new trend in acute ischemic stroke management · 7/4/2019 1 new trend in acute ischemic stroke...
TRANSCRIPT

7/4/2019
1
New trend in acute ischemic
stroke management
Jesada Keandoungchun, MD
Acute Stroke treatment base on level I evidence
Stroke units
ASA in 48 h
1993 1995 1997 2007 2008-18
IV rtPA in 3 h
IV rtPA in 4.5 h
Hemicraniectomy
1998
IA proUK in 6 h
2004 2005
CLOTBUST
MERCI in 8 h
PWI/DWI mismatch 2003 IVT +
Antiplatelets
Neuroprotection
Anticoagulant
IV/IA ++IV/IA
All stroke patients are potentially eligible
↓ 3% in mortality
↓ 5% in long term dependency
Benefits persists up to 10 y
Lancet 2004; 363: 834–5
Routine Care as Specialist
Stroke UnitIVT: Number needed to treat to excellent recovery (mRS 0, 1)
Hacke W et al. Lancet 2004;363:768-774.
Lees KR et al. Lancet 2010;375:1695-1703.
2.5 vs 3.2%; OR 23
1 vs 0.8%; OR 22
8.2 vs 9.1%; OR 11
ASA 160-300 mg in 48 h (IST, CAST, MAST-I)
Stroke 2000;31:1240-1249
3 days after onset
Early Hemicraniectomy in Malignant MCA infarct
Lancet Neurol 2007; 6: 215–22

7/4/2019
2
Acute Ischemic Stroke treatment: level I evidence
Stroke units
ASA in 48 h
1993 1995 1997 2007 2008-10
IV rtPA in 3 h
IV rtPA in 4.5 h
Hemicraniectomy
1998
IA proUK in 6 h
2004 2005
CLOTBUST
MERCI in 8 h
PWI/DWI mismatch 2003 IVT +
IV/IA ++IV/IA
Lancet 2008; 371: 1612–23
Acute Stroke treatment base on level I evidence
Stroke units
ASA in 48 h
1993 1995 1997 2007 2008-18
IV rtPA in 3 h
IV rtPA in 4.5 h
Hemicraniectomy
1998
IA proUK in 6 h
2004 2005
CLOTBUST
MERCI in 8 h
PWI/DWI mismatch 2003 IVT +
Antiplatelets
Neuroprotection
Anticoagulant
IV/IA ++IV/IA
Thailand: IV rtPA, Stroke unit
NEW TREND
Female 81 y present with quadriparesis, drowsy, ophthalmoparesis (NIHSS 24) 1 h and S/P CABG for 2 days.
Thrombolysis: postoperative stroke
Neurol Clin 2006; 24: 783-793
Major surgery within 14 days
INCLUSION criteria
• Age ≥ 18 years
• Onset < 4.5 hours
• Clinical diagnosis of ischemic stroke
EXCLUSION criteria
• SBP ≥ 185 or DBP ≥ 110 mmHg
• Symptoms rapidly improving or minor symptoms (NIHSS ≤ 4)
• Seizure with postictal deficit
• Plasma glucose < 50
• Arterial puncture at a noncompressible site or LP within 7 days
• Major surgery within 14 days
• GI hemorrhage or urinary tract hemorrhage within 21 days
• Stroke or head trauma or MI within 3 months
• Symptoms of SAH (diffuse headache, stiffness of neck)
• Previous intracranial hemorrhage
• If oral anticoagulant, INR >1.7, heparin in previous 48 h, aPTT > 40
• Platelet count < 100,000
• Intraaxial intracranial neoplasm
