neuropeptides in the arthritic tmj and symptoms and signs from the
TRANSCRIPT

Neuropeptides in the Arthritic TMJ and Symptoms andSigns From the Stomatognathic System With SpecialConsideration to Rheumatoid Arthritis
Anna Appelgren, DDSGraduate StudentDepartment of Clinical Oral PhysiologyFaculty of Dentistry
Björn Appalgren, DDS, PhD. MAAssociate ProfessorDepartment of Clinical Oral PhysiologyFaculty of Dentistryand Department of Physiology and
Pharmacology
Sigvard Kopp, DDS. PhDProfessorDepartment of Clinical Oral PhysiologyFaculty of Dentistry
Thomas Lundeberg, MD, PhDAssociate ProfessorDepartment of Physiology and
Pharmacology
Karolinska InstituteHuddinge, Sweden
Elvar Theodorsson, MD. PhDProfessorDepartment of Clinical ChemistryKarolinska HospitalHuddinge. Sweden
Corresptsndence to:Dr Anna AppelgrenDepartment of Clinical Oral PhysiologyFaculty of DentistryKarolinska InstituteBox 4064S-141 04 Huddinge. Sweden
Tbe contribution of the nervous system to the patbopbysiology ofrheumatoid artbritis bas been proposed to be mediated by certainneuropeptides. Neuropeptide V, calcitonin gene-related peptide,substance P, and neurokinin A are considered modulators ofinflammatory ¡oint disease. Parameters of pain, as well as occlusalsigns of tissue destruction from the arthritic TMj and tbe corre-sponding neuropeptide concentrations in TMJ synovial fluid, wereinvestigated in patients witb various inflammatory joint diseases.Tbe patients with rheumatoid artbritis were also examined in aseparate diagnostic group. Visual analog scale, palpatory tender-ness, maximal voluntary moutb opening, and anterior open bitewere correlated to neuropeptide-like immunoreactwities of tbeabove four neuropeptides. It was found tbat bigh concentrations ofcalcitonin gene-related peptide and neuropeptide Y in TMJ fluidare associated witb pain, impairment of mandibular mobility, andocclusal signs of TMJ destruction in patients witb rheumatoidarthritis. Tbe results indicated neuropeptide involvement inrbeumatoid artbritis, proposing a potentiation of tbe symptomsand signs by tbe inflammatory action of calcitonin gene-relatedpepiide and neuropeptide Y.
J OROFACIAI. PAIN \995-.,9-.2l5-225.
key words: neuropeptides, rheumatoid arthritis,temporomandibular joint, pain, occlusion
Since the classic axon-reflex experiments performed by Lewis in1936, indicating release of proinflammatory substances fromperipheral terminals of primary afférents, the concept of neu-
rogenic inflammation has been the focus of intense research.Dysregulation of the immnne system has been considered responsi-ble for the pathogenesis of inflammation. The immune system, sup-posedly the driving force of the pathogenesis of mflammation, can-not be isolated from the influence of other body components in aninflammatory process such as rheumatoid arthritis (RA). Studiesduring the last decade have implicated the role of the central andperipheral nervous system in the development of RA.' The contri-bution of the nervous system to the pathophysiology of RA hasbeen proposed to be mediated by certain neuropeptides.- The pre-sent study deals with the neuropeptides substance P (SP), calcitoningene-related peptide (CGRP), neurokinin A (NKA), and neuropep-tide Y (NPY).
Joumsl of Orofacial Pain 2 1 5

Appelgren et al
Substance P is found in small-diameter, unmyeii-nated sensory neurons and has been sbown toamplif)' experimental adjuvant artbritis in rats,' roactivate macrophages in tbe pannus to secreteprosraglandins," and to activate synoviocytes tosecrete prostaglandin E2 (PGE.1) and collagenase.*Substance P also bas local effects sucb as vasodi-latation, increased capillary permeability, andrelease of histamine from mast cells."'Like SP,CGRP is found in C fibers,̂ and CGRP may coop-erate witb SP in mediating local reflex reactionsdue ro activation of sensory nerves. In addition,CGRP has a strong vasodilatory effect in jointsand muscles and is several times more porent as avasodilator than is SP.' Sensory nerve endings ofseveral organs contain NKA, which is known tobe released into the spinal cords of cats on induc-tion of experimental knee joint arthritis.'" How-ever, the involvement of NKA in the local develop-ment of arthritis is unknown and warrants furtherinvestigation. Neurnpeptide Y is produced withnorepinephrine in certain efferent sympatheticnerve fibers" and has a srrong and long-srandmgvasoconstrictive effect on both the arterial andvenous side of vessels such as those of skeletalmuscles. Increased activity in efferent nerves of thesympathetic system has been associated with anincrease in joint inflammation and destruction.''Sympathetic vasoconstriction, in the acutelyinflamed rat knee joints, has been replaced by aneuropeptide-mediated vasodilator response,enhancing responsiveness ro SP. In this case, ir hasbeen proposed that CCRP contributes to tbehyperemia of inflamed joints." Tbus, neuropep-tides have been suggested as neurogenic mediatorsin rhe local neural mechanisms involved in theinflammatory process.
The neuropeptides SP, CGRP, NPY, and NKAare present in nerves of human synovium.'"'Decreased peptidergic innervarion in rhe synovialtissue of patients wirh RA has raised the quesrionwhether reduced neuropeptide immunoreactivity inrheumatoid synovium is a result of an increasedrelease into the synovial fluid or of ihe desrrticrionof nerve fibers."-" High concentrations of SP werefound in rhe synovial fluid from knee joinrs ofpatients with RA compared to that nf patients withosteoarthritis, who had higher level of SP-likeimmunoreactivities in the synovial tissue."^ BothCGRP and NPY have been found in higher concen-trations in the knee joint of arthritic parients thanin control subjects wirh degenerative or traumaticjoint disease.'"-" In fluid from human arthiiric rem-poromandibular joints (TMJs), the levels of SP,CGRP, NKA, and NPY exceeded tbose in plasma.
and CGRP and NPY were correlated to tbe intra-articular temperature, stipulating neuropeptid^"mediated microcirculatory changes.'""
