nerve injuries in gynecologic laparoscopy · in benign gynecologic surgery, ... longer surgical...
TRANSCRIPT
Review Article
Nerve Injuries in Gynecologic Laparoscopy
Osama S. Abdalmageed, MD, Mohamed A. Bedaiwy, MD, PhD, and Tommaso Falcone, MD*From the Women’s Health Center, Department of Obstetrics & Gynecology, Faculty of Medicine (Dr. Abdalmageed), Assiut University, Assiut, Egypt,
Division of Reproductive Endocrinology and Infertility (Dr. Bedaiwy), Department of Obstetrics and Gynecology (Dr. Bedaiwy), University of British
Columbia, Vancouver, British Columbia, Canada, and Department of Obstetrics and Gynecology (Dr. Falcone), Cleveland Clinic Foundation,
Cleveland, Ohio.
ABSTRACT Nerve injuries during gynecologic endoscopy are an infrequent but distressing complication. In benign gynecologic surgery,
The authors decla
Corresponding au
Department of O
tion, 9500 Euclid
E-mail: falconet@
Submitted Augus
Available at www
1553-4650/$ - see
http://dx.doi.org/1
most of these injuries are associated with patient positioning, although some are related to port placement. Most are poten-tially preventable with attention to patient placement on the operating room bed and knowledge of the relative anatomy of thenerves. The highest risk group vulnerable to these injuries includes women who have extreme body mass index and those withlonger surgical times in the Trendelenburg position. Upper and lower limb peripheral nerves are the most common nervesinjured during gynecologic endoscopy. These injuries can result in transient or permanent sensory and motor disabilitiesthat can interrupt patient recovery in an otherwise successful surgery. Numerous strategies are suggested to reduce the fre-quency of nerve injuries during gynecologic endoscopies. Proper patient positioning and proper padding of the pressure areasare mandatory to prevent malposition-related nerve injuries. Anatomic knowledge of the course of nerves, especially ilioin-guinal and iliohypogastric, nerves can minimize injury. Journal of Minimally Invasive Gynecology (2017) 24, 16–27� 2016AAGL. All rights reserved.
Keywords: Brachial plexus; Gynecologic endoscopy; Laparoscopy complications; Lithotomy; Lumbosacral plexus; Nerve injury; Trendelenburg
Iatrogenic nerve injuries after gynecologic laparoscopicprocedures are not common but do occur. The main causesare poor patient positioning during anesthesia, improperuse of stirrups, inadequate padding protecting nerve-exposed areas, lengthy operations, and closure of lowerlateral port trocar insertion sites [1,2]. The most commonnerves susceptible to injury originate from the lumbar,lumbosacral, and brachial plexus, but any nerves in theupper and lower limbs and the lower anterior abdominalwall can be affected. Most injuries have a good prognosisand are self-limited with spontaneous recovery or physicaltherapy. However, some patients will need long-term treat-ment and medical therapy for treatment of chronic painand may need surgical intervention [2].
Identifying patients who are vulnerable to neurologiccomplications is important in the prevention and early
re that they have no conflict of interest.
thor: Tommaso Falcone, MD, Professor and Chairman,
bstetrics and Gynecology-A81, Cleveland Clinic Founda-
Avenue, Cleveland, OH 44195.
ccf.org
t 1, 2016. Accepted for publication September 7, 2016.
.sciencedirect.com and www.jmig.org
front matter � 2016 AAGL. All rights reserved.
0.1016/j.jmig.2016.09.004
identification of nerve injuries related to gynecologic lap-aroscopies. Surgeon awareness of the anatomy of thesenerves and injury mechanisms can help avoid most in-juries. Therefore, in this article we review the anatomy ofthe female pelvis and the risks and mechanisms of nerveinjury associated with gynecologic laparoscopic surgeries.We also review preventive strategies to reduce periopera-tive neuropathies.
Incidence
The exact incidence of nerve injuries caused by gyneco-logic laparoscopic surgery is not well documented, possiblybecause such injuries are uncommon and usually resolve ontheir own. Bohrer et al [3] conducted a prospective cohorttrial of 616 female patients who underwent elective gyneco-logic surgeries to evaluate the incidence and the prognosis ofpostoperative neuropathies related to vaginal surgeries. Theyfound that the overall incidence of nerve injuries was 1.8%and that the most frequently injured nerves were the lateralfemoral cutaneous nerve of the thigh and the femoral nerve[3]. A retrospective study of the medical records of 1210 pa-tients who underwent major pelvic surgeries estimated theincidence of postoperative neuropathy to be 1.9% [4].
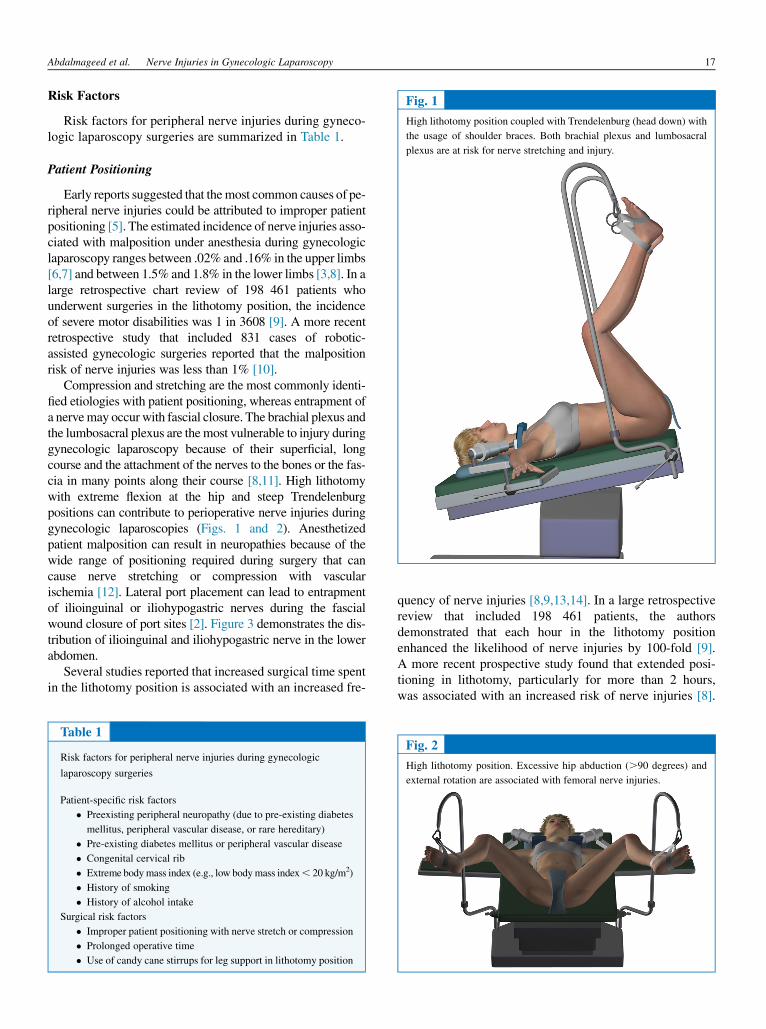
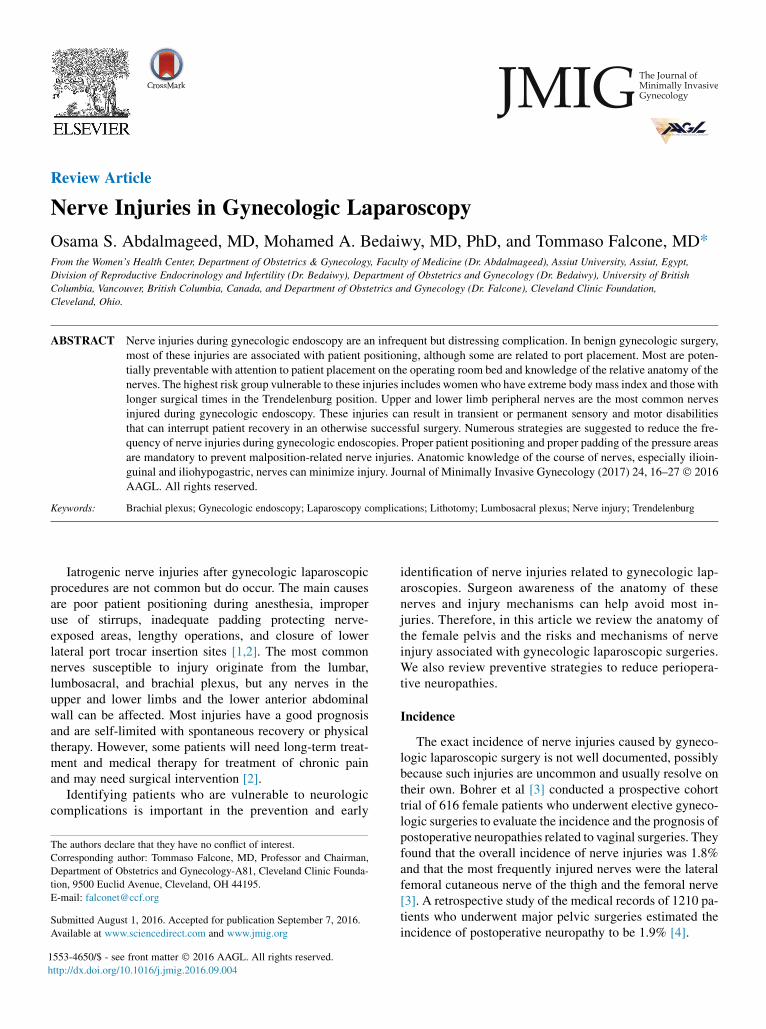
Fig. 1
High lithotomy position coupled with Trendelenburg (head down) with
the usage of shoulder braces. Both brachial plexus and lumbosacral
plexus are at risk for nerve stretching and injury.
