neurology: a handbook for action - north norfolk clinical ... - a... · neurology: a handbook for...
TRANSCRIPT
Neurology: A handbook for action
An audit of neurological services in Norfolk, Great Yarmouth and Waveney

3

1
Introduction
This Quality Neurology report follows an audit of the neurology services in Norfolk, Great Yarmouth and Waveney during 2012.
The auditors consulted with over 250 people: professionals, patients and their carers across four localities. This included people with the following conditions:
• Multiple system atrophy (MSA)• Dystonia• Guillan-Barré syndrome (GBS)• Trigeminal neuralgia• Epilepsy• Peripheral neuropathy• Brain tumour • Temporal arteritis• Multiple sclerosis (MS)• Spina bifida• Hemifacial spasms• Progressive supranuclear palsy (PSP)• Paraproteinaemic demyelinating neuropathy (PDN)• Parkinson’s disease• Motor neurone disease (MND)• Myasthenia• Corticobasal degeneration (CBD)• Migraine• Susac syndrome• Acquired brain injury (ABI)
Data was collected through focus groups, questionnaires, and interviews.
This Quality Neurology audit was measured against the ‘quality requirements’ (QRs) set out in the National Service Framework (NSF) for long-term neurological conditions. The NHS Outcomes Framework was also taken into account. You can read more about both of these frameworks on our website: www.ncssupport.org.uk
2
Key findings
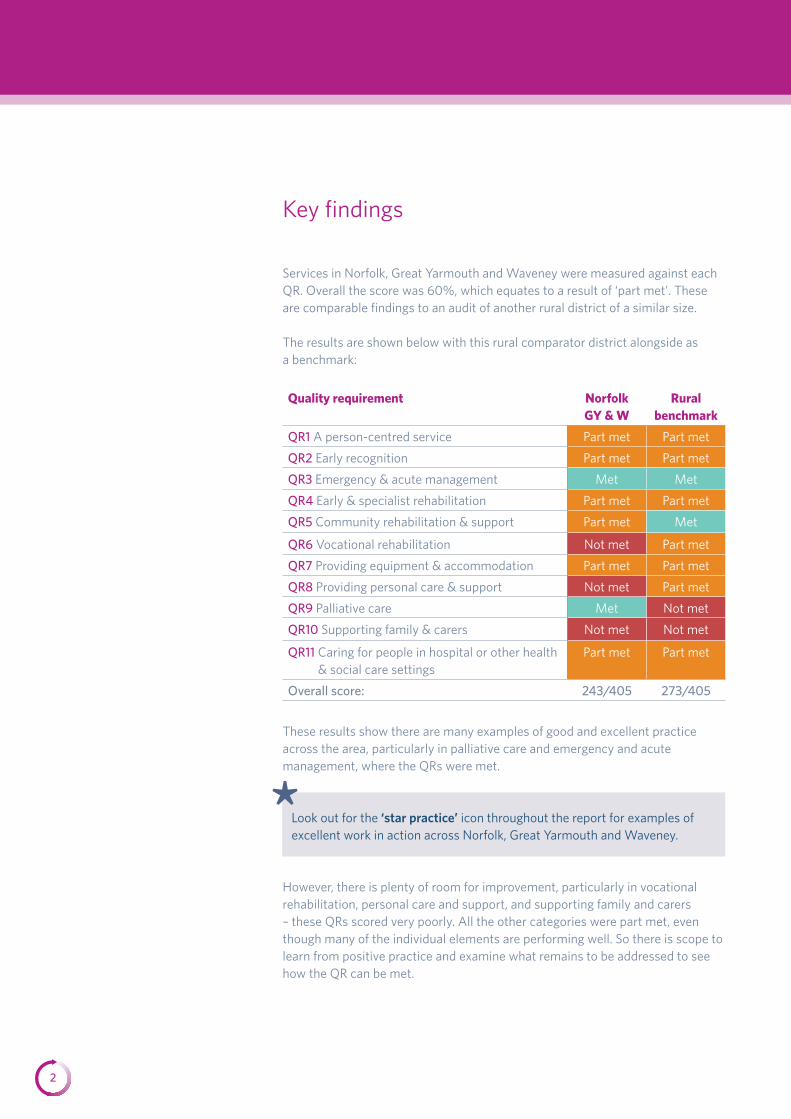
Services in Norfolk, Great Yarmouth and Waveney were measured against each QR. Overall the score was 60%, which equates to a result of ‘part met’. These are comparable findings to an audit of another rural district of a similar size.
