new trends in gastric polyps: evolving classification …
TRANSCRIPT

"NEW TRENDS IN GASTRIC POLYPS: EVOLVING CLASSIFICATION AND
PATHOGENESIS"
Gregory Y. Lauwers, MD Senior Member
H. Lee Moffitt Cancer Center & Research Institute Tampa, FL
• Heterotopia or Hamartomatous• Regenerative or Inflammatory• Neoplastic (Adenoma/papilloma/papillary adenoma)• Cystic Polyps• Miscellaneous (Cronkhite-Canada) / Fundic Glandular cysts)
– Hererotopic pancreas– Cystic Inflammatory Fibroid Polyp– Xanthelasma– Others
19721979
1990
2003
1990

2013 - MORSON & DAWSON’S 5TH EDITION
FGP: 77%Hyperplastic:14.4%
2% 0.7%
Carmack SW. Am J Gastroenterol 2009;104:1524

FGP: Fundic Gland Polyp; GHP:Gastric Hyperplastic Polyp
Prevalence of gastric polyp / age
Sonnenberg A., Digestive and Liver Disease 47 (2015)
Prevalence of gastric polyps:3.75%

Sonnenberg A., Digestive and Liver Disease 47 (2015)

OUTLINE• Fundic Gland Polyps
– Familial Adenomatous Polyposis– Gastric Adenocarcinoma & Proximal Polyposis [GAPPS]
• Hyperplastic Polyps– Prolapse and Inverted Variant– ‘Syndromic’ Differential Diagnosis On Pinch Biopsies
• Pyloric Adenoma• Gastric Adenocarcinoma Fundic Gland Type/ Oxyntic
Adenoma
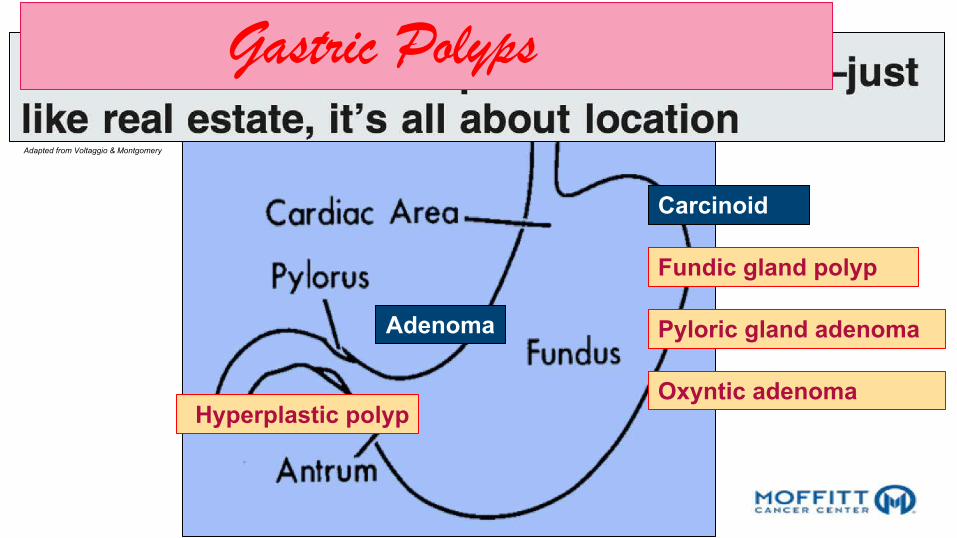
Carcinoid
Pyloric gland adenoma
Hyperplastic polyp
Fundic gland polyp
Adenoma
Oxyntic adenoma
Gastric PolypsAdapted from Voltaggio & Montgomery

BODY/FUNDUS
MUC5AC
MUC5-AC
MUC6MUC6
H+/K+ ATP ase
Pepsinogen I
MUC5AC /MUC6 Secretory Stomach / Intestine 11p15.5
OXYNTIC MUCOSA ANTRAL MUCOSA

OUTLINE• Fundic Gland Polyps
– Familial Adenomatous Polyposis– Gastric Adenocarcinoma & Proximal Polyposis [GAPPS]
• Hyperplastic Polyps– Prolapse and Inverted Variant– ‘Syndromic’ Differential Diagnosis On Pinch Biopsies
• Pyloric Adenoma• Gastric Adenocarcinoma Fundic Gland Type/ Oxyntic
Adenoma
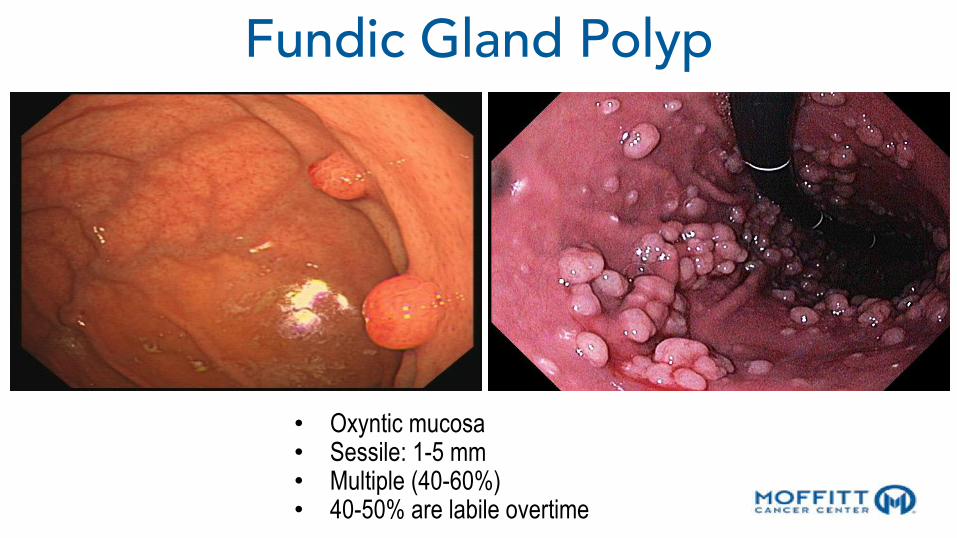
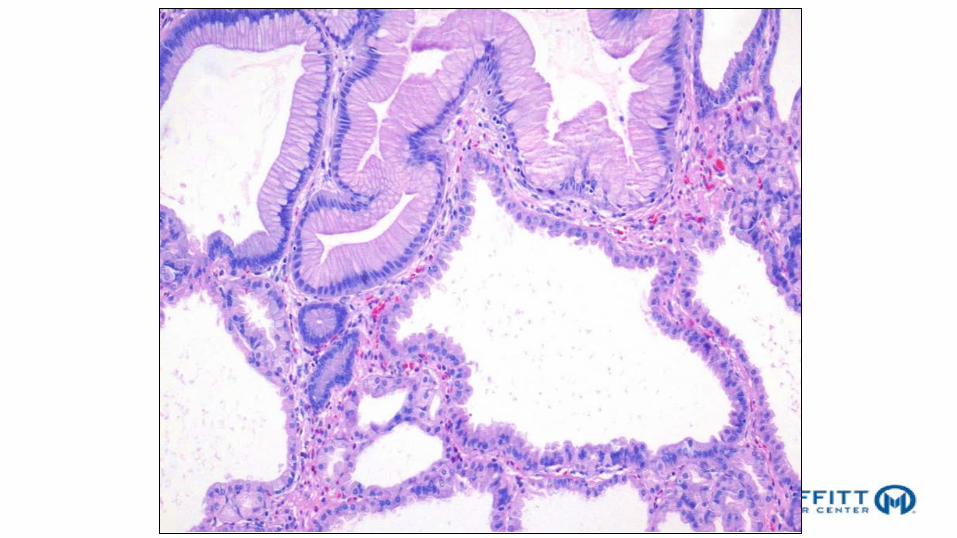
• Oxyntic mucosa• Sessile: 1-5 mm• Multiple (40-60%)• 40-50% are labile overtime
Fundic Gland Polyp
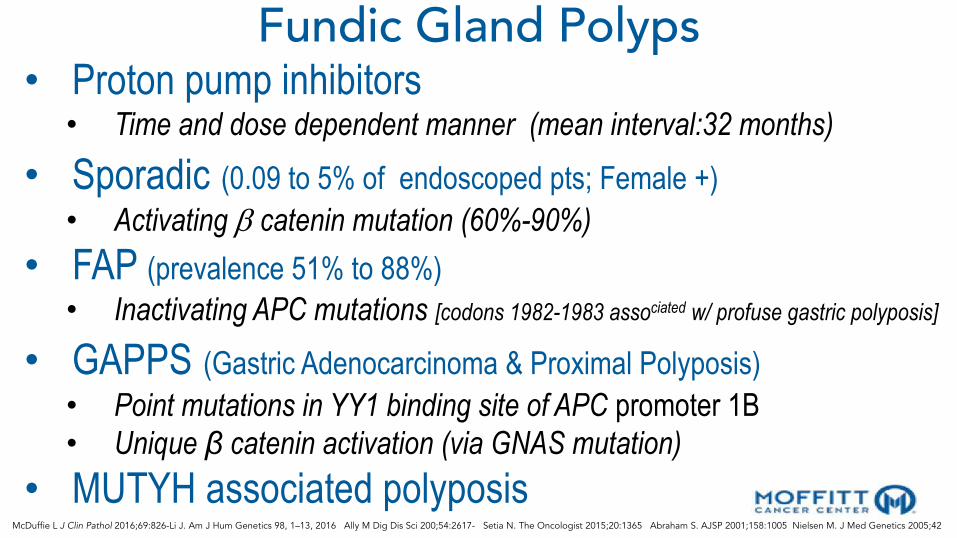
Fundic Gland Polyps• Proton pump inhibitors• Time and dose dependent manner (mean interval:32 months)
• Sporadic (0.09 to 5% of endoscoped pts; Female +)• Activating b catenin mutation (60%-90%)
• FAP (prevalence 51% to 88%)• Inactivating APC mutations [codons 1982-1983 associated w/ profuse gastric polyposis]
• GAPPS (Gastric Adenocarcinoma & Proximal Polyposis)• Point mutations in YY1 binding site of APC promoter 1B• Unique β catenin activation (via GNAS mutation)
• MUTYH associated polyposisMcDuffie L J Clin Pathol 2016;69:826-Li J. Am J Hum Genetics 98, 1–13, 2016 Ally M Dig Dis Sci 200;54:2617- Setia N. The Oncologist 2015;20:1365 Abraham S. AJSP 2001;158:1005 Nielsen M. J Med Genetics 2005;42