Abdalmageed et al. Nerve Injuries in Gynecologic Laparoscopy 17
Risk Factors
Risk factors for peripheral nerve injuries during gyneco-logic laparoscopy surgeries are summarized in Table 1.
Patient Positioning
Early reports suggested that themost common causes of pe-ripheral nerve injuries could be attributed to improper patientpositioning [5]. The estimated incidence of nerve injuries asso-ciated with malposition under anesthesia during gynecologiclaparoscopy ranges between .02% and .16% in the upper limbs[6,7] and between 1.5% and 1.8% in the lower limbs [3,8]. In alarge retrospective chart review of 198 461 patients whounderwent surgeries in the lithotomy position, the incidenceof severe motor disabilities was 1 in 3608 [9]. A more recentretrospective study that included 831 cases of robotic-assisted gynecologic surgeries reported that the malpositionrisk of nerve injuries was less than 1% [10].
Compression and stretching are the most commonly identi-fied etiologies with patient positioning, whereas entrapment ofa nervemay occur with fascial closure. The brachial plexus andthe lumbosacral plexus are themost vulnerable to injury duringgynecologic laparoscopy because of their superficial, longcourse and the attachment of the nerves to the bones or the fas-cia in many points along their course [8,11]. High lithotomywith extreme flexion at the hip and steep Trendelenburgpositions can contribute to perioperative nerve injuries duringgynecologic laparoscopies (Figs. 1 and 2). Anesthetizedpatient malposition can result in neuropathies because of thewide range of positioning required during surgery that cancause nerve stretching or compression with vascularischemia [12]. Lateral port placement can lead to entrapmentof ilioinguinal or iliohypogastric nerves during the fascialwound closure of port sites [2]. Figure 3 demonstrates the dis-tribution of ilioinguinal and iliohypogastric nerve in the lowerabdomen.
Several studies reported that increased surgical time spentin the lithotomy position is associated with an increased fre-
Table 1
Risk factors for peripheral nerve injuries during gynecologic
laparoscopy surgeries
Patient-specific risk factors
� Preexisting peripheral neuropathy (due to pre-existing diabetes
mellitus, peripheral vascular disease, or rare hereditary)
� Pre-existing diabetes mellitus or peripheral vascular disease
� Congenital cervical rib
� Extreme bodymass index (e.g., low bodymass index, 20 kg/m2)
� History of smoking
� History of alcohol intake
Surgical risk factors
� Improper patient positioning with nerve stretch or compression
� Prolonged operative time
� Use of candy cane stirrups for leg support in lithotomy position
quency of nerve injuries [8,9,13,14]. In a large retrospectivereview that included 198 461 patients, the authorsdemonstrated that each hour in the lithotomy positionenhanced the likelihood of nerve injuries by 100-fold [9].A more recent prospective study found that extended posi-tioning in lithotomy, particularly for more than 2 hours,was associated with an increased risk of nerve injuries [8].
Fig. 2
High lithotomy position. Excessive hip abduction (.90 degrees) and
external rotation are associated with femoral nerve injuries.

Fig. 3
The shaded areas demonstrate the distribution of ilioinguinal and iliohypo-
gastric nerves, which should be avoided during lateral port insertion in gy-
necologic laparoscopy. The main anatomic landmark is the ASIS. Avoid
placing trocars, especially those requiring fascial closure, below this level.
18 Journal of Minimally Invasive Gynecology, Vol 24, No 1, January 2017
Similarly, a positive correlation was observed betweenbrachial plexus injuries and extended operative duration[11,15]. However, Winfree et al did not find the duration tobe an important risk factor for postoperative peripheralneuropathy but suggested that nerve injuries can occurduring long and short operations. The introduction ofrobotic-assisted laparoscopic surgeries may require patientpositioning in the steepest degree (head-down tilt 30–40 de-grees) of the Trendelenburg position, which is associatedwith patient sliding and possible brachial plexus injuries[17]. Robotic-assisted laparoscopy can increase the risk ofperioperative neuropathies because of its heavy arms, itspositioning near to the lower extremities, and the need toplace the patient in an extreme position [18].
Support Devices
Some types of leg supports increase the risk of nerve injuriesbecause of inadequate support (e.g., ‘‘candy cane’’ leg sup-ports). Shoulder braces can lead to nerve compression as well.
Port Placement
Lateral port placement and lateral port fascial closure inthe lower abdomen can result in iliohypogastric and ilioin-
guinal nerve injuries if the ports are placed low in theabdomen [18].
Patient-Specific Predisposing Factors
Some patients are more susceptible to nerve injuriesbecause of the presence of predisposing factors [5] such aspre-existing generalized peripheral neuropathy [19]. The un-derlying cause of peripheral neuropathy can be diabetes melli-tus or peripheral vascular disease; in rare cases, it is hereditary[20–23]. Patients with controlled or uncontrolled disease are atan increased risk for perioperative neuropathies [24]. Althoughthere are no comparative data, we assume that because uncon-trolled diabetics are at greater risk for diabetic neuropathy, theywould also be at higher risk for perioperative neuropathies thatare due to ischemia.
The presence of a cervical rib is a risk factor for brachialplexus entrapment during surgery [16]. Studies have shownthat patients with an extreme high or low body mass index,particularly when it is less than 20 kg/m2, and those whoare older than 60 years of age are more susceptible to nervepressure injuries. In these patients, the peripheral nervesseem to be less protected and more sensitive to pressure[17,24,25–27]. A history of smoking or alcohol intake isconsidered a risk factor for perioperative peripheral nerveinjuries [28]. Other patient-related conditions that can in-crease the risk of postoperative peripheral neuropathyinclude hypovolemia, hypotension, electrolyte disturbance,and malnutrition [5].
Pathophysiology and Classification
The peripheral nerves consist of bundles of nerve fibersthat conduct signals from and to the central nervous system.The axon is surrounded by a myelin sheath and Schwanncells. Each nerve is walled with triple layers of connectivetissue: deep endoneurium, superficial epineurium, and peri-neurium in between. The vasa nervorum are minute arteriesresponsible for the blood supply of the interior of the nervesand their coverings.
Postoperative neuropathy after gynecologic laparoscopysurgeries can be the consequence of pressure, stretching,entrapment, or laceration of the nerves [29]. Although lowerlateral trocar placement and fascial wound closure duringgynecologic laparoscopy can be associated with direct par-tial or complete nerve laceration, it is usually a result ofentrapment [1]. The degree of nerve trauma can be classifiedaccording to its severity by Seddon’s or Sunderland’s classi-fications, as shown in Table 2 [30,31]. The use ofclassification systems can help the surgeon anticipate thepatient’s prognosis and treatment options.