The results are shown below with this rural comparator district alongside as a benchmark:
Quality requirement Norfolk GY & W
Rural benchmark
QR1 A person-centred service Part met Part met
QR2 Early recognition Part met Part met
QR3 Emergency & acute management Met Met
QR4 Early & specialist rehabilitation Part met Part met
QR5 Community rehabilitation & support Part met Met
QR6 Vocational rehabilitation Not met Part met
QR7 Providing equipment & accommodation Part met Part met
QR8 Providing personal care & support Not met Part met
QR9 Palliative care Met Not met
QR10 Supporting family & carers Not met Not met
QR11 Caring for people in hospital or other health & social care settings
Part met Part met
Overall score: 243/405 273/405
These results show there are many examples of good and excellent practice across the area, particularly in palliative care and emergency and acute management, where the QRs were met.
However, there is plenty of room for improvement, particularly in vocational rehabilitation, personal care and support, and supporting family and carers – these QRs scored very poorly. All the other categories were part met, even though many of the individual elements are performing well. So there is scope to learn from positive practice and examine what remains to be addressed to see how the QR can be met.
Look out for the ‘star practice’ icon throughout the report for examples of excellent work in action across Norfolk, Great Yarmouth and Waveney.
*
3
Priorities for neurology
Service users and professionals raised the same priorities during the audit about why some services are falling short.
Major priorities are:
• Communication People urgently need better communication about what services are
available, and professionals need to be consistent in how they communicate this. • Co-ordinated care
Clearer care pathways are essential – each patient needs a single, integrated care plan.
• Support Patients need to know where to go for help, and support should be more readily available to enable patients and their carers to self-manage their condition.
• Variety & inequity There is variation in service provision, access, and continuity, with over- assessment and duplication in some places meaning resources are wasted, while in others patients do not get the services they need. Patients need equitable access to services.
• Rehabilitation Specialist and community rehabilitation is needed that promotes self-management, independence, and personal support at the earliest stage possible.
• Access to services Patients need improved access to some core specialist services, especially psychological support and specialist nurses.
• Preventative care Professionals are confined to providing urgent and reactive care. More
capacity for preventative care and supporting patients to self-manage would improve patient wellbeing and reduce spend.
• Clarity Clear care pathways, roles, and responsibilities, and referral routes are needed for professionals to work efficiently and improve patient pathways.
The most urgent concerns agreed are:
• Education & professional training Non-specialist and care home staff need better training, with mandatory
competency standards. Gaps in training cause unnecessary admissions and spend.
• Information Information needs to be streamlined so that clearer materials are available to both professionals and patients. It is essential that patients are given clear information both at diagnosis and to support self-management.

4
Quick wins for neurology
In addition to our key recommendations, here is a list of four quick wins for neurology – our recommendations for delivering improvements to patient care right away:
Produce a neurology services information booklet for both patients & professionals
Available through professionals and online, this booklet should give comprehensive detail about all the neurology services available and signpost to further support that patients can access.
Getting the right information means patients can access the appropriate services and are supported to self-manage as much as possible. The booklet will also support professionals to manage patients effectively and improve care pathways.
Implement integrated care pathways (ICPs)
Collaboration is the key to good patient care, and implementing ICPs is essential. Norfolk has already piloted and developed ICPs for Parkinson’s and MS. Implementing these pathways would facilitate better care for this condition and could also influence pathways for others.
