nhs - payment by results · nhs payment by results ... four pronged approach to reform. this...
TRANSCRIPT

NHS Payment by results Topic Gateway Series
NHS payment by results Topic Gateway Series No. 41
1
Prepared by Liz Murby and Technical Information Service November 2007

NHS Payment by results Topic Gateway Series
About Topic Gateways
Topic Gateways are intended as a refresher or introduction to topics of interest
to CIMA members. They include a basic definition, a brief overview and a fuller
explanation of practical application. Finally they signpost some further resources
for detailed understanding and research.
Topic Gateways are available electronically to CIMA members only in the CPD
Centre on the CIMA website, along with a number of electronic resources.
About the Technical Information Service
CIMA supports its members and students with its Technical Information Service
(TIS) for their work and CPD needs.
Our information and accounting specialists work closely together to identify or
create authoritative resources to help members resolve their work related
information needs. Additionally, our accounting specialists can help CIMA
members and students with the interpretation of guidance on financial reporting,
financial management and performance management, as defined in the CIMA
Official Terminology 2005 edition.
CIMA members and students should sign into My CIMA to access these services
and resources.
The Chartered Institute of Management Accountants 26 Chapter Street
London SW1P 4NP
United Kingdom
2
T. +44 (0)20 7663 5441 F. +44 (0)20 7663 5442 E. [email protected] www.cimaglobal.com

NHS Payment by results Topic Gateway Series
3
Definition
‘Payment by results’ (PbR) is the name of the current funding flows mechanism
employed in the UK NHS. It is defined by the Department of Health in the
following statement of intent:
‘The aim of payment by results is to provide a transparent, rules based system for
paying trusts. It will reward efficiency, support patient choice and diversity, and
encourage activity for sustainable waiting time reductions.
Payment will be linked to activity and adjusted for case mix. Importantly, this
system will ensure a fair and consistent basis for hospital funding rather than
being reliant, principally, on historic budgets and the negotiating skills of
individual managers.’
Context PbR is a sector specific funding flows mechanism, although similar systems exist
in some other developed health economies. For this reason students are unlikely
to study this specific topic.
However, the topic has associations with the current CIMA syllabus. CIMA
students will learn and may be examined on this topic in paper P1, Management
Accounting Performance Evaluation, chapter 8, Developments in Management
Accounting and paper P2, Management Accounting Decision Management,
Chapter 10, Activity-based approaches.
Overview
PbR is part of the NHS reforms initiated by the NHS Plan (2000) which set out a
four pronged approach to reform. This approach has been described as a 'supply
side' and a 'demand side' reform programme.
A 2003 consultation (Payment by results: preparing for 2005) on the technical
aspects of payment by results, identified four principle policy directions that PbR
was intended to underpin.
Devolution: the belief that important decisions should be taken as close to the
patient as possible, within a national framework of standards and accountability.
Choice: the belief that patients should be able to take key decisions about the
care they receive from the NHS.

NHS Payment by results Topic Gateway Series
4
Plurality: the belief in a 'mixed' economy of public and private sector healthcare
provision. Over the last several years there has been a growth in independent
sector hospital provision in England. PbR makes the price of each procedure
transparent to all.
Investment: NHS investment is made on the basis that the NHS must spend the
money wisely and efficiently. The national tariff is the 'new' basis of NHS funding
and provides a series of benchmarks against which relative costs can be
measured.
Background and history Information setting out the recent history behind the development of the PbR
framework is found on the Department of Health website. www.dh.gov.uk
[Accessed 12 March 2008]
The NHS plan, together with Delivering the NHS plan, sets out a major
programme of NHS investment, expansion and reform over a ten year period.
Consequently, the PbR initiative is being implemented incrementally, in terms of
both scope and financial impact.
In terms of scope, PbR began in a small way in 2003-04 and was extended in
2004-05. For the majority of NHS Trusts, PbR included only elective care in
2005-06. The following year, PbR was extended to include non-elective, accident
and emergency, outpatient and emergency admissions for all Trusts.
2007-08 marked a year of consolidation with no significant changes to the tariff.
The financial impact of PbR was also introduced gradually with a four year
transition path, which comes to a close in 2008-09.
The relevant consultation processes governing these changes are outlined below.
Consultations and policy developments post 2000 In July 2000, the NHS plan introduced the government’s intention to link the
allocation of hospital funds to the activity undertaken by hospitals.
www.dh.gov.uk
[Accessed 12 March 2008]
In order to optimise extra resources, the government proposed major changes to
the way money flows around the NHS. The plan also included differentiation
between incentives for routine surgery and those for emergency admissions.
Hospitals would be paid for the elective activity they undertake, a system of
payment by results.