• IE, Aortic dissection
• CT show ICH, multilobar infarct (hypodensity > 1/3 cerebral hemisphere)
IV Thrombolysis eligible criteria3-4.5 h
Age ≤80 y
without DM + prior stroke
NIHSS ≤25
not taking any OACs
Conclusions: application of SMART criteria is safe and effective
Journal of Stroke and Cerebrovascular Diseases, 2016; 25 (5): 1110–1118

7/4/2019
3
Journal of Stroke 2015;17(2):123-126
Endovascular Therapy (EVT) in 6 hHighly Effective Reperfusion evaluated in Multiple Endovascular Stroke Trials (HERMES)
collaboration RECANALIZATION REPERFUSION Recovery
Endovascular Therapy in 6 h
EVT with stent retriever (I, A) in
AIS receiving IV r-tPA in 4.5 h + ICA or M1-MCA (BA)
prestroke mRS 0 -1, age ≥18 y, NIHSS ≥6
ASPECTS ≥6
EVT (groin puncture) in 6 h TSS EVT guideline 2016
ASA Guidelines 2015Mean NIHSS: MR CLEAN 17: RAMA 18 (sICH 6%)
28.5
33
19
35.8
18
16
35.7
28
43
0
21
22
0% 20% 40% 60% 80% 100%
Ramathibodi
MR CLEAN
control
mRS 0-2 mRS 3 mRS 4-5 mRS 6
↑ 14%
Endovascular Therapy: ASA Guidelines 2015
EVT with stent retriever (I, A) in
AIS receiving IV r-tPA in 4.5 h
ICA or M1-MCA
prestroke mRS 0-1, age ≥18 y
NIHSS ≥6
ASPECTS ≥6
EVT (groin puncture) in 6 h
JAMA. 2016;316(12):1279-1288
Concept of acute stroke: Time is Brain
Minutes Hours
Every 1 minute delay in Supratentorial Stroke
“Death of 1.9 million neurons, 14 billion synapses, 12
km of myelinated fibers, accelerated aging 3.1 wk”
Stroke 2006; 37: 263-266
Infarct growth rates in patients with ICA or MCA occlusions: DEFUSE 2
Stroke. 2018; 49: 768-771
50%: slow growth: < 3 ml/h
30%: medium growth: 3-10 ml/h
20%: rapid growth: 15-100 ml/h
JNNP 2018; 0: 1–7
New trend in acute ischemic stroke management
Time base Tissue base

7/4/2019
4
CTP mismatch: CBF/TmaxThrombectomy 6 to 24 Hours after Stroke with a Mismatch
between Deficit and Infarct (DAWN trial)
• AIS 6-24 h (median 12 h), ICA or MCA-M1 occlusion + mismatch between clinical deficit & infarct volume
NEJM 2018;378:11-21
mRS 0-2: 49 vs 13%, posterior probability of superiority, >0.999
sICH: 6 vs 3%, P=0.50, Mortality 19 vs 18%, P=1.0
Thrombectomy for Stroke at 6 to 16 Hourswith Selection by Perfusion Imaging (DEFUSE 3 trial)
• AIS 6-16 h (median 12 h), ICA or MCA-M1 occlusion + perfusion mismatch
NEJM 2018;378:11-21
mRS 0-2: 45 vs 17%, OR 2.67 P<0.001
sICH: 7 vs 4%, P=0.75, Mortality 14 vs 26%, P=0.05
Intervent Neurol 2018;7:513–521
rCBF <0.3 143 Tmax>6s 422ml
M 70 y + Rt. anterior circulation infarct, NIHSS 19
NIHSS after EVT: 14, D5: 5; mRS 3M: 2