The documentation of the pathophysiology "*"RA in the TMJ is scarce, althcmgh the TM.I, «henexposed to inflammation, has characteristics simi-lar to other arthritic joints. Pain, reduced mobil'ty,and tissue destruction are also main featuns ofTMJ arthritis. Formation of a rheumatoid pannusof vascular granulation tissue," which destroysarticular cartilage and bone, is a severe conse-quence of chronic RA in the TMJ. Immunoreactivefibers for SP, CGRP, and NPY bave been found intbe TMJ capsule of the monkey and rat.^'-" Tbemost prominent clinical signs of arthritis in thestomatognatbic system are an anterior open bite,reduced mandibular mobiliry, and tenderness ofthe TMJ laterally and posteriorly.-' Sources andeffects of neuronal mediators in the pathogenesisof inflammation and pain presenr a complexitythat must be understood to improve diagnosticsand treatment of the acute and chronic phases ofthe inflammatory process.
The relation between the severity of the chnicalsigns of arthritis in the TMJ and the presence ofneuropeptides in rhe synovial fluid has not yetbeen established. The aim of this study was there-fore to investigate wherher the levels of SP, CGRP,NPY, and NKA in the synovial fluid of thearthritic TMJ were correlated ro pain, decreasedmandibular mobiliry, and occlusal signs of jointdestruction in rhe sromatognathic system.
Materials and Methods
Patients
This study comprised 46 TMJs of 23 patients (19women and 4 men) with signs and symptoms ofTMJ arthritis and wirh a median age of 50 years(mean - 46.9). The parienrs vifirh RA were of spe-cial inreresr and were allocared inro a separategroup, rhe RA group, while the resr of the patients,having inflammatory |omt diseases other than RA,formed rhe non-rheumaroid arthriris (NRA)group. The RA group comprised 14 patients: ninewirh posirive rheumaroid factors and five withnegarive rheumatoid factors. The NRA groupcomprised nine patients: two with ankylosingspondyliris (AS); one wirh psoriatic arthroparhy(PA); two with systemic lupus eryrhemarosus(SLE); two with chronic unspecific polyarthritis(CUPA); and two with chronic unspecific mono-arthritis (CUMA). The two groups were examined
216 Volume 9. Number 3. 1995

oelgren et al
together as ;in inflammatory entity (RA -f NRAgroup), and as two separate subgroups. The meanage was 46,9 years for the RA -̂ NRA group, 48,6years ± 1.9 for the RA group, and 44,3 years ± 3,0for the NRA group. The tnean duration of rhegeneral dtsease was 11.9 years for the RA -f NRAgroup, 11,0 years + 3,2 for the RA grotip, and14,9 years ± 3.9 for rhe NRA group. The meanduration of symptotns tn the TMJ was 4,0 yearsfor the RA + NRA group, 4.9 years ± 2,1 for theRA group, and 2,6 years ± 0.7 for the NRAgroup.
Procedure
This study was approved hy the Ethical Committeeof the Huddtnge Hospital, No. 176/91, Allpatients were examtncd at their first and secondvisits. Both these sessions tncluded blood plasmasampling, clinical examtnation, arthrocentesis,and intra-articular methylprednisolonc adminis-tration. Each session started with collection ofvenous blood samples, clinical examination, andarthrocentesis of the symptomatic TMJs, unilater-ally or bilaterally. Before the arthrocentesis, localanesthesia of the auriculotemporal nerve was per-formed with 20 mg of lidocaine (1 mL ofXylocaine, Astra Pharmaceuticals, Södertälje,Sweden, 20 mg/mL], followed by intra-arricukrinfusion of 1 mL of isototiic saline into the upperjoint compartment. After 20 seconds, the salinewas aspirated. The samples were mixed with 0,1mL of aprotinin (Trasylol, Bayer, Leverkusen,Germany) and 0,1 mL of heparin, cold-cen-trifuged (800 G), and immediately frozen at-70"C. Both sessions ended with intra-articularinjections of 28 mg of methylprednisolone (0.7mL of Depo-Mcdrol, Up|ohn, Kalamazoo,Michigan, 40 mg/mL| with a mean of 47,3 days ±3 between the visits. All patients were referred forradiologie examination of the TMJ includingtomography at the first visit.
Blood
Ten mL of venous blood samples were collectedand mixed with 0,25 mL of heparin (5,000 IU/mL)and 0.25 mL of aprotinin (Trasylol), immediatelycooled ro 0°C, and centrifuged at 3,000 rpm for10 minutes. The plasma was then frozen at -70°C,
Blood samples were also taken for determina-tion of the acute phase reactants: erythrocyte sedi-mentation rate (ESR); C-reactive protein (CRP);rheumatoid factor (RE); and antinuclear antibodyrate (ANA).
