nephrologists' experience with and attitudes towards decisions to forego dialysis1
TRANSCRIPT

Journal of the American Society of Nephrology 1235
Nephrologists’ Experience with and Attitudes TowardsDecisions To Forego Dialysis1
Peter A. Singer,2 and the End-Stage Renal Disease Network of New England3
PA. Singer, Department of Medicine and Centre forBioethics, University of Toronto, Toronto, Ontario, Can-ada
End-Stage Renal Disease Network of New England,New Haven, CT
(J. Am. Soc. Nephrol. 1992; 2:1235-1240)
draw dialysis in competent patients or incompetentpatients with clear prior wishes; they disagree about
the management of incompetent patients with un-clear prior wishes. Increased use of advance direc-lives would help avoid this latter situation.
Key Words: Medical ethics. life support. living wills. dialysis
ABSTRACTEthicists and lawyers agree that competent adult
patients or their surrogate decision-makers have theright to forego life-sustaining treatment, but the views
of practicing physicians have not been well-studied.To examine nephrologists’ experience with and atti-tudes towards decisions to forego dialysis, a ques-tionnaire was sent to all I 6 1 nephrologists performingchronic dialysis in six New England states; I 18 (73%)responded. The proportion of nephrologists who re-ported withholding (not starting) dialysis from thecited numbers of patients during the previous year
was 11%, 0; 58%, 1 to 5; 20%, 6 to 10; 8%, 11 to 15;
and 3%, �16. For withdrawing (stopping), the pro-portions were 19%, 0; 73%, 1 to 5; 9%, 6 to 10; and0%, � I I . The nephrologists withheld dialysis moretimes than they withdrew it (x2 26; P = 0.004). If
requested to do so by a competent patient, 88% ofnephrologists would stop dialysis. If requested by the
family of an incompetent patient, 90% would stop ifthe patient had clear prior wishes, but only 63%would stop if prior wishes were unclear. With com-petent patients, the issue of withdrawal of dialysiswas usually raised by the patient (56%). With incom-petent patients, the issue was raised by the family(42%) or nephrologist (30%). It was concluded thatdecisions to withhold dialysis are more frequent thandecisions to withdraw it. Moreover, nephrologists
agree about the management of requests to with-
I Received February 25, 1991. Accepted August 28, 1991.2 Correspondence to Dr. P. singer, dentre for Bioethics, University of Toronto.
Toni Neuroscience Building, 6 Queen’s Pork cres. West, Toronto, Ontario, can-ado M5S-1A8.
3 The Network Working Committee included Michael Kovaichik (chairman),
Lewis cohen, Michael Germain, connie Hill, Jean Kammerer, and Jenny Kitsen.
1046-6673/0207-1235$03.00/0Journal of the American society of Nephrologycopy�ght is 1992 by the American society of Nephrology
N me percent of patients receiving dialysis diebecause dialysis Is withdrawn (stopped) (1 ,2).
Withdrawal of dialysis accounts for 22 to 26% ofdeaths among dialysis patients (1 .3). It is the secondmost common cause of death after cardiovascularcauses in the elderly and the third most commoncause overall for dialysis patients (4). Patient char-actenistics associated with withdrawal of dialysis in-dude older age. diabetes mellitus, comorbid degen-erative disease, white race, and residence in a nuns-ing home (1 ,2). There are no published data ondecisions to withhold (not start) dialysis.
