new and emerging treatments for osteoarthritis management: will the dream come true with...
TRANSCRIPT

1. Introduction
2. DMOADs targeting pathways
of cartilage catabolism and
anabolism
3. DMOADs targeting
subchondral bone remodeling
4. Targeting inflammatory
pathways
5. Gene therapy in OA
6. Perspectives: microRNAs and
small interfering
RNA-based therapeutic
approaches in OA
7. Conclusion
8. Expert opinion: toward
targeted personalized
medicine in OA
Review
New and emerging treatments forosteoarthritis management: willthe dream come true withpersonalized medicine?Camille Roubille, Jean-Pierre Pelletier & Johanne Martel-Pelletier†
†University of Montreal Hospital Research Centre (CRCHUM), Notre-Dame Hospital, Department
of Medicine, Osteoarthritis Research Unit, Montreal, Quebec, Canada
Introduction: Osteoarthritis (OA) is a dynamic process involving the main tis-
sues of the joint for which a global approach should be considered. No
disease-modifying OA drug (DMOAD) has yet been approved. New therapeu-
tic strategies are needed that would be cost effective by reducing the need for
pharmacological interventions and surgical management while targeting
specific pathways leading to OA. The treatment landscape of OA is about to
change based on new agents having shown some structural effects and
emerging therapies with DMOAD effects.
Areas covered: In this review based on a Medline (via PubMed) search, prom-
ising new and emerging therapies with a potential structural effect (DMOAD)
will be discussed including growth factors, platelet-rich plasma, autologous
stem cells, bone remodeling modulators, cytokine inhibition, gene therapy,
and RNA interference.
Expert opinion: DMOAD development should focus on targeting some phe-
notypes of OA patients evidenced with sensitive techniques such as magnetic
resonance imaging, as a single treatment will unlikely be appropriate for all
OA patients. This will allow the development of DMOADs based on persona-
lized medicine. An exciting new era in DMOAD development is within reach,
provided future clinical trials are sufficiently powered, systematically
designed, use the appropriate evaluation tools, and target the appropriate
categories of OA patients.
Keywords: disease-modifying osteoarthritis drug, gene therapy, knee osteoarthritis, MRI, stem
cells, strontium ranelate, subchondral bone
Expert Opin. Pharmacother. (2013) 14(15):2059-2077
1. Introduction
Osteoarthritis (OA) is a whole joint disease characterized by degradation and loss ofarticular cartilage, hypertrophic bone changes with osteophyte formation, subchon-dral bone remodeling, and inflammation of the synovial membrane. Importantadvances have been made in understanding its pathological processes, and promisingnew structure-modifying therapeutic agents that may slow or arrest the progression ofthe disease are being developed, aimed at improving current treatment.
OA is a multifactorial disease resulting in the failure of the joint ‘organ,’ leadingto the degeneration of articular tissues. This disease may result from genetic predis-position, aging, mechanical stress, or low-grade systemic inflammation associatedwith trauma and obesity [1]. Joint tissue cells are responsible for the maintenanceof a healthy extracellular matrix. Modification in their environment, such asmechanical factors, could activate these cells’ anabolic function to repair tissue dam-age. Under stimulation by growth factors at an early stage of OA, the cells produce
10.1517/14656566.2013.825606 © 2013 Informa UK, Ltd. ISSN 1465-6566, e-ISSN 1744-7666 2059All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

inadequate molecules, as well as osteophytes. With time, thisattempt fails and leads to an imbalance favoring degradation.During OA, the cells in cartilage, synovial membrane, andsubchondral bone release proteinases (e.g., metalloproteinases[MMPs] and aggrecanases [ADAMTS]) and inflammatorycytokines including interleukin-1b (IL-1b) and tumor necrosisfactor-a (TNF-a), which enhance the synthesis of proteinasesand other factors to further degrade the joint tissues, over-whelming endogenous inhibitors for example. Cartilage extra-cellular matrix is degraded and replaced by a matrix that isunable to withstand normal mechanical factors. A number ofstudies have demonstrated the importance of the cross-talk between cartilage, synovial membrane, and subchondralbone in the pathophysiology of OA. Synovial inflammation,secondary to the release of cartilage fragments into the synovialfluid, and subchondral bone remodeling by its release of solublemediators affect the cartilage by sustaining its degradation.Even if the precise interaction between cartilage erosion,
chronic synovial inflammation, and remodeling of subchon-dral bone is not yet determined, magnetic resonance imaging(MRI) has contributed to improve our understanding of theOA process and different phenotypes, underlining the inter-connection of these three joint tissues.Data reported poor correlation between cartilage preserva-
tion and symptoms. This is probably due to the fact that artic-ular cartilage is avascular and aneural and that OA pain ismost likely multifactorial, involving synovitis and subchon-dral bone lesions. This could explain why a sole agent hasnot achieved both symptomatic and structural effects so far.However, in our opinion, the overall goal in OA managementremains cartilage preservation.
One of the most exciting challenges in the field of rheuma-tology is to find novel therapeutics that will modify the struc-tural changes that occur in the joint tissues during the disease.The development of new OA treatment needs an innovativeand global approach. New therapeutic strategies that wouldbe cost effective by reducing the need for pharmacologicalinterventions and surgical management, while targetingspecific pathways leading to OA, are needed. Targetingcartilage changes (catabolism and anabolism), subchondralbone remodeling, and synovial inflammation and/or low-grade inflammation are the main thrusts of research indisease-modifying OA drug (DMOAD) development.
The present review will focus on therapies with DMOADeffect, not only new agents having evidence of structuraleffects, but also promising emerging treatments with a poten-tial for structural impact.
2. DMOADs targeting pathways of cartilagecatabolism and anabolism
2.1 Growth factors: bone morphogenetic protein-7
and fibroblast growth factor-18Two growth factors involved in OA cartilage repair are cur-rently in clinical trials: bone morphogenetic protein-7(BMP-7), also known as osteogenic protein-1, and fibroblastgrowth factor-18 (FGF-18).
In vivo, in animal models, BMP-7 demonstrated reparativeeffects on articular cartilage degradation [2]. In vitro, humanchondrocytes also promote cartilage formation in response toBMP-7 treatment [3]. One completed Phase I trial using aweekly intra-articular injection of BMP-7 found no dose-limiting toxicity. By the 12th week of treatment, there was atrend toward a greater symptomatic improvement comparedto placebo in knee OA patients who received 0.1 and 0.3 mgof BMP-7 [4]. Another Phase I trial ([5]-NCT01133613) anda Phase II trial ([5]-NCT01111045) have been completed butresults are not yet available.
In a meniscal tear rat model of OA, biweekly intra-articular injections of FGF-18 for 3 weeks induced chondro-genesis and cartilage repair, with dose-dependent increasesin cartilage thickness of the tibial plateau [6]. Two Phase Istudies ([5]-NCT01033994 and 00911469) have been com-pleted. The first placebo-controlled Phase I study [7] evaluatedthe DMOAD effects of intra-articular administration ofFGF-18 after single or multiple escalating doses over a3-week period in primary knee OA patients (Kellgren-Law-rence [KL] grades 2 or 3) with no major knee surgery plannedfor at least 1 year after the FGF-18 injection. Outcomes weretibiofemoral cartilage volume change assessed by MRI, loss ofjoint space width (JSW) measured by X-rays, as well as theWestern Ontario and McMaster Universities OsteoarthritisIndex (WOMAC) pain and function scores after 1 year.A dose-dependent reduction in tibiofemoral cartilage volumeloss was found in patients treated with FGF-18 compared to
Article highlights.
. OA should be considered a dynamic process and may bea systemic disease with several pathways to target forDMOAD development.
. Promising emerging therapies include autologous MSCs,PRP, bone remodeling modulators, cytokine inhibitors,and gene therapy.
. With the advent of DMOADs, physicians should aim attreating a ‘patient’ rather than a ‘disease.’ Combiningtherapeutics at both local and systemic levels to impactboth symptoms and joint structural changes will likely bethe future strategy instead of a sole drug, at least at thebeginning of the treatment.
. Selectively targeting some phenotypes of OA patientsevidenced by sensitive tools, such as MRI, may allow thedevelopment of DMOADs based onpersonalized medicine.
. Clinical trials that would be sufficiently powered,systematically designed and, based on reliable evaluationtechniques, targeting the appropriate categories of OApatients should translate the concept of DMOAD fromdream to reality.
This box summarizes key points contained in the article.
C. Roubille et al.
2060 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