Clinical Parameters
The patients were questioned about their TMJpain with reference to a visual analog scale (VAS)from 0 to 10 (0 - no pain, 10 - worst pain everexperieticed). The patients were examined for ten-derness on palpation of the TMJ (on both sides):
0 = no tenderness1 = tenderness lateral or posterior to rhe TLVIJ
without palpebral pain reflex2 = tenderness either lateral or posterior to the
TMJ with palpebral pain reflex or tendernessboth lateral and posterior without palpebralreflex
3 = tenderness lateral and posterior to TMJ withpalpebral reflex at one site
4 = tenderness lateral and posterior to TMJ andpalpebral reflexes at both sites
The degree of anterior open bite (AÜB) wasexamined;
0 = occlusal contacts of canmes, premolars, andmolars
1 = occlusal contacts posterior to the canine2 = occlusal contacts posterior to the first pre-
molar3 = occlusal contacts posterior to the second pre-
molar4 = occlusal contacts posterior to the first molar5 = occlusal contacts solely on the third molar
The maximal voluntary movement (MVM) wasmeasured as the distance in millimeters betweenthe maxillary and mandibular right medial incisorswith the addition of the vertical overbite,
Neuropeptides
The joint fluid aspirates and blood plasma wereanalyzed for concentrations of neuropeptide-likeimmunoreactivities (Np-LI), ie, SP-LI, CGRP-LLNKA-LL and NPY-LL Technical difficulties withthe radioimmunoassay limited the number of con-centrations from the SP assay. Therefore, SP-LIcould not be correlated to the clinical parametersin the separate RA group; the correlations repre-sent the inflammatory entity of the RA -̂ NRAgroup. Samples were purified and concentratedusing reverse-phase CIS cartridges (Sep Pak,Waters, Milford, MA) and analyzed using compet-itive radioimmunoassays,'^
The SP-LI was analyzed using antiserum S2, andintra-assay and interassay coefficients of variationwere 7% and llTo, respectively. Samples withconcentrations of SP-LI below the formal detectionlimit of the assay were concentrated in the car-
Journal of Orofacial Pain 217

Appelgren et al
Table 1 Correlation Coefficients Between the Ncuropeptide-like Immunoreactiviries in TMJ Fluidand the Clinical Parameters
Palpatory tendsrness
AOB
Overall' RA group
S1S2SIS2S iS3S IS3
SP-Ll
-0,58"NSNSNSNS
-0,56*-0 66**
NS
11
1414141414131414
CGRP-Ll
NSNSNSNSNS
0 42 "-0 71 ***
NS
n
32263226312632
26
NPY-Ll
NSNSNSNSNSNS
-0,35*-0,43*
n
353835283528352 8 -
CGRP-LI
NSNSNS
0,87"'NS
0,78*"-0,51*
0,71"
n
la13181218131813
NPY-LI
NSNS
0 45*0 56*
NS0,76"*
NS
-0,75'"
n
20132015201520
15
tDats from iheRA group ardihe NRA group, SI = first ;•P e ,05,
iior: NS ^ Fioi sign i II can I
tridges to detect the minute concentrations. Thereported concentrations of SP-Lt thus reflect thattfie samples have heen concentrated and expressthe estimated concentrations in the original sam-pies before extraction. The NKA-Lt was analyzedusing antiserum K12, and intra-assay and interas-say coefficients of variation were 7% and 12%,respectively,"' The CGRP-LI was analyzed usingantiserum CGRPR8, and intra-assay and interassaycoefficients of variation were 8% and 14%, respec-tively. The NPY-LI was analyzed using antiserumNl , and intra-assay and interassay coefficients ofvariation were 7% and 12%, respectively,'*Normal reference ranges for blood plasma inhealthy individuals obtained with the radioim-munoassays used in this study areas follows: SP-LI< 15 pmol/L, CGRP-LI < 96 pmol/L, NKA-LI < 12pmol/L, and NPY < 50 pmol/L.'"«'
Statistics
The correlation between the clinical variablesAOB, MVM, and the neuropeptides was tested by-Pearson's product-moment correlation coefficient.The correlation between the data from the clinicalvariables VAS, palpatory tenderness, and the neu-ropeptides was rested by Kendall's rank correla-tion coefficient. The tests were performed two-tailed, and P < .05 was considered statisticallysignificant.
Results
All neuropeptide concentrations in the TMJ fluidexceeded those in plasma. The RA + NRA groupexposed correlations between SP-LI, CGRP-LI,
and NPY-LI in the TMJ fluid and VAS as wellas MVM, The VAS was positively correlated toCGRP-LI and NPY-LI but negatively to SP-LL TheMVM was negatively correlated to al! three pep-tides. The RA group demonstrated the most andthe strongest correlations between C]GRP-LI, NPY-LI, and the clinical parameters. The VAS and AOBwere positively correlated to CGRP-LI and NPY-LI, and the MVM was negatively correlated to thesame neuropeptides, Neurokinin A was not relatedto any of the investigated parameters. The jointaspirate volumes ranged between 0,2 and 1,3 mL,with an average of 0.53 mL. Arthritic radiologiechanges supported the inflammatory origin of thedevelopment of an anterior open bite. Tomographyof the TMJ revealed loss of condylar bone and ero-sions on either the condylar or temporal compo-nents of the TMJ in patients with an AOB ofgreater than three.
The correlation coefficients between the investi-gated neuropeptides and the clinical variables andthe number of observations in the RA + NRA group,as well as in the RA group, are shown in Table 1.Means and standard errors of the mean (SEM) ofSP-LI, CGRP-LI, and NPY-LI in the RA + NRAgroup and in the RA group are shown in Table 2.
Blood
The neuropeptide concentrations and acute-phasereactants in blood plasma refer to the samplesfrom session 1. The means of acute-phase reac-tants for the RA + NRA group were 30.7 mm/hfor ESR and 25,4 mg/L for CRP. The mean ANAtiter was 1:94.6, and the mean RF tirer was1:138.6. The mean neuropeptide concentrations inblood plasma of the same group were (in pmol/L):
218 Volumes, Number3, 1995

Appelgrer) et al
SP-LI, 3.S; CGRP-Ll, 5.1; and NPY-LI, 36.2. Themeans in tbe RA group were the following: ESR,41.5 mm/h; RF titer, 1:120; ANA titer, 1:137.5;CRP, 33.0 mg/L; and (in pmol/L): SP-LI, 5.3;CGRP-LI, 8.2; and NPY-LI, 47.0. No associationwas found between the investigated acute-phasereactants and the neuropeptide concentrations inTMJ fluid.