DAWN, DEFUSE 3-
IVT 4.5-9 h

7/4/2019
5
IVT 4.5-9 h or wake up stroke
• AIS 4.5-9 h or wake up (median 7 h) + perfusion mismatch
Lancet 2019 doi.org/10.1016/S0140-6736(19)31053-0
mRS 0-1: 36 vs 29%, P=0.01
sICH: 5 vs 0.5%, P=0.03, Mortality 14 vs 9%, P=0.19
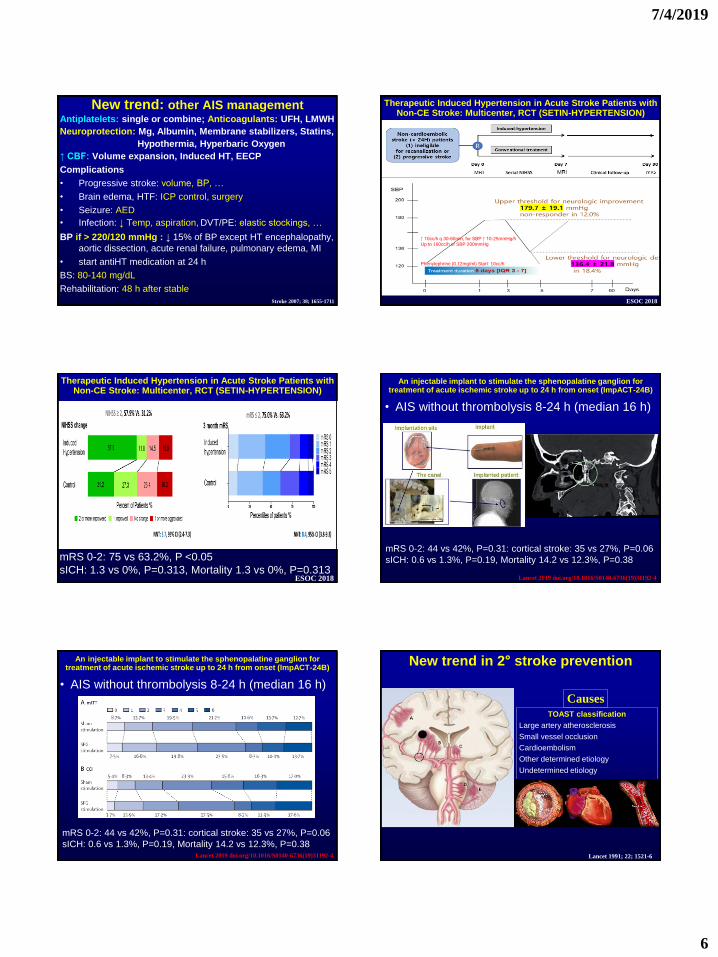
Antiplatelets: single or combine; Anticoagulants: UFH, LMWH
Neuroprotection: Mg, Albumin, Membrane stabilizers, Statins,
Hypothermia, Hyperbaric Oxygen
↑ CBF: Volume expansion, Induced HT, EECP
Complications
• Progressive stroke: volume, BP, …
• Brain edema, HTF: ICP control, surgery
• Seizure: AED
• Infection: ↓ Temp, aspiration, DVT/PE: elastic stockings, …
BP if > 220/120 mmHg : ↓ 15% of BP except HT encephalopathy,
aortic dissection, acute renal failure, pulmonary edema, MI
• start antiHT medication at 24 h
BS: 80-140 mg/dL
Rehabilitation: 48 h after stable
New trend: other AIS management
Stroke 2007; 38; 1655-1711
CHANCE: Clopidogrel in High-Risk Patients with Acute
Nondisabling Cerebrovascular Events
• RCT: Clopidogrel 75 mg (300mg d1) + ASA 75-300mg for 21 days then Clopidogrel
vs ASA
• 5,170 AIS patients (age ≥40y): NIHSS≤3, TIA (ABCD2 ≥ 4) within 24 h; F/U 90 d
• BP < 160/100
1° outcome: stroke: 8.2 vs 11.7% (HR 0.68; 0.57-0.81)
2° outcome: severe bleeding: 0.2 vs 0.2% (HR 0.94; 0.24-3.79)
hemorrhagic stroke: 0.3 vs 0.3% (HR 1.01; 0.38-2.70)
• Chinese: CYP2C19 *2 50% *3 7% in Asian
• Traditional Chinese Medicine 24%N Engl J Med 2013;369:11-19
Circulation. 2015;132:40-46
1 year
Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA
Platelet-oriented inhibition in new TIA and minor ischemic stroke (POINT) trial
Clopidogrel 600mg day1 + ASA vs ASA (162 mg OD x 5 days then 50-325 mg 90 days)
AIS NIHSS≤3, TIA (ABCD2 ≥4) within 12 h; F/U 90 d
N Engl J Med 2018; 379:215-225
TARDIS: The Triple Antiplatelets For Reducing Dependency In Ischemic Stroke
PROBE: A+D+C vs ASA+Dypyridamole or Clopidogrel 1M
3096 AIS/TIA (NIHSS 2.8, ABCD2 >4) patients in 48 h; F/U 90 d
Early stop trial
Lancet. 2018;391: 850-859
6 vs 7%
20 vs 9%
Antiplatelet Treatment
1. Administration of aspirin is recommended in patients with AIS within 24 to 48
hours after onset. For those treated with IV alteplase, aspirin administration
is generally delayed until 24 hours later but might be considered in the
presence of concomitant conditions for which such treatment given in the
absence of IV alteplase is known to provide substantial benefit or
withholding such treatment is known to cause substantial risk.