NHS Payment by results Topic Gateway Series
5
In November 2002, the government issued a response to the consultation paper,
'Reforming financial flows: payment by results', on plans for the introduction of
PbR. http://digbig.com/4wxqx
[Accessed 19 May 2008]
In August 2003, the government issued the consultation paper Payment by
results: preparing for 2005. This identified the key decisions needed for
implementing the next stage of PbR. It outlined how PbR will apply to NHS
foundation trusts from April 2004 and to all NHS trusts from April 2005.
Feedback was sought on the proposed approaches. http://digbig.com/4wxqy
[Accessed 19 May 2008]
Key elements of payment by results 1. The national tariff
The national tariff is the inflation adjusted national average cost of procedure.
It comprises three components:
• a definition (the healthcare resource group or HRG, backed up by detailed
clinical definition)
• a currency (the time spent in hospital, from admission to discharge)
• a financial sum (based on the NHS defined 'average' cost).
2. Healthcare resource groups (HRGs)
HRGs are a standard method of analysing clinical procedures and hospital
activity, based upon diagnosis and any interventions.
http://digbig.com/4wxra
[Accessed 19 May 2008]
3. The market forces factor (MFF)
The MFF is an adjustment to the tariff that reflects the different costs of
healthcare provision in different parts of the country.
It was developed to adjust the unavoidable variations in input costs, for
example, staff costs, regional weighting, land, buildings and equipment in
health care delivery.

NHS Payment by results Topic Gateway Series
6
4. NHS reference costs
NHS reference costs are an analysis of each HRG's spending at the end of the
financial year. They are a standardised presentation of the costs of NHS
services, prepared and published annually. http://digbig.com/4wxrb
[Accessed 19 May 2008]
The underlying intention of reference costs publication is to allow cost
comparisons between services through the use of a consistent approach to
costing.
Differences between reference costs and the tariff arise from:
• the effects of time related inflation, data collection and other adjustments
• a variation in the scope of each.
Application
How payment by results works 1. Tariff for hospital in-patient procedure
For each HRG, the Department of Health publishes tariffs (prices) for urgent
and non-urgent ‘spells’ (a ‘spell’ refers to time spent in hospital from
admission to discharge).
The tariff is based upon the inflation-adjusted national average NHS cost of
the procedure in question.
The prices are derived from Department of Health ‘reference costs’, which use
the cost information provided by all NHS providers as part of their annual
reference costs submission. They reflect the actual (rather than budgeted) cost
of procedures, and should ensure full recovery of all relevant support
functions and overhead costs.
2. Regional adjustment
This is an adjustment to the price, to reflect the fact that the cost of running a
hospital varies from one part of the country to another. This is known as the
MFF.
3. Income calculation
The price multiplied by the MFF represents the amount of income an NHS
Trust can expect to receive for each procedure it undertakes.
NHS Payment by results Topic Gateway Series
7
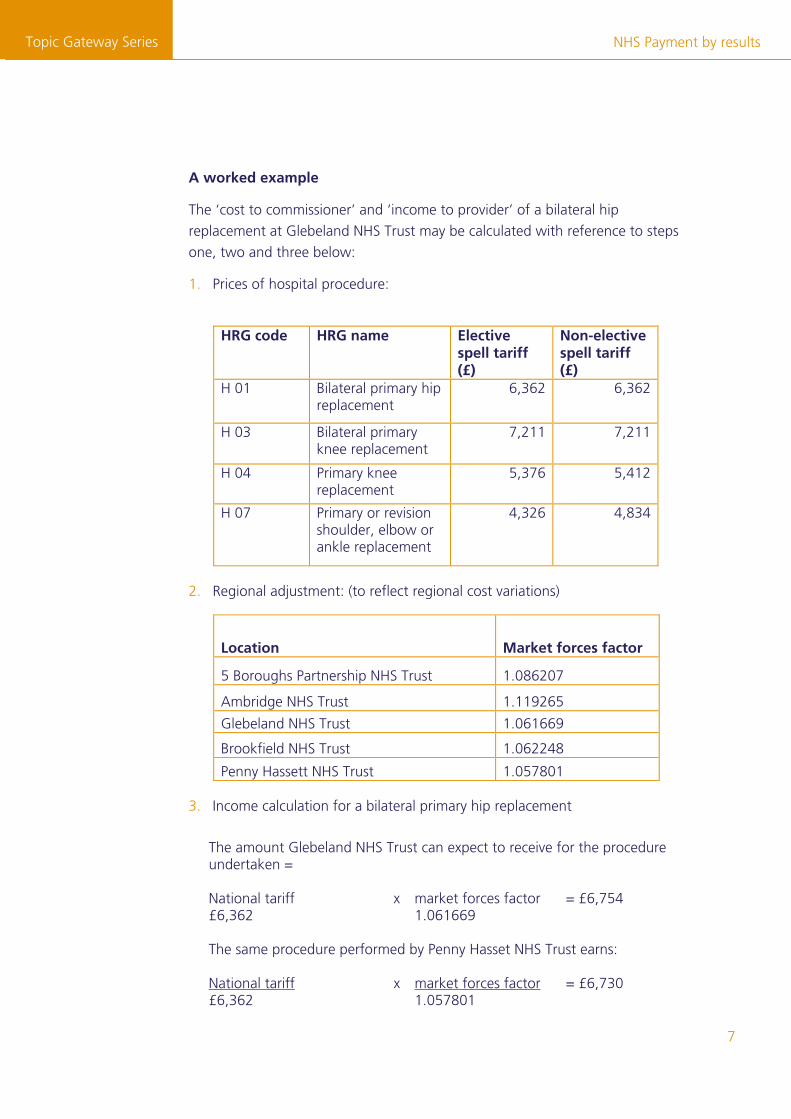
A worked example
The ‘cost to commissioner’ and ‘income to provider’ of a bilateral hip
replacement at Glebeland NHS Trust may be calculated with reference to steps
one, two and three below:
1. Prices of hospital procedure:
HRG code HRG name Elective
spell tariff (£)
Non-elective spell tariff (£)
H 01 Bilateral primary hip replacement
6,362 6,362
H 03 Bilateral primary knee replacement
7,211 7,211
H 04 Primary knee replacement
5,376 5,412
H 07 Primary or revision shoulder, elbow or ankle replacement
4,326 4,834
2. Regional adjustment: (to reflect regional cost variations)
Location Market forces factor
5 Boroughs Partnership NHS Trust 1.086207
Ambridge NHS Trust 1.119265
Glebeland NHS Trust 1.061669
Brookfield NHS Trust 1.062248
Penny Hassett NHS Trust 1.057801
3. Income calculation for a bilateral primary hip replacement
The amount Glebeland NHS Trust can expect to receive for the procedure undertaken = National tariff x market forces factor = £6,754 £6,362 1.061669 The same procedure performed by Penny Hasset NHS Trust earns: National tariff x market forces factor = £6,730 £6,362 1.057801

