neumologia
DESCRIPTION
capitulo 1TRANSCRIPT

Authors: Webb, Richard W.; Higgins, Charles B.
Title: Thoracic Imaging: Pulmonary and Cardiovascular Radiology, 1st Edition
Copyright ©2005 Lippincott Williams & Wilkins
> Table of Contents > 1 - Congenital Bronchopulmonary Lesions
1
Congenital Bronchopulmonary Lesions
Richard W. Webb
Congenital bronchopulmonary lesions represent a variety of vascular and nonvascular abnormalities of the lung and
mediastinum. They often have characteristic plain film and computed tomography (CT) findings. Congenital
abnormalities of the aorta and great vessels are reviewed in Chapter 35.
BRONCHIAL ANOMALIESAnomalies of bronchial anatomy include abnormal origin, absent branches, and supernumerary branches (Table 1-1).
Minor variation in subsegmental bronchial anatomy is common but clinically insignificant; a detailed knowledge of
subsegmental bronchial anatomy is not necessary for clinical practice. Segmental bronchial anomalies are less
frequent and not often of significance.
Tracheal BronchusTracheal bronchi are common anomalies, present in about 0.1% of the population. A tracheal bronchus usually arises
from the right tracheal wall, at or within 2 cm of the tracheal bifurcation. It supplies a variable portion of the
medial or apical right upper lobe, most often the apical segment (Fig. 1-1); in occasional cases, the entire right
upper lobe bronchus arises from the trachea (Fig. 1-2). When a tracheal bronchus is present, the azygos arch is seen
above the tracheal bronchus. Tracheal bronchus is sometimes referred to as a “pig bronchus” or “bronchus suis” as it
is common in pigs and other cloven-hoofed animals.
In most cases, this anomaly is insignificant. However, recurrent infection or bronchiectasis may result, since the
tracheal bronchus is often slightly narrowed at its origin. A left tracheal bronchus, supplying the apical posterior
segment of the left upper lobe, is rarely present; it is much less common than right-sided tracheal bronchi.
Accessory Cardiac BronchusAccessory cardiac bronchus is a supernumerary bronchus with an incidence of about 0.1%. It arises from the medial
wall of the bronchus intermedius or right lower lobe bronchus and extends inferiorly and medially toward the
mediastinum or heart. It may terminate within the mediastinum (Fig. 1-3). In some cases, the cardiac bronchus is a
short, blind-ending bronchial stump without associated alveolar tissue; in others, a longer branching bronchus is
present, associated with rudimentary lung tissue. In most cases, this anomaly is an incidental finding; occasionally,
chronic infection or hemoptysis is associated.
Bronchial IsomerismBronchial isomerism refers to bilateral symmetry of the bronchi and associated pulmonary lobes. It may be isolated
or associated with a variety of anomalies, particularly congenital heart disease. Bronchial anatomy may be
bilaterally
right sided (associated with asplenia) or left sided (associated with polysplenia). P.2
Page 1 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

TABLE 1-1. BRONCHIAL ANOMALIES
Subsegmental anomalies
Common but insignificant
Tracheal bronchus
Incidence 0.1%
Arises from right tracheal wall; rare on left
Usually supplies apical segment of right upper lobe; rarely entire right upper lobe
Increased incidence of infection or bronchiectasis
Accessory cardiac bronchus
Incidence 0.1%
Arises from medial wall of bronchus intermedius
Usually blind ending or supplies rudimentary lung
May terminate in the mediastinum
Increased incidence of infection or hemoptysis
Bronchial isomerism
Symmetrical bronchial anatomy
Bilateral right of left-sided bronchial anatomy
Associated with congenital heart disease, other anomalies
Page 2 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

BRONCHIAL ATRESIABronchial atresia is a developmental defect characterized by local narrowing or obliteration of a lobar, segmental, or
subsegmental bronchus (Table 1-2). It is most common in the left upper lobe, followed by the right upper, and right
middle lobes; it may occur in the lower lobes but is less common. This entity is usually detected incidentally in
adults and is undoubtedly etiologically related to congenital lobar emphysema (CLE). Patients usually have no
symptoms, but lung distal to the obstruction may occasionally become infected. In patients with chronic infection,
resection may be necessary.
The lobe or segment distal to the bronchial obstruction usually remains aerated because of collateral ventilation
(Figs. 1-4 and 1-5). Air trapping and decreased perfusion in the distal lung cause it to be hyperlucent and
hypovascular in 90% of cases. Affected lung is often increased in volume, resulting in mediastinal shift or shift of a
fissure. In 80% of cases, mucus accumulates within dilated bronchi distal to the obstruction, resulting in a tubular,
FIG. 1-1. Tracheal bronchus. A. Coronal CT reconstruction shows a tracheal bronchus (Tr Br) arising from the
right tracheal wall just above the carina. B. The azygos arch (Azygos) is visible above the bronchus. CT (1.25-
mm detectors) shows the origin of the tracheal bronchus. As in this case, slight narrowing at the origin of the
bronchus is typical. The bronchus supplies the apical segment of the right upper lobe. C. The tracheal carina
is seen slightly below B. D. Below C, the main right upper lobe bronchus (RUL) gives rise to the anterior (Ant
Seg) and posterior (Post Seg) segmental bronchi.
Page 3 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

branching, or ovoid density (mucous plug or mucocele). CT shows the affected lung to be lucent, hypovascular, and
increased in volume. Mucus within dilated bronchi appears low in attenuation. Expiratory radiographs or CT scans
show air trapping (see Fig. 1-5B).
P.3
FIG. 1-2. Tracheal bronchus in a patient with pneumonia. A. Coronal reconstruction shows the entire right
upper lobe bronchus (RUL) arising from the right tracheal wall above the carina. The apical segmental
bronchus extends superiorly. B. Transaxial CT shows the right upper lobe bronchus (arrow) giving rise to
anterior and posterior segments. Patchy areas of increased lung opacity reflect the presence of pneumonia.
Page 4 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

The combination of these typical radiographic findings in a young patient is strongly suggestive of the diagnosis.
Bronchoscopy may be warranted to rule out another cause of bronchial obstruction, such as tumor.
FIG. 1-3. Accessory cardiac bronchus. A. Scan at the level of the bronchus intermedius. B. Slightly below A, a
bronchus arises from the medial wall of the bronchus intermedius (arrow). This represents the origin of a
cardiac bronchus. C. Slightly below B, the cardiac bronchus (arrow) is seen extending into the mediastinum
medial to the hilum. D. Below C, the bronchus is no longer seen.
P.4
FIG. 1-3. (Continued.)
TABLE 1-2. BRONCHIAL ATRESIA
Narrowing or obliteration of a lobar, segmental, or subsegmental bronchus
Left upper lobe > right upper lobe > right middle lobe > lower lobes
Detected incidentally in adults
Page 5 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Infection may occur
Mucous plug distal to obstructed bronchial segment
Distal lung
Lucent
Increased in volume
Decreased vessel size
Air trapping on expiration
Rule out obstructing tumor
Page 6 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-4. Bronchial atresia. Chest radiograph shows a classic bronchial atresia involving the left upper lobe.
The upper lobe is increased in volume, with mediastinal shift toward the opposite side (white arrow). The
lobe is lucent, and vascularity is decreased. A large, oval mucous plug (black arrow) is visible distal to the site
of bronchial obstruction.
P.5
Page 7 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

CONGENITAL LOBAR EMPHYSEMACLE is characterized by marked overinflation of a lobe (Table 1-3). Most cases present within the first month of life;
symptoms of respiratory distress are typical. Presentation after the first month may occur.
Most cases of CLE are associated with partial or complete bronchial obstruction occurring as a result of (1) deficient
cartilage; (2) external compression, usually by an anomalous vessel or bronchogenic cyst; or (3) luminal
abnormalities such as mucosal folds. Some cases may not be associated with bronchial obstruction.
CLE is most common in the left upper lobe, followed by the right middle lobe and right upper lobe. Only a few
percent occur in the lower lobes. Radiographs show marked overinflation and air trapping in the affected lobe, but
the lobe may sometimes appear opaque because of retained fetal lung fluid. Mediastinal shift away from the
abnormal lobe often occurs, and normal lobes are reduced in volume. Resection is often necessary.
FIG. 1-5. Bronchial atresia. A. CT shows a branching mucous plug (white arrow) in the location of the
posterior segment of the right upper lobe. Lung distal to the bronchus (black arrows) is hyperlucent and
hypovascular. Slight mediastinal shift to the left side is present. B. Expiratory CT shows air trapping in the
lung distal to the obstructed bronchus. Normal lung increases significantly in attenuation relative to A.
TABLE 1-3. CONGENITAL LOBAR EMPHYSEMA
Partial or complete bronchial obstruction caused by:
Deficient cartilage
External compression
Luminal abnormalities
Some cases unassociated with bronchial obstruction
Left upper lobe > right middle lobe > right upper lobe > lower lobes
Respiratory distress in neonates
Presentation after 1st month uncommon
Marked overinflation of lobe
Air trapping
Page 8 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

