neuro exam cctp papp 1-8-2019
TRANSCRIPT
1
Newborn Neurological Assessment
Elizabeth Papp, MSN, RN, CNS, FNP
Content Credit & Gratitude: Sue Peloquin, MS, RN, PNP
October 12th, 2018

2
Objectives
•Review components of the newborn neurological assessment
• Identify normal findings
• Identify abnormal findings
• What do these findings mean?
Value of the neonatal neurological examination
1. Detect lesions in the CNS
2. Detect lesions in the peripheral nervous system
3. Determine severity of abnormalities
4. Confirm a baby is/isn’t at risk on admission
5. To evaluate change in clinical status
6. Planning investigations/follow up
7. Predict outcomes/Parental counseling
3

Anatomy!
4
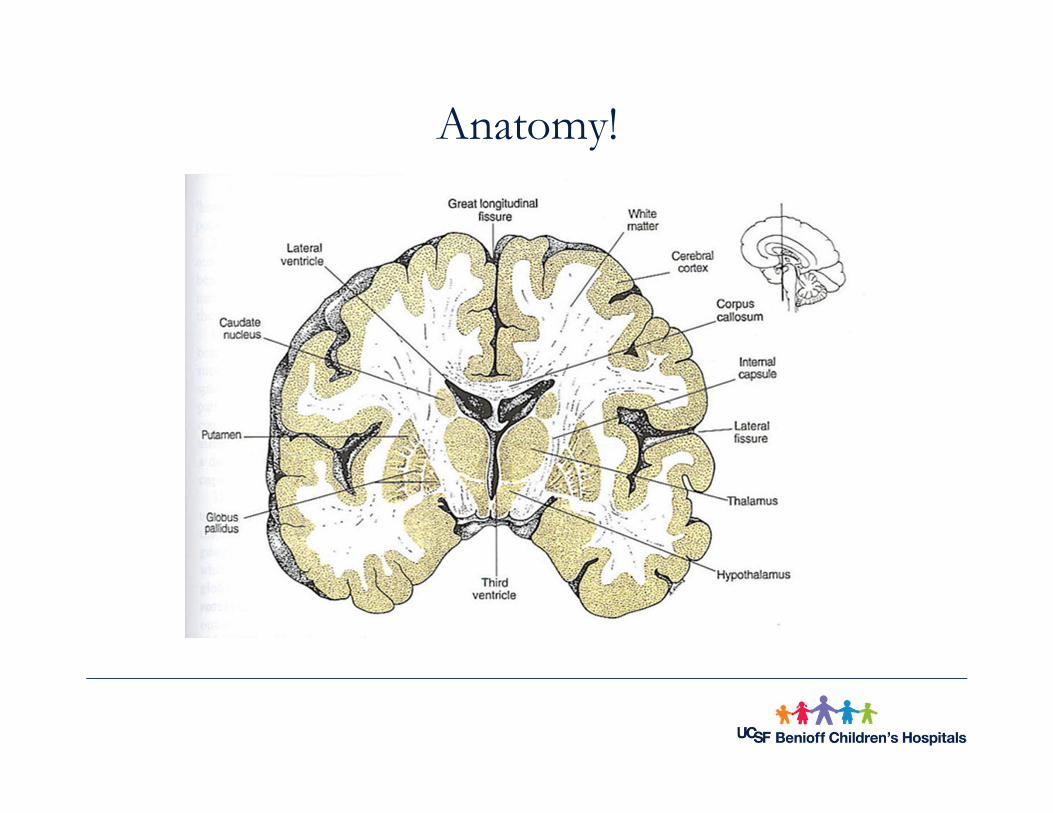
Anatomy!
5

What do we mean when we say WNL?
▪ Alert without irritability, jitteriness, or lethargy
▪ Responds appropriately to stimulation
▪ Absence of seizure activity
▪ Cry is present without hoarseness, shrillness, or weakness (or infant is intubated)
▪ Face symmetrical
▪ Moves all extremities equally and spontaneously
▪ Moro, grasp and suck reflexes are present
▪ Pupil reaction is brisk, pupil size is WNL
▪ Absence of neuro drains or monitoring devices
6