2. Aspirin is not recommended as a substitute for acute stroke treatment in
patients who are otherwise eligible for IV alteplase or mechanical
thrombectomy.
3. In patients presenting with minor stroke, treatment for 21 days with dual
antiplatelet therapy (aspirin and clopidogrel) begun within 24 hours can be
beneficial for early secondary stroke prevention for a period of up to 90 days
from symptom onset.
4. Ticagrelor is not recommended (over aspirin) in the acute treatment of
patients with minor stroke.
I, A
III, B-R
IIa, B-R
III, B-R
7/4/2019
6
Antiplatelets: single or combine; Anticoagulants: UFH, LMWH
Neuroprotection: Mg, Albumin, Membrane stabilizers, Statins,
Hypothermia, Hyperbaric Oxygen
↑ CBF: Volume expansion, Induced HT, EECP
Complications
• Progressive stroke: volume, BP, …
• Brain edema, HTF: ICP control, surgery
• Seizure: AED
• Infection: ↓ Temp, aspiration, DVT/PE: elastic stockings, …
BP if > 220/120 mmHg : ↓ 15% of BP except HT encephalopathy,
aortic dissection, acute renal failure, pulmonary edema, MI
• start antiHT medication at 24 h
BS: 80-140 mg/dL
Rehabilitation: 48 h after stable
New trend: other AIS management
Stroke 2007; 38; 1655-1711
Therapeutic Induced Hypertension in Acute Stroke Patients with Non-CE Stroke: Multicenter, RCT (SETIN-HYPERTENSION)
ESOC 2018
Phenylephrine (0.12mg/ml) Start: 10cc/h
↑ 10cc/h q 30-60min, for SBP ↑ 10-25mmHg/h
Up to 160cc/h or SBP 200mmHg
Therapeutic Induced Hypertension in Acute Stroke Patients with Non-CE Stroke: Multicenter, RCT (SETIN-HYPERTENSION)
ESOC 2018
mRS 0-2: 75 vs 63.2%, P <0.05
sICH: 1.3 vs 0%, P=0.313, Mortality 1.3 vs 0%, P=0.313
An injectable implant to stimulate the sphenopalatine ganglion for treatment of acute ischemic stroke up to 24 h from onset (ImpACT-24B)
• AIS without thrombolysis 8-24 h (median 16 h)
Lancet 2019 doi.org/10.1016/S0140-6736(19)31192-4
mRS 0-2: 44 vs 42%, P=0.31: cortical stroke: 35 vs 27%, P=0.06
sICH: 0.6 vs 1.3%, P=0.19, Mortality 14.2 vs 12.3%, P=0.38
An injectable implant to stimulate the sphenopalatine ganglion for treatment of acute ischemic stroke up to 24 h from onset (ImpACT-24B)
• AIS without thrombolysis 8-24 h (median 16 h)
Lancet 2019 doi.org/10.1016/S0140-6736(19)31192-4
mRS 0-2: 44 vs 42%, P=0.31: cortical stroke: 35 vs 27%, P=0.06
sICH: 0.6 vs 1.3%, P=0.19, Mortality 14.2 vs 12.3%, P=0.38