It is reasonable to assume that cases of CLE that go unrecognized at birth may be diagnosed years later as bronchial
atresia.
PULMONARY BRONCHOGENIC CYSTBronchogenic cysts are foregut duplication cysts and result from abnormal development of the lung bud. They are
lined by pseudostratified ciliated columnar epithelium, typical of bronchi. The cyst wall may also contain smooth
muscle, mucous glands, or cartilage. Bronchogenic cysts are filled with fluid, which can be serous, hemorrhagic, or
highly viscous and gelatinous because of its high protein content.
Bronchogenic cysts may be mediastinal or pulmonary. Mediastinal bronchogenic cysts are much more common than
pulmonary cysts. They are discussed along with mediastinal masses in Chapter 8.
Pulmonary bronchogenic cysts are most common in the medial lung and the lower lobes (Table 1-4). They are
sharply circumscribed and round or oval. The cyst wall may calcify. Rarely, the cyst may contain milk of calcium and
appear dense. Little change in size is typically seen over time unless infection occurs.
Sometimes the abnormal lobe retains fetal lung fluid
Resection often necessary
P.6
TABLE 1-4. PULMONARY BRONCHOGENIC CYST
Foregut duplication cyst
Lined by bronchial epithelium
Fluid contents can be serous, hemorrhagic, or viscous
Less common than mediastinal bronchogenic cysts
Most commonly in medial lung and lower lobes
Page 9 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Sharply circumscribed and round or oval
Thin wall; occasionally calcifies
Contents 0-20 HU in half; often 20-80 HU; milk of calcium rare
Infection occurs in 75%
Rapid increase in size
Blurring of outer edge
Air-fluid level
Air in cyst may remain after infection
FIG. 1-6. Pulmonary bronchogenic cyst. A sharply marginated round nodular opacity (arrow) is visible in the
right lower lobe. This measured 0 HU in attenuation. This appearance is typical of a fluid-filled bronchogenic
cyst.
Page 10 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

About half of fluid-filled bronchogenic cysts appear to be low in attenuation on CT (0 to 20 HU) (Fig. 1-6). However,
as with mediastinal bronchogenic cysts, the CT attenuation of a pulmonary bronchogenic cyst is variable. High CT
numbers (40 to 80 HU), suggesting a solid mass, can be seen. Such cysts contain blood or thick, proteinaceous fluid.
Typically, the cyst wall appears very thin on CT or is invisible. They may be related to a small bronchus or may be
isolated.
Infection eventually occurs in 75% of cases. In the presence of acute infection, a rapid increase in size of the cyst
may be seen. Also, the outer cyst wall may become less well defined because of surrounding lung inflammation.
During or after infection, a cyst may contain air (Fig. 1-7; see also Fig. 9-29 in Chapter 9) or a combination of air and
fluid (with an air-fluid level). When the cyst contains air, its wall appears very thin.
CONGENITAL CYSTIC ADENOMATOID MALFORMATIONCongenital cystic adenomatoid malformation (CCAM) consists of a multicystic, intralobar mass of disorganized lung
tissue, derived primarily from bronchioles. About 70% present during the first week of life, but 10% are diagnosed
after the first year, and rare cases in adults have been reported.
CCAMs can involve an entire lobe. Lower lobes are most often involved, but any lobe can be affected. The CCAM
communicates with the bronchial tree and is supplied by the pulmonary artery; systemic arterial supply is rarely
FIG. 1-7. Pulmonary bronchogenic cyst. A thin-walled, sharply marginated, air-filled bronchogenic cyst is
visible in the left lung. The presence of air within the cyst indicates prior infection.
Page 11 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

present.
CCAMs are often classified into three types, which have different histology, gross pathologic findings, radiographic
appearance, and prognosis (Table 1-5).
Type I CCAMs (55% of cases) contain one or more cysts more than 2 cm in diameter (Fig. 1-8). They usually present
as a large, air-filled multicystic lesion, sometimes with air-fluid levels, which may occupy the entire hemithorax.
Type II CCAMs (40% of cases) contain multiple cysts less than 2 cm in diameter. They present as an air-filled
multicystic mass or a solid mass or area of consolidation (see Fig. 1-9). This type may be associated with a poor
prognosis because of associated renal and cardiac abnormalities.
P.7
TABLE 1-5. CONGENITAL CYSTIC ADENOMATOID MALFORMATION
Multicystic, intralobar mass of disorganized lung tissue
70% present in 1st week; 10% after 1st year
Respiratory distress in neonates; recurrent infection in adults
Most common in lower lobe
Three types
Type I (55%)
One or more cysts, >2 cm in diameter
May appear initially as solid mass
Large air-filled multicystic lesion
Sometimes with air-fluid levels
May occupy the entire hemithorax
Type II (40%)
Multiple cysts <2 cm in diameter
Page 12 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

May appear initially as solid mass
Air-filled multicystic mass or focal consolidation
Associated renal and cardiac abnormalities
Often a poor prognosis
Type III (5%)
Microscopic (<3-5 mm) cysts
Solid mass
Page 13 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
Type III CCAMs (5% of cases) contain microscopic (less than 3 to 5 mm) cysts and present radiographically as a solid
mass.
Sonography can be used for prenatal diagnosis. Findings include polyhydramnios, fetal hydrops, and a solid or cystic
mass in the fetal thorax. Fetal surgery may be attempted.
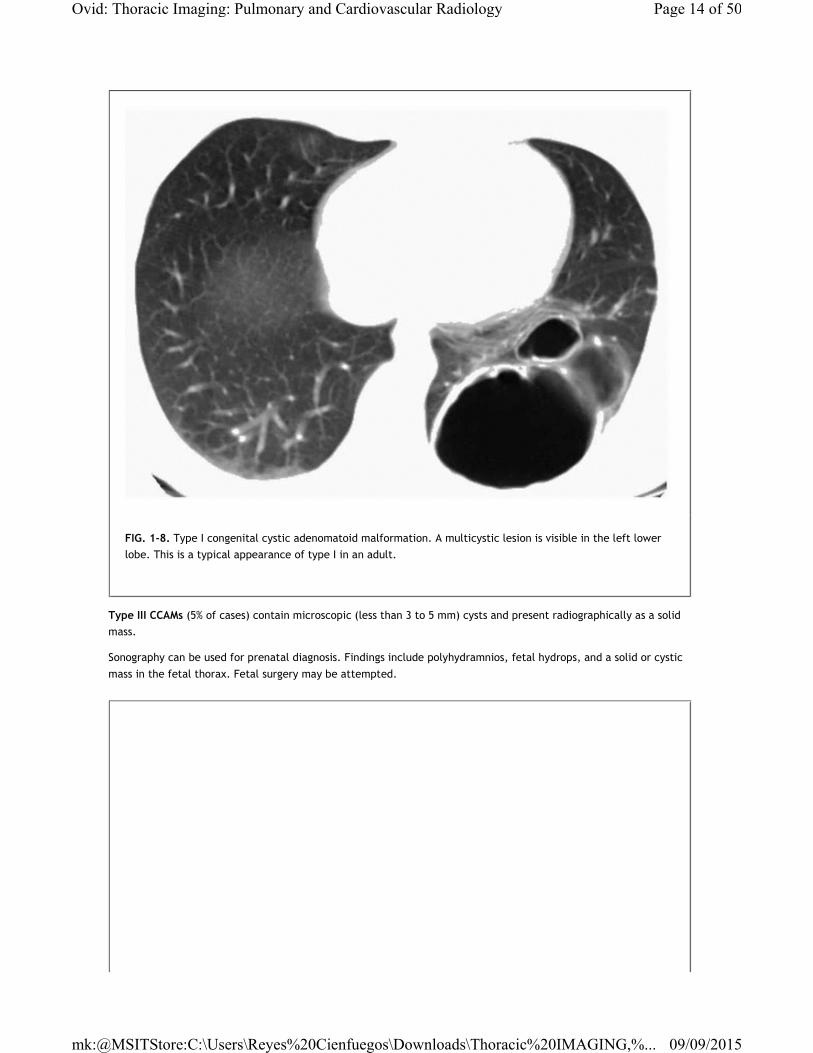
FIG. 1-8. Type I congenital cystic adenomatoid malformation. A multicystic lesion is visible in the left lower
lobe. This is a typical appearance of type I in an adult.
Page 14 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