Neuropeptides and Clinical Parameters
SP-Ll. Because of SP-LI concentrations below tbeformal detection limit of tbe assay, tbe analysis ofthe correlations between SP-LI levels and clinicalparameters was restricted to tbe RA 4. NRA group.In session 1, SP-LI showed a negative correlationwith palpatory tenderness {r = -.58, F < .01, n =14) and MVM [r = -.66, P < .01, n = 14). In ses-sion 2, a negative correlation between SP-LI andVAS (í- = -.56, P < .05, n = 12) was found.
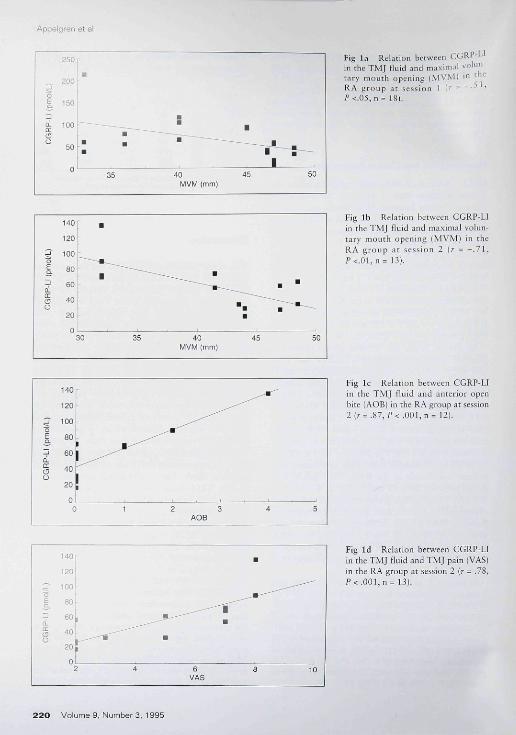
CGRP-LI. In session 1, CGRP-LI showed a nega-tive correlation witb MVM in the RA + NRA group(r - -.71, P < .01, n = 32) as well as separately in theRA group {r = -.51. P < .05, n = 18; Fig la) and theNRA group {r = -.73, F < .03, n = 14).
In session 2, the RA -1- NRA group showed apositive correlation between CGRP-LI and VAS(r = .42, F < .01, n = 26), but no statistically signif-icant correlation was found witb tbe other clinicalvariables. The RA group, bowever, showed a nega-tive correlation between CGRP-LI and MVM (r =-.71, P < .01, n = 13; Fig lb) and a strong positivecorrelation between CCRP-LI and AOB on thecontralateral side (r = .87, F < .001; n = 12; Fig lc)and with VAS ¡r = .78, F < .001, n = 13; Fig Id).
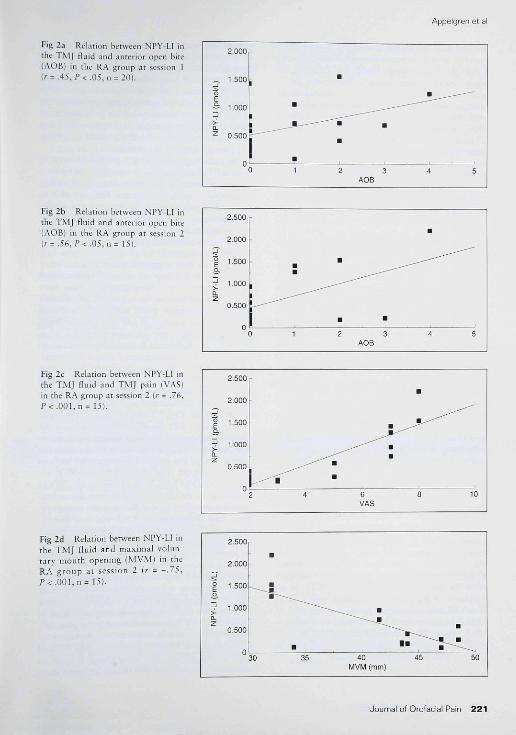
NPY-LI. In session 1, the only statistically sig-nificant correlation in the RA •+ NRA group wasfound between NPY-LI and MVM (r = -.35, F <.05, n = 35). The RA group exposed a weak, butstatistically significant, positive correlationbetween NPY-LI and AOB on the conttalateralside {r = .45, F < .05, n = 20; Fig 2a). The NRAgroup exposed a weak negative correlationbetween NPY-LI and palpatory tenderness (r =-.44, P < .03, n = 15).