Sporadic FGP: Dysplasia is rare (1%)FAP patients: 25-48% (LGD>HGD [0-12%])
Risk increase w/ the size of polyps and severity of duodenal polyposisRare cases of ACA
Series of 24 FAP pts [follow-up of 6 yrs] 87% persisted (54%) or regressed (33%)13% progressed to HGD/IMC
(sporadic LGD progression rate: 5-14%)
• Recommendations:– Sporadic: no follow-up– FAP: Follow q. 2/3 years (suggested):
• Look for large polyps (>1cm)• Sample extensively
Goddard AF. Gut 2010;59:1270-1276 Arnason T. Histopathology 2014;65:353

Gastric adenocarcinoma and proximal polyposisof the stomach (GAPPS): a new autosomaldominant syndromeD L Worthley,1 K D Phillips,2 N Wayte,3 K A Schrader,4 S Healey,5 P Kaurah,4
A Shulkes,6 F Grimpen,7 A Clouston,7 D Moore,8 D Cullen,9 D Ormonde,9
D Mounkley,10 X Wen,11 N Lindor,11 F Carneiro,11 D G Huntsman,4
G Chenevix-Trench,5 G K Suthers2,12
ABSTRACTObjective The purpose of this study was the clinical andpathological characterisation of a new autosomaldominant gastric polyposis syndrome, gastricadenocarcinoma and proximal polyposis of the stomach(GAPPS).Methods Case series were examined, documentingGAPPS in three families from Australia, the USA andCanada. The affected families were identified throughreferral to centralised clinical genetics centres.Results The report identifies the clinical and pathologicalfeatures of this syndrome, including the predominantdysplastic fundic gland polyp histology, the exclusiveinvolvement of the gastric body and fundus, the apparentinverse association with current Helicobacter pyloriinfection and the autosomal dominant mode ofinheritance.Conclusions GAPPS is a unique gastric polyposissyndrome with a significant risk of gastricadenocarcinoma. It is characterised by the autosomaldominant transmission of fundic gland polyposis,including areas of dysplasia or intestinal-type gastricadenocarcinoma, restricted to the proximal stomach, andwith no evidence of colorectal or duodenal polyposis orother heritable gastrointestinal cancer syndromes.
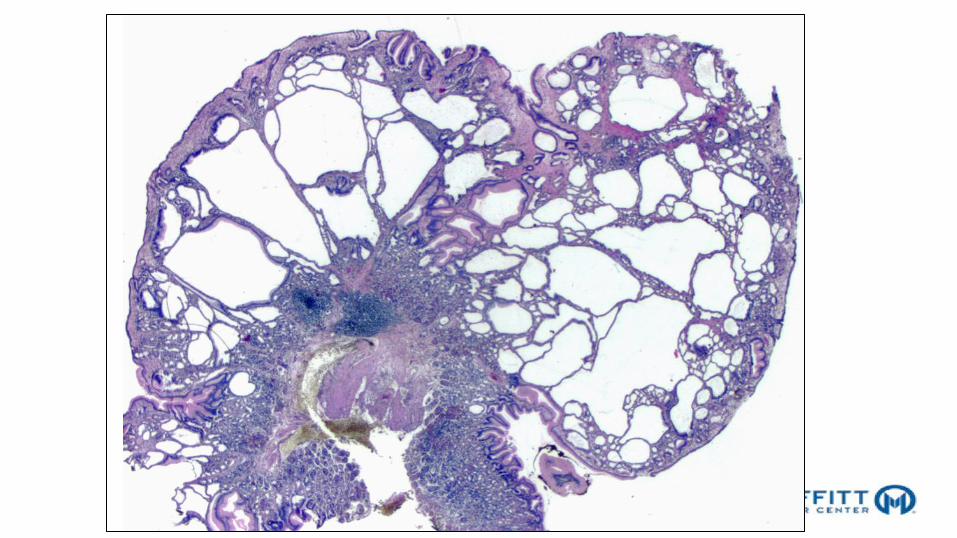
INTRODUCTIONFundic gland polyps (FGPs) are the most commongastric polyps. They are diagnosed in w5% ofgastroscopies and account for up to 70% of allsampled gastric polyps.1 2 Sporadic FGPs are usuallysmall (<5 mm), few in number (usually <10) andare restricted to the gastric body and fundus.3 FGPsare histologically characterised by prominent cysticspaces lined by flattened parietal, chief and mucousneck cells.3
FGPs are directly associated with chronic protonpump inhibitor (PPI) therapy and inversely associ-ated with Helicobacter pylori infection, suggestinga possible connection between FGPs and perturbedgastric acid homeostasis.4 Fundic gland polyposismay also be a manifestation of inherited gastroin-testinal polyposis syndromes, particularly familialadenomatous polyposis (FAP) which is charac-terised by hundreds to thousands of adenomatouspolyps in the colorectum and, without colectomy,the almost inevitable development of colorectalcancer. Other inherited gastric polyp syndromes
include MUTYH-associated polyposis (MAP),generalised juvenile polyposis syndrome (GJPS),PeutzeJeghers syndrome (PJS) and Cowdensyndrome.5 6 However, FGPs are relatively rare inMAP, an autosomal recessive disorder, and GJPS andPJS are often characterised by the presence ofspecific hamartomatous (rather than purelydysplastic fundic gland) polyps.5 6
Sporadic FGPs are usually innocuous, butsyndromic FGPs can progress to dysplasia andgastric adenocarcinoma.7e9 Therefore, cliniciansmust distinguish patients with sporadic versussyndromic fundic gland polyposis so that additionalscrutiny is provided for the latter withoutsubjecting the majority of patients to needlessinvestigation.Here we describe a new autosomal dominant
syndrome characterised by fundic gland polyposisand gastric cancer. We refer to the syndrome asgastric adenocarcinoma and proximal polyposis ofthe stomach (GAPPS). This report documents thedetailed clinical and pathological features of GAPPSin a large Australian family and in two smallerNorth American families. We propose diagnosticcriteria and management strategies for GAPPS andexamine potential factors that may contribute tothe pathogenesis.
METHODSDNA and pathology samples were collectedfollowing informed written consent and approvalby the local institutional review board. In lieu ofBMJ Publishing Group consent forms beingprovided, all individual sex-specific information wasremoved from this description to reduce the prob-ability of an individual being identified. Histopa-thology, where available, was reviewed andreported by a gastrointestinal pathologist (FC).Mutations in APC, MUTYH, CDH1, SMAD4,BMPR1A, STK11 and PTEN were excluded in allfamilies by sequence analysis of exons and flankingregions as well as by assays for deletion or dupli-cation of exons. Immunohistochemistry, micro-satellite testing, gastrin amide and progastrin assayswere performed using published methods.10 11
H pylori status was determined primarily by histo-pathology, although serology, rapid urease test ongastric biopsies and the urea breath test wereperformed in some patients. H pylori infection wasconsidered to be present if detected on any test, and
1Division of Digestive and LiverDiseases, Columbia University,New York, New York, USA2SA Clinical Genetics Service,SA Pathology, South Australia,Australia3School of Medicine, Universityof Queensland, Queensland,Australia4Hereditary Cancer Program, BCCancer Agency, BritishColumbia, Canada5Queensland Institute ofMedical Research, Queensland,Australia6Department of Surgery,University of Melbourne,Victoria, Australia7Royal Brisbane and Women’sHospital, Queensland, Australia8Women’s and Children’sHospital, South Australia,Australia9St John of God Hospital,Western Australia, Australia10Flinders Medical Centre,South Australia, Australia11Institute of MolecularPathology and Immunology ofthe University of Porto(IPATIMUP) and MedicalFaculty/Hospital S. Joao, Porto,Portugal12Department of Paediatrics,School of Paediatrics &Reproductive Health, Faculty ofHealth Sciences, University ofAdelaide, SA, Australia
Correspondence toDr Graeme Suthers, SA ClinicalGenetics Service SA PathologyWomen’s & Children’s Hospital,North Adelaide, SA 5006,Australia;[email protected]
Revised 7 June 2011Accepted 24 June 2011Published Online First3 August 2011
774 Gut 2012;61:774e779. doi:10.1136/gutjnl-2011-300348
Case report
group.bmj.com on May 1, 2012 - Published by gut.bmj.comDownloaded from
² Key features: • FG polyposis w/occasional
hyperplastic* & adenomatous polyps [*hyperproliferative aberrant pits & flat dysplasia in 100% of cases]– sparing the antrum– intestinal type gastric cancer
• Autosomal dominant inheritance (Incomplete penetrance)
• No (rare ?) colonic adenomas
Worthley DL Gut 2012, 61:774-779 ; *De Boer B. Am J Surg Pathol 2018;42:1-8; McDuffie LA J Clin Pathol 2016;69:826-833