In infancy, CCAMs present as a space-occupying lesion. Symptoms of respiratory distress are common. In neonates,
CCAMs usually present as a solid mass regardless of its type. Types I and II may become air filled over a period of
days to weeks. They are often associated with progressive air trapping and mediastinal shift to the opposite side.
The treatment of choice is excision of the affected lobe. The prognosis of neonates with CCAMs is adversely affected
by large CCAM size, underdevelopment of uninvolved lung (i.e., the presence of associated lung hypoplasia), and the
presence of associated fetal hydrops or other congenital anomalies.
In adults, CCAMs usually present as an air-filled or airand fluid-filled cystic or multicystic mass. Most adults present
with recurrent pneumonia, although recurrent pneumothorax has also been associated. Occasionally,
bronchioloalveolar carcinoma may arise in relation to a CCAM.
PULMONARY ARTERIOVENOUS MALFORMATIONCongenital arteriovenous malformations (AVMs), also known as arteriovenous fistula, likely result from deficient
formation or abnormal dilation of pulmonary capillaries due to a developmental defect in the capillary wall. From
35% to 67% of cases are associated with Osler-Weber-Rendu syndrome (hereditary hemorrhagic telangiectasia), in
which AVMs are found in the skin, mucous membranes, and viscera (Table 1-6). Also, AVMs may rarely occur in
patients with hepatopulmonary syndrome or as a result of trauma.
Pulmonary arteriovenous fistulas slowly enlarge over time and are usually first diagnosed in adulthood. More than
two thirds of AVMs are found in the lower lobes, and they are typically subpleural in location. Fistulas are multiple in
FIG. 1-9. Type II congenital cystic adenomatoid malformation. A solid mass (arrows) is visible in the right
lower lobe, containing an opacified vessel. Type II may present as an air-filled or fluid-filled mass.
Page 15 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
35% of patients and bilateral in 10%.
Simple and Complex Arteriovenous MalformationsA simple AVM is a single, dilated vascular sac connecting one artery and one vein (Figs. 1-10 and 1-11). It is most
frequent and accounts for the bulk of cases of AVM. Complex AVMs, which have more than one feeding artery, are
rare.
Radiographically, a simple fistula appears as a peripheral, well-defined round, oval, lobulated, or serpentine density.
Large vessels (feeders) extending centrally toward the hilum are usually visible (see Figs. 1-11C, 1-12 and 1-13).
Enlargement of fistulas over a period of months or years is common and rapid increase in size can occur.
At CT, a simple AVM is visible as a smooth, sharply defined, round or elliptical nodule, almost always in a subpleural
location (see Figs. 1-12 and 1-13). Arteriovenous fistulas characterized by a tangle of tortuous, dilated vessels are
seen as lobulated, serpiginous masses and can often be suspected as being vascular simply by their morphology. In
both instances, the feeding pulmonary artery branch and draining pulmonary vein are dilated, and with fistulas of
significant size (larger than 1 to 2 cm), the feeders are easily recognizable. In general, the feeders are about half
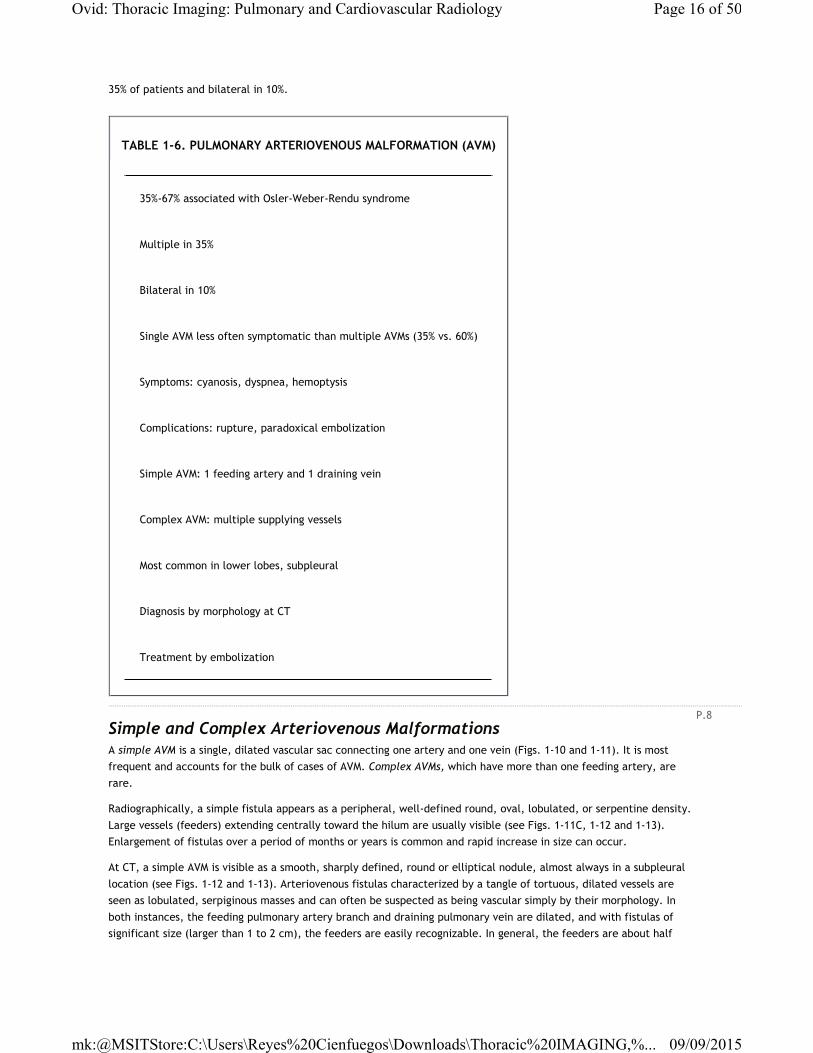
TABLE 1-6. PULMONARY ARTERIOVENOUS MALFORMATION (AVM)
35%-67% associated with Osler-Weber-Rendu syndrome
Multiple in 35%
Bilateral in 10%
Single AVM less often symptomatic than multiple AVMs (35% vs. 60%)
Symptoms: cyanosis, dyspnea, hemoptysis
Complications: rupture, paradoxical embolization
Simple AVM: 1 feeding artery and 1 draining vein
Complex AVM: multiple supplying vessels
Most common in lower lobes, subpleural
Diagnosis by morphology at CT
Treatment by embolization
P.8
Page 16 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

the diameter of the fistula.
Spiral CT without contrast infusion is highly accurate in demonstrating AVMs and their architecture (see Figs. 1-11C,
1-12 and 1-13). In most cases, morphologic findings are sufficient for diagnosis of AVM (see Figs. 1-12B and E), but
contrast infusion may be used for confirmation (see Fig. 1-12C). Following the bolus injection of contrast, pulmonary
AVMs show rapid contrast opacification and washout, occurring in phase with opacification and washout of the main
pulmonary artery and the right ventricle.
In general, AVMs appearing less than 2 cm in diameter on chest radiographs are asymptomatic. Single fistulas are less
commonly symptomatic (35%) or associated with positive physical findings (70%) than are multiple fistulas (60% and
85%, respectively). An AVM results in a right to left shunt, and cyanosis is common, depending on the size of the
shunt. The most frequent symptoms occurring in patients with AVMs are dyspnea, palpitation, hemoptysis, and chest
pain. Cerebrovascular accidents (see Fig. 1-12H) associated with polycythemia or paradoxical embolization through
the AVM from systemic veins are serious and potentially fatal complications. Rupture can result in pulmonary
FIG. 1-10. Simple arteriovenous malformation. A single artery (white arrow) supplies a simple malformation
drained by a single vein (black arrow). As is typical, the fistula is subpleural in location.
Page 17 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

hemorrhage (Fig. 1-14) or hemothorax (Fig. 1-15). Without treatment, approximately 25% of patients with AVMs
experience worsening of symptoms, and 50% of these will eventually die as a result of complications.
Pulmonary arteriography is advisable if embolization or surgical excision of the fistula is planned (see Fig. 1-12F and
G). Transcatheter occlusion of fistulas using wire coils is the treatment of choice for simple AVMs. Recanalization of
an AVF may occasionally occur after coil embolization. Complex AVMs (Fig. 1-16) are more often symptomatic that
simple fistulas, because of a larger shunt. They are more difficult to treat because many feeders may be present,
but wire coil embolization may be successful.
Pulmonary TelangiectasiaPulmonary telangiectasia is an uncommon form of AVM characterized by innumerable very small fistulas scattered
throughout both lungs. Symptoms are common and progressive, and cyanosis is present in all patients. Unlike simple
AVMs, pulmonary telangiectasia is typically discovered by 10 years of age. Radiographs can be normal. If abnormal,
radiographic findings are often limited to an abnormal pattern of pulmonary vessels, including (1) a coarse spidery
appearance of pulmonary vessels, (2) vascular tortuosity, and (3) areas of hypervascularity. On angiograms, beaded
or tortuous vessels, small aneurysmal sacs, or multiple ill-defined areas of vascular blush are visible. Treatment of
this condition is difficult and prognosis is poor. Surgery is not possible because of the multiplicity of lesions.
P.9
Page 18 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-11. Simple arteriovenous malformation (AVM). A. A well-defined, smooth, round, 3-cm nodule is visible
on chest radiograph. B. Pulmonary arteriogram shows a simple AVM. The feeding artery is opacified. C. Simple
AVM shown on CT in a different patient. A subpleural AVM is supplied a large artery and vein branch. The
feeders are about half the diameter of the fistula.
P.10
FIG. 1-12. Multiple arteriovenous malformations (AVMs) in a 30-year-old woman with Osler-Weber-Rendu
syndrome. A. Chest radiograph shows a nodule in the right upper lobe (arrow). B. Spiral CT with 1.25-mm
detectors shows a well-defined subpleural nodule with a feeding vessel (arrow), representing a vein. This
appearance is typical of AVMs. C. With contrast injection, dense opacification of the fistula and feeding vein is
Page 19 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

seen. D. Coronal reconstruction shows the subpleural fistula and feeding artery and draining vein. E. Multiple
other fistulas were visible. A small fistula (arrow) in the lower lobe may be diagnosed based on its
morphology. F. Arteriogram performed at the time of embolization shows the fistula in C to G. The fistula
shown in F has been occluded by wire coils. H. T2-weighted MRI of the brain shows findings of infarction. This
is a common complication of AVMs.
P.11
Page 20 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-12. (Continued.)
P.12
FIG. 1-13. Multiple arteriovenous malformations in a 19-year-old woman with Osler-Weber-Rendu syndrome.
A. Multidetector spiral HRCT obtained with 1.25-mm detectors shows three small subpleural nodules (arrows).
B. A maximum intensity projection image (MIP) of a stack of HRCT images at the same level shows a small
arteriovenous malformation (arrows) with feeding vessels. C-E. Transaxial (C), coronal (D), and sagittal (E)
Page 21 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

