new drugs for asthma
TRANSCRIPT
NEW DRUGS
FOR ASTHMA*Grerk Sutamtewagul, MD
PGY-3 Internal Medicine ResidentTexas Tech University Health Sciences Center
November 15, 2013
* Semin Respir Crit Care Med 2012;33:685-694
The Need for New Asthma Therapy• Substantial patients burden
• 300 million patients worldwide• 7.8% of the US population†
• More than half of the patients appear to be poorly controlled.• 80% due to poor compliance• Some due to fear of side effects
† MMWR Jan 14, 2011 Vol 60 supplement
The Need for New Asthma Therapy• Inhaled corticosteroid (ICS) does not modify the course of
the disease even started early in childhood‡.• 2-year treatment period followed by 1-year observation in
preschool children• No difference at the end of 1-year observation in terms of episode-
free days, time to first systemic steroid, time to first supplementary asthma treatment
‡ Guilbert, T. et al. N Engl J Med 2006;354:1985-1997
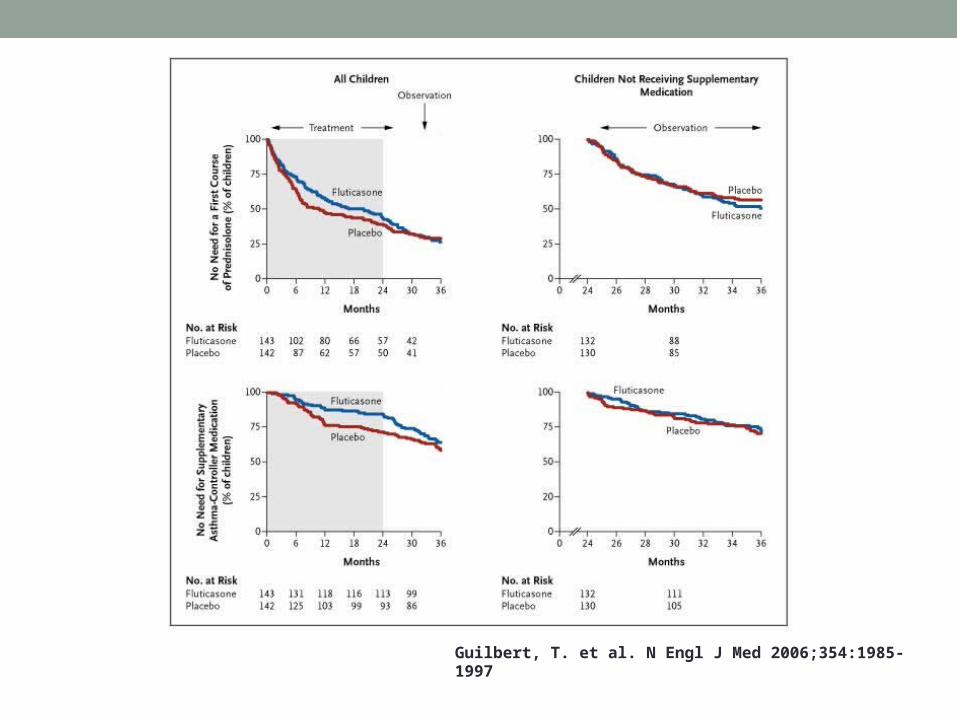
Guilbert, T. et al. N Engl J Med 2006;354:1985-1997
The Need for New Asthma Therapy• 5-10% have uncontrolled asthma despite effective inhaled
therapy.• What we need
• Drugs with similar mechanism but less side effects• New classes of drug to treat asthma• New classes of drug that modify the course of the disease
The Need for New Asthma Therapy• Improvement in understanding basic pathophysiology of
asthma in molecular level• IgE in pathogenesis of asthma• Cytokines and cell signalling• Immunomodulating pathway
• Recognition of different phenotypes of asthma• Allergic asthma with elevated IgE – Omalizumab

Allergic mechanism in Asthma
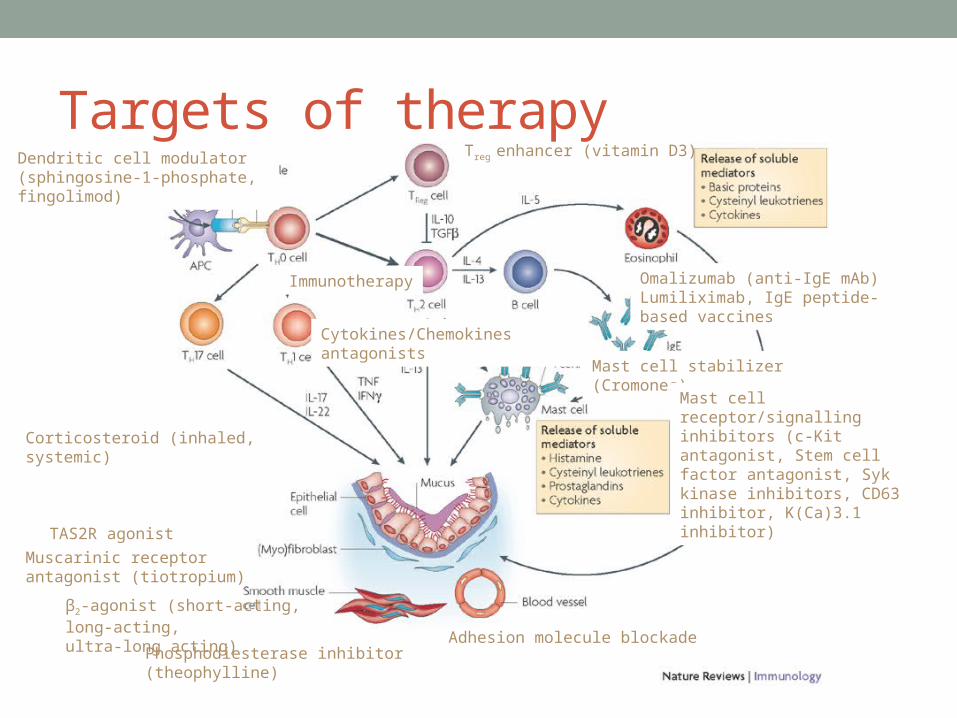
Targets of therapy
β2-agonist (short-acting, long-acting,ultra-long acting)
Corticosteroid (inhaled, systemic)
Omalizumab (anti-IgE mAb)Lumiliximab, IgE peptide-based vaccines
Leukotrienes modifiers e.g. montelukast
Mast cell stabilizer (Cromones)
Phosphodiesterase inhibitor (theophylline)
Mast cell receptor/signalling inhibitors (c-Kit antagonist, Stem cell factor antagonist, Syk kinase inhibitors, CD63 inhibitor, K(Ca)3.1 inhibitor)
Adhesion molecule blockade
Immunotherapy
Treg enhancer (vitamin D3)Dendritic cell modulator (sphingosine-1-phosphate, fingolimod)
Cytokines/Chemokines antagonists
Muscarinic receptor antagonist (tiotropium)
TAS2R agonist
NEW BRONCHODILATORSUltra-long-acting beta-2 agonists
Muscarinic receptor agonist
Bitter taste receptor agonist
New Bronchodilators• Bronchodilators use
• Relieving bronchoconstriction (short-acting)• Preventing bronchoconstriction (long-acting beta-agonist or LABA:
formoterol, salmeterol – lasting 12 hrs)
• Ultra-LABAs in development (lasting > 24 hrs) for once-daily use
• Long-acting muscarinic receptor agonist (LAMA), e.g. tiotropium, can be a useful add-on for severe asthma‡.
