new irradiation techniques in non metastatic breast …rorc.tums.ac.ir/portals/11/1395/5-95/dr....
TRANSCRIPT
New Irradiation techniques in
non metastatic breast cancer
Dr.zhaleh karimimoghaddam
Assistant professor of Radiation Oncology
Of Zanjan University of Medical Science
Introduction
1. APBI
2. Hypo fractionation
Why PBI?
1. decreases breast recurrence → longer survival
NSABP trial (B-06)from large well-controlled RCT after 20 yr f/u reported that :the same result in OS & LC in MRM vs. BCS+WBI but
-more cancer related death in MRM group
-more vascular death in BCS+WBI group
After BCS and whole-breast RT, most of
ipsilateral breast tumor recurrences
(IBTR) occur in the primary tumor
cavity and can be classified into two main
categories; true recurrences and
elsewhere recurrences.

Prospective Randomised
Trials of Lumpectomy+/- XRT
Trial % off patients recurring
L alone L+XRT
NSABP B-06 36 12
Milan 24 6
Scottish 25 6
Overall,, whole breast RT decreases breast recurrence by a factor off 3 or 4..
Recurrences are predominantly at the site off the original cancer
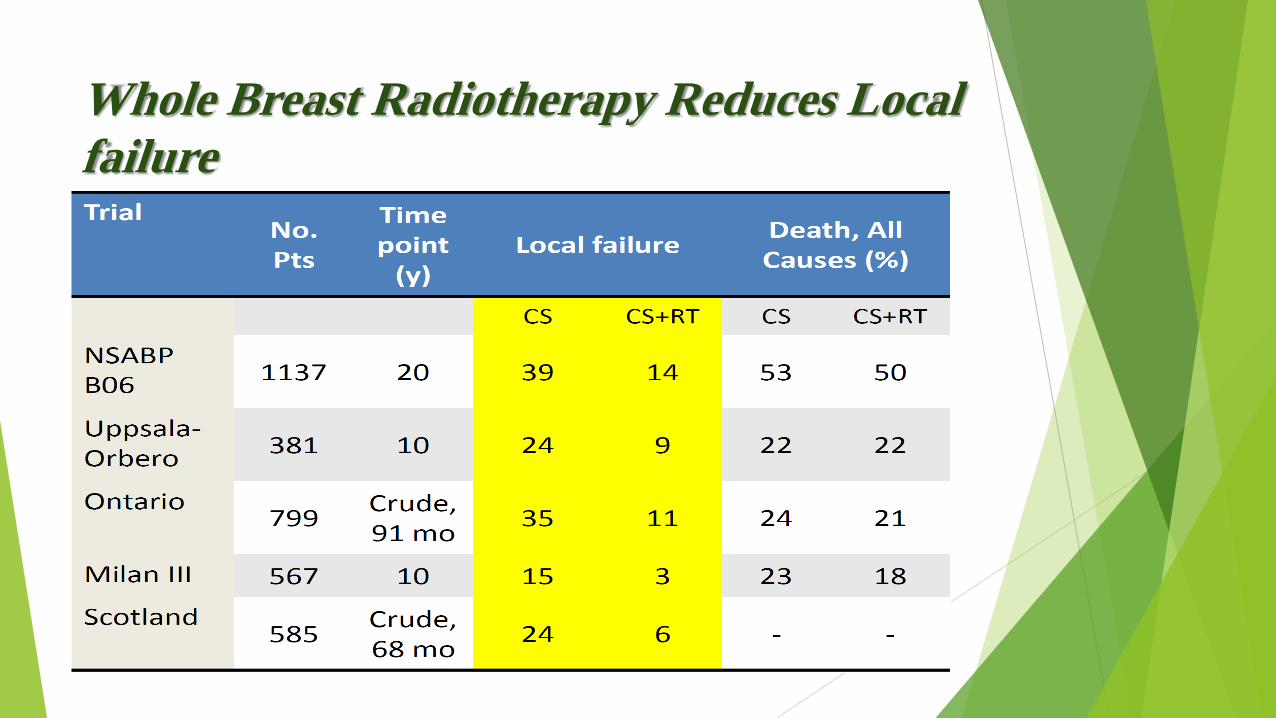
Whole Breast Radiotherapy Reduces Local
failure
Why PBI?
2)minimize PTV→ reduction in treatment
toxicity NSABP B-06 → 1,039 patients → were treated with lumpectomy
it was reported through follow-up that 75% of local recurrences occurred at or
near the lumpectomy site and that WBRT was irrelevant to the findings .
Freedman et al.
reported on IBTR following BCS and WBI in 1,990 for women with stages 0-
II
breast cancer with a median follow-up period of 6.7 years.
They classified recurrences according to their location.
The 15-year actuarial rate of a true/marginal recurrence was 7% compared
with an elsewhere recurrence rate of 6%
Recurrence Pattern 91% of local recurrence after breast conserving therapy
occurs near the site of the primary tumor, even when
radiotherapy is not given.
Thus, the occult tumors in other quadrants may remain
dormant, never becoming clinically relevant; and
radiotherapy to the site of the original tumor may be
adequate
Fisher et al Samsung Oncology 1992;8:161.
Veronesi et al N Engl J Med 1993;328:1587