Before starting your neuro exam…▪ Gestational age at birth
▪ Gestational age now
▪ Head circumference at birth
▪ Head circumference now
▪ Head shape/sutures
▪ Dysmorphisms
▪ Respiratory support
▪ Medications
▪ Encephalopathic
7

Normal Newborn Exam
8 Newborn Neuro Exam - Normal

Systematic Neurologic Exam
9

Neonatal Neurological Assessment
General appearance
Mental status
Cranial nerves
Motor exam
Reflexes
Coordination
Sensory
Wt, Lth, HC, dysmorphismWakefulness, behaviorPupils, grimace, gag, reflexesBulk, power, toneDeep tendon & primitiveGeneral movementsLight touch, pain, temp

General Appearance
▪ Appearance: remove infant’s covers without awakening and observe the patient for:
• Weight/length proportion for gestation
• Head shape and size
▪ State
▪ Skin
▪ Dysmorphic features
▪ Symmetry
11

General Appearance
12

General Appearance
13

14
Cortical Thumb

15
Port Wine Stain

Café Au Lait
16

Sacral Skin Tag
17

Sacral Dimple
18

Head
19
Full term head circumference = 35 cm +/- 2 cm

20
Hair Whorl

21
Sutures and Fontanelles
• There are a total of 6 fontanelles
• Palpate anterior and posterior fontanelles as part of your neuro assessment
• Fontanelles are commonly used to evaluate ICP
• Size in newborns is quite variable

Bulging Fontanelle
22

Head Shapes
23
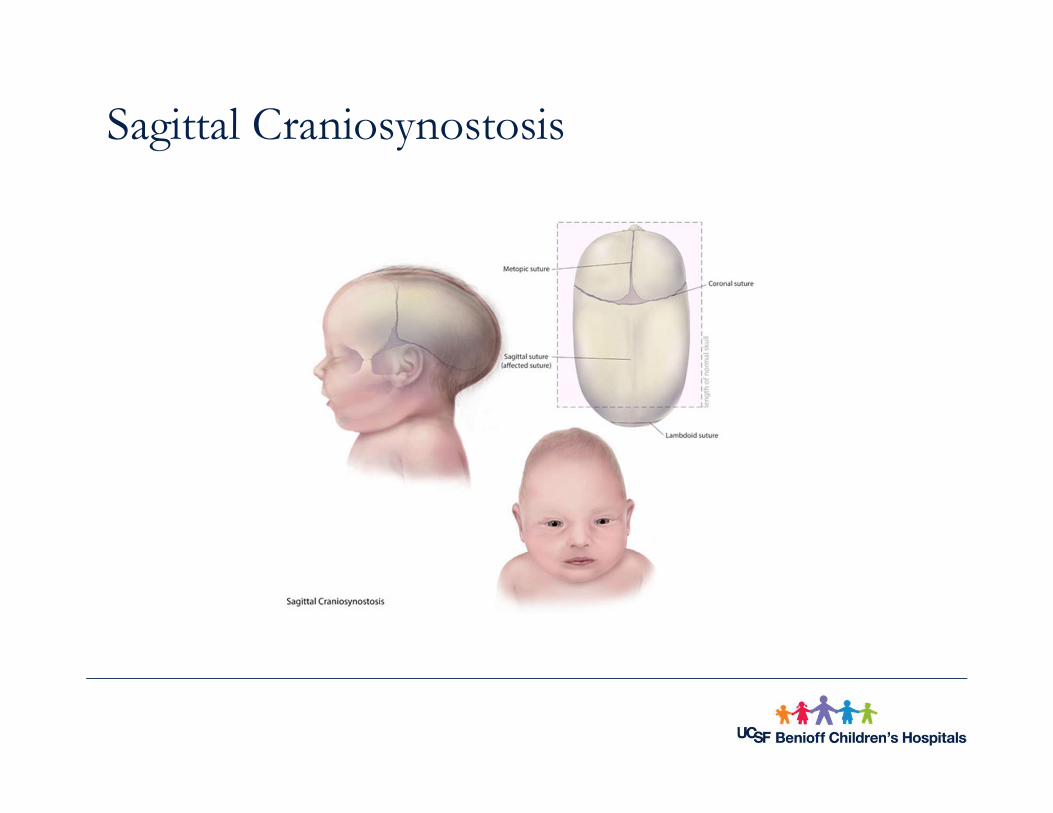
Sagittal Craniosynostosis
24