• Bitter taste receptor (TAS2R) agonist can cause bronchodilation†.
‡ N Engl J Med. 2012 Sep 27;367(13):1198-207. Epub 2012 Sep 2.† Am J Physiol Lung Cell Mol Physiol. 2012 Dec 1;303(11):L953-5

Meta-analysis comparing Tiotropium and Placebo - effect on PEF
Respir Care. 2013 Oct 29
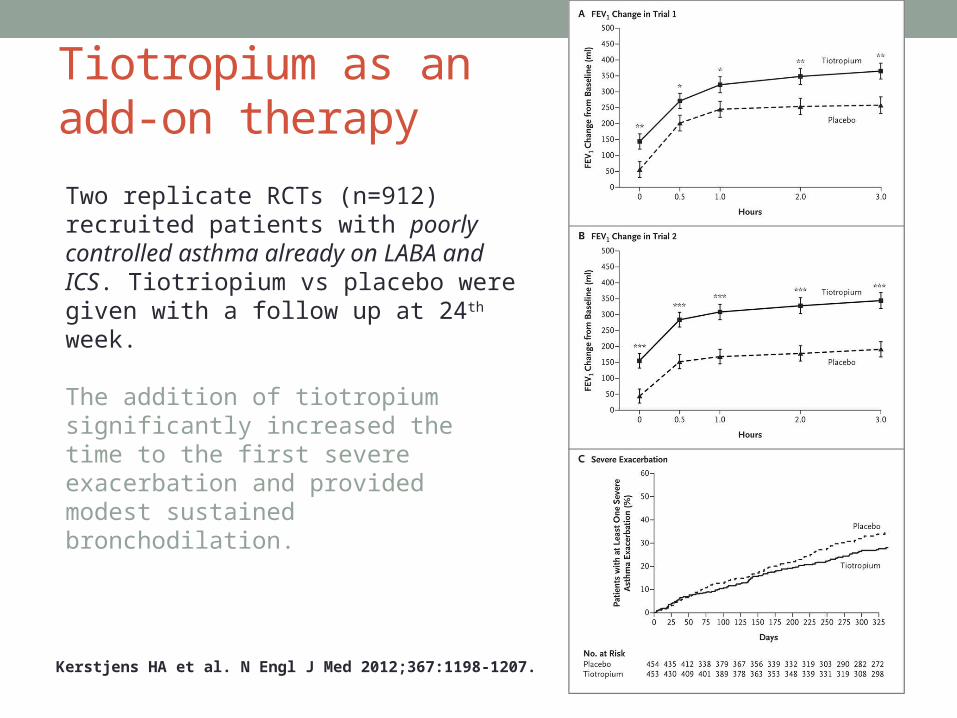
Tiotropium as an add-on therapy
Kerstjens HA et al. N Engl J Med 2012;367:1198-1207.
Two replicate RCTs (n=912) recruited patients with poorly controlled asthma already on LABA and ICS. Tiotriopium vs placebo were given with a follow up at 24th week.
The addition of tiotropium significantly increased the time to the first severe exacerbation and provided modest sustained bronchodilation.
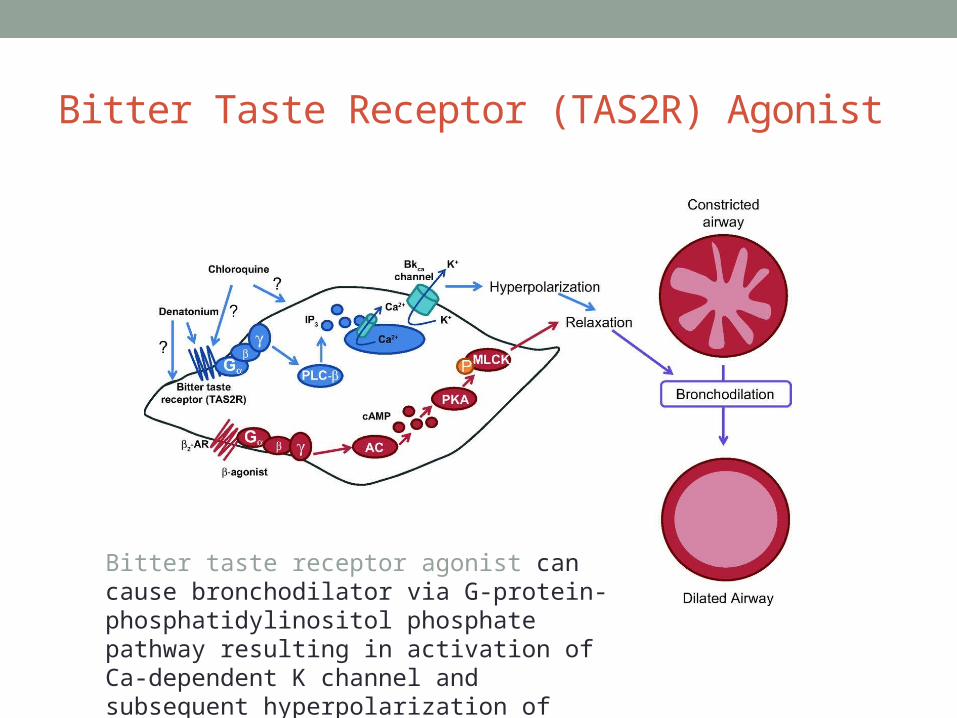
Bitter Taste Receptor (TAS2R) Agonist
Bitter taste receptor agonist can cause bronchodilator via G-protein-phosphatidylinositol phosphate pathway resulting in activation of Ca-dependent K channel and subsequent hyperpolarization of smooth muscle cell.
