new developments in the management of prostate cancer
DESCRIPTION
New Developments In The Management of Prostate Cancer. Dr. Manish Patel Urological Cancer Surgeon Westmead Public and Private Hospital Sydney Adventist Hospital Senior Lecturer, University of Sydney. New Developments In The Management of Urological Cancers Agenda. - PowerPoint PPT PresentationTRANSCRIPT

New Developments In The New Developments In The Management of Prostate CancerManagement of Prostate Cancer
Dr. Manish Patel Dr. Manish Patel
Urological Cancer SurgeonUrological Cancer Surgeon Westmead Public and Private HospitalWestmead Public and Private Hospital
Sydney Adventist HospitalSydney Adventist HospitalSenior Lecturer, University of SydneySenior Lecturer, University of Sydney
New Developments In The New Developments In The Management of Urological CancersManagement of Urological Cancers
AgendaAgenda• Prostate Cancer- PSA testing
– Controversy on screening.
• Prostate Cancer- New developments in treatment.– Pros and cons of each treatment.

Prostate Cancer- PSA testingProstate Cancer- PSA testing
• Mr J.B. 51 year old.
• Mild LUTS
• Hypertension
• Asks his G.P. for a test for prostate cancer?
• What should the G.P discuss with him?

Prostate Cancer- PSA testingProstate Cancer- PSA testing• Digital Rectal Exam
– Important
– 15% of cancers have abnormal DRE but “normal” PSA
• PSA– Blood test
– Can detect early Cancer
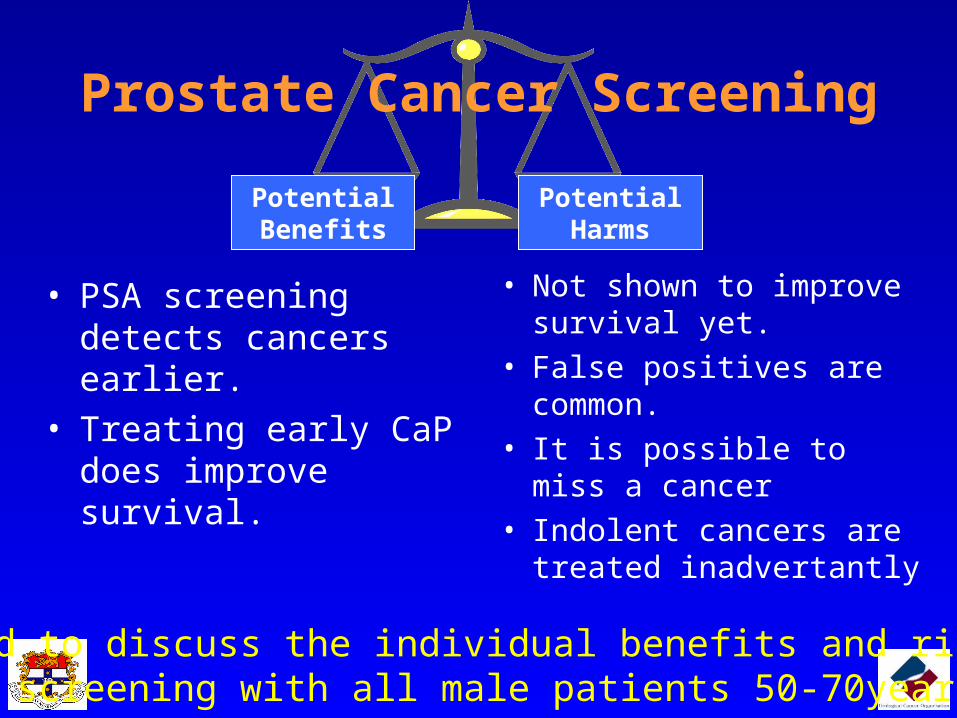
Potential Benefits
Prostate Cancer Screening
Potential Harms
Need to discuss the individual benefits and risksof screening with all male patients 50-70years.
• PSA screening detects cancers earlier.
• Treating early CaP does improve survival.
• Not shown to improve survival yet.
• False positives are common.• It is possible to miss a cancer• Indolent cancers are treated
inadvertantly