Courtesy of P. Kumarasinghe
Hyperproliferative aberrant pit w/ inverted foveolarhyperplasia (+/- FGP)

De Boer B. Am J Surg Pathol 2018;42:1-8
Hyperproliferative Aberrant Pits
Ki-67 MUC5AC

De Boer B. Am J Surg Pathol 2018;42:1-8
Flat LGD in the setting of hyperproliferative aberrant pit
Flat HGD in the setting of hyperproliferative aberrant pit
Ki-67
Ki-67

OUTLINE• Fundic Gland Polyps
– Familial Adenomatous Polyposis– Gastric Adenocarcinoma & Proximal Polyposis [GAPPS]
• Hyperplastic Polyps– Prolapse and Inverted Variant– ‘Syndromic’ Differential Diagnosis On Pinch Biopsies
• Pyloric Adenoma• Gastric Adenocarcinoma Fundic Gland Type/ Oxyntic
Adenoma

Mean age: 65yrs - Antrum:60%.Sessile/pedunculated - Multiplicity: 20%.
Hyperplastic Polyp

25%
12%
21%
27%
15%HP gastritisAuto Im. GastritisReact. Gastro.OthersNormal
Mucosal background of Hyperplastic Polyps

MUC5 MUC6MUC5-AC MUC6
Hyperplastic Polyp

Dysplasia:1.8-16.4%; Carcinoma:0.3-7.1% (avg 2.1%) (> 2.0 cm)
Carmack SW. Nat Rev; Gastroenterol hepatol 2009;6:331-341 Goddard AF. Gut 2010;59:1270-1276

208 polypoid lesions reported as hyperplastic polyps
Polypoid fov. hyperplasia:49%
Hyperplastic polyp:31%
Prolapse polyp:20%Gonzalez-Obeso E. Am J Surg Pathol 2011;35;670-677
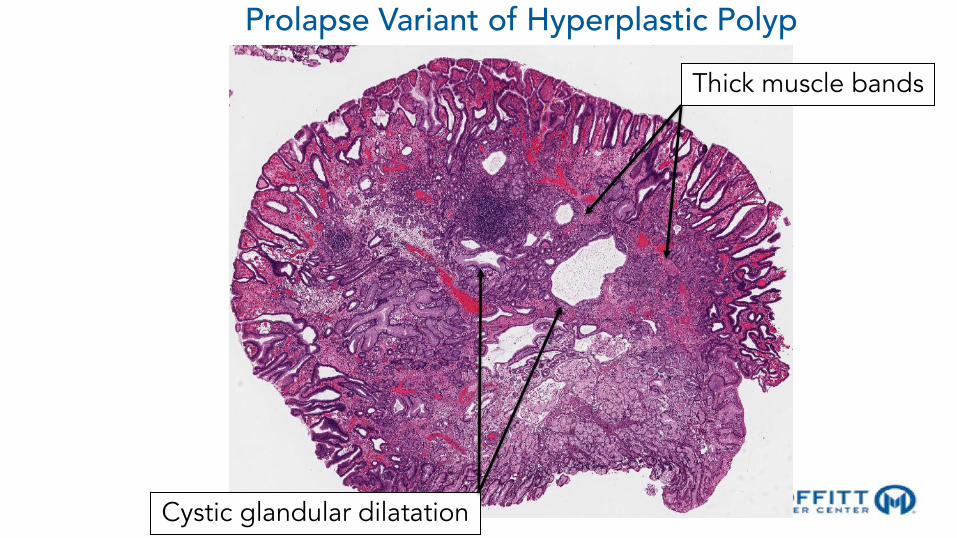
Cystic glandular dilatation
Prolapse Variant of Hyperplastic Polyp
Thick muscle bands
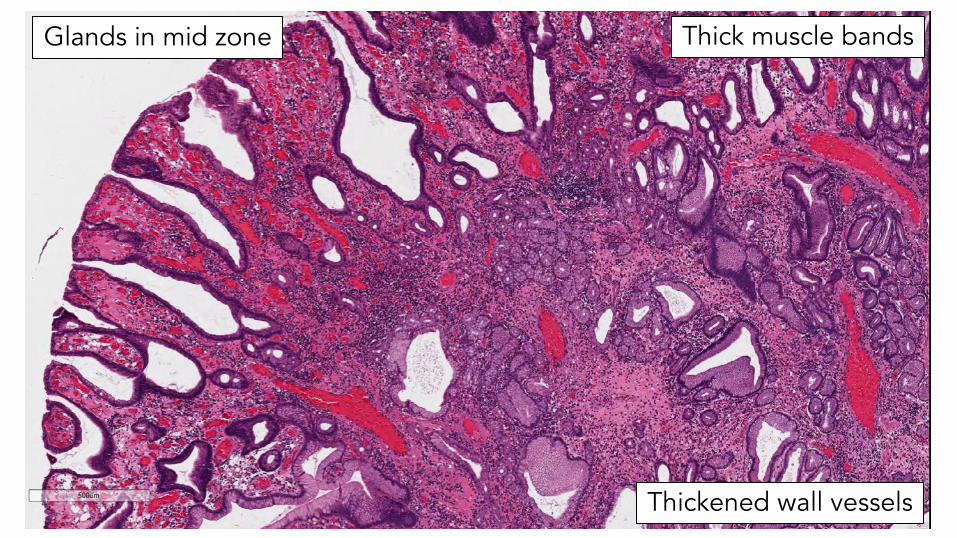
Thick muscle bands
Thickened wall vessels
Glands in mid zone
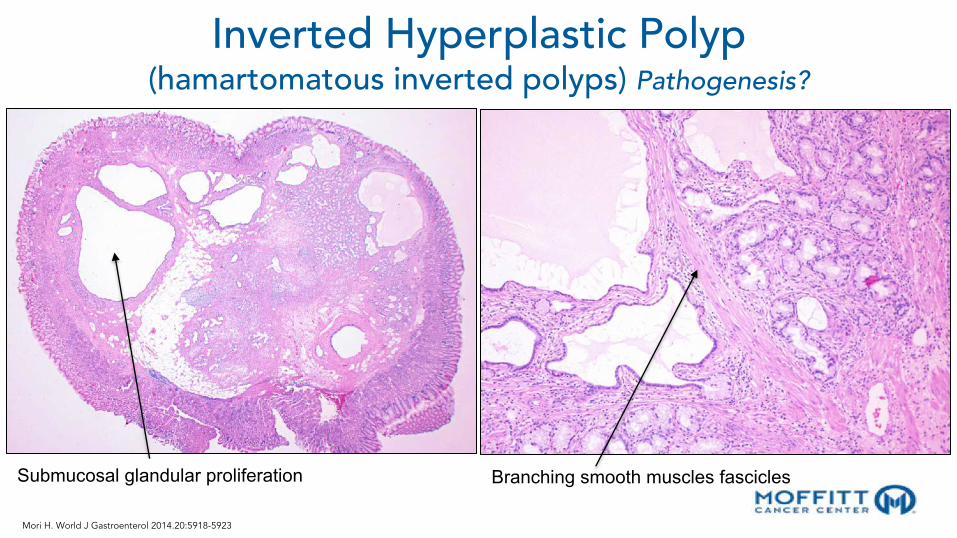
Inverted Hyperplastic Polyp(hamartomatous inverted polyps) Pathogenesis?
Submucosal glandular proliferation Branching smooth muscles fascicles
Mori H. World J Gastroenterol 2014.20:5918-5923

Differential diagnosis of hyperplastic polyps is challenging on superficial pinch biopsies
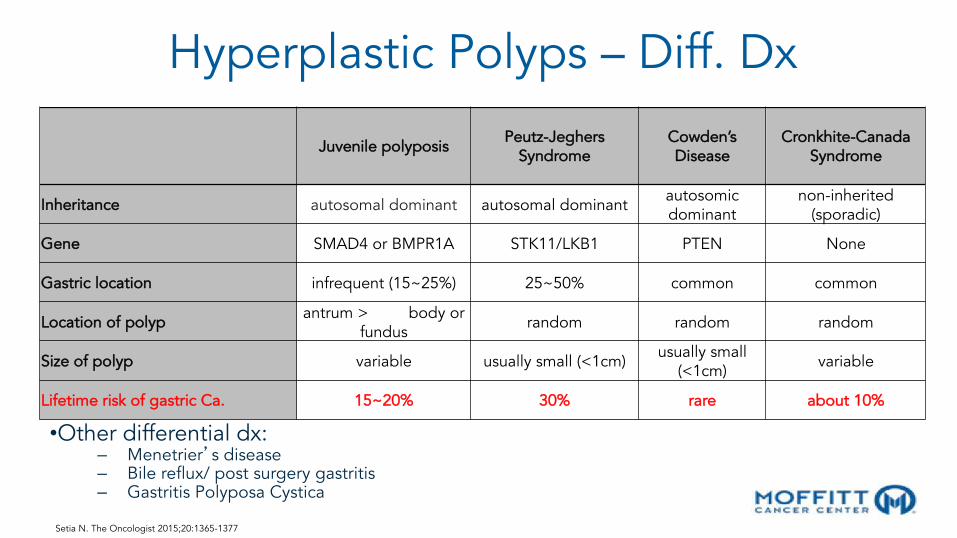
Hyperplastic Polyps – Diff. Dx
•Other differential dx:– Menetrier�s disease– Bile reflux/ post surgery gastritis– Gastritis Polyposa Cystica
Juvenile polyposis Peutz-Jeghers Syndrome
Cowden’s Disease
Cronkhite-Canada Syndrome
Inheritance autosomal dominant autosomal dominant autosomic dominant
non-inherited (sporadic)
Gene SMAD4 or BMPR1A STK11/LKB1 PTEN None
Gastric location infrequent (15~25%) 25~50% common common
Location of polyp antrum > body or fundus random random random
Size of polyp variable usually small (<1cm) usually small (<1cm) variable
Lifetime risk of gastric Ca. 15~20% 30% rare about 10%
Setia N. The Oncologist 2015;20:1365-1377