placebo, particularly in the lateral compartment. A reductionin the lateral JSW loss was also evidenced in the FGF-18group compared to placebo. However, no significant symp-tomatic difference between the FGF-18-treated group andplacebo group was observed with regard to the WOMACpain and function scores. Tolerance of the active treatmentwas good and no safety issue was observed. A proof-of-concept Phase II study in patients with acute cartilage injuriesof the knee is ongoing ([5]-NCT01066871).
2.2 Platelet-rich plasma: rationale, primary results in
knee OA, and current issuesAutologous platelet-rich plasma (PRP) is plasma from thepatient’s own blood, in which the platelet concentration isabove baseline values [8]. The rationale for using PRP is thatplatelets contain storage pools of growth factors, includingtransforming growth factor-b (TGF-b), platelet-derivedgrowth factor (PDGF), vascular endothelial growth factor,as well as cytokines, chemokines, and other mediators [9],which are currently thought to accelerate the natural healingprocess and promote cartilage repair after local injection.Moreover, as TGF-b and PDGF can stimulate the prolifera-tion of mesenchymal stem cells (MSCs), these factors maydirect the local mesenchymal and epithelial cells to migrate,divide, and increase collagen and matrix synthesis [10]. Never-theless, the exact mechanism of how PRP could improve car-tilage healing in OA remains to be determined. It is suggestedthat PRP may have an indirect effect by reducing synovialinflammation and modulating cytokinic local environmentor a direct effect by stimulating the chondral anabolism andslowing the catabolic activity [11]. Indeed, growth factors con-tained in PRP may increase expression of the chondrocytephenotype and stimulate the differentiation of MSCs aswell as reduce IL-1 synthesis. Moreover, platelet-releasedgrowth factors may regulate endogenous hyaluronic acid(HA) synthesis [10], which could contribute to its action.
First reports of PRP efficacy in musculoskeletal conditionsconcerned sports- and overuse-related injuries, such as tendi-nitis, acute rotator cuff tears, and knee cartilage lesions [12].Nowadays a growing literature portrays PRP as a simple,low-cost, minimally invasive and promising therapy for kneeOA because of its potential for articular cartilage repair. How-ever, high-quality studies sufficiently powered to support suchpostulate are lacking; indeed, the literature contains mostlyanecdotal reports and case series or studies of small samplesize or uncontrolled studies [13-16]. On the other hand, somestudies compared PRP to HA for ethical reasons, while othersused placebo. Explanation of the data is also complicated by alack of standardization of study protocols, especially PRPpreparation and subsequent variability in platelet concentra-tions, as well as platelet activation status. Some used freshPRP, avoiding cold storage which is thought to potentiallyalter platelet function [11], while others preferred to freezePRP and delay intra-articular injection to assess the sample
quality [17]. Moreover, the role of white blood cell (WBC) fil-tering during PRP preparation remains uncertain as WBCsare not only a source of cytokines and enzymes but can alsorelease proteases and reactive oxygen [17]. Additional issuesare the number and frequency of injections for optimalresults, and for which OA patients this therapy would be themost effective [11]. Future clinical trials are needed to addressthese issues.
A recent prospective study enrolling 150 patients withdegenerative knee cartilage lesions and OA compared50 patients treated with PRP to 50 patients each receivingeither low-molecular-weight HA (LWHA) or high-molecu-lar-weight HA (HWHA) [13]. At 2 months, the PRP groupshowed improvement similar to the LWHA group but moreimprovement than the HWHA group. However, at 6 months,a better benefit in the PRP group was found [13]. Furthermore,PRP in patients under 50 years old with only cartilage lesionsor early OA had better results than LWHA, arguing thatyounger patients with early disease could have a better chanceto benefit from PRP therapy [17]. Spakova et al. [18] also com-pared PRP to viscosupplementation, both injected weekly for3 weeks, in a cohort of 120 knee OA patients (KL grades1 -- 3). Data showed a significantly better improvement inWOMAC and pain intensity numeric rating scale at 3 and6 months in both groups with statistically superior results inthe PRP group. Three main randomized controlled trials(RCTs) in knee OA, two comparing PRP to HA and one com-paring PRP to placebo, have been published so far [11,17,19].Filardo et al. [17] evaluated with various clinical scores 109knee OA patients (KL grades up to 3), 55 treated with HAand 54 with PRP (both 3 weekly injections) at 2, 6, and12 months. PRPs were obtained through a double-spinningprocedure providing a high concentration of platelets but alsocontaining WBCs, and were frozen before injection. Bothgroups improved and no statistical differences were foundbetween HA and PRP patients for all scores. A trend favoringthe PRP group was noted only in patients with low-gradearticular degeneration (KL grade up to 2) at 6 and 12 months.Sanchez et al. [19] compared at short-term follow-up (24 weeks)plasma rich in growth factors (PRGF) (single spinning proce-dure providing WBC-free PRP with a low platelet concentra-tion) with HA, both administered 3 times on a weekly basis.The primary outcome measure was a 50% decrease in kneepain from baseline to week 24. Compared with the rate ofresponse to HA, the rate of response to PRGF was significantat 14.1% points higher. However, no significant differenceswere found between PRGF and HA groups with regard to allsecondary outcomes measured, including WOMAC. Recently,Patel et al. [11] evaluated 78 patients (156 knees) with bilateralknee OA divided into 3 groups, one receiving a single injectionof PRP (WBC filtered), one 2 injections of PRP 3 weeks apart,and one a single injection of saline as placebo control group.WOMAC and Visual Analog Scale (VAS) pain and overall sat-isfaction were measured at 6 weeks, and at 3 and 6 months.Both groups treated with PRP compared to the placebo group
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2061
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.
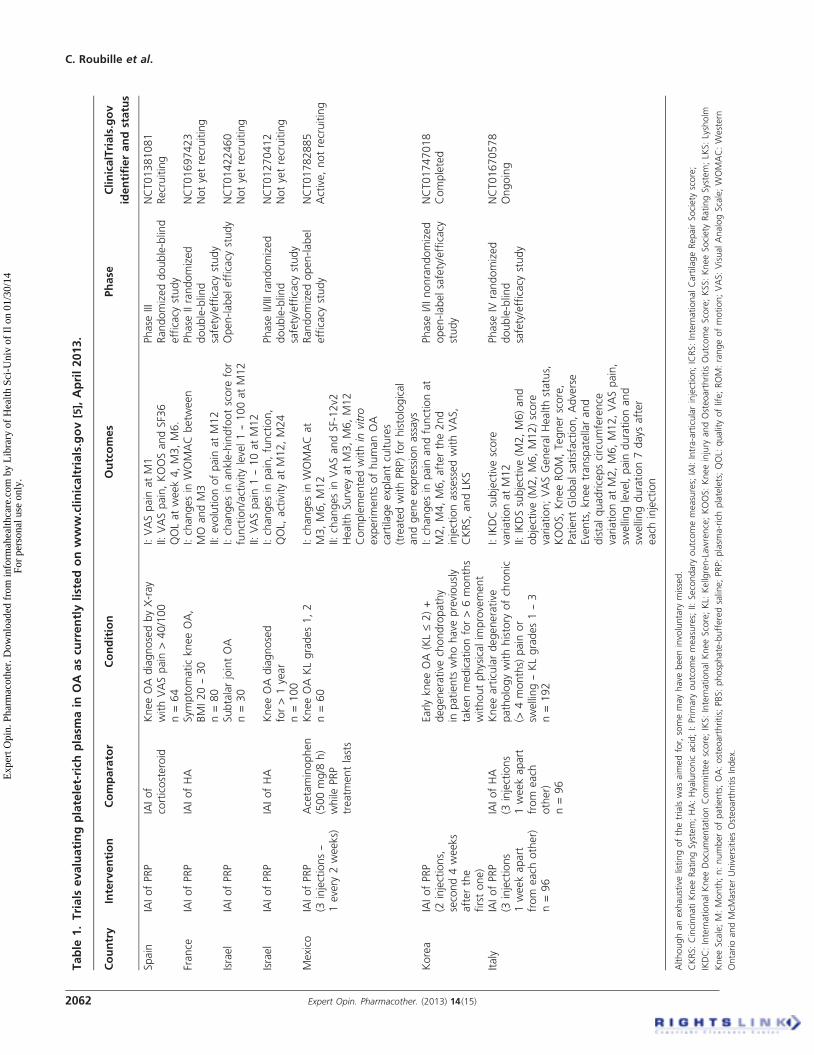
Table
1.Trials
evaluatingplatelet-rich
plasm
ain
OA
ascu
rrentlylistedonwww.clinicaltrials.gov
[5],April2013.
Country
Intervention
Comparator
Condition
Outcomes
Phase
ClinicalTrials.gov
identifierandstatus
Spain
IAIofPRP
IAIof
corticosteroid
KneeOAdiagnosedbyX-ray
withVASpain
>40/100
n=64
I:VASpain
atM1
II:VASpain,KOOSandSF36
QOLatweek4,M3,M6.
Phase
IIIRandomizeddouble-blind
efficacy
study
NCT01381081
Recruiting
France
IAIofPRP
IAIofHA
Sym
ptomatickneeOA,
BMI20--30
n=80
I:changesin
WOMAC
betw
een
MO
andM3
II:evolutionofpain
atM12
Phase
IIrandomized
double-blind
safety/efficacy
study
NCT01697423
Notyetrecruiting
Israel
IAIofPRP
SubtalarjointOA
n=30
I:changesin
ankle-hindfootscore
for
function/activitylevel1--100atM12
II:VASpain
1--10atM12
Open-labelefficacy
study
NCT01422460
Notyetrecruiting
Israel
IAIofPRP
IAIofHA
KneeOAdiagnosed
for>1year
n=100
I:changesin
pain,function,
QOL,
activityatM12,M24
Phase
II/IIIrandomized
double-blind
safety/efficacy
study
NCT01270412
Notyetrecruiting
Mexico
IAIofPRP
(3injections--
1every
2weeks)
Acetaminophen
(500mg/8
h)
while
PRP
treatm
entlasts
KneeOAKLgrades1,2
n=60
I:changesin
WOMAC
at
M3,M6,M12
II:changesin
VASandSF-12v2
HealthSurveyatM3,M6,M12
Complementedwithin
vitro
experiments
ofhumanOA
cartilageexplantcultures
(treatedwithPRP)forhistological
andgeneexpressionassays
Randomizedopen-label
efficacy
study
NCT01782885
Active,notrecruiting
Korea
IAIofPRP
(2injections,
second4weeks
afterthe
firstone)
EarlykneeOA
(KL£2)+
degenerative
chondropathy
inpatients
whohave
previously
takenmedicationfor>6months
withoutphysicalim
provement
I:changesin
pain
andfunctionat
M2,M4,M6,afterthe2nd
injectionassessedwithVAS,
CKRS,andLK
S
Phase
I/IInonrandomized
open-labelsafety/efficacy
study
NCT01747018
Completed
Italy
IAIofPRP
(3injections
1weekapart
from
each
other)
n=96
IAIofHA
(3injections
1weekapart
from
each
other)
n=96
Kneearticulardegenerative
pathologywithhistory
ofchronic
(>4months)
pain
or
swelling--KLgrades1--3
n=192
I:IKDCsubjectivescore
variationatM12
II:IKDSsubjective(M
2,M6)and
objective(M
2,M6,M12)score
variation;VASGeneralHealthstatus,
KOOS,KneeROM,Tegnerscore,
PatientGlobalsatisfaction,Adverse
Events,kneetranspatellarand
distalquadricepscircumference
variationatM2,M6,M12,VASpain,
swellinglevel,pain
durationand
swellingduration7days
after
each
injection
Phase
IVrandomized
double-blind
safety/efficacy
study
NCT01670578
Ongoing
Althoughanexhaustivelistingofthetrialswasaim
edfor,somemayhave
beeninvoluntary
missed.
CKRS:CincinnatiKneeRatingSystem;HA:Hyaluronic
acid;I:Primary
outcomemeasures;
II:Secondary
outcomemeasures;
IAI:Intra-articularinjection;ICRS:InternationalCartilageRepairSociety
score;
IKDC:InternationalKneeDocumentationCommitteescore;IKS:InternationalKneeScore;KL:
Kellgren-Lawrence;KOOS:Kneeinjury
andOsteoarthritisOutcomeScore;KSS:KneeSociety
RatingSystem;LK
S:Lysholm
KneeScale;M:Month;n:numberofpatients;OA:osteoarthritis;
PBS:phosphate-bufferedsaline;PRP:plasm
a-richplatelets;QOL:
qualityoflife;ROM:rangeofmotion;VAS:VisualAnalogScale;WOMAC:Western
OntarioandMcM
asterUniversitiesOsteoarthritisIndex.
C. Roubille et al.
2062 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

had statistically significantly better results within 2 -- 3 weeksand lasting until 6 months. It is noteworthy that all these stud-ies described improvement in pain scores but did not assess car-tilage damage. Several studies are currently ongoing (Table 1),but we found no study that aimed at evaluating the structuralDMOAD effect of PRP. However, given the rationale of usingPRP in OA, partly based on the fact that growth factors mayinfluence cartilage repair through their potential effects onstem cells, PRP may be a future DMOAD. For this reason,investigation of its structural effects in future trials is needed.
2.3 Blocking nitric oxideNitric oxide (NO) contributes to extracellular matrix damagein OA [20]. Inducible NO synthase (iNOS) is responsible forexcessive and sustained NO production by chondrocytes.Selective inhibition of iNOS reduced the progression ofexperimental OA in an animal model [21]. However, a recent2-year RCT (Phase II/III) of an oral iNOS inhibitor (cinduni-stat) showed no superiority of cindunistat over placebo forrate of change in joint space narrowing (JSN) and no effecton pain or function. Only a transient slowing of JSN wasnoted in KL grade 2 OA patients at 48 weeks, which wasnot sustained at 96 weeks of follow-up. No slowing in OAprogression was evidenced in KL grade 3 OA patients [22].
2.4 Regenerative medicine in cartilage repair:
potential for stem cellsThe capacity of adult cartilage to regenerate is limited becauseof its avascular nature. Regeneration of normal cartilage is agreat challenge. Regenerative therapy is based on stem cellsand other tissue-engineering strategies aimed at replacingOA tissue with native-like functional tissue with the sameproperties as normal cartilage. Even though limited clinicaltrial data on the therapeutic impact of stem cells in OA havebeen reported to date, regenerative medicine may be a prom-ising emerging therapy for future OA management. Severaltypes of stem cells may be used: embryonic stem cells(ESCs) and adult stem cells, which are progenitor cells locatedinside differentiated tissues, such as MSCs, induced pluripo-tent stem cells, and in situ chondrogenic progenitor cells(CPCs) [23]. ESCs are pluripotent and immortal stem cells,with the advantage of a potential sustained differentiationinto chondrogenic lineage when stimulated by the growthfactors of the TGF-b family and bone morphogenic protein(e.g., BMP-7), but also the possibility of inducing teratomas.
MSCs may be a promising therapy for OA because of theirmultilineage potential, immunosuppressive activities, andlimited immunogenicity. Bone marrow and adipose tissueare the two main sources of MSCs for cell therapy. MSCsare defined by their plastic adherence property, their pheno-type (positive for CD73, CD90, and CD105 and negativefor hematopoietic markers such as CD11b, CD19, CD34,CD45, and HLA-DR), although no specific marker hasbeen identified, and by their capacity to differentiate into
chondrocytes, osteoblasts, and adipocytes [24]. They are hypo-immunogenic as they express low levels of HLA class I anti-gens and no HLA class II antigens. Hence, an allogeneictransplantation of MSCs does not require HLA matching [25].MSCs can contribute to cartilage repair and protect it fromfurther degradation by two main characteristics relevant tothe therapeutic applications. First, they can differentiateinto chondrocytes in the presence of adequate environmentalfactors such as growth stimuli (TGF-b, FGF, and BMP),transcriptional factors (SOX9, RUNX-2), and physicalparameters. MSCs loaded on a three-dimensional scaffoldwith appropriate stimuli can induce cartilage repair [25]. Sec-ondly, MSCs may possess anti-inflammatory, anti-apoptotic,anti-fibrotic, pro-angiogenic, wound-healing, and immuno-suppressive properties. MSC-mediated immunomodulationis not a constitutive property and requires exposure to pro-inflammatory cytokines (TNF-a, interferon-gamma, IL-1).After activation, immunosuppressive properties are mainlymediated via the secretion of soluble paracrine mediatorssuch as growth factors and cytokines which can inhibit T-and B-cell proliferation and function. This paracrine activitymay prevent or delay the cartilage degradation, especially inearly stages of OA, by favoring a regenerative local environ-ment, regulating immune infiltration and inhibiting localinflammation, as well as stimulating the proliferation andthe differentiation of the remaining progenitors present inthe cartilage [25]. Indeed, it is suggested that MSCs may beused to stimulate the CPCs that are already present in therepair tissue of the OA joint and manipulate them towardcartilage regeneration via differentiation into chondrocytesproducing type II collagen, instead of transplanting cells tocreate cartilage de novo [23]. All these key properties makeMSCs attractive for being considered an innovative therapyfor OA.
Furthermore, Johnson et al. [26] recently demonstrated in amouse model that a small heterocyclic compound called kar-togenin can stimulate endogenous progenitor cells to differen-tiate and proliferate as cartilage-producing chondrocyteswithout any marker for hypertrophic chondrocytes or bonecells. This technique using endogenous stem cells seemsattractive, promoting a (perfect) genetic match and a targetedlocalization, and avoiding external stem-cell delivery.
Hence, whether by means of MSCs or of a chemical com-pound, stimulating the differentiation of one’s own CPCsmight also be a future therapeutic strategy for cartilage repairin OA.
2.4.1 Preclinical and clinical studies using stem cells
in cartilage regenerationThe proof of concept of therapeutic benefit of bone marrowand adipose tissue-derived MSCs (ASCs) has been demon-strated in vivo using experimental animal models of OA.Intra-articular injection of an autologous MSCs in goat jointssubjected to total meniscectomy and resection of the anteriorcruciate ligament resulted in regeneration of meniscal tissue
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2063
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

