new israeli guidelines for celiac diseae
TRANSCRIPT

New Israeli guidelines for Celiac Diseae
SHIMON REIF, MD DEPARTMENT OF PEDIATRICS HADASSAH MEDICAL CENTER

Celiac Disease Why is it so important
• Very common disease
• Uncommon presentation – Atypical symptoms
• Treatable disease

Healthy subjects
Latent coeliac disease
Silent coeliac disease
Manifest coeliac disease Villous atrophya
Normal mucosa
DR3-DQ2 DR5/7-DQ2 DR4-DQ8
Gen
etic
incl
inat
ion
Celiac iceberg

Definition • Traditional definition Disease of the proximal small intestine
characterized by an abnormal small intestinal mucosa and associated with permanent intolerance to gluten
• Modern definition T-lymphocyte mediated small intestinal
enteropathy induced by gluten in genetically predisposed individuals

The Changing Celiac Epidemiology
1980 1990 2000 >
AGA EMA TTG
The availability of sensitive serological markers made it possible to discover Celiac Disease even when the clinical suspicion was low.
DGP 2007

Pathogenesis
• Genetic predisposition
• Environmental triggers – Dietary – Non dietary?
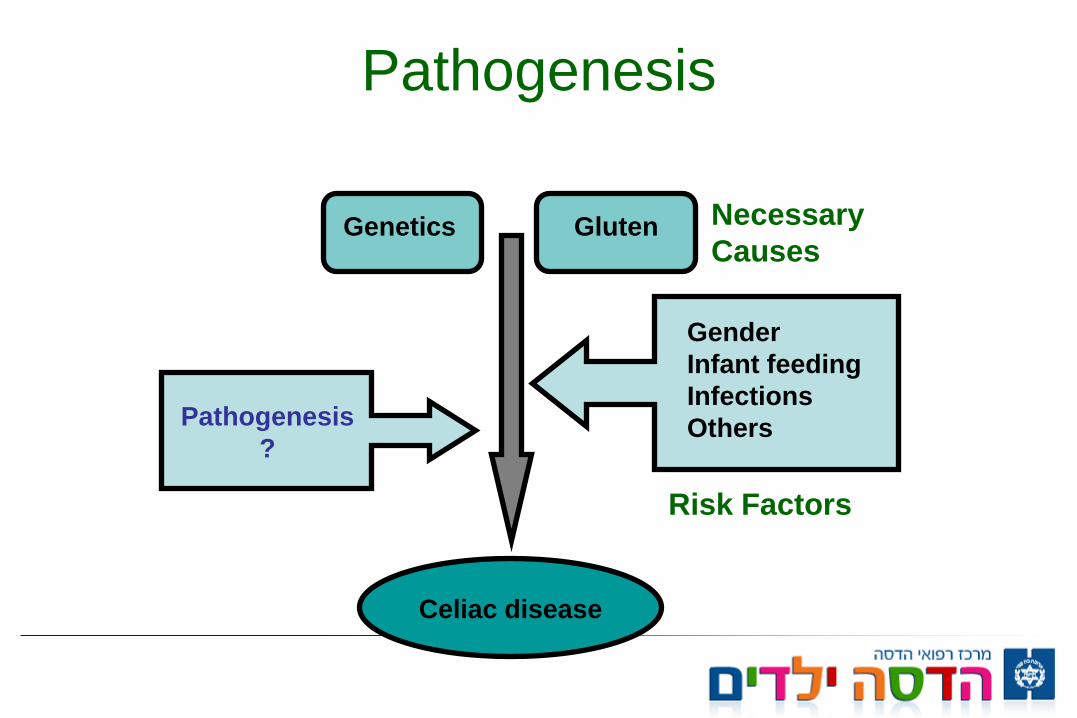
Pathogenesis
Celiac disease
Genetics Gluten Necessary Causes
Gender Infant feeding Infections Others
Risk Factors
Pathogenesis ?

