglas
AHP Director, NHS Lothian
Co-Chair of AHP Operational Measures Steering Group
@lynneahpd

AHP Operational Measures 2012 SG National Delivery Plan item 6.1 said that AHPs should be able to “monitor the quality of AHP service delivery, including user experience, by implementing the national data
set and using quality measures/dashboard agreed for national and local reporting, particularly in relation to the nationally agreed outcomes for integration of health and social care services”
Deliverable not achieved by end of NDP in 2015 so SG and ADSG set up steering group to address this and initiated project for NSS
Phase 1 from October – April (extended by 2 months due to issues in pilot board)
Aims were to test proposed dataset for accuracy, explore data currently generated in 2 pilot boards and test feasibility of bringing in AHP data from boards to ISD
The KPIs of the proposed dataset generated by the steering group are: Individual service user(s) clinical activity (including some basic outcome data and
not just number of contacts as in CC7)
Other clinically related activity Waiting times Workforce Episode of care (including some basic outcome data)

AHP Operational Measures KPIs
Work force
Referral (Demand)
Clinical Activity (Service
user)
Other Activity
(Population)
Episode of Care
Waiting Times
The total number of AHPs employed in
Health & Social Care
The number of new service users
referred or self referring to a specific AHP Profession or
Service in a given
time period.
How long a service user has to wait from receipt of referral to first contact (this may be a direct or indirect
contact and may not involve a clinician seeing the service user)
Activity is the time spent on clinical work completed by
AHPs that can be attributed to an individual or group of
service users
The time spent on other clinically related activity
completed by AHPs not attributed to an
individual or group of service users but is still part of the AHP role i.e.
public health work, non-specific advisory
work, educational sessions
An AHP episode can take place in any setting and is initiated by a referral or admission that involves
a first contact and is ended by a discharge.
35

AHP clinical pathways
Referral Vetting 1st Contact Inter-vention(s)
Onward Referral/ Transfer
Discharge Outcome
To Self Care & NHS24 MATS Data To other care
Referral & Waiting Times Episode of Care
Illustrating Service Users Care Journey & Data Capture
Operational Measures Patient Level Data Submitted to ISD

Data from AHP clinicians N.B. Data will fall out of existing electronic systems without
the need for duplication of recording where possible

Health Board: HB1 No. of Referrals: 8,000 % of Scotland: 16%
Profession: PROF9 No. of Referrals: 7,500 % of Scotland: 15%
Mock AHP Operational Measures Dashboard
Service User Referrals Episode of Care Waiting Times
Workforce Individual Service User(s) Clinical Activity
Other Clinically Related Activity
HB1
HB8
HB4
HB5
HB3
Active Episodes of Care by Health Board
Scottish Average
HB1
HB8
HB4
HB5
HB3
Average Length of Input by Profession
Scottish Average
0
5000
10000
15000
20000
25000
July August September
Waiting Times Under 4 Weeks by Profession
Service user Clinical Activity in Profession Profession : PROF2
Contact type : TYPE4 % of clinical activity : 16%
Other Clinically Related Activity by Board
Health Board: PROF2 No. of hours per month : 14 % of total activity : 19%
HB1
HB9
HB10
HB4
HB2
HB7
HB3
Number of AHPs in Post by Health Board
Scottish Average

AHP operational Measures (cont.) The report at the end of phase 1 will include business case
proposals for phase 2 as well as conclusions for the aims Accuracy of dataset
Data currently collected
Infrastructure in boards and mechanics of data transfer to ISD
It will be circulated to AHP Operational Measures Steering Group, AHP team in SG and the ADSG at the end of May
Poster to be presented about project at NHS Scotland event
Initial support from AHP team in SG to continue project through more development phases aiming towards a Business As Usual project in ISD at some point in the future

Questions?
Additional questions can be answered by the ISD project team
Or by Euan McComiskie, AHP Advisor, ISD
[email protected] @EMAHPInfo

Coffee Remember to Visit Exhibitors
Back for 11.40
#eNMAHP

NHS Grampian
Helen Chisholm

NHS Grampian – This year’s key eHealth issues for us
• Continued roll out of Trakcare for all AHP MSK services
• Use of technology to support discharge planning for amputees
• Development work in Community Nursing – SCI Gateway referrals & Vision Community Module
• Development of video consultations within OPD at Dr Gray’s
• Use of technology for diabetes education with patients and healthcare professionals

What’s gone well and why
• Providing Data – supporting caseload/waiting list management and service improvement
• Excellent collaboration between services, eHealth and health intelligence colleagues
Amputee project
• Feasible, acceptable, effective and efficient
• Potential impact on length of stay, patient experience, cost savings
“It was brilliant - it made me feel that my input to the experience was important. It made me feel very positive, and made me aware of the practicalities required for my release from hospital. I was very happy we were able to do things this way.”