Microcephaly
25

Macrocephaly
26

27
Hydrocephalus
Hydrocephalus means water on the brain• An accumulation of CSF due to impaired flow, reabsorption or
excessive production
Symptoms• Increasing head circumference• Full/bulging fontanelle• Split sutures• Setting sun sign• High shrill cry
Treatment• Shunting

Caput vs. Cephalhematomavs. Subgaleal bleeds
28

29
Caput vs. Cephalohematoma

Neonatal Neurological Assessment
General appearance
Mental status
Cranial nerves
Motor exam
Reflexes
Coordination
Sensory
Wt, Lth, HC, dysmorphismWakefulness, behaviorPupils, grimace, gag, reflexesBulk, power, toneDeep tendon & primitiveGeneral movementsLight touch, pain, temp

Assessment of Mental Status
31
Best time to examine an infant is in between feeds
Arousal can be assessed by:• Spontaneous eye opening• Movements of the face and extremities• Response to stimulation
Irritable- agitated and cries
Lethargic – cannot maintain an alert state
Jitteriness (Tremulousness)

Excessive Arousal
32
• Jitteriness (Tremulousness)
• Can be seen in normal children
• More frequently seen in babies with:
– Encephalopathy
– Drug dependent mothers
• May distinguish from seizures with EEG/aEEG
• Features are less common that seizures
– Provocation by stimulation
– Absence of eye movements
– Lack of change in respiratory pattern
33
Mental Status
Factors affecting assessment of mental status
• Infant State
• Gestational Age
• Illness
• Medications

34
Mental Status: Gestational Age
• Gestational age is an important factor
• 28 weeks = more prolonged periods of quiet alert activity
• 32 weeks = sleep-wake cycling begins to occur
• 36 weeks = very clear state changes
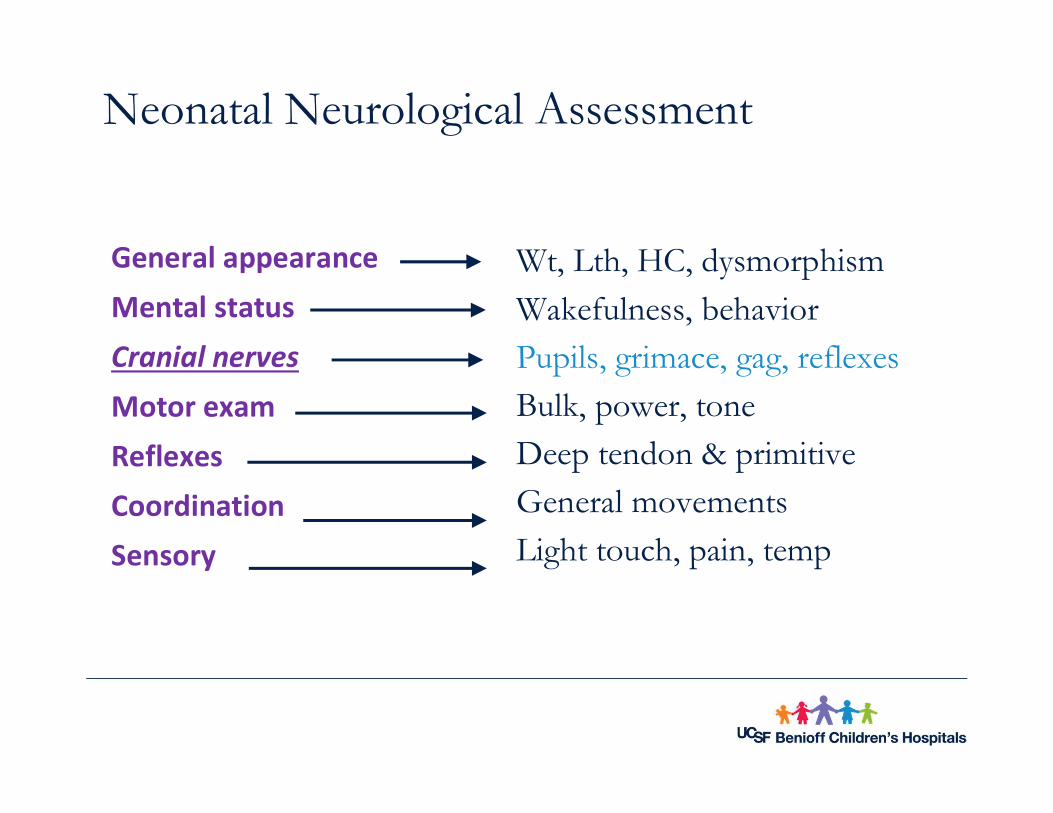
Neonatal Neurological Assessment
General appearance
Mental status
Cranial nerves
Motor exam
Reflexes
Coordination
Sensory
Wt, Lth, HC, dysmorphismWakefulness, behaviorPupils, grimace, gag, reflexesBulk, power, toneDeep tendon & primitiveGeneral movementsLight touch, pain, temp