Dietary Factors
• Wheat - (15% protein, 75% starch)
• Rye prolamines - secalins • Barley prolamines - hordeins • Oats prolamines - avenins
Gluten Gliadin
(alcohol soluble) Prolamine
Glutenin (alcohol insoluble))


5
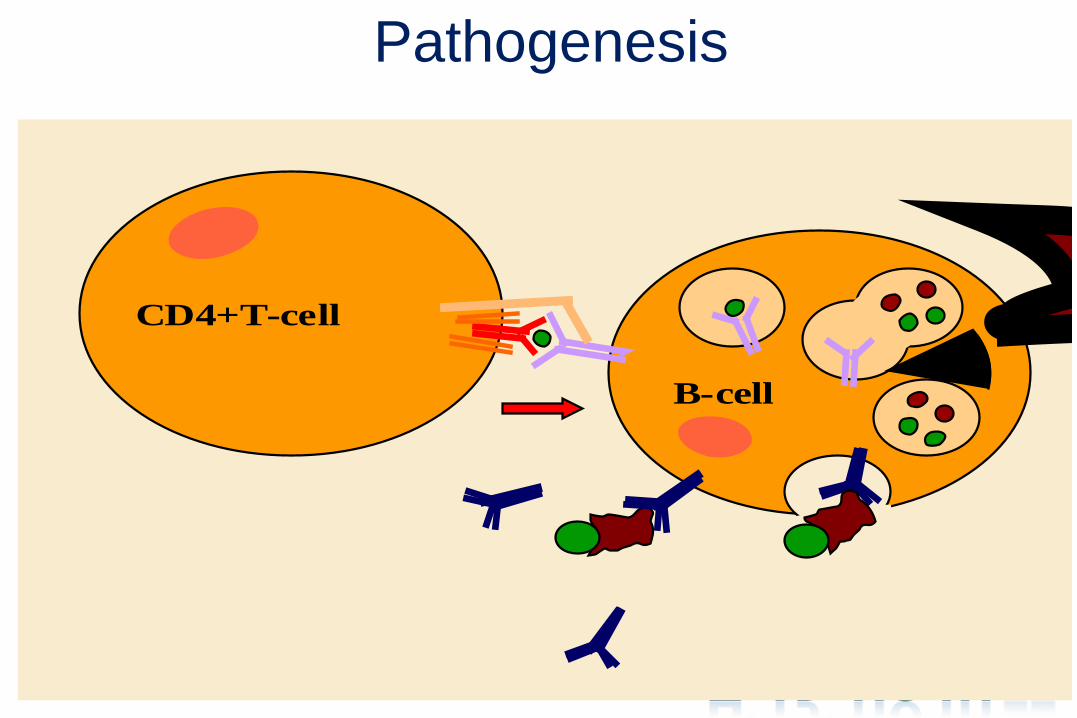
Submucosa
T B AGA, EMA,
atTG
Cytokines (IL2, IL15) Tk
P
TTG 3
4 7 APC
2 1
6b
6a
8
2a
2b
8

Prevalence of Celiac Disease is Higher in Other Autoimmune Conditions
Type 1 Diabetes Mellitus: 3.5 - 10%
Thyroiditis: 4 - 8%
Arthritis: 1.5 - 7.5%
Autoimmune liver diseases: 6 - 8%
IgA Deficiency: 5-7%
• Down Syndrome: 4-19% • Turner Syndrome: 4-8%
General Population: 1%
Genetics
• Concordance in monozygotic twins is 70%
• Concordance in HLA-identical siblings 30 – 40%
• suggesting other genes involved and environmental factors


Clinical Manifestations
• Gastrointestinal (“classical”)
• Non-gastrointestinal ( “atypical”)
• Asymptomatic
In addition, Celiac Disease may be associated with other conditions, and mostly with: • Autoimmune disorders • Some syndromes

Gastrointestinal Manifestations
• Diarrhea, malabsorption • Abdominal pain , IBS • Abdominal distention • Constipation • FTT, Short statue • Vomiting, anorexia, irritability • Edema • Increased stool mass

Non GI Manifestations
• Anemia • Osteoporosis, osteopenia • Neurologic: neuropathy, myopathy, convulsions • Hepatic: Elevated transaminases - most common 10-
25%, Hepatitis, PBC • OBGYN: Infertility, recurrent abortion, amenorrhea,
sperm abnormalities, delayed puberty • Aptos stomatitis, Enemal hypoplasia

Hematopoietic
• anemia - iron or folate deficiency, but also increased blood loss
• B12 deficiency in severe cases • hyposplenism - may resolve with dietary therapy • thrombocytosis with Howell-Jolly bodies • bleeding diathesis

Osteopenic bone disease
• decrease Ca absorption • decrease in absorption fat-soluble vitamin D • binding of Ca and Mg in lumen by unabsorbed
dietary fatty acids

Neurologic symptoms
• peripheral neuropathy • myopathy • cerebellar ataxia • myoclonus • cerebral atrophy and dementia • cerebral vasculitis • brain-stem encephalitis • epilepsy and cerebral calcifications