MIP reconstruction images show other subpleural fistulas (arrows).
P.13
FIG. 1-14. Osler-Weber-Rendu syndrome with multiple arteriovenous malformations shown on CT and
pulmonary hemorrhage. Patchy areas of ground-glass opacity (arrows) in the left lung represent blood due to
rupture of an arteriovenous malformation.
Page 22 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-15. Arteriovenous malformation (AVM) and hemothorax in a young woman with acute chest pain and
shortness of breath. A. CT shows a right pleural effusion with a region of high attenuation indicating clot. A
rounded lesion opacified by contrast is visible in the lung periphery (arrow). This appearance suggests AVM. B.
Arteriogram shows a simple AVM in the lung periphery. Wire-coil embolization was performed, with resolution
of the symptoms.
P.14
Page 23 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
PULMONARY AGENESIS, APLASIA, AND HYPOPLASIA
Agenesis and Aplasia
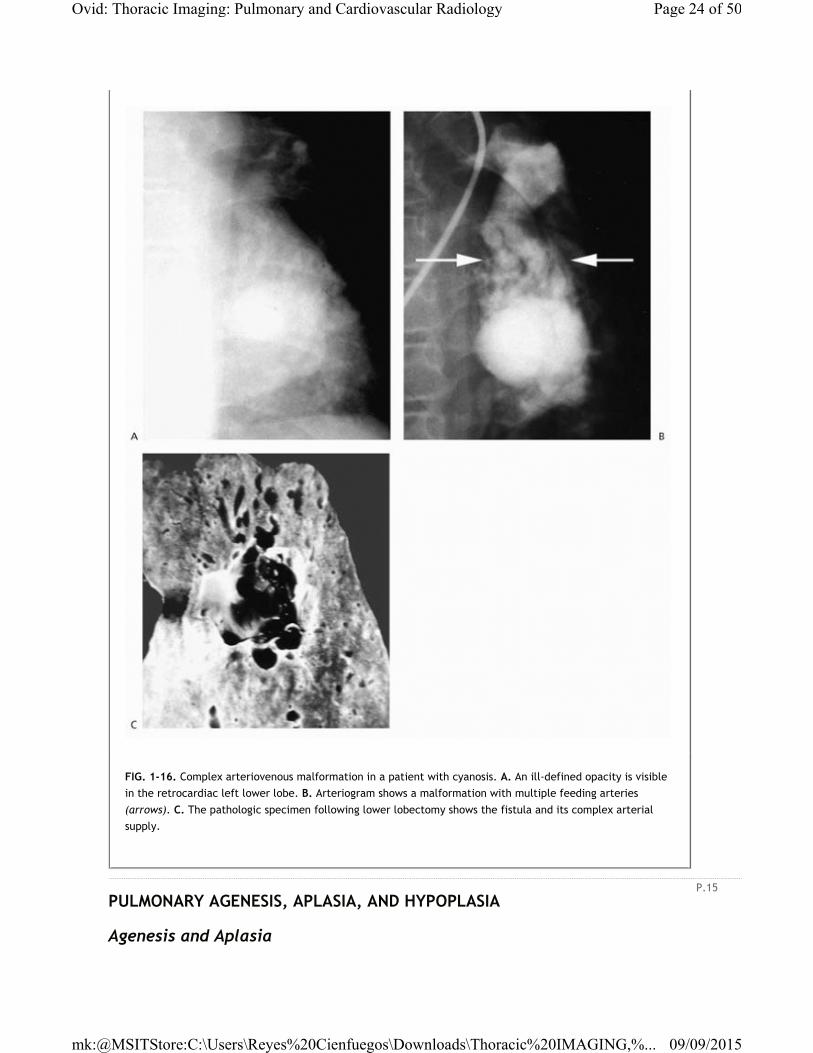
FIG. 1-16. Complex arteriovenous malformation in a patient with cyanosis. A. An ill-defined opacity is visible
in the retrocardiac left lower lobe. B. Arteriogram shows a malformation with multiple feeding arteries
(arrows). C. The pathologic specimen following lower lobectomy shows the fistula and its complex arterial
supply.
P.15
Page 24 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Pulmonary agenesis and aplasia are nearly the same, and a distinction is not usually necessary. Pulmonary agenesis
represents complete absence of a lung, its bronchi, and its vascular supply. Pulmonary aplasia is characterized by
complete absence of a lung and its vascular supply, but a rudimentary bronchus is present (Fig. 1-17), ending in a
blind pouch (Table 1-7). Either side may be affected. Associated congenital anomalies are often present.
Radiographically, pulmonary agenesis and aplasia result in opacification of a hemithorax and marked mediastinal
shift (see Fig. 1-17). The heart is displaced into the posterior hemithorax on the side of agenesis or aplasia, along
with other mediastinal structures. On lateral radiographs, the anterior chest appears abnormally lucent because of
herniation of the remaining lung into the opposite hemithorax. CT demonstrates absence of the lung and pulmonary
artery with marked mediastinal shift. In patients with agenesis, bronchi are also absent.
HypoplasiaPulmonary hypoplasia represents abnormal lung development associated with a reduction in lung volume and often a
decrease in the number of alveoli and bronchial divisions (see Table 1-7). There may also be anomalous lobes or
segments, or they may be reduced in number. Hypoplasia is associated with other anomalies in hypogenetic lung
(scimitar) syndrome. It may also result from abnormal lung development due to deficient vascular supply (e.g.,
proximal interruption of the pulmonary artery) or lung compression during gestation (e.g., congenital diaphragmatic
hernia [Fig. 1-18], space-occupying lesions, cystic adenomatoid malformation, sequestration, thoracic deformity, or
oligohydramnios). The pulmonary artery supplying the lung is reduced in size or absent (see Fig. 1-18E), and the size
of pulmonary vessels is reduced on the affected side. Mediastinal shift toward the hypoplastic lung occurs with
hypogenetic lung syndrome and proximal interruption of the pulmonary artery. Mediastinal shift may or may not be
present when hypoplasia results from an ipsilateral space-occupying lesion.
Page 25 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
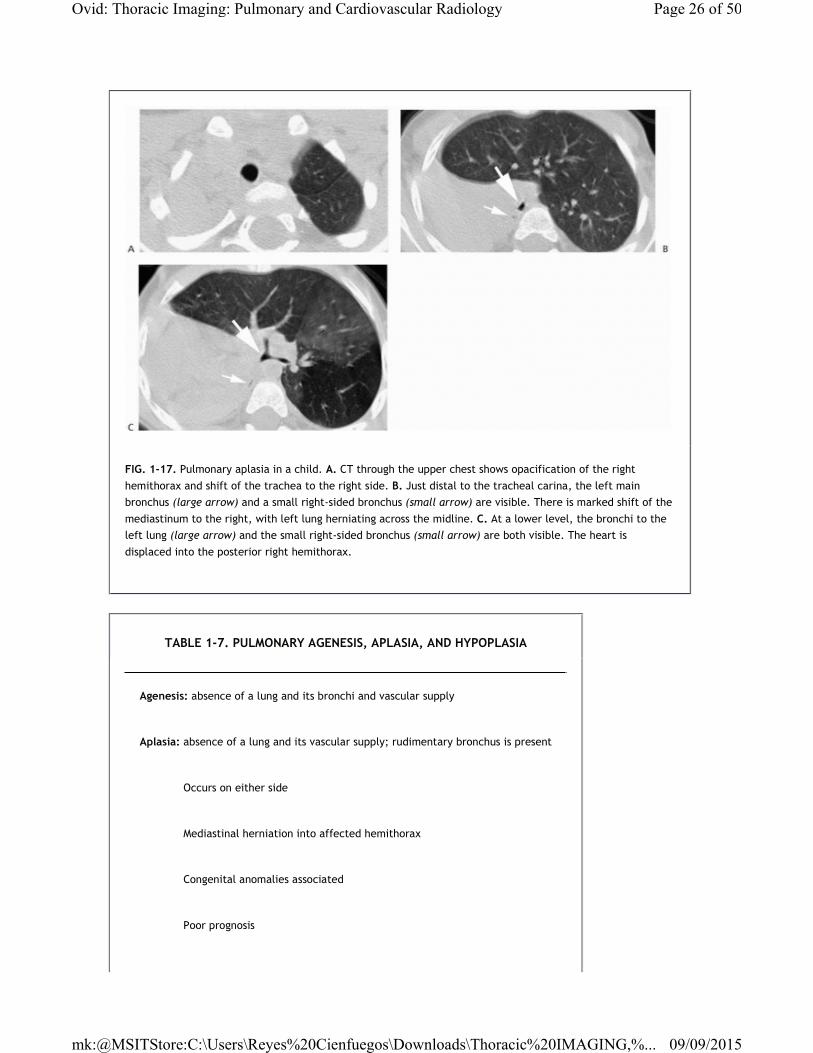
FIG. 1-17. Pulmonary aplasia in a child. A. CT through the upper chest shows opacification of the right
hemithorax and shift of the trachea to the right side. B. Just distal to the tracheal carina, the left main
bronchus (large arrow) and a small right-sided bronchus (small arrow) are visible. There is marked shift of the
mediastinum to the right, with left lung herniating across the midline. C. At a lower level, the bronchi to the
left lung (large arrow) and the small right-sided bronchus (small arrow) are both visible. The heart is
displaced into the posterior right hemithorax.
TABLE 1-7. PULMONARY AGENESIS, APLASIA, AND HYPOPLASIA
Agenesis: absence of a lung and its bronchi and vascular supply
Aplasia: absence of a lung and its vascular supply; rudimentary bronchus is present
Occurs on either side
Mediastinal herniation into affected hemithorax
Congenital anomalies associated
Poor prognosis
Page 26 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Hypoplasia
Abnormal lung development
Decreased alveoli and bronchial divisions
Deficient lobes or segments may be present
Causes:
Hypogenetic lung syndrome
Proximal interruption of pulmonary artery
Lung compression during development
P.16
Page 27 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
Pulmonary agenesis and aplasia are usually associated with a poor prognosis, with few patients surviving to
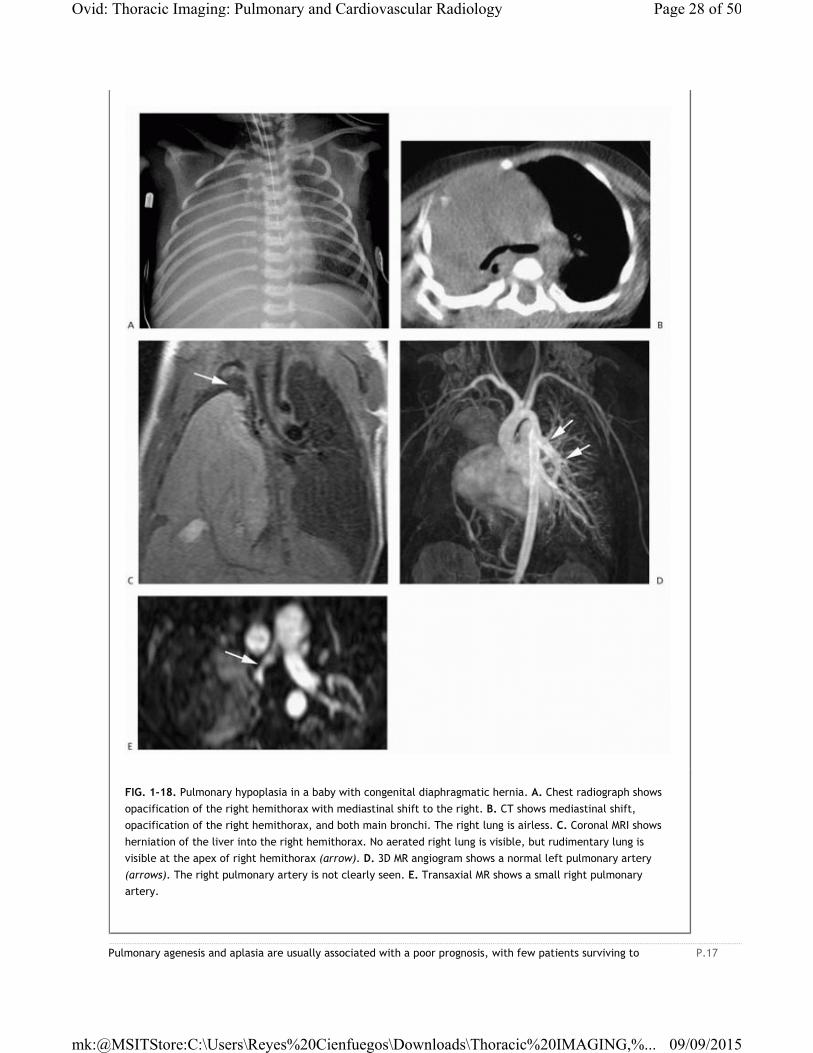
FIG. 1-18. Pulmonary hypoplasia in a baby with congenital diaphragmatic hernia. A. Chest radiograph shows
opacification of the right hemithorax with mediastinal shift to the right. B. CT shows mediastinal shift,
opacification of the right hemithorax, and both main bronchi. The right lung is airless. C. Coronal MRI shows
herniation of the liver into the right hemithorax. No aerated right lung is visible, but rudimentary lung is
visible at the apex of right hemithorax (arrow). D. 3D MR angiogram shows a normal left pulmonary artery
(arrows). The right pulmonary artery is not clearly seen. E. Transaxial MR shows a small right pulmonary
artery.
P.17
Page 28 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

