neuroblastoma in adults and adolescents : an indolent course with poor survival
TRANSCRIPT
2028
Neuroblastoma in Adults and AdolescentsAn Indolent Course with Poor Survival
BACKGROUND. Neuroblastoma rarely occurs in adults, and less than 10% of casesLoraine M. Franks, M.D.1
Andrew Bollen, M.D.2 occur in patients older than 10 years. It has been suggested that the behavior of
this disease may be different in older patients than in young children. The purposeRobert C. Seeger, M.D.3
Daniel O. Stram, Ph.D.4,5 of this study was to investigate the presentation, biologic features, and outcome
of adolescent and adult patients with neuroblastoma to define differences fromKatherine K. Matthay, M.D.1
childhood neuroblastoma.1 Department of Pediatrics, University of Califor- METHODS. Medical record and pathology reviews were conducted for 16 patientsnia, San Francisco, California. age 13 years or older (13–33 years) at diagnosis who presented with neuroblastoma
at the University of California-San Francisco (UCSF) during the period 1968–19952 Department of Pathology, University of Cali-fornia, San Francisco, California. (patients with intracerebral tumors, esthesioneuroblastoma, or ganglioneuroma
were excluded). Six of these patients received their original diagnosis at UCSF, and3 Department of Pediatrics, University of South-the others were referred after diagnosis. The survival for the same period for allern California, and Children’s Hospital, Los
Angeles, California. neuroblastoma patients ages 13–18 years (n Å 38) registered in the Children’s
Cancer Group (CCG) was compared with the survival for those ages 1–13 years (n4 Children’s Cancer Group, Arcadia, California.Å 1912). Three of the UCSF patients were enrolled in CCG studies.
5 Department of Preventive Medicine, University RESULTS. Biologic characteristics observed in adolescents and adults differedof Southern California, Los Angeles, California.
from those observed in younger patients. In the UCSF population, only 6 of
15 tested patients age 13 or older had elevated urinary catecholamines, and
0 of 6 tested patients had MYCN amplification. There were two patients with
Stage I disease, three with Stage II, two with Stage III, and nine with Stage IV.
Primary sites were adrenal, pelvic, and retroperitoneal in four cases each;
mediastinal in two cases; and paraspinal in two cases. Metastases in nine
patients at diagnosis were observed in bone in five; in bone marrow in four;
in lymph nodes in three; in the liver in two; and in the pleura, breast, and
dura in one patient each. 131I-metaiodobenzylguanidine uptake was observed
in 9 of 11 patients. Initial treatment included surgery for 13 of 16 patients,
chemotherapy for 10 of 16, radiation therapy for 7 of 16, and autologous bone
marrow transplantation for 1 of 16. Relapses occurred in 15 of 16 patients and
death in 13 of 16, with overall survival 30% 5 years after diagnosis. Only 1
patient currently remains free of clinical disease 24 months after diagnosis.
Several of these patients had long courses from diagnosis to death, with multi-
ple recurrences and/or chronic, persistent disease. In the CCG data base, 76%Supported in part by Children’s Cancer Groupof patients ages 13 – 18 years had metastatic disease at diagnosis. In this group,CA13539 from Division of Cancer Treatment,
Department of Health and Human Services, and only 1 of 32 had MYCN amplification. The actuarial survival of all CCG patientsby the generous support of the Conner Fund, ages 13 – 18 years was 7% at 5 years and 4% at 10 years, whereas that forCampini Foundation, and Cynthia Freeman patients ages 1 – 13 years was 30% at 5 years and 23% at 10 years.Fund.
CONCLUSIONS. Neuroblastoma in adolescents and adults has different biologic
characteristics and a longer course than in children; nevertheless, ultimatelyAddress for reprints: Katherine K. Matthay,M.D., Department of Pediatrics, Box 0106, Uni- the outcome is poor regardless of stage. A much more aggressive or innovativeversity of California Medical Center, San Fran- therapeutic approach is needed for these patients. Cancer 1997; 79:2028 – 35.cisco, CA 94143-0106.
q 1997 American Cancer Society.
Received January 31, 1997; accepted February15, 1997. KEYWORDS: neuroblastoma, adult, adolescent, outcome.
q 1997 American Cancer Society
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer

Neuroblastoma in Adults/Franks et al. 2029
N hood neuroblastoma for survival and MYCN gene am-plification.
euroblastoma, a tumor of neural crest cells arisingin the sympathetic nervous system, is the most
common extracranial solid tumor in children, com-prising 8–10% of childhood cancers, and up to nearly MATERIALS AND METHODS
The detailed clinical study included all patients ¢1350% of cancer in newborn infants. Neuroblastoma istypically a tumor of early childhood, with 36% of pa- years of age with neuroblastoma who were evaluated
at the UCSF between January 1, 1968 and August 1,tients diagnosed before the age of 1 year, 75% beforeage 5 years, and ú90% before age 10 years.1–3 It is a 1995. Six of these patients received their original diag-
nosis at UCSF, whereas the other ten were referredtumor with marked biologic heterogeneity, and corre-spondingly variable prognosis, shown to correlate with after diagnosis. Original pathologic diagnosis was
made on tissue sections of biopsy or surgical speci-a variety of clinical, laboratory, and molecular parame-ters. Risk groups can be defined in children with neu- mens, and pathology for all 16 patients was reviewed
by pathologists at UCSF, and confirmed to be neuro-roblastoma receiving current standard therapy ac-cording to a number of these factors, most often in- blastoma. Patients with intracranial primary tumors
and those found to have esthesioneuroblastoma orcluding the minimum evaluation of anatomic stage,age °1 year at diagnosis, histopathologic classifica- ganglioneuroma were excluded. Sixteen patients met
these criteria for neuroblastoma, and were reviewedtion, and MYCN gene amplification.2–6 For example,children with Evans Stage I and II disease have ú90% for this study. There were 9 males and 7 females, rang-
ing in age from 13 to 33 years at diagnosis. Clinicalsurvival with surgical treatment only,4,7 and the cur-rent outlook for those patients with Stage III disease information was obtained by patient chart review and
recent follow-up through contact with the patient’sis excellent using multimodality therapy (in the rangeof 70% of patients overall, and 90% for those with physician. Staging of disease was performed in each
case using the criteria of Evans et al.4 Other clinicalfavorable histopathology and single copy MYCN).8,9 In-fants with Stage IV disease have an estimated survival and biologic factors, including sites of metastatic dis-
ease, MYCN oncogene amplification, and urinary cate-of 60–70%, but if subgroups with tumors containingonly single copy MYCN or those with hyperdiploid tu- cholamine metabolites, were recorded when available.