Cranial Nerves

Cranial Nerves
Cranial Nerve Exam - Newborn

Cranial Nerves
Abnormal Cranial Nerve Exam

CN VII
• Controls movement of the face
• Most common cause of facial asymmetry
• Birth related damage to CN VII (facial nerve)
• Muscles in the forehead and eyelids may be affected
• Facial asymmetry is evident without baby crying

Cranial Nerve VII

Vision…CN II, III, IV, VI
▪ 26 Weeks – infant blinks to light
▪ 32 Weeks – Light provokes eye closure; roving eye movement
▪ 34 Weeks – 90% infants track a fluffy red ball
▪ 37 Weeks – Infant will turn toward a soft light
▪ 38-49 Weeks – Visual Fixation and Following are well developed

Eyes… CN II, III, IV, VI
▪ Eyes – forced closure of eyelids is common
▪ Most newborns open eyes spontaneously to suck
▪ Ocular alignment in the newborn is poor
Dysconjugate

Dysconjugate eye movement
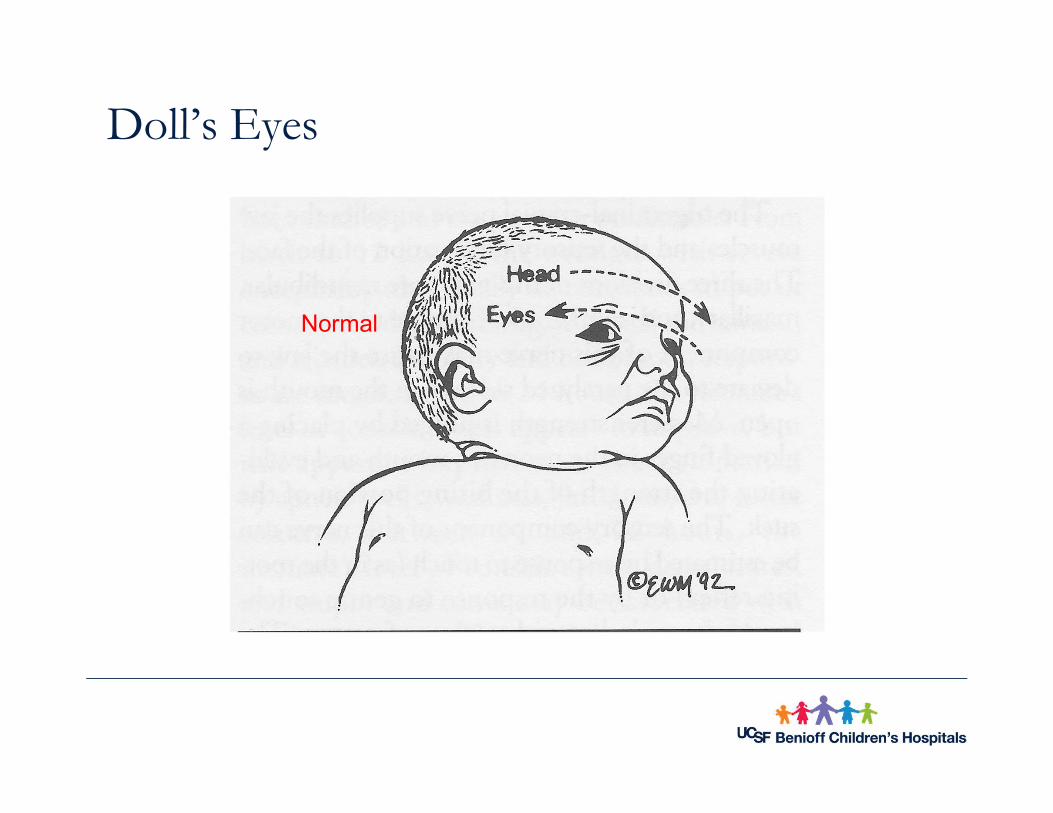
Doll’s Eyes
Normal
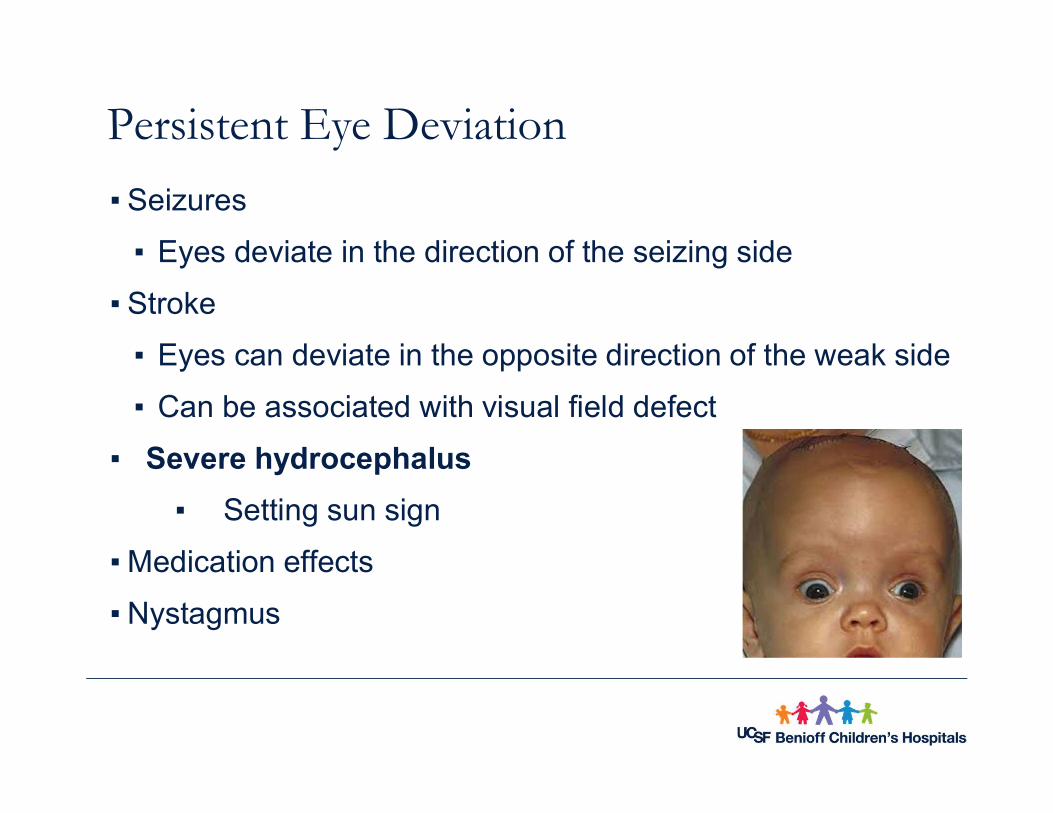
Persistent Eye Deviation
▪ Seizures
▪ Eyes deviate in the direction of the seizing side
▪ Stroke
▪ Eyes can deviate in the opposite direction of the weak side
▪ Can be associated with visual field defect
▪ Severe hydrocephalus
▪ Setting sun sign
▪ Medication effects
▪ Nystagmus