Prostate Cancer- PSA testingProstate Cancer- PSA testing
PSA Test: 3.0 ng/ml, F/T 9%, Normal DRE
Is this normal?AgeAge Median PSAMedian PSA Normal RangeNormal Range
40-49 0.7ng/ml 0-2.5ng/ml
50-59 0.9ng/ml 0-3.5ng/ml
60-69 1.2ng/ml 0-4.5ng/ml
70+ 1.4ng/ml 0-6.5ng/ml
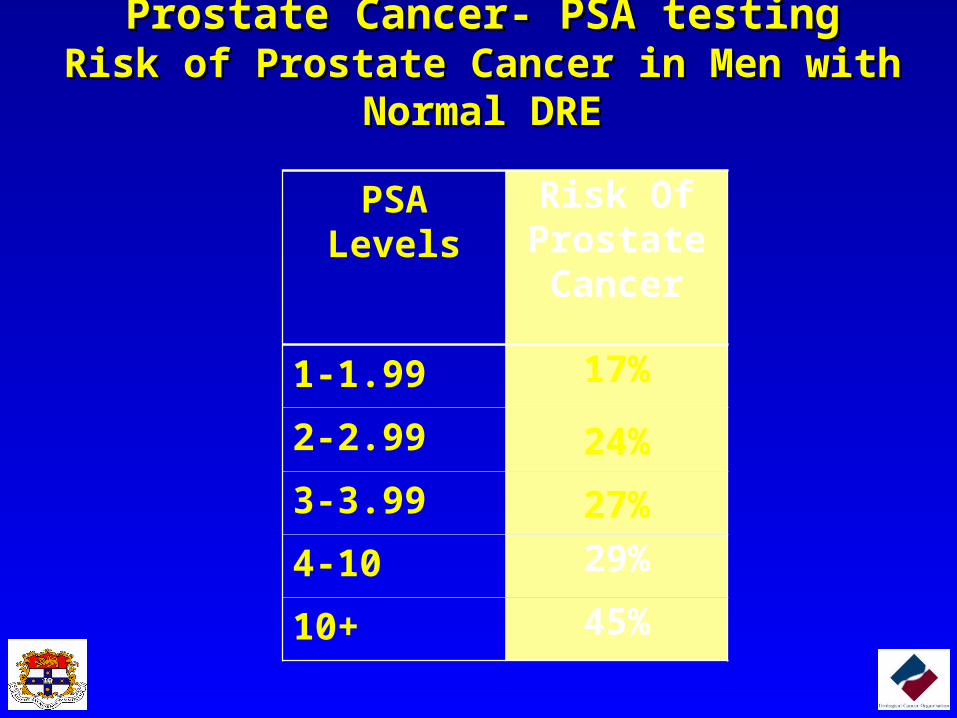
Prostate Cancer- PSA testingProstate Cancer- PSA testingRisk of Prostate Cancer in Men with Normal DRERisk of Prostate Cancer in Men with Normal DRE
PSA Levels Risk Of Prostate Cancer
1-1.99 17%
2-2.99 24%
3-3.99 27%
4-10 29%
10+ 45%

Prostate Cancer- PSA testingProstate Cancer- PSA testing Free to Total (%) Does Help Specificity.

Prostate Cancer- PSA testingProstate Cancer- PSA testingPSA Velocity is important to calculatePSA Velocity is important to calculate
• Men with PSA below 4.0ng/ml– PSA velocity > 10%/yr =30% risk CaP– PSA velocity >0.5ng/ml/yr = 45% risk CaP– PSA velocity >2.0ng/ml/yr = high risk of death– More accurate with multiple measures over time.
1.5
2
2.5
3
3.5
Jan-05 Jul-05 Jan-06
Patient 1Patient 2Patient 3
Prostate Cancer- PSA testingProstate Cancer- PSA testingProstate Biopsy With Local Anaesthetic BlockProstate Biopsy With Local Anaesthetic Block
• Mr J.B.’s risk of cancer is approx 50%.
• Chooses to have a prostate biopsy
• Very well tolerated under local anaesthetic.– Pudendal nerve block.