Our top three priorities going forward
1. Robust caseload management/scheduling tools for community nursing & AHPs – releasing time to care for patients
2. Further development of video consultation across NHSG
3. Further development of technology being used to communicate with & educate patients/HCPs
What we need from the network – support & sharing of experiences from across Scotland

NHS Fife
Ben Morrison

NHS Fife This year’s key eHealth issues for us •E-Communication.
•Use of Technology to further support Tele-health and Tele-care.
•Ongoing development of current systems.

What’s gone well and why
• Text Reminder.
• Roll out of LYNC.
• IPAD work.
• Tiara Development Group.
• Set up of AHP E-Health Delivery and Clinical Groups.

Our top three priorities going forward
• 1. Sharing the learning event in September.
• 2. Rolling out Electronic Pages to services.
• 3. Using video calls and emails with patients to reduce face to face contact.
• Continue to share learning from the network to help support ongoing developments.

NHS Dumfries and Galloway
Justina Ritchie
Linda McKechnie

Community Mental Health
Dataset • Isd CHAD Dataset
• New coding
• Dataset changes
• Formstream File Note
• Drop downs developed

Qlikview Dashboard
• Reporting of CHAD • Analysis of Performance
Activities and Outcomes

Key Challenges for 2016/2017
•Financial situation
•Pressure on service to have clinical development time
•Change management locally

NHS Borders
David Thomson

NHS Borders This year’s key eHealth issues for us •Integration – systems access and links
•Remote Access & Coverage in rural areas
•Support Systems replacement
•Internet Access for patients
•Prioritisation & Finance
•Project support

NHS Borders • Reactions:

NHS Borders What’s gone well and why
• Service & Clinical Engagement especially IM&T working with clinical staff
• JET Dashboard
• Ward View, supporting Patient Flow
• Whole System approach

NHS Borders Our top three priorities going forward
1. Replacement for Community System incl NMAHP engagement as end users
2. Electronic Patient Records & Communications
3. Integrated systems for Primary, Secondary and Social Care incl TeleHealth Care
• What we need from the network • View of the collective
• Shared Information on Successes
• National eHealth Strategy & Implementation plan including any support to our Board

eNMAHP Round Table Discussion Lesley Holdsworth
•Our Biggest achievement of the last Year
•Networks top 3 priorities for 2016/2017

Round Table Discussions Achievements
Challenges

NSS Discovery
Jamie Gray- NSS
Information for
Quality Improvement,
Benchmarking
Performance Management

NSS Discovery - What is it? Provides comparative information to help review, monitor and plan services and support quality improvement.

NSS Discovery - Who is it for?
Provides managers , analysts and clinicians with comparative and benchmarking information to underpin service planning
and delivery.

NSS Discovery - What does it show?
1. Presents information at NHS Board, Hospital & specialty level . 2. Authorised users can access more detailed information, including patient level data, to support further
investigations 3. Comparisons with Scottish, English and Welsh benchmarking data will be available within the system