Why PBI?
3)shorter treatment time
Accelerated PBI (APBI)with shorter duration of
RT usually one week therefore:
-fewer transport
-lower cost
-quickly start of systemic therapy

Why PBI?
4)better cosmetic results
lesser irradiated volume and
fewer telangectasis and fibrosis
Accelerated Partial Breast Irradiation
Rationale Most recurrences occur within 2cm of lumpectomy from prospective and RND trials (>2/3 1st failure)
Decreased Treatment time and QOL
Potential reduction in treatment toxicity
Multiple different techniques with short follow up

APBI Established methods
External beam (3.85gy BID x 5 days)
Most common in USA
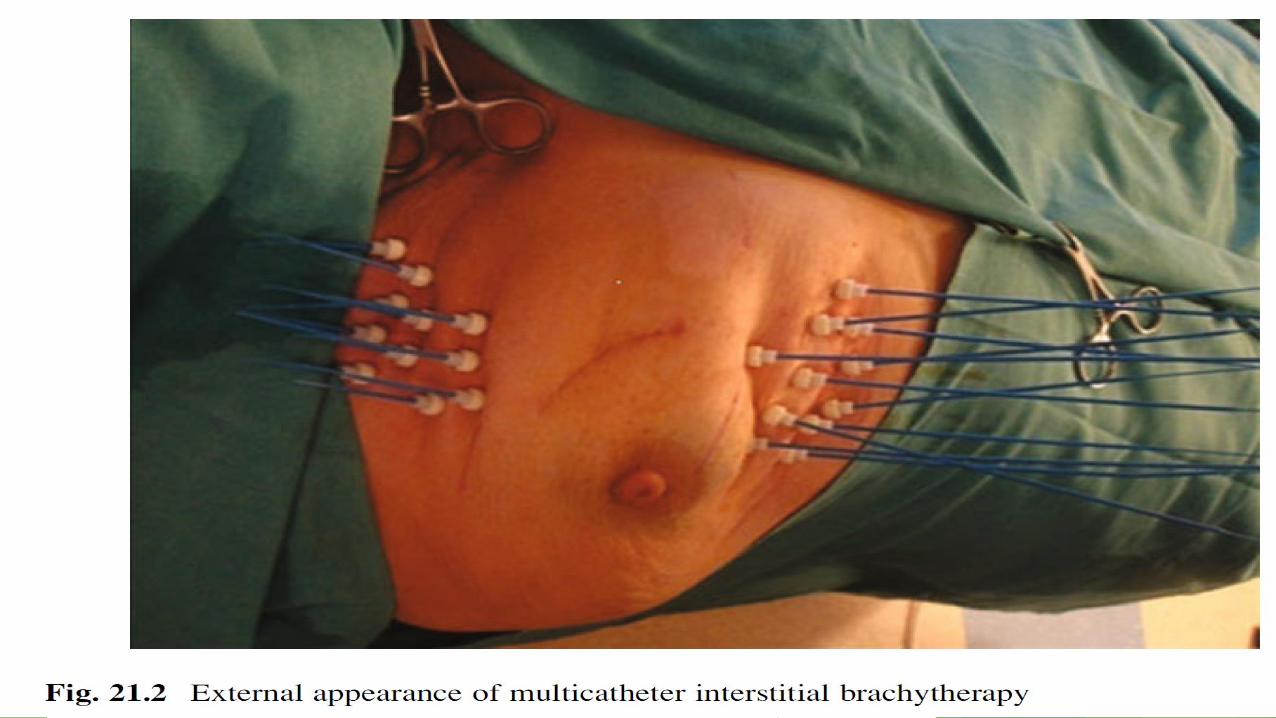
Interstitial Brachytherapy: LDR, HDR
Multi-catheter
Intracavitary:
Intraoperative Electrons: ELIOT
Intraoperative Orthovoltage Photons: TARGIT-A
Mammosite