Training for non-neurology staff
Non-specialist staff, such as GPs, general nurses and care home staff need better training, with mandatory competency standards. Training on the nature of neurological conditions and the specific needs of patients is essential, because gaps in training are causing unnecessary admissions and spend. Elearning would be a useful complement to standard training in a number of disciplines.
Brief reference guides for non-specialists
Develop simple prompt cards for non-specialists listing what to ask patients about their specific conditions, to ensure people get the care they need. For example, the card would highlight the importance of asking a Parkinson’s patient when they take their medication and making sure they get it on time.
Look out for the ‘kEy RECoMMENDATIoNS’ through the pages of this report for specific action points to improve care under each QR.
**
5
QR1 A person-centred service
Integrated assessments across health and social care are incredibly rare. While a single assessment process is used in some areas, professionals agree there is generally over-assessment and duplication. Service users commented on the mass of paperwork and the lengthy processes involved, while others report never having been assessed.
Variation
Professionals have variable access to assessments, care plans and records. Very few people say they have a care plan in place.
Information & signposting
Sharing patient information between professionals is a real problem.
Patients and professionals are unsure about the services on offer and this information is not readily available. There is difficulty accessing some services, particularly psychological, respiratory, and occupational therapy.
Specialist nurses
Some patients have access to a specialist nurse, but others do not. Among those that do, views on the benefits were varied. This contrasts to NCS audits in other localities, where patients have often singled out the wide-ranging benefits of specialist nurse services.
Part met 73%
‘What’s a care plan? Where do you get one of those? I don’t know what it is. I presume it’s the care that’s on offer for you…’ (Partner of someone with MSA)
‘Everyone has different systems, different notes, and they’re not linked in together.’ (Brain Tumour UK)
People should be offered integrated assessment and planning of their health and social care needs, be able to make informed decisions, and be supported where possible to manage their own condition.
Medicine for the elderly The Norfolk and Norwich University Hospitals NHS Foundation Trust (Norfolk and Norwich) is taking steps to address the problems with integration through a multi-disciplinary assessment in a ‘one-stop shop’ system.
*
Sharing information An electronic pen for capturing data is being trialled. The pen is aimed at ensuring patient-held and professionally-held notes are similar.
*
kEy RECoMMENDATIoNS
• Guidelines on the assessment process
• Integrated care pathways that increase collaboration on assessment and information sharing
• A patient information booklet for all neurological conditions that signposts to specific services, made available across Norfolk and online
•An information booklet for staff listing colleagues’ roles and locations
•Expand SystmOne into all health and social care settings and use it for single assessment
• Specialist nurses sharing responsibilities more strategically to improve capacity issues
**

6
QR2 Early recognition
Diagnosis is given in different ways; some patients get the news by letter or telephone. After diagnosis patients have difficulty knowing what support is available.
There are teams of specialist neurology nurses for MS, Parkinson’s and MND and two community-based epilepsy nurses at Norfolk Community Healthcare Trust. There is no knowledge among staff who took part in the audit of any nurses for rarer neurological conditions.
Accessing specialists
GPs generally have good access to specialists, but they need clarity about the roles and responsibilities of different teams and care pathways, to help them make the right referrals. Community multidisciplinary team members have capacity issues that affect their attendance at clinics.
Training gaps
Training is offered, but there are barriers to staff taking it up that need to be addressed. Gaps in training often cause unnecessary hospital admissions. If respiratory or acute urinary infections are recognised and treated earlier, this could prevent admissions.
‘It’s just education all along and especially on the professional side. They need to understand because it causes no end of distress.’ (Carer for someone with Parkinson’s)
Part met 83%
People should have prompt access to specialist neurological expertise for an accurate diagnosis and treatment as close to home as possible.
Multidisciplinary clinics There are disease-specific multidisciplinary clinics for people with some common conditions, although these do not run consistently across the whole area due to transport issues.