NEW CORTICOSTEROIDSDesigning new corticosteroids to decrease side effects
Dissociated steroids
Nonsteroidal selective glucocorticoid receptor agonists
New Corticosteroids• ICSs are the most effective anti-inflammatory therapy for
asthma.• Currently available ICSs can be absorbed from the lung,
leading to potential systemic side effects.• New corticosteroids’ preferred properties
• Reduced absorption from the lungs• Inactivated in the circulation• Dissociated steroid (trans-activation vs cis-activation vs trans-
repression)• Nonsteroidal selective glucocorticoid receptor agonist (SEGRA)
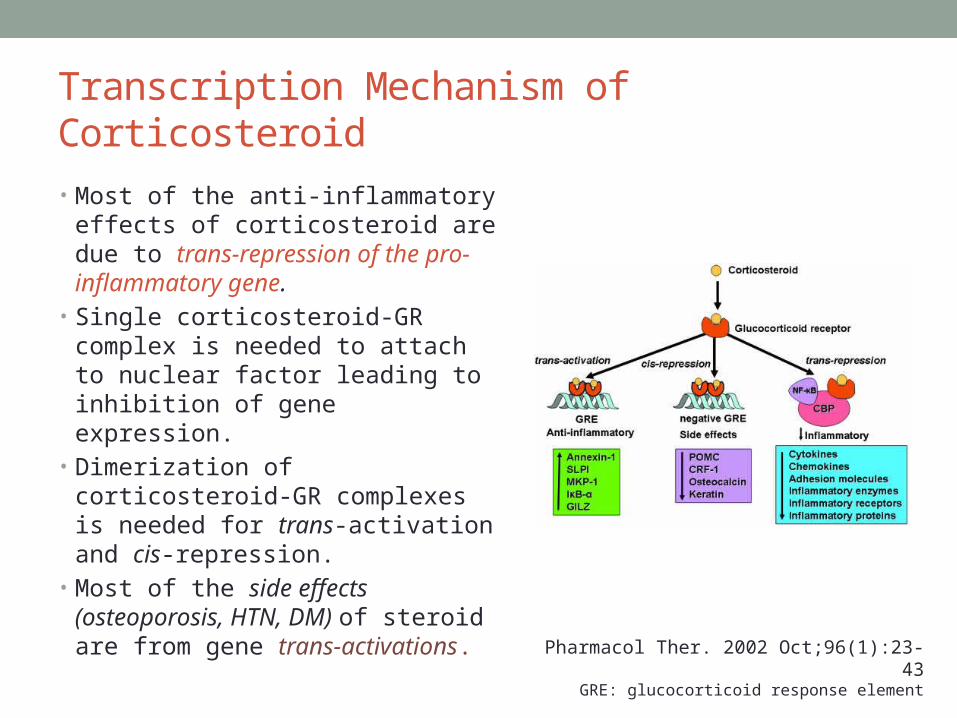
Transcription Mechanism of Corticosteroid
• Most of the anti-inflammatory effects of corticosteroid are due to trans-repression of the pro-inflammatory gene.
• Single corticosteroid-GR complex is needed to attach to nuclear factor leading to inhibition of gene expression.
• Dimerization of corticosteroid-GR complexes is needed for trans-activation and cis-repression.
• Most of the side effects (osteoporosis, HTN, DM) of steroid are from gene trans-activations.
Pharmacol Ther. 2002 Oct;96(1):23-43GRE: glucocorticoid response element
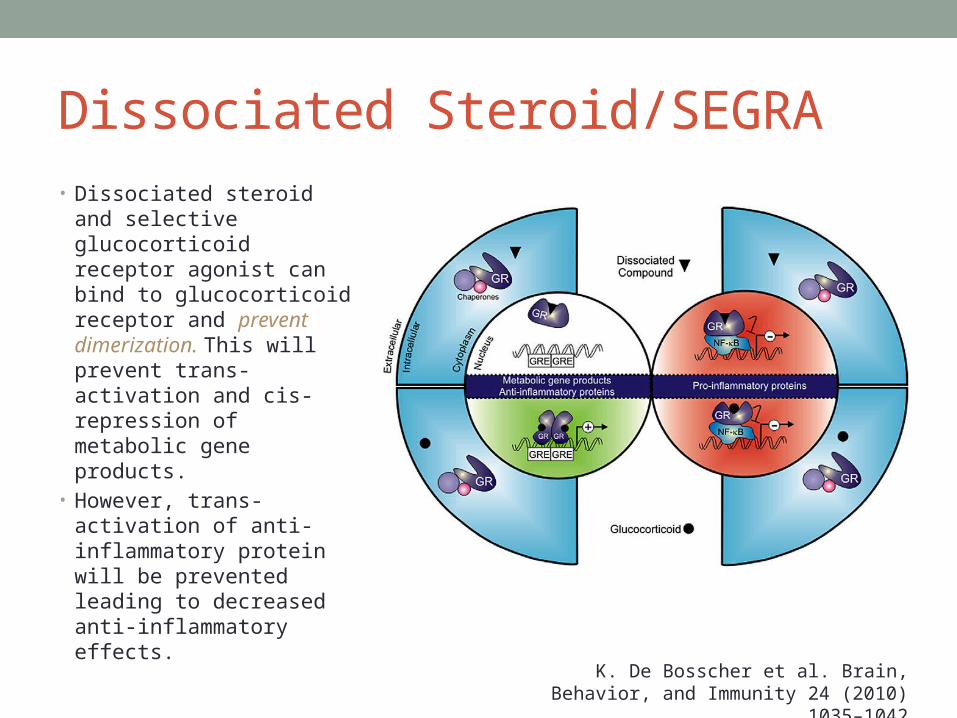
Dissociated Steroid/SEGRA• Dissociated steroid and
selective glucocorticoid receptor agonist can bind to glucocorticoid receptor and prevent dimerization. This will prevent trans-activation and cis-repression of metabolic gene products.
• However, trans-activation of anti-inflammatory protein will be prevented leading to decreased anti-inflammatory effects.
K. De Bosscher et al. Brain, Behavior, and Immunity 24 (2010) 1035–1042
TARGETING ALLERGIC INFLAMMATIONLipid mediators and cytokines modulation
Targeting Lipid Mediators• Problems: More than 100 mediators are involved in the
complex inflammatory process in asthma.• The only mediator antagonists available are cysteinyl-
Leukotriene CysLT1 receptor antagonists e.g. montelukast.
• 5’-lipooxygenase and 5’-lipooxygenase-activating protein inhibitors are in development.