NSABP B39 / RTOG 0413
>4300pts accrued
Tis-T2,N1-3
<3cm
WBRT 50-50.4Gy/25-28f +10-16Gy
Boost
38.5Gy/10f 3DCRT or 34Gy/10fMammosite
or multilumen BT
Stratified
ER status
DCIS/invasive/n1
Menopausal
Chemotherapy
• Primary Endpoint: IBTR
•Secondary:
OS, recurrence free survival
•Awaiting initial results 15 sept 2015 now closed to accrual.

External beam APBI:
Initial cosmetic results from RAPID
RAPID (Olivotto et al) WBRT
vs. APBI No IBTR results yet
Worse patient reported cosmesis in
ABPI from physician, nurse, and
patient 36mo median FU
J Clin Oncol. 2013 Nov
10;31(32):4038-45. doi:
10.1200/JCO.2013.50.5511. Epub
2013 Jul 8.
a multicenter randomized trial
2135 women
>40yr
DCIS or Invasive
<3cm
Node Neg
WBRT 50gy/25 or 42.5/16 +/-
Boost
3DCAPBI
38.5gy/10BID
RAPID
Results : Between 2006 and 2011, 2,135 women were
randomly assigned to 3D-CRT APBI or WBI. Median
follow-up was 36 months. Adverse cosmetic at 3 years
was increased among those treated with APBI
compared with WBI as assessed by trained nurses (29%
v 17%; P < .001), by patients (26% v 18%; P = .0022),
and by physicians reviewing digital photographs (35% v
17%; P < .001). Grade 3 toxicities were rare in both
treatment arms (1.4% v 0%), but grade 1 and 2
toxicities were increased among those who received
APBI compared with WBI (P < .001).
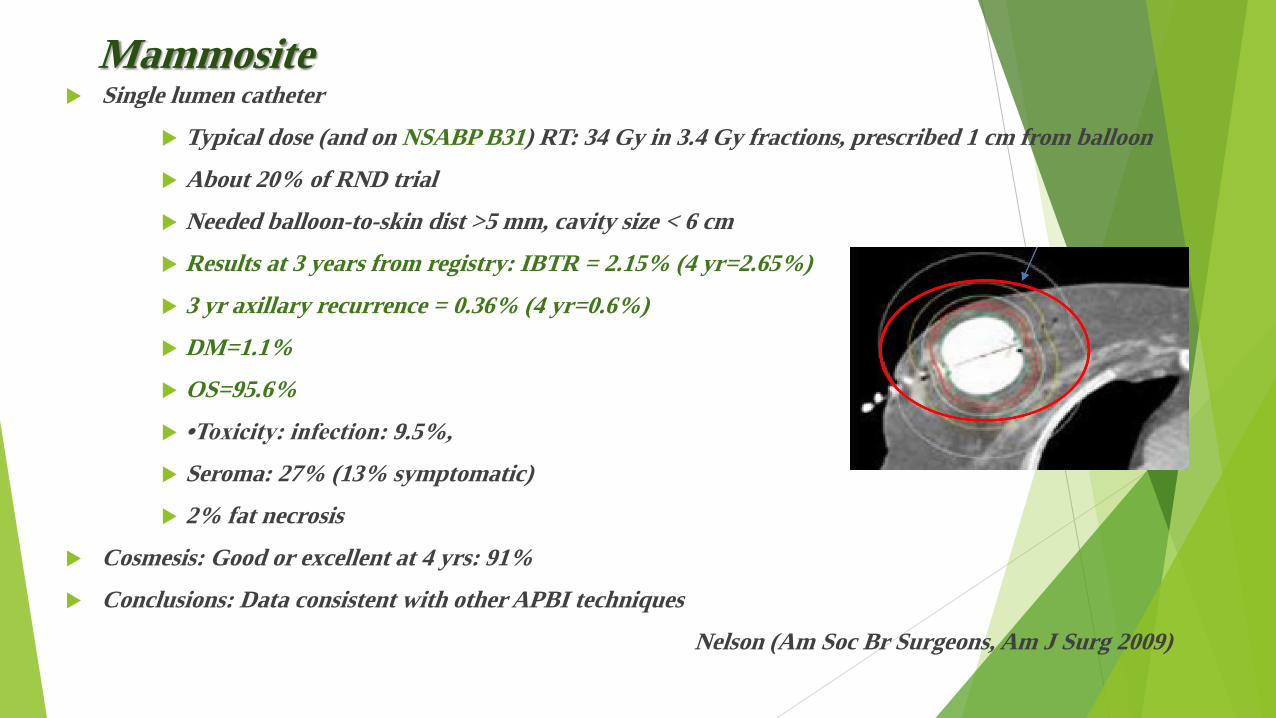
Mammosite Single lumen catheter
Typical dose (and on NSABP B31) RT: 34 Gy in 3.4 Gy fractions, prescribed 1 cm from balloon
About 20% of RND trial
Needed balloon-to-skin dist >5 mm, cavity size < 6 cm
Results at 3 years from registry: IBTR = 2.15% (4 yr=2.65%)
3 yr axillary recurrence = 0.36% (4 yr=0.6%)
DM=1.1%
OS=95.6%
•Toxicity: infection: 9.5%,
Seroma: 27% (13% symptomatic)
2% fat necrosis
Cosmesis: Good or excellent at 4 yrs: 91%
Conclusions: Data consistent with other APBI techniques
Nelson (Am Soc Br Surgeons, Am J Surg 2009)