Perioperative peripheral neuropathy can cause a varietyof signs and symptoms such as loss of sensation, pain, numb-ness, and muscle weakness with motor disabilities; inabilityto move a limb; and loss of reflexes [26]. The severity ofnerve damage is proportional to the degree and duration of

Table 2
Classification of nerve injury according to the degree severity
Classification
Nerve pathology Pathophysiology PrognosisSunderland [30] Seddon [31]
I Neuropraxia
(Class I)
Possible demyelination at the site
of injury
No Wallerian degeneration
Focal conduction block Full recovery within 1 day up to
12 weeks
II Axonotmesis
(Class II)
Some axon injury with Wallerian
degeneration
Intact endoneurium, perineurium, and
epineurium
Complete loss of nerve function at
the site of injury and distally
Full recovery (slow/up to 4 months)
III Axon and endoneurium disruption
with Wallerain degeneration
Intact epineurium and epineurium
Complete loss of nerve function at
the site of injury and distally
Variable (full to incomplete within
weeks to months)
IV Axonal, endoneurium, and
perineurium disruption
Intact epineurium
Complete loss of nerve function at
the site of injury and distally
Unlikely for recover without
surgical intervention
V Neurotmesis
(Class III)
Complete transection or tearing of the
nerve (disruption in all nerve layers)
Complete loss of nerve function at
the site of injury and distally
No recovery without surgical
intervention
Abdalmageed et al. Nerve Injuries in Gynecologic Laparoscopy 19
nerve compression [32]. Nerve injuries caused by pressurecan occur within 15 to 30 minutes from the start of the pro-cedure, although it is possible that motor nerve fibers can beaffected within 60 seconds [33]. These are not associatedwith axonal damage.
Conduction Block (Neuropraxia)
Neuropraxia is the mildest type of nerve injury and is notassociated with axonal damage (noWallerian degeneration).Nerve stretching and compression usually result in tempo-rary nerve ischemia that leads to transient focal axonal con-duction block (neuropraxia) across the affected portion ofthe nerve [30,34,35]. This transient conduction blockusually resolves in few minutes. However, if it isassociated with elevated venous pressure and edema, itmay lead to sustained dysfunction that requires weeks tomonths to completely resolve [36,37]. Consistent andchronic nerve compression will result in Schwan celldamage and demyelination, which can interrupt impulseconduction down the nerve [38]. Motor nerve fibers seemto more affected by slight nerve injury [39]. The averagetime for recovery of neuropraxia is 4 to 6 weeks [40].
Axonal Damage (Axonotmesis)
Profound nerve compression or traction can lead to phys-ical axonal disruption and result in Wallerian degeneration;the supporting Schwan cells are usually not affected. Axonaldamage affects motor, sensory, and autonomic function [39].This incomplete nerve injury can lead to prolonged dysfunc-tion that requires weeks to months to completely resolve[35,41]. The proximal axon grows at rate 2 to 3 mm/day[42]. However, recovery is usually complete in most casesbecause the Schwan cell layer is intact [43].
Nerve Damage (Neurotmesis)
Neurotmesis is the most severe form of nerve injury and iscaused by nerve compression, stretching, or complete nervetransection or ligation. This type of nerve injury is associatedwith complete neural separation (neurotmesis), includingdisruption of both the axon and Schwan cells. This type ofinjury has the worst prognosis and will not resolve withoutsurgical intervention [16,35].
Upper Extremity Nerve Injuries
The nerve supply of the upper extremities originates fromthe spinal nerve roots in C5-T1; it is integrated to form thebrachial plexus and its peripheral nerves. The brachialplexus is a somatic network of nerve fibers that provides mo-tor and sensory innervation to the upper limbs and shouldergirdle. The peripheral nerves of the upper limbs include 5main nerves: ulnar, radial, median, axillary, and musculocu-taneous. Upper extremity nerve injuries can be attributed topoor positioning of the anesthetized patient and to directcompression of the superficial nerves against hard surfaces.
Brachial Plexus Nerve Injuries
Brachial plexus injuries are uncommon in gynecologiclaparoscopy surgeries but represent the most seriouscomplication because of improper positioning of the anes-thetized patient [7,16]. Table 3 illustrates the summary ofbrachial plexus major nerve injuries with common clinicalfeatures. Extensive arm abduction (Fig. 4), external rota-tion, and posterior shoulder displacement can result inbrachial plexus stretching and ischemia [5]. Directcompression of the brachial plexus can also occur if bracesare placed too medially. According to a cadaver study that
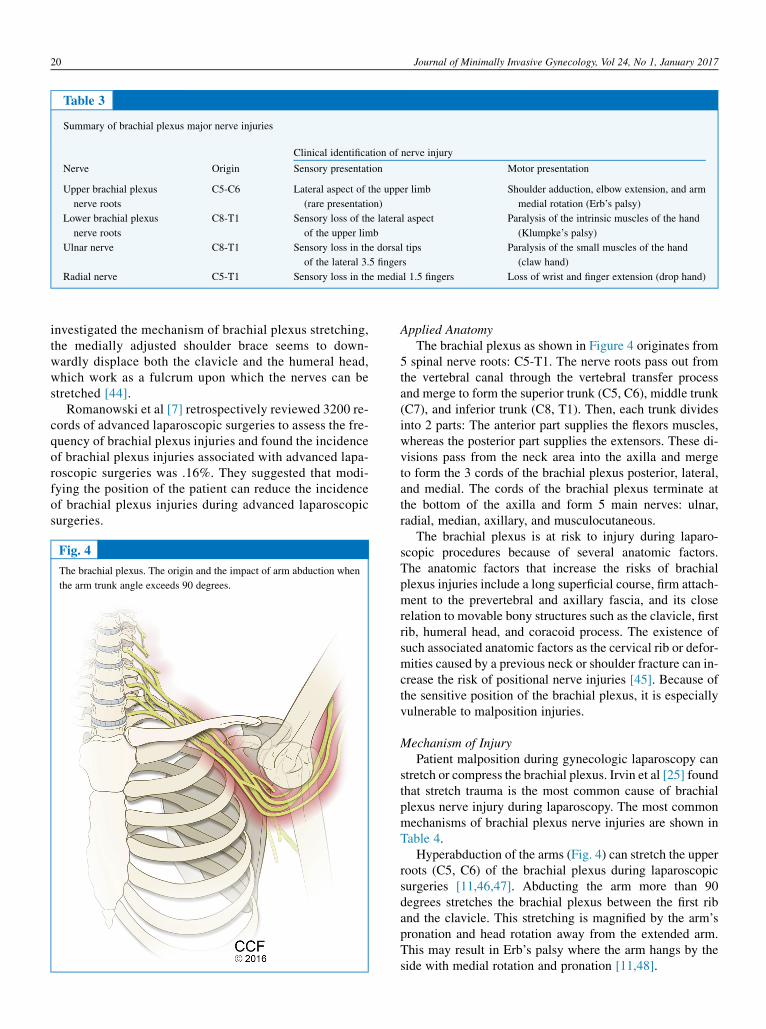
Table 3
Summary of brachial plexus major nerve injuries
Nerve Origin
Clinical identification of nerve injury
Sensory presentation Motor presentation
Upper brachial plexus
nerve roots
C5-C6 Lateral aspect of the upper limb
(rare presentation)
Shoulder adduction, elbow extension, and arm
medial rotation (Erb’s palsy)
Lower brachial plexus
nerve roots
C8-T1 Sensory loss of the lateral aspect
of the upper limb
Paralysis of the intrinsic muscles of the hand
(Klumpke’s palsy)
Ulnar nerve C8-T1 Sensory loss in the dorsal tips
of the lateral 3.5 fingers
Paralysis of the small muscles of the hand
(claw hand)
Radial nerve C5-T1 Sensory loss in the medial 1.5 fingers Loss of wrist and finger extension (drop hand)
20 Journal of Minimally Invasive Gynecology, Vol 24, No 1, January 2017
investigated the mechanism of brachial plexus stretching,the medially adjusted shoulder brace seems to down-wardly displace both the clavicle and the humeral head,which work as a fulcrum upon which the nerves can bestretched [44].