adulthood. In patients with lung hypoplasia, the prognosis depends on the degree of abnormality and associated
anomalies.
HYPOGENETIC LUNG (SCIMITAR) SYNDROMEA rare anomaly, almost always occurring on the right side, hypogenetic lung syndrome is characterized by (1)
hypoplasia of the lung with abnormal segmental or lobar anatomy, (2) hypoplasia of the ipsilateral pulmonary artery,
(3) anomalous pulmonary venous return to the inferior vena cava (or right atrium, hepatic veins, etc.), and (4)
anomalous systemic arterial supply to a portion of the hypoplastic lung, usually the lower lobe (Table 1-8). Although
these four features often coexist, hypogenetic lung syndrome shows considerable variation in the degree to which
each feature is expressed. Patients may exhibit some features of this syndrome but not others.
This syndrome is usually diagnosed in patients less than 30 years of age, and more than half have symptoms.
Recurrent respiratory infections and dyspnea on exertion are most common. Congenital heart lesions, most
commonly septal defects and patent ductus arteriosus, are associated in 25%. Surgical treatment involves
implantation of the anomalous vein into the left atrium.
FIG. 1-19. Scimitar syndrome in two different patients. Plain radiographs usually show displacement of the
mediastinum toward the right side, reduction in size of pulmonary artery branches in the right lung (best
shown in A), and the anomalous pulmonary vein paralleling the right heart border (arrows).
TABLE 1-8. HYPOGENETIC LUNG (SCIMITAR) SYNDROME
Four features typical (although each not always present):
Hypoplasia of the lung with abnormal segmental or lobar anatomy
Hypoplasia of the ipsilateral pulmonary artery
Page 29 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Radiographically, the appearance of scimitar syndrome is often characteristic (Fig. 1-19). The hypoplastic lung is
recognizable because of dextroposition of the heart, mediastinal shift to the right side, and right diaphragmatic
elevation. CT may show abnormal bronchial anatomy on the side of the hypoplastic lung.
Hypoplasia of the pulmonary artery is usually recognizable by the decreased size of vessels within the hypoplastic
lung (see Fig. 1-19A). Because most of the pulmonary blood
flow must traverse the normal artery on the side opposite the hypoplastic lung, the opposite pulmonary artery
appears enlarged, further increasing the contrast between the right and left vasculature.
Anomalous pulmonary venous return (scimitar vein)
Anomalous systemic arterial supply to lower lobe
Almost always on the right side
Mediastinal shift toward the hypoplastic lung
Reduced size of ispilateral pulmonary artery
Anomalous (scimitar) vein usually paralleling right heart border
Congenital heart disease in 25% (atrial septal defect, patent ductus arteriosus)
Symptoms: recurrent infection, dyspnea
P.18
Page 30 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
When the anomalous vein is visible radiographically, it appears as a broad arcuate band at the right lung base,
paralleling the right heart border and extending to the diaphragmatic surface (see Figs. 1-19, 1-20 and 1-21). This
venous shadow often resembles a scimitar (see Figs 1-20 and 1-21D), hence the nickname of this syndrome. In nearly
two thirds of patients, the scimitar vein drains the entire right lung. On CT, the scimitar vein is located in close
relation to the major fissure. Left-sided scimitar syndrome, with the anomalous vein entering the coronary sinus, is
rarely seen.
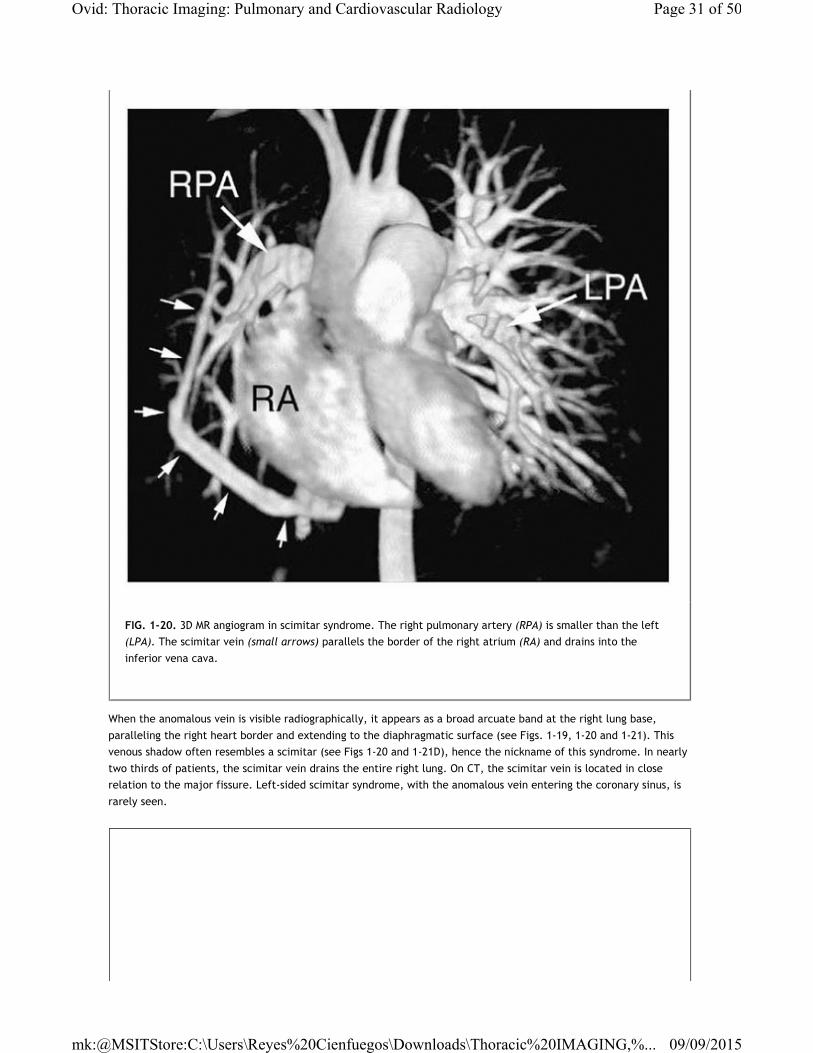
FIG. 1-20. 3D MR angiogram in scimitar syndrome. The right pulmonary artery (RPA) is smaller than the left
(LPA). The scimitar vein (small arrows) parallels the border of the right atrium (RA) and drains into the
inferior vena cava.
Page 31 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Systemic arteries, usually multiple and usually arising below the diaphragm, typically supply the lower lobe. These
FIG. 1-21. CT in scimitar syndrome. A-C. Lung window scans show typical CT findings of scimitar syndrome,
with hypoplasia of the right lung, evidenced by mediastinal shift to the right, relatively small arteries in the
right lung, and the scimitar vein (white arrows), seen in cross section. The scimitar vein drains into the
inferior vena cava (IVC). Small vessels seen posteriorly (black arrows in C) are systemic arteries supplying the
lung base. D. Right pulmonary arteriogram shows opacification of the scimitar vein (arrows). E. Arteriogram
shows anomalous systemic arteries supplying the right lung base.
TABLE 1-9. PROXIMAL INTERRUPTION OF THE PULMONARY ARTERY
Congenital absence of a main pulmonary artery
Almost always on the side opposite the aortic arch (i.e., usually the right)
Hypoplastic ipsilateral lung
Reduced size of ipsilateral pulmonary vessels
Lung vascular supply derived from bronchial arteries
Mediastinal shift toward the hypoplastic lung
Congenital heart disease common (tetralogy of Fallot, septal defects)
Page 32 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