and in a delay of cartilage degradation [27]. Similarly, otherencouraging results of transplantation of MSCs in experimen-tal animal models of OA were reported [28,29]. In a mousemodel with early-stage collagenase-induced OA, a singleintra-articular injection of ASCs inhibited synovial inflamma-tion and cartilage destruction [30]. Safety and biodistributionof human ASCs after intra-articular injection have recentlybeen evaluated in severe combined immunodeficiency mice.Interestingly, 15% of these MSCs were detectable in the jointfor the first month and 1.5% engrafted on the long term, atleast 6 months [31].In humans, several studies using autologous MSCs deliv-
ered intra-articularly have been conducted in patients witharticular cartilage defects and OA [25]. However, transitioningthese strategies from filling a small defect in an otherwisehealthy cartilage to resurfacing an entire degraded joint sur-face in late-stage OA may be a real challenge. Hence, resultsfrom studies on cartilage defects should not be extrapolatedto OA [32].Although of limited evidence, some clinical studies
explored the therapeutic impact of stem cells in OA. At first,case reports described transplantation of MSCs through aninvasive approach (surgery) [33,34]. Later, introduction ofautologous MSCs within the joint by intra-articular injection,which represents a less invasive strategy, was reported tobe feasible and safe. Indeed, after intra-articular injection,MSCs are directly implanted in the injured site, which hasbeen suggested to avoid systemic distribution and toxicity aswell as to promote longer survival [31]. Davatchi et al. [35]
recently reported a reduction in pain after an intra-articularknee injection of autologous bone-marrow-derived MSCs(BM-MSCs) in four patients with moderate to severe kneeOA. Emadedin et al. [36] described a case series of six patientswith late knee OA who received an intra-articular injection ofBM-MSCs. Koh et al. [37] evaluated 18 patients with kneeOA who received intra-articular injections of autologousMSCs derived from the adipose synovium of the infrapatellarfat pad combined with PRP. The WOMAC and the VASscores were both significantly decreased after the intervention.However, the latter authors previously reported [38] no signifi-cant difference in the improvement in pain scores betweenknee OA patients who received MSCs plus PRP and thosewho received PRP alone. However, the lack of control groupsin case reports or case series on a small number of patients ham-pers any conclusion from being drawn on clinical efficiency.Stem-cell-based therapies are considered a promising
approach to delay OA progression, administered by intra-articular injection of exogenous stem cells or by harnessingendogenous stem cells for cartilage regeneration. Nevertheless,these preliminary results need to be confirmed with furtherstudies investigating not only the therapeutic potential ofMSCs, which is currently being explored in 14 Phase I/IItrials (Table 2), but also the biodistribution and survival ofMSCs after intra-articular injection as well as the safety ofsuch strategy. Cell therapy meets several challenges related
to cartilage. First, no specific differentiation factors for MSCchondrogenesis are clearly evidenced so far and this can limitthe clinical application of cell therapy. Moreover, to replacethe cartilage defect with a tissue having the same mechanicaland biological properties as native cartilage and achieve carti-lage-to-cartilage integration within the joint surface remain tobe optimized. To address this latter issue, several strategies arebeing developed to improve scaffolds combining MSCs, ade-quate chondrogenic factors, and various biomaterials. Anotherchallenge is to provide an adequate microenvironment ensur-ing the delivery of appropriate signals to stem cells, similar totheir initial niche, to maintain and stabilize their chondro-genic phenotype following implantation. Significant clinicalissues also remain to be addressed such as what type of stemcells, growth factors, and scaffolds should be used, in whichOA patients, and at which stage of the disease. For instance,the optimal MSC source for cell therapy in OA is still notclearly determined. The chondrogenic potential of ASCscompared with BM-MSCs remains controversial, some hav-ing suggested that ASCs may have the greatest chondrogenicpotential [39], while others argued for a lower chondrogenicpotential [40-42]. Nevertheless, ASCs are easier to obtain thanBM-MSCs [43]. Moreover, the influence on the regenerativepotential of stem cells of age, gender, and body weight, as obe-sity has been suggested to reduce the potential of ASCs [44],also have to be taken into account. Finally, the long-term safety of cell therapy also has to be evaluated, with regardto not only general hypothetical risks such as tumorigenesis orinfections, but also local complications such as ossification [40].Several Phase I and II trials are currently investigating thetherapeutic effect of MSCs (Table 2), which should hopefullyanswer some of these questions. Notably, the DMOAD struc-tural effect of such strategy will be assessed by MRI in most ofthe studies. Some clinical challenges and still unaddressedissues may currently temper immediate prospects of usingcell therapy in the near future in OA. Nevertheless, in ouropinion, cell therapy remains a promising emerging and inno-vative therapeutic strategy for OA, provided future researchfocuses on optimizing specific protocols for cartilage regener-ation, and on evaluating benefit-risk ratio, both at preclinicaland clinical levels, based on well-designed RCTs.
3. DMOADs targeting subchondral boneremodeling
Subchondral bone is at the interface between articular carti-lage and trabecular bone. Loss of integrity of the osteochon-dral junction in OA removes the barrier between intra-articular and subchondral compartments, and is associatedwith the invasion of articular cartilage by vascular channelsoriginating from the subchondral bone. A cross-talk betweensubchondral bone and cartilage as well as an increasedsubchondral turn-over was shown to play a key role in thedevelopment of OA and interest in subchondral bone as atherapeutic target is growing [45,46]. At present, the potential
C. Roubille et al.
2064 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

Table
2.Trials
evaluatingstem
cellsin
OA
ascu
rrentlylistedonwww.clinicaltrials.gov
[5],April2013.
Country
Intervention
Comparator
Condition
Outcomes
Phase
ClinicalTrials.
govidentifier
andstatus
Iran
IAIofautologous
BM-M
SCs
Case
group:MSCs
injectedatM1,M4after
boneaspirationand
placeboatM6afterfirst
injection
Intra-articularinjectionof
placebo
Controlgroup:placebo
injectedatM1,M4after
boneaspirationand
MSCsatM6afterfirst
injection
KneeOA
diagnosedby
MRI
n=40
Follow-upatweeks2,
6,M3andM6afterfirst
injection
I:WOMAC
+VAS,physical
improvementat2weeks
II:jointsw
elling,jointerythema,
deteriorationofjointfunction,
allergic
reactionatM3
MRIbefore
andatM6
Phase
IIrandomized
double-blind
efficacy
studyvs
placebo
NCT01504464
Completed
Malaysia
IAIofautologous
BM-M
SCsin
HA
(third
injectionofHA
ina
3-w
eeklyinjection
regim
en)
Intra-articularinjectionof
HA
(3-w
eeklyinjection
regim
en)
Mild
tomoderate
knee
OA
n=50
I:cartilagethickness/M
RIat
12months
II:VAS,IKDC
atM1,M3,M6,
M9,M12;progressionofOA
assessedbyX-rays
atM12
Phase
IIopen-label
randomized
efficacy
study
NCT01459640
Recruiting
India
IAIofautologous
BM-M
SCs
KneeOA
KLgrades3,4
n=10
I:WOMAC
pain,atM3,M6,
M12;adverseevents
atM12
II:changesin
MRIwithcartilage
mapping+clinicalim
provement
atM6,M12
Phase
I/II
open-labelsafety/
efficacy
study
NCT01152125
Enrollingby
invitation
Spain
IAIofBM-M
SCs
expandedexvivo
KneeOA
KLgrades2,
3,4
n=12
I:feasibility,safety
atM0,M3,
M6,M12,M24
Clinicalreview,questionnaires
II:efficacy
atM0,M3,M6,
M12,M24
Clinicalexploration,
questionnaires
MRIatM6,M12,M24
Phase
I/II
nonrandomized
open-labelsafety/
efficacy
study
NCT01183728
Ongoing
Spain
IAIofallogenicBM-M
SCs
(healthydonor)
expandedin
vivo
Intra-articularinjectionof
HA
KneeOA
KLgrades2,
3,4
n=30
I:adverseevents
Clinicalreview
andpain,
disability,QOLatM3,M6,M12
II:WOMAC
pain,SF36,QOLat
M0,M3,M6,M12
MRIatM0,M6,M12for
cartilagedegeneration
Phase
I/II
randomized
double-blindsafety/
efficacy
controlled
study
NCT01586312
Recruiting
Mexico
IAIofautologous
BM-M
SCs
Acetaminophen(oral)
KneeOA
KLgrades2,3
n=30
I:safety,WOMAC,KSS,SF36,
VASat1week
II:efficacy,WOMAC,KSS,VAS
at4weeksandM6
Phase
Irandomized
open-labelstudy
NCT01485198
Recruiting
Althoughanexhaustivelistingofthetrialswasaim
edfor,somemayhave
beeninvoluntarily
missed.
ACR:AmericanCollegeofRheumatology;
BM:bonemarrow;I:primary
outcomemeasures;
II:secondary
outcomemeasures;
IAI:intra-articularinjection;ICRS:InternationalCartilageRepairSociety
score;IKDC:
InternationalKneeDocumentationCommitteescore;IKS:InternationalKneeScore;HA:Hyaluronic
acid;HAQ:HealthAssessmentQuestionnaire;KL:
Kellgren-Lawrence;KOOS:Kneeinjury
andOsteoarthritisOutcome
Score;KSS:KneeSociety
RatingSystem;M:month;MRI:Magneticresonance
imaging;MSC:Mesenchym
alstem
cells;n=:numberofpatients;OA:osteoarthritis;
PBS:phosphate-bufferedsaline;PRP:platelet-rich
plasm
a;QOL:
qualityoflife;ROM:rangeofmotion;SAS:Short
ArthritisassessmentScale;SF-36:short
form
(36)healthsurvey;
TKA:totalkneearthroplasty;
VAS:VisualAnalogScale;WOMAC:Western
Ontarioand
McM
asterUniversitiesOsteoarthritisIndex.
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2065
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