The type and extent of treatment received was re-mors are examined, the survival is ú95%.3,10–12 Chil-dren older than age 1 year at diagnosis with Stage IV corded, as well as the outcome in each case.
In addition, to obtain the benefit of larger num-neuroblastoma still have a relatively poor prognosis,with survival in the range of 20–30%, despite intensive bers (although with less detailed clinical information),
the authors extracted from the CCG database themultimodality therapy that frequently includes abla-tive chemotherapy and autologous bone marrow or stage, age, MYCN oncogene copy number, and follow-
up information on all patients with neuroblastomaperipheral blood stem cell transplantation.3,2,13–18
The rare adult patient with neuroblastoma may registered from 1973 to 1993. This included 3 of the16 UCSF patients. All patients in the CCG databasehave a very different outcome from pediatric patients.
The scattered reports in the medical literature of adults are °18 years of age at diagnosis. Life tables werecalculated using Kaplan and Meier analysis to estimatewith this disease suggest that, at least in some cases,
long term survival may be worse than for younger pa- survival.27
tients, even in patients with localized disease, althoughthe course may be more prolonged.19–26 A paucity of RESULTS
Patient characteristicsinformation is available on the relevance of stage,MYCN amplification, and histopathology to prognosis The characteristics and treatments of the patients
from UCSF are shown in Table 1. Of the 16 patientsin the adolescent and adult patient. Therefore, the au-thors undertook a detailed retrospective analysis of all studied, 9 were male and 7 were female. The median
age at diagnosis was 22 years and 8 months (range,patients ¢13 years of age diagnosed with neuro-blastoma at the University of California, San Francisco 13–33 years). At the time of diagnosis, two patients
had Evans Stage I disease, three patients had Stage II(UCSF) over the past 25 years to further study thebiologic and clinical heterogeneity in this disease with disease, two patients had Stage III disease, and nine
patients had Stage IV disease. Of note, 6 of 7 of therespect to the effect of stage, age, and biologic factorson the disease course and survival. In addition, an adolescent patients age 13–18 years had Stage IV dis-
ease, whereas only 3 of 9 of the patients ú18 yearsadolescent group (range, 13–18 years) diagnosed withneuroblastoma and registered with the Children’s had Stage IV disease. The primary site of tumor was
the pelvis in four patients, the adrenal gland in fourCancer Group (CCG) was studied to acquire a largernumber of patients to compare with cases of child- patients, the retroperitoneum in four patients, the me-
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer

2030 CANCER May 15, 1997 / Volume 79 / Number 10
TABLE 1University of California San Francisco Patient Characteristics
Age Therapy atStage UPN (yrs) Gender Primary site Metastases at diagnosis Time to first progession/death diagnosis
I 16 13 M Retroperitoneum — 1 y 10 mos/21 yrs 6 mos S, RI 6 30 F Pelvis — 3 yrs 4 mos/11 yrs 5 mos SII 7 20 M Thoracic spine — CR 0 24 mos from dx S, C, RII 10 25 M Pelvis — 4 yrs 3mos/5 yrs 2mos S, C, RII 5 33 F Epidural space — 2 yrs 5 mos/4 yrs 1 mo S, RIII 2 32 M Mediastinum — 2 yrs 11 mos/16 yrs 5 mos S, CIII 9 36 F Adrenal — 1 yr/AWD 0 2 yrs from dx S, C, RIV 8 15 F Pelvis Brain, breast, spine, bone 1 yr 2 mos/2 yrs 9 mos C
marrowIV 14 15 M Pelvis Paratracheal, pleura 4 mos/1 yr 7 mos RIV 13 16 F Adrenal Liver, paravertebral, DWD 0 2 m from dx S
cervical lymph nodesIV 11 16 M Mediastinum Bone marrow, 6 mos/1 yr 10 mos C, R
subcutaneousIV 15 17 M Adrenal Skull, spine, scapula, 3 yrs 9 mos/4 yrs 10 mos S, C
pelvis, femur,humerus
IV 1 18 M Adrenal Bone marrow, skull, 2 yrs/3 yrs 5 mos S, C, BMT (TBI)spine, long bones,supraclavicular lymphnodes
IV 12 25 F Retroperitoneum Mediastinum, liver 6 yrs 11 mos/AWD 11 yrs from dx S, CIV 3 28 M Retroperitoneum Clavicle, mediastinal 4 mos/1 yr 3 mos S, C
lymph nodes, bonemarrow
IV 4 32 F Retroperitoneum Ileum, pelvis 8 mos/3 yrs 7 mos S
UPN: unique patient number; F: female; M: male; CR: clinical remission; dx: diagnosis; AWD: alive with disease; DWD: died with disease; S: surgery; C: chemotherapy; R: radiation therapy; ABMT: autologous
bone marrow transplant; TBI: total body irradiation.