Targeting Lipid Mediators
• Prostaglandin D2 is released from mast cells, Th2 cells and dendritic cells.• DP2 receptor (CRTh2) chemotaxis of Th2 and eosinophil
• DP1 receptor vasodilation, enhancing Th2 polarization
• Thromboxane prostanoid receptor airway smooth muscle constriction
• CRTh2 inhibitors: AMG-853 OC000459 and MK-2746• DP1/DP2 inhibitors: in development
• PGD2 synthesis inhibitors: in development
Cytokine Blockade
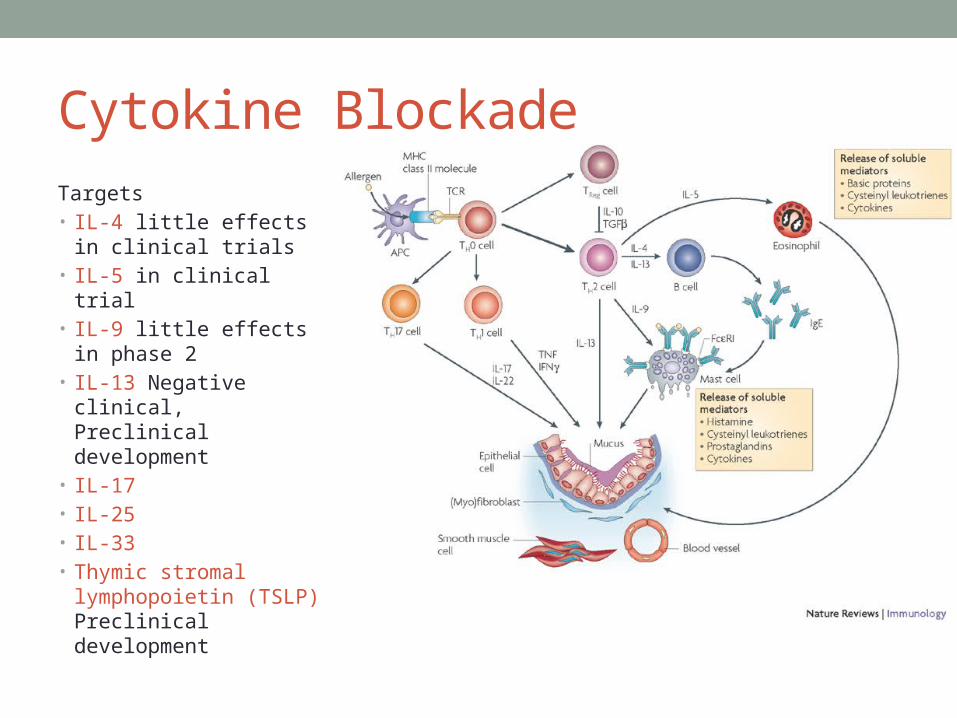
Targets• IL-4 little effects in
clinical trials• IL-5 in clinical trial• IL-9 little effects in
phase 2• IL-13 Negative clinical,
Preclinical development• IL-17• IL-25• IL-33• Thymic stromal
lymphopoietin (TSLP) Preclinical development
Interleukin-4 and Interleukin-13• Pitrakinra
• Mutated IL-4 (recombinant human IL-4 mutein)• Blocking IL-4Rα, the common receptor for IL-4 and IL-13• Reduces the late response to inhaled allergen in mild asthmatics§
• Clinical studies in severe asthma have been disappointing.• Patients with high eosinophil count and rs8832, rs1029489 GG
genotype (compared to AG or GA) have a decrease in asthma exacerbation on pitrakinra.¶
§ Lancet. 2007 Oct 20;370(9596):1422-31¶ J Allergy Clin Immunol. 2012 Aug;130(2):516-22.e4.
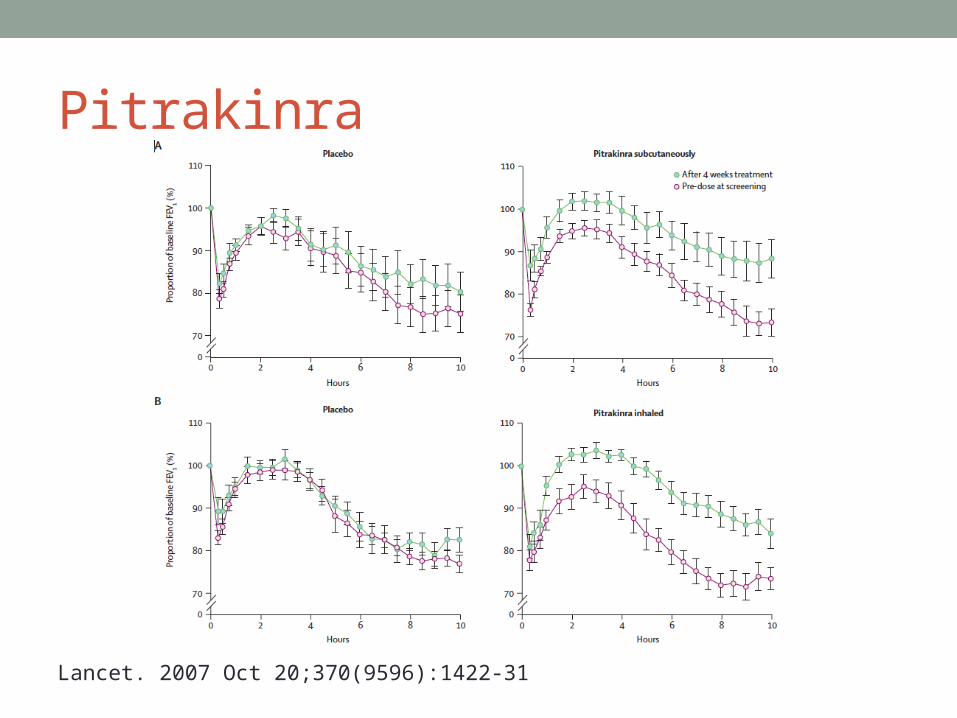
Pitrakinra
Lancet. 2007 Oct 20;370(9596):1422-31
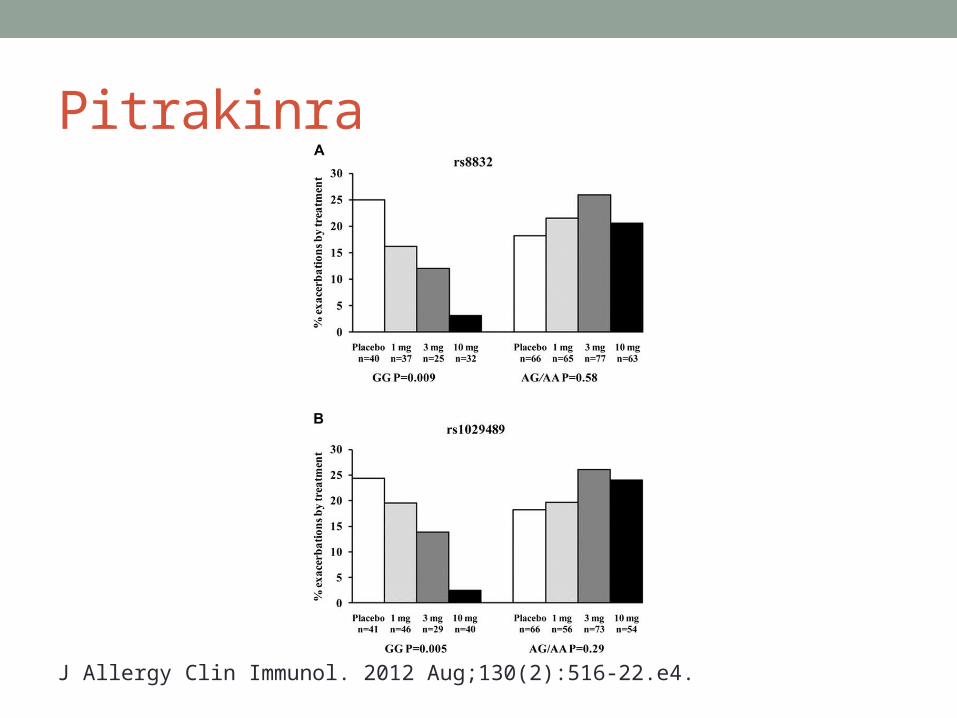
Pitrakinra
J Allergy Clin Immunol. 2012 Aug;130(2):516-22.e4.