Table
2.Trials
evaluatingstem
cellsin
OA
ascu
rrentlylistedonwww.clinicaltrials.gov[5],April2013(continued).
Country
Intervention
Comparator
Condition
Outcomes
Phase
ClinicalTrials.
govidentifier
andstatus
India
IAIofallogenicMSCs
exvivo
cultured+HA
Intra-articularinjectionof
placebo(plasm
alyte-A)+
HA
KneeOA
KLgrades2,3
n=60
I:adverseevents,safety
atM24
II:WOMAC,X-ray,
MRI
WORMS,VAS,intakeof
analgesics
atM24
Phase
IIrandomized
double-blindsafety/
efficacy
placebo-controlled
study
NCT01453738
Ongoing
Iran
IAIofautologousBM-
MSCs
Ankle
OA
n=6
I:safety
atM2,M6
II:pain
SF-36,function,MRI
defect
atM6
Phase
Iopen-label
study
NCT01436058
Completed
Malaysia
IAIofallogenicexvivo
culturedMSCs+HA
Intra-articularinjectionof
placebo
(plasm
alyte)+HA
KneeOA
KLgrades2,3
n=72
I:adverseeventatM12
II:WOMAC,X-ray,
VAS,MRI
WORMS,intakeofanalgesics
at
M12
Phase
IIrandomized
double-blind
placebo-controlled
study
NCT01448434
Ongoing
China
IAIofadipose-M
SCsat
M0,M1,M3
Intra-articularinjectionof
placebo(PBS)atM0,M1,
M3
KneeOA
diagnosed
withX-ray
n=120
Follow-upat6months
I:WOMAC
atM6
II:adverseevents,KSSatM6
Phase
I/II
open-labelstudy
NCT01809769
Ongoing
Korea
IAIofautologous
adipose-M
SCs
KneeOA
n=18
I:safety,WOMAC
atM24
II:MRI,VAS,KSS,X-ray,
histologicalevaluationsatM24,
arthroscopyatM6
Phase
I/II
nonrandomized
open-labelstudy
NCT01300598
Completed
USA
IAIofautologousadipose
MSCs+PRP
‘currentproven
diagnosisofkneeOA
withconsistent
symptomatology’;
n=500
I:VAS,QOL,
intakeof
analgesics,adverseevents
at
M3,M6
II:Xrays
atM6
Phase
I/II
open-labelstudy
NCT01739504
Recruiting
Spain
IAIautologousBM-
MSCsexpandedexvivo
KneeOA
KLgrades2,3
n=15
I:feasibility,safety
atM12
II:MRIatM6,M12,HAQ,
SF36atM3,M6,M12
Phase
I/II
open-labelstudy
NCT01227694
Ongoing
France
ADIPOA
IAIofautologous
adipose-M
SCs
KneeOA
ACRgrades3,
4(m
oderate
tosevere
medialand/orlateral
tibiofemoralkneeOA
withindicationofTKA)
n=18
I:adverseevents
atM12
II:WOMAC,ROM,MRI,SAS,
QOLatM12
Phase
Inonrandomized
open-labelstudy
NCT01585857
Recruiting
Althoughanexhaustivelistingofthetrialswasaim
edfor,somemayhave
beeninvoluntarily
missed.
ACR:AmericanCollegeofRheumatology;
BM:bonemarrow;I:primary
outcomemeasures;
II:secondary
outcomemeasures;
IAI:intra-articularinjection;ICRS:InternationalCartilageRepairSociety
score;IKDC:
InternationalKneeDocumentationCommitteescore;IKS:InternationalKneeScore;HA:Hyaluronic
acid;HAQ:HealthAssessmentQuestionnaire;KL:
Kellgren-Lawrence;KOOS:Kneeinjury
andOsteoarthritisOutcome
Score;KSS:KneeSociety
RatingSystem;M:month;MRI:Magneticresonance
imaging;MSC:Mesenchym
alstem
cells;n=:numberofpatients;OA:osteoarthritis;
PBS:phosphate-bufferedsaline;PRP:platelet-rich
plasm
a;QOL:
qualityoflife;ROM:rangeofmotion;SAS:Short
ArthritisassessmentScale;SF-36:short
form
(36)healthsurvey;
TKA:totalkneearthroplasty;
VAS:VisualAnalogScale;WOMAC:Western
Ontarioand
McM
asterUniversitiesOsteoarthritisIndex.
C. Roubille et al.
2066 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

DMOAD effect of anti-osteoporotic agents is currently beingexplored in OA [47].
After promising preclinical findings in OA animal models,particularly in early OA [48,49], clinical trials with bisphospho-nates in human OA have provided mixed results. In a cross-sectional study in postmenopausal women with knee OA,alendronate and estrogen therapy decreased the frequency ofbone marrow lesions (BMLs) detected by MRI, and alendro-nate use alone was associated with less severity of kneepain [50]. In a double-blind 1-year RCT of 284 patients withmild to moderate knee OA, risedronate decreased theWOMAC index but the reduction in JSN was found to benonsignificant compared to placebo [51]. In contrast, a2-year RCT found no significant effect of risedronate onWOMAC index or radiographic progression [52].
While most commonly used osteoporosis treatmentsincluding bisphosphonates act by inhibiting bone resorp-tion, strontium ranelate (SrRan) not only decreases boneresorption but also increases bone formation, and is cur-rently portrayed as the first potential DMOAD. Our groupfound that in vitro SrRan inhibited the resorptive propertiesof human subchondral bone osteoblasts by reducing the syn-thesis of some MMPs and modulating osteoprotegerin(OPG) and receptor activator of nuclear factor-kB ligand(RANKL) levels [53]. SrRan was also reported to stimulatecartilage matrix formation by human chondrocytes in vitro[54]. In vivo, in an experimental dog OA model, therapeuticdosages of SrRan significantly reduced the progression ofOA structural changes and inhibited the expression ofIL-1b and key proteases involved in cartilage degradation [55].Together, these data suggest that SrRan could target thethree major tissues involved in OA, namely the cartilage,subchondral bone, and synovium. In clinical studies, thedrug was found to reduce the radiological progression of spi-nal OA and back pain in women with osteoporosis and OAafter a 3-year treatment [56]. A recent 3-year double-blind,randomized, placebo-controlled Phase III trial, the SrRanEfficacy in Knee Osteoarthritis Trial (registrationISRCTN41323372), demonstrated that treatment withSrRan was associated with a significant protective effect onjoint structure and clinically relevant improvement of symp-toms in patients with knee OA [57]. In brief, the groupstreated with SrRan at both 1 and 2 g/day had less JSN andfewer radiological progressors compared to placebo. In addi-tion, patients treated with SrRan 2 g/day had a greaterreduction in WOMAC total score, as well as pain and phys-ical function subscores, than the placebo. A subgroup ofpatients from that trial was included in a study exploringthe effect of SrRan on cartilage volume loss and BMLs usingMRI [58]. Data showed that SrRan has a beneficial impact onboth cartilage and subchondral bone. As in vitro and in vivodata [53-55] demonstrated that SrRan has combined anti-catabolic and pro-anabolic properties, although speculative,SrRan could have a direct impact on cartilage as well as apositive effect on the cross-talk between subchondral bone
and cartilage. The loss of osteochondral integrity may exposethe cartilage to mediators released from subchondral chan-nels stimulating chondrocytes combined with a possibledirect effect on the chondrocytes and may partly accountfor the impact of SrRan on cartilage loss, in addition to itspreponderant effect on BMLs.
In this line of thought, Roux and Richette [59] recentlyproposed using BMLs seen on MRI as a relevant inclusioncriterion for clinical trials to explore the potential DMOADeffect of bone-acting agents instead of JSN, since the effectseen using X-rays might be irreversible or due to other fac-tors including meniscal extrusion. In a recent MRI study inknee OA patients, the significant reduction in pain andBMLs at 6 months after a single infusion of a zoledronicacid compared to placebo supports this proposal [60]. Hence,selecting patients with early OA and BMLs might be neces-sary in future studies to allow personalized and targetedOA therapy.
The data on the DMOAD properties of SrRan open thedoor to other promising bone pathways to target OA.Hence, targeting the OPG/RANKL system, which is criticalfor bone turn-over [46,61,62] appears interesting. RANKL,localized on osteoblasts, enhances osteoclastogenesis viainteraction with the receptor RANK, localized on osteo-clasts. OPG, produced by osteoblasts, is a secreted decoyreceptor for RANKL that serves as a physiological inhibitorof RANKL-driven osteoclast activities. Data showed thatOPG, RANK, and RANKL are also expressed and producedby human chondrocytes [63], and on human OA chondro-cytes the OPG/RANKL ratio was reduced, whereas theRANK/RANKL ratio was increased [63]. An imbalance inthe OPG/RANKL system, both in synovial fluid and serum,has been associated with OA severity [64]. The pro-resorptive effect of RANKL on the osteoclastogenesis processcould therefore be targeted by the use of either OPG or ananti-RANKL antibody. A study carried out in an experimen-tal mouse model of OA revealed, upon OPG administration,reduced cartilage degradation through an effect on trabecu-lar bone [65]. The potential of RANKL inhibition as aDMOAD is therefore interesting. Denosumab is a fullyhuman IgG2 monoclonal antibody that binds humanRANKL with a high affinity and which has been approvedfor use in postmenopausal osteoporosis [66] and in oncology.By analogy, in rheumatoid arthritis (RA), a Phase II RCTevaluated the effects of denosumab in addition to methotrex-ate (MTX) on structural damage. At 6 months, the increasein the MRI erosion score from baseline was lower in patientsreceiving 60 mg of denosumab and significance reached with180 mg of denosumab compared to placebo [67]. Denosu-mab has not yet been evaluated as a DMOAD.
Cathepsin K inhibitors may also be prospective DMOADs.In preclinical models, cathepsin K inhibition showed benefi-cial effects on protection of subchondral bone loss and againstcartilage degradation, and suggested reduced osteophyteformation [68].
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2067
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

The use of parathyroid hormone (PTH) as a DMOAD isalso conceivable but not yet evaluated. Recombinant humanPTH (1 -- 34), teriparatide, is a bone anabolic therapy usedfor osteoporosis. In a mouse meniscal/ligamentous injurymodel of knee OA, intermittent teriparatide systemic injec-tions decreased cartilage degeneration and induced matrixregeneration [69].Calcitonin also appears an option. In a Phase IIa RCT in
knee OA [70], oral calcitonin improved the Lequesne’s functionscore, whereas no difference was found in terms of pain reliefcompared to placebo. Moreover, the nasal form of calcitoninwas found to improve WOMAC total score and subscales(pain, stiffness, and function) [71]. This study was limited bythe absence of a control group. A 2-year Phase III trial inknee OA patients resulted in the symptom-modifying efficacyof oral calcitonin with a significant improvement in WOMACpain, function, and stiffness scores compared to placebo. Withregard to structural effects, oral calcitonin did not impact JSW,which was the primary endpoint, but significantly increasedcartilage volume compared to placebo, suggesting somestructure-modifying efficacy [72]. Another Phase III trial wasterminated early, probably due to an imbalance in prostate can-cer events in male subjects, as indicated on the Clinical Trialswebsite ([5]-NCT00704847). Of note, the European MedicinesAgency’s Committee for Medicinal Products for Human Userecommended in 2012 that calcitonin therapy should only beused for short-term periods because of an increased risk for can-cer of 0.7 -- 2.4% with long-term use, especially with intra-nasal calcitonin [73]. This could limit the potential use ofcalcitonin as a DMOAD.Vitamin D supplementation failed to reduce WOMAC
pain or cartilage volume loss as assessed by MRI comparedto placebo in a recent 2-year knee OA trial [74]. AnotherRCT evaluating whether vitamin D supplementation canslow knee cartilage loss assessed by MRI in OA patients isongoing [75].
4. Targeting inflammatory pathways
Several pro-inflammatory cytokines play a pivotal role in OApathogenesis. In particular, IL-1b and TNF-a are key cyto-kines favoring the degeneration of articular cartilage matrix,which makes them prime targets for OA treatment [76].IL-1b stimulates joint tissue to produce several proteasesinvolved in cartilage degradation and reduces the productionof matrix macromolecules such as aggrecan. It was recentlyreported that one IL-1 receptor antagonist (IL-1Ra) haplotypecould be associated with increased OA progression [77].Targeting IL-1b in OA seems a logical approach to slow thedisease progression, either directly with recombinant humanIL-1Ra, antibodies against the cytokine or its specific recep-tor, or through gene therapy as described further on. Intra-articular injection of recombinant human IL-1Ra was foundto be protective against the development of induced OA ina dog model and associated with a reduction in the expression
of some MMPs [78], providing evidence of a role of IL-1 incartilage degradation. However, after a promising pilot clini-cal study [79] reporting that intra-articular injection of ana-kinra (a recombinant non-glycosylated version of the humanIL-1Ra) was well tolerated in 13 OA patients and improvedpain as well as WOMAC total scores through 3 months,Chevalier et al. [80] performed a 12-week double-blind RCTassessing the efficacy of a single intra-articular injection of50 or 150 mg of anakinra versus placebo in 170 patientswith moderate-to-severe knee OA evaluated 4 weeks later.Anakinra was found to be safe and well tolerated. Patientstreated with anakinra showed no significant difference versusplacebo in score change from baseline to week 4 in theWOMAC index. However, significant short-term pain reliefwas evidenced at day 4 with the 150 mg anakinra injectioncompared to placebo. In this study, several factors couldhave negatively impacted the evaluation of treatment responsesuch as the inclusion of patients with low-level pain at base-line, the short half-life of the drug, suggesting that repeatedinjections are necessary to obtain a sustained symptomaticeffect, and a strong placebo effect. Of note, the structuraleffect of such strategy has not been investigated and theabsence of symptomatic effect does not mean absence of struc-tural effect. In contrast, 3 months of daily subcutaneous injec-tions of anakinra in three patients with erosive hand OAshowed improvement of pain and disability [81]. Additionally,a double-blind, placebo-controlled RCT using a systemicadministration of a monoclonal antibody (AMG 108)directed against the functional type 1 receptor of IL-1 demon-strated no significant difference in the level of pain at 6 weekswhen compared to the placebo [82]. However, a trend towardefficacy favoring AMG 108 was found in patients with high-baseline WOMAC pain [83]. Additionally, although no differ-ence in the incidence of serious infections related to thereduction of neutrophil count was seen compared to placebo,such biological therapy may expose patients to serious adverseevents [83].
Briefly, most of the studies so far have failed to show abeneficial symptomatic effect of IL-1b inhibition in OA.However, a Phase II proof-of-concept study assessing the effi-cacy and safety of subcutaneous injections of gevokizumab, apotent anti-IL-1b antibody, compared to placebo, in thetreatment of active erosive OA of the hand, is currently enroll-ing ([5]-NCT01683396). Another study on the safety andeffect on pain of a single intra-articular administration of can-akinumab, an anti-IL-1b monoclonal antibody, in patientswith knee OA is completed but not yet published ([5]-NCT01160822). Further studies evaluating the effect ofanti-IL-1b, especially of repeated intra-articular injectionsfor instance on a weekly basis, or of biologic agents with sus-tained half-life, are needed before burying the concept ofIL-1 inhibition in OA management [84]. Moreover, as men-tioned above, studies should also evaluate the effect not onlyon pain, but also on the joint structure, which is the targetbenefit that we are looking for.
C. Roubille et al.
2068 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