Decisions to forego (I.e. , withhold or withdraw) di-alysis are ethical and legal under certain circum-stances (5- 1 1 ). The ethical basis of these decisionsis the principle of individual autonomy. The legalbasis is the common law right of self-determlnationand the Constitutional right of liberty. After a decadeof scholarly debate, policy guidelines. state legisla-tion, and legal cases (culminating in the U.S. Su-preme Court decision in the case of Nancy Cruzan),the circumstances under which patients may foregolife-sustaining treatments such as dialysis have be-come increasingly well-defined. Competent adult pa-tients may choose to forego treatment. Incompetentpatients may also forego treatment if there is clear
and convincing evidence that this is the decision theywould make if competent. Clear and convincing evi-dence would Include a written instruction advancedirective (living will) or specific verbal statementsthat apply to the dialysis decision. The use of a proxyadvance directive (durable power of attorney forhealth care), wherein the patient while competentappoints a proxy to make decisions on his or herbehalf after he or she becomes Incompetent. wouldprobably also satisfy the clear and convincing stand-and.
Unfortunately, only 15% of Americans have com-pleted an advance directive (1 2). All too frequently,there is no clear evidence available about whether an
incompetent patient would want to receive on foregodialysis. What should the physician do in this situa-

Foregoing Dialysis
1236 Volume 2 - Number 7 - 1992
tion? In states requiring clear and convincing evi-
dence of the prior wishes of a patient (Missouri andNew York), dialysis must be continued. In other
states, the physician may use substituted judgmentor best interests tests. With substituted judgment,the patient’s surrogate (e.g. , a spouse on family mem-ben) applies the preferences and values of the patientto the dialysis decision “to reach the decision theincapacitated person would make if he or she were
able to choose” (5). The problem with this test Is thatempirical studies show low rates of concordance onhealth care decisions between patients and theirlikely surrogates ( 13). When no information is knownabout the preferences and values of the patient. thesurrogate uses the best interests test, choosing as areasonable person In the patient’s situation wouldchoose, according to a set of “objective, societallyshared criteria” (5). The problem with the best inter-ests test is that “objective. societally shared criteria”are difficult to specify in a morally pluralistic society.
Because of the clinical Importance of decisions toforego dialysis and the growing public interest indecisions to forego life-sustaining treatment, we un-dertook a survey of nephrologists regarding their ex-penience with and attitudes towards decisions to
forego dialysis. In particular. we examined the follow-ing questions. How many times do nephrologlsts
withhold dialysis relative to the number of times theywithdraw it? How do nephnologists respond to re-
quests to withdraw dialysis from competent patients,incompetent patients with clear prior wishes, andincompetent patients with unclear prior wishes?What is the decision-making process when dialysisis withdrawn?
METHODS
The research design is a cross-sectional question-name survey. The questionnaire requests infonma-tion about respondent demographics (age. sex, edu-cation, religious commitment). practice pattern (sizeof practice. type of dialysis facility), and experience
with and attitudes towards foregoing dialysis. Thequestions regarding how nephrobogists respond torequests to withdraw dialysis were presented as fob-lows.
(1) Assume that a patient In your practice has askedto stop dialysis. According to a psychiatric consult-ant, the patient is competent. As the patient’s ne-phnologist, you have discussed the request to stopdialysis at length with your patient, but the patient
continues to request that dialysis be stopped. Whatwould you do in this situation?
(2) Assume that the family of an irreversibly incom-petent patient requests that dialysis be stopped. Thefamily provides clean evidence that the patient hadsaid he/she would not want to continue dialysis inhis/her current situation. What would you do?
(3) Assume that the family of an irreversibly incom-
petent patient requests that dialysis be stopped. The
patient had never discussed whether he/she wouldwant to continue dialysis in his/her current situa-tion. What would you do?
(4) Assume that the dialysis team caring for an
irreversibly incompetent patient feels that dialysisshould be stopped. The patient had never discussedwhether he/she would want to continue dialysis inhis/her current situation. The family demands thatthe dialysis be continued. What would you do?
Because we felt nephrobogists were familiar withthe terms “competent” and “incompetent,” we usedthese in the questionnaire. Strictly speaking, com-petency is a legal determination; its clinical counter-part is known as “decision-making capacity. “ More-over, our questions asked nephrobogists about their“dialysis patients” and, as such, were not specific topatients with end-stage renal disease (ESRD). Thefull questionnaire is available from the authors uponrequest.