Interleukin-5• IL-5 is important for eosinophilic inflammation.• Mepolizumab is a blocking antibody to IL-5.
• Depletes eosinophil from the circulation and the sputum of asthmatics
• No effect on response to inhaled allergen, airway hyperresponsiveness, lung function or exacerbation frequency
• Reduces exacerbation in patients with persistent sputum eosinophilia despite high dose ICS but no improvement in lung function.§
• IL-5Rα blocker is currently studied.
§ PLoS One. 2013;8(3):e59872
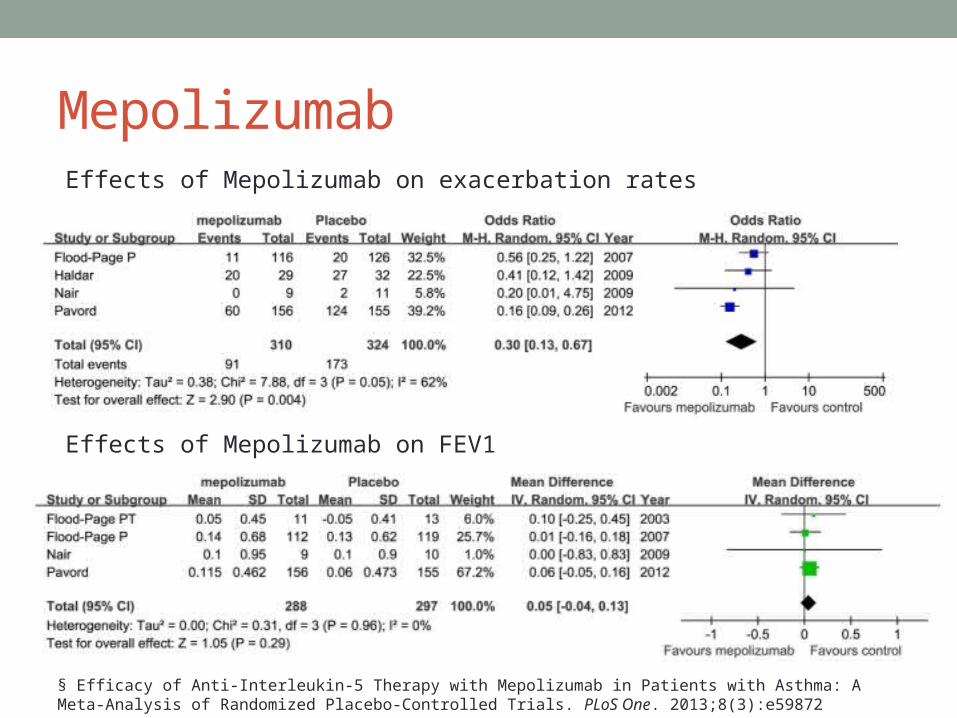
MepolizumabEffects of Mepolizumab on exacerbation rates
Effects of Mepolizumab on FEV1
§ Efficacy of Anti-Interleukin-5 Therapy with Mepolizumab in Patients with Asthma: A Meta-Analysis of Randomized Placebo-Controlled Trials. PLoS One. 2013;8(3):e59872
Other Interleukins• Anti-TNF-α
• No beneficial effect on lung function, symptoms, or exacerbations• Increased reports of pneumonia and cancer
• IL-17• May be a target in severe asthma with neutrophillic inflammation
• IL-10• Broad spectrum of antiinflammatory effects• Efficacy has not been demonstrated in asthma.
• IL-12 and Interferons• Not effective and results in unacceptable side effects

NOVEL ANTIINFLAMMATORY TREATMENTSPhosphodiesterase inhibitors
Kinase inhibitors
Adhesion molecule blockade
PPARγ Agonists
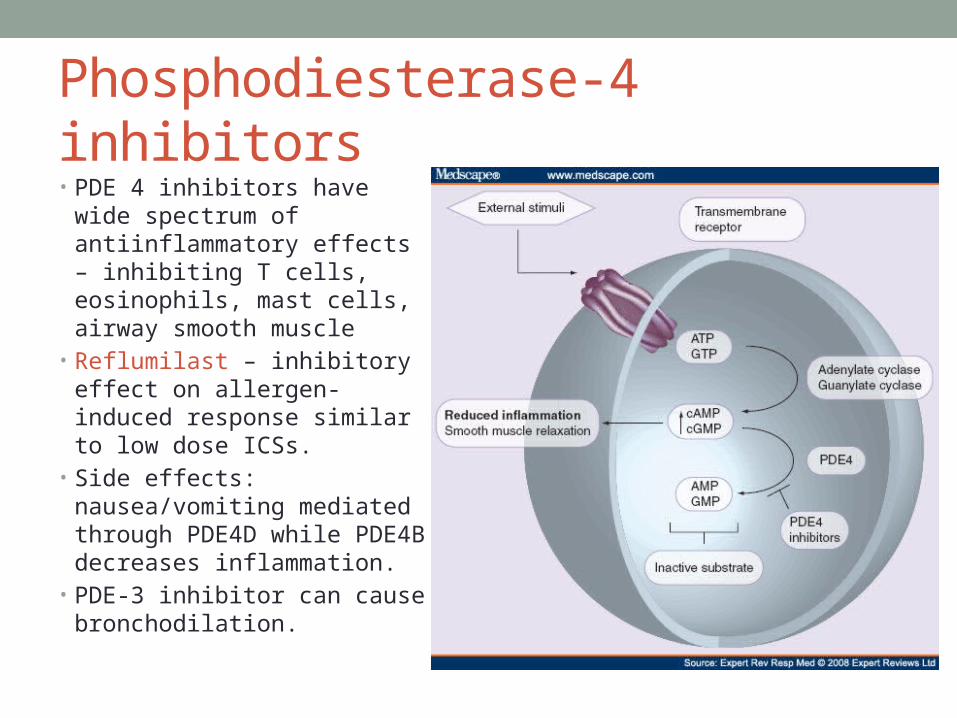
Phosphodiesterase-4 inhibitors• PDE 4 inhibitors have wide
spectrum of antiinflammatory effects – inhibiting T cells, eosinophils, mast cells, airway smooth muscle
• Reflumilast – inhibitory effect on allergen-induced response similar to low dose ICSs.
• Side effects: nausea/vomiting mediated through PDE4D while PDE4B decreases inflammation.