*
kEy RECoMMENDATIoNS
• A patient information booklet for all neurological conditions that signposts to specific services, made available across Norfolk and online
• An information booklet for staff listing colleagues’ roles and locations
•Condition-specific information packs for GPs and consultants to give to patients
•Prompts for non-specialists about what to ask neurology patients
• A journey map or disease pathway covering both health and social care roles
**
7
QR3 Emergency & acute management
Patients had positive experiences of immediate emergency acute care and acute care staff; however, experiences of admissions were mixed when the admission was for a non-neurological reason.
Specialist nurses
There is no specialist nurse support in the acute settings at either the Queen Elizabeth or James Paget University Hospitals NHS Foundation Trust (James Paget).
Medication
There is not consistent access to medication on time, particularly for Parkinson’s patients where drugs must be given according to individual patients’ needs.
Intermediate & community care
Many professionals are not aware of the intermediate care options, and there are lengthy step-up and step-down waiting times.
There are problems meeting patients’ expectations of planned care and support in the community after discharge from specialist units. This is due to funding, capacity and available services. Professionals say that patients’ expectations need to be better managed.
‘We find a lot of problems when patients go into hospital. Parkinson’s patients have their own [drug] routine and that is very important – but it doesn’t happen.’(Carer for someone with Parkinson’s who runs a support group)
‘I cannot praise the hospital staff highly enough for the care and dedication they show me and my wife at our meetings.’ (Person with CBD)
‘…the speed at which I was informed of my condition, given it’s not one that’s too familiar – within an hour of being in the hospital I’d been given a fact sheet with all the Q and As on it.’ (Person with Guillan-Barré syndrome)
‘We did have a big meeting with social services before we left Addenbrookes hospital, and in Cambridge they had these wonderful ideas of what was going to happen when we came home, and none of it happened.’ (Carer for someone with epilepsy)
Met 91%
People needing emergency admission should be assessed and treated in a timely manner.
Medication on time for Parkinson’s The Norfolk and Norwich have set targets to improve access to medication at the right time and seen marked improvements. They are using the Parkinson’s UK ‘Get it on time’ materials to help them, which include information booklets and checklists. In this case, the targets are part of the Commissioning for Quality and Innovation payment framework, or CQUIN.
*
kEy RECoMMENDATIoNS
• Training for non-neurological staff about what to focus on for admissions of neurology patients
• A flagging system when a neurology patient is admitted to a non-neurology ward
• Copy good practice to get ‘medication on time’ initiatives into other hospitals
**
8
QR4 Early & specialist rehabilitation
Specialist rehabilitation on a more local level is effective and enables independence, but access to rehabilitation is variable and dependent on the condition and need. Patients say that inconsistencies in referral pathways are barriers to accessing timely and appropriate rehabilitation, and the variability of self-referral options impacts how well they can self-manage.
Access
The only patients with access to rehabilitation at the weekend are those with stroke. Professionals find that although there is meant to be an allocation of neurology rehabilitation beds in acute care, these cannot be identified. There are also problems getting people in acute settings the equipment they need for rehabilitation before they can go home.
Inconsistency in measuring rehabilitation progress
Different measurement scales are used by different areas and teams, leading to confusion on actual patient progress.
Access to equipment
Smaller pieces of equipment are easier to access, especially if linked to an occupational therapist where users report a speedy and personal service. Larger or specialist equipment is harder to access; people tend to purchase it themselves if they can.
Discharge processes
The discharge process from secondary to primary care is unclear. Agreed pathways would help get patients discharged sooner and consistent follow-up support in the community.
‘…before I got home [from hospital], all of the equipment that [the occupational therapist] had wanted for me was there; it was all done and sorted.’ (Person with Guillain-Barré syndrome)
Part met 69%
People who would benefit from it should receive timely, ongoing, high quality rehabilitation services in hospital or other specialist settings to meet their continuing and changing needs.