In session 2, in tbe RA + NRA group, there wasa negative correlation between MVM and NPY-LI(r = -.42, P < .05, n = 28). In tbe RA group, NPY-LI was correlated to all clinical parameters exceptto palpatory tenderness. The NPY-LI was posi-tively correlated to AOB on the contralateral side{r = .56, F < .05, n = 15; Fig 2b); showed a positivecorrelation witb VAS (r = .76, F < .001, n = 15;Fig 2c); and was negatively correlated with MVM
001 1 5 F i 2 d )
Table 2 Mean Neuropeptide Concentrations ofNeuropepnde-like Immunoreactivities in TMJ Fluid
SP-LI
CGRP-LI
NPY-LI
S1S2SIS2SIS2
Overallt
Np (pmol/L)
95102
9370
771654
SEM
22.323 21399 5
131111
RA group
Np ¡pmol/L) SEM
6658
649697
_11.18.7
94.9166
tData From the RA group and Ihe NRA group. NP - neuropeplideconcenlrgtion- SI = first session, S2 ^ second session
Discussion
This study presents reiationships between concen-trations of SP-LI, CGRP-LI, and NPY-LI in TMJfluid and clinical parameters related to pain,mobility, and destruction of the TMJ. Although allpatients, on their first visit, were given one intra-articular methylprednisolone injection, the corti-costeroid effect was not evaluated in this study.The effect of methylprednisolone on inflammatoryreactions is well documented, and consequently animprovement of symptoms is to be expected.Correlations berween tbe neuropeptide concentra-tions and the clinical variables from visit one andvisit two are presented separately, witb visit oneoccurring prior to steroid administration and visittwo after steroid administration. A relationshipbetween the symptoms and signs from the arthriticTMJ and the neuropeptide content in the |ointfluid is demonstrated irrelevant of the methyipred-nisolone effect. The neuropeptide concentrationsin the TMJ fluid, well exceeding tbose inplasma,^'-'-' indicate a local release of neuropep-tides. Althougb elevated acute-phase reactantswere not associated with high neuropeptide con-centrations locally in the arthritic TMJ fluid, theysupported other clinical manifestations of an ongo-ing inflammatory process. Anesthesia of theauriculotemporal nerve, possibly reducing theafferent activity and thereby the neuropeptiderelease, may have influenced tbe Np-LI in the TMJaspirates. It is therefore important to point outthat all patients received similar anesthesia, andthe presumably decreased peptidetgic activity was,nevertheless, significant enough to disclose neu-ropeptide concentrations above the plasma level.Tbe occurrence of a rheumatoid pannus in thearthritic TMJ does sometimes complicate thearthrocentesis, and by consequence, the aspiration
Journal of Orofacisl Pain 219
Appelgren et al
Fig la Relation between CGR"" 'in the TMJ fluid and maximal volun-tary mouth opening (MVM) 1" ''̂ '-'RA group ac session 1 I ' - "•-''^'1̂ <.Ü5, n = IS).
(pm
ol/L
)C
GR
P-L
I
140 B
120
100
80
60
40
20
•
30 35 40MVM (mm)
•
45 50
Fig lb Relation between CGRP-LIin the TMJ fluid and maximal volun-tary mouth opening (MVM) in theRA group at session 2 {r - - . 7 1 ,P<.01,n= 13).
_)
(pm
oC
GR
P-L
I
140
120
100
80
60
40
20
0
i•
1 2 3AOB
4 5
Fig le Relation between CGRP-Uin the TMJ fluid and anterior openbite (AOB) in the RA group at session2(j' = .87, P<.001,n = 12).
•d
(pm
oC
GR
P-L
I
140
120
100
SO
60
40
20 1
2 4
m
,6
VAS
•
,8
^ — ^
10
Fig Id Relation between CGRP-LIin the TMJ fluid and TMJ pain (VAS)in the RA group at session 2 (r - .78,P< .001 ,n^ 13).
2 2 0 Volume 9. Number3. 1995
Appelgren et al
Fig 2a Relation between NPY-LI inthe TMJ fluid and anterior open bite(AOB) in rhe RA group at session II--- .45, P<.05, n = 20).
1 (pm
ol/L
)N
PY
-
2 000
1 500
1.000
0.500
•
•
3 1
•
•
2 3A08
4
.-——'
5
Fig 2b Relation between NPY-LI inthe TMJ tliiid and anterior open bite(AOB) in the RA group at session 2(r= .56, P<.05, n= 15).
2 3AOB
Fig 2c Relarion between NPY-LI inthe T.MJ fluid and TMJ pain ¡VAS]m the IIA group at session 1 [r = .76,P< .001, n - 15).
(pm
ol/L
NP
Y-L
I
2.500
2.000
1.500
1.000
0.500
04
^ ^
m
6VAS
8 10
Fig 2d Relation between NPY-LI intbe TMJ fluid and maximal volun-tary mouth opening (MVM) in theRA group at session 2 ¡r = - .75 ,i'<.OO),n = 15).
amol
/LJP
Y-L
I
2.500
2.000
1.500
1.000
0.500
•
•30 35 40
MVM (mm)
• • 7 ^45
••
50
Journal of Orofacial Pain 2 2 1

Appelgren et al
of joint fluid. Aspiration from the soft tissue of thepannus is seldom successful since the aspirateseither (1) contain mostly blood, thus reflecting theneuropeptide concentrations in the plasma, or (2)allow insufficient voltimes for radioimmunoassayanalysis. We have, however, no reason to believethat the neuropeptide concentrations in the jointfluid should differ from those in the pannus.Therefore, when successfully performed, aspiratesfrom the pannus do reflect the neuropeptide con-centrations in the joint fluid. Our results indicate arelationship between neuropeptides in the arthriticTMJ fluid and joint pain, reduced mandibularmobility, and occlusal signs of tissue destruction inpatients with rheumatoid arthritis.
In this study, assessed pain is expressed in twodifferent aspects, as pain at rest and function byVAS and as a response to external pressure by pal-patory tenderness, Substance-P fibers are found inthe synovial lining of the TMJ and ad|acent perios-teum,'"" and both SP and CGRP are proposed tobe involved in the propagation of noxious nocicep-tive impulses," In addition, SP and NPY have beenshown to amplify experimental adjuvant arthritisand joint destruction in rats,''- We therefore hadreason to expect palpatory tenderness to correlatepositively to these peptides. At session 1, palpatorytenderness correlated negatively both to SP-LI inthe RA -I- NRA group and to NPY-LI levels in theNRA group. The VAS was also negatively corre-lated to SP-LI. Palpatory tenderness and VAS,although both tools for pain assessment, demon-strated different relationships with the paiti-associ-ated neuropeptides. It appears that these parame-ters reflect different aspects of inflammatory painresponse, where possibly different cellular-response mechanisms account for the mediation.The negative relation between SP-LI and bothpain-related parameters is contradictory to thedocumented nociceptive properties of SP; however,an anti-inflamtnarory role of sensory nerves cannotbe disregarded.^-
Calcitonin gene-related peptide is a potentvasodilator and its inflammatory role has been dis-cussed.'"•""" Since CGRP is released directly fromthe nociceptive C-fiber terminals" and is involvedin the propagation of noxious nociceptive impulsesfrom the periphery," we did expect VAS, as anindicator of pain, to be associated with CGRP,The VAS was accordingly positively correlated toCCRP levels in the RA group and in the RA +NRA group. These findings suggest the involve-ment of CGRP in the mediation of TMJ pain inpatients vi'ith RA and other arthritides.