Interstitial APBI Matched Pair: Intersitial PBI vs. WBI
Methods: 199 pts with early-stage breast CA (Stage I/II)
RT: LDR 50 Gy at 0.52 Gy/hr (60%) or HDR 32 Gy in 4 Gy or 34 Gy in 3.4 Gy
Cosmesis: Good to excellent in 98.3% of pts
Antonucci, Beaumont, IJROBP 2009
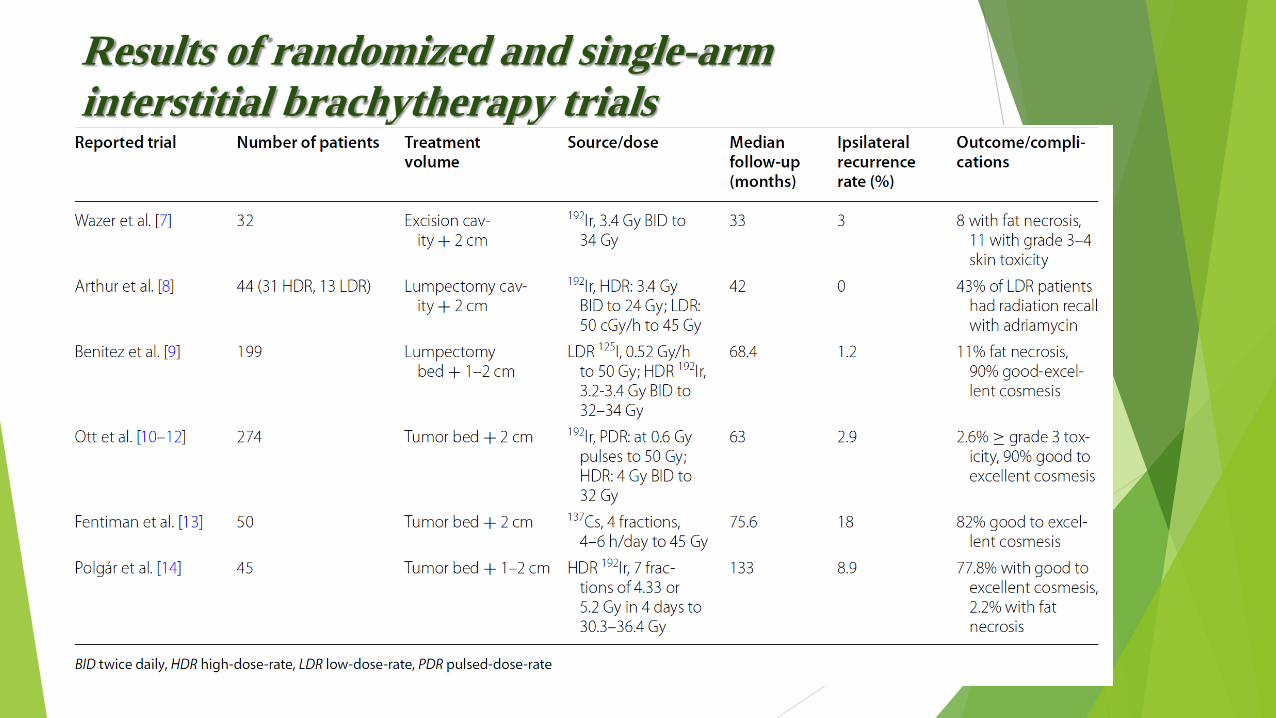
Results of randomized and single-arm
interstitial brachytherapy trials