Romanowski et al [7] retrospectively reviewed 3200 re-cords of advanced laparoscopic surgeries to assess the fre-quency of brachial plexus injuries and found the incidenceof brachial plexus injuries associated with advanced lapa-roscopic surgeries was .16%. They suggested that modi-fying the position of the patient can reduce the incidenceof brachial plexus injuries during advanced laparoscopicsurgeries.
Fig. 4
The brachial plexus. The origin and the impact of arm abduction when
the arm trunk angle exceeds 90 degrees.
Applied AnatomyThe brachial plexus as shown in Figure 4 originates from
5 spinal nerve roots: C5-T1. The nerve roots pass out fromthe vertebral canal through the vertebral transfer processand merge to form the superior trunk (C5, C6), middle trunk(C7), and inferior trunk (C8, T1). Then, each trunk dividesinto 2 parts: The anterior part supplies the flexors muscles,whereas the posterior part supplies the extensors. These di-visions pass from the neck area into the axilla and mergeto form the 3 cords of the brachial plexus posterior, lateral,and medial. The cords of the brachial plexus terminate atthe bottom of the axilla and form 5 main nerves: ulnar,radial, median, axillary, and musculocutaneous.
The brachial plexus is at risk to injury during laparo-scopic procedures because of several anatomic factors.The anatomic factors that increase the risks of brachialplexus injuries include a long superficial course, firm attach-ment to the prevertebral and axillary fascia, and its closerelation to movable bony structures such as the clavicle, firstrib, humeral head, and coracoid process. The existence ofsuch associated anatomic factors as the cervical rib or defor-mities caused by a previous neck or shoulder fracture can in-crease the risk of positional nerve injuries [45]. Because ofthe sensitive position of the brachial plexus, it is especiallyvulnerable to malposition injuries.
Mechanism of InjuryPatient malposition during gynecologic laparoscopy can
stretch or compress the brachial plexus. Irvin et al [25] foundthat stretch trauma is the most common cause of brachialplexus nerve injury during laparoscopy. The most commonmechanisms of brachial plexus nerve injuries are shown inTable 4.
Hyperabduction of the arms (Fig. 4) can stretch the upperroots (C5, C6) of the brachial plexus during laparoscopicsurgeries [11,46,47]. Abducting the arm more than 90degrees stretches the brachial plexus between the first riband the clavicle. This stretching is magnified by the arm’spronation and head rotation away from the extended arm.This may result in Erb’s palsy where the arm hangs by theside with medial rotation and pronation [11,48].

Table 4
Brachial plexus nerve injuries and preventive strategies
Nerve Mechanisms of injury Preventive strategies
Upper brachial plexus
nerve roots (C5-C6)
Hyperextension of the armsmore than 90 degrees (magnified
by arm pronation and head rotation away from the arm)
Tuck the pronated arms to the sides of the patient, centralize
the head, and keep the extended arms in supination.
Lower brachial plexus
nerve roots (C8-T1)
Steep Trendelenburg position 30–40 degrees (magnified by
extended arms and the use of shoulder braces)
Try to minimize the angle of inclination in Trendelenburg
position and avoid the use of shoulder braces. If the braces
used, apply them to the acromioclavicular joint and use gel
pads, egg crate or foam mattress pads.
Ulnar nerve (C8-T1) Compression of the ulnar nerve at the point of the medial
epicondyle against hard surface or extreme prolonged
flexion of the elbow
Adequate padding over the posteromedial elbow. Keep the
arms supinated if extended on boards. Keep the arms
pronated if the arms tucked at the patient’s sides.
Radial nerve (C5-T1) Pressure of the radial nerve against the humerus Avoid the position of the arm at the edge of the arm board.
Abdalmageed et al. Nerve Injuries in Gynecologic Laparoscopy 21
The steep Trendelenburg position can stretch the lowerbrachial plexus roots (C8, T1), particularly when the armsare extended (Fig. 1). Injury to the lower roots results inclaw hand (Klumpke’s hand). This stretching is due to ceph-alad movement of the body in relation to the arms, especiallywhen wristlets are used to secure the arms [11,49]. Shoulderbraces, which are used to protect the patient from slidingwhile in the steep Trendelenburg position, seem toincrease brachial plexus traumas, particularly when thearms are extended [7,11]. Braces should not be placed toomedial or too lateral to avoid brachial plexus roots anddivision injuries [16]. The use of wristlet supports can leadto nerve compression injury of the brachial plexus [11].
Sequelae of InjuryBrachial plexus neuropathies can lead to sensory andmotor
deficits. Minor brachial plexus injury can cause transient sen-sory impairment on the medial side of the upper limb. Themore severe affection of the upper roots (C5 and C6) classi-cally leads to Erb’s palsy syndrome (waiter’s tip hand). Injuryof the lower roots (C8 and T1) classically causes Klumpke’sparalysis syndrome (claw hand) [11,18]. Horner’s syndrome(ipsilateral ptosis, miosis, and anhydrosis) may accompanybrachial plexus injuries, particularly when the (T1) nerveroot is injured because of involvement of the nearbycervical chain [11].
Upper Extremity Peripheral Nerve Injuries
The peripheral nerves supplying the upper extremities arederived from the brachial plexus. Themost commonly injurednerves in the upper limbs are the radial nerve and the ulnarnerve because of their course (Table 3). The radial nervecan be compressed while passing through the spiral groove,whereas the ulnar nerve is the most vulnerable to injury whereit is related to the olecranon fossa of the humerus.
Applied AnatomyThe radial nerve passes directly along the spiral groove of
the humerus. Themotor component of the radial nerve inner-
vates the extensor muscles of the wrist and the fingers,whereas its sensory component supplies the posterior aspectof the lateral 3.5 fingers.
The ulnar nerve passes close to the medial epicondyle(passing through the olecranon groove) of the humerus. Atthis point, the superficial ulnar nerve is more susceptible tocompression against the operating table or arm boards[5,20]. The ulnar nerve sensory component supplies themedial 1.5 fingers and its motor component supplies thesmall muscles of the hand [39]. Extreme or prolongedflexion of the elbow across the chest can cause ulnar nervestretching around the medial epicondyle and subsequentinjury [50]. When the arms are tucked on the side of the pa-tient, extra padding should be placed at the elbow.
Mechanism of InjuryPersistent pressure on the humerus or the medial epicon-
dyle of the elbow during arm positioning can damage theradial or the ulnar nerves [51]. The radial nerve can be com-pressed between the edge of the operating table and the hu-merus while passing over the spiral grove, particularly withinadequate padding of the arm. The ulnar nerve can be com-pressed if the patient forearm is pronated on the arm board orwhen the arm is supinated and tucked at the patient side,particularly with inadequate padding to the elbow joint(Table 4) [39].
Sequelae of InjuryRadial nerve neuropathy can lead to paresthesia in the
lateral 3.5 fingers and loss of function in the extensor mus-cles in the wrist and the fingers (wrist drop) [52], whereas ul-nar nerve neuropathy can cause sensory loss or paresthesia inthe medial 1.5 fingers, which may result in claw hand [53].
Lumbosacral Plexus Nerve Injuries
The lumbosacral plexus originates from the third, fourth,and fifth lumbar nerve roots and from the first, second, andthird sacral nerve roots with minimal contribution from thesecond lumbar and fourth sacral nerve root. The most

22 Journal of Minimally Invasive Gynecology, Vol 24, No 1, January 2017
common neuropathies reported with surgeries in the lithot-omy position, summarized in Table 5, involve the femoral,ilioinguinal, iliohypogastric, and lateral femoral cutaneousnerves of the thigh and the sciatic, obturator, and the com-mon peroneal and saphenous nerves. Table 6 summarizesthe most commonmechanisms of lumbosacral nerve injuriesduring laparoscopic surgeries.
Femoral Nerve Injury
The frequency of femoral nerve injuries recorded in gyne-cologic surgeries has recently decreased because of thereduction of the use of self-retaining retractors, which withtheir lateral plates can compress the nerve. A retrospectivereview estimated that femoral nerve motor injuries relatedto the lithotomy position occur in approximately 1 of every50 000 surgeries [9].