TOAST classification
Large artery atherosclerosis
Small vessel occlusion
Cardioembolism
Other determined etiology
Undetermined etiology
Lancet 1991; 22; 1521-6
Causes
New trend in 2° stroke prevention

7/4/2019
7
Caplan: Neurology 1989;39;1246
Small artery occlusion 46%
Large artery stenosis
Intracranial 36%
Extracranial 10%
Cardioembolic 8%
Arch Neurol. 2002; 59:259-263
Stroke mechanism: Lacunar Infarct Cerebral Angiography
Intracranial stenosis: vascular wall imaging
Stroke. 2014;45:2457-2460
7T MRI
NeuroImage 168 (2018) 452–458
Adapt from Frontiers in Neurology 2016; 37: 1-16
AF detection AAA
PFO, …
DVT leg/ pelvis
D-dimer, APS, …
Genetic testing- GLA gene analysis
(www.geneticrama.com)
- Prothrombin mutation
(FII20210G>A)
- FV Leiden
(FV1691G>A)
- MELAS 3243 A>G
- NOTCH3 gene
- RNA gene, …
CT chest, Abdomen
PET
Leptomeningeal Biopsy
Causes of Ischemic Stroke
The more you look, the more you find
Stroke. 2014;45:1186-1194
2nd stroke prevention based on level I evidence
†Calculations based on mean follow-up of 3.9 years in PROGRESS
(NNT=25) and median 4.9 years in SPARCL (NNT=45)
Lancet 2008; 371: 1612–23
7/4/2019
8
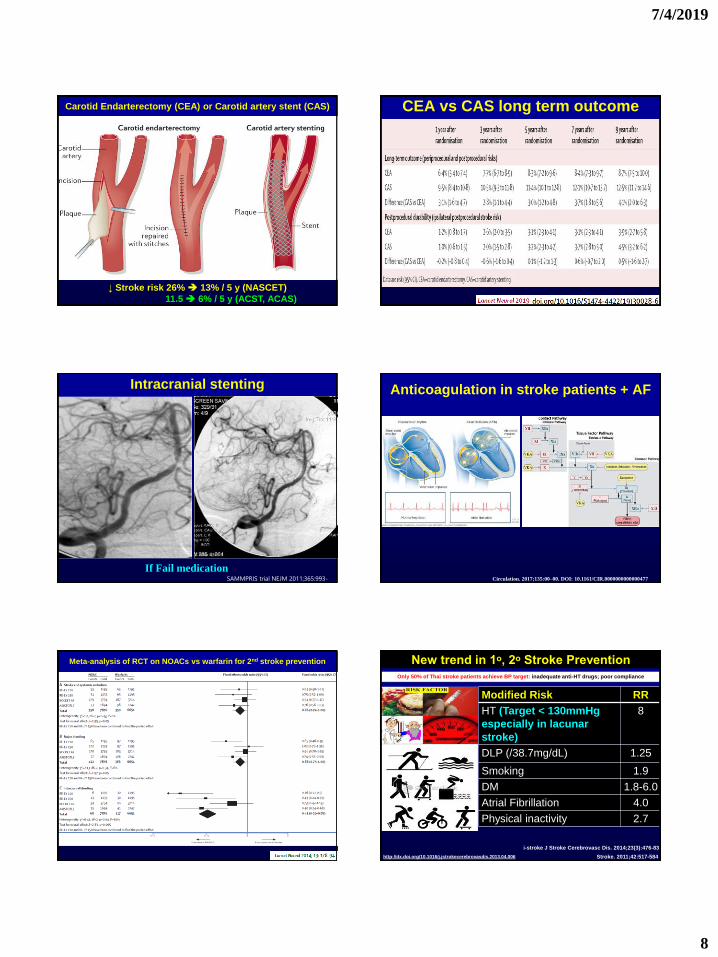
Carotid Endarterectomy (CEA) or Carotid artery stent (CAS)
↓ Stroke risk 26% 13% / 5 y (NASCET)
11.5 6% / 5 y (ACST, ACAS)
CEA vs CAS long term outcome
Intracranial stenting
If Fail medicationSAMMPRIS trial NEJM 2011;365:993-
1003
Anticoagulation in stroke patients + AF
Circulation. 2017;135:00–00. DOI: 10.1161/CIR.0000000000000477
Meta-analysis of RCT on NOACs vs warfarin for 2nd stroke prevention New trend in 1ᵒ, 2ᵒ Stroke Prevention
Modified Risk RR
HT (Target < 130mmHg
especially in lacunar
stroke)
8
DLP (/38.7mg/dL) 1.25
Smoking 1.9
DM 1.8-6.0
Atrial Fibrillation 4.0
Physical inactivity 2.7
Stroke. 2011;42:517-584http://dx.doi.org/10.1016/j.jstrokecerebrovasdis.2013.04.006
Only 50% of Thai stroke patients achieve BP target: inadequate anti-HT drugs; poor compliance
i-stroke J Stroke Cerebrovasc Dis. 2014;23(3):476-83

7/4/2019
9
Conclusion: new trend in acute ischemic stroke management
Acute Stroke treatment
• IVT < 4.5 4.5-9 h
• EVT up to 24 h or more
• Antiplatelets: ASA ASA + loading Clopidogrel
• Increase CBF: induce HT, …
2◦ stroke prevention
• Antiplatelets: single or combined
• Anticoagulants: warfarin NOACs
• …
Primary prevention: BP target <130