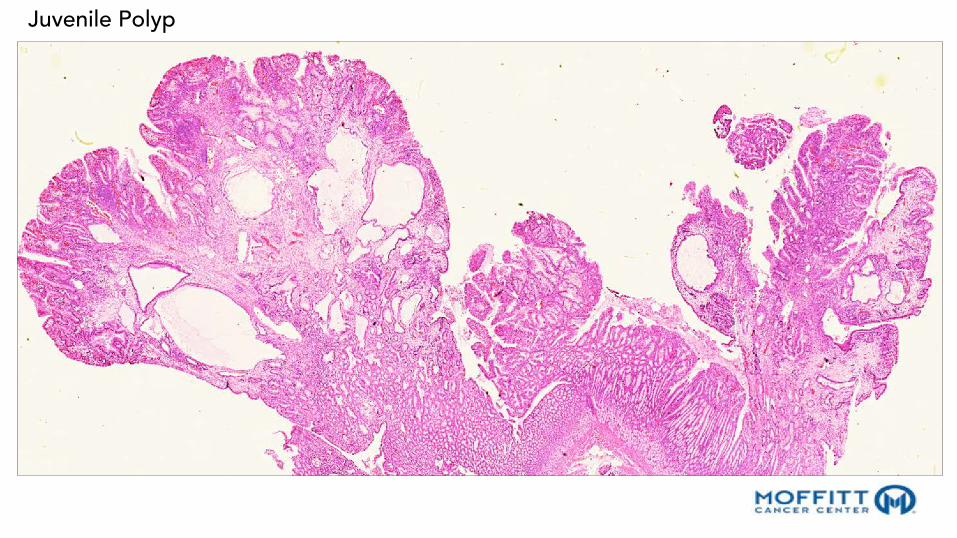
• Median age of pts presenting w/ gastric polyps ~40 years (identified as early as 7)• Rounded & sessile when small. Pedunculated w/lobular appearance as they enlarge• 59% >1 gastric JPs polyp & can develop massive gastric polyposis without lower GIT
involvement• Dysplasia can de detected in up to 14% of polyps
Juvenile Polyps [Polyposis]
Setia N. The Oncologist 2015;20:1365-1377 Gonzalez RS. Histopathology 2017;70:918-928 Ma C. Am J Surg Pathol 2014;38:1618-1626
Juvenile Polyp

No smooth muscle fibers
Disorganized pits / glands of varying sizes & shapes
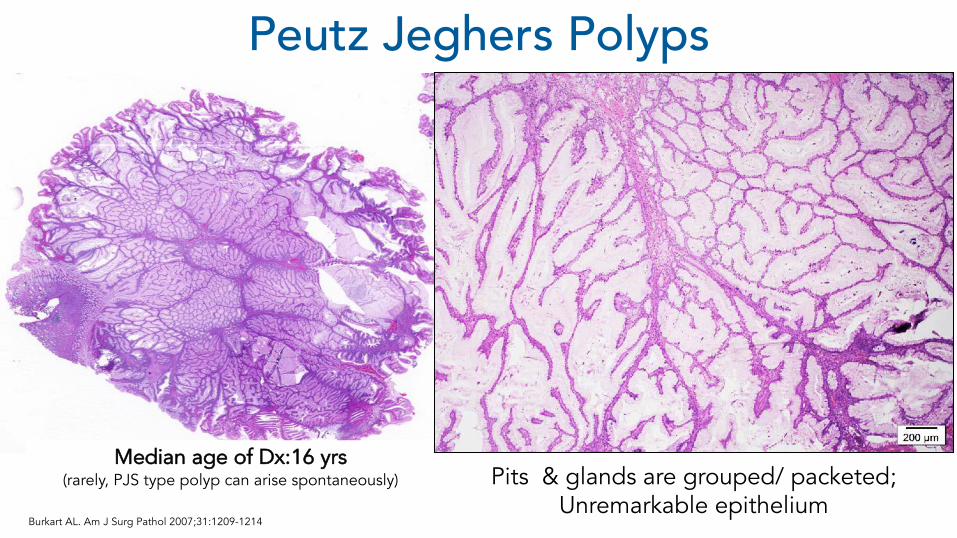
Pits & glands are grouped/ packeted; Unremarkable epithelium
Median age of Dx:16 yrs(rarely, PJS type polyp can arise spontaneously)
Peutz Jeghers Polyps
Burkart AL. Am J Surg Pathol 2007;31:1209-1214

• Dysplasia is noted in 2-3% of PJ polyps.• Increased risk of GI cancer through the hamartoma-adenoma-
carcinoma sequence and de novo malignant change.• Lifetime risk of gastric cancer estimated at 29% Syngal S. Am J Gastroenterol 2015;110:223-262 Setia N. The Oncologist 2015;20:1365-1377
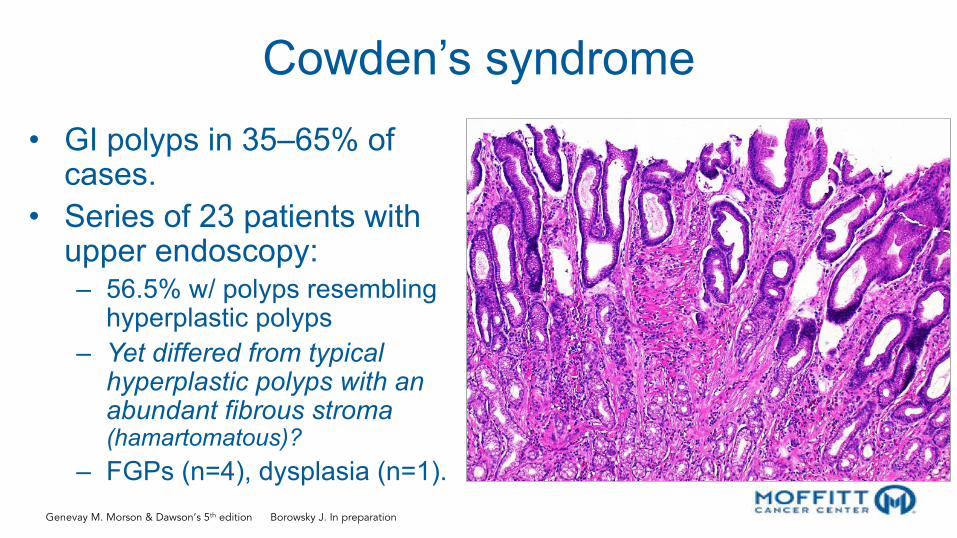
Cowden’s syndrome
• GI polyps in 35–65% of cases.
• Series of 23 patients with upper endoscopy:– 56.5% w/ polyps resembling
hyperplastic polyps– Yet differed from typical
hyperplastic polyps with an abundant fibrous stroma (hamartomatous)?
– FGPs (n=4), dysplasia (n=1).
Genevay M. Morson & Dawson’s 5th edition Borowsky J. In preparation

Cronkhite Canada Syndrome
Frequently delayed diagnosis / ectodermal frequently follow GIT by weeks to months
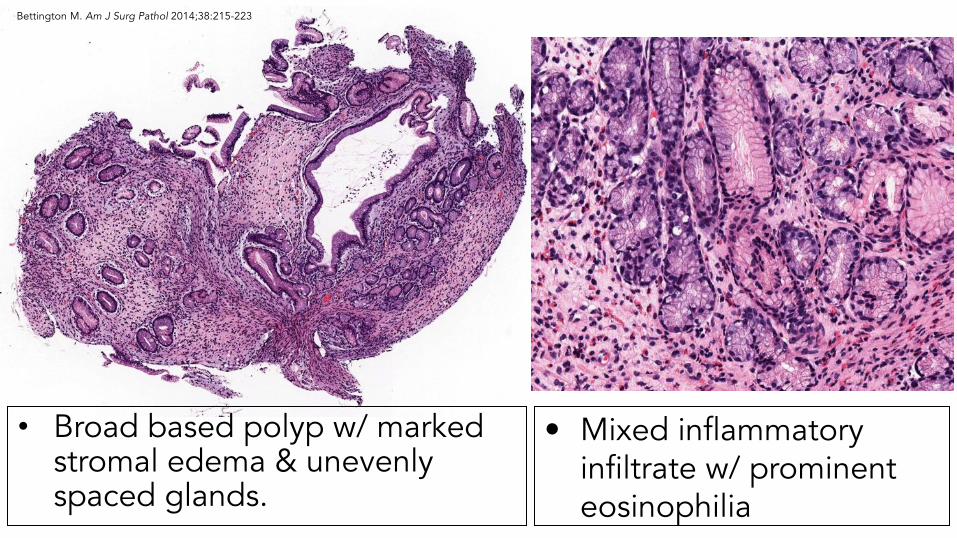
• Broad based polyp w/ marked stromal edema & unevenly spaced glands.
• Mixed inflammatory infiltrate w/ prominent eosinophilia
Bettington M. Am J Surg Pathol 2014;38:215-223
OUTLINE• Fundic Gland Polyps
– Familial Adenomatous Polyposis– Gastric Adenocarcinoma & Proximal Polyposis [GAPPS]
• Hyperplastic Polyps– Prolapse and Inverted Variant– ‘Syndromic’ Differential Diagnosis On Pinch Biopsies
• Pyloric Adenoma• Gastric Adenocarcinoma Fundic Gland Type/ Oxyntic
Adenoma