NHS Payment by results Topic Gateway Series
8
Under PbR, a basic premise is the application of the national tariff and therefore
the ‘cost to commissioner’ is the same regardless of the provider used. The actual
income received by the provider may be different due to the top-up provided in
the form of the MFF, which is paid to providers by the Department of Health.
Related tools and techniques The primary objective of PbR is the delivery of optimal efficiency in health service
provision by NHS organisations.
A range of topic gateways providing guidance and information relevant to
management accounting is available to CIMA members. Those topic gateways,
which may be of particular interest and value for those operating under a PbR
regime, include:
• activity based costing and management (ABC/ABM)
• planning and forecasting.
Other helpful tools and approaches include:
• target costing
• value analysis
• value engineering
• just-in-time (JIT)
• total quality management (TQM)
• materials requirements planning (MRP)
• kaizen
• lean manufacturing
• cause-effect analysis (‘fishbone’ diagrams).
The topic gateways are available from www.cimaglobal.com/mycima [Accessed 12 March 2008]

NHS Payment by results Topic Gateway Series
9
Further information
Articles
Banham, R. Off target? CFO Magazine, May 2000, Volume 16, Issue 6,
pp 127-130
Bayou, M. and Reinstein, A. Three routes for target costing. Managerial Finance,
1998, Volume 24, Number 1, pp 28-45
Chen, R.C. and Chung, C.H. Cause-effect analysis for target costing. Accounting
Quarterly, Winter 2002, Volume 3, Issue 2, pp 1-9
Cooper, R. and Chew, W. B. Control tomorrow’s costs through today’s designs. Harvard Business Review, January-February 1996, Volume 74, Issue 1, pp 88-97
Davila, A. and Wouters, M. Designing cost-competitive technology products
through cost management. Accounting Horizons, 2004, Volume 18, Issue 1, pp
13-26
Ellwood, S. The NHS financial manager in 2010. Public Money and Management,
January-March 2000, Volume 20, Issue 1, pp 23-30
Ellwood, S. Full-cost pricing rules within the National Health Service internal
market: accounting choices and the achievement of productive efficiency.
Management Accounting Research, 1996, Volume 7, pp 25-51
Gagne, M. L. and Discenza, R. Target costing. Journal of Business and Industrial
Marketing, 1995, Volume 10, Issue 1, pp 16-22
Jackson, A. and Lapsley, I. The diffusion of accounting practices in the new
‘managerial’ public sector. International Journal of Public Sector Management,
2003, Volume 16, Number 5, pp 359-372
Lockamy, A. and Smith, W. Target costing for supply chain management: criteria
and selection. Industrial Management and Data Systems, 2000, Volume 100,
Numbers 5-6, pp 210-218
Sakurai, M. Target costing and how to use it. Journal of Cost Management for
the Manufacturing Industry, Summer 1989, Volume 3, Number 2, pp 39-50
Spear, S. Fixing healthcare from the inside, today. Harvard Business Review,
September 2005, Volume 83, Issue 11, p. 162