• PDE-3 inhibitor can cause bronchodilation.

Roflumilast• Roflumilast can inhibit
both the early and late phase response in patients with mild allergic asthma.
Respir Res. 2011; 12(1): 140
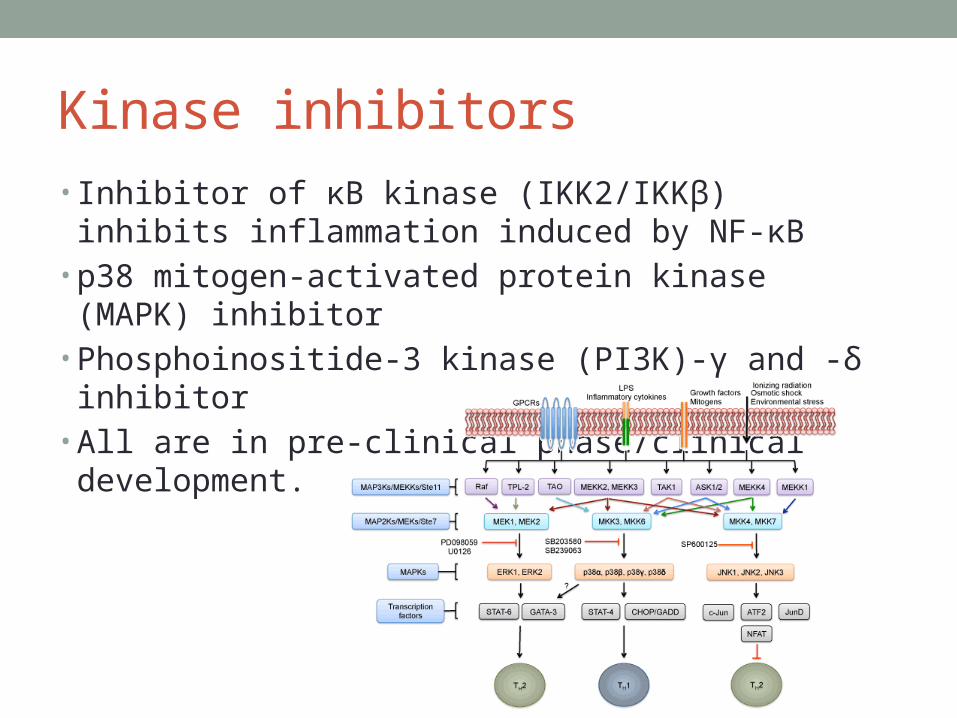
Kinase inhibitors• Inhibitor of κB kinase (IKK2/IKKβ) inhibits inflammation
induced by NF-κB• p38 mitogen-activated protein kinase (MAPK) inhibitor• Phosphoinositide-3 kinase (PI3K)-γ and -δ inhibitor• All are in pre-clinical phase/clinical development.
Other novel antiinflammatory drugs• Adhesion molecule blockade
• Adhesion molecules play important role in recruitment of inflammatory cells from the circulation to the airways.
• PPAR (peroxisome proliferator-activated receptor)-γ agonist • Wide spectrum of anti-inflammatory effects• Polymorphism of PPARγ gene is linked to increased risk of asthma• Rosiglitazone marginally improves lung function in smoking
asthmatics.
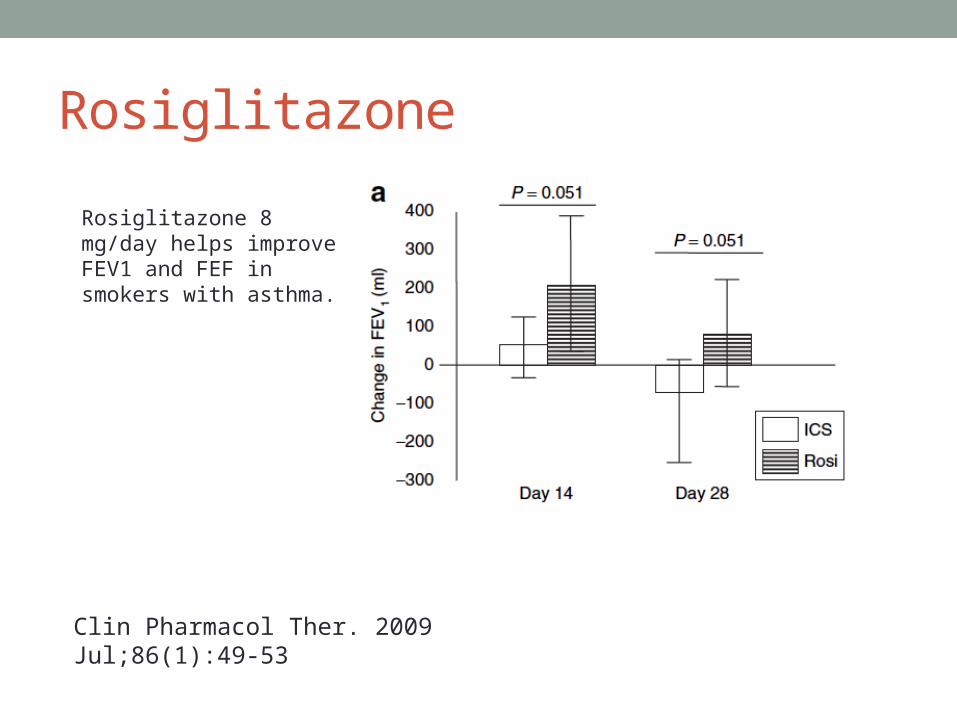
Rosiglitazone
Clin Pharmacol Ther. 2009 Jul;86(1):49-53
Rosiglitazone 8 mg/day helps improve FEV1 and FEF in smokers with asthma.

ANTI-ALLERGY TREATMENTSAnti-IgE therapy
Mast cell inhibitors
Syk Kinase inhibitors

Anti-IgE therapy• Omalizumab, monoclonal antibody that blocks IgE, is now
used in treatment of selected patients with severe asthma.
• More potent anti-IgE antibodies are in development.• Low-affinity IgE receptor (FcεRII or CD23) antagonist
seems to be well tolerated and reduces IgE concentrations in patient with mild asthma in a phase I study.§
§ J Allergy Clin Immunol. 2003 Sep;112(3):563-70.