diastinum in two patients, and the epidural space and with 1 patient having elevated vanillylmandelic acid(VMA), homovanillic acid (HVA), and dopamine, 3 pa-thoracic spine in one patient each. Sites of metastatic
disease present at diagnosis in the nine Stage IV pa- tients having elevated VMA and HVA, 1 patient withonly elevated VMA, and 1 patient with only elevatedtients were found in bone in five patients, bone mar-
row in four patients, lymph nodes in three patients, dopamine. Many of the adult and adolescent patientsseen at UCSF were referred for 131I-metaiodobenzyl-liver in two patients, and the pleura, breast, and brain
in one patient each. The pathology was determined to guanidine (MIBG) therapy, and therefore 11 of the 16patients had MIBG scans in an effort to assess thebe neuroblastoma in 12 patients, ganglioneuroblas-
toma in 3 patients, and neuroblastoma with partial extent of disease as well as to evaluate the possibilityof using 131I-MIBG as therapy. Of the 11 patients whogangliocytic differentiation in 1 patient.underwent MIBG scans, 9 had MIBG uptake in theareas of disease.Biology
None of the six patients tested at UCSF showed tumorMYCN amplification. This is in accord with the larger Treatment and Course
Surgical resection was attempted in 14 of the 16 pa-number of adolescent tumor samples available fortesting in the CCG Biology Reference Laboratory, in tients. In the two patients with Stage I disease, both
had complete resection of the primary tumor at diag-which only 1 of the 32 tumors from adolescents age13–18 years at diagnosis showed amplification of the nosis. However, both had recurrences of disease, one
with distant metastases at 1 year and 10 months andMYCN gene. In contrast, in the CCG database, 20% ofpatients ageõ13 years had an increased tumor MYCN the other with a local recurrence at 3 years and 5
months from diagnosis. The three patients with Stagecopy number.5 Only 6 of 15 patients (40%) seen atUCSF showed elevation of urinary catecholamines, II disease all underwent partial surgical resections at
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer
Neuroblastoma in Adults/Franks et al. 2031
the time of diagnosis. Two of these tumors were para-spinal with epidural extension, the other involved thepelvis, and all had ú90%, but not complete resection.Of these 3 patients, 1 had an initial local recurrence(2 years and 5 months from diagnosis), 1 had a distantrecurrence (4 years and 3 months from diagnosis), and1 was in clinical remission 2 years from diagnosis. Eachof the 2 patients with Stage III disease underwent par-tial resections initially; 1 went on to have local recur-rence at 2 years and 11 months, and the other had adistant recurrence 1 year later. Of the nine patientswith Stage IV disease, two underwent biopsy only, andthe remaining seven underwent more extensive resec-tions attempted of either the primary tumor and/ormetastases, including one patient with a pelvic pri-
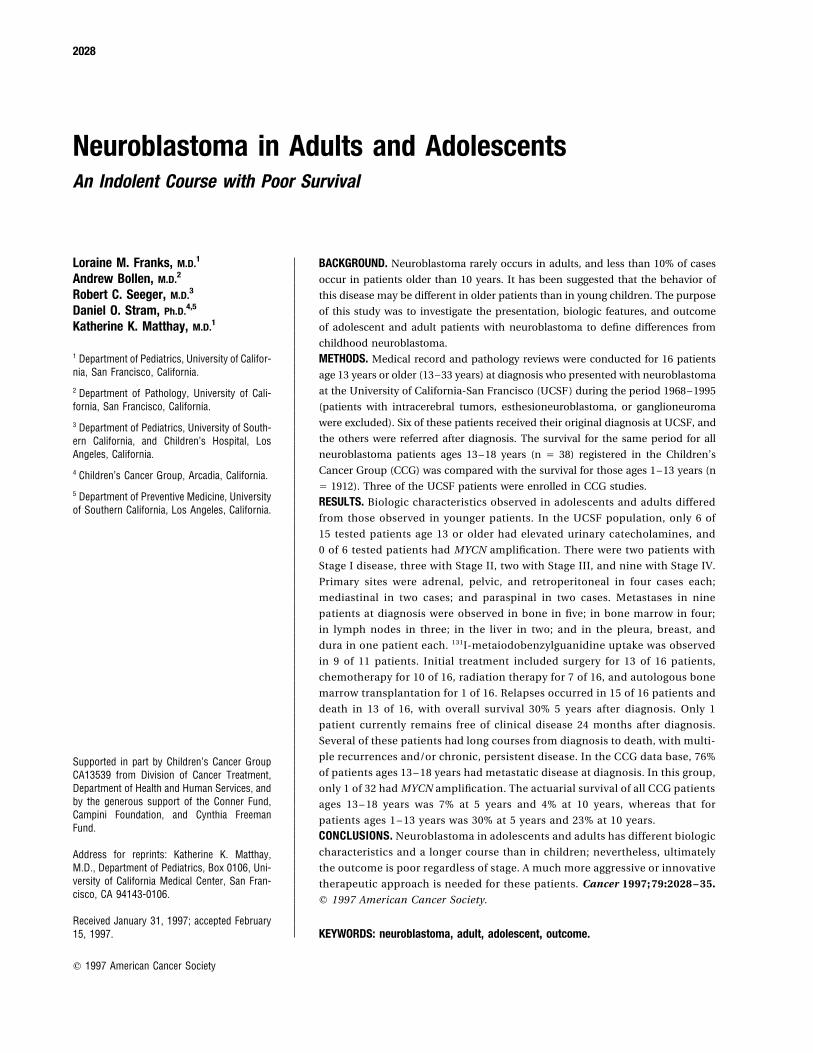
FIGURE 1. Overall survival of adult and adolescent patients with neuro-mary tumor who underwent a partial resection of ablastoma seen at the University of California at San Francisco (n Å 16).brain metastasis to relieve increased intracranial pres-
sure; the pathologic diagnosis was made from thisspecimen. Eight of the nine patients with Stage IV dis-ease had progressive disease after initial surgery and chemotherapy (unique patient number [UPN] 5).