Intraoperative APBI


Targeted intraoperative radiotherapy versus
whole breast radiotherapy for breast cancer
(TARGIT-A trial): an international,
prospective, randomized, non-inferiority phase
III trial
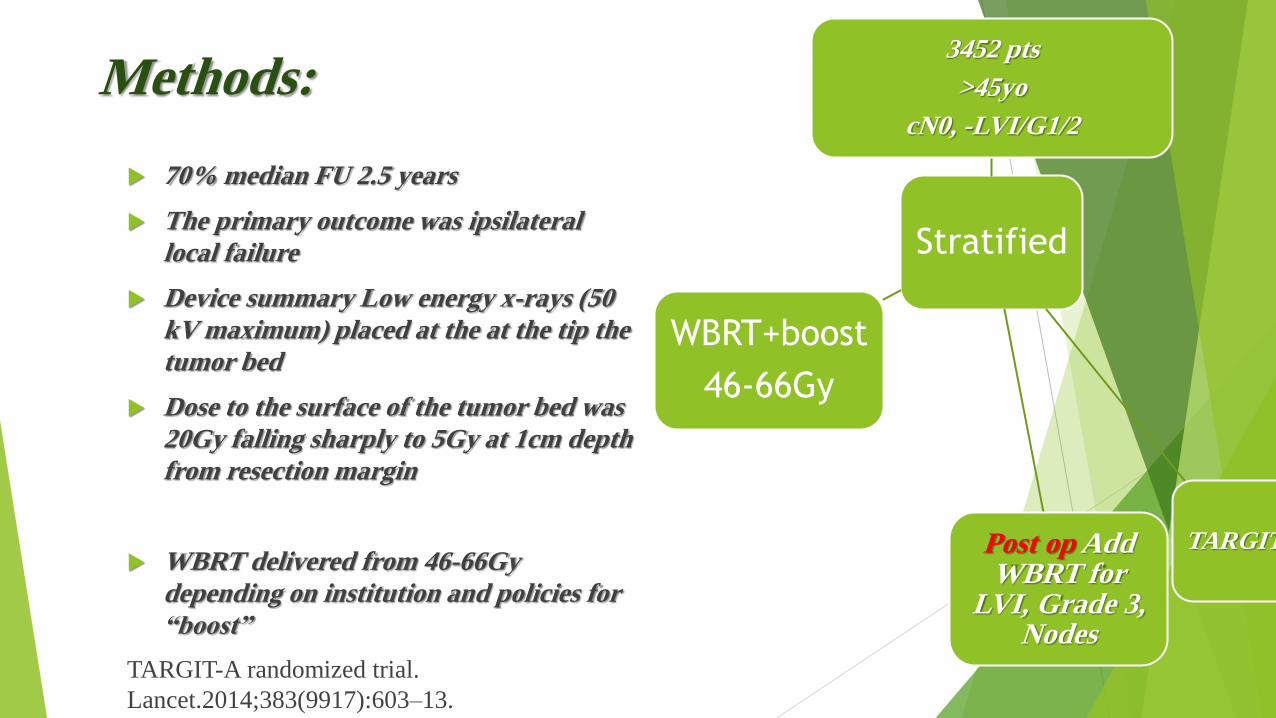
Methods:
70% median FU 2.5 years
The primary outcome was ipsilateral
local failure
Device summary Low energy x-rays (50
kV maximum) placed at the at the tip the
tumor bed
Dose to the surface of the tumor bed was
20Gy falling sharply to 5Gy at 1cm depth
from resection margin
WBRT delivered from 46-66Gy
depending on institution and policies for
“boost”
TARGIT-A randomized trial.
Lancet.2014;383(9917):603–13.
Stratified
3452 pts
>45yo
cN0, -LVI/G1/2
TARGIT Post op Add WBRT for
LVI, Grade 3, Nodes
WBRT+boost
46-66Gy