The questionnaire was mailed on January 5, 1990,
to all 161 nephnobogists on the mailing list of ESRDNetwork of New England. ESRD Network of NewEngland is a private, not-for-profit organization. un-der contract with the Health Care Financing Admin-istratlon, responsible for quality assurance of di-alysis and renal transplant programs. It is responsi-ble for 68 Medicare-certified dialysis facilities(serving 4,670 patients) and 14 renal transplant pro-grams in Connecticut, Maine, Massachusetts, NewHampshire, Rhode Island, and Vermont. The ESRDmailing list is believed to contain all nephrobogists inNew England who are significantly associated with achronic dialysis facility. Nonrespondents received awritten reminder at 4 wk after the mailing date ofthe questionnaires.
The responses were analyzed by univaniate andbivaniate analyses. In univanlate analyses, the dataare presented as the proportion of respondents givingeach response for a given question. In bivaniate anal-yses, we examined whether demographic and prac-tice factors are associated with the frequency of fore-
going dialysis by using x2 and analysis of variancetests. The Cochran-Mantel-Haenszeb x2 test was usedto stratify bivaniate analyses for a second independ-ent variable (size of practice). Statistical tests wereperformed by using the SAS computer program.
This study was approved by the Human Investiga-tion Committee of Yale University School of Medicine.
RESULTS
One hundred and eighteen nephrobogists returnedquestionnaires, for a response rate of 73%. Becausenot all respondents answered each question. the re-sults below do not always add up to 1 18.

Singer et al
Journal of the American Society of Nephrology 1237
Respondent Characteristics
The study group included 108 men (92%) and 9women (8%). The median age was 42 yr (range, 30 to65 yr). The median year of graduation from medicalschool was 1973 (range 1949 to 1984). and the me-dian year of completion of nephrobogy training was1 979 (range, 1 954 to 1 989). Ninety-five respondents(8 1 %) were board-certified in nephrobogy. Five re-
spondents (4%) considered themselves “very nell-gious,” 3 1 (26%) “moderately religious.” 42 (36%)“somewhat religious,” and 40 (34%) “not religious.”Ten respondents (9%) attended religious servicesonce or more a week, 22 ( 19%) attended 1 to 3 timesa month, 58 (49%) attended less than once a month,and 28 (24%) never attended religious services. Sixty-nine respondents (59%) worked in a hospital-baseddialysis facility, 14 (12%) In a fnee-standdngfacility.and 35 (30%) in both. Thirty-five respondents (30%)worked primarily In a for-profit facility. and 80(70%)worked In a nonprofit facility. Thirteen respondents(1 1 %) had less than 10 dialysis patients in theirpractice, 7 (6%) had 1 0 to 20 patients, 35 (30%) had21 to 50 patients, 39 (33%) had 51 to 100 patients,and 24 (20%) had more than 100 dialysis patients intheir practice.
Experience with Withholding and WithdrawingDialysis
The number of times the nephrologists withheld
and withdrew dialysis during the preceding 1 and 5yr is shown in Table 1 . For both 1 and 5 yr. thenumber of times the nephrobogists withheld dialysiswas greater than the number of times they withdrewdialysis (x2 25.9; df = 10; P 0.004 during thepreceding year; x2 63.6; df = 25; P < 0.001 duringthe preceding 5 yr). Moreover, 58 respondents (52%)said they withhold dialysis more often than theywithdraw it, 1 9 (1 7%) said they withhold dialysis less
TABLE I . Number of times dialysis was withheld orwithdrawn
Number ofTimes0
Precedi ng Year Preced ing 5 Yr
Withhold Withdraw Withhold WithdrawN(%) N(%) N(%) N(%)
0 12(11) 22(19) 2(2) 6(5)1-5 66 (58) 86 (73) 36 (34) 41 (36)6-10 23(20) 10(9) 28(26) 42(37)
11-15 9(8) 0(0) 13(12) 15(13)16-20 2(2) 0(0) 8(8) 5(4)>20 1(1) 0(0) 20(19) 5(4)