Prostate Cancer-Options of TreatmentProstate Cancer-Options of TreatmentMr J.B. Has Prostate CancerMr J.B. Has Prostate Cancer
• Biopsy results:• Gleason Score 3+3=6• In 2/12 cores involving 25%-50% of the cores.
• Treatment Decisions Depend On:– Patient’s normal life expectancy
– Aggressiveness of cancer
– Cure rates of individual treatments
– Tolerability of side effects.
• What Are His Options Of Treatment?

Prostate Cancer-Options of TreatmentProstate Cancer-Options of Treatment
• Active Surveillance
• Radical Prostatectomy
• Seed Brachytherapy
• External Beam Radiotherapy
• HIFU (High Intensity Focused Ultrasound)
Indolent Cancer• A cancer that is small and low
grade and unlikely to grow in the man’s lifetime.
• Incidence of indolent cancers is increasing (>30%).
• Mr J.B. Could have active surveillance.

Prostate Cancer-Options of TreatmentProstate Cancer-Options of TreatmentActive SurveillanceActive Surveillance
• Treatment for small low grade cancers with low biological potential.
• Very close monitoring 3 monthly– PSA
– DRE
– Biopsy at 6 months, 18 months and 2 yearly after.
• Treat curatively if any sign of cancer growth.
Patel et.al J Urol 2004

Pros and Cons of Active Surveillance
Pros• No major procedure• No side effects of
treatment
Cons• Anxiety will lead to
treatment in 15%• 50% will progress
over 10 years• Although no side
effects not likely to improve overall quality of life.

A Biopsy At 6 Months Is Very Predictive
Of Cancer Growth.
Months
140120100806040200
Fre
edom
Fro
m P
rogre
ssio
n
1.0
.8
.6
.4
.2
0.0
2nd Biopsy -ve
Log Rank Test p=0.002
2nd Biopsy +ve
Patel et.al. J Urol. 2004;171(4):1520

Prostate Cancer-Options of TreatmentProstate Cancer-Options of Treatment Radical Prostatectomy

(R) Cavernous(R) Cavernous|nerve|nerve
ProstateProstate
FeetFeet
HeadHead

Recovery of Erections after RP By Extent of Preservation of Neurovascular
Bundles

Sural Nerve Grafts- For patients Undergoing NVB Resection
Undergoes radical prostatectomy with unilateral neurovascular bundle resection
Also has sural nerve graft placed

Recovery of Potency for Unilateral Resection with Nerve Graft compared to No Nerve Graft
Months
60483624120
Pro
po
rtio
n P
atie
nts
Re
cove
rin
g E
rect
ile F
un
ctio
n 1.0
.8
.6
.4
.2
0.0
Unilateral nerve graft n=45
No nerve graft n=17
Patel et.al. AUA 2003

Pros and Cons of SurgeryPros and Cons of Surgery
Pros• Excellent cancer control• Evaluate the lymph nodes• Accurate prognosis• Radiotherapy possible
after surgery
Cons
• Recovery 2-3 weeks
• Major Surgery
• Possible incontinence
• Possible impotence

Prostate Outline
UrethraRectum
Prostate Cancer-Options of TreatmentProstate Cancer-Options of TreatmentSeed BrachytherapySeed Brachytherapy

Brachytherapy (seed)• Toxicity
– Urinary• Frequency/Urgency• Retention• Bleeding
– Rectal• Same
– Impotence• L/T same as surgery (bilateral nerve sparing)