CT Scan Showing Occipital Calcifications in a Boy with
Celiac Disease and Epilepsy

OB-GYN
• Impaired fertility in women • Sperm abnormalities • high incidence of spontaneous abortion • low birth-weight babies • reduced breast milk production • Amenorrhea • paripartum exacerbation or first presentation • correctable with gluten-free diet
Renal and liver disease
• Glomerulonephritis • IgA nephropathy may respond to gluten-free diet • PBC, PSC and chronic active hepatitis • Elevated transaminases - most common 10-25% • Non specific hepatitis • Responds to GFD

Dermatitis Herpetiformis
• Erythematous macule > urticarial papule > tense vesicles
• Severe pruritus
• Symmetric distribution
• 90% no GI symptoms
• 75% villous atrophy
• Gluten sensitive
Garioch JJ, et al. Br J Dermatol. 1994.

Involve the secondary dentition May be the only presenting sign of Celiac Disease
Dental Enamel Defects

Recurrent Aphtous Stomatitis
By permission of C. Mulder, Amsterdam (Netherlands)

Osteoporosis
Low bone mineral density improves in children on a gluten-free diet.

The Celiac Iceberg
Symptomatic Celiac Disease
Silent Celiac Disease
Latent Celiac Disease
Genetic susceptibility: - DQ2, DQ8 Positive serology
Manifest mucosal lesion
Normal Mucosa

Serologic Tests for CD Why are thet so important
• Non-invasive, inexpensive, patient acceptance
• Diagnostic markers • Subclinical markers for at-risk individuals
(ex: family members), screening, earlier treatment
• Follow-up, monitoring, active vs inactive disease
• Major contributionto the diagnosis, pathogenesis and treatment of CD

TO SCREEN OR NOT TO SCREEN??
• No General Screening
• Selective screening
• High index of suspicious

Who to screen
• First degree relative Associated syndromes • Down, Turner Associated diseases • Type I DM, thyroiditis • Selective IgA deficiency < 5 mg%

Laboratory studies (Malabsorption)
• Common nutritional deficiencies at diagnosis: – Iron deficiency – Folate deficiency – Fat malabsorption (steatorrhea) – Carbohydrate malabsorption (flat glucose
tolerance test, abnormal xylose test)
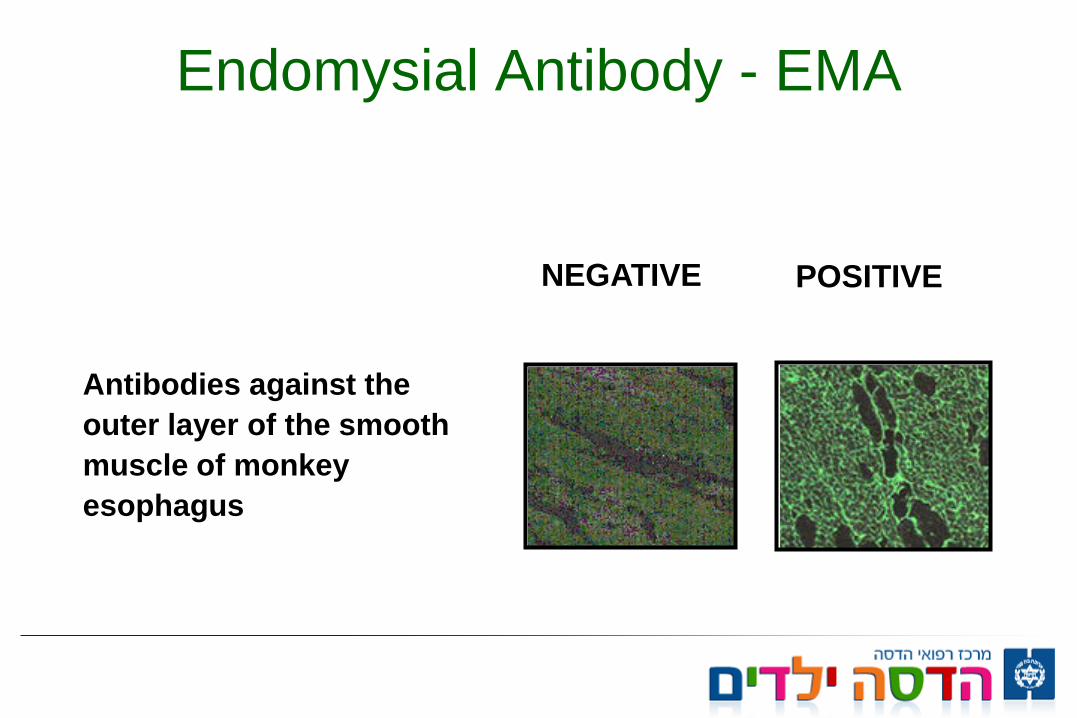
Endomysial Antibody - EMA
Antibodies against the outer layer of the smooth muscle of monkey esophagus
NEGATIVE POSITIVE
Antiendomysial antibodies (IgA)
Disadvantages: –Technically difficult to interpret with inter-
observer variability –Inappropriate for mass screening (Time
consuming) –Lower sensitivity in children < 2 years –Absent in IgA deficiency