Totals 113 118 107 114
0 During the entire preceding 1- or 5-yr time periods (i.e. . not numberof times per year).
often, and 34 (3 1 %) said they withhold dialysis just
as often a� they wkhd�w It.Respondents with larger dialysis practices had a
tendency to withdraw dialysis more (x2 34; df 8;
P < 0.001 during the preceding year; x2 = 49. 1 ; df
20; P < 0.00 1 during the preceding 5 years). but thisfinding Is not surprising because these nephrologlstscared for more patients at risk of withdrawal from
dialysis. Practice size was not associated with the
number of times dialysis was withheld (x2 = 22; df =
20; P = 0.3 during the preceding year; x2 29; df20; P = 0.09 during the preceding 5 years). Whenstratified for practice size, none of the following phy-sician factors were associated with the frequency ofwithholding or withdrawing dialysis: age; year ofgraduation from medical school; year of completionof nephrobogy training; board certification; religiosityor attendance at religious services; whether the ne-phrologist’s facility was hospital based, freestanding,or both; and for-profit status of the dialysis facility.
Thirty-one respondents (28%) said the frequencyof withholding dialysis had Increased during the past5 yr. 9 (8%) said the frequency had decreased, and69 (63%) saId it had remained the same. Twentyrespondents (1 8%) said the frequency of withdrawingdialysis had increased during the past 5 yr. 2 (2%)said the frequency had decreased, and 92 (81 %) saidIt had remained the same. Seventeen respondents(1 5%) said patients and families were requesting tostop dialysis more often during the past 5 yr, 2 (2%)said they were requesting to stop dialysis less often,
and 92 (83%) said there was no change in the fre-quency of this request.
Response to Clinical Scenarios Involving With-drawal of Dialysis
Table 2 shows how nephrobogists said they wouldrespond to clinical situations Involving the with-
drawal of dialysis (see Methods). For the competentpatient. 101 respondents (88%) would stop dialysis.For the incompetent patient with clear prior wishes
whose family requests that dialysis be stopped, 104respondents (90%) would stop dialysis. For the in-
competent patient with unclear prior wishes whosefamily requests that dialysis be stopped. 72 respond-ents (63%) would stop dialysis. For the incompetentpatient with unclear prior wishes where the teamwanted to stop but the family wanted to continue,only 1 respondent (1 %) said he would stop dialysis.