Increased activitry in efferent nerves of thethetic system has been associated with increases mjoinr mflammation and destruction.'' As a regulatorof the severity of joinr inflammation, it is plausiblethat NPY also is involved in the pain respmi'̂ '̂ fromthe arthritic TMJ. In this study, high concenrrarionsof NPY-LI were associated with increased iomtpain in the RA group only. It is therefore likely thatNPY does contribute to the mediation of inflamma-tory pain of rheumatoid arthritis.
The pathology of the TMJ is a frequent cause ofreduced voluntary mouth opening (MVM) inarthritic patients. Tissue destruction as well as sub-sequent healing in the arthritic TMJ are able tocreate adhesions between the temporal and condy-lar components of the TMJ, reducing mobility ofthe mandible. Destruction of TMJ cartilage andbone tissue is clinically reflected by reduced MVMand the development of an anterior open bite(AOB), It has heen suggested that microcirculatorydysfunction in RA may act as a pathogenic factorin joint destruction."' Neuropeptides have beenshown to contribute to the hyperemia of inflamedjoints." Neuropeptide Y, SP, and CGRP have beenproposed to be involved in not only vascular regu-lation, but also immunoregulation and bonemetabolism,'" Substance P stimulates pannus for-mation," and its inflammatory action is potenti-ated by CCRP," We have previously shown thatincreased NPY levels in the TMJ are associatedwith reduced intra-articular temperature, suggest-ing neuropeptide-mediated microcirculatory failurein the arthritic TMJ,'" Synovial fluid acidosis wasfound in knees with destructive arthritis,'"' and theobserved hypoxia of the joint tissues could there-fore implicate NPY involvement in the arthriticdestruction of the joints, Consequently, we hadreason to expect that SP, CCRP, and NPY arerelated to MVM and AOB. In this study, MVMappears to he the clinical variable with the strong-est relation to the neuropeptide content in the syn-ovial fluid of the arthritic TMJ, and it is demon-strated that increased levels of these neuropeptidesare associated with an impairment of the mandibu-lar mobility in patients with RA, An anterior biteopening indicates tissue destruction of the jointwith subsequent deterioration of the dental occlu-sion. This process is irreversible and adds muscularpain and tension to the patient's clinical panoramaof symptoms. Our findings indicate that release ofCGRP and NPY promotes destruction of joint car-tilage and bone tissues, which in turn explains partof the negative relation between CGRP-LI andNPY-LI and MVM, The NRA group showed nostatistically significant correlation between these
222 Volume 9, Number3, 1995

seigren el al
neuropeptides and AOB, Therefore, we believethat action of CGRP and NPY in arthritic jointdestruction may be particularly pronounced inrheumatoid arthritis.
We had expected NKA to be related to sume ofthe clinical parameters, but no correlations werefound in any of the groups. The reason is unclear,and further studies are needed to elucidate the roleof NKA in TMJ arthritis.
It can be concluded tbat high concentrations ofCGRP and NPY in the TMJ fluid are associatedwith pain, impairment of mandibular mobility,and occlusai signs of TMJ destruction in patientswith rheumatoid arthritis. The results of this studyindicate neuropeptide involvement in rheumatoidarthritis in particular, proposing a potentiation ofthe symptoms and signs of TMJ arthritis hy theinflammatory action of CCRP and NPY,
Acknowledgments
This study was supported by grams from the Swedish MedicalResearch Board (7464); School of Dentistry, KaroHnskaInstirute; Swedish National Association Against Rheumatism;King Gustav Vth SO-year Anniverbary Fund; Professor NannaSwarrï Foundation; Anna-Greta Crafoords Foundation; LariHiertas Memorial Fund; and the Swedish Dental Society,
References
PA,1, Kidd BL, Mapp PI, Gibson SJ, Terry JM, RevelIbrahim NBN, et al. Hypothesis, A neurogenic mechanismfor symmetrical arthritis. Lancet 1989;2i 1128-1130,
2, Levine JD, Goetzl EJ, Basbaum AI, Contrihntion of thenervous system to the pathophysiology of rheumatoidarthritis and othtr polyathritides. Rheum Dis Clin NorthAm 19S5;13:369-3fí3,
3, Levine JD, Clark R, Devor M, Htimb C, Moskowitz MA,Basbaum I A. Imranenronal suhstance P contributes to theseverity of experimental arthritis. Science 19S4;226:547-549.
4, Härtung H-P, Wolters K, Toyka KV, Substance P, Bindingproperties and studies on cellular responses in guinea pigmacrophages. J Immunol I986;13é;3S56-3S6.î,
5, Lotz M, Carson DA, Vaughan JH, Substance P activationof rheumatoid synoviocytes: Neural pathway ir pathogen-esis of arthritis- Science 19g7;235.893-89,S-
6, Bisset GW, Lewis GP, A spectrum of pharmacologicalactivity in some biologically active peptides, Br J Pharma-col i962;19:16S-lg2,
7, Juan H, Sametz W, Histamine-induced release of arachi-donic acid and prostaglandins in the peripheral vascularbed. Arch Pharmacol 1980;314:183-190,
8, Lundberg JM, Franco-Cere ceda A, Hua X-Y, Hëkfeh T,Fischer JA, Co-existence of suhstance P and calcitoningene-related peptide-like immunoreactivities in sensorynerves m relation to cardiovascular and bronchoconstrie-tor effects of capsaicin, Eur J Pharmacol 1985ilO8:315-3)9.