Tubular Pyloric gland adenomaTubulo-villous Pyloric gland adenoma
Pyloric Gland Adenoma (<3% of all polyps)Oberhuber G. Virchows Archiv; 2000; 437:581-90

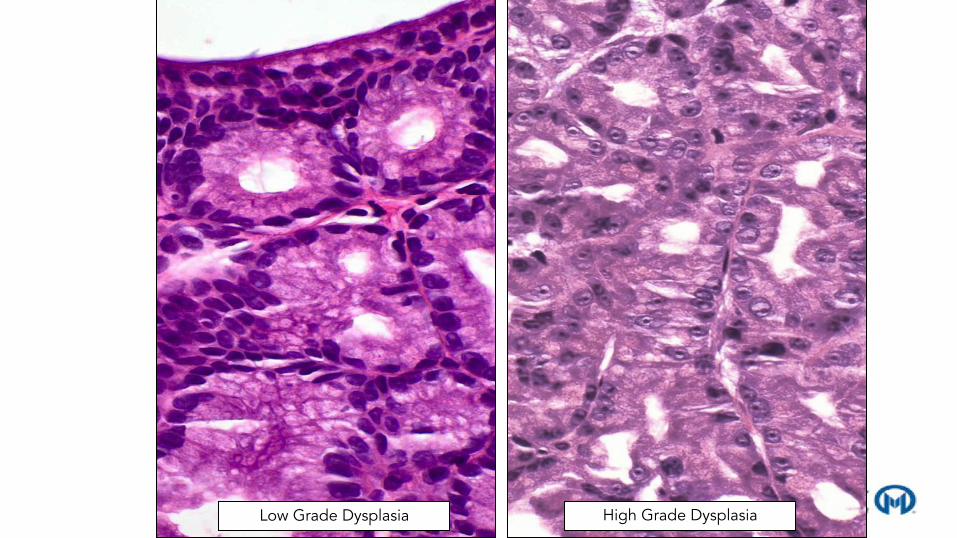
High Grade DysplasiaLow Grade Dysplasia
Choi WT. Histopathology 2018; In press
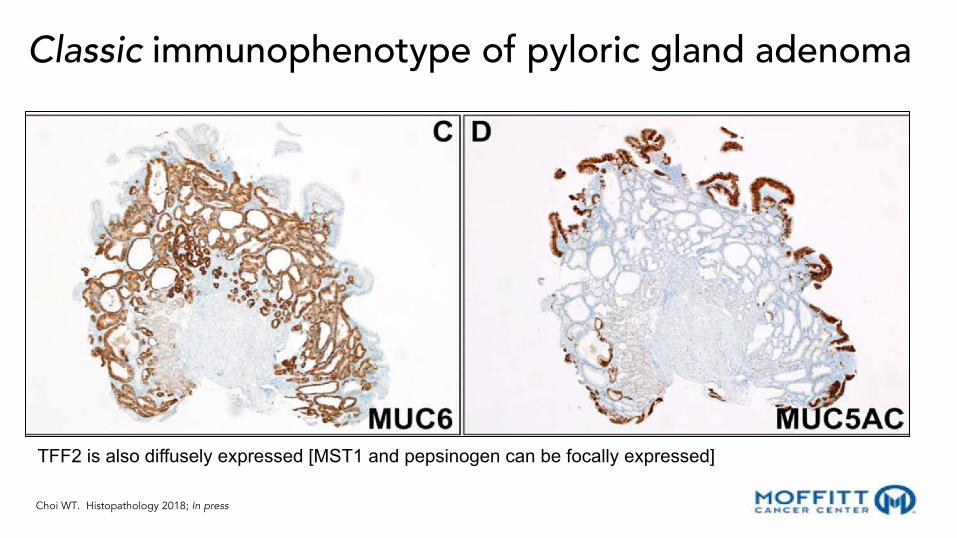
TFF2 is also diffusely expressed [MST1 and pepsinogen can be focally expressed]
Classic immunophenotype of pyloric gland adenoma

Choi WT. Histopathology 2018; In press
Pyloric gland adenomas w/ aberrant phenotype
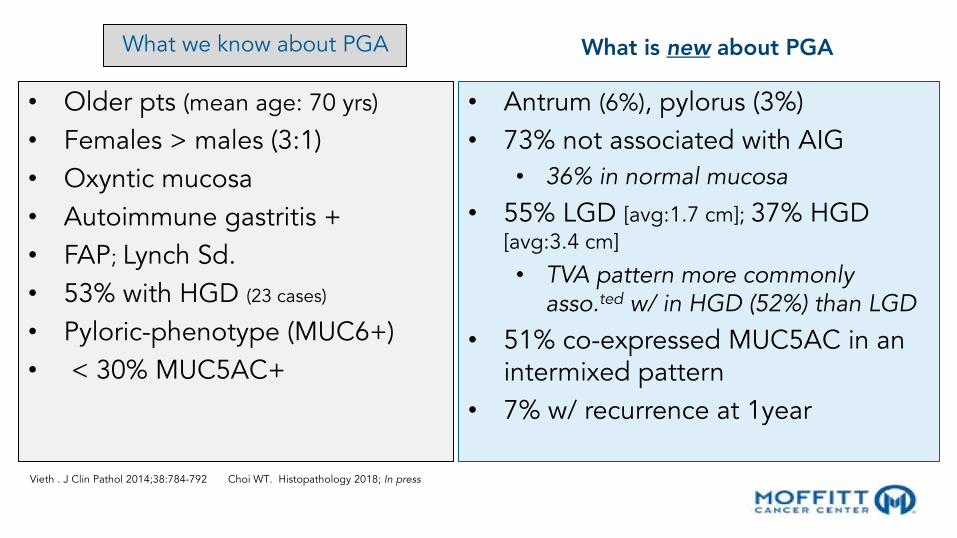
What we know about PGA
• Older pts (mean age: 70 yrs)
• Females > males (3:1)• Oxyntic mucosa• Autoimmune gastritis +• FAP; Lynch Sd.• 53% with HGD (23 cases)
• Pyloric-phenotype (MUC6+)• < 30% MUC5AC+
What is new about PGA
• Antrum (6%), pylorus (3%)• 73% not associated with AIG
• 36% in normal mucosa
• 55% LGD [avg:1.7 cm]; 37% HGD [avg:3.4 cm]
• TVA pattern more commonly asso.ted w/ in HGD (52%) than LGD
• 51% co-expressed MUC5AC in an intermixed pattern
• 7% w/ recurrence at 1year
Vieth . J Clin Pathol 2014;38:784-792 Choi WT. Histopathology 2018; In press