may be visible using CT (see Fig. 1-21C and E).
In some patients, findings of the scimitar syndrome may be associated with “horseshoe lung.” Horseshoe lung is a
rare congenital malformation in which an isthmus of pulmonary parenchyma extends from the right lung base across
the midline behind the pericardium and fuses with the base of the left lung. Horseshoe lung may occur in the
absence of scimitar syndrome.
PROXIMAL INTERRUPTION OF THE PULMONARY ARTERYThis anomaly can closely resemble hypogenetic lung syndrome. In proximal interruption of the pulmonary artery, the
proximal portion of a main pulmonary artery, usually the right, fails to develop (Table 1-9). The ipsilateral lung is
hypoplastic because of deficient growth but has a normal number of lobes and segments, and bronchial anatomy is
normal. Vessels within the lung appear small (Fig. 1-22), whereas those on the opposite side are much larger. The
lung vascular supply is derived from hypertrophied bronchial arteries (see Fig. 1-22B). This entity is often associated
with congenital heart disease, most typically tetralogy of Fallot and septal defects. This anomaly usually occurs on
the side opposite the aortic arch (Fig. 1-23). When the interrupted pulmonary artery and aorta are ipsilateral, the
incidence of congenital heart disease is higher than when they are not.
P.19
FIG. 1-21. (Continued.)
Page 33 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-22. Proximal interruption of the right pulmonary artery. A. Chest radiograph shows mediastinal shift to
the right with small right pulmonary vessels and a large left pulmonary artery (arrow). B. Contrast-enhanced
CT shows the ascending aorta (Ao) and a large left pulmonary artery (LPA), but the right pulmonary artery is
absent. Large bronchial arteries (arrows) supply the right lung. C. Lung window scan shows hypoplasia of the
right lung and small right lung vessels.
P.20
Page 34 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

UNILATERAL PULMONARY VEIN ATRESIAIn unilateral pulmonary vein atresia, another rare entity, long segments of the pulmonary veins of one lung are
congenitally atretic (Table 1-10). The involved lung can be normal in size or hypoplastic, and it often shows
increased interstitial densities because of venous stasis, edema, and fibrosis. The ipsilateral pulmonary artery may
appear small. Radionuclide imaging shows decreased perfusion. Angiography shows decreased size of the ipsilateral
pulmonary artery, peripheral pruning, contrast stasis, and nonvisualization of the pulmonary veins. Symptoms
include hemoptysis and infection.
PULMONARY VEIN VARIXDilation of a pulmonary vein branch (pulmonary vein varix) can be congenital or acquired (Table 1-11). One or more
veins appear dilated or tortuous near the point they enter the left atrium. With congenital varices, symptoms are
usually absent, although rupture rarely occurs.
Acquired varies are associated with chronically elevated left atrial pressure, as in mitral stenosis. These most
commonly involve the right inferior pulmonary vein. On plain radiographs, these are visible through the right part of
the heart shadow and often appear rounded and sharply defined. They may mimic the appearance of a lung nodule,
leading to further evaluation. CT is diagnostic.
FIG. 1-23. Proximal interruption of the left pulmonary artery in a patient with right aortic arch. A. Chest
radiograph shows mediastinal shift to the left. B. Contrast-enhanced CT shows the ascending aorta (Ao), a
right-sided descending aorta (DA), and a large right pulmonary artery (RPA), but the left pulmonary artery is
absent. Large bronchial arteries (arrows) supply the hypoplastic left lung.
TABLE 1-10. PULMONARY VEIN ATRESIA
Pulmonary veins of one lung atretic
Lung hypoplastic or normal in volume
Reduced size of ispilateral pulmonary artery
Increased interstitial opacity in lung
TABLE 1-11. PULMONARY VEIN VARIX
Page 35 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
ANOMALOUS PULMONARY VEIN DRAINAGEAnomalous pulmonary vein drainage involves drainage of a pulmonary vein branch into the right atrium, coronary
sinus, or systemic vein, producing a left-to-right shunt (Table 1-12).
Partial anomalous pulmonary venous drainage is present in about 0.5% of the population and is usually
asymptomatic. The anomalous vein may drain into various vascular structures. On the right, the most common are
the superior vena cava (Fig. 1-24), azygos vein, inferior vena cava, and right atrium. On the left, drainage may be
through the left brachiocephalic vein, persistent left superior vena cava (vertical vein; Fig. 1-25), or coronary sinus.
Drainage may also be below the diaphragm.
Total anomalous pulmonary venous drainage must be associated with a septal defect and is best considered to be a
type of congenital heart disease.
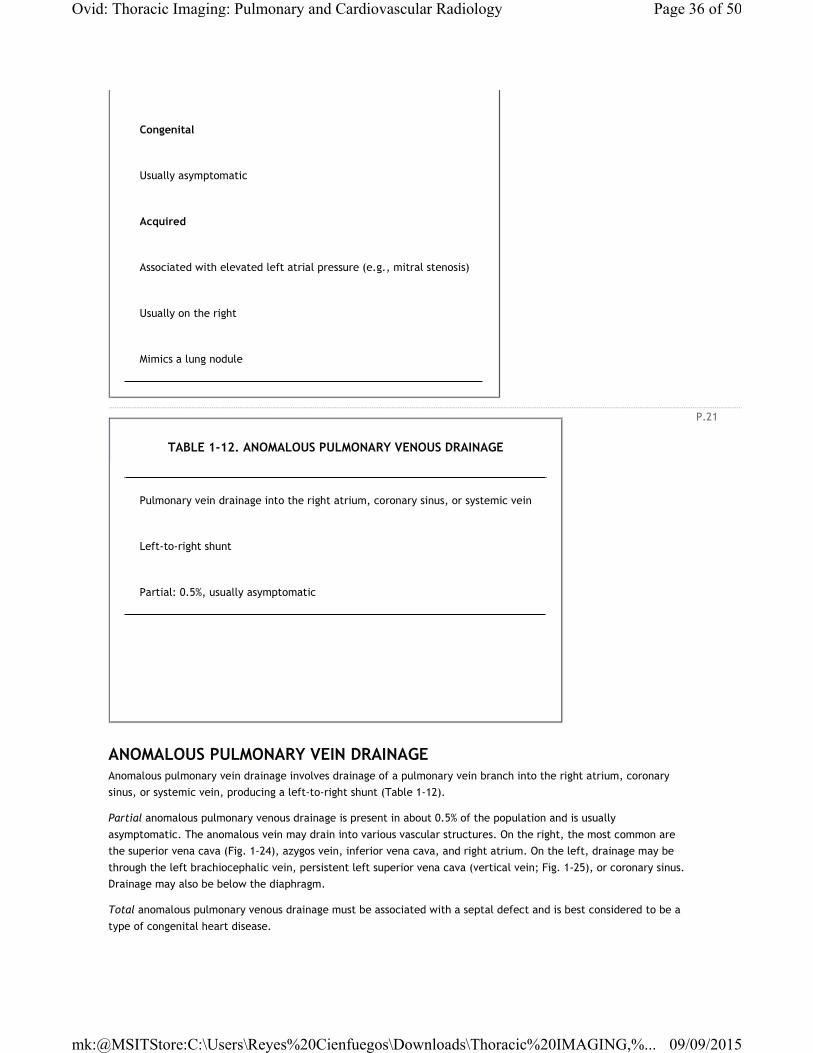
Congenital
Usually asymptomatic
Acquired
Associated with elevated left atrial pressure (e.g., mitral stenosis)
Usually on the right
Mimics a lung nodule
P.21
TABLE 1-12. ANOMALOUS PULMONARY VENOUS DRAINAGE
Pulmonary vein drainage into the right atrium, coronary sinus, or systemic vein
Left-to-right shunt
Partial: 0.5%, usually asymptomatic
Page 36 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