Decision-Making Process
Who has the right to decide whether to stop dl-alysis? In the case of a competent patient, 1 08 ne-phrologlsts (94%) said that the patient had the rightto decide whether dialysis should be stopped, 3 (3%)said the patient and family. 2 (2%) said the patient
Foregoing Dialysis
1238 Volume 2 . Number 7 ‘ 1992
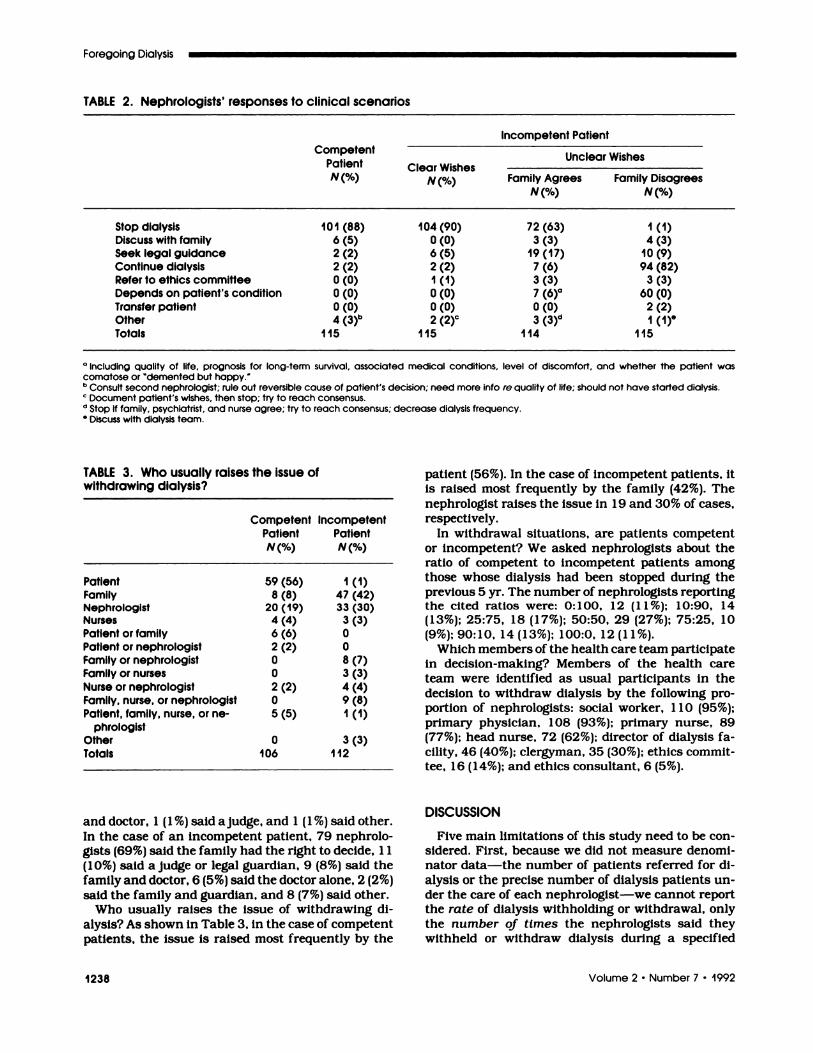
TABLE 2. Nephrologists’ responses to clinical scenarios
Competent.
PatientN(%)
Incompetent Patient
Clear WishesN(%)
Unclear.
Wishes
Family AgreesN(%)
Family DisagreesN(%)
Stop dialysis 101 (88) 104 (90) 72 (63) 1 (1)Discuss with family 6 (5) 0 (0) 3 (3) 4 (3)Seek legal guidance 2 (2) 6 (5) 19 (17) 10 (9)Continue dialysis 2 (2) 2 (2) 7 (6) 94 (82)Refer to ethics committee 0 (0) 1 (1) 3 (3) 3 (3)Depends on patient’s condition 0 (0) 0 (0) 7 (6)#{176} 60 (0)Transfer patient 0 (0) 0 (0) 0 (0) 2 (2)Other 4 (3)b 2 (2)C 3 (3)d I (1)#{176}Totals 115 115 114 115
“ Including qualify of life. prognosis for long-term survival. associated medical conditions. level of discomfort. and whether the patient wascomatose or ‘demented but happy.b Consult second nephrologist: rule out reversible cause of patient’s decision: need more info re quality of life: should not have started dialysis.� Document patient’s wishes, then stop; try to reach consensus.d Stop if family, psychiatrist. and nurse agree; try to reach consensus; decrease dialysis frequency.$ Discuss with dialysis team.
TABLE 3. Who usually raises the issue ofwithdrawing dialysis?
CompetentPatientN(%)
IncompetentPatientN(%)
Patient 59 (56) 1 (1)Family 8 (8) 47 (42)Nephrologist 20 (19) 33 (30)Nurses 4 (4) 3 (3)Patient or family 6 (6) 0Patient or nephrologist 2 (2) 0Family or nephrologist 0 8 (7)Family or nurses 0 3 (3)Nurse or nephrologist 2 (2) 4 (4)Family, nurse, or nephrologist 0 9 (8)Patient, family, nurse, or ne- 5 (5) 1 (1)
phrologistOther 0 3 (3)Totals 106 112
and doctor, 1 (1 %) said ajudge, and 1 (1 %) said other.In the case of an incompetent patient. 79 nephrobo-gists (69%) said the family had the right to decide, 1 1(1 0%) said a judge or legal guardian, 9 (8%) said thefamily and doctor, 6 (5%) said the doctor alone, 2(2%)said the family and guardian, and 8 (7%) said other.