Applied AnatomyThe femoral nerve starts as the largest branch of the lum-
bar plexus and is composed of nerve roots L2-L4. It exits thepsoas muscle from its lateral border within the abdomen. Itdescends in the interval between the psoas muscle and theiliacus. The femoral nerve leaves the pelvis below theinguinal ligament to end in the upper third of the thigh whereit branches into anterior and posterior divisions.
Mechanism of InjuryAn inappropriate lithotomy position can be associated
with femoral nerve injury. Prolonged hip flexion, extremeabduction, and external rotation can be associated withstretching and entrapment of the femoral nerve under theinguinal ligament with subsequent interruption of the nerveblood supply and femoral neuropathy [51]. A surgical assis-tant leaning on the patient’s inner thigh during surgery canresult in femoral nerve compression [16].
Table 5
Summary of lumbosacral major nerve injuries
Nerve Origin
Clinical identification of nerve injury
Sensory presentation
Femoral nerve L2-L4 Numbness over the thigh
Obturator nerve L2-L4 Numbness over the upper medial thigh
Sciatic nerve L4-S3 Numbness below the knee (sciatica)
Common peroneal nerve L4-S3 Numbness over the lateral calf and dorsum
the foot
Tibial nerve L4-S3 Numbness of the toes and foot plantar sur
Lateral femoral
cutaneous nerve
L2-L3 Pain or paresthesia of anterioposterior late
(meralgia paresthetica)
Ilioinguinal and
iliohypogastric nerves
T12-L1 Sharp burning pain radiating from incisio
mons, libia, or thigh
Sequelae of Femoral Nerve InjuryFemoral nerve injury can lead to paresthesias of the ante-
romedial aspect of the thigh and themedial aspect of the calf.If the motor fibers of the femoral nerve are involved, the pa-tient may find it difficult to walk because of weakness in hipflexion, adduction, and knee extension. Femoral nerve neu-ropathy results in weakness in the quadriceps muscle with aweak or absent patellar reflex. The classic postoperative pre-sentation of femoral nerve injury is falling when trying to getout of bed and difficulty in climbing stairs [16].
Lateral Femoral Cutaneous Nerve of the Thigh Injury
The lateral femoral cutaneous nerve of the thigh providessensory supply to the lateral surface. A prolonged lithotomyposition can result in lateral femoral cutaneous nervecompression with an estimated incidence of .4% [18].
Applied AnatomyThe lateral femoral cutaneous nerve of the thigh originates
from nerve roots L2-L4 and exits the spinal cord between theL2 andL3 vertebrae. It passes along the outer edge of the psoasmuscle and then below or within the lateral aspect of theinguinal ligament near its insertion to the anterior superior iliacspine (ASIS). However, in rare cases, the lateral cutaneousnerve may enter the thigh lateral to the ASIS or mediallynear the insertion of the inguinal ligament to the pubis [54].
Mechanism of InjuryAs with the femoral nerve, the lateral femoral cutaneous
nerve of the thigh can be injured during gynecologic laparos-copy by entrapment below the inguinal ligament because ofexcessive hip flexion, abduction, and external rotation. Ac-cording to Litwiller et al [55], hip external rotation during li-thotomy results in increased strain on the lateral femoralcutaneous nerve of the thigh.
Motor presentation
Weakness in hip flexion (difficult climbing stairs)
Weakness in hip adduction (minor ambulatory problem)
Weakness in the ankle dorsiflexion and plantar flexion,
and weakness in knee flexion
of Weakness in dorsiflexion of the ankle and toes
(foot drop)
face Weakness of the plantar flexion of the ankle and toes
(cavus deformity foot)
ral thigh None
n site to None

Table 6
Lumbosacral plexus nerve injuries and preventive strategies
Nerve Mechanisms of injury Preventive strategies
Femoral nerve (L2-L4) Prolonged hip flexion, extreme abduction, and external
rotation. Surgical assistant leaning on the inner thigh of
the patient.
Proper positioning of the patient in lithotomy position with
limitation of hip flexion, abduction, and external rotation.
Obturator nerve (L2-L4) Prolonged excessive hip flexion.
Sciatic nerve (L4-S3) Hip flexion with extension of the knee. Hip abduction and
external rotation with flexed knee.
Lateral femoral cutaneous
nerve (L2-L4)
Excessive flexion, abduction and external rotation of the hip.
Common peroneal nerve Compression between the head of the fibula and the candy
cane stirrups. Prolonged knee flexion with excessive hip
external rotation.
Avoid the use of candy cane stirrups. Avoid excessive knee
flexion and external rotation of the hip. Adequate padding
of the knee area.
Ilioinguinal and
iliohypogastric
nerves (T12-L1)
Insertion of the lateral side port at the site of nerves course
of the lower abdomen with stitch closure of the fascial
defects.
Avoid the nerve course sites. Avoid the use of stitch closure
of the fascial defect. If the fascial defects were closed, do
not tight the stitching.
Abdalmageed et al. Nerve Injuries in Gynecologic Laparoscopy 23
Sequelae of Lateral Cutaneous Nerve of the Thigh InjuryMeralgia paresthetica results from lateral femoral cuta-
neous nerve compression. The classic presentation isburning pain, paresthesia (numbness and tingling), and hy-poesthesia over the anterior and the lateral aspects of thethigh down to the knee [56]. In most affected patients, mer-algia paresthetica is a benign self-limited condition that doesnot require any intervention [57].
Obturator Nerve Injury
The obturator nerve originates from the lumbar plexusand emerges in the abdomen from the medial border of thepsoas muscle.
Applied AnatomyThe obturator nerve begins from the anterior division
of L2-L4 and travels in the substance of the psoas muscleto appear from its medial border. It then runs in front ofthe sacroiliac joint to the lesser pelvis. The obturatornerve travels down to the obturator notch to exit the pelvisthrough the obturator foramen where it splits into anteriorand posterior branches. Both divisions innervate the thighadductor muscles. The anterior branch gives sensoryinnervation to the medial surface of the mid-thigh andthe hip joint, whereas the posterior branch innervatesthe knee joint.
Mechanism of InjuryThis nerve is most commonly injured during endometri-
osis excision, retroperitoneal surgeries, transobturator tapeinsertion, and paravaginal defect repair [58]. It is suggestedthat prolonged hip flexion leads to obturator nerve stretchingat the bony obturator foramen [59]. A cadaver-based studydemonstrated that the most important factor in obturatornerve injury is a hip abduction [55].
Sequelae of Obturator Nerve InjuryUnilateral obturator nerve neuropathy leads to sensory
loss or paresthesia in the upper inner thigh and weak adduc-tion with minor ambulatory problems [59]. Pressure andstretching injury rarely lead to motor affection [60].
Sciatic Nerve Injury
The sciatic nerve is the largest and longest nerve in thehuman body. It is located in the back of the leg and providesmotor and sensor innervation to the lower limbs. Sciaticnerve neuropathy related to the lithotomy position is rela-tively uncommon. Sciatic nerve injuries result in sensorysymptoms in .4% of cases [61] and severe motor sequelaein 1 in 25 000 surgeries [18].
Applied AnatomyThe sciatic nerve originates from the anterior division
roots of the lumbosacral trunk (L4-S3). It runs posteriorlydown the thigh to exit the pelvis through the sciatic foramento enter the gluteal region. It descends on the posterior aspectof the thigh to the apex the popliteal fossa where it forms 2branches: the tibial and common peroneal nerves. Thesciatic nerve supplies the thigh flexor muscles and providesboth motor and sensory supply to the lower extremitiesbelow the knee.
Mechanism of InjuryPatients with a low body mass index are more vulner-
able to sciatic nerve neuropathy, especially if placed inthe lithotomy position for a long duration [62]. Hipflexion, especially if combined with knee extension(high lithotomy position), can cause sciatic nerve stretchinjury [18]. Hip abduction and external rotation canstretch the sciatic nerve, particularly when the knee isflexed [63,64].

24 Journal of Minimally Invasive Gynecology, Vol 24, No 1, January 2017
Sequelae of Sciatic Nerve InjurySciatic nerve injury can cause hypoesthesia or paresthesia
over the posterior aspect of the thigh, calf, and sole of thefoot [65]. Severe damage may cause weakness with hipextension and knee flexion. It may also lead to foot dropassociated with paresthesia over the calf and the dorsum ofthe foot due to weakness in the dorsiflexion foot muscles(anterior and lateral compartment) [66].