Another approach is the intra-articular injection of anautologous anti-proinflammatory cytokine product namedOrthokin, consisting of autologous conditioned serumobtained after incubation with glass beads to induce thesynthesis of various anti-inflammatory cytokines such asIL-1Ra, IL-4, IL-10, and IL-13. Two RCTs provided contro-versial results. On the one hand, the first reported study failedto show any difference between WOMAC and VAS painscore, and Knee injury and Osteoarthritis Outcome Score(KOOS) between Orthokin and saline over 12 months offollow-up [85]. On the other hand, the second demonstratedsignificantly better outcomes compared to saline andHA [86]. Further RCTs will be needed before consideringthis technique in routine practice.
Targeting TNF-a in OA with infliximab and adalimumabhas also been evaluated in a few trials providing conflictingresults. In an open-label pilot trial in 10 patients with erosiveOA of the hands, monthly intra-articular injections of inflix-imab reduced pain in all patients, without adverse reactionsafter 1 year of follow-up [87]. In contrast, another open-label study [88] in 12 patients with erosive hand OA whoreceived subcutaneous injections of adalimumab every2 weeks for 12 weeks showed no improvement in the num-ber of tender joints, grip strength, disability, pain, and globaldisease assessment. However, there was a statistically signifi-cant improvement in the number of swollen joints comparedto baseline. An RCT [89] including 60 patients with erosivehand OA treated with subcutaneous injections of adalimu-mab or placebo every 2 weeks for 12 months failed to dem-onstrate the control of structural damage on radiography assimilar percentages of patients in both groups had eitherdevelopment of new erosions or progression of existing ero-sions. There were also no significant differences betweengroups as regards pain and swelling on palpation, gripstrength, morning stiffness, pain severity score, and func-tion. However, palpable soft tissue swelling in interphalan-geal finger joints at baseline was identified as the strongestpredictor of erosive progression in these joints and adalimu-mab was found to halt the erosive progression compared toplacebo in these joints with destructive features on radiogra-phy and palpable effusion [89]. A Phase II study also showedthe lack of efficacy of adalimumab in hand OA [90]. A recentopen-label evaluation of adalimumab for 12 weeks in20 patients with knee OA and clinical effusion reportedthat 70% of the patients achieved an Osteoarthritis ResearchSociety International/Outcome Measures in RheumatologyClinical Trials response at week 12 [91]. In these studies, dif-ferences within results from erosive hand OA and knee OAcould reflect different disease phenotypes.
In conclusion, the current evidence does not support theuse of anti-cytokine therapy in all OA patients. Further trialsare needed, especially with respect to the selection of OApatients who may be speculated to benefit most from suchtherapy [92]. As for strategies targeting subchondral boneremodeling, selecting patients with early OA and synovitis
may be necessary in future studies for targeted and personal-ized OA management. However, the method for selectinginflammatory OA patients, whether only clinically basedwith synovial effusion of a swollen and painful joint, orMRI-based with radiological synovitis, remains to bedetermined.
Another pro-inflammatory cytokine, IL-6, could be oftherapeutic benefit to OA patients, but to our knowledge nostudy has yet assessed IL-6 inhibition in OA.
Emerging data suggest that activated macrophages mayplay a role in the maintenance and progression of OA [93].Once activated, macrophages express the functional form ofthe folate receptor-b (FR-b), and these FR-b macrophagesinfiltrate OA synovial tissues [94]. Therefore, molecules thatcould link the FR-b would specifically target the OA activatedmacrophages expressing FR-b. Thus, an attractive therapeutichypothesis would be to assess such a specifically designed mol-ecule able to modulate the function of the FR-b OA activatedmacrophages as a potential targeted DMOAD.
In OA, inflammation does not seem to affect only thejoints but may also be more systemic than previouslythought. In other words, a low-grade systemic inflammationmay play a critical role in OA pathogenesis. Indeed, recentstudies showing an increased risk of hand OA in obesepatients opened the door to a role of adipokines, inflamma-tory mediators released by adipose tissue. Associationsbetween adipokine concentration and OA severity [95] aswell as with local synovial tissue inflammation [96] havebeen reported. Moreover, OA affects aging patients with sig-nificant comorbidities such as atherosclerosis. It is thustempting to speculate that low-grade inflammation linksthese two diseases, as recently discussed for RA. Hence, atight control of inflammation is recommended to preventcardiovascular disease in RA. Whether immunomodulatoryagents would have beneficial effects on atherosclerosis inOA and RA is open to discussion. Furthermore, in non-arthritis patients, a randomized controlled CardiovascularInflammation Reduction Trial will investigate whetherlow-dose MTX (target dose 20 mg/week) compared to pla-cebo will reduce major vascular events among stable post-myocardial infarction patients with either type 2 diabetesor metabolic syndrome ([5]-NCT01594333). Additionally,another interesting study performed in mice genetically atrisk for Alzheimer’s disease showed that induced OA couldexacerbate and accelerate the development of neuroinflam-mation [97]. Based on these results, it was hypothesizedthat systemic low-grade inflammation during metabolicsyndrome (obesity, insulin resistance, lipid abnormalities,and hypertension) or aging could initiate and/or perpetuatethe OA process via inflammatory mediators such as adipo-kines and cytokines [98]. Once activated, OA joint cellsmight in turn release inflammatory mediators into thejoint and the blood stream, increasing the low-gradeinflammation, which can induce other conditions, such asAlzheimer’s and cardiovascular diseases. This systemic
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2069
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

low-grade inflammatory concept needs to be considered forfurther studies in OA.
5. Gene therapy in OA
Gene therapy is a promising specific and selective technologythat aims at transferring anti-arthritic genes to tissues by intra-articular injection using various different vectors and based ondirect, in vivo, and indirect, ex vivo, strategies, or implant.The advantages of gene therapy are to allow local and sus-tained delivery of therapeutic gene products to a small num-ber of target joints, and to avoid exposing non-target organsto the drug and subsequent adverse events [99].The induction of expression of anti-inflammatory cyto-
kines and growth factors using gene transfer may providean attractive approach for the treatment of OA. The first tar-get to be investigated in ex vivo gene therapy for both OAand RA was human IL-1Ra. It was shown that the localincrease of IL-1Ra production by intra-articular injectionof either transduced synovial cells [100] or a plasmid vectorand lipids [101] reduces the progression of OA-inducedlesions. The efficacy of gene transfer of IL-1Ra was also dem-onstrated in several RA animal models [102,103]. The firstclinical study of IL-1Ra gene transfer was performed byEvans et al. [104] by injection of autologous synovial fibro-blasts into metacarpophalangeal joints of nine femalepatients with RA scheduled for joint replacement surgeryshortly after transplantation. This study confirmed the feasi-bility and safety of such gene transfer into human joints [105]
and paved the way for further studies, especially in OA. Asproposed by Evans et al. [99], OA seems to be a better targetthan RA for intra-articular gene therapy, as it affects a lim-ited number of joints, without any extra-articular involve-ment. Another ex vivo gene delivery therapy in OA, namedTissueGene-C, based on retrovirally transduced allogenichuman chondrocytes expressing TGF-b, was assessed in aPhase I study in OA patients prior to total knee arthro-plasty [106]. There was no serious adverse event reported.Phase II studies are currently ongoing ([5]-NCT01671072and NCT01825811), exploring its effects on symptoms aswell as on cartilage as assessed by MRI.In vivo gene delivery therapy using adenoassociated virus
(AAV) vectors is emerging, given the advantages of AAV,which are non-integrating viruses that do not generate anydisease, and have low immunogenicity [99]. AAV may providean effective and safe in vivo gene-delivery techniquein OA [107], especially with self-complementing viruses(scAAV) [108]. Recently, Watson et al. [109] demonstrated, ina horse model, a successful transduction of the synovial fibro-blasts and of chondrocytes using scAAV vector encoding forhuman IL-1Ra injected in larger joints similar in size tohuman joints. Evans et al. [99] are currently developing anin vivo gene therapy using recombinant scAAV to deliverIL-1Ra cDNA into OA joints.
6. Perspectives: microRNAs and smallinterfering RNA-based therapeuticapproaches in OA
RNA interference and microRNAs (miRNAs) are excitingapproaches for the future treatment of OA by targetingcartilage repair genes and are expected to be part of the nextgeneration of OA therapeutic agents. Small interferingRNAs (siRNAs) can silence gene activity and specifically tar-get intracellular pathways. They can be delivered into thecell cytoplasm by mechanical means or using lipid-based for-mulations or expression vectors encoding short hairpinRNA [110]. However, siRNA-based therapy is still at an exper-imental stage in rheumatic diseases, especially in OA. As forgene therapy, the challenge of siRNA-based therapy is tolocally deliver the selective product to the specific cell typesin sufficient concentrations and in a sustained fashion toensure efficiency while avoiding not only off-target effectsbut also potential systemic toxicity [110]. Using OA animalmodels, two studies demonstrated positive effects of such anapproach [111,112]. Also proposed is to target monocytesthrough delivery of a combination of an anti-inflammatorysiRNA with an anti-osteoclastogenic siRNA to reduce bothsynovitis and bone resorption in RA and possibly in OA [110].
An additional field of research in OA concerns miRNAs,which are small noncoding RNA molecules naturally pro-duced by cells, which regulate posttranscriptional gene expres-sion [113]. The recognition that some miRNAs may play acentral role in cartilage and its dysregulation in OA providesa potential therapeutic target. Recently shown was that thedownregulation of miR-194 stimulated chondrogenic differ-entiation of human ASCs by increasing the expression ofits direct target gene SOX5, a key transcription factor forcartilage differentiation. Also found was that miR-194 wasupregulated in IL-1b-induced OA and associated with adecrease in SOX5 expression, suggesting that miR-194 andSOX5 could be targets for OA therapy [114]. Additionally,miR-140 was found decreased in human OA cartilage in com-parison to normal cartilage [115] and this miR is a direct regu-lator of the insulin-like growth factor-binding protein-5(IGFBP-5) [115] and ADAMTS5 expression. Transgenicmice overexpressing miR-140 in cartilage were resistant toantigen-induced arthritis [116]. Data also showed that anothermiR, miR-27a, indirectly downregulates both MMP-13 andIGFBP-5 in human OA chondrocytes [115]. Furthermore, inIL-1b-stimulated OA chondrocytes, miR-146a was found tobe upregulated [117]. Hence, it is suggested that administrationof both miR-140 and miR-146 into the joint might be anovel therapeutic target in early OA [118]. Other miRNAshave been found to act on different targets involved in OApathophysiology; however, more data are needed.
The challenge of in vivo applications is the difficulty ofdelivering siRNAs and miRNAs into cells such as chon-drocytes [118]. Nevertheless, even if there is currently onlylimited information on miRNA expression and function in
C. Roubille et al.
2070 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