Three other patients with localized disease receivedtherapy, with initial recurrence at the primary tumorsite in four patients and distant metastases in four chemotherapy only after recurrent disease was found,
2–4 years after the original diagnosis. One of the 15patients. The remaining patient with Stage IV diseasedied 2 months from diagnosis after having refused patients underwent ABMT preceded by myeloablative
chemotherapy and TBI as part of initial therapy. Onetreatment. Overall, of 14 patients who underwent at-tempts at initial resection of the primary tumor, there patient underwent ABMT after recurrence, and two
patients with recurrent disease received ABMT or pe-were 7 local recurrences and 5 distant failures, 1 pa-tient was in clinical remission at last follow-up, and 1 ripheral blood stem cell rescue after 131I-MIBG treat-
ment.patient died 2 months after diagnosis.Radiation therapy was received by 13 of the 16 Disease recurrence or progression was docu-
mented in 15 of the 16 patients studied. The exceptionpatients at some time during the course of their treat-ment, including 2 patients who received total body was 1 patient with Stage II disease who was in clinical
remission 24 months from diagnosis. One patient withirradiation (TBI) as conditioning for autologous bonemarrow transplantation (ABMT). These two patients Stage IV disease died within 2 months of diagnosis
after having refused therapy. The remaining 14 pa-also received radiation therapy to primary tumor sitesduring subsequent recurrences. Seven patients under- tients had progression or recurrences of the neuro-
blastoma; 7 had initial local or regional recurrenceswent radiation therapy as part of the initial treatment.Only one of these patients had local tumor recurrence, occurring from 1 year and 2 months to 6 years and 11
months after the original diagnosis (median, 2 yearsbut five had distant recurrence. One patient receivedintraoperative radiation therapy to a recurrent local and 11 months) and the remaining 7 patients had ini-