Common Peroneal Nerve Injury
The common peroneal nerve is a branch of the sciaticnerve and is the most frequently injured nerve during sur-geries that involve the lithotomy position. Motor disabilitiescaused by common peroneal nerve injuries are estimated tooccur in 1 of every 4500 lithotomy operations [9].
Applied AnatomyThe common peroneal nerve (also named as the common
fibular nerve or external popliteal nerve) starts as a branch ofthe sciatic nerve at the apex of the popliteal fossa. It windsalong the lateral side of the popliteal fossa and around thefibula neck. At this point, the common peroneal nerve is sub-cutaneous and can be entrapped against the head of the fib-ula. The common fibular nerve ends within the peroneallongus muscle by branching into 2 divisions: the superficialand deep fibular nerves. The motor component of the super-ficial and the deep fibular nerves are responsible for footeversion and dorsiflexion by supplying the muscles of thelateral and posterior compartment, whereas the sensorycomponent of the common peroneal nerve gives cutaneousinnervation to the posterolateral aspect of the leg.
Mechanism of InjuryThe common peroneal nerve can be injured during surgeries
that use the lithotomy position because of direct pressure andstretching. The use of hanging candy cane stirrups is a recog-nized risk factor for pressure injury (Fig. 1). Stretch trauma ofthe commonperoneal nerve is related to prolonged knee flexionand can be exacerbated by excessive hip external rotation. Theuse of boot stirrups helps protect against this type of injury [18].Extra padding should be used in this area during surgery.
Sequelae of Common Peroneal Nerve InjuryCommon peroneal nerve injury can be associated with hy-
posthesia or paresthesia affecting the dorsum of the foot andthe lateral surface of the leg. Severe damage can lead to ‘‘footdrop’’ that manifests with the loss of foot dorsiflexion, loss oftoes extension, and loss of lateral rotation of the ankle.
Other Lithotomy Position–Related Nerve Injuries
Both the tibial and saphenous nerves can be compressedagainst a hard surface while the patient is in the lithotomyposition. Adequate padding minimizes the risk of these in-juries [67].
Iliohypogastric and Ilioinguinal Nerve Injury
Injury to the ilioinguinal and iliohypogastric nerves typi-cally occurs as a result of nerve ligation during closure of thelateral port-fascial defects in the lower abdomen [68]. In aretrospective study, the estimated incidence of abdominalwall nerve injury during laparoscopic gynecologic surgerieswas 4.9% [2]. The course of ilioinguinal and iliohypogastricnerves makes them vulnerable to trauma during gynecologiclaparoscopy surgery [2,68].
Applied AnatomyThe ilioinguinal and iliohypogastric nerves are composed
of the T12-L1 nerve roots. Both nerves run along the abdom-inal oblique muscles to supply the area between the ASISand iliac crest. Whiteside et al [1] conducted a cadaver-based study and demonstrated the relationship of the ilioin-guinal and iliohypogastric nerves to lateral trocar placementsites in laparoscopy. Their study also found that the ilioin-guinal nerve should be 3.1 cm medial and 3.7 cm inferiorto the ASIS, whereas the iliohypogastric nerve should be2.1 cm medial and .9 cm inferior to the ASIS (Fig. 3) [1].Rahn et al [69] conducted a similar cadaver-based studyand found that the ilioinguinal nerve should be 2.5 cmmedial and 2.4 cm inferior to the ASIS and the iliohypogas-tric nerve should be 2.5 cm medial and 2 cm inferior to theASIS. Both the ilioinguinal and the iliohypogastric nervesare pure sensory. The iliohypogastric nerve innervates theskin over the gluteal and hypogastric regions, whereas theilioinguinal nerve innervates the skin of the groin, innerthigh, and labia majora.
Mechanisms of InjuryA retrospective study of the risk factors for abdominal wall
nerve injury during gynecologic laparoscopy found that neu-ropathy is mainly caused by entrapment of the ilioinguinaland iliohypogastric nerves during fascial closure of the lateralport site. In the same study, unrepaired fascial wounds werenot associated with postoperative neuropathies [2].
Sequelae of Iliohypogastric and Ilioinguinal Nerve InjuryThe most common presentation of ilioinguinal/iliohypo-
gastric neuropathies includes sharp, burning, lancinatingpain radiating from the incision site to the suprapubic areaor the vulva with paresthesia over the nerve distributionarea [4,70]. This neurologic pain can occur immediately orweeks to months after surgery [71]. The neurologic painmay persist for months or years due to persistent neuralconstriction caused by scarring [69] and can be relievedwith a local anesthetic [70].
Prevention of Nerve Injury During GynecologicLaparoscopy
Safe and proper positioning of the patient on the operatingroom table is a joint responsibility of the surgeon and

Fig. 5
Proper patient positioning with appropriate relative angles and padding
of upper and lower limb sensitive areas: side view.
Abdalmageed et al. Nerve Injuries in Gynecologic Laparoscopy 25
anesthesiologist [26]. Proper positioning with adequatepadding of all pressure points can minimize the possibilityof nerve injury [72,73]. Ghomi et al [74] performed a descrip-tive study to explore the importance of patient positioningwhen using the Trendelenburg position in robotic-assisted gy-necologic surgery for benign lesions and found that these sur-geries could be performed efficiently without the use of thesteep position.
Fig. 6
Proper patient positioning with appropriate relative angles and padding
of upper and lower limb sensitive areas: perineal view.
Prevention of Brachial Plexus Injuries
Table 4 summarizes the common strategies to prevent up-per extremity nerve injuries during gynecologic laparoscopysurgeries. The brachial plexus is commonly injured duringgynecologic laparoscopy. To avoid brachial plexus injuries,the patient’s arms should be tucked carefully at his or hersides. If it is necessary to extend the arms, the trunk armangle should preferably be limited to 90 degrees to preventhyperabduction nerve injury [18]. The best position for thehead is the central position; posterior displacement of theshoulder should be avoided to decrease stretching and pres-sure on the brachial plexus. Shoulder braces and wrist re-straints should also be avoided [16]. Gel pads and eggcrate or foam mattress pads can replace shoulder braces toprevent patient sliding from the Trendelenburg position. Ifit is necessary to use shoulder braces, they should beadjusted to the acromioclavicular joint directly [39,60].Even with correct placement of shoulder braces directlyover the acromioclavicular joint, the risk of brachialplexus injury is still present.
A number of measures can be taken to minimize postoper-ative ulnar nerve neuropathy: using elbow pads, avoiding armabduction, pronation of the forearm, and avoiding prolonged orextreme elbowflexion [50,75]. Both armsmust be tucked at thepatient’s side pronated with adequate padding (foam padding)over the posteromedial elbow to protect the ulnar nerve frompressure against a hard surface [75]. If the arms are placedon boards, the forearm should be placed in a supine positionwith padding to help protect the ulnar nerve from compression[39]. Martin et al suggested placing the arms in a comfortablesling position with elbow flexion angle. 90 degrees to mini-mize injuries to the brachial plexus [76]. The angle of the bedhead tilt used for the Trendelenburg position should be limitedto 30 degrees, especially if the arms are extended [77].Figures 5, 6, and 7 demonstrate the proper patientpositioning for gynecologic laparoscopy surgeries.
Prevention of Lower Extremities Nerve Injuries
The recommended strategies to minimize lower extrem-ities nerve injuries during gynecologic laparoscopy are sum-marized in Table 6.
Proper leg Placement in the Lithotomy PositionCorrect placement of the patient in a lithotomy position is
critical for the prevention of position-related nerve injuries.
The surgeon should limit the hip flexion, abduction, andexternal rotation to minimize nerve injuries [39,64].
A proper lithotomy position depends on the type of thesurgery performed. The ideal position for laparoscopy isthe low lithotomy position, with the thigh-trunk angle about170 degrees. A trunk-thigh angle of less than 170 degreesmay cause obturator nerve strain, and an angle more than180 degrees may cause lumbar spine stress [18]. Vaginal sur-geries may necessitate a high lithotomy position to improveexposure. The trunk-thigh angle should be greater than 60degrees to minimize the strain on the sciatic and femoralnerves. The angle of the knee should be kept between 90and 120 degrees to avoid pressure on the sciatic nerve andto allow a better venous return.