the musculoskeletal system, proof-of-concept studies inpreclinical models can be expected in the near future [119].
7. Conclusion
Recent advances in the field of OA pathogenesis have eluci-dated the key roles of several pathways which can be targeted.A relevant step toward identifying new targets is to considerthat OA is not only a dynamic process involving the mainarticular tissues (cartilage, subchondral bone, and synovialmembrane) but also a systemic disease with low-grade inflam-mation. Promising emerging therapies include biologicalagents such as autologous stem cells, PRP, interleukin-1 inhib-itors, as well as bone remodeling modulators such as SrRan,and gene therapy. Future trials on DMOADs might succeedin bridging the gap between symptomatic drugs and surgery.
8. Expert opinion: toward targetedpersonalized medicine in OA
No DMOAD has yet been approved, whereas OA representsa huge unmet medical need worldwide in an aging popula-tion. Moreover, one should keep in mind that OA can alsooccur at younger ages, for example, in patients with inflam-matory rheumatic disorders or as a result of sports injuries.Based on the promising studies on different drugs and innova-tive techniques (e.g., MRI) to evaluate the joints, we can hopeand speculate that the treatment landscape of OA is about tochange, as it has in the past decade for RA and osteoporosis.The key concept to manage DMOAD development will beto target patients selectively according to the drug propertiesbecause OA, like other pathologies, is a heterogeneous diseaseand not all OA patients will respond to a sole drug. Indeed,for maximal benefit, a next step in DMOAD research is likelyto evaluate a drug in patients in whom specific features as wellas disease stage have been identified. It is unlikely that therewill be a sole powerful DMOAD molecule that will benefitthe general OA population, being effective on symptomsand on structural damage, which would be evaluated onlyusing radiographic changes (reduction of JSN). It seemsmore conceivable that future RCTs will demonstrate that amolecule has preferential DMOAD effects in some pheno-types of OA patients evidenced with sensitive techniquessuch as MRI, at a particular stage of the disease. This impliesthat future RCTs will need to select candidates in whom itwould be relevant to evaluate a DMOAD, focusing on a pre-determined population of OA patients. For instance, focusingon patients at higher risk of progression would probably bemore relevant while improving the probability of demonstrat-ing a beneficial effect.
It is our belief that for DMOAD development, MRIappears to be the most sensitive and reliable technique toselect patients for enrollment, to investigate the effect on car-tilage volume changes, BMLs, and synovitis in a sole exam,and to help identify predictive factors of treatment
responsiveness. Solutions to evaluate knee MR images haveprogressed at a rapid rate during the last decade and fullyautomated systems for quantifying cartilage, BMLs, osteo-phytes, synovial fluid, and bone volume and their changesover time have already been developed [120-123].
The therapeutic concepts aiming at targeting specific fea-tures of OA such as BMLs or synovitis, using locally deliveredchemical or biological agents, might seem contradictory to theconcept of a global therapeutic approach supporting systemicstrategies. Targeted and systemic strategies are not necessarilyconflicting but may be complementary and perhaps com-bined. Indeed, it is now well established that OA is not onlycartilage driven but rather a whole joint disease involvingother articular tissues. On a larger scale, OA often affectsseveral joints at the same time and therefore needs a moresystemic approach. Moreover, the role of low-grade inflam-mation, if proven, would argue for a global systemic manage-ment of OA. Thus, with the advent of DMOADs, physicianswould not treat a ‘disease’ but rather a ‘patient’ in acomprehensive way.
Another challenge in DMOAD development is to bothrelieve pain and arrest joint structural progression. It seemsboth desirable and desired (notably by the regulatory authori-ties), but unlikely, that a sole DMOAD will have this abilityto reduce pain in the very short term. A combination of twotherapeutic strategies would seem more conceivable, at least atthe beginning of the treatment, as one would expect that if aDMOAD can stop the disease progression, pain relief willensue. Further research to understand the underlying pathwayslinking pain, joint function, and structural progression in OA ismandatory. Moreover, safety concerns of long-term OA man-agement with DMOADs need to be taken into account.
For some of the agents discussed in the present review,adverse events, theoretical risks, or concerns have beendescribed, either in OA or in osteoporosis management:potential increased risk of cancer (very rare) with long-term use of calcitonin, atypical femoral fractures withbisphosphonates, hypocalcemia and risk of infections withdenosumab, cardiovascular, venous thromboembolism, andcutaneous adverse reactions with SrRan [73], in addition tothe well-known risks of TNF inhibitors such as infections,and the theoretical risks of infections with all intra-articular injections. Regarding MSC-based therapy, very fewadverse events have been reported to date. In a recent system-atic literature review [124], the most serious adverse events wereone infection and one pulmonary embolism probably relatedto bone marrow aspiration, and two unrelated tumors. How-ever, caution should be exercised regarding the inherenttheoretical risks of tumor development with such strategy.Increased pain and swelling were the main other adverseevents. Long-term safety studies for PRP are also needed,even if minimal risks of immunogenicity or tumor areexpected given that PRP is prepared from autologous serum.
In our opinion, SrRan is currently the most promisingagent with some evidence of DMOAD structural effect.
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2071
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

However, the European Medicines Agency recently recom-mended that the use of SrRan be restricted based on an anal-ysis of pooled data from randomized studies in around7500 postmenopausal women with osteoporosis, showing anincreased risk of myocardial infarction compared with placebo(relative risk 1.6; 95% CI 1.07 -- 2.38). No increased risk ofmortality was observed [125].DMOAD treatment is mostly aimed at an older population
than RA patients. A single future or emerging DMOAD willunlikely be appropriate for all OA patients, partly consideringthe influence of age, weight, disability, and other comorbid-ities such as cardiovascular diseases. Hence, it would seemmandatory to determine the long-term safety of new andemerging OA treatments and to evaluate benefit-risk ratio.With regard to SrRan, further RCTs specifically designedand sufficiently powered should assess not only the cardiovas-cular risk of OA patients treated with SrRan, but also the car-diovascular risk of OA patients in general, independent of thetreatments they receive, as there is less evidence in this condi-tion than in RA or psoriasis for example. In the meantime, thelegal restrictions and contraindications must be followed, butwe should not, however, definitively bury the concept ofSrRan as a DMOAD because of these concerns which needto be confirmed. More precisely, those adverse events shouldalso be counterbalanced with the wide and more frequentadverse events, including cardiovascular events, of currentlyused treatments in OA management such as nonsteroidalanti-inflammatory drugs, corticosteroids, and analgesics,especially in older patients.
Obviously, in the development of novel DMOADs, con-sideration should be given to the cost of such management,including the cost of a pre-therapeutic MRI to predictwhether the given DMOAD is likely to succeed, and thecost of the biologic agents, gene therapy, or stem cell therapydescribed above. OA is considerably more prevalent than RAand osteoporosis, and given the current lack of effective struc-tural treatment for OA, it is more than likely that physicianswill largely be tempted to use a newly available DMOADwhich will be demonstrated both effective and safe. Thisis likely to create a significant expense which cannot beneglected. On the other hand, the cost of the disease itself,both from a societal and individual patient perspective, isalso considerable including, in particular, indirect costsrelated to inactivity and reduced work efficacy as well as costsfrom surgical management. Therefore, developing adequate(targeted) DMOADs will be crucial to reduce the medicaland economic burden of such a major public health problem.
In conclusion, an exciting and promising new era inDMOAD development may be within reach, provided thatfuture clinical trials are sufficiently powered, systematicallydesigned, use the right evaluation techniques, and target theappropriate, more homogeneous, categories of OA patients.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of this manuscript.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Goldring MB. Chondrogenesis,
chondrocyte differentiation, and articular
cartilage metabolism in health and
osteoarthritis. Ther Adv
Musculoskelet Dis 2012;4:269-85
2. Jelic M, Pecina M, Haspl M, et al.
Regeneration of articular cartilage
chondral defects by osteogenic protein-1
(bone morphogenetic protein-7) in sheep.
Growth Factors 2001;19:101-13
3. Gavenis K, Heussen N,
Schmidt-Rohlfing B. Effects of low
concentration BMP-7 on human
osteoarthritic chondrocytes: comparison
of different applications. J Biomater Appl
2012;26:845-59
4. Hunter DJ, Pike MC, Jonas BL, et al.
Phase 1 safety and tolerability study of
BMP-7 in symptomatic knee
osteoarthritis. BMC Musculoskelet
Disord 2010;11:232
5. Available from: www.clinicaltrials.gov/
6. Moore EE, Bendele AM, Thompson DL,
et al. Fibroblast growth factor-18
stimulates chondrogenesis and cartilage
repair in a rat model of injury-induced
osteoarthritis. Osteoarthritis Cartilage
2005;13:623-31
7. McPherson R, Flechsenhar K, Hellot S,
et al. A randomized, double-blind,
placebo-controlled, multicenter study of
rhFGF18 administered intraarticularly
using single or multiple ascending doses
in patients with primary knee
osteoarthritis (OA), not expected to
require knee surgery within 1 year.
Osteoarthritis Cartilage
2011;19(Suppl 1):S35-S6
8. Pietrzak WS, An YH, Kang QK, et al.
Platelet-rich and platelet-poor plasma:
development of an animal model to
evaluate hemostatic efficacy.
J Craniofac Surg 2007;18:559-67
9. Anitua E, Andia I, Ardanza B, et al.
Autologous platelets as a source of
proteins for healing and tissue
regeneration. Thromb Haemost
2004;91:4-15
10. Dhillon RS, Schwarz EM, Maloney MD.
Platelet-rich plasma therapy - future or
trend? Arthritis Res Ther 2012;14:219
. This review details the rationale and
the pre-clinical and clinical evidence
supporting the potential of PRP in
treating muskuloskeletal conditions.
11. Patel S, Dhillon MS, Aggarwal S, et al.
Treatment with platelet-rich plasma is
more effective than placebo for knee
osteoarthritis: a prospective,
double-blind, randomized trial. Am J
Sports Med 2013;41:356-64
12. Taylor DW, Petrera M, Hendry M,
et al. A systematic review of the use of
platelet-rich plasma in sports medicine as
a new treatment for tendon and ligament
injuries. Clin J Sport Med
2011;21:344-52
13. Kon E, Mandelbaum B, Buda R, et al.
Platelet-rich plasma intra-articular
injection versus hyaluronic acid
viscosupplementation as treatments for
C. Roubille et al.
2072 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