NSS Discovery - Examples of how it can be used?
To see where my Board’s residents are being treated and what they are being treated for
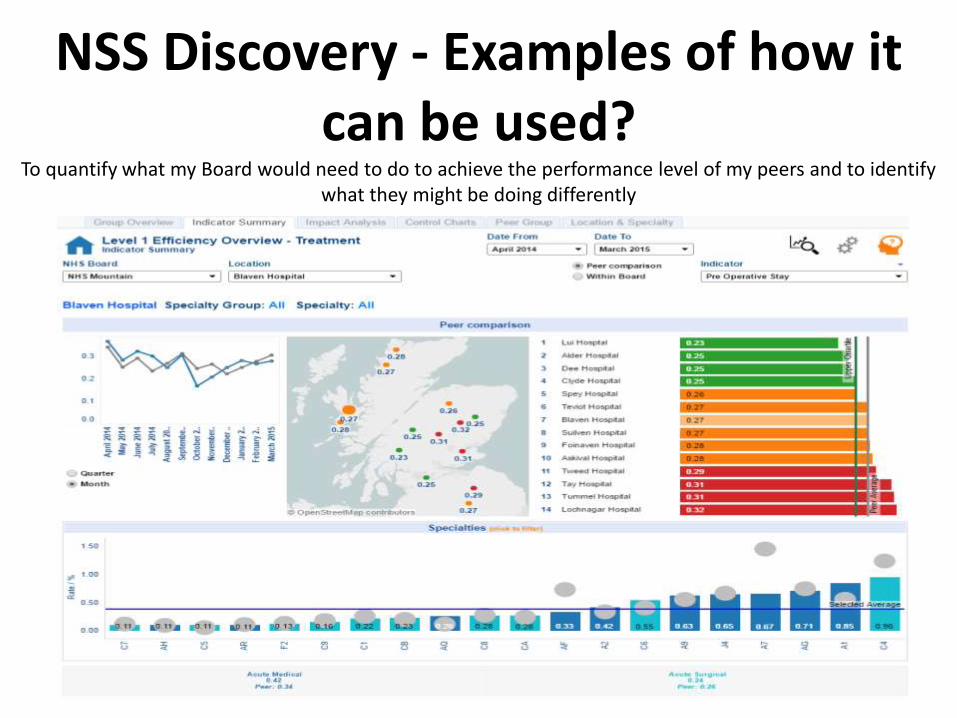
NSS Discovery - Examples of how it can be used?
To quantify what my Board would need to do to achieve the performance level of my peers and to identify what they might be doing differently

NSS Discovery - Examples of how it can be used?
To identify productive opportunities within a specific field e.g. potential areas for increasing the number of Day Case surgeries

Topic Measures
Alcohol AM1] % of mothers recorded at booking as screened for alcohol use in the last three months
AM2] % of mothers identified at booking as drinking1 or more units a week in the last three months
AM3] Number of alcohol brief interventions carried out in maternity setting
Breastfeeding BF1] Exclusive breast milk feeding percentage at first visit (10days)
BF2] Exclusive breast milk feeding percentage at first 6-8 week check
Drugs
DM1] % of pregnancies where illicit drug use is recorded
DM3] proportion of singleton babies with
A) low birth weight
B) pre-term birth
C) small head circumference
Smoking Smk1a: % of pregnant women identified as current smokers (at booking); or
Smk4: proportion of pregnant women who successfully quit smoking (assessed at 1 month from quit
date) during pregnancy (per 1000 identified as smokers at booking)
Mode of Delivery
% live singleton births by mode of delivery
27-30 month review
% of eligible children reviewed
• Age group at review
% children reviewed with no concerns
% children reviewed with at least one concern
• % by developmental domain
•% by deprivation
•% by gender & ethnicity
NSS Discovery – Maternity Dashboard


Excellence In Care
•Provide a secure, fit-for-purpose, Scotland-wide nursing and midwifery benchmarking, performance and continuous improvement monitoring tool and that will be complimented by a support service (wrap around service).
•It will meet the requirements of stakeholders (NHS Boards and Scottish Government) and incorporate agreed deliverables stated in the Scottish National Approach report ‘Excellence in Care’.

Excellence In Care
Phase 1 - Data and metrics development and build a benchmarking, quality improvement and management tool for acute adult nursing, by end March 2017. Phase 2- Data and metrics development and build a benchmarking, quality improvement and management tool for acute maternity and paediatric nursing, - by October 2017. Phase 3 - Data and metrics development and build a benchmarking, quality improvement and management tool for mental health nursing, interface - by March 2018.

The NSS Visualisation Estate
Source
Discovery
Primary Care
Procurement
District Nursing
NHS Network Public Internet
Prescribing
Audits
Excellence in Care Nursing Dashboard
Excellence in Care Nursing
Dashboard

NSS Discovery- Not just a tool, but a
service!
NSS Discovery incorporates a professional, customer focussed support service in response to user requests and to assist users in maximising the utility and effectiveness of the information
contained within NSS Discovery.

For more information on accessing and using NSS Discovery, email us at:
or
visit our website: nss.discovery.scot.nhs.uk

Scottish Government eHealth Website and Communications
Nicola Radley
eHealth Clinical Strategy Manager



Case Studies
• Sharing good practice • Using digital technology
to support safe, effective, person centred care
• NMAHPs are a rich source

Thank You
@eHealthScotland
#eNMAHP
www.ehealth.nhs.scot

Lunch Remember to Visit Exhibitors
Back for 1.30pm
#eNMAHP

A Technology Enabled Workforce
Sharon Levy
University of Edinburgh

The Technology
Enabled Workforce
Sharon Levy RN

Global
nursing
market

My UG students
eHealth & Digital nursing Young(er) digital natives

In the next 18 minutes…
Me, me, me…
Reflection on clinical IT and nursing
(workforce)
eHealth training and education
The vision
Questions???