CNIII and Pupils
• Normal: 2-3cm, brisk equal reaction to light
• Abnormalities
• Encephalopathy
• Drug exposure
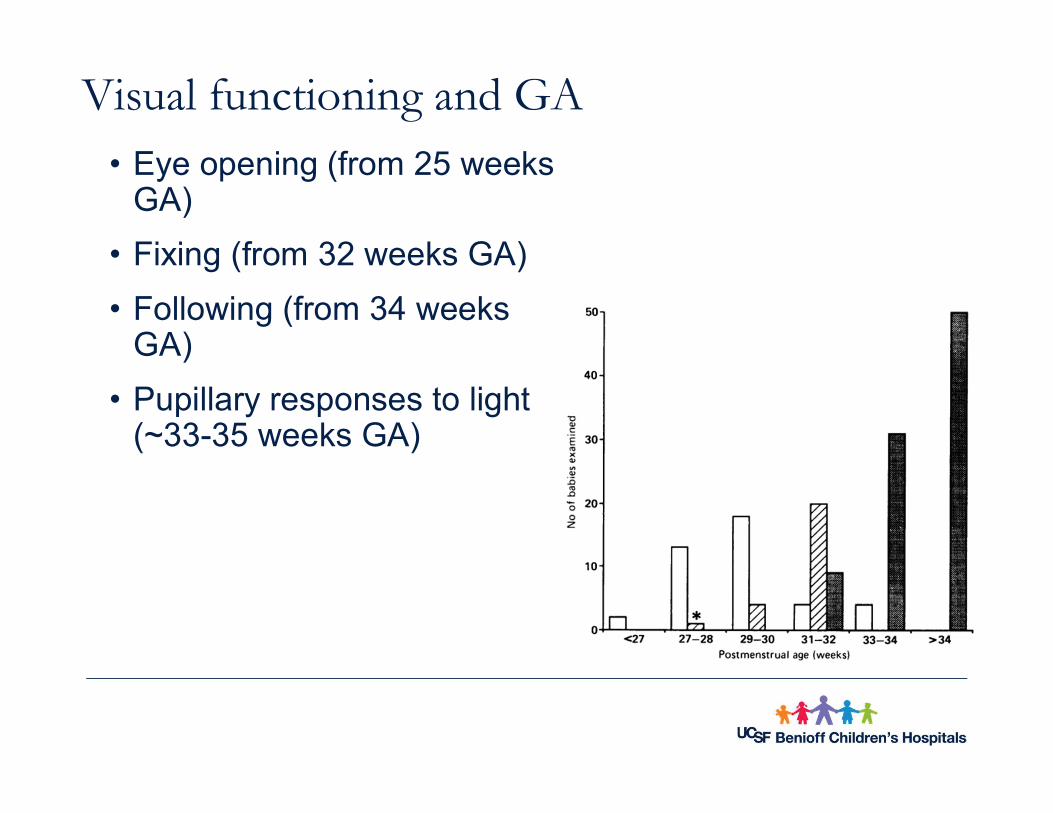
Visual functioning and GA• Eye opening (from 25 weeks
GA)
• Fixing (from 32 weeks GA)
• Following (from 34 weeks GA)
• Pupillary responses to light (~33-35 weeks GA)