Mast cell Inhibitors• Mast cell stabilizers
• Cromones (Sodium cromoglycate, nedocromil sodium)• Furosemide • Short-acting, not effective as long-term controllers
• Stem cell factor (SCF)• Key regulator of mast cell survival• Acts via c-Kit, effective in animal model
• c-Kit antagonist (masitinib)• A potent tyrosine kinase inhibitor that block c-Kit and PDGFR• Reduction in steroid use and symptoms in patients with severe
steroid-dependent asthma¶
¶ Allergy. 2009 Aug;64(8):1194-201
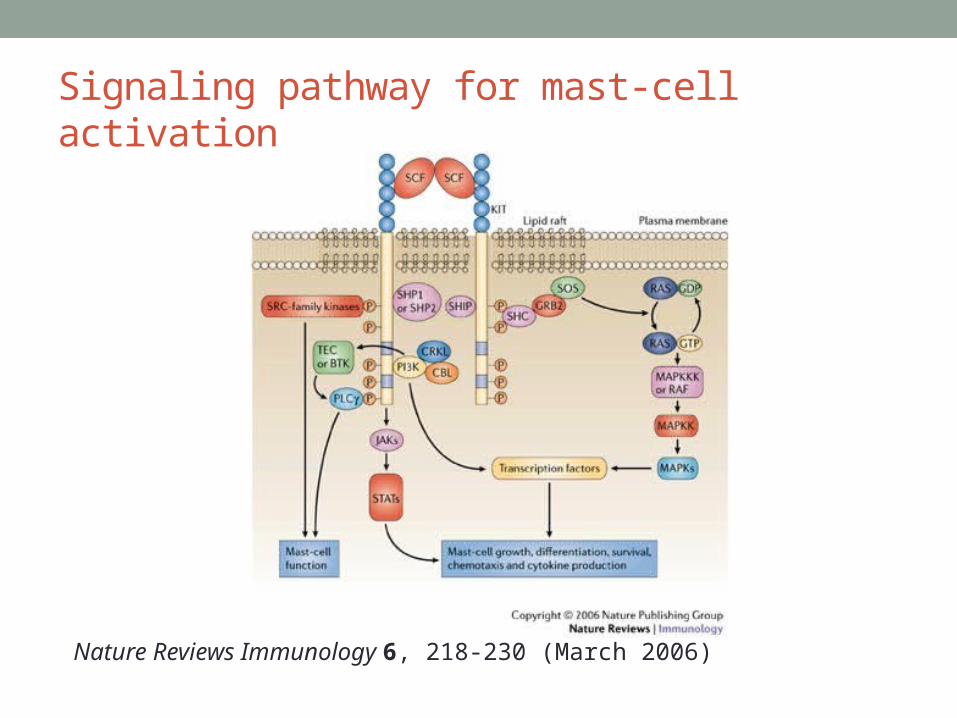
Signaling pathway for mast-cell activation
Nature Reviews Immunology 6, 218-230 (March 2006)
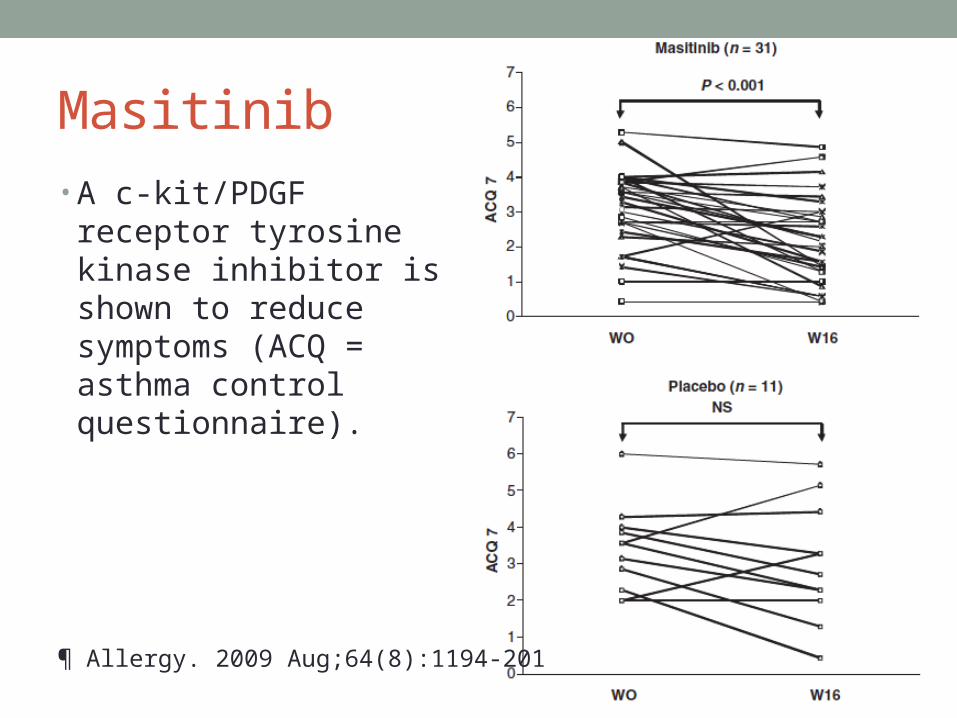
Masitinib• A c-kit/PDGF receptor
tyrosine kinase inhibitor is shown to reduce symptoms (ACQ = asthma control questionnaire).
¶ Allergy. 2009 Aug;64(8):1194-201
Syk kinase Inhibitors• Spleen tyrosine kinase is involved in activation of mast
cells and other immune cells.• Still in pre-clinical studies for asthma
IMPROVED IMMUNOTHERAPYSpecific Immunotherapy
Targeting Treg
Targeting Dendritic Cells
Specific Immunotherapy• Sublingual immunotherapy
• Well tolerated• Effective in reducing symptoms and medication use for allergic
asthma§
• Need long-term study and comparison with ICS
§ Clin Respir J. 2013 Oct 4 Epub ahead of print
Specific immunotherapy• Injection Allergen Immunotherapy
• Cochrane Database 2010 has included 88 trials§
• Significant reduction in asthma symptoms and medication• Improvement in bronchial hyperreactivity• NNT = 3 to avoid one deterioration in asthma symptoms• NNT = 4 to avoid one requiring increased medication• The effect size is comparable to ICS.• Local and systemic reactions are common.• Limitation: significant heterogeneity
§ Cochrane Database Syst Rev. 2010 Aug 4;(8):CD001186

Targeting Tregs• Specific immunotherapy increases Treg numbers and
their expression of IL-10 suppressed Th2 responses decrease IgE synthesis
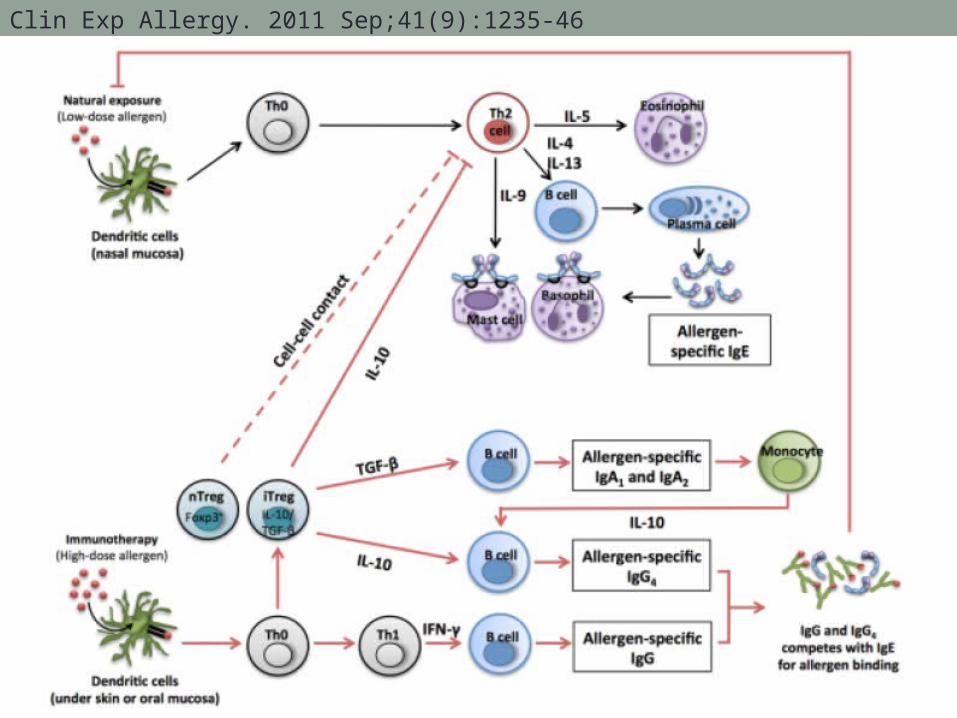
Clin Exp Allergy. 2011 Sep;41(9):1235-46

Targeting Tregs• Tregs from patients with corticosteroid resistant produce
less IL-10.• This can be restored in vitro and in vivo by vitamin D3.