Journal of PathologyJ Pathol 2013; 229: 579–587Published online 4 February 2013 in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/path.4153
ORIGINAL PAPER
Frequent GNAS and KRAS mutations in pyloric gland adenomaof the stomach and duodenumAkiko Matsubara,1 Shigeki Sekine,2* Ryoji Kushima,1 Reiko Ogawa,2 Hirokazu Taniguchi,1 Hitoshi Tsuda1 andYae Kanai2
1 Pathology and Clinical Laboratories, National Cancer Centre Hospital, Tokyo, Japan2 Molecular Pathology Division, National Cancer Centre Research Institute, Tokyo, Japan
*Correspondence to: Shigeki Sekine, Molecular Pathology Division, National Cancer Centre Research Institute, 5-1-1 Tsukiji, Chuo-ku, Tokyo104–0045, Japan. e-mail: [email protected]
AbstractGastric and duodenal adenomas exhibit a significant morphological and phenotypical diversity and are classifiedinto intestinal-type, foveolar-type and pyloric gland adenomas. We analysed the mutations in GNAS, KRAS, BRAFand CTNNB1 and the expressions of mismatch repair (MMR) proteins in 80 gastric and 32 duodenal adenomas withhistologically distinct subtypes, as well as in 71 gastric adenocarcinomas. Activating GNAS mutations were foundin 22 of the 35 pyloric gland adenomas (PGAs; 63%) but in none of the foveolar-type or intestinal-type adenomasor the adenocarcinomas. Fourteen PGAs (41%), two foveolar-type adenomas (9%), five intestinal-type adenomas(9%) and one adenocarcinoma (1%) had KRAS mutations. BRAF mutations were absent in all the adenomas andadenocarcinomas that were examined. CTNNB1 mutations were only found in two intestinal-type adenomas (4%).Notably, 13 of the 14 KRAS-mutated gastric and duodenal PGAs had concurrent GNAS mutations. The loss of theMMR proteins, which is indicative of microsatellite instability, was observed in one PGA (3%), 12 foveolar-typeadenomas (52%), one intestinal-type adenoma (2%) and five adenocarcinomas (7%). These observations indicatethat each histological subtype of gastric and duodenal adenomas has a distinct genetic background. In particular,the present study identified the frequent presence of activating GNAS mutations, which are often associated withKRAS mutations, as a characteristic genetic feature of PGAs of the stomach and duodenum.Copyright © 2012 Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Keywords: pyloric gland adenoma; stomach, duodenum; GNAS; KRAS
Received 22 August 2012; Revised 8 November 2012; Accepted 24 November 2012
No conflicts of interest were declared.
Introduction
Gastrointestinal adenomas are benign polypoid epithe-lial neoplasms that may have some malignant poten-tial [1,2]. Gastric adenomas are known to exhibitsignificant phenotypic diversity and can be classifiedinto morphologically and immunophenotypically dis-tinct subtypes. According to the 2010 World HealthOrganization (WHO) classification, gastric adenomasare primarily classified into two categories: intestinal-type and gastric-type [3]. Gastric-type adenomas canbe further subclassified into foveolar-type and pyloricgland adenomas (PGAs) [3]. In contrast to gastricadenomas, the histological diversity of duodenal ade-nomas is less well recognized. Most duodenal adeno-mas exhibit intestinal-type differentiation [4], but somestudies have also reported the presence of PGAs inthe duodenum [5–7]. On the other hand, foveolar-typeadenomas have been rarely reported in the duodenum.
Intestinal-type adenoma is the most common ade-nomatous polyp in the upper gastrointestinal tract [8].
These adenomas exhibit the histological and immuno-histochemical features of small intestinal epitheliumand consist of intestinal-type epithelial cells, includ-ing absorptive, goblet and Paneth cells (Figure 1A, B,H) [3]. The immunohistochemical expression of intesti-nal epithelial markers, such as MUC2 and CD10, hasalso been described [3,9]. A previous study reportedan incidence of 24% for the malignant transformationof gastric intestinal-type adenomas [2].
Foveolar-type adenoma has long been recognizedas a prototype of gastric-type adenomas and is com-prised of foveolar-type epithelial cells with an apicalmucin cap (Figure 1C, D) [7]. Immunohistochemically,foveolar-type adenoma is positive for MUC5AC (amarker of gastric foveolar epithelium) and negative forMUC6 (a pyloric gland-type mucin) [7,10]. Foveolar-type adenoma usually exhibits low-grade dysplasia andis thought to be associated with a low risk of malignanttransformation [2,7].
PGA is a relatively rare type of adenoma that hasbeen increasingly recognized as a distinct variant ofgastric-type adenoma [6,7]. PGA occurs in both the
Copyright © 2012 Pathological Society of Great Britain and Ireland. J Pathol 2013; 229: 579–587Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com
GNASmutation
Original Article
Gastric adenocarcinoma of the fundic gland type sharescommon genetic and phenotypic features with pyloricgland adenoma
Ryoji Kushima,1 Shigeki Sekine,2 Akiko Matsubara,1 Hirokazu Taniguchi,1 Masahiro Ikegami3 andHitoshi Tsuda1*1Pathology and Clinical Laboratory Division, National Cancer Center Hospital, 2Department of Molecular Pathology,National Cancer Center Research Institute and 3Department of Pathology, Jikei University School of Medicine,Tokyo, Japan
Gastric adenocarcinoma of the fundic gland type (GAFG) andpyloric gland adenoma (PGA) have recently been recognizedas rare types of neoplasia. We performed comparative immu-nohistochemical and genetic analyses of 3 GAFGs and 12PGAs. All of the 3 GAFGs were diffusely positive forpepsinogen-I, MIST1 and MUC6, indicating the predomi-nantly chief cell/mucous neck cell differentiation of thesetumors. A small number of H.K-ATPase-positive parietal cellswere also scattered. PGAs invariably exhibited diffuse MUC6and TFF2 expression, consistent with the pyloric gland dif-ferentiation of these tumors. Ten of the 12 PGAs also unex-pectedly exhibited focal expression of pepsinogen-I andMIST1, suggesting that PGAs often show focal chief celldifferentiation and phenotypically resemble mucous neckcells rather than pyloric glands. The mutation analysesrevealed activating GNAS mutations, which have beenreported to be frequently detected in PGAs, in two of theGAFGs. While GAFGs and PGAs are morphologically distinctlesions, our observations showed their partially overlappingimmunohistochemical profiles and shared presence ofGNAS mutations, in addition to their common occurrence inthe fundic gland mucosa. Based on these observations, wesuggest that both GAFGs and PGAs are closely relatedlesions characterized by a mucous neck cell/chief celllineage phenotype.
Key words: chief cell, gastric adenocarcinoma of the fundicgland type, GNAS, mucous neck cell, pyloric gland adenoma
Gastric adenocarcinoma of the fundic gland type (GAFG)(chief cell predominant type) is a recently proposed subtypeof gastric adenocarcinomas.1,2 GAFG is composed of irregu-larly branching and anastomosing tubules lined by pale gray-blue, basophilic columnar cells with mild nuclear atypia,resembling chief cells. Cells positive for H.K-ATPase differ-entiating towards parietal cells have also been reported to bescattered in some GAFGs..1,2 However, molecular analysesfocusing on GAFG has never been reported previously.
Pyloric gland adenoma (PGA) is another rare type of gastrictumor which has been increasingly recognized as a distinctvariant of gastric-type adenoma.3–5 PGA is composed ofclosely packed pyloric-type glands lined by cuboidal/columnarcells with round nuclei and pale or eosinophilic cytoplasm.3–5
Recently, we reported that frequent GNAS and KRAS muta-tions occurring at high frequencies are characteristic geneticfeatures of PGAs of the stomach and duodenum.6
Currently, GAFGs and PGAs are thought to be entirelydistinct types of tumors. However, it is becoming increasinglyclear that GAFG and PGA share some clinicopathologicalfeatures: both lesions typically arise in the fundic glandmucosa, occur in older patients, and consistently expressMUC6.1–6 Furthermore, while GAFG is regarded as a low-grade malignancy that occasionally shows submucosalgrowth, some authors have questioned the malignant poten-tial of GAFGs based on their clinically benign nature andeven suggested that GAFGs should be re-classified asoxyntic gland polyps/adenomas.2,7 Based on these findings,we examined the potential relationships between GAFG andPGA, paying special attention to their genetic and phenotypicfeatures.
Correspondence: Ryoji Kushima, MD, PhD, Pathology and ClinicalLaboratory Division, National Cancer Center Hospital, 5-1-1Tsukiji,Chuoku 104-0045 Tokyo, Japan. Email: [email protected]
*Present address: Department of Pathology, National DefenseMedical College, Tokorozawa, Japan.
Disclosure: The authors declare that they have no conflict ofinterest.
Received 11 March 2013. Accepted for publication 14 May 2013.© 2013 The AuthorsPathology International © 2013 Japanese Society of Pathology andWiley Publishing Asia Pty Ltd
Pathology International 2013; 63: 318–325 doi:10.1111/pin.12070
bs_bs_banner
aberration in PGAs. We anticipate that the absence of KRASmutations might be a potentially useful characteristic for dis-criminating between GAFGs and PGAs, however, consider-ing the small number of GAFGs analyzed in the presentstudy, further analyses are required to confirm this prospect.