tial distant recurrences occurring from 4 months to 4tumor in the abdomen. One patient received heavyparticle radiation to a spinal metastasis. years and 3 months after the original diagnosis (me-
dian, 8 months).Thirteen patients received standard chemothera-peutic agents, including cyclophosphamide or ifos- The ultimate survival of adults and adolescents
with neuroblastoma at UCSF in this study is poor, withfamide in 13 patients, doxorubicin in 12 patients, eto-poside in 12 patients, cisplatin or carboplatin in 11 75% survival at 2 years, 44% survival at 5 years, 37%
survival at 10 years, and 10% survival at 20 years frompatients, vincristine in 7 patients, dacarbazine in 5patients, and miscellaneous other drugs in 7 patients. diagnosis (Fig. 1). At last follow-up, 13 of the 16 pa-
tients died of disease, from 2 months to 21 years andTen of these patients began therapy at the time ofdiagnosis. Three patients never received chemother- 6 months after diagnosis (median, 3 years and 7
months). Two of the 16 patients were alive with recur-apy, including two with Stage IV disease, of whom 1died 2 months from diagnosis after refusing therapy; rent disease at last follow-up. Both patients had multi-
ple distant metastases, with follow-up at 1 year andthe other received only radiation therapy. One patientwith Stage II disease received only antineoplastin28 11 months and 10 years and 10 months, respectively.
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer
2032 CANCER May 15, 1997 / Volume 79 / Number 10
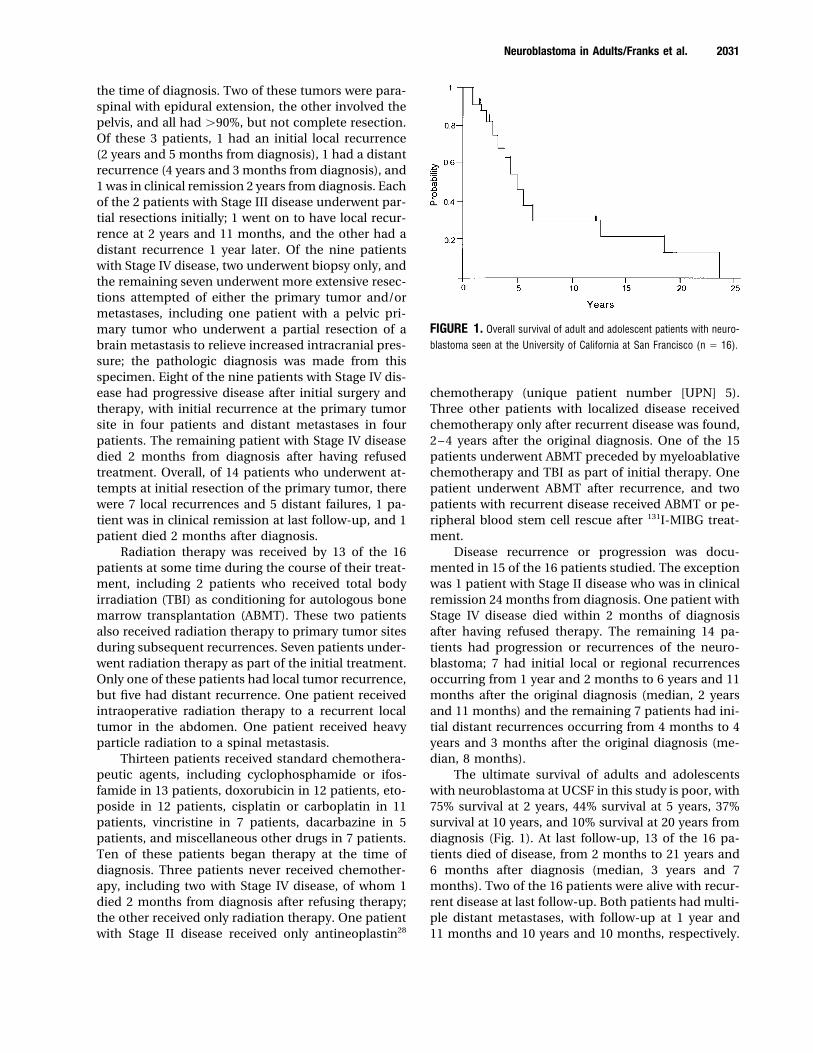
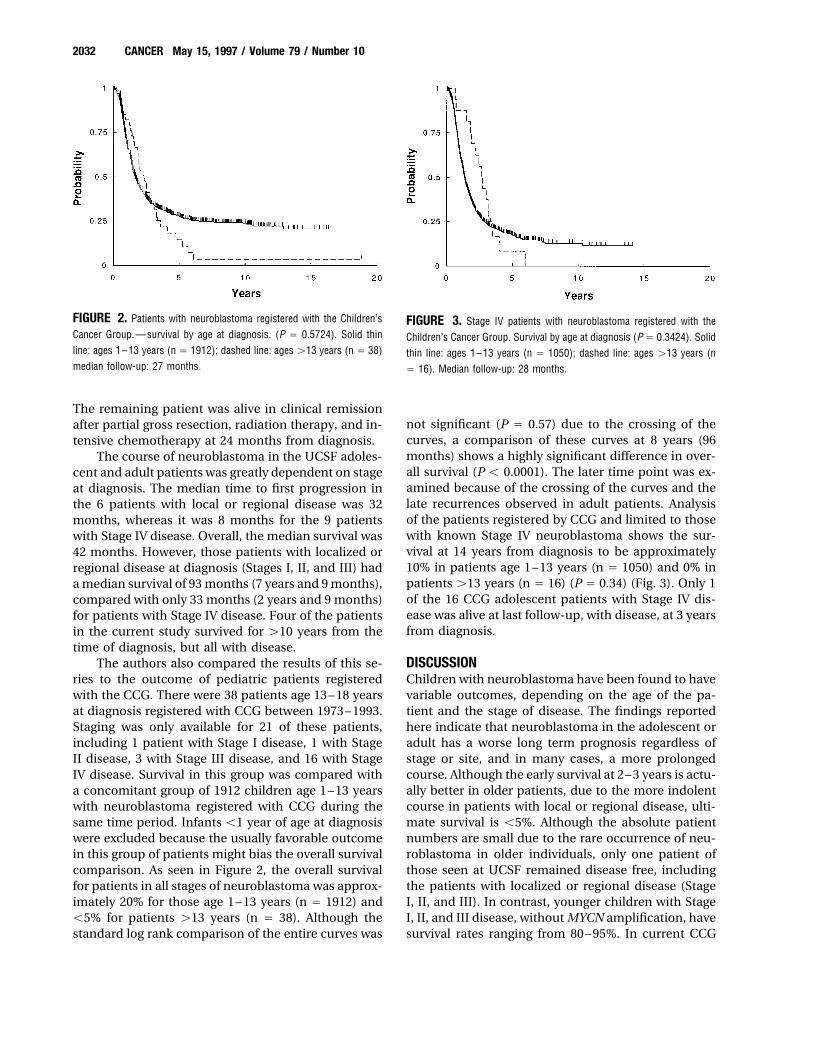
FIGURE 2. Patients with neuroblastoma registered with the Children’s FIGURE 3. Stage IV patients with neuroblastoma registered with theCancer Group.—survival by age at diagnosis. (P Å 0.5724). Solid thin Children’s Cancer Group. Survival by age at diagnosis (P Å 0.3424). Solidline: ages 1–13 years (n Å 1912); dashed line: ages ú13 years (n Å 38) thin line: ages 1–13 years (n Å 1050); dashed line: ages ú13 years (nmedian follow-up: 27 months. Å 16). Median follow-up: 28 months.