Brain SD, Wilhams TJ, Tippins JR, Cdcitonin gene relatedpepridf IS,I piiteiir vasodilator. Nature I986;313i54-5é,Hope PJ, Schaibk- HG, Jarrot B, Duggan AW. Release andpersistente of immunoreactive nejrokinin A in the spinalcord is associated with chemical arthritis. Pain 1990;(suppl 51:230,
Lundberg JM, Terenius L, Hökfelt T, Martling C-R,Tatemoto K, Mutt V, et al, Neuropeptide Y |NPY)-likeimniunoreactivity in peripheral noradrenergic neurons andeffects of NPY on sympathetic function. Acta PhysiolScand 1982;1]6:477-48Ü,
Levine JD, Dardick SJ, Roizen MF, Helms C, Basbaum ALContrihLition of sensory afférents and sympathetic efier-onts to joint injury in experimental arthritis, J Neurosci19S6;é;3423-3429,Lam FY, Ferrell WR, Acute inflammation in the ral kneeloint attenuates sympathetic uasotonstriction butenh.mCLb neuropeptide-mediated vasodilatation assessedhy bscr Doppler perfusion iniüging. J Neurosci 1993;Í2:443^49 ,
Silva da Peieira JA, Carmo-Fonseca M, Peptide containingnerves in human synovia: lmmunohistochemical evidencefor decreased innervation in rheumatoid arthritis. JRheumatoi I99i);l7:1592-I599,Veale DJ, Fitzgerald O, Sympathetic nervous system inchronic joint pain [letter], Ann Rheum Dis 1993;S2:552,Menkes CJ, Rcnoux M, Laoussadi S, Mauhorgne A,Bruxelle J, Cesselin F, Substance P levels in the synoviumand synovial fluid from patients with rheumatoid arthritisand osteoarthritis, J Rheumatoi 1993;20:714-717,Larsson J, EkWom A, Henriksson K, Lundeberg T, Theo-dorsson E, Immunoreactive tachykinins, calcitoningene-related peptide and neuropeptide Y in human syn-ovial fluid from inflamed joints, Neurosci Lett I989;100:326-330,Larsson J, Ekhloni A, Henriksion K, Lundeberg T,Thtodorsson E, Concentration of substance ?, neurokininA, calcitonin gene-related peptide, neuropeptide Y andvasoactive intestinal poiypeptide in synovial fluid fromknee joints in patients suffering from rheumatoid arthritis,Scand J Rheumatoi 1991;20:326-335,Appelgrin A, Appelgren B, Eriksson S, Kopp S, LundehergT, Theodursson E, Neuropeptides in temporomandibularjoints with rheumatoid arthritis; A chnical study, Scand JDent Res 1991;99:519-521,Appeigren A, .Appelgren B, Kopp S, Lundeberg T,Theotlorsson E, Relation hetween the intra-articular tem-perature of the temporomandihular ]oint and the presenceof neuropeptide Y-hke immunoreactivity in the |oint fluid-Acta Odontol Scand 1993phl-S .,Appelgren A, Appelgren B, Kopp S, Lundeberg T,Theodorsson E, Relation between intra-articular tempera-ture of the arthritic temporomandibular joint and presenceof calcitonin gene-related peptide in the joint fluid. ActaÜdontol5cand 1993;51:2S5-291.Rodnan GP, Rheumatoid arthritis. In: Schumacher HR(ed). Primer on the Rheumatic Diseases, Atlanta, GA:Arthritis Foundation, 1983:3S-48,Johansson A-S, Isacsson G, Isberg A, Granholm A-C.Distribution of substance P-like immunoreactive nervefibers in temporomandibular joint soft tissues of monkey,Scand J Dent Res 1986;94:225-230,ichikawa H, Wakisaka S. Matsuo S, Akai M, Peptidergicinnervation of the temporomandibul-ir disc in the rat,Experientia l989;4j:303-304.
Journal of Orotacial Pain 2 2 3

Appelgren et al
25. Tegdberg Â, Kopp S. Subjective symproms from the sio.matognaihic system in individuals wirh rheumatoid arthri-tis and osteoarrhrosis. Swcd Dent I 19«?;! 1:11-22.
26. Thcotlorsson-Nor heim E, Hemsfii A, Rroilin E, LiindliergJM. Sample handling techniquei when analyzing regula,tory pcprides. Lift Sti 19íí7;41:845-848.
27. Brodiii E, l.rudetors N, Oaalsgard C-J, Tlieodorsson-Norheim E, Rosell S. Tachykinin multiplicity in the rarcenrral nervous system as studied using antisera againstsubstance P and neurokinin A. Regul Pept 1986:13:253-272.
28. Theodorsson-Norheiiii H, Hemsen A, Lundberg JM.Chromatographie characterization of immnnüreactivity inplasma and tissue extracts. Scand J Clin Lab Invest 1 9S5;45:355-366.
29. Theodorsson-Norhi'im E, Brodin E, Norheim 1, Roseli S.Antisera raised against eledoisin and kassmin detectimmunoreactive material in rat tissue extracts: Tissue dis-tribution and Chromatographie charatterizariun. RegulPept 1984;9:229-244.
30. Sluka KA, Dougherty PM. Sorkin LS, Willis WD,Westlund KN. Neural cbanges in acute arthritis in mon-keys. III. Changes in substance P, calcitiimri gene-relatedpeptide and gluramate in the dorsal horn of the spinalcurd. Brain Res Brain Res Rev 1992:17:29-38.
31. Buma P, Verschuren C, Versleyen D, Van der Kraan P,Oeirreicher AB. Calcitonin gene-related pepride, sub-srante P and CAP-43/B50 mimunoreactivity in the normaland arthrotic knee ioint of rbe mouse. Histochemistry1992:98:327-339.