Who usually raises the issue of withdrawing di-abysis? As shown in Table 3, in the case of competentpatients. the issue is raised most frequently by the
patient (56%). In the case of incompetent patients. itis raised most frequently by the family (42%). Thenephrologist raises the issue in 1 9 and 30% of cases,respectively.
In withdrawal situations, are patients competentor incompetent? We asked nephrobogists about theratio of competent to incompetent patients amongthose whose dialysis had been stopped during theprevious 5 yr. The number of nephrologists reportingthe cited ratios were: 0: 1 00. 1 2 (1 1 %); ! 0:90, 14(13%); 25:75, 18 (17%); 50:50, 29 (27%); 75:25, 10(9%); 90:10, 14 (13%); 100:0, 12 (11%).
Which members of the health care team participatein decision-making? Members of the health cane
team were identified as usual participants in thedecision to withdraw dialysis by the following pro-portion of nephnobogists: social worker, 1 1 0 (95%);primary physician, 1 08 (93%); primary nurse, 89(77%); head nurse, 72 (62%); director of dialysis fa-cility, 46 (40%); clergyman, 35 (30%); ethics commit-tee, 16 (14%); and ethics consultant, 6 (5%).
DISCUSSION
Five main limitations of this study need to be con-sidered. First, because we did not measure denomi-nator data-the number of patients referred for dl-alysis or the precise number of dialysis patients un-den the care of each nephrobogist-we cannot reportthe rate of dialysis withholding or withdrawal, onlythe number of times the nephrologlsts said theywithheld or withdraw dialysis during a specified

Singer et al
Journal of the American Society of Nephrology 1239
period (the preceding 1 or 5 yr). Even with denomi-
naton data, we could report only prevalence but not
incidence rates of decisions to forego dialysis becausethe latter would require a cohort study. Second, ne-
phrologists’ responses regarding how often theywithheld or withdraw dialysis may have been subject
to recall bias. Third, it is not certain that nephnobo-gists’ responses to the dialysis withdrawal scenarios
accurately predict their future practices. Fourth, ab-though the 73% response rate is respectable for asurvey of physicians, nonresponders may be lessinterested than responders in ethical issues andtherefore less likely to consider foregoing dialysis.Finally, It may not be appropriate to generalize theexperiences and attitudes of nephrologlsts in NewEngland to nephrologists in other regions of theUnited States or other countries such as Canada.
Despite these limitations, we conclude that ne-phrologists in this survey reported that they withhelddialysis more times than they withdrew it during thepreceding 1- and 5-yr periods. This finding is impor-tant for two reasons. First, empirical studies thatfocus on withdrawal (which is easier to measure) maysubstantially underestimate the overall rate of deci-sions to forego (i.e. , withhold or withdraw) life-sus-taming treatment. Second, preferentially withhold-ing rather than withdrawing treatment tends to denypatients the opportunity of a trial of therapy. Physi-clans may withhold rather than withdraw dialysisbecause it Is emotionally easier to refrain from acting
than to act. As the President’s Commission con-cluded, however, “neither law nor public policyshould mark a difference in moral seriousness be-
tween stopping and not starting treatment” (5). Wedid not examine the reasons for withholding butsuggest that future studies should explore why phy-sicians withhold dialysis more than they withdrawit.