Pros and Cons of BrachytherapyPros• Not a major procedure• Quick recovery• Initially potency
preserved
Cons• Only controls low risk disease• L/T outcomes not known thus
hesitate in young patients.• Won’t know prognosis for 1-2
years• L/T impotence same as surgery• Significant rectal and urinary
side effects.• Unable to have surgery after
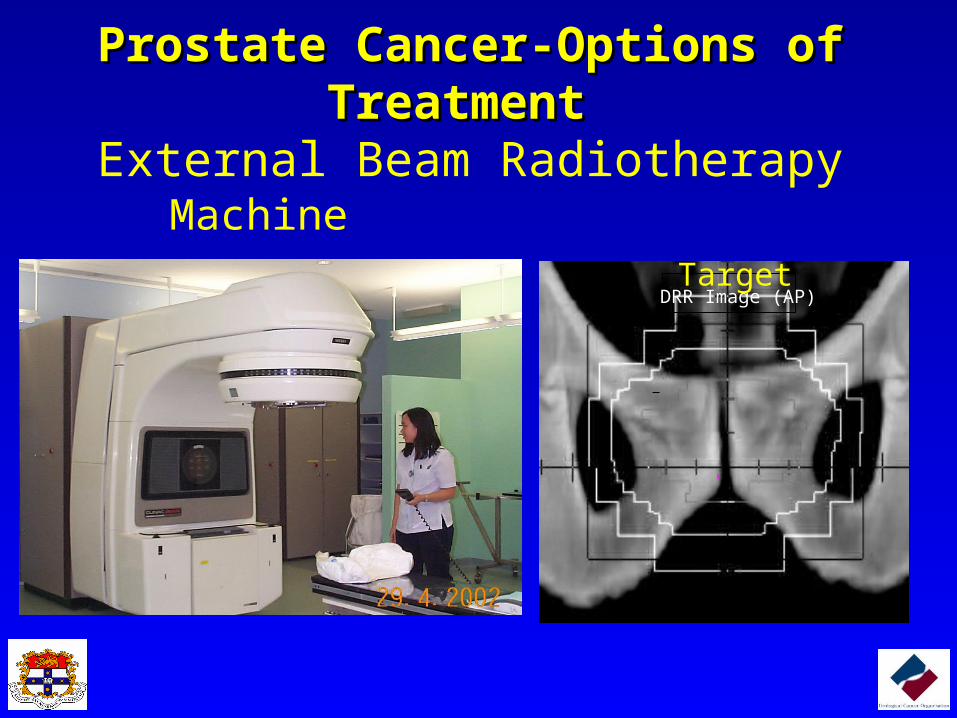
Prostate Cancer-Options of TreatmentProstate Cancer-Options of Treatment External Beam Radiotherapy
DRR Image (AP)
MachineTarget
External Beam Radiotherapy• Toxicity
– Urinary• Frequency/Urgency• Retention/Stricture• Bleeding
– Rectal• Same
– Impotence• L/T same as surgery (bilateral nerve sparing)

Pros and Cons of RadiotherapyPros• Not major surgery• Initially potency
preserved
Cons• 7 weeks treatment• Won’t know prognosis
for 1-2 years• L/T impotence same as
surgery• Significant rectal and
urinary side effects.• Unable to have surgery
after

Prostate Cancer-Options of TreatmentProstate Cancer-Options of Treatment New Treatments- HIFU
•Minimally invasive
•US focused in the prostate causes coagulative necrosis
•Temporary catheter for 2 weeks.
•Experimental, but recent results are encouraging.

HIFUAdvantages• Minimally invasive• Relieves obstructive
symptoms• Early cancer cure appears
similar to XRT• Treatment is repeatable• Possible to have surgery
afterwards.• 90% potency
Disadvantages• New technology- L/T
results unknown.• Expensive• Limited to small
prostates and Gleason 7 or less.

Mr J.B
• Chose radical prostatectomy
• Continent after 2 weeks.
• Started penile rehabilitiation at 6 weeks
• Potent at 4 months.
• PSA recurrence free so far.

Case 2
• Mr AB
• 72 year old
• HT
• Coronary stents
• PSA 15.2ng/ml
• Rectal exam: large hard right sided nodule.
Case 2
• Prostate Biopsy:
• Gleason 4+4
• 6/12 cores involved

Following Diagnosis- Need to Be Staged.A CT Scan Will
detect metastases to the lymph nodes.
A Bones Scan will detect cancer in the bones