Fig. 7
Proper patient positioning with appropriate relative angles and padding
of upper and lower limb sensitive areas: top view.
26 Journal of Minimally Invasive Gynecology, Vol 24, No 1, January 2017
The angle of hip abduction should be 90 degrees or less tominimize strain on the obturator nerve. The extent of externalhip rotation should be minimized so as not to increase thepressure on the femoral, obturator, or sciatic nerves. It isbelieved that candy cane stirrups enhance the risk of theexternal hip rotation. The legs must be padded around theknee to protect the common peroneal nerve from trauma [39].
Leg SupportTraditional candy cane stirrups give little support to the
legs during laparoscopy. They are considered a risk factorfor uncontrolled hip abduction and external rotation. Whenthe leg comes in contact with the support pole, it can placepressure on the common peroneal nerve and cause injury.Adequate padding should be placed between the lateralfibular head and the stirrups or the supporting pole to preventcommon peroneal nerve compression [47]. Figures 5, 6, and 7demonstrate the proper patient positioning for gynecologiclaparoscopy surgeries.
Prevention of Ilioinguinal and Iliohypogastric NerveInjuries
The best way to avoid ilioinguinal and iliohypogastricnerve injuries is to place side ports above the ASIS. Otherstrategies to prevent ilioinguinal and iliohypogastric nerveinjuries include using a side-port trocar that is no largerthan 5 mm, which avoids the need to close the fascial defectin the lower abdomen, and, if necessary, avoiding a tightclosure by accurately approximating the fascial edges [2].
Conclusion
Neurologic injuries after gynecologic surgery are relativelyuncommon. However, when they occur they are very distress-ing to the patient and delay convalescence time and decreasequality of life. Most are self-limited or respond to conservativetreatment such as physical therapy. Several critical factors candecrease the frequency of occurrence. First, knowledge of the
anatomy of the peripheral nerves of the upper and lower limbsand the anterior abdominal wall is important. Second, theentire surgical team should pay close attention to the patientpositioning step. The entire team is responsible, and all shouldparticipate. Finally, a discussion should be had with the patientof the risk factors that predispose her to this complication.
References
1. Whiteside JL, Barber MD, Walters MD, Falcone T. Anatomy of ilioin-
guinal and iliohypogastric nerves in relation to trocar placement and
low transverse incisions. Am J Obstet Gynecol. 2003;189:1574–1578.
discussion 1578.
2. Shin JH, Howard FM. Abdominal wall nerve injury during laparoscopic
gynecologic surgery: incidence, risk factors, and treatment outcomes. J
Minim Invasive Gynecol. 2012;19:448–453.
3. Bohrer JC, Walters MD, Park A, Polston D, Barber MD. Pelvic nerve
injury following gynecologic surgery: a prospective cohort study. Am
J Obstet Gynecol. 2009;201:531.
4. Cardosi RJ, Cox CS, Hoffman MS. Postoperative neuropathies after
major pelvic surgery. Obstet Gynecol. 2002;100:240–244.
5. Sawyer RJ, RichmondMN, Hickey JD, Jarrratt JA. Peripheral nerve in-
juries associated with anaesthesia. Anaesthesia. 2000;55:980–991.
6. Dawson DM, Krarup C. Perioperative nerve lesions. Arch Neurol. 1989;
46:1355–1360.
7. Romanowski L, Reich H,McGlynn F, AdelsonMD, Taylor PJ. Brachial
plexus neuropathies after advanced laparoscopic surgery. Fertil Steril.
1993;60:729–732.
8. Warner MA, Warner DO, Harper CM, Schroeder DR, Maxson PM.
Lower extremity neuropathies associated with lithotomy positions.
Anesthesiology. 2000;93:938–942.
9. Warner MA, Martin JT, Schroeder DR, Offord KP, Chute CG. Lower-
extremity motor neuropathy associated with surgery performed on pa-
tients in a lithotomy position. Anesthesiology. 1994;81:6–12.
10. UlmMA, FlemingND, Rallapali V, et al. Position-related injury is uncom-
mon in robotic gynecologic surgery. Gynecol Oncol. 2014;135:534–538.
11. Shveiky D, Aseff JN, Iglesia CB. Brachial plexus injury after laparo-
scopic and robotic surgery. J Minim Invasive Gynecol. 2010;17:414–420.
12. Saidha S, Spillane J, Mullins G, McNamara B. Spectrum of peripheral
neuropathies associated with surgical interventions: a neurophysiolog-
ical assessment. J Brachial Plex Peripher Nerve Inj. 2010;5:9.
13. Sukhu T, Krupski TL. Patient positioning and prevention of injuries in
patients undergoing laparoscopic and robot-assisted urologic proced-
ures. Curr Urol Rep. 2014;15:398.
14. Salati M, Cardillo G, Carbone L, et al. Iatrogenic phrenic nerve injury
during thymectomy: the extent of the problem. J Thorac Cardiovasc
Surg. 2010;139:e77–e78.
15. Uribe JS, Kolla J, Omar H, et al. Brachial plexus injury following spinal
surgery. J Neurosurg Spine. 2010;13:552–558.
16. Winfree CJ, Kline DG. Intraoperative positioning nerve injuries. Surg
Neurol. 2005;63:5–18. discussion 18.
17. Ghomi A. Robotics in practice: new angles on safer positioning.
Contemp Ob Gyn. 2012;57:26–37.
18. Barnett JC, Hurd WW, Rogers RM Jr, Williams NL, Shapiro SA.
Laparoscopic positioning and nerve injuries. JMinim Invasive Gynecol.
2007;14:664–672. quiz 673.
19. Hughes RA. Peripheral neuropathy. BMJ. 2002;324:466–469.
20. Muller-Vahl H, Munte TF, Vahl CF. Postoperative ulnar nerve palsydis
it an unpreventable complication? Anesth Analg. 1993;77:404–405.
21. Pou Serradell A, De Paiva VJ, Alameda F, Lloreta J, Blasco R,
Piqueras A. [Familial recurrent paralysis of the brachial plexus. Tomacu-
lous neuropathy]. Rev Neurol (Paris). 1992;148:123–128.
22. VerhagenWI, Gabre€els-FestenAA, vanWensen PJ, et al. Hereditary neu-
ropathy with liability to pressure palsies: a clinical, electroneurophysio-
logical and morphological study. J Neurol Sci. 1993;116:176–184.
Abdalmageed et al. Nerve Injuries in Gynecologic Laparoscopy 27
23. Chance PF. Overview of hereditary neuropathy with liability to pressure
palsies. Ann N Y Acad Sci. 1999;883:14–21.
24. Massey EW, Pleet AB. Compression injury of the sciatic nerve during a
prolonged surgical procedure in a diabetic patient. J Am Geriatr Soc.
1980;28:188–189.
25. IrvinW, AndersenW, Taylor P, Rice L.Minimizing the risk of neurologic
injury in gynecologic surgery. Obstet Gynecol. 2004;103:374–382.
26. Bouyer-Ferullo S. Preventing perioperative peripheral nerve injuries.
AORN J. 2013;97:110–124.
27. Jones HD. Ulnar nerve damage following general anaesthetic. A case
possibly related to diabetes mellitus. Anaesthesia. 1967;22:471–475.
28. Parks BJ. Postoperative peripheral neuropathies. Surgery. 1973;74:
348–357.
29. Smith S. Complications of laparoscopic and hysteroscopic surgery. In:
Azziz R,AlvarezMurphyA, editors.PracticalManual of Operative Lap-
aroscopy and Hysteroscopy. New York, NY: Springer; 1992. p. 199–215.
30. Sunderland S. A classification of peripheral nerve injuries producing
loss of function. Brain. 1951;74:491–516.
31. Seddon HJ. A classification of nerve injuries. Br Med J. 1942;2:237–239.
32. Lee SK, Wolfe SW. Peripheral nerve injury and repair. J Am Acad Or-
thop Surg. 2000;8:243–252.