Targit A: 2014
Intraoperative radiotherapy versus
external radiotherapy for early breast
cancer (ELIOT): a randomized
controlled equivalence trial(2013) (ELIOT): a randomized controlled equivalence trial. Lancet
Oncology. 2013;14(13):1269–77.

Key differences from TARGIT
Done in Italy only
IORT 21Gy with Electrons vs
50Gy+10Gy boost
Resultes 5y IBTR WBRT: 0.4%
5y IBTR Intraop: 4.4%
OS same
Intra-op Conclusions
Randomized data demonstrate safety and efficacy
Allows post-surgery RT for high risk groups without toxicity
Statistically Significant increase LRR vs WBRT
Long term data still lacking
Continue to follow patients….
ESMO Clinical Practice
Guidelines 2015
in the ELIOT (single dose of electrons) and
TARGIT (single intra-operative dose 50 kV X-rays) randomized trials, the ipsilateral breast recurrence
rate was significantly
higher in the APBI groups, compared with the WBRT trial
Results 5y IBTR WBRT: 0.4%
5y IBTR Intraop: 4.4%

ASTRO taskforce for APBI
Suitable group
age≥60
N 0
T1 primary cancers
Positive ER status
negative lymph vascular space invasion (LVSI)
widely negative margins (>2mm)
no multicentricity