Treatment OptionsTreatment Options
• Watchful Waiting
• XRT plus Hormone therapy
• HDR Brachytherapy plus Hormone Therapy
• Radical Prostatectomy
Prostate Cancer-Options of TreatmentProstate Cancer-Options of TreatmentNeed Adjuvant Androgen Deprivation Therapy Need Adjuvant Androgen Deprivation Therapy
For High Risk Disease.For High Risk Disease.
• Hot flushes
• Lethargy
• Depression/mood swings
• Weight gain
• Anaemia
• Osteoporosis
• Impotence
• Muscle loss
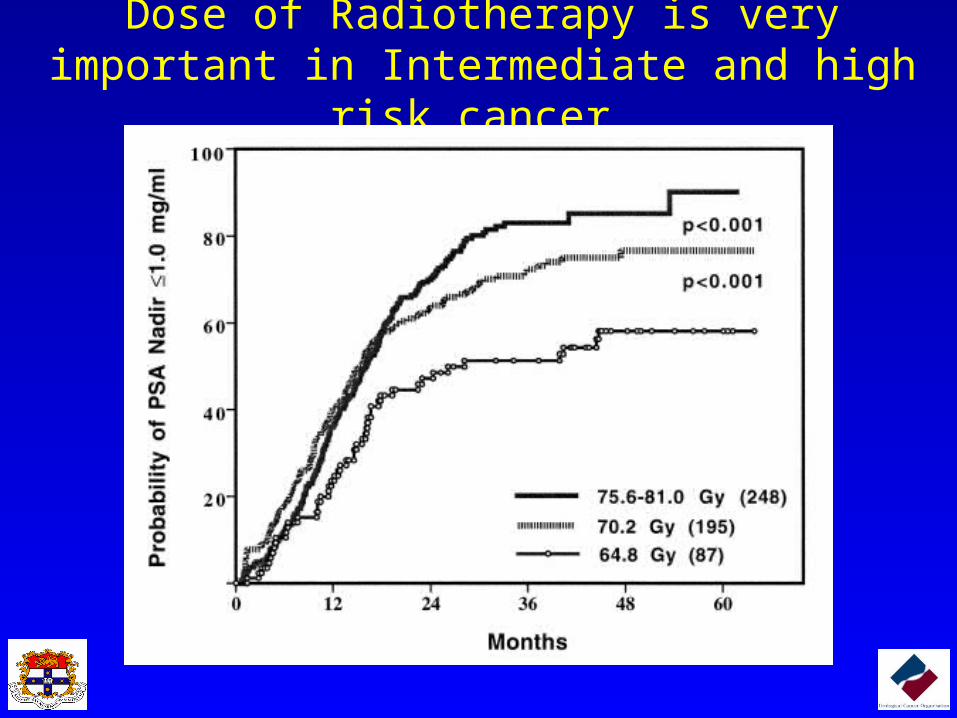
Dose of Radiotherapy is very important in Intermediate and high risk cancer.

External Beam RadiotherapyExternal Beam Radiotherapy
From Liebel and Fuks. MSKCC, 2000From Liebel and Fuks. MSKCC, 2000
Prostate Cancer-Options of TreatmentProstate Cancer-Options of TreatmentHigh Dose Rate Brachytherapy.High Dose Rate Brachytherapy.
Increases dose to the prostate locallyFor high risk disease

HDR Brachytherapy Boost• Used for high risk prostate cancers• Used in conjunction with hormones and external
beam radiotherapy• Advantages
– Higher radiation dose
– Theoretically better cancer result
• Disadvantages– Much higher urinary side effects
– No Long term studies

Pros and Cons Of Prostate Cancer Treatments
Cancer CureSide Effects
Pros Cons
Radical Prostatectomy
Highest Cure RateCancer removedLymph nodes treatedSalvage XRT
Recovery timeIncontinenceED
Robotic Prostatectomy
Lower than open operation.
Earlier discharge Worse incontinence
BrachytherapyOnly effective in low risk disease
Early recoverySevere urinary and rectal SEED
External Beam Radiotherapy
Moderate cure rate Same as above
HDR Brachytherapy
Effective for high risk disease
Severe urinary SEED
HIFUHIFUPossibly equivalent to XRT.
Minimally invasiveMultiple treatments
Irritative urinay SE

SummarySummary
• Age specific PSA is Important but PSA velocity Age specific PSA is Important but PSA velocity and F/T ratio are important when PSAs are low.and F/T ratio are important when PSAs are low.– Have a low threshold to referHave a low threshold to refer..
• Treatment decisions for prostate cancer depend onTreatment decisions for prostate cancer depend on– likely threat of the cancer to lifelikely threat of the cancer to life– cure rate achieved by the treatmentcure rate achieved by the treatment– side-effect profile.side-effect profile.