Specialist rehabilitation Specialist rehabilitation centre Caroline House was cited by patients as particularly exemplary:
‘It’s quite incredible. When I was at Caroline House, there were only 27 of us and we all had a room each. And the staff–patient ratio... I know it’s an acute specialist unit, but it was – it surprised me … that side of things was quite amazing.’ (Person with Guillan-Barré syndrome)
*
kEy RECoMMENDATIoNS
• A secondary to primary care discharge pathway and policy to support sustainable rehabilitation
• A common progress assessment tool for all professionals
•Explicit information for professionals and patients on equipment, with eligibility criteria and clear guidelines on who is responsible for providing it
**

9
QR5 Community rehabilitation & support
Patients and professionals say more attention should be paid to enabling people to keep well and independent. Community care predominantly reacts to urgent need at the moment rather than proactively supporting self-management or preventative care.
Holistic care
Patients say that each professional deals with ‘a bit of them’ but no one considers them as a whole. This is exacerbated by poor communication between teams, departments and specialisms.
Self-management
Self-management is encouraged through self-referral and voluntary sector support. However, very few service users appear to be referring themselves to any services, possibly because of a lack of information about what is available and how to access the system.
Integrated care
Health and social services are not integrated on the whole, although steps have been taken to address this in some areas.
‘With any long-term condition, but especially where the brain’s involved, it involves different parts of your body. So my continence nurse does that bit, and the speech therapist does that bit, and the physio does the bits in between. But they don’t talk to each other about me, so nobody knows all of me, they each know bits of me.’ (Person with MS)
Part met 77%
People living at home should have ongoing access to a comprehensive range of rehabilitation, advice and support to meet their continuing and changing needs.
Supporting integration Norfolk Community Healthcare has appointed a two-year post to lead integration, and co-ordinators are supporting complex needs patients by working across health and social care. Staff from various care settings have collaborated to develop an integrated care pathway for Parkinson’s and MS.
*
kEy RECoMMENDATIoNS
• Better access to self-care programmes and information
• A key worker system to improve the co-ordination of care
• Implement existing integrated care pathways (ICPs) for Parkinson’s and MS and develop ICPs for other neurological conditions
**

10
QR6 Vocational rehabilitation
Social care professionals did not attend the audit, so this category has only been scored from the perspective of the healthcare professionals who attended. The score for their answers is 38%, meaning QR6 was ‘not met’ for healthcare.
Signposting & support
Some professionals signpost from the health service to vocational support. However, this is not comprehensive and the professionals contributing say they do not know what or who to refer to.
Third sector
There are good links with third sector organisations. People rely on the voluntary sector to provide the signposting and support they need.
People report that the Norfolk Coalition of Disabled People is a very good service. It provides support, advice, and information, but not vocational support specifically.
Stopping work
People say they do not have the psychological support they need to make decisions about stopping work. They also do not have the educational support to look for alternative employment. Partners often give up work themselves to provide full-time care without sufficient support.
‘Headway have been quite good, but we are [trying to get back into education] with no advice and you don’t know if you’re going down the right track. Because you want to do the best thing you can and not end up somewhere that’s not relevant.’ (Carer for someone with epilepsy)
‘I don’t know what’s out there, what help is there if he has to give up work, and I’ve had to give up work myself.’ (Person with MS)
Not met 38%
People should have access to appropriate vocational assessment, rehabilitation and ongoing support.
kEy RECoMMENDATIoNS
• Better information systems for both patients and professionals that support people to remain employed or to return to work
**
11
QR7 Providing equipment & accommodation
Currently there is no single point of contact for obtaining equipment in Norfolk. Professionals are uncertain about who to ask and there are no clear agreements between health and social services about who pays for and provides equipment. This is particularly problematic for people with a rapidly advancing condition and those making the choice to die at home.
Specialist & expensive equipment
This is difficult to obtain. Patients report extremely long waiting times for hoists, stair lifts and wheelchairs.
Loaning or trying equipment
There is an apparent lack of specialist equipment to loan or to try. This includes stand-up wheelchairs, outdoor wheeled walkers and standing frames.
Timeliness
Service users report wide variation in how long it takes to get equipment and modifications to homes.
Point of contact
A joint equipment store will soon be shared between health and social care. However, budgets will not be pooled, which could mean continued distribution inequalities.