My journey

Designing a website for nurses (1996)

The notion of caring and (information technology) revolution do
not appear to go comfortably hand in hand yet it seems that
revolutionary thinking is necessary to facilitate advances in nursing practice to take place … ...an account of a computing project
which has taken place in an NHS trust hospital aimed at
incorporating the World Wide Web as a resource for nurses and
midwives in facilitating practice development. It is argued that a
computer will never be able to replace the physical care given by nurses to people, but that it has the potential of providing access to a comprehensive nursing knowledge resource which could
support research based practice to address care needs. LEVY, S.
& FLECK, E. (1997) Focusing on needs: an Internet link for nurses.
Nursing Standard, 11, 1-5

Computers in clinical practice
Perth & Kinross 1997

Computers will reduce paper-wok
Strongly Agree
Agree
Disagree
Strongly Disagree
Don't Know
Missing
The P&K Study Results n = 513

IT will improve communication
Strongly Agree
Agree
Disagree
Strongly Disagree
Don't Know
Missing

Record work-load accurately
Strongly Agree
Agree
Disagree
Strongly Disagree
Don't Know
Missing

Computers enable quick access to info
Agree
Strongly Agree
Disagree
Strongly Disagree
Don't Know
Missing

Conclusion
Prior to implementation:
Overwhelming positive attitudes
High proportion of staff who believe that current information gathering is inefficient.

Telehealth, Telecare….
LEVY, S., JACK, N., BRADLEY, D., MORISON, M. & SWANSTON, M. (2003) ‘Perspectives on
telecare: the client view’ Journal of Telemedicine & Telecare, 9, 156-160.
LEVY, S., BRADLEY, D., MORISON, M., SWANSTON, M. & HARVEY, S. (2002) ‘Future patient care:
tele-empowerment’ Journal of Telemedicine & Telecare, 8, 52-4.
BRADLEY, D. A., WILLIAMS, G., BROWNSELL, S. J. & LEVY, S. (2002) ‘Community alarms to Telecare
- the need for a systems strategy for integrated telehealth provision’ Technology & Disability, 14, 63-74.
LEVY, S., BRADLEY, D. A., MORISON, M. J., SWANSTON, M. T. & HARVEY, S. (2002) ‘Community
nursing in the tele-first century: fiction or reality?’ Journal of Community Nursing, 16, 4-9.
LEVY, S., BRADLEY, D. A. & SWANSTON, M. T. (2002) ‘The technology prescription: linking telecare
and informatics by using a need-led paradigm’ Health Informatics Journal, 8, 88-94.
LEVY, S., BRADLEY, M. J. M., SWANSTON, M. T. & WILSON, S. (2001) ‘Power as a concept in the
evaluation of telehealth’ in Organisation Development In Health Care RUSHMER, R. K., DAVIES,
H. T. O., TAVAKOLI, M. AND MALEK, M. (Ed.) Strategies issues in health care management
Edinburgh, Ashgate Publishing Ltd.
BRADLEY, D., LEVY, S. & BROWNSELL, S. (2001) ‘From caring home to smart house: a needs led
evolution’ New Technology in the Human Services, 14, 18-28.

‘National Programme for IT starts October 2002
Initial studies on clinical engagement focused solely on Doctors and these survey results grabbed the headlines
The biggest IT project in
the world EVER…

RCN E-Health Surveys
Year Responses
2004 2,020
2005 1,776
2006 4,451
2007 2,635
2010 1313
2012 1158

04 05 06 07 10 12
Fully
adequate
Reasonably
adequate
Inadequate
None 53% 22% 26% 17% ----- -----
Have you had adequate
information about NHS IT Developments

04 05 06 07 10 12
Fully
adequate
Reasonably
adequate
Inadequate
None 63% 63% 62% 66% 54% 46%
How much consultation has there
been with you about introducing eHealth in your workplace

04 05 06 07 10 12
Very
important
68% 65% 58% 69% 90% ----
Important 24% 24% 29% 23% 8% ----
How important is IT training to the success of (eHealth)

04 05 06 07 10 12
None 51% 54% 57% 55% 52% 53%
How much IT training have you
had in working time in the last 6 months