ASTRO taskforce for APBI Cautionary group
age <60
T2 primary disease
pure DCIS <3 cm,
close margins (<2 mm),
focal LVSI
multifocal or multicentric disease
invasive lobular carcinoma
or ER negativity
ASTRO taskforce for APBI
Unsuitable group
tumor size >3 cm
positive margins
any positive lymph nodes or no axillary surgery
extensive LVSI
multicentricity
DCIS >3cm
or the presence of a BRCA1 or 2 mutation
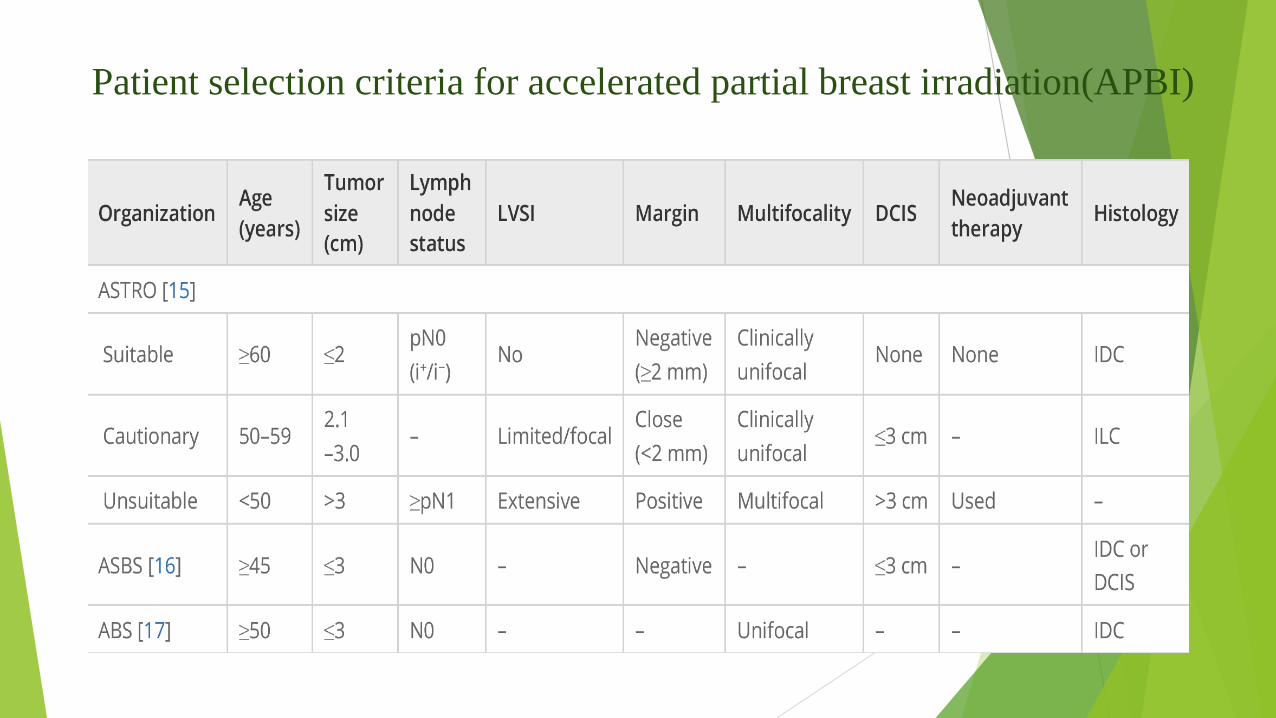
Patient selection criteria for accelerated partial breast irradiation(APBI)

Conclusion
Currently, the standard of care after BCS is still WBI, not APBI. However,
the role
of APBI will continue to be defined by the mature results of ongoing randomized
trials from large cooperative groups in the next 5–10 years.

Hypo fractionation


ASTRO criteria for HF :
Age ≥ 50 years at the time of diagnosis; had a first and only diagnosis of breast cancer;
pT1-T2N0 patients based on the American Joint Committee on Cancer TNM staging classification were treated with breast-conserving surgery; and did not receive chemotherapy.

four large multicenter randomized
clinical trials were conducted;
one in Canada and three in England: the Ontario
Clinical Oncology Group (OCOG) Trial. the Royal Marsden
Hospital/
Gloucester Oncology Centre (RMH/GOC) Trial, the UK
Standardization
of Breast Radiotherapy Trial A (START A), and the UK
Standardization of
Breast Radiotherapy Trial B (START B).

Inclusion criteria, dose and fraction properties, local control and survival rates
in
randomized large hypo fractionation trials Study Inclusion criteria Total dose
(Gy)/fraction/
time
Local recurrence (%)
5 y/10 y
Survival (%)
5 y/10 y
OCOG
n =1,234
BCS
T1-T2, N0, M0
<25 cm width
Uninvolved inked
margin
50 Gy/25/35 d
42.5 Gy/16/22 d
3.2%/6.7%
2.8%/6.2%
91.7%/84.4%
92.3%/84.6%
RMH/GOC
n = 1,410
BCS
T1-3, N0-1, M0
Complete
Macroscopic
resection
50 Gy/25/5 wk
42.9/13/5 wk
39 Gy/13/5 wk
7.9%/12.1%
7.1%/9.6%
9.1%/14.8%
START A
n = 2,236
BCS or mastectomy
T1-3,N0-1, M0
Clear tumor
margins >1 mm
50 Gy/25/5 wk
41.6 Gy/13/5 wk
39 Gy/13/5 wk
3.6%
3.5%
5.2%
88.8%
88.1%
88.7%
START B
n = 2,215
BCS or mastectomy
T1-3, N0-1
Clear tumor
margins >1 mm
50 Gy/25/5 wk
40 Gy/15/3 wk
3.3%
2.2%
87.5%
90.4%