Tissue Transglutaminase enzyme
• Transglutaminase is the substrate of antiendomysium
• In celiac disease the transglutaminase is the autoantigen
• Antibodies detected by ELISA • Ideal for mass screening

Deamidated Gliadin Peptide DGP - ELISA
• Entirely synthetic peptide. • Contains fewer than 35 amino acids. • This peptide is derived from whole molecule
gliadin and has been selectively deamidated, causing glutamine to convert to glutamic acid, mimicking the action of tTG.
• Detects both IgA and IgG isotopes.

HLA testing
• HLA DQ2 – 95% of CD • DQ8 – 5% • DQ2 – 30% of general population • Therefore HLA testing has a high negative
predicting value • Negative DQ2/DQ8 excludes CD with 99%
confidence

Diagnosis of CD (original ESPGAN/Interlaken criteria)
• Abnormal small intestinal mucosa (usually flat) on gluten containing diet
• Clinical response to a gluten free diet • Histologic response to a gluten free diet • Histologic + clinical relapse following
gluten challenge
Revised ESPGAN criteria
mandatory requirements: 1. Abnormal small intestinal mucosa (usually flat) on
gluten containing diet 2. Full clinical remission after withdrawal of gluten from
the diet 3. Presence of antibodies (EMA/TTG) at diagnosis and
their disappearance on GFD support the diagnosis
Israeli Guidelines for Celiac Disease Diagnosis & Treatment
• Amir Bentov - Macabi • Shimon Reif – Hadassah, Jerusalem • Michal Kori – Kaplan, Rechovot • Michael Wilshanski – Hadassah, Jerusalem • Yoram Buyanover – Safra, Tel Hashomer • Ron Shaul – Rambam, Haifa • Raanan Shamir – Schneider, Petah-Tikva





Histological Features
Normal 0 Infiltrative 1 Hyperplastic 2
Partial atrophy 3a Subtotal atrophy 3b Total atrophy 3c
Horvath K. Recent Advances in Pediatrics, 2002.


Background
• The prevalence of CD in Israel is the same as in most of other countries around 1%
• Due to numerous new guidelines in many societies and new diagnostic tools the Israeli society of Pediatric Gastroenterology decided to summit Israeli guidelines for CD


Indications for serology test
• Abdominal pain • Abdominal Distention • Chronic or intermittent
diarrhea • FTT • Weight loss • Iron deficiency anemia • Constipation – not
responding to treatment
• Chronic fatigue • Short statue • Delayed puberty • Recurrent aphtous
stomatitis • Dermatitis Herpetiforme • Osteopenia, recurrent
fractures • Persistent elevated liver
enzymes

Conditions require serology tests
• First degree relatives with CD • IgA Deficiency Genetic conditions • Down, Turner, Williams Syndromes Autoimmune disorders • Type 1 Diabetes mellitus • Autoimmune Hepatitis • Autoimmune thyroidits

Genetic Tests • Its main goal is as negative predictor • Negative test R/O almost completely CD Indications • Uncertain diagnosis or discrepancy between
tests. e.g. clinical symptoms, compatible biopsy and negative serology
• First degree relatives • Can be initial test in genetic or autoimmune
disease associated with CD

Serologic Tests
• Gold standard screening test • Initial test in symptomatic patient • The preferred test is IgA TTG • Apply to any age • If IgA deficiency exist perform serologic test
base on IgG e.g. DGP-IgG

Serologic Tests
• In cases of border line result of TTG the preferred additional test is EMA
• Anti gliadin test should not be performed due to its low specificity and sensitivity
• DGP can use as complementary test in conditions when TTG is negative and clinical symptoms exist or in IgA deficiency