J Clin Invest. 2006 Jan;116(1):146-55
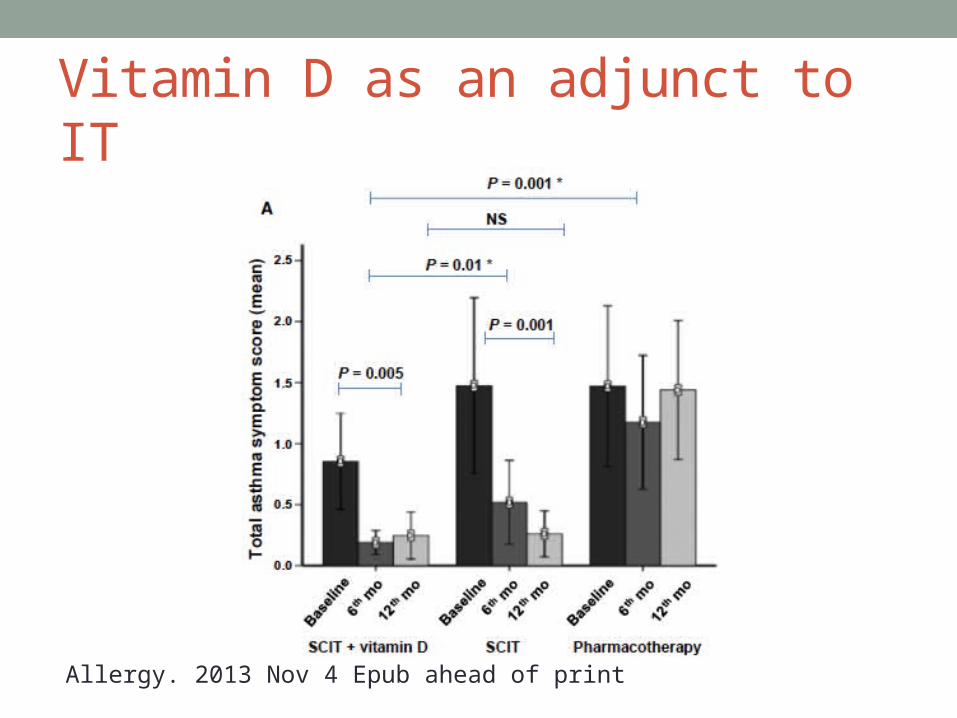
Vitamin D as an adjunct to IT
Allergy. 2013 Nov 4 Epub ahead of print
Targeting Dendritic Cells• Several classes of drug have been shown to suppress
myeloid dendritic cell activation• Prostacyclin (PGI2) e.g. iloprost• Sphingosine-1-phosphate and analogues (fingolimod)
• In preclinical development
Bronchial thermoplasty• Controlled thermal energy to airway wall• Aim to reduce hyperresponsiveness and smooth muscle
mass• Found to be effective in long-term (5-year) and relatively
safe in severe persistent asthma¶
¶ J Allergy Clin Immunol. 2013 Aug 30.
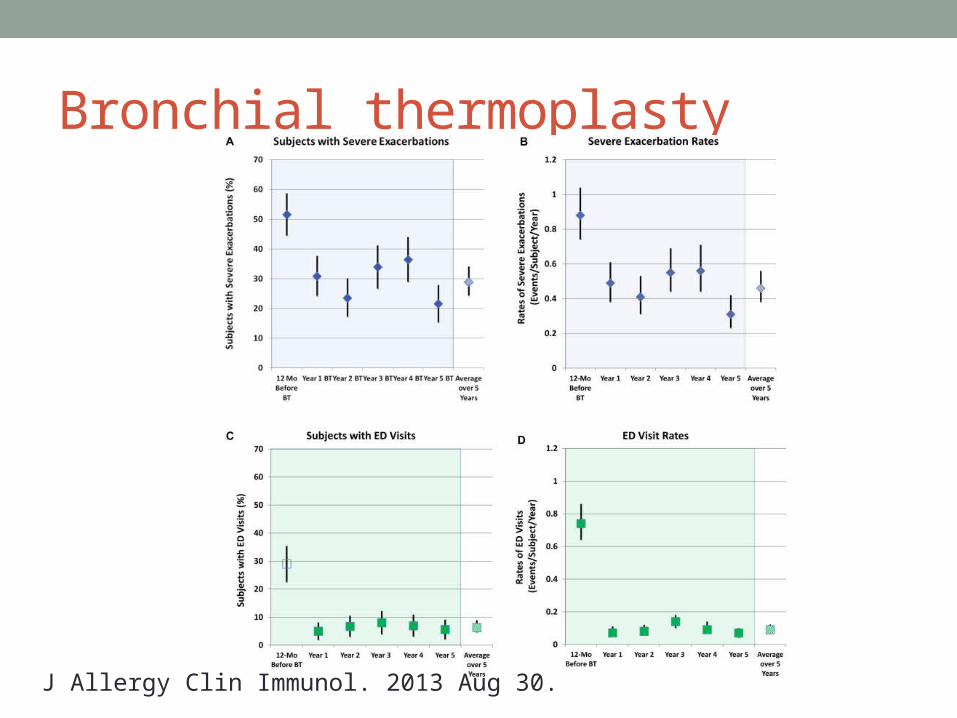
Bronchial thermoplasty
J Allergy Clin Immunol. 2013 Aug 30.