2012: Positioning nursing in
the digital world


My UG students
eHealth & Digital nursing Young(er) digital natives

Understanding
and
knowledge
Preparing for
Practice
Learning through
practice
• eHealth landscape
• IT Security • Information
governance • Informatics
• Access to a ‘playground’ of
electronic training systems
• Scenarios linking to patient pathways stimulating
reflective practice
• Full read and write capability to interact with clinical systems on placements
• Under supervision of
mentor/supervisor • Increased
competence leading to enhanced understanding and knowledge
Developing Technology Enabled NMAHPs in Scotland
Steps in the Pre-registration Journey:
through training to qualification
Higher Education Setting NHS Setting
Staff with
understanding,
knowledge
and practical
technological
competencies
that support
Scotland’s
triple aim
enhancing the
efficient
delivery of high
quality person
centred care
=
✔

Developing understanding and
knowledge
• eHealth policy and practice landscape
• IT Security
• Information governance
• Informatics • Digital skills
To ensure that the pre-registration
NMAHP workforce have
demonstrable
competencies in relation to their
theoretical understanding
and knowledge of ehealth in line with
professional
requirements
• Range of easily
accessible online modules
• Nationally endorsed
• Used by all HEIs
• Accessed through NES
Why? In what? Through?
1. Develop national resources
2. Endorse available others
3. Review
available others, ‘tartanise’ and rebrand
Options?
• Review resource implications of
‘tartanising’ Sheffield modules
• Develop a set of costed
recommendations for
consideration
Suggested approach
By end of????
Timescales
Key Drivers
• Setting the
Direction
• NDP / ALIP
• Everyone Matters
• Vision for a
Healthier Scotland

Preparing for Practice
• practically
navigating electronic care systems in the learning
environment • Using
electronic systems to support reflective and educational
development
To ensure that the
pre-registration NMAHP workforce
have practical eHealth
confidence and competencies
• Having access within HEI settings to a range of
electronic systems that are similar to those found within placement settings
Why? In what? Through? • Systems
suppliers provide access to training modules creating a ‘playground’ that HEIs can
easily access • HEI access
through SWAN/NR3 network
Options?
• Suppliers approached to
establish appetite for such an
approach
• Develop a set of costed
recommendations for
consideration
Suggested approach
By end of
???
Timescales
If progressed: • develop a prototype
and ‘test’ within
Edinburgh University • Present findings at
BCS summit in October 2016

Learning through Practice
• in the administration of clinical patient management
systems and understand how they can be used to contribute to shaping
patient care plans
To ensure that the
pre-registration NMAHP workforce
can competently use electronic
systems to support patient care and their own learning experience in line with professional
registration requirements
• NHS boards
facilitating full read and write access to clinical systems for all NMAHP students on placements under supervision
of clinical supervisor
• HEIs utilising this experience within the educational
environment
Why? In what? Through?
1. HEIs negotiate locally to determine where
responsibilities lie
2. A national, consistent approach is agreed
Options?
• Establish full national picture in
relation to access
• CNO/CHPO publish a position
statement about how this
should be achieved detailing
where responsibilities lie for
enabling
Suggested approach
By end of
???
System
specifications to
enable this shared
with suppliers

The end!

NMAHP eHealth Network
Margaret Allan

Quality Framework
Electronic Drug Cupboards
Digitally enabled Pre-operative Information
Trakcare

Wardview
Synopsis Project
Vital Signs Project

Thank You

NHS Forth Valley
Catherine Ritchie

NMAHP
Maternity Webpage
Apps
Podcast Development
HePMA


AHPs ([email protected])
Dietitians Week
NHS Scotland Poster Event
Innovation Award
BDA Ibex Award
AHP eHealth Team

NHS Western Isles
Karen France

Patient Centred Care Pathways
• Why?
– Traditional ways of working are not cost or time efficient
– Unnecessary travel (and appointments?)
– 4% of income goes on patient travel
– Need to improve patient experience and allow patients to design their own pathways
– Appetite to change and be more innovative

5 themes
– Proactive secondary care
– Anticipatory Care Pathways
– TEC
– DOIT Referral Pathways
– Patient Travel and Video Conferencing

– Increase patient satisfaction
– Outcomes the same as, or better than before the changes
– (Reduce spend)

NHS Lothian
Laura Sandison

NHS Lothian This year’s key eHealth issues for us •Implementation of Paperlite
•Health and Social Care integration
•Developing close links between Nursing, Midwifery and AHP Informatics Groups to share best practice and solve common issues
• Enhance NMAHP presence and impact on eHealth and on Trak Boards