BRONCHOPULMONARY SEQUESTRATIONBronchopulmonary sequestration is a congenital malformation resulting from abnormal budding of the foregut and its
associated structures during the period that lung, bronchi, and pulmonary vessels are developing. Pathologically,
sequestration represents an area of disorganized pulmonary parenchyma without normal pulmonary arterial or
bronchial communications (i.e., it is sequestered from bronchi and pulmonary arteries). Sequestration usually
receives its blood supply from branches of the thoracic or abdominal aorta, and aortography is usually necessary
before surgical excision in order to visualize these arterial branches. Fatal hemorrhage can occur if these systemic
arteries are accidentally cut during surgery. There are two forms of sequestration—intralobar and extralobar.
Although they share some features, they differ significantly in several important clinical and radiographic
characteristics.
Intralobar SequestrationIntralobar sequestration is the more common of these two malformations. In this anomaly, sequestered lung lies
within the visceral pleura of one of the lobes. It occurs most often on the left side, and approximately two thirds are
found adjacent to the diaphragm in relation to the posterior basal segment of the left lower lobe (Table 1-13). In
almost 75% of cases, the arterial supply of an intralobar sequestration is from the descending thoracic aorta; others
receive supply from branches of the abdominal aorta or from intercostal arteries. These systemic arteries often
enter the lung via the inferior pulmonary ligament. Usually venous drainage is by pulmonary veins, but drainage into
the azygos or hemiazygos system is not uncommon.
Intralobar sequestration usually presents in adults or older children. Acute or recurrent infection is most common as
a presenting complaint (Fig. 1-26). Hemoptysis may occur. The systemic arterial to pulmonary venous shunt
produced by interlobar sequestration is usually small and clinically insignificant. However, cases resulting in
congestive heart failure have been reported. Bilateral sequestrations may occur. Connection to the esophagus is
rarely seen. Association with other anomalies is uncommon.
FIG. 1-24. Partial anomalous pulmonary vein drainage in a patient with a tracheal bronchus. A. The tracheal
bronchus is visible arising from the right tracheal wall (arrow). B. At a lower level, a right superior pulmonary
vein (v) branch enters the superior vena cava (S).
P.22
Page 37 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-25. Partial anomalous pulmonary vein drainage. A. A left pulmonary vein (arrow) enters a left superior
vena cava (vertical vein). B. At a higher level, the left superior vena cava (arrow) is visible lateral to the
aortic arch. C. The left superior vena cava (arrow) drains into the left brachiocephalic vein (bv).
P.23
Page 38 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-26. Intralobar sequestration in a young woman with recurrent left lower lobe pneumonia. A and B.
Patchy consolidation is visible in the left lower lobe (arrows). C. Angiogram shows several branches (small
arrows) of the descending aorta resulting in opacification of the sequestration (Seq). Drainage is into the
azygos vein (large arrow).
P.24
TABLE 1-13. INTRALOBAR SEQUESTRATION
Page 39 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Uncomplicated intralobar sequestration can have a variety of appearances. It may appear as (1) a homogeneous and
well-defined mass lesion (Fig. 1-27), (2) a cystic or multicystic air and fluid-filled lesion, (3) a hyperlucent and
hypovascular region of lung (Fig. 1-28), or (4) a combination of these. Hyperlucency is common in uncomplicated
sequestration due to air trapping; this may be difficult to recognize on chest radiographs but is commonly seen at CT
(see Fig. 1-28). The presence of mucous or fluid-filled cysts with air-fluid levels can be seen with or without
infection. In such cases, a sequestration can closely mimic lung abscess. Rarely, bilateral sequestrations may be
seen. These often are supplied by a single artery (Fig. 1-29).
On CT, bronchi or normal pulmonary arteries can be shown draped over the lesion (see Fig. 1-28) but do not enter a
sequestration. With contrast-enhanced spiral CT, the supplying systemic arteries are often visible (see Figs. 1-27 and
1-28). If not, aortography can be used to confirm the diagnosis. The draining veins can also be identified following
contrast infusion.
More common than extralobar sequestration
Within visceral pleural of lobe
65% at left base
No pulmonary artery or bronchial supply
Arterial supply from thoracic aorta in 75%
Drainage via pulmonary veins in most
Presentation in older children or adults
Recurrent infection
Imaging appearances:
Homogeneous and well-defined mass lesion
Cystic or multicystic air- and fluid-filled lesion
Hyperlucent and hypovascular region of lung
Combination of these
Page 40 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
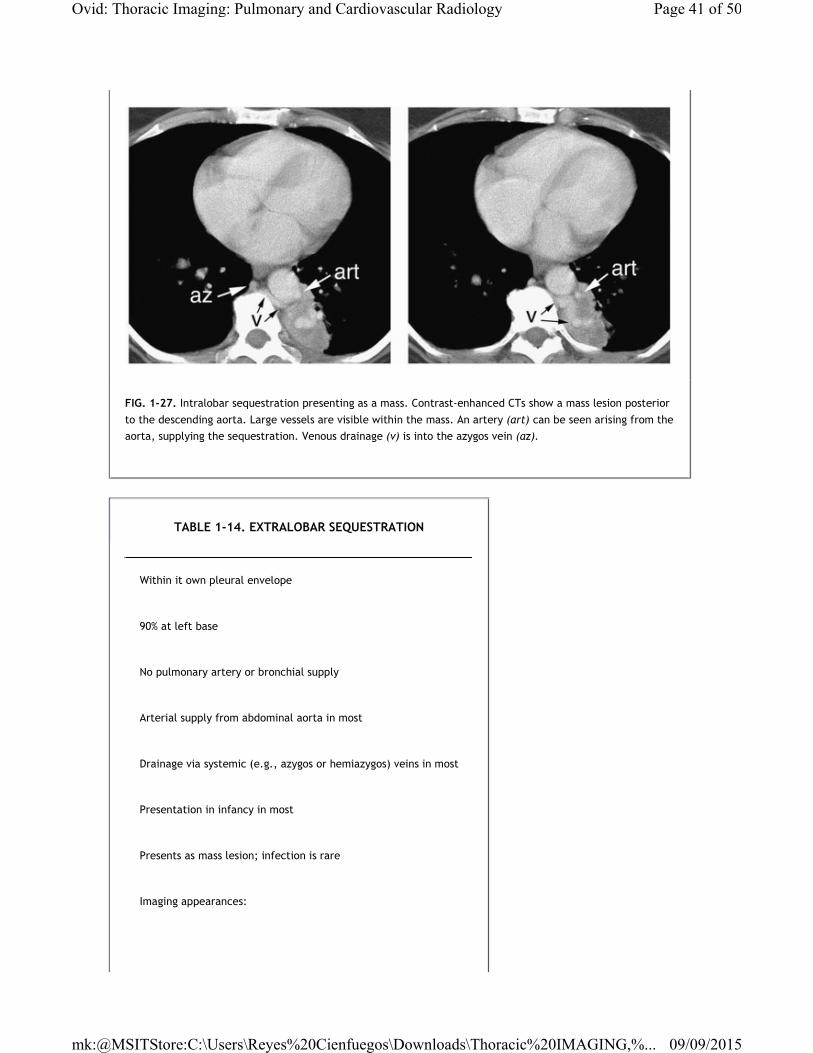
FIG. 1-27. Intralobar sequestration presenting as a mass. Contrast-enhanced CTs show a mass lesion posterior
to the descending aorta. Large vessels are visible within the mass. An artery (art) can be seen arising from the
aorta, supplying the sequestration. Venous drainage (v) is into the azygos vein (az).
TABLE 1-14. EXTRALOBAR SEQUESTRATION
Within it own pleural envelope
90% at left base
No pulmonary artery or bronchial supply
Arterial supply from abdominal aorta in most
Drainage via systemic (e.g., azygos or hemiazygos) veins in most
Presentation in infancy in most
Presents as mass lesion; infection is rare
Imaging appearances:
Page 41 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Extralobar SequestrationExtralobar sequestration represents an anomaly in which the sequestered tissue is enclosed within its only pleural
envelope; it is less common than intralobar sequestration. Approximately 90% of cases are visible at the left lung
base, contiguous with the left hemidiaphragm (Table 1-14). Arterial supply is usually from the abdominal aorta and
drainage is almost always by means of systemic veins (inferior vena cava, azygos, hemiazygos, or portal veins),
producing a left-to-right shunt. Rarely, they may be located within the diaphragm or immediately below the
diaphragm in the upper abdomen.
Homogeneous and well-defined mass lesion
May contain fluid-filled cystic areas
Rarely contains air
P.25
Page 42 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
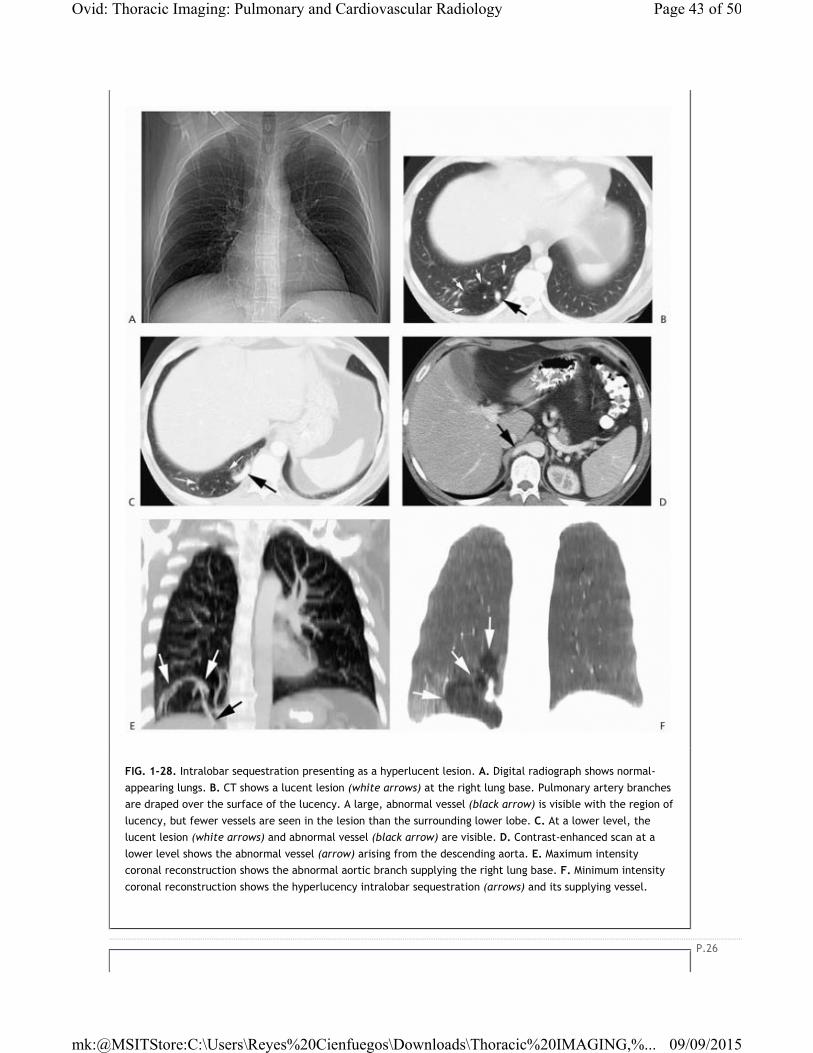
FIG. 1-28. Intralobar sequestration presenting as a hyperlucent lesion. A. Digital radiograph shows normal-
appearing lungs. B. CT shows a lucent lesion (white arrows) at the right lung base. Pulmonary artery branches
are draped over the surface of the lucency. A large, abnormal vessel (black arrow) is visible with the region of
lucency, but fewer vessels are seen in the lesion than the surrounding lower lobe. C. At a lower level, the
lucent lesion (white arrows) and abnormal vessel (black arrow) are visible. D. Contrast-enhanced scan at a
lower level shows the abnormal vessel (arrow) arising from the descending aorta. E. Maximum intensity
coronal reconstruction shows the abnormal aortic branch supplying the right lung base. F. Minimum intensity
coronal reconstruction shows the hyperlucency intralobar sequestration (arrows) and its supplying vessel.
P.26
Page 43 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-29. Bilateral intralobar sequestrations supplied by a single anomalous branch of the descending aorta
(subtracted arteriogram).
Page 44 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-30. Extralobar sequestration in a neonate. A. Chest radiograph shows a soft tissue mass at the left base
(arrows). B and C. Contrast-enhanced CTs show a soft tissue mass with arterial supply (arrows) from the
aorta. D. Aortogram performed via umbilical artery catheter shows anomalous arteries supplying the left base.
P.27
TABLE 1-15. COMPARISON OF INTRALOBAR AND EXTRALOBAR SEQUESTRATION
Intralobar sequestration Extralobar sequestration
Patient age Adult or older child Infant or child
Symptoms Infection common Infection rare
Morphology Within a lobe Within its own pleural envelope
Page 45 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Extralobar sequestration is often diagnosed in infancy (unlike intralobar sequestration) (Table 1-15). It is detected
incidentally or presents as a mass lesion (Fig. 1-30). Unlike intralobar sequestration, infection is rare. Associated
congenital anomalies, particularly diaphragmatic abnormalities and ipsilateral lung hypoplasia, are common. Because
of its complete pleural envelope, extralobar sequestration rarely becomes infected.
Location 65% at left base 90% at left base
Arterial supply Thoracic or abdominal aorta Usually abdominal aorta
Venous drainage Usually pulmonary veins Usually systemic veins
Appearance Commonly contains air Rarely contains air
FIG. 1-31. Extralobar sequestration in an adult. PA (A) and lateral (B) chest radiographs show a mass (arrows)
at the left base. C. Contrast-enhanced CT shows opacified vessels (black arrow) within the mass (white
Page 46 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