Serologic Tests
• In conditions when TTG level is < 3 normal value with minimal clinical symptoms we recommend follow up with normal diet and repetitive TTG testing.
• If TTG increase above 3 normal level biopsy should be performed
Serologic Tests
• Serologic test should be performed in expertise labs with standardization based on ROC curves.
• It should define 10 folds of normal value as upper limit
• The test should use linear kits
Duodenal Biopsy
• Duodenal biopsy should be obtained by EGD • Biopsies should be retrieved from second and
third part of duodenum (4 minimum), and bulb (1 minimum)
• Histological characteristics should include IEL, villous crypt ratio, villous damage.
• Marsh score is the preferred method
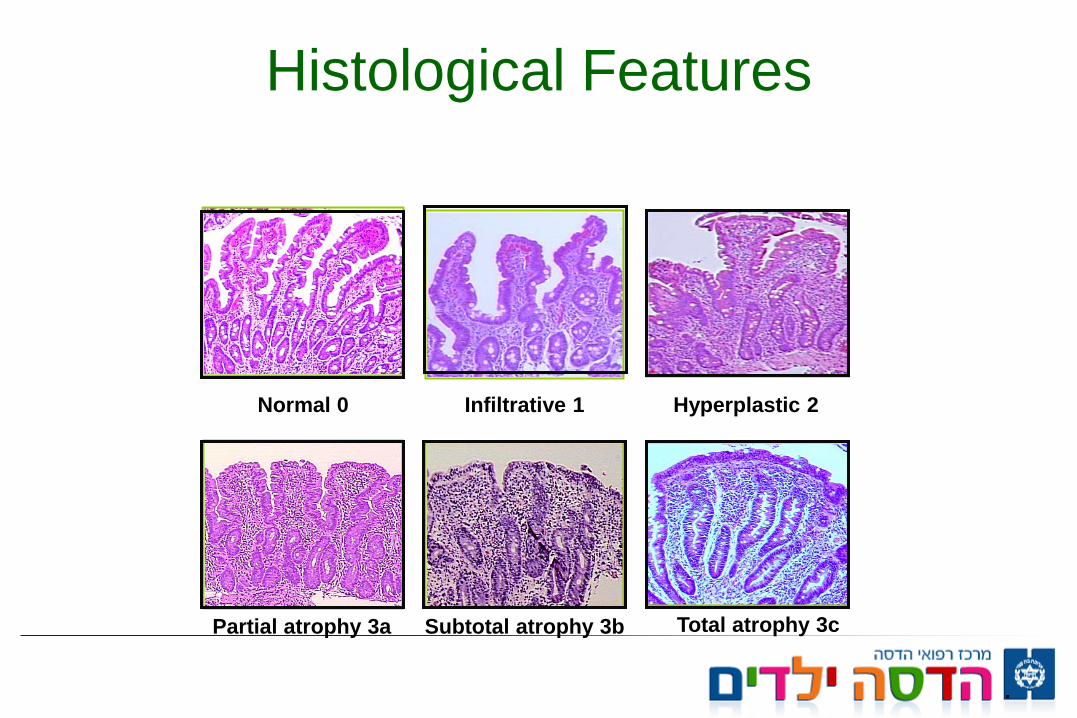
Histological Features
Normal 0 Infiltrative 1 Hyperplastic 2
Partial atrophy 3a Subtotal atrophy 3b Total atrophy 3c
.

Duodenal Biopsy
• Biopsy recommended as diagnostic tool when serology test is positive and associated with any of the clinical indications
• If there is clinical indication with negative serology biopsy should be considered and determined by pediatric gastroenterologist
• Patients who were diagnosed based only on biopsy (negative serology) require further gluten challenge with biopsy
Duodenal Biopsy
• In cases with negative serology, marsh 1 histology other etiologies for mucosal inflammation should be searched

Duodenal Biopsy
• In cases with typical symptoms suggesting CD, and TTG>10 folds TTG should be repeated with a complementary serologic test e.g. EMA
• If all serologic tests are positive pediatric gastroenterologist can avoid biopsy
• HLA is recommended in this scenario • GFD should be started only after completing all
those evaluations

Treatment
• The current only treatment is lifelong GFD • Any food containing <20 ppm gluten should be
avoided • Wheat, barely, and rye should be avoided
including products that may contain trace of those grains

Treatment
• Oat although several studies prove it not being toxic, many products of oat contain toxic grains. We recommend to avoid it at least in the first years till full clinical and serologic recovery achieved
• Later on, oat can be introduced with close monitoring of symptoms as well as TTG level

Follow up • Growth • Adherence to diet • Adequate nutritional support • Check for iron and other nutritional deficiency • Serologic test • Liver, thyroid tests • Known complications • Yearly follow up • Initial follow up more frequent and close