cartilage pathology: from early
degeneration to osteoarthritis.
Arthroscopy 2011;27:1490-501
14. Kon E, Buda R, Filardo G, et al.
Platelet-rich plasma: intra-articular knee
injections produced favorable results on
degenerative cartilage lesions. Knee Surg
Sports Traumatol Arthrosc
2010;18:472-9
15. Sampson S, Reed M, Silvers H, et al.
Injection of platelet-rich plasma in
patients with primary and secondary knee
osteoarthritis: a pilot study. Am J Phys
Med Rehabil 2010;89:961-9
16. Sanchez M, Anitua E, Azofra J, et al.
Intra-articular injection of an autologous
preparation rich in growth factors for the
treatment of knee OA: a retrospective
cohort study. Clin Exp Rheumatol
2008;26:910-13
17. Filardo G, Kon E, Di Martino A, et al.
Platelet-rich plasma vs hyaluronic acid to
treat knee degenerative pathology: study
design and preliminary results of a
randomized controlled trial.
BMC Musculoskelet Disord 2012;13:229
18. Spakova T, Rosocha J, Lacko M, et al.
Treatment of knee joint osteoarthritis
with autologous platelet-rich plasma in
comparison with hyaluronic acid. Am J
Phys Med Rehabil 2012;91:411-17
19. Sanchez M, Fiz N, Azofra J, et al.
A randomized clinical trial evaluating
plasma rich in growth factors (PRGF-
Endoret) versus hyaluronic acid in the
short-term treatment of symptomatic
knee osteoarthritis. Arthroscopy
2012;28:1070-8
20. Martel-Pelletier J, Wildi LM,
Pelletier JP. Future therapeutics for
osteoarthritis. Bone 2012;51:297-311
.. A complete review of OA therapeutics
in development, especially regarding
pain, and including results of
preclinical trials.
21. Pelletier JP, Jovanovic D, Fernandes JC,
et al. Reduced progression of
experimental osteoarthritis in vivo by
selective inhibition of inducible nitric
oxide synthase. Arthritis Rheum
1998;41:1275-86
22. Hellio le Graverand MP, Clemmer RS,
Redifer P, et al. A 2-year randomised,
double-blind, placebo-controlled,
multicentre study of oral selective iNOS
inhibitor, cindunistat (SD-6010), in
patients with symptomatic osteoarthritis
of the knee. Ann Rheum Dis
2013;72:187-95
. This RCT evidenced no superiority of
cindunistat over placebo for rate of
change in JSN and no
symptomatic effect.
23. Muhammad H, Schminke B, Miosge N.
Current concepts in stem cell therapy for
articular cartilage repair. Expert Opin
Biol Ther 2013;13:541-8
. An interesting review about stem cell
therapy in cartilage repair, underlining
the potential of in situ chondrogenic
progenitor cells.
24. Pittenger MF, Mackay AM, Beck SC,
et al. Multilineage potential of adult
human mesenchymal stem cells. Science
1999;284:143-7
25. Gupta PK, Das AK, Chullikana A, et al.
Mesenchymal stem cells for cartilage
repair in osteoarthritis. Stem Cell
Res Ther 2012;3:25
26. Johnson K, Zhu S, Tremblay MS, et al.
A stem cell-based approach to cartilage
repair. Science 2012;336:717-21
.. The authors reported that a small
heterocyclic compound called
kartogenin can stimulate endogenous
progenitor cells to differentiate and
proliferate as cartilage-producing
chondrocytes without any marker for
hypertrophic chondrocytes or
bone cells.
27. Murphy JM, Fink DJ, Hunziker EB,
et al. Stem cell therapy in a caprine
model of osteoarthritis. Arthritis Rheum
2003;48:3464-74
28. Grigolo B, Lisignoli G, Desando G,
et al. Osteoarthritis treated with
mesenchymal stem cells on
hyaluronan-based scaffold in rabbit.
Tissue Eng Part C Methods
2009;15:647-58
29. Alfaqeh H, Norhamdan MY, Chua KH,
et al. Cell based therapy for osteoarthritis
in a sheep model: gross and histological
assessment. Med J Malaysia
2008;63(Suppl A):37-8
30. ter Huurne M, Schelbergen R, Blattes R,
et al. Antiinflammatory and
chondroprotective effects of intraarticular
injection of adipose-derived stem cells in
experimental osteoarthritis.
Arthritis Rheum 2012;64:3604-13
31. Toupet K, Maumus M, Peyrafitte JA,
et al. Long-term detection of human
adipose derived mesenchymal stem cells
after intra-articular injection in SCID
mice. Arthritis Rheum 2013;65:1786-94
. This study assessed the safety and the
biodistribution of intra-articular
injection of human adipose-derived
MSCs in severe combined
immunodeficiency (SCID) mice.
The authors reported that 15% of
these MSCs were detectable in the
joint for the first month and 1.5%
engrafted on the long-term, at least
6 months.
32. Diekman BO, Guilak F. Stem cell-based
therapies for osteoarthritis: challenges and
opportunities. Curr Opin Rheumatol
2013;25:119-26
33. Kuroda R, Ishida K, Matsumoto T, et al.
Treatment of a full-thickness articular
cartilage defect in the femoral condyle of
an athlete with autologous bone-marrow
stromal cells. Osteoarthritis Cartilage
2007;15:226-31
34. Wakitani S, Nawata M, Tensho K, et al.
Repair of articular cartilage defects in the
patello-femoral joint with autologous
bone marrow mesenchymal cell
transplantation: three case reports
involving nine defects in five knees.
J Tissue Eng Regen Med 2007;1:74-9
35. Davatchi F, Abdollahi BS,
Mohyeddin M, et al. Mesenchymal stem
cell therapy for knee osteoarthritis.
Preliminary report of four patients. Int J
Rheum Dis 2011;14:211-15
36. Emadedin M, Aghdami N, Taghiyar L,
et al. Intra-articular injection of
autologous mesenchymal stem cells in six
patients with knee osteoarthritis.
Arch Iran Med 2012;15:422-8
37. Koh YG, Jo SB, Kwon OR, et al.
Mesenchymal stem cell injections
improve symptoms of knee osteoarthritis.
Arthroscopy 2013;29:748-55
38. Koh YG, Choi YJ. Infrapatellar fat
pad-derived mesenchymal stem cell
therapy for knee osteoarthritis. Knee
2012;19:902-7
39. Estes BT, Diekman BO, Gimble JM,
et al. Isolation of adipose-derived stem
cells and their induction to a
chondrogenic phenotype. Nat Protoc
2010;5:1294-311
40. Filardo G, Madry H, Jelic M, et al.
Mesenchymal stem cells for the treatment
of cartilage lesions: from preclinical
findings to clinical application in
orthopaedics. Knee Surg Sports
Traumatol Arthrosc 2013;21:1717-29
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2073
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

41. Kim HJ, Im GI. Chondrogenic
differentiation of adipose tissue-derived
mesenchymal stem cells: greater doses of
growth factor are necessary. J Orthop Res
2009;27:612-19
42. Afizah H, Yang Z, Hui JH, et al.
A comparison between the chondrogenic
potential of human bone marrow stem
cells (BMSCs) and adipose-derived stem
cells (ADSCs) taken from the same
donors. Tissue Eng 2007;13:659-66
43. Jorgensen C, Noel D. Mesenchymal stem
cells in osteoarticular diseases.
Regen Med 2011;6:44-51
44. Roldan M, Macias-Gonzalez M,
Garcia R, et al. Obesity short-circuits
stemness gene network in human adipose
multipotent stem cells. FASEB J
2011;25:4111-26
45. Suri S, Walsh DA. Osteochondral
alterations in osteoarthritis. Bone
2012;51:204-11
46. Kwan Tat S, Lajeunesse D, Pelletier JP,
et al. Targeting subchondral bone for
treating osteoarthritis: what is the
evidence? Best Pract Res Clin Rheumatol
2010;24:51-70
. This review summarizes pathological
changes in the osteochondral bone
during OA and the rationale of
targeting this tissue in OA.
47. Lajeunesse D, Pelletier JP,
Martel-Pelletier J. Osteoporosis and
osteoarthritis: bone is the common battle
ground. Medicographia 2010;32:391-8
48. Pelletier JP, Troncy E, Bertaim T, et al.
Treatment with tiludronic acid helps
reduce the development of experimental
osteoarthritis lesions in dogs with
anterior cruciate ligament transection
followed by reconstructive surgery:
a 1-year study with quantitative magnetic
resonance imaging. J Rheumatol
2011;38:118-28
49. Moreau M, Rialland P, Pelletier JP, et al.
Tiludronate treatment improves
structural changes and symptoms of
osteoarthritis in the canine anterior
cruciate ligament model.
Arthritis Res Ther 2011;13:R98
50. Carbone LD, Nevitt MC, Wildy K,
et al. The relationship of antiresorptive
drug use to structural findings and
symptoms of knee osteoarthritis.
Arthritis Rheum 2004;50:3516-25
51. Spector TD, Conaghan PG,
Buckland-Wright JC, et al. Effect of
risedronate on joint structure and
symptoms of knee osteoarthritis: results
of the BRISK randomized, controlled
trial [ISRCTN01928173].
Arthritis Res Ther 2005;7:R625-33
52. Bingham CO III, Buckland-Wright JC,
Garnero P, et al. Risedronate decreases
biochemical markers of cartilage
degradation but does not decrease
symptoms or slow radiographic
progression in patients with medial
compartment osteoarthritis of the knee:
results of the two-year multinational knee
osteoarthritis structural arthritis study.
Arthritis Rheum 2006;54:3494-507
53. Tat SK, Pelletier JP, Mineau F, et al.
Strontium ranelate inhibits key factors
affecting bone remodeling in human
osteoarthritic subchondral bone
osteoblasts. Bone 2011;49:559-67
54. Henrotin Y, Labasse A, Zheng SX, et al.
Strontium ranelate increases cartilage
matrix formation. J Bone Miner Res
2001;16:299-308
55. Pelletier JP, Kapoor M, Fahmi H, et al.
Strontium ranelate reduces the
progression of experimental dog
osteoarthritis by inhibiting the expression
of key proteases in cartilage and of
IL-1beta in the synovium.
Ann Rheum Dis 2013;72:250-7
56. Bruyere O, Delferriere D, Roux C, et al.
Effects of strontium ranelate on spinal
osteoarthritis progression.
Ann Rheum Dis 2008;67:335-9
57. Reginster JY, Badurski J, Bellamy N,
et al. Efficacy and safety of strontium
ranelate in the treatment of knee
osteoarthritis: results of a double-blind,
randomised placebo-controlled trial.
Ann Rheum Dis 2013;72:179-86
.. This landmark RCT first demonstrated
that strontium ranelate has structural
DMOAD effects in knee OA as
assessed by X-rays.
58. Martel-Pelletier J, Roubille C,
Raynauld JP, et al. Disease modifying
effect of strontium ranelate in a phase III
knee osteoarthritis study (SEKOIA) using
quantitative MRI: reduction in bone
marrow lesion size associated with
cartilage protective effect. Osteoporos Int
2013;24:S51
. This study supported the structural
DMOAD effects of strontium ranelate
in knee OA on the reduction of
cartilage volume loss as assessed by
MRI, with a beneficial effect on both
cartilage and subchondral bone.
59. Roux C, Richette P. Impact of
treatments for osteoporosis on
osteoarthritis progression. Osteoporos Int
2012;23(Suppl 8):S881-3
60. Laslett LL, Dore DA, Quinn SJ, et al.
Zoledronic acid reduces knee pain and
bone marrow lesions over 1 year:
a randomised controlled trial.
Ann Rheum Dis 2012;71:1322-8
. This RCT demonstrated a significant
reduction in pain and BMLs as
assessed by MRI at six months after a
single infusion of a zoledronic acid in
knee OA patients, and supports the use
of MRI to select patients in OA trials
to evidence DMOAD effect.
61. Tat SK, Pelletier JP, Velasco CR, et al.
New perspective in osteoarthritis: the
OPG and RANKL system as a potential
therapeutic target? Keio J Med
2009;58:29-40
62. Kwan Tat S, Pelletier JP, Lajeunesse D,
et al. The differential expression of
osteoprotegerin (OPG) and receptor
activator of nuclear factor kappaB ligand
(RANKL) in human osteoarthritic
subchondral bone osteoblasts is an
indicator of the metabolic state of these
disease cells. Clin Exp Rheumatol
2008;26:295-304
63. Kwan Tat S, Amiable N, Pelletier JP,
et al. Modulation of OPG, RANK and
RANKL by human chondrocytes and
their implication during osteoarthritis.
Rheumatology (Oxford)
2009;48:1482-90
64. Pilichou A, Papassotiriou I,
Michalakakou K, et al. High levels of
synovial fluid osteoprotegerin (OPG) and
increased serum ratio of receptor
activator of nuclear factor-kappa B ligand
(RANKL) to OPG correlate with disease
severity in patients with primary knee
osteoarthritis. Clin Biochem
2008;41:746-9
65. Kadri A, Ea HK, Bazille C, et al.
Osteoprotegerin inhibits cartilage
degradation through an effect on
trabecular bone in murine experimental
osteoarthritis. Arthritis Rheum
2008;58:2379-86
66. Josse R, Khan A, Ngui D, et al.
Denosumab, a new pharmacotherapy
option for postmenopausal osteoporosis.
Curr Med Res Opin 2013;29:205-16
C. Roubille et al.
2074 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.
67. Cohen SB, Dore RK, Lane NE, et al.
Denosumab treatment effects on
structural damage, bone mineral density,
and bone turnover in rheumatoid
arthritis: a twelve-month, multicenter,
randomized, double-blind,
placebo-controlled, phase II clinical trial.
Arthritis Rheum 2008;58:1299-309
68. Hayami T, Zhuo Y, Wesolowski GA,
et al. Inhibition of cathepsin K reduces
cartilage degeneration in the anterior
cruciate ligament transection rabbit and
murine models of osteoarthritis. Bone
2012;50:1250-9
69. Sampson ER, Hilton MJ, Tian Y, et al.
Teriparatide as a chondroregenerative
therapy for injury-induced osteoarthritis.
Sci Transl Med 2011;3:101ra93
70. Manicourt DH, Azria M, Mindeholm L,
et al. Oral salmon calcitonin reduces
Lequesne’s algofunctional index scores
and decreases urinary and serum levels of
biomarkers of joint metabolism in knee
osteoarthritis. Arthritis Rheum
2006;54:3205-11
71. Esenyel M, Icagasioglu A, Esenyel CZ.
Effects of calcitonin on knee
osteoarthritis and quality of life.
Rheumatol Int 2013;33:423-7
72. Karsdal MA, Alexandersen P, John MR,
et al. Oral calcitonin demonstrated
symptom-modifying efficacy and
increased cartilage volume: results from a
2-year Phase 3 trial in patients with
osteoarthritis of the knee.
Osteoarthritis Cartilage 2011;19:S35
73. Reginster JY, Pelousse F, Bruyere O.
Safety concerns with the long-term
management of osteoporosis.
Expert Opin Drug Saf 2013;12:507-22
. This is a recent and exhaustive review
of the adverse events and safety
concerns of some of the anti-bone
remodeling treatments used in OA.
74. McAlindon T, LaValley M, Schneider E,
et al. Effect of vitamin D
supplementation on progression of knee
pain and cartilage volume loss in patients
with symptomatic osteoarthritis:
a randomized controlled trial. JAMA
2013;309:155-62
. This 2-year RCT failed to show a
beneficial effect of vitamin D on
symptoms and cartilage volume loss
in OA.
75. Cao Y, Jones G, Cicuttini F, et al.
Vitamin D supplementation in the
management of knee osteoarthritis: study
protocol for a randomized controlled
trial. Trials 2012;13:131
76. Kapoor M, Martel-Pelletier J,
Lajeunesse D, et al. Role of
proinflammatory cytokines in the
pathophysiology of osteoarthritis.
Nat Rev Rheumatol 2011;7:33-42
77. Wu X, Kondragunta V, Kornman KS,
et al. IL-1 receptor antagonist gene as a
predictive biomarker of progression of
knee osteoarthritis in a population
cohort. Osteoarthritis Cartilage
2013;21:930-8
78. Caron JP, Fernandes JC,
Martel-Pelletier J, et al.
Chondroprotective effect of intraarticular
injections of interleukin-1 receptor
antagonist in experimental osteoarthritis.
Suppression of collagenase-1 expression.
Arthritis Rheum 1996;39:1535-44
79. Chevalier X, Giraudeau B, Conrozier T,
et al. Safety study of intraarticular
injection of interleukin 1 receptor
antagonist in patients with painful knee
osteoarthritis: a multicenter study.
J Rheumatol 2005;32:1317-23
80. Chevalier X, Goupille P, Beaulieu AD,
et al. Intraarticular injection of anakinra
in osteoarthritis of the knee:
a multicenter, randomized, double-blind,
placebo-controlled study.
Arthritis Rheum 2009;61:344-52
. This RCT showed no symptomatic
efficacy of a single intra-articular
injection of anakinra in knee OA.
81. Bacconnier L, Jorgensen C, Fabre S.
Erosive osteoarthritis of the hand: clinical
experience with anakinra.
Ann Rheum Dis 2009;68:1078-9
82. Cohen SB, Proudman S, Kivitz AJ, et al.
A randomized, double-blind study of
AMG 108 (a fully human monoclonal
antibody to IL-1R1) in patients with
osteoarthritis of the knee.
Arthritis Res Ther 2011;13:R125
83. Chevalier X, Conrozier T, Richette P.
Desperately looking for the right target
in osteoarthritis: the anti-IL-1 strategy.
Arthritis Res Ther 2011;13:124
84. Martel-Pelletier J, Pelletier JP.
Osteoarthritis: a single injection of
anakinra for treating knee OA?
Nat Rev Rheumatol 2009;5:363-4
85. Yang KG, Raijmakers NJ, van Arkel ER,
et al. Autologous interleukin-1 receptor
antagonist improves function and
symptoms in osteoarthritis when
compared to placebo in a prospective
randomized controlled trial.
Osteoarthritis Cartilage 2008;16:498-505
86. Baltzer AW, Moser C, Jansen SA, et al.
Autologous conditioned serum
(Orthokine) is an effective treatment for
knee osteoarthritis.
Osteoarthritis Cartilage 2009;17:152-60
87. Fioravanti A, Fabbroni M, Cerase A,
et al. Treatment of erosive osteoarthritis
of the hands by intra-articular infliximab
injections: a pilot study. Rheumatol Int
2009;29:961-5
88. Magnano MD, Chakravarty EF,
Broudy C, et al. A pilot study of tumor
necrosis factor inhibition in erosive/
inflammatory osteoarthritis of the hands.
J Rheumatol 2007;34:1323-7
89. Verbruggen G, Wittoek R,
Vander Cruyssen B, et al. Tumour
necrosis factor blockade for the treatment
of erosive osteoarthritis of the
interphalangeal finger joints: a double
blind, randomised trial on structure
modification. Ann Rheum Dis
2012;71:891-8
90. Chevalier X, Ravaud P, Maheu E, et al.
A randomized, multicentre, double blind,
placebo-controlled trial of antiTNFalpha
(adalimumab) in refractory hand
osteoarthritis: the Dora study.
Arthritis Rheum 2012;64:S1042
91. Maksymowych WP, Russell AS, Chiu P,
et al. Targeting tumour necrosis factor
alleviates signs and symptoms of
inflammatory osteoarthritis of the knee.
Arthritis Res Ther 2012;14:R206
92. Chevalier X, Eymard F, Richette P.
Biologic agents in osteoarthritis: hopes
and disappointments.
Nat Rev Rheumatol 2013;9:400-10
93. Bondeson J, Wainwright SD, Lauder S,
et al. The role of synovial macrophages
and macrophage-produced cytokines in
driving aggrecanases, matrix
metalloproteinases, and other destructive
and inflammatory responses in
osteoarthritis. Arthritis Res Ther
2006;8:R187
94. Tsuneyoshi Y, Tanaka M, Nagai T, et al.
Functional folate receptor beta-expressing
macrophages in osteoarthritis synovium
and their M1/M2 expression profiles.
Scand J Rheumatol 2012;41:132-40
95. Yusuf E, Ioan-Facsinay A, Bijsterbosch J,
et al. Association between leptin,
adiponectin and resistin and long-term
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2075
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