What’s gone well and why
• AHP SuperUser network
• AHP Informatics Group
• Community Nursing Informatics Group
• Maternal and Child Health Informatics Group
• NMAHPs representation at TrakCare Boards
• National leader for preparing for implementing Scottish Government Operational Measures
• Implementation of the following: – SCI store / Clinical Portal / Emergency Care Summary (ECS) / Key Information Summary (KIS) / Secure
Global Desktop (SGD)

Our top three (four!) priorities going forward
1. Improve Health & Social Care Integration and support new model of care/GIRFEC
2. Lothian wide implementation of Paperlite
3. Improve & enhance the technology and data underpinning NMAHP Quality Improvement projects.
4. Lothian NMAHPs to be National Leaders in eHealth developments and improvement programs
• What we need from the network – Support NMAHPs in all eHealth projects and help provide a voice to promote our eHealth priorities
Content provided by Euan McComiskie, Fiona Stratton, Caroline Myles, Helena Aitken, Lorraine Somerville & Marina Copping and collated and presented by Laura Sandison Physiotherapist, Western General Hospital

NHS Highland
Helen Bryers/Mark Fleming

NHS Highland This year’s key eHealth issues for us • New e-health governance structure
– Strategy, Delivery and Clinical reference groups
– Main aim: • Develop electronic patient record & clinical portal view
• Fully integrated & shared between disciplines including lab results
• NMAHP e-health group – Supports local projects such as digital pens &
Florence/Motiva (text messaging & clinical support)

Overview what’s gone well
• Implementation of ‘ward view’
• Community nursing team using digital pens
• Midwives use Florence text message system for:
– postnatal care & public health messages
– supporting mothers’ awareness of fetal movements
• Why? – staff are keen to take these forward

Our top three priorities going forward
• E-record: Expansion of PMS/electronic dashboards/clinical letters to SCI store/Maternity module
• AHPs & community nursing working on replacement for
MIDAS system (currently used in A&B) • AHPs looking at implementation of AHP operational
measures & e-system to support • Keep all the small projects going/encourage staff to use
technology to support practice
• What we need from the network: LEARNING from others

QUIZ !! Answers Prize!!
Whilst Mark sets up Brendan!!

Digital Health and Care Institute Top 5 Projects
Relevant to NMAHPs
Brendan Faulds

NHS Glasgow approach to eHealth Leadership
Catherine McGee

Catherine McGee
AHP e Health Clinical Lead GGC

Greater Glasgow & Clyde


NHS Greater Glasgow and Clyde
The review is to ensure that as an organisation we are appropriately structured to meet the demands of wider organisational change .
• The advent of Health and Social Care Partnerships
• The restructure to the management of Acute Services from a functional to geographical model
• Increased dependency and reliance on technology within core clinical services.
• Challenges of ‘round the clock' demands for our services
• Technological changes that require a skill set change and change of support approach.
• Potential impact of ‘shared services’ and other national drivers such as the e Health Strategy and Scotland’s
• Digital Future Framework

eHEALTH
• Rationalise the number of systems across GGC and consolidate around 3 cornerstone applications
• Clinical Portal
• Universal GP it services through EMIS
• Reduction of Patient Management Systems from 20 -1 using TRAKCARE,
• Improved information provision to managers and clinicians using Micro strategy

Clinical Leadership In e Health
• Clinical Leadership:
– eHealth Clinical Leads
– eHealth IT Consultant
– eHealth Nursing Leads
– eHealth AHP Lead

Clinical Engagement
• Empowerment
• Consultation
• Joint decision making
• Power sharing
• Democratic leadership
• Management by objective

Aim of the New Arrangements • Lead on eHealth enabled transformation, often
beyond their own area of clinical expertise
• Create direction aligning others around it.
• Assuring e health solutions are reflective of clinically derived priorities and have the widest possible sponsorship.
• Influence and engage colleagues across a broad range of stakeholders, linking to and influencing appropriately, extant management governance bodies,
• Systematically ensure that clinicians views and needs are driving decision making


The e health strategy board ensures alignment of e health strategy with key board( and partner) priorities and NHS Strategy and policy ; providing senior oversight to the prioritisation of the programme and its execution.
NHS GGC eHealth Strategy Board

Remit
• Develops the eHealth Strategy, ensuring
it is aligned and co-ordinated with key priorities, strategies, policies and wider service development and rationalisation
• Agrees priorities for delivery by the eHealth Programme Board
• Acts as an escalation body for issues, providing decision support to agreed programmes of work when required

• Develops plans for significant new investments including scrutiny of business cases and associated benefits realisation plans prior to presentation to the appropriate governance body.
• Approves budgets for eHealth Projects/Programmes
• Ensures effective links between eHealth (and Care) and the clinical and care community.
• Reports to the Chief Executive/Chief Officers Group

AHP eHealth Steering Group
• Streamline e Health AHP projects ideas
• Support existing projects
• Agree on eHealth priorities for AHPs
• Approve or reject project proposals based on the priorities.