NHS Payment by results Topic Gateway Series
10
Swenson, D. et al. Best practices in target costing. Management Accounting
Quarterly, Winter 2003, Volume 4, Issue 2, pp 12-17
Tinkler, M. and Dubé, D. Strength in numbers. CMA Management, September
2002, Volume 76, Issue 6, pp 14-17
Books (2005). CIMA Official Terminology. Oxford: CIMA Publishing
CIMA research Bourn and Sutcliffe. (eds). (1996). Management accounting in healthcare. London: CIMA
Ellwood, S. (1996). Cost-based pricing in the NHS internal market. CIMA
Research Studies. London: CIMA
Northcott, D. and Llewellyn, S. (2004). Decision making in health care: exploring
cost variability. CIMA Research Executive Summary. Available from:
www.cimaglobal.com/researchexecsummaries [Accessed 12 March 2008]
Other research (2005). NHS Costing Manual. Department of Health http://digbig.com/4wxrc
[Accessed 19 May 2008]
(2005). Financial management in the NHS: NHS (England) summarised accounts
2003-04. National Audit Office and Audit Commission
(2004). Achieving first-class financial management in the NHS: a sound basis for
better healthcare. Audit Commission. www.audit-commission.gov.uk
[Accessed 12 March 2008]
(1999). Target costing for effective cost management: product cost planning at
Toyota Australia. IFAC Financial and Management Accounting Committee
Websites The Audit Commission www.audit-commission.gov.uk
[Accessed 12 March 2008]
Specific pages of interest include Payment by Results.

NHS Payment by results Topic Gateway Series
11
Chartered Institute of Management Accountants (CIMA)
www.cimaglobal.com [Accessed 12 March 2008]
Connecting for Health Supports the NHS to deliver better, safer care to patients, via new computer
systems and services, that link GPs and community services to hospitals.
http://digbig.com/4wxrd
[Accessed 19 May 2008]
UK Department of Health www.dh.gov.uk/en/index.htm [Accessed 12 March 2008]
Specific pages of interest are:
Payment by Results http://digbig.com/4wxre [Accessed 19 May 2008]
BMA - Caring for the NHS http://digbig.com/4wxrf [Accessed 19 May 2008]
Health Matters Health Matters is an independent non-profit UK magazine covering the NHS,
public health and health politics. www.healthmatters.org.uk
[Accessed 12 March 2008]
Healthcare Resource Groups: Casemix
The Casemix Service develops clinical grouping methodologies and software
products that enable the NHS to record clinical activity.
http://digbig.com/4wxrh
[Accessed 19 May 2008]
Healthcareworkforce.nhs.uk
Provides one stop access to NHS healthcare workforce planning information,
knowledge, intelligence and practical tools.
www.healthcareworkforce.nhs.uk
[Accessed 12 March 2008]
The King’s Fund
The King's Fund is an independent charitable foundation working for better
health, especially in London. www.kingsfund.org.uk/index.html [Accessed 12 March 2008]

NHS Payment by results Topic Gateway Series
[Accessed 12 March 2008]
NHS Costing Manual
Sets out the principles and practice of costing to be applied in the NHS.
http://digbig.com/4wxrj [Accessed 19 May 2008]
NHS Networks
Promotes and connects the many networks which exist throughout the
NHS, and encourages the formation of new ones.
www.networks.nhs.uk/1.php
[Accessed 12 March 2008]
Office of Health Economics
Provides independent research, advisory and consultancy services on
policy implications and economic issues within the pharmaceutical,
health care and biotechnology sectors.
www.ohe.org/page/index.cfm
[Accessed 12 March 2008]
12
No responsibility for loss occasioned to any person acting or refraining from action as a result of any material in this publication can be accepted by the authors or the publishers.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means method or device, electronic (whether now or hereafter known or developed), mechanical, photocopying, recorded or otherwise, without the prior permission of the publishers.
Permission requests should be submitted to CIMA at [email protected]
Copyright ©CIMA 2006
First published in 2006 by:
The Chartered Institute of Management Accountants 26 Chapter Street London SW1P 4NP United Kingdom
Printed in Great Britain