GAFG and PGAs are currently thought to be entirely dis-tinct tumors. However, based on their common localization inthe fundic gland area, partially overlapping immunohis-tochemical profiles and shared genetic alterations, wesuggest that GAFGs and PGAs are closely related lesionscharacterized by a mucous neck cell/chief cell lineagephenotype.
ACKNOWLEDGEMENT
The authors thank Dr Jason Mills (Washington UniversitySchool of Medicine, St. Louis, MO, USA) for his generous giftof the anti-MIST1 antibody, and Ms Sachiko Miura and MsChizu Kina for their skilful technical assistance. This studywas supported in part by a grant for the Development ofCancer Research and a grant for Scientific Research fromthe Ministry of Health, Labour, and Welfare, and by theNational Cancer Center Research and Development Fund(23-A-11), Japan.
REFERENCES
1 Ueyama H, Yao T, Nakashima Y et al. Gastric adenocarcinomaof fundic gland type (chief cell predominant type): Proposal for anew entity of gastric adenocarcinoma. Am J Surg Pathol 2010;34: 609–19.
2 Singhi AD, Lazenby AJ, Montgomery EA. Gastric adenocarci-noma with chief cell differentiation: A proposal for reclassifica-tion as oxyntic gland polyp/adenoma. Am J Surg Pathol 2012;36: 1030–35.
3 Chen ZM, Scudiere JR, Abraham SC, Montgomery E. Pyloricgland adenoma: An entity distinct from gastric foveolar typeadenoma. Am J Surg Pathol 2009; 33: 186–93.
4 Kushima R, Vieth M, Borchard F, Stolte M, Mukaisho K, HattoriT. Gastric-type well-differentiated adenocarcinoma and pyloricgland adenoma of the stomach. Gastric Cancer 2006; 9: 177–84.
5 Vieth M, Kushima R, Borchard F, Stolte M. Pyloric glandadenoma: A clinico-pathological analysis of 90 cases. VirchowsArch 2003; 442: 317–21.
6 Matsubara A, Sekine S, Kushima R et al. Frequent GNAS andKRAS mutations in pyloric gland adenoma of the stomach andduodenum. J Pathol 2013; 229: 579–87.
7 Montgomery EA, Voltaggio L. Biopsy Interpretation of the Gas-trointestinal Tract Mucosa. Volume 2: Neoplastic. Philadelphia,PA: Wolters Kluwer/Lippincott Williams & Wilkins, 2012; 85–8.
8 Lennerz JK, Kim SH, Oates EL et al. The transcription factorMIST1 is a novel human gastric chief cell marker whose expres-sion is lost in metaplasia, dysplasia, and carcinoma. Am JPathol 2010; 177: 1514–33.
9 Hattori T, Fujita S. Tritiated thymidine autoradiographic study oncellular migration in the gastric gland of the golden hamster. CellTissue Res 1976; 172: 171–84.
10 Hanby AM, Poulsom R, Playford RJ, Wright NA. The mucousneck cell in the human gastric corpus: A distinctive, functionalcell lineage. J Pathol 1999; 187: 331–7.
11 Cornaggia M, Capella C, Riva C, Finzi G, Solcia E. Electronimmunocytochemical localization of pepsinogen I (PgI) in chiefcells, mucous neck cells and transitional mucous-neck/chiefcells of the human fundic mucosa. Histochemistry 1986; 85:5–11.
12 Bredemeyer AJ, Geahlen JH, Weis VG et al. The gastric epi-thelial progenitor cell niche and differentiation of the zymogenic(chief) cell lineage. Dev Biol 2009; 325: 211–24.
13 Ramsey VG, Doherty JM, Chen CC, Stappenbeck TS,Konieczny SF, Mills JC. The maturation of mucus-secretinggastric epithelial progenitors into digestive-enzyme secretingzymogenic cells requires Mist1. Development 2007; 134: 211–22.
14 Landis CA, Masters SB, Spada A, Pace AM, Bourne HR, VallarL. GTPase inhibiting mutations activate the alpha chain of Gsand stimulate adenylyl cyclase in human pituitary tumours.Nature 1989; 340: 692–6.
15 Freda PU, Chung WK, Matsuoka N et al. Analysis of GNASmutations in 60 growth hormone secreting pituitary tumors: Cor-relation with clinical and pathological characteristics and surgi-cal outcome based on highly sensitive GH a nd IGF-I criteria forremission. Pituitary 2007; 10: 275–82.
16 Lee SH, Jeong EG, Soung YH, Lee JW, Yoo NJ, Lee SH.Absence of GNAS and EGFL6 mutations in common humancancers. Pathology 2008; 40: 95–7.
Figure 8 GNAS mutations in the GAFGs. Missense mutations areindicated by the arrowheads. Sequencing was performed using areverse primer.
Fundic gland and pyloric gland neoplasia 325
© 2013 The AuthorsPathology International © 2013 Japanese Society of Pathology and Wiley Publishing Asia Pty Ltd
Kushima R. Pathology International 2013
41%48%
OUTLINE• Fundic Gland Polyps
– Familial Adenomatous Polyposis– Gastric Adenocarcinoma & Proximal Polyposis [GAPPS]
• Hyperplastic Polyps– Prolapse and Inverted Variant– ‘Syndromic’ Differential Diagnosis On Pinch Biopsies
• Pyloric Adenoma• Gastric Adenocarcinoma Fundic Gland Type/ Oxyntic
Adenoma
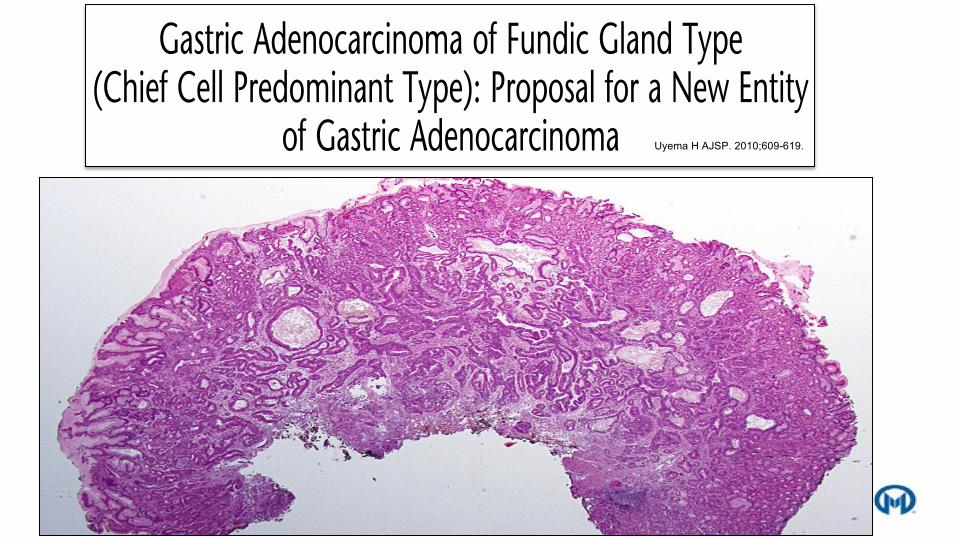
Gastric Adenocarcinoma of Fundic Gland Type(Chief Cell Predominant Type): Proposal for a New Entity
of Gastric AdenocarcinomaHiroya Ueyama, MD,*w Takashi Yao, MD,* Yutaka Nakashima, MD,z Katsuya Hirakawa, MD,yYumi Oshiro, MD,JMinako Hirahashi, MD,z Akinori Iwashita, MD,# and Sumio Watanabe, MDw
Abstract: Only a few cases of gastric adenocarcinoma of fundicgland type have been reported. Gastric adenocarcinoma withchief cell differentiation (GA-CCD) has been recently reportedas a new variant of gastric adenocarcinoma. However, itsclinicopathologic features are uncertain. To elucidate them, GA-CCDs exhibiting pepsinogen-I expression (10 lesions: Group A)and randomly selected gastric adenocarcinomas of differentiatedtype (111 lesions: Group B) were evaluated in this study. Celldifferentiation by MUC2, MUC5AC, MUC6, CD10, pepsino-gen-I, H+/K+-ATPase and chromogranin A, cell proliferationby Ki-67, and overexpression of p53 protein were evaluatedimmunohistochemically. In Group A, all GA-CCDs werelocated in the upper third of the stomach. Tumors were small,with the average maximum diameter ranging from 4 to 20(average, 8.6) mm. Histologically, GA-CCDs were well-differ-entiated adenocarcinomas composed of pale gray-blue, baso-philic columnar cells with mild nuclear atypia, resembling chiefcells. Immunohistochemically, scattered positivity for H+/K+-ATPase was observed in addition to expression of pepsinogen-Iand MUC6, indicating focal differentiation toward parietal cells.In Group B, pepsinogen-I was very focally expressed in 2 cases.As these 2 cases exhibited different clinicopathological andhistologic features, they cannot be categorized as GA-CCD.Mild atypism, no lymphovascular invasion, low proliferativeactivity, no overexpression of p53, and no recurrence indicatedless aggressiveness of GA-CCD. GA-CCD is rare, but it hasdistinct clinicopathological characteristics, especially in terms oftumor location, histologic features, phenotypic expression, andlow-grade malignancy. We propose gastric adenocarcinoma offundic gland type (chief cell predominant type) as a new entity ofgastric adenocarcinoma.
Key Words: gastric cancer, chief cell differentiation, pepsinogen-I,H+/K+-ATPase
(Am J Surg Pathol 2010;34:609–619)
Gastric adenocarcinoma of the intestinal type byLauren classification is very similar to that of the
differentiated type by Nakamura classification.12,18 Withrecent advances in mucin histochemistry and immuno-histochemistry, it has been clarified that intestinal-typeadenocarcinoma by Lauren classification contains thegastric phenotype.2,8,15,21,22,26,29
Although differentiated adenocarcinomas with thegastric phenotype including the foveolar type and pyloricgland type have been reported, there are only a few casesof adenocarcinomas with differentiation of fundicglands.27,28 Several cases of parietal cell carcinoma havebeen reported. However, differentiation of parietal cellswas confirmed by staining for H+/K+-ATPase in only 1case.28 Other cases of parietal cell carcinoma could betermed oncocytic adenocarcinomas, because immunohis-tochemical staining of H+/K+-ATPase characteristic forparietal cells were not carried out, or were negative.1,13,25
With regard to gastric adenocarcinoma with chief celldifferentiation, (GA-CCD) only 1 case has been reportedin a recent paper by Tsukamoto et al.27
We collected samples from 10 cases of GA-CCDand elucidated the associated clinicopathologic features,cell differentiation, and biologic behavior.
MATERIALS AND METHODS
Samples and Tissue Collection
Group AGA-CCDs are defined as neoplastic lesions, mainly
composed of highly differentiated columnar cells mimick-ing the fundic gland cells, mainly chief cells, with nuclearatypia. They grow in irregularly anastomosing glandsand acini, and have the ability to invade the stroma.In addition to the histologic similarity, differentiationtoward the chief cells was confirmed by immunohistochem-ical staining with pepsinogen-I (a marker for chief cells).Copyright r 2010 by Lippincott Williams & Wilkins
From the *Department of Human Pathology; wDepartment of Gastro-enterology, Juntendo University School of Medicine, Tokyo;zDivision of Pathology; yDivision of Gastroenterology, JapaneseRed Cross Fukuoka Hospital; zDepartment of Anatomic Pathology,Pathological Sciences, Graduate School of Medical Sciences, KyushuUniversity; #Department of Pathology, Fukuoka University Chi-kushi Hospital, Fukuoka; and JDepartment of Pathology, JapaneseRed Cross Matsuyama Hospital, Matsuyama, Japan.
Correspondence: Takashi Yao, MD, Department of Human Pathology,Juntendo University School of Medicine, 2-1-1 Hongo, Bunkyo-Ku,Tokyo, Japan, 113-8421 (e-mail: [email protected]).
ORIGINAL ARTICLE
Am J Surg Pathol ! Volume 34, Number 5, May 2010 www.ajsp.com | 609
Uyema H AJSP. 2010;609-619.