‘Dereham Hospital has everything there, so [occupational therapists] will even come on the same day if they’re out that way. They just ring me up and say “I’ll pop it over” – so brilliant.’ (Person with MS)
‘We had a wheelchair especially for motor neurone people – it tilts and does everything. Unfortunately they sent it out to her without any gears or a seat. It took 93 days to get that corrected … I’m sick of it all.’ (Carer for someone with MND)
‘Nine months we’ve been waiting for a lift belt. Our living room has been half full with them but none of the things will actually bloody fit!’ (Carer for someone with MND)
Part met 58%
kEy RECoMMENDATIoNS
• A single point of contact• Information about what
equipment is available• Criteria for obtaining equipment
and a self-assessment tool for eligibility
People should receive timely and appropriate assistive technology / equipment and adaptations to accommodation.
Voluntary sector Charities like the Red Cross and MND Association provide some equipment on an ad hoc basis:
‘[The Red Cross] have a fantastic place. We were directed there when we were looking for a bath lift. They have everything under the sun all laid out, you can try it. I would highly recommend it.’ (Carer for someone with MND)
*
**

12
QR8 Providing personal care & support
Social care professionals did not attend the audit, so this category has only been scored from the perspective of the healthcare professionals who attended. The score for their answers is 8%, meaning QR8 was ‘not met’ for healthcare.
Young people
There is a lack of age-appropriate residential care options for young people. However, the Vauxhall Centre provides day care to younger people and the voluntary organisation Headway also gives some care for younger people.
Day care
Professionals say that personal budgets have taken away the need to supply additional day care. Some service users say they are frustrated at having to pay for day care services, while others are happy to pay because of the value they place on the social support they receive there.
Nursing care
Some education is supplied in nursing homes, but usually this is patient-specific with a gap in holistic general training. Professionals cite issues with the capacity to provide education in nursing homes. High staff turnover in the care home sector also means that regular training is needed to maintain staff competency.
Support in the community
People say that hospital support is good but follow-up care in the community is poor, often with only charities to support them. Community support is particularly problematic for people living on the border between two areas.
‘We don’t get any professional help.’ (Carer for a young person with epilepsy)
Not met 8%
Health and social care work together to enable people to achieve maximum choice about living independently at home.
kEy RECoMMENDATIoNS
• Stronger links with social services to guarantee services are integrated
• Clear referral processes to community care after discharge from acute settings
• Clear information on who provides care to people living in border areas
• Give service users more information about personal budgets
• Establish elearning for nursing and residential homes to use as part of the induction package for new staff
**

13
QR9 Palliative care
There is a wide range of palliative and end-of-life care services. This includes a ‘hospice at home’ service, a palliative care consultant, out-of-hours service, good coverage from Macmillan nurses, a rapid response palliative care team, and day care at Tapping House.
End-of-life planning
Some people with a comprehensive care plan have considered the end of their life.
Non-specialist staff training
There is no formal advice or training for non-specialist staff delivering palliative care in the community. However, there is good peer support from both the Coleman Centre and the Priscilla Bacon unit. Indeed, the Priscilla Bacon palliative care unit have monthly team meetings with specialist neurology nurses to discuss individual patient cases.
Currently there is no training specifically for staff who have to have end-of-life conversations with people. Staff say there are capacity issues in terms of providing education in nursing homes.
Met 90%
‘We put down the whole plan, and it was amazing. Even end-of-life wishes, which are so important. So that it wasn’t just what I wanted, but also what I didn’t want to happen, so that [my partner] doesn’t have to worry about it.’ (Person with MS)
‘Tapping House provide alternative treatments I can access any time.’ (Person with MND)
People in the later stages of neurological conditions are to receive a comprehensive range of palliative care services when they need them.
Gold Standards Framework The Gold Standards Framework for palliative care has been adapted specifically for neurology in Great Yarmouth and Waveney. Meetings are held for GPs, community staff, consultants and palliative care nurses to discuss patient care.