The remaining patient was alive in clinical remissionnot significant (P Å 0.57) due to the crossing of theafter partial gross resection, radiation therapy, and in-curves, a comparison of these curves at 8 years (96tensive chemotherapy at 24 months from diagnosis.months) shows a highly significant difference in over-The course of neuroblastoma in the UCSF adoles-all survival (P õ 0.0001). The later time point was ex-cent and adult patients was greatly dependent on stageamined because of the crossing of the curves and theat diagnosis. The median time to first progression inlate recurrences observed in adult patients. Analysisthe 6 patients with local or regional disease was 32of the patients registered by CCG and limited to thosemonths, whereas it was 8 months for the 9 patientswith known Stage IV neuroblastoma shows the sur-with Stage IV disease. Overall, the median survival wasvival at 14 years from diagnosis to be approximately42 months. However, those patients with localized or10% in patients age 1–13 years (n Å 1050) and 0% inregional disease at diagnosis (Stages I, II, and III) hadpatients ú13 years (n Å 16) (P Å 0.34) (Fig. 3). Only 1a median survival of 93 months (7 years and 9 months),of the 16 CCG adolescent patients with Stage IV dis-compared with only 33 months (2 years and 9 months)ease was alive at last follow-up, with disease, at 3 yearsfor patients with Stage IV disease. Four of the patientsfrom diagnosis.in the current study survived for ú10 years from the
time of diagnosis, but all with disease.The authors also compared the results of this se- DISCUSSION
Children with neuroblastoma have been found to haveries to the outcome of pediatric patients registeredwith the CCG. There were 38 patients age 13–18 years variable outcomes, depending on the age of the pa-
tient and the stage of disease. The findings reportedat diagnosis registered with CCG between 1973–1993.Staging was only available for 21 of these patients, here indicate that neuroblastoma in the adolescent or
adult has a worse long term prognosis regardless ofincluding 1 patient with Stage I disease, 1 with StageII disease, 3 with Stage III disease, and 16 with Stage stage or site, and in many cases, a more prolonged
course. Although the early survival at 2–3 years is actu-IV disease. Survival in this group was compared witha concomitant group of 1912 children age 1–13 years ally better in older patients, due to the more indolent
course in patients with local or regional disease, ulti-with neuroblastoma registered with CCG during thesame time period. Infants õ1 year of age at diagnosis mate survival is õ5%. Although the absolute patient
numbers are small due to the rare occurrence of neu-were excluded because the usually favorable outcomein this group of patients might bias the overall survival roblastoma in older individuals, only one patient of
those seen at UCSF remained disease free, includingcomparison. As seen in Figure 2, the overall survivalfor patients in all stages of neuroblastoma was approx- the patients with localized or regional disease (Stage
I, II, and III). In contrast, younger children with Stageimately 20% for those age 1–13 years (n Å 1912) andõ5% for patients ú13 years (n Å 38). Although the I, II, and III disease, without MYCN amplification, have
survival rates ranging from 80–95%. In current CCGstandard log rank comparison of the entire curves was
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer

Neuroblastoma in Adults/Franks et al. 2033
TABLE 2Literature Review: Summary of Outcome
No. of patients Age range No. dead of disease No. alive with disease No. alive, no diseaseReference (M:F) (yrs) (mos from dx) (mos from dx) (mos from dx)
Lopez et al. (1980)19 4 (0:4) 17–52 2 (3–16) 1 (23) 1 (35)Tang et al. (1975)20 27 (16:11) 15 ú 50 24 (NR) 3 patients alive ú5 yrs, with no report of disease statusAllan et al. (1986)21 3 (1:2) 25–34 3 (20–69) 0 0Dosik et al. (1978)22 6 (3:3) 16–37 2 (2–17) 2 (11–18) 2 (8)Aleshire et al. (1985)23 8 (5:3) 26–75 4 (7–18) 1 (32) 3 (32–54)Prestidge et al. (1989)24 5 (2:3) 18–34 3 (10–62) 2 (44–133) 0Grubb et al. (1984)25 1 (0:1) 58 0 0 1 (48)Kaye et al. (1985)26 3 (0:3) 20–38 1 (18) 2 (4–20) 0Total 57 (27:30) 15–75 39 (2–69) 8 (4–133) 7 (8–54)
F: female; M: male; dex: diagnosis; mos: months; NR: not reported.
study 3881, those rare patients who developed disease given the prolonged recurrence course observed insome of the patients in the current study.progression did so early, within 12 months of diagno-
sis, unlike the long median time to progression of 32 In the patients seen at UCSF, the primary tumorsoccurred in similar locations to that of younger pa-months observed in the UCSF adult/adolescent pa-
tients. Although in UCSF patients with Stage IV disease tients, with abdominal primaries being the most com-mon. The lower percentage of abdominal primary tu-the median time to progression was 8 months, similar
to younger children, there were 2 patients with very mors observed in the adult patients at UCSF (8 of 16)is in accord with the literature review in which in 57late first recurrences, at 45 and 83 months, respec-
tively. The authors also observed several patients with patients, the primary site was thoracic in 19% (n Å11), abdominal in 44% (n Å 25), cervical in 12% (n Åprolonged survival and multiple recurrences after first
recurrence, in contrast to the usual brief 3–4-month 7), pelvic in 9% (n Å 5), and in an extremity in 2% (nÅ 1). Approximately 14% (n Å 8) had multiple tumorsmedian survival observed in children with Stage IV
disease recurring after transplant. The median time present at diagnosis with no identifiable primary site.Although the numbers are small, there was a higherfrom recurrence to death for UCSF adult/adolescent
patients was 17 months, but included 4 of 15 patients proportion of pelvic tumors (25%) in the current series,which in young children are said to have a more favor-with ú4 years survival after recurrence prior to death.
Adolescent patients registered on CCG protocols were able outcome than primary tumors in other locations,particularly in patients with Stage III and IV disease,less likely than the UCSF group to exhibit any referral
bias, but showed a similar poor outcome and pro- in which the 3-year progression free survival was 70%for pelvic lesions compared with 47% for nonpelviclonged course. Although the survival curves of the chil-
dren age 1–13 years and the adolescents ú13 years tumors.29 In addition, pelvic tumors in young patientsmore commonly had favorable biologic factors thanoverlap initially, the curves separate after 5 years, re-
sulting in a highly significant difference in long term tumors observed elsewhere. In contrast, all the pelvictumors in the current UCSF series recurred. Metastaticsurvival, even though the overall comparison of the
Kaplan–Meier analysis was not significant. disease occurred in a similar pattern in children andadolescent/adults, with the bone marrow, lymphIn a review of the pertinent literature, 57 adoles-
cent and adult patients with neuroblastoma have been nodes, bone, and liver being the most common sites,although the frequency of bone marrow involvementreported in 8 separate reviews since 1975.19–26 The age
range was 15–75 years. Five patients were Evans Stage in the current UCSF series of adults and adolescentswith Stage IV disease appeared to be lower than inI at diagnosis, 9 patients were Stage II, 7 patients were
Stage III, and 36 patients were Stage IV. The overall younger children.Pathologically, the tumors were identical to thosepatient outcomes are summarized in Table 2. The sur-
vival by stage is seen in Table 3, for those patients in observed in children, with a range of differentiationfrom immature neuroblastoma to ganglioneuroblas-whom this information was available (n Å 30). It is
important to note that although 7 of 30 patients in the toma. It is interesting that none of the 6 tumors testedat UCSF and only 1 of 32 tumors from CCG had MYCNliterature were alive without disease, follow-up ranged
from only 8 to 54 months, which is relatively short oncogene amplification, a finding usually reported in
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer

2034 CANCER May 15, 1997 / Volume 79 / Number 10
TABLE 3Literature Review: Outcome by Stage (n Å 30)
No. of No. dead of disease No. alive with disease No. alive, without diseasepatients (mos from dx) (mos from dx) (mos from dx)
Stage I 4 2 (12–18) 0 2 (32–54)Stage II 5 0 3 (22–133) 2 (32–48)Stage III 5 3 (7–20) 1 (20) 1 (8)Stage IV 16 10 (3–69) 4 (11–44) 2 (8–35)Total 30 15 (3–69) 8 (11–133) 7 (8–54)
n: number of patients; dx: diagnosis.