Sucking & Swallowing
▪ At what gestational age do infants start to coordinate their suck, swallow and breathing?
48

Neonatal Neurological Assessment
General appearance
Mental status
Cranial nerves
Motor exam
Reflexes
Coordination
Sensory
Wt, Lth, HC, dysmorphismWakefulness, behaviorPupils, grimace, gag, reflexesBulk, power, toneDeep tendon & primitiveGeneral movementsLight touch, pain, temp

Muscle Tone
▪ Tone is the resistance to stretch
▪ 2 kinds
• Phasic tone (deep tendon reflexes)
• Postural tone- trunk and limbs letting themselves be maintained against gravity
‒ Important to think of GA and state

Postural Tone
Maintenance of tone requires an intact:
• Central Nervous System
• Peripheral Nervous System
• If decreased:
• Trunks and limbs cannot maintain themselves against gravity
• Infant appears hypotonic

Hypotonia
• Common symptom of neurological dysfunction
• Occurs in diseases of
• Brain
• Spinal Cord
• Peripheral Nerves
• Neuromuscular Junctions
• Muscles

Normal toneGeneralised
hypotonia
Abn. tone distribution: flexed arms,
ext. legs

Normal tone Generalised hypotonia Increased extensor tone
The picture can't be displayed. The picture can't be displayed.

Traction Response
The picture can't be displayed.

Head Lag

Hypotonia

Hypertonia
• Less common finding in the neonate
• If present, passive manipulation of the limbs increases the tone.
• Opisthotonus (marked hypertonia) can be seen with severe HIE, tetanus, bacterial meningitis

Marked Hypertonia

Neonatal Neurological Assessment
General appearance
Mental status
Cranial nerves
Motor exam
Reflexes
Coordination
Sensory
Wt, Lth, HC, dysmorphismWakefulness, behaviorPupils, grimace, gag, reflexesBulk, power, toneDeep tendon & primitiveGeneral movementsLight touch, pain, temp

Developmental Reflexes
Reflex Onset
Suck 28 weeks
Rooting 28 weeks
Palmar Grasp 28-32 weeks
Tonic Neck 35 weeks
Moro 28-32 weeks
Stepping 35-36
Truncal incurvation 28 weeks
Babinski 34-36 weeks

Moro

Neonatal Neurological Assessment
General appearance
Mental status
Cranial nerves
Motor exam
Reflexes
Coordination
Sensory
Wt, Lth, HC, dysmorphismWakefulness, behaviorPupils, grimace, gag, reflexesBulk, power, toneDeep tendon & primitiveGeneral movementsLight touch, pain, temp

Abnormal Neurological Exam: Causes
▪ Hypoxic Ischemic Encephalopathy (HIE)
▪ Infection
▪ Perinatal Stroke
▪ Intracranial Hemorrhage
▪ Congenital Brain Malformations
▪ Inborn Errors of Metabolism
▪ Genetic Brain Malformations
▪ Drug Exposure
Pain?
64
What if something is abnormal?
▪ Up to 1/3 of well babies have some “abnormal” findings
• Important to do a thorough exam!
▪ If more than 2 abnormalities, do a full neuro exam
▪ If more than 3 abnormalities on full exam:
• Repeat at another time
• Consider neuroimaging
• Discuss a neuro consult
65

Competent Neonate

References
▪ Volpe, JJ, Neurology of the Newborn, Philadelphia, PA. W.B. Saunders, 2008
▪ Fenichel GM, Neonatal Neurology, Philadelphia, PA. Elsevier 2007
▪ Shellhaas et. al. Clin Neurophysiology 2007; 118: 2156-2167
▪ Silverstein, F.S., Jensen, F.E. Annals of NeurologyVol 62 (2) 2007
▪ Stanford University
▪ University of Utah