*
kEy RECoMMENDATIoNS
• Follow the Gold Standards Framework for everybody with a neurological condition
• Ensure advance care planning can be discussed with all neurology patients
• Provide ongoing training, particularly to care homes, on managing a person’s end-of-life care needs for living with a neurological condition
**
14
QR10 Supporting family & carers
Social care professionals did not attend the audit, so this category has only been scored from the perspective of the healthcare professionals who attended. The score for their answers is 12%, meaning QR10 was ‘not met’ for healthcare.
While carer support is available and most carers say they are consulted ‘to some extent’, there is not enough information available about the support on offer to carers and this support varies depending on the location.
Supporting carers
Healthcare professionals with voluntary sector partnerships can provide carers with the skills to support them in their caring role, including how to move and handle the cared-for person. Carers are given the opportunity to work in partnership with specialist teams where possible; however, this is a postcode lottery. Staff say they do not have much capacity to support carers any more than they already do.
Of the carers we consulted, very few have a carer’s plan, or even know what this is.
Continuing healthcare
There is fast-track one- to two-day continuing-care provision, although it is not clear how often this can be accessed.
Out-of-hours, crisis prevention services & emergency needs
These services are not provided evenly across the area or known about by all professionals. Our survey found that a number of people accessed A&E because they did not know where else to go, which suggests that patients are not aware of these services either. Community matrons often respond to emergency needs rather than social services.
Not met 12%
‘Nobody has ever suggested to me that I might go and talk to someone as well. As a carer, you can’t, you don’t have that back-up. We’ve got good family support but if we did not have that, as a carer you become very isolated.’ (Carer for someone with focal dystonia)
Carers should have access to support and services that recognise their needs, both in their role as carer and in their own right.
kEy RECoMMENDATIoNS
• Urgent priority: produce explicit information about the carer support services available and distribute to both professionals and carers
• Map and highlight all respite services in the information booklet mentioned in QR1 and QR2
• Inform carers of their right to a carer’s assessment
**
15
QR11 Caring for people in hospital or other health & social care settings
Difficulties mainly seem to arise when patients are admitted to non-neurological wards with problems not associated with their neurological condition. People reported an overall lack of understanding of specific conditions among staff and a lack of equipment. This has a detrimental effect on patients’ wellbeing and sometimes causes increased impairment and disability. Support for people with epilepsy is particularly problematic.
Liaison with community teams
There is some liaison between professionals and community teams when patients are admitted to another care setting. Community hospitals generally have close links with community teams, but this is not universal.
Mobility
Patients who need help with moving struggle to access radiological departments. There are also poor facilities for hoisting patients in many outpatient departments.
Part met 60%
People with long-term neurological conditions are to have their specific neurological needs met while receiving treatment or care for other reasons in any health or social care setting.
Alerts for neurology patients The Norfolk and Norwich has an alert system in place for neurology admissions, and the James Paget is in the process of setting up a similar system.
*
kEy RECoMMENDATIoNS
• An alert system that prompts hospital and care home staff to seek advice about a person’s neurological condition when they are admitted for a non-neurological reason
• Copy good practice to get ‘medication on time’ initiatives into other hospitals
• Accessible education for non-neurology staff on how to manage specific neurological conditions
**
Thank you
Thanks to everyone who kindly gave up their time to share their experiences and contribute to this audit.
The experts in neurology solutions
NCS helps commissioners and service providers improve quality of care while driving down costs. As a not-for-profit organisation with two Department of Health grants, we have an ethos of keeping costs to a minimum.
We can work with you to analyse what’s happening locally and then support you to achieve your goals. Our bespoke service solutions are tried and tested. Get in touch to find out more about partnering with us.
372 Edgware RoadLondon NW2 6ND
020 8438 0715

4
© Neurological Commissioning Support 2013
NCS 002
Neurological Commissioning Support Ltd, 372 Edgware Road, London NW2 6ND

1
The audit in Norfolk, Great Yarmouth and Waveney has given us a strong picture of local neurology services for the first time. The clear recommendations NCS has provided will help us to make effective decisions about neurology services in the future.” Anne Dray Director of Development NHS Norfolk and Waveney
‘‘