20–30% of neuroblastomas in younger children.5 In approach may be inappropriate in patients with adultneuroblastoma because of the much worse prognosisaddition, only 40% of the current series of tumors se-
creted catecholamine metabolites, which is much of adults with localized neuroblastoma compared withchildren with similar involvement, for whom surgerylower than the 90% reported in pediatric patients with
neuroblastoma.3 It is possible that these differences, alone is often sufficient therapy.9 Although the authorscannot conclude that intensive therapy, even withsuch as lack of MYCN amplification, may be part of
the different biologic behavior, including the slower ABMT, would improve survival in adults, it is possiblethat more aggressive initial therapy including radia-progression of neuroblastoma in adults.
The treatment of the patient group seen at UCSF tion and chemotherapy may be of benefit, even inpatients with low stage disease.was variable, but 13 of the patients received intensive
combination chemotherapy with active agents, 10 ofwhom were treated from diagnosis. All but two pa-
CONCLUSIONStients underwent surgical resection, either completeThere are currently no standard treatment guidelinesor partial, depending on the location and extent of thefor patients who present with neuroblastoma aftertumor and the presence of metastatic disease. Radia-early childhood. Given the UCSF experience, as welltion therapy was also varied and was given to 13 ofas the findings in CCG and the literature review, ado-the 16 patients, but often after recurrence. The authorslescents and adults with localized disease who havealso reported two adult patients with neuroblastomabeen treated conservatively in the past may benefitwho were treated with ABMT. Both of these patientsfrom more intensive initial therapy. Those patientshad local recurrences at 13 and 17 months, respec-with advanced disease at diagnosis have had a uni-tively, after transplant, and both subsequently died.formly poor prognosis, similar to younger childrenEven with intensive or myeloablative therapy, thewith metastatic neuroblastoma. It is unclear if longeroutcome was poor for these patients. However, thecourses of therapy or more intensive treatment willpatients with more advanced disease at diagnosis wereeventually make a difference in the outcomes of thesethose that received the most intensive treatment,patients. In addition, the role of differentiating agentswhereas patients with localized or minimal diseaseor other biologic approaches, such as immunologicwere often observed clinically after resection, with notherapy, are currently being studied and may be usedinitial chemotherapy or radiation. It was only afterincreasingly in these patients. It is also imperative thatsubsequent recurrences in these patients with lowerbiologic studies continue on tumor tissue from adultstage disease that further therapy was administered.patients to discover why these tumors behave differ-The one patient who was recently diagnosed (UPNently, and why they lack MYCN amplification and are7) did receive intensive chemotherapy and radiationoften negative for catecholamine secretion.therapy after gross surgical resection of an epidural
neuroblastoma. In the other localized cases, the treat-ment was comparable to the treatment usually given REFERENCES
1. Matthay KK, Schwartz A. Congenital malignant disorders.to younger patients, in whom patients with localizedIn: Ballard R, Avery M, Taeusch W, editors. Diseases of theneuroblastoma are treated with surgery and, only oc-newborn. Philadelphia: W.B. Saunders Company, 1991:casionally, radiation. Children with disseminated neu-1025–48.
roblastoma are routinely treated with aggressive che- 2. Matthay KK. Neuroblastoma. In: Pochedly C, editor. Neo-motherapy, radiation therapy, surgery, and occasion- plastic diseases in childhood. Harwood Academic Publish-
ers, 1994:735–78.ally myeloablative therapy with ABMT. This risk-based
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer
Neuroblastoma in Adults/Franks et al. 2035
3. Brodeur GM, Castleberry RP. Neuroblastoma. In: Pizzo PA, 15. Philip T, Zucker JM, Bernard JL, Lutz P, Bordigoni P, PlouvierE, et al. Improved survival at 2 and 5 years in the LMCE1Poplack DG, editors. Principles and practice of pediatric on-
cology. 2nd edition. Philadelphia: J.B. Lippincott Company, unselected group of 72 children with stage IV neuroblastomaolder than 1 year of age at diagnosis: is cure possible in a1993:739–68.