AHP Operational Groups
• Staff at the core
• Operationalise priorities from the strategy and steering groups.
• Support and share ideas of lessons learned and the way forward

Success - Is it working ??

Coffee Break Please Visit Exhibitors
Back at 3.10pm
#eNMAHP

eHealth Headlines from The Clinical Strategy and OOH Services Review
Bettina Sizeland
Head of eHealth Strategy and Policy

Two major new policy initiatives published recently with eHealth implications
• The Clinical Strategy addresses
current healthcare challenges by proposing a greater focus on preventative measures and realistic medicine supported by broader integrated primary care services and well resourced specialist hospital centres.
• The November 2015 OOH Review recommends changes to current OOH and urgent care Practice to improve co-ordination and local service delivery.

The eHealth requirements
i) Digitising existing paper records eg casenotes. ii) Increased access to electronic patient records. iii) Electronic hospital prescribing and administration. iv) Real-time access to management information. v) Health and social care integration support for info sharing,
joint working. vi) Common shareable patient summaries for health and social
care. vii) Electronic workflow management across systems eg ADASTRA
and Trackcare. viii) Remote monitoring for rural/ remote areas. ix) Clinical intelligence for individual health outcome
improvement x) Patient and carer access to their health and social care
information for self management and joint decision making.

eHealth Actions – being progressed
• Increased access to electronic patient records. Regional clinical portal cross-border work, Board level clinical portal rollout to GPs and community services. Community system enhancement required and integration with GP IT systems.
• Real-time access to management information. Business
intelligence tools eg Microstrategy, Wardview, Tablau available and used in some Boards to manage capacity.
• Remote monitoring for rural/ remote areas. National TEC programme supports video conferencing and home monitoring solutions.

eHealth Actions – under development
• Electronic hospital prescribing and administration. Full business case for national delivery. Further work required to develop medicines reconciliation standards and solutions.
• Information sharing between health and social care providers. ISB
work has supported information exchange platform and H&SC portal development, unique identifier and data matching development. National information governance agreed. Further work required to identify local support required.
• Common shareable patient summaries including health and social care information. ECS rollout to scheduled care and under consideration for community pharmacy. Electronic ACPs being specified and used to identify those at risk. Further work required to identify social care summary requirements.

eHealth Actions – further work required • Digitising existing paper records. Case notes, nursing notes, social work notes
mainly paper. Work required to develop and digitise joint assessments, care plans.
• Electronic workflow management across systems. Issues noted in OOH review for ADASTRA around variation in implementation. Cross-boundary Clinical portals and integration arrangements such as federated trackcare should offer workflow improvements.
• Clinical intelligence for health outcome improvement. Currently limited to research and some clinical areas eg cancer, diabetes, renal. Existing local and national business intelligence tools eg Discovery are being developed to provide clinical intelligence.
• Patient and carer access to health and social care information and services.
Patient portal, TEC digital platform development, NHS24 web landscape review will offer technical solutions. GP digital services fund will deliver basic online services. Further work required to incorporate social care information and embed for self management and joint decision making.

Thoughts on priorities/ actions?
• Gaps/ opportunities
• Low hanging fruit?

NES eNMAHP Leadership Programme
Ann Rae
Jane Harris

Quality Education for a Healthier Scotland
Evaluation of the Impact and
Enhancement of the NMAHP
Leadership Programme: eHealth
Applications in Healthcare
Ann Rae and Jane Harris
June 2016

Quality Education for a Healthier Scotland
Methodology
Demographics
Satisfaction Impact
Recommendations

Quality Education for a Healthier Scotland
Discussion
NMAHP
eHealth
Network
supporting
the
programme