Radiographically and on CT, extralobar sequestration appears as a sharply marginated mass lesion, which does not
contain air (unlike intralobar sequestration) (see Figs. 1-30 and 1-31). It is usually homogeneous in appearance but
may contain cystic areas. Its supplying artery may be seen on CT. If not, aortography may be need for diagnosis.
ANOMALOUS SYSTEMIC ARTERIES WITHOUT SEQUESTRATION (SYSTEMIC ARTERIAL MALFORMATION)Systemic arteries may supply normal basal segments of lung (Table 1-16). Although these lesions can be thought of as
representing systemic AVMs, they are unassociated with the large, dilated vascular sac typically seen with pulmonary
AVMs. Rather, the arteriovenous communications in patients with systemic arterial malformations usually represent
normal capillaries.
arrows).
P.28
P.29
Page 47 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

FIG. 1-32. Anomalous systemic arteries without sequestration in a patient with hemoptysis. A. Radiograph of
the right lower lobe appears normal. B. Pulmonary arteriogram shows an area of lung (*) without pulmonary
artery supply. C. An abnormal arterial branch (arrows) from the descending aorta supplies this region of lung.
TABLE 1-16. SYSTEMIC ARTERY MALFORMATION
Page 48 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...

This lesion is probably best thought of as anomalous systemic arterial supply to an area of lung due to persistence of
an embryonic aortic branch. The pulmonary parenchyma in the region supplied by the anomalous artery is normal, as
are bronchial communications (Fig. 1-32). The pulmonary artery supply to these areas can be normal or absent.
A relationship may exist between systemic arterial malformations and pulmonary sequestration, and both these
lesions represent different points on the spectrum of anomalies affecting the pulmonary artery, systemic arteries,
and bronchial development. Some cases have been reported in which intralobar sequestration on one side coexists
with systemic arterial malformation on the other. In such cases, both lesions are typically supplied by the same
aortic branch.
Because systemic arterial malformation results in a left-to-left arterial shunt, left ventricular enlargement and
congestive heart failure can occur. Hemoptysis may also occur. However, most patients have no symptoms. If the
anomalous vessel supplies an area of lung also supplied by the pulmonary artery, treatment involves ligation or
embolization of the anomalous vessel.
SELECTED READING
Dines DE, Arms RA, Bernatz PE, Gomes MR. Pulmonary arteriovenous fistulas. Mayo Clin Proc 1974; 49:460-
465.
Do KH, Goo JM, Im JG, et al. Systemic arterial supply to the lungs in adults: spiral CT findings. Radiographics
2001; 21:387-402.
Fitch SJ, Tonkin ILD, Tonkin AK. Imaging of foregut cysts. Radiographics 1986; 6:189-201.
Ghaye B, Szapiro D, Fanchamps JM, Dondelinger RF. Congenital bronchial abnormalities revisited.
Radiographics 2001; 21: 105-119.
Ikezoe J, Murayama S, Godwin JD, et al. Bronchopulmonary sequestration: CT assessment. Radiology 1990;
176:375-379.
Arterial supply to lung from thoracic or abdominal aorta
Lung normal
Bronchi normal
Pulmonary artery normal or absent in affected region
Pulmonary vein drainage normal
Congestive heart failure or hemoptysis
Page 49 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...
Mata JM, Caceres J, Lucaya J, Garcia-Conesa JA. CT of congenital malformations of the lung. Radiographics
1990; 10:651-674.
McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, Matsumoto S. Bronchogenic cyst: imaging features
with clinical and histopathologic correlation. Radiology 2000; 217:441-446.
Patz EF Jr, Müller NL, Swensen SJ, Dodd LG. Congenital cystic adenomatoid malformation in adults: CT
findings. J Comput Assist Tomogr 1995; 19:361-364.
Rappaport DC, Herman SJ, Weisbrod GL. Congenital bronchopulmonary diseases in adults: CT findings. AJR
Am J Roentgenol 1994; 162:1295-1299.
Remy J, Remy-Jardin M, Wattinne L, Deffontaines C. Pulmonary arteriovenous malformations: evaluation
with CT of the chest before and after treatment. Radiology 1992; 182:809-816.
Roehm JOF, Jue KL, Amplatz K. Radiographic features of the scimitar syndrome. Radiology 1966; 86:856-859.
Rosado-de-Christenson ML, Stocker JT. Congenital cystic adenomatoid malformation. Radiographics 1991;
11:865-886.
Sener RN, Tugran C, Savas R, Alper H. CT findings in scimitar syndrome. AJR Am J Roentgenol 1993; 160:1361.
Shenoy SS, Culver GJ, Pirson HS. Agenesis of lung in an adult. AJR Am J Roentgenol 1979; 133:755-757.
Yamanaka A, Hirai T, Fujimoto T, et al. Anomalous systemic arterial supply to normal basal segments of the
left lower lobe. Ann Thorac Surg 1999; 68:332-338.
Page 50 of 50Ovid: Thoracic Imaging: Pulmonary and Cardiovascular Radiology
09/09/2015mk:@MSITStore:C:\Users\Reyes%20Cienfuegos\Downloads\Thoracic%20IMAGING,%...