33. Adedeji R, Oragui E, Khan W, Maruthainar N. The importance of cor-
rect patient positioning in theatres and implications of mal-positioning.
J Perioper Pract. 2010;20:143–147.
34. Haftek J. Stretch injury of peripheral nerve. Acute effects of stretching
on rabbit nerve. J Bone Joint Surg Br. 1970;52:354–365.
35. Seddon H. Three types of nerve injury. Brain. 1943;66:237–288.
36. Ochoa J, Fowler TJ, Gilliatt RW. Anatomical changes in peripheral nerves
compressed by a pneumatic tourniquet. J Anat. 1972;113(Pt 3):433–455.
37. Rydevik B, Nordborg C. Changes in nerve function and nerve fibre
structure induced by acute, graded compression. J Neurol Neurosurg
Psychiatry. 1980;43:1070–1082.
38. Mackinnon SE, Dellon AL, Hudson AR, Hunter DA. Chronic human
nerve compressionda histological assessment. Neuropathol Appl Neu-
robiol. 1986;12:547–565.
39. Bradshaw AD, Advincula AP. Optimizing patient positioning and un-
derstanding radiofrequency energy in gynecologic surgery. Clin Obstet
Gynecol. 2010;53:511–520.
40. Campbell WW. Evaluation and management of peripheral nerve injury.
Clin Neurophysiol. 2008;119:1951–1965.
41. Mackinnon SE. Pathophysiology of nerve compression. Hand Clin.
2002;18:231–241.
42. Cajal SR. Degeneration & Regeneration of the Nervous System Vol. 1.
New York, NY: Hafner; 1959.
43. Bridge PM, Ball DJ, Mackinnon SE, et al. Nerve crush injuriesda
model for axonotmesis. Exp Neurol. 1994;127:284–290.
44. Jackson L, Keats AS. Mechanism of brachial plexus palsy following
anesthesia. Anesthesiology. 1965;26:190–194.
45. Kim DH, Murovic JA, Tiel RL, Kline DG. Mechanisms of injury in
operative brachial plexus lesions. Neurosurg Focus. 2004;16:E2.
46. Plastaras CT, Chhatre A, Kotcharian AS. Perioperative upper extremity
peripheral nerve traction injuries.Orthop Clin North Am. 2014;45:47–53.
47. Kuponiyi O, Alleemudder DI, Latunde-Dada A, Eedarapalli P. Nerve
injuries associated with gynaecological surgery. Obstet Gynaecol.
2014;16:29–36.
48. Chin P, Poole G. Bilateral brachial plexus injury during laparoscopic
sigmoid colectomy. Austr N Z J Surg. 2003;73:86–88.
49. Fleisch MC, Bremerich D, Schulte-Mattler W, et al. The preven-
tion of positioning injuries during gynecologic operations.
Guideline of DGGG (S1-Level, AWMF registry no. 015/077,
2015). Geburtsh Frauenh. 2015;75:792–807.
50. Stahl S, Norman D, Zinman C. [Postoperative ulnar nerve palsy of the
elbow]. Harefuah. 1997;133:533–535. 590.
51. Kvist-Poulsen H, Borel J. Iatrogenic femoral neuropathy subsequent to
abdominal hysterectomy: incidence and prevention. Obstet Gynecol.
1982;60:516–520.
52. Nawrot P, Romanowski L, Nowakowski A, Kubaszewski L. [Modern
opinions on treatment of the compressive neuropathies of the radial
nerve]. Chir Narzadow Ruchu Ortop Pol. 2007;72:323–326.
53. Warner MA, Warner ME, Martin JT. Ulnar neuropathy. Incidence,
outcome, and risk factors in sedated or anesthetized patients. Anesthe-
siology. 1994;81:1332–1340.
54. Williams PH, Trzil KP. Management of meralgia paresthetica. J Neuro-
surg. 1991;74:76–80.
55. Litwiller JP, Wells RE Jr, Halliwill JR, Carmichael SW, Warner. Effect
of lithotomy positions on strain of the obturator and lateral femoral
cutaneous nerves. Clin Anat. 2004;17:45–49.
56. Nahabedian MY, Dellon AL. Meralgia paresthetica: etiology, diagnosis,
and outcome of surgical decompression.AnnPlast Surg. 1995;35:590–594.
57. Harney D, Patijn J. Meralgia paresthetica: diagnosis and management
strategies. Pain Med. 2007;8:669–677.
58. Corona R, De Cicco C, Schonman R, Verguts J, Ussia A, Koninckx PR.
Tension-free vaginal tapes and pelvic nerve neuropathy. J Minim Inva-
sive Gynecol. 2008;15:262–267.
59. Vasilev SA. Obturator nerve injury: a review of management options.
Gynecol Oncol. 1994;53:152–155.
60. Bradshaw AD, Advincula AP. Postoperative neuropathy in gynecologic
surgery. Obstet Gynecol Clin North Am. 2010;37:451–459.
61. Romfh JH, Currier RD. Sciatic neuropathy induced by the lithotomy
position. Arch Neurol. 1983;40:127.
62. Batres F, Barclay DL. Sciatic nerve injury during gynecologic procedures
using the lithotomy position.Obstet Gynecol. 1983;62(3 Suppl):92s–94s.
63. Korompilias AV, Payatakes AH, Beris AE, Vekris MD, Afendras GD,
Soucacos PN. Sciatic and peroneal nerve injuries. Microsurgery.
2006;26:288–294.
64. Chan JK, Manetta A. Prevention of femoral nerve injuries in gyneco-
logic surgery. Am J Obstet Gynecol. 2002;186:1–7.
65. Sunderland S, Walshe F. Nerves and nerve injuries. Baltimore MD:
Williams and Wilkins; 1968.
66. Burkhart FL, Daly JW. Sciatic and peroneal nerve injury: a complica-
tion of vaginal operations. Obstet Gynecol. 1966;28:99–102.
67. Welch MB, Brummett CM, Welch TD, et al. Perioperative peripheral
nerve injuries: a retrospective study of 380,680 cases during a 10-
year period at a single institution. Anesthesiology. 2009;111:490–497.
68. El-Minawi AM,Howard FM. Iliohypogastric nerve entrapment following
gynecologic operative laparoscopy.Obstet Gynecol. 1998;91(5 Pt 2):871.
69. Rahn DD, Phelan JN, Roshanravan SM, White AB, Corton MM. Ante-
rior abdominal wall nerve and vessel anatomy: clinical implications for
gynecologic surgery. Am J Obstet Gynecol. 2010;202:234.
70. Vanderlinden RG, Midha R, Vanderlinden L. Ilioinguinal/iliohypogas-
tric neuropathy. In: Bendavid R, Abrahamson J, Arregui M, Bernard
Flament J, Phillips EH, editors. Abdominal Wall Hernias. New York,
NY: Springer; 2001. p. 737–739.
71. Stulz P, Pfeiffer KM. Peripheral nerve injuries resulting from common
surgical procedures in the lower portion of the abdomen. Arch Surg.
1982;117:324–327.
72. Chapron C, Pierre F, Querleu D, Dubuisson JB. [Complications of lap-
aroscopy in gynecology]. Gynecol Obstet Fertil. 2001;29:605–612.
73. Natalin RA, Landman J. Positional and neuromuscular complications
of laparoscopic and robotic urologic surgery. In: Ghavamian R, editor.
Complications of Laparoscopic and Robotic Urologic Surgery. New
York, NY: Springer; 2010. p. 35–41.
74. Ghomi A, Kramer C, Askari R, Chavan NR, Einarsson JI. Trendelen-
burg position in gynecologic robotic-assisted surgery. J Minim Invasive
Gynecol. 2012;19:485–489.
75. Stoelting RK. Postoperative ulnar nerve palsydis it a preventable
complication? Anesth Analg. 1993;76:7–9.
76. Martin GL, Nunez RN, Martin AD, Andrews PE, Castle EP. A novel
and ergonomic patient position for laparoscopic kidney surgery. Can
J Urol. 2009;16:4580–4583.
77. Gagnon J, Poulin EC. Beware of the Trendelenburg position during pro-
longed laparoscopic procedures. Can J Surg. 1993;36:505–506.