Skin toxicity and cosmetic outcome rates in large
randomized hypo fractionation trials Study n Total dose
(Gy)/fraction/time
Toxicities skin (%)
5y/10y
Excellent/good
cosmesis or no
change (%)
Adverse cosmetic
results (%) 5y/10y
OCOG
n = 1,234
50 Gy/25/35 d
42.5 Gy/16/22 d
17.7%/29.5%
13.9%/33.2%
79.2%/71.3%
77.9%/69.8%
20.8%/28.7%
22.1%/30.2%
RMH/GOC
n = 1,410
50 Gy/25/5 wk
42.9/13/5 wk
39 Gy/13/5 wk
12.0%/18.1%
13.0%/18.0%
5.6%/12.0%
60.4%/46.6%
54.3%/42.0%
69.7%/43.9%
60.4%/46.6%
54.3%/42.0%
69.7%/43.9%
START A
n = 2,236
50 Gy/25/5 wk
41.6 Gy/13/5 wk
39 Gy/13/5 wk
31.1%
25.0%
2.6%
59.0%
58.1%
65.9%
42.9%
43.6%
32.1%
START B
n = 2,215
50 Gy/25/5 wk
40 Gy/15/3 wk
42.3%
38.2%
58.8%
64.5%
42.2%
36.5%
According to the data obtained in all
these randomized trials, standard and
HF treatment models revealed similar
results with regard to local recurrence,
survival,
and adverse cosmetic results.

Systematic review and meta-analysis
comparing hypo fractionated
with conventional fraction radiotherapy in
treatment of early breast cancer (23 studies)
Surgical Oncology(8 June 2015),china
Meta-analysis demonstrated
hypo fractionation
radiotherapy (HFRT) was associated with
decreased grade 2/3 acute skin reactions
compared with
conventional fraction RT (CFRT), either 2.5-
3.0 Gy per fraction or 5.0-6.5 Gy per fraction.

HFRT with 2.5-3.0 Gy per fraction significantly
decreased moderate/marked photographic changes
in breast appearance
compared with CFRT while HFRT with more than
3.0 Gy
per fraction significantly increased
moderate/marked photographic changes.

HFRT cost one-third lower than CFRT.
local regional recurrence,
distant metastasis, overall survival, disease free
survival, excellent/good cosmetic comes,
symptomatic radiation pneumonitis, ischemic
heart disease and symptomatic rib fracture,
there was no significant
difference between two arms.
Where is boost location in HF?
tumor bed boost
14 Gy/7 fractions in RMH/GOC trials
10 Gy/5 fractions in the START A and B trials
no patients were given boost irradiation in the
Canadian trials
ASTRO guideline stated that “the task force
agreed that the use of HF-WBI alone (without
a boost) is not appropriate when a tumor bed
boost is thought to be indicated

tumor bed boost (NCCN 2016)
Recommended in patients with higher risk
characteristics (such as age<50,high grade
disease, or patients with focally positive
margins) in order to reduce local relapse.
typical boost doses are 10 to 16 Gy in 4 to 8
fraction.
RTOG 1005 (2014)
A Phase III Trial Of Accelerated Whole Breast
Irradiation With Hypo fractionation Plus
Concurrent Boost Versus Standard Whole
Breast Irradiation Plus Sequential Boost For
Early-Stage Breast Cancer

To determine whether an accelerated course of
hypo fractionated WBI including a
concomitant boost to the tumor bed in 15
fractions following lumpectomy will prove to be
non-inferior in local control to a regimen of
standard WBI with a sequential boost following
lumpectomy for early-stage breast cancer
patients.
“Don’t initiate whole breast radiotherapy
as a part of breast conservation
therapy in women age ≥50 with
early stage invasive breast cancer
without considering shorter treatment schedules.”
ASTRO Guidelines
Conclusions:
Based on available evidence, HFRT with 2.5-3.0 Gy
per fraction should be the better choice for treatment of
early breast cancer patients.
THE END