4. Evans AE, D’Angio GD, Randolph J. A proposed staging for small subgroup? J Clin Oncol 1991;9:1037–44.16. Pole J, Casper J, Elfenbein G, Gee A, Gross S, Janssen W,children with neuroblastoma: Children’s Cancer Study
Group A. Cancer 1971;27:374–8. et al. High-dose chemoradiotherapy supported by marrowinfusions for advanced neuroblastoma: a Pediatric Oncology5. Seeger RC, Brodeur GM, Sather H, Dalton A, Siegel SE, Wong
KY, et al. Association of multiple copies of the N-myc onco- Group study [published erratum appears in J Clin Oncol1991;9(6):1094]. J Clin Oncol 1991;9:152–8.gene with rapid progression of neuroblastoma. N Engl J Med
1985;313:1111–6. 17. Dini G, Lanino E, Garaventa A, Rogers D, Dallorso S, ViscoliC, et al. Myeloablative therapy and unpurged autologous6. Shimada H, Chatten J, Newton WA, Sachs N, Hamoudi AB,
Chiba T, et al. Histopathologic prognostic factors in neuro- bone marrow transplantation for poor-prognosis neuro-blastoma: report of 34 cases. J Clin Oncol 1991;9:962–9.blastic tumors: definition of subtypes of ganglioneuroblas-
toma and an age-linked classification of neuroblastomas. J 18. Ohnuma N, Takahashi H, Kaneko M, Uchino J, Takeda T,Iwafuchi M, et al. Treatment combined with bone marrowNatl Cancer Inst 1984;73:405–16.
7. Nitschke R, Smith EI, Shochat S, Altshuler G, Travers H, transplantation for advanced neuroblastoma: an analysis ofpatients who were pretreated intensively with the protocolShuster JJ, et al. Localized neuroblastoma treated by surgery.
A Pediatric Oncology Group Study. J Clin Oncol 1988; of the Study Group of Japan. Med Pediatr Oncol 1995;24:181–7.6(8):1271–9.
8. West DC, Shamberger RC, Macklis RM, Kozakewich HP, 19. Lopez R, Karakousis C, Rao U. Treatment of adult neuro-blastoma. Cancer 1980;45:840–4.Wayne AS, Kreissman S, et al. Stage III neuroblastoma over
1 year of age at diagnosis: improved survival with intensive 20. Tang CK, Hajdu SI. Neuroblastoma in adolescence andadulthood. NY State J Med 1975;1434–8.multimodality therapy including multiple alkylating agents.
J Clin Oncol 1993;11(1):84–90. 21. Allan SG, Cornbleet MA, Carmicael J, Arnott SJ, Smyth JF.Adult neuroblastoma: report of three cases and review of9. Matthay K, Seeger RC, Haase GM, Stram DO, O’Leary M,
Shimada H, et al. Treatment and outcome for stage III neu- the literature. Cancer 1986;57:2419–21.22. Dosik GM, Rodriguez V, Benjamin RS, Bodey GP. Neuro-roblastoma based on prospective biologic staging. Med Pedi-
atr Oncol 1994;23:173. blastoma in the adult. Effective combination chemotherapy.Cancer 1978;41:56–63.10. Strother D, Shuster JJ, McWilliams N, Nitschke R, Smith EI,
Joshi VJ, et al. Results of Pediatric Oncology Group protocol 23. Aleshire SL, Glick AD, Cruz VE, Bradley CA, Parl FF. Neuro-blastoma in adults. Pathologic findings and clinical out-8104 for infants with stages D and DS neuroblastoma. J Pedi-
atr Hematol/Oncol 1995;17(3):254–9. come. Arch Pathol Lab Med 1985;109:352–6.24. Prestidge BR, Donaldson SS. Treatment results among adults11. Look AT, Hayes FA, Nitschke R, McWilliam NB, Green D.
Cellular DNA content as a predictor of response to chemo- with childhood tumors: a 20-year experience. Int J RadiatOncol Biol Phys 1989;17:507–14.therapy in infants with unresectable neuroblastoma. N Engl
J Med 1984;311:231–4. 25. Grubb BP, Thant M. Neuroblastoma in an adult. SouthernMed J 1984;77:1180–2.12. Matthay KK, Luken J, Stram DO, Shimada H, Brodeur G,
Seeger R. Prognosis for stage IV neuroblastoma less than 26. Kaye JA, Warhol MJ, Kretschmar C, Landsberg L, Frei E.Neuroblastoma in adults—three case reports and a reviewone year at diagnosis: a prospective Children’s Cancer
Group Study. Proc Am Soc Clin Oncol 1995;14:446. of the literature. Cancer 1986;58:1149–57.27. Peto R, Pike MC, Armitage P, Breslow NE, Cox DR, Howard13. Stram DO, Matthay KK, O’Leary M, Reynolds CP, Haase GM,
Atkinson JB, et al. Consolidation chemoradiotherapy and SV, et al. Design and analysis of randomized clinical trialsrequiring prolonged observation of each patient. II. Analysisautologous bone marrow transplantation vs. continued che-
motherapy for metastatic neuroblastoma: a report of two and examples. Br J Cancer 1977;35:1–39.28. Burzynski SR. Therapy of high grade glioma in children withconcurrent Children’s Cancer Group studies. J Clin Oncol
1996;14:2417–26. infusions of antineoplastin A10 and AS2-1. Protocol spon-sored by Burzynski Research Institute, Houston, Texas, 1993.14. Matthay KK, Seeger RC, Reynolds CP, Stram DO, O’Leary
M, Harris RE, et al. Allogeneic vs. autologous purged bone 29. Haase GM, O’Leary MC, Stram DO, Lukens JN, Seeger RC,Shimada J, et al. Pelvic neuroblastoma—implications for amarrow transplantation for neuroblastoma: a report from
the Children’s Cancer Group. J Clin Oncol 1994;12(11):2382– new favorable subgroup: a Children’s Cancer Group Experi-ence. Ann Surg Oncol 1995;2(6):516–23.9.
/ 7b56$$1078 04-18-97 00:18:08 cana W: Cancer