32. Raud J, Lundeberg T. Brodda-Jansen C, Tbeodorsson E,Hedqvist P. Potent anti-inflammarory action of calcitoningene-relared peptide. Biocliem Biopbys Res Cnmmun1991; 180:1429-1435.
.Î3. Brain SD, Williams TJ. Inflammatory oedema induced bysynergism between CGRP and mediators of increased "as-cular permeability, Br J Pharmacol 1985;86:85 5-Sii('.
34. Luuis SM, Jobnsrone D, Millest AJ, Rüssel NJW, Di.^krayCE. [minunizarion with calcitonin gene-relartJ [«ptidL-reduces the inflammatory response ro adjuvant .irtiiritis inrhe rat. Neuroscience 1990;39:727-731.
35. Sundler F, Brodin E, Ekblad E, Hâkansson R, UddEii.in R.Sensory nerve fibers distr ibution of substance P,neutokinin A and calciriinin gene-relared peptide. In:Hâkansson R, Sundler ¥ ¡eds). Tachykinin Antagonists.Amsterdam: Elsevier Science Publisbers, 1985:3-14.
36. Goldie L Tbe synovial microvascular derangement inrheumatoid arthritis and osteoarthritis. Acta OrtbopScand 1970:40:751-764.
37. Hoher P. Local effector of capsaicin-sensitive nerve end-ings: Involvemenr of lachykinins, calcitonin gene-relatedpeptide and otber neurnpeptides. Neuroscience 1988;24:739-768.
38. Kimball ES, Fisber MC, Potentiation of IL-J-inducedBALB73T3 fibrobkst proliferation by neuropeptides. JImmunol 1988^141:4203-4208.
39. Louis SM, Jamieson A, Rüssel NJW, Dockray GE. Therole of substance P and calcitonin gene-related peptide inneurogenic plasma exrravasation and vasodilarion in therat. Neuroscience 1989;32:581-586.
40. Geborek P, Saxne T, Pettersson H, Wollheim FA. Synovialfluid acidosis correlates wirh radiological )oint destructionin rheumatoid knees. J Rheumatol 1989;16:468-472.
224 Volume 9. Number 3, 1995

aelgren et al
Resumen
El Papel de los Neuropépt idos en la Art iculaciónTemporomandibular Artrítica y los Sintomas y Signos delSistema Estomatognático con Consideración Especial ala Artritis Reumatoidea
Se ha planteado que la contribución del sistema nen/ioso a lapatofisiologia de la artritis (eumatoidea es mediada por ciertosneuropéptidos. El neuropéptido Y. el péptido reiacionado al gende la calcitonina, la substancia P y la neurocmina A son consid-erados moduiadores de la enfermedad inílamatona de la articu-lación En este estudio se investigaron los parámetros del doior.asi como los signos oclusales de destrucción tisular de la articu-iaclón temporomandibular CATM) artrítica y ias concentracionesde neuropéptidos correspondientes ai fiuido sinovial de ia ATM,en pacientes con vanas enfermedades inflamatorias de la articu-lación. Los pacientes con artritis reumatoidea también fueronexaminados en un grupo de diagnóstico separado. Se correia-cionó ia escaia anáioga visuai, ia sensibilidad a ia paipación, iaapertura bucal voiuntaria máiíima. y ia mordida abierta antenor alas inmunoreactividades de ios cuatro neuropéptidos menciona-dos anteriormente Se encontró que ias concentraciones aitasdel péptido reiacionado ai gen de ia caicitomna y dei neuropép-tido Y en ei fluido temporomandibular están asociadas al dolor,ai deterioro de la movilidad mandibuiar. y a ios signos ociusalesde destrucción de ia ATÍvi en pacientes con artritis reumatoidea.Los resuitados indicaron que ios neuropéptidos estaban envuel-tos en ia artritis reumatoidea. y se piantea que la potencia deios síntomas y signos puede eievarse debido a ia acción inflam-atoria dei péptido reiacionado ai gen de ia caicitomna y del neu-ropéptido Y.
Zusammenfassung
Neuropept ide im arlhr i t ischen Kiefergelenk undSymptome und Zeichen des stomatognathen Systemsmit spezieller Beachtung der rheumaloiden Arthritis
Der Beitrag des Nervensystems zur Pathophysiologie derrheumatoiden Artliritis wird—so wird angenommen—durciigewisse Neuropeptide vermittelt. Das Neuropeptid V. "calci-tonin gene-related peptide," Substant? P und Neurokinin A sindvermutete iviodu i atoren der entzündlicíien Geienkerkrankung.Bei Patienten mit verschiedenen Geienkerkrankungen wurdenSchmerzparameter, okkiusale Zeichen der Gemebszerstorungim arthritischen Kiefergeienk und Ne uropeptidkonzent ration en inder Synoviaiflussigkeit der entsprechenden Kiefergeienkegemessen. Die Patienten mit rheumatoider Arthntis wurden ineiner separaten diagnostischen Gruppe zusammergefasst.Visual anaiog scale. Paipationsempfindiichkeit, maximaieivlundöifnung und frontoffener Biss wurden mit der neuropep-tidahnlichen immunoreaktivität der obengenannten vierSubstanzen in Zusammenhang gebracht. Man fand, dass beipatienten mit rheumatoider Arthritis iiohe Konzentrationen von'calcitonin gene-related peptide" und Neuropeptid Y imKiefergelenk vergeseiischaftet sind mit Schmer;en,Einschränkung der Unterkieferbeweglichkeit und okkiusaienZeichen von Kiefergeienkzerstorung Die Resultate weisen aufeine Beteiiigung der Neuropeptide an der rheumaloiden Arthritishin; die entzCindiiche Wirkung von "caicitonin gene-related pep-tide" und Neuropeptid Y scheint eine Verstärkung defSymptome und Zeiclien herbeizuführen.
Journal of Orofacial Pain 2 2 5