progression of hand osteoarthritis.
Ann Rheum Dis 2011;70:1282-4
96. de Boer TN, van Spil WE,
Huisman AM, et al. Serum adipokines in
osteoarthritis; comparison with controls
and relationship with local parameters of
synovial inflammation and cartilage
damage. Osteoarthritis Cartilage
2012;20:846-53
97. Kyrkanides S, Tallents RH, Miller JN,
et al. Osteoarthritis accelerates and
exacerbates Alzheimer’s disease pathology
in mice. J Neuroinflammation
2011;8:112
98. Berenbaum F. Osteoarthritis as an
inflammatory disease (osteoarthritis is not
osteoarthrosis!). Osteoarthritis Cartilage
2013;21:16-21
99. Evans CH, Ghivizzani SC, Robbins PD.
Arthritis gene therapy and its tortuous
path into the clinic. Transl Res
2013;161:205-16
.. This is an excellent state-of-the-art
review on gene therapy in arthritis.
100. Pelletier JP, Caron JP, Evans C, et al. In
vivo suppression of early experimental
osteoarthritis by interleukin-1 receptor
antagonist using gene therapy.
Arthritis Rheum 1997;40:1012-19
101. Fernandes J, Tardif G, Martel-Pelletier J,
et al. In vivo transfer of
interleukin-1 receptor antagonist gene in
osteoarthritic rabbit knee joints:
prevention of osteoarthritis progression.
Am J Pathol 1999;154:1159-69
102. Bakker AC, Joosten LA, Arntz OJ, et al.
Prevention of murine collagen-induced
arthritis in the knee and ipsilateral paw
by local expression of human
interleukin-1 receptor antagonist protein
in the knee. Arthritis Rheum
1997;40:893-900
103. Otani K, Nita I, Macaulay W, et al.
Suppression of antigen-induced arthritis
in rabbits by ex vivo gene therapy.
J Immunol 1996;156:3558-62
104. Evans CH, Robbins PD, Ghivizzani SC,
et al. Clinical trial to assess the safety,
feasibility, and efficacy of transferring
a potentially anti-arthritic cytokine gene
to human joints with rheumatoid
arthritis. Hum Gene Ther
1996;7:1261-80
105. Evans CH, Robbins PD, Ghivizzani SC,
et al. Gene transfer to human joints:
progress toward a gene therapy of
arthritis. Proc Natl Acad Sci USA
2005;102:8698-703
106. Ha CW, Noh MJ, Choi KB, et al. Initial
phase I safety of retrovirally transduced
human chondrocytes expressing
transforming growth factor-beta-1 in
degenerative arthritis patients.
Cytotherapy 2012;14:247-56
107. Gouze E, Gouze JN, Palmer GD, et al.
Transgene persistence and cell turnover
in the diarthrodial joint: implications for
gene therapy of chronic joint diseases.
Mol Ther 2007;15:1114-20
108. Kay JD, Gouze E, Oligino TJ, et al.
Intra-articular gene delivery and
expression of interleukin-1Ra mediated
by self-complementary adeno-associated
virus. J Gene Med 2009;11:605-14
109. Watson RS, Broome TA, Levings PP,
et al. scAAV-mediated gene transfer of
interleukin-1-receptor antagonist to
synovium and articular cartilage in large
mammalian joints. Gene Ther
2013;20(6):670-7
110. Apparailly F, Jorgensen C. siRNA-based
therapeutic approaches for rheumatic
diseases. Nat Rev Rheumatol
2013;9:56-62
111. Santangelo KS, Bertone AL. Effective
reduction of the interleukin-1beta
transcript in osteoarthritis-prone guinea
pig chondrocytes via short hairpin
RNA mediated RNA interference
influences gene expression of mediators
implicated in disease pathogenesis.
Osteoarthritis Cartilage 2011;19:1449-57
112. Chen LX, Lin L, Wang HJ, et al.
Suppression of early experimental
osteoarthritis by in vivo delivery of the
adenoviral vector-mediated
NF-kappaBp65-specific siRNA.
Osteoarthritis Cartilage 2008;16:174-84
113. Bartel DP. MicroRNAs: genomics,
biogenesis, mechanism, and function.
Cell 2004;116:281-97
114. Xu J, Kang Y, Liao WM, et al.
MiR-194 regulates chondrogenic
differentiation of human adipose-derived
stem cells by targeting Sox5. PLoS One
2012;7:e31861
115. Tardif G, Hum D, Pelletier JP, et al.
Regulation of the IGFBP-5 and
MMP-13 genes by the microRNAs
miR-140 and miR-27a in human
osteoarthritic chondrocytes.
BMC Musculoskelet Disord 2009;10:148
116. Miyaki S, Sato T, Inoue A, et al.
MicroRNA-140 plays dual roles in both
cartilage development and homeostasis.
Genes Dev 2010;24:1173-85
117. Yamasaki K, Nakasa T, Miyaki S, et al.
Expression of MicroRNA-146a in
osteoarthritis cartilage. Arthritis Rheum
2009;60:1035-41
118. Miyaki S, Asahara H. Macro view of
microRNA function in osteoarthritis.
Nat Rev Rheumatol 2012;8:543-52
119. Pers YM, Jorgensen C. MicroRNA in
2012: Biotherapeutic potential of
microRNAs in rheumatic diseases.
Nat Rev Rheumatol 2013;9:76-8
120. Dodin P, Abram F, Pelletier JP, et al.
A fully automated system for
quantification of knee bone marrow
lesions using MRI and the Osteoarthritis
Initiative cohort. J Biomed
Graph Comput 2013;3:51-65
121. Dodin P, Martel-Pelletier J, Pelletier JP,
et al. A fully automated human knee 3D
MRI bone segmentation using the ray
casting technique. Med Biol
Eng Comput 2011;49:1413-24
122. Dodin P, Pelletier JP, Martel-Pelletier J,
et al. Automatic human knee cartilage
segmentation from 3D magnetic
resonance images. IEEE Trans
Biomed Eng 2010;57:2699-711
123. Li W, Abram F, Pelletier JP, et al. Fully
automated system for the quantification
of human osteoarthritic knee joint
effusion volume using magnetic
resonance imaging. Arthritis Res Ther
2010;12:R173
. [120-123]: These four papers point to
important advances in knee MRI with
the development of fully automated
systems for the quantification of
bone marrow lesions, bone and
osteophytes, cartilage volume, and
synovial fluid.
124. Peeters CM, Leijs MJ, Reijman M, et al.
Safety of intra-articular cell-therapy with
culture-expanded stem cells in humans:
a systematic literature review.
Osteoarthritis Cartilage
2013;doi:10.1016/j.joca.2013.06.025
125. Available from: http://www.ema.europa.
eu/ema/index.jsp?curl=pages/
news_and_events/news/2013/04/
news_detail_001774.
jsp&mid=WC0b01ac058004d5c1
C. Roubille et al.
2076 Expert Opin. Pharmacother. (2013) 14 (15)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.

AffiliationCamille Roubille1, Jean-Pierre Pelletier2 &
Johanne Martel-Pelletier†3
†Author for correspondence1Research Fellow,
University of Montreal Hospital Research Centre
(CRCHUM), Osteoarthritis Research Unit,
1560 Sherbrooke Street East, Montreal,
Quebec, Canada2Professor of Medicine,
University of Montreal; Director,
Rheumatic Diseases Unit,
Department of Medicine,
University of Montreal;
Head, Arthritis Division, University of Montreal
Hospital Centre (CHUM);
Head, Chair in Osteoarthritis of the University of
Montreal; Director, Osteoarthritis Research Unit,
University of Montreal Hospital Research Centre
(CRCHUM), 1560 Sherbrooke Street East,
Montreal, Quebec, Canada3Professor of Medicine,
University of Montreal; Head, Chair in
Osteoarthritis of the University of Montreal;
Director, Osteoarthritis Research Unit,
University of Montreal Hospital Research Centre
(CRCHUM), 1560 Sherbrooke St. East, Y-2616,
Montreal, Quebec, H2L 4M1,
Canada
Tel: +514 890 8000, ext. 26658;
Fax: +514 412 7583;
E-mail: [email protected]
New and emerging treatments for osteoarthritis management
Expert Opin. Pharmacother. (2013) 14(15) 2077
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 01
/30/
14Fo
r pe
rson
al u
se o
nly.