Chief cells
Parietal cells
H+/K+ ATP ase
Pepsinogen I

H+/K+ATPASE PEPSINOGEN
MUC-6 MUC-5AC

“Gastric adenocarcinoma with chief cell differentiation”?P53Ki-67
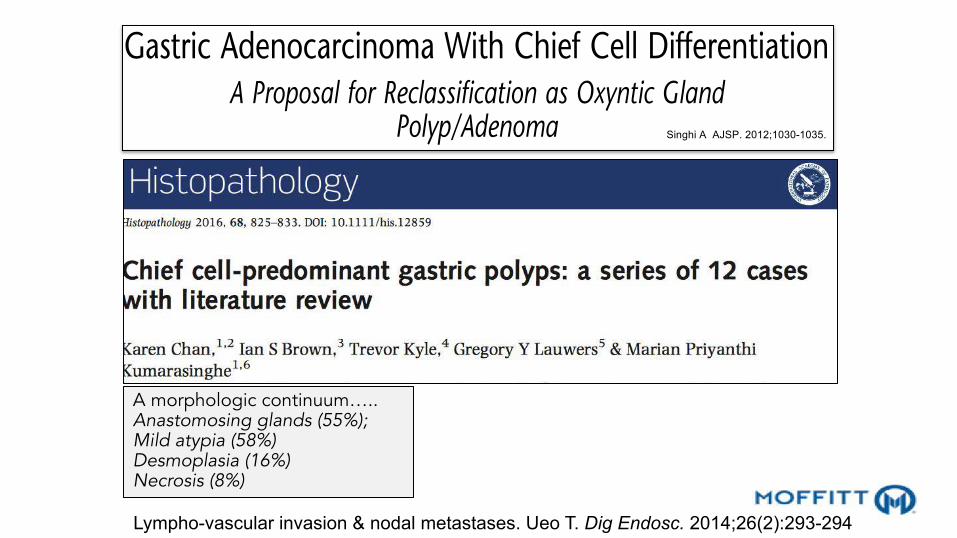
Gastric Adenocarcinoma With Chief Cell DifferentiationA Proposal for Reclassification as Oxyntic Gland
Polyp/Adenoma
Aatur D. Singhi, MD, PhD,* Audrey J. Lazenby, MD,w and Elizabeth A. Montgomery, MD*
Abstract: Gastric adenocarcinoma with chief cell differentiation(GA-CCD) has been reported as a new, rare variant of gastricadenocarcinoma. Only 12 cases in Japanese patients have beendescribed to date, but they demonstrate distinct clinicopathologicfeatures. To further characterize these lesions, we have collected 10additional cases. Patients ranged in age from 44 to 79 years (mean,64.2 y) with a relatively equal sex distribution (6 women and 4men). Stratified by race, 4 patients were Hispanic, 2 were White,2 were African American, 1 was Asian (Chinese), and the racewas unknown for 1 patient. All patients presented with gastro-esophageal reflux that prompted an endoscopic examination. Themajority of GA-CCDs were identified in the fundus (7 of 10, 70%)and the remaining in the cardia (n=3). Grossly, they were solitaryand polypoid, ranging in size from 0.2 to 0.8 cm (mean, 0.4 cm).Histologically, all cases were centered in the deep mucosa, withfocal involvement of surface foveolar epithelium in 3 (30%) casesbut not the submucosa. The tumors consisted of clustered glandsand irregular branching cords of oxyntic epithelium. Thin wisps ofradiating smooth muscle separated the epithelium, but desmo-plasia was distinctly absent in all cases. The oxyntic mucosa was 1to 2 cells thick and composed of a mixture of mucous neck, pa-rietal, and chief cells. In 7 of 10 (70%) cases, chief cells were thepredominant cell type, whereas the remaining 3 cases consistedprimarily of mucous neck cells. The nuclei were mildly enlargedwith slight nuclear pleomorphism, but no mitotic figures wereidentified. In addition, necrosis, lymphovascular invasion, andperineural invasion were absent. Immunohistochemically, GA-CCDs were diffusely positive for MUC6 (10 of 10, 100%) andnegative for MUC5AC (0%) and MUC2 (0%). Ki-67 im-munolabeling demonstrated variable expression, with the highestareas ranging from 0.2% to 10%. Clinical follow-up was availablefor 9 of 10 (90%) patients and ranged from 6 to 39 months. Onepatient had persistence of lesion at 6 months because of incompleteremoval, whereas the other 8 were disease free. In summary, GA-CCDs are solitary, mucosal lesions of the gastric cardia/fundus
that arise in patients from multiple ethnic backgrounds. Consid-ering that patients within this study and those reported previouslyhave had neither true recurrence nor progression of disease, theselesions are best regarded as benign. Consequently, the term GA-CCD is contradictory and we prefer the descriptive term “oxynticgland polyp/adenoma” until further studies can clarify thepathogenesis of these lesions and their natural history.
Key Words: fundic gland polyp, oxyntic gland adenoma, chiefcell hamartoma
(Am J Surg Pathol 2012;36:1030–1035)
Gastric adenocarcinoma is one of the most commoncancers worldwide, accounting for over 934,000 cases
annually. Approximately 700,000 people succumb to thismalignancy each year, and the 5-year survival rate in theUnited States is 24%.3 It constitutes a heterogenous groupof tumors with variable clinical and pathologic features.Many classification systems for gastric adenocarcinomaexist that are based on tumor location, invasiveness, histo-logic features, growth pattern, and even mucin immuno-phenotyping. Most institutions use the World HealthOrganization classification, which recognizes 5 main histo-logic types and various rare entities.9 The advantage of theWorld Health Organization classification system is the rec-ognition of morphologic patterns; however, it does not takeinto account epidemiologic data or histogenesis.
Recently, a new histologic type of gastric ad-enocarcinoma termed gastric adenocarcinoma with chiefcell differentiation (GA-CCD) was described by Tsukamotoet al15 as a report of a single case. A subsequent follow-upstudy of 10 cases of GA-CCD by Ueyama et al17 expandedon the clinicopathologic features of this entity. However,other than in a single case report from German colleaguesthat we believe reflects the same entity, it has yet to be welldescribed in non-Japanese patients.11 Herein, we report aseries of 10 additional patients with this lesion, characterizingit further with special attention to its spectrum of histologicfeatures and biological behavior.
MATERIALS AND METHODSTen cases of GA-CCD collected between 2008 and
2011 were retrieved from the consultation files of 2 of theauthors (E.A.M. and A.J.L.) and from The Johns Hopkins
From the *Department of Pathology, The Johns Hopkins MedicalInstitutions, Baltimore, MD; and wDepartment of Pathology,University of Nebraska, Omaha, NE.
Conflicts of Interest and Source of Funding: The authors have disclosedthat they have no significant relationships with, or financial interestin, any commercial companies pertaining to this article.
Correspondence: Elizabeth A. Montgomery, MD, The Johns HopkinsMedical Institutions, 401N Broadway, Weinberg 2242, Baltimore,MD 21231-2410 (e-mail: [email protected]).
Copyright r 2012 by Lippincott Williams & Wilkins
ORIGINAL ARTICLE
1030 | www.ajsp.com Am J Surg Pathol ! Volume 36, Number 7, July 2012
Singhi A AJSP. 2012;1030-1035.
A morphologic continuum…..Anastomosing glands (55%); Mild atypia (58%)Desmoplasia (16%)Necrosis (8%)
Lympho-vascular invasion & nodal metastases. Ueo T. Dig Endosc. 2014;26(2):293-294

SUMMARY: NEW TRENDS IN GASTRIC POLYPS• Fundic Gland Polyps
– Familial Adenomatous Polyposis• Frequently dysplastic but low rate of progression
– Gastric Adenocarcinoma & Proximal Polyposis [GAPPS]• ‘Atypical’ lesions (Hyperproliferative Aberrant Pits)
• Hyperplastic Polyps– New Variants
• Prolapsed and inverted of limited clinical significance– ‘Syndromic’ Differential Diagnosis on Pinch Biopsies
• Better characterization of upper GIT lesions• Pyloric Adenoma
• Expanding clinical associations; spectrum from LGD to HGD and natural history• Gastric Adenocarcinoma Fundic Gland Type/ Oxyntic Adenoma
• Spectrum of lesions; predominantly ‘low grade’; GNAS mutation shared w/ PGA