Priorities for 2016/2017 Table Top Discussion
Lesley Holdsworth
Mark Fleming

Priorities for 2016/2017

NMAHP Priority eHealth Issues
Jackie Stephen
eHealth Lead
NHS Borders

Jackie Stephen NHS Borders Ehealth Lead
eHealth Strategy 2014-17 Update

eHealth Governance
** Information Sharing Board also reports to Local Authority Sectoral Board
Board Governance Board Collective Governance Scottish Government Led Collective Governance
Cabinet Secretary Chief Executives Group
Scottish Government H&SC Management Board
NHS Board Internal Governance Clinical Change Leadership
Group eHealth Strategy Board
eHealth Leads (NHS Boards)
eHealth Programme Board
Portfolio Management Groups
Existing Systems
National Systems
Programme and Project Boards
Board and Consortium
Programme and Project Boards
Safer Medicines Working Group

A Consistent Journey

• To enhance the availability of appropriate information for healthcare workers and the tools to use
and communicate that information effectively to improve quality.
• To support people to communicate with NHS Scotland, manage their own health and wellbeing,
and to become more active participants in the care and services they receive.
• To contribute to care integration and to support people with long term conditions.
• To improve the safety of people taking medicines and their effective use.
• To provide clinical and other managers across the health and social care spectrum with the timely
management information they need to inform their decisions on service quality, performance and
delivery.
• To maximise efficient working practices, minimise wasteful variation, bring about measurable
savings and ensure value for money.
• To contribute to innovation occurring through the Health Innovation Partnerships, the research
community and suppliers, including the small and medium enterprise (SME) sector.
eHealth Strategic Aims

The Goals – Mutually Supportive
By 2020 there will be a Personalised Electronic Patient Record so that individuals are enabled and confident to digitally access and jointly manage the health and care information that is important to them and their wellbeing.
Health and care workers can access the information they need relating to an individual from an Electronic Patient Record in order to provide the best healthcare possible for that individual.
For patients and service users For health and care workers

1. Ensuring what is in place is fully resilient and
meets current and future core service
demands.
2. Fully exploiting the investments already made
in existing systems, filling key functionality
gaps and installing the change programmes
that will increase the efficiency of current
processes.
3. Being more innovative and ambitious,
identifying and committing to projects that have
the potential to be transformative and either
directly or indirectly cash releasing.
The High-Level Challenges

eHealth Budget 2016-17
• Revenue Based (no specific capital provision)
• 2015-16 – core £88m
• 2016-17 – core £77m with additional budgets of:-
• £3m for HEPMA
• £9m for Technology Enabled Care (telehealth/telecare)
• £2m revenue , £2m capital(plus £2m c/f) for Primary Care digitalisation
• “Bundled” with main allocation.
• SG contribution is roughly one third of
NHSScotland IT budget (£250m last IM&T
survey) • 2% of 2016-17 NHSScotland overall budget

Meeting Current And Future Core Service Demands
(Examples)
• Renewal of client and server infrastructure (local and national).
• Upgrading of server and desktop operating system environment.
• N3 to SWAN migration.
• New NHSMail service (with enhanced collaboration services).
• Atos MTS extension with infrastructure replacement.
• MiDIS replacement.
• Additional shared services.

Filling Key Functionality Gaps And Making Current
Processes More Efficient
(Examples)
• Mobile capability – in premises and in the field.
• Digitalisation and eForms.
• CHI transformation (single point of positive patient
identification and record locator service).
• Child Health transformation (national and local).
• Hospital Electronic Prescribing and Administration
(HEPMA).
• National Patient Management System Rollout.
• GP IT Re-provisioning.
• Health and Social Care integration

Service Transformation
(Examples)
• Patient portal underpinned by a digital access platform.
• with two-way connections to Personal Health Management environments –
predominantly provided by commercial and third sector.
• Increased digital support for self-management.
• Technology Enabled Care Programme (integrated Telehealth and
Telecare at scale).
• Digitalising Primary Care (integrated with GP IT reprovisioning and with
community systems enhancement).
• Advanced Data Analytics.
• New Information Security Framework.

Outomes (bundling of allocations) vs collective management.
Local vs regional vs centralised (“Once for Scotland”).
Convergence vs opportunity. Personalised vs off-the-shelf/standard.
Innovation vs tried and tested.
Need to share vs need to maintain confidentiality.
Key Tensions

The Prioritisation Challenge
Demands + Expectations > Budget also > Skills Availability
Maintaining and refreshing existing estate and renewing
critical contracts
Supporting existing processes
“As is”
Increasingly paper-light ways of working and 24/7 business
Needs more resilient and “always on” systems
“As is” but greater capacity
Add new functionality and services
Service change and transformation

Questions??

Working Together The Network Going Forward
Lesley Holdsworth
Mark Fleming

Prize Draws

Evaluation
Closing Remarks
Lesley Holdsworth
Mark Fleming

Thanks You
Safe Journey