We further conclude that consensus exists regard-ing the management of competent patients and in-competent patients with clear prior wishes. Eighty-eight percent of nephrologists were willing to stopdialysis upon the request of a competent patient. Thisfinding is encouraging because It suggests that theattitudes of nephrobogists are in accord with publicpolicy In medical ethics, which emphasizes the rightof competent adult patients to determine the courseof their own medical cane. (Of course, nephrologistsshould discuss and attempt to address their patients’reasons for stopping dialysis, and depression should
be carefully excluded.) When requested by the familyof an incompetent patient with clear prior wishes,
90% of nephrologists would stop dialysis. This result,which is comparable to nephrologists’ responses to
the competent patient, demonstrates that the atti-tudes of nephrologists are in accord with public policyin medical ethics, as enunciated recently in the Cru-zan decision, that Incompetent patients with clear
prior wishes should be permitted to forego life-sus-
taming treatment.
However, nephnologists disagree about the man-
agement of incompetent patients with unclear prior
wishes. When requested by the family of an Incom-
petent patient with unclear prior wishes, only 63%
of nephrologists said they would stop dialysis. Incontrast to the consensus in response to the previous
two scenarios, the nephnobogists’ responses to theincompetent patient with unclear prior wishes sug-gest that they have difficulty with this situation. Thisfinding may reflect the nephnobogists’ discomfort Inmaking decisions to stop dialysis with substitutedjudgment or best interests standards.
Unfortunately, many patients for whom the deci-sion to withdraw dialysis is considered are incompe-tent and have expressed no clean wishes about thedecision to continue or stop dialysis. This situationadmits no satisfactory resolution. If dialysis is con-tinued, and the patient would have wanted It stopped,then the patient must endure suffering he or shewould not have intended for himself or herself. Ifdialysis is stopped, and the patient would havewanted it continued, then the patient’s life is termi-nated prematurely. In the absence of clear evidenceof the patient’s wishes, there is no way to minimizethese two types of error.
What should the dialysis community do? In theabsence of a satisfactory method to address the sit-uation of the incompetent patient with unclear priorwishes, dialysis units should try to prevent this sit-uation by discussing with patients their preferences
for dialysis before patients become incompetent andby recording these discussions In an advance direc-tive. This strategy would shift patients from an eth-ically, legally, and clinically problematic scenario (in-competent, unclear prior wishes) to a less problem-atic one (incompetent, clean prior wishes).
Although investigators have begun to evaluate ad-vance directives in other clinical settings (14-21),important questions remain about the use of advancedirectives in dialysis units. Should the policy focuson who will make decisions for the patient (proxydirective), on what decisions will be made for thepatient (instruction directive), or on both? Whichhypothetical clinical situations and life-sustaIningtreatments (other than dialysis) should be includedin the instruction directive? Do dialysis patients findsuch advance discussions desirable? When shouldthe discussions occur? Who should Initiate them?How can the use of advance directives be promotedin dialysis facilities? Once incompetent, will patientsreceive the type of care they request in the advancedirective? What is the impact of advance directiveson costs? Because of the enduring patient-healthprofessional relationships, dialysis units representan excellent model for research on advance direc-tives.

Foregoing Dialysis � .- � -.‘ .� ... �. �.. . -�. � ,..� ..,‘.� .�
1240 Volume 2 . Number 7 . 1992
ACKNOWLEDGMENTS
We are grateful to J.F. Jekel, M.D. , and Angela R. Holder, LL.M. . for
reviewing an earlier version of this article and to three anonymous
reviewers for helpful comments. Dr. Singer is supported by a Cana-
dian Life and Health Insurance Association Medical Scholarship.
The Centre for Bioethics is supported as a Health System Linked
Research Unit by the Ontario Ministry of Health and by the Bertha
Rosenstadt and William C. Harris Estates. ESRD Network of New
England is supported by HCFA contract no. 500-88-00 1 4. This study
was performed while Dr. Singer was a Robert Wood Johnson Clinical
Scholar at Yale University School of Medicine. The research was
used in partial fulfillment of the requirements for a Master of Public
Health degree from Yale University.
REFERENCES
1 . Neu S, Kjellstrand CM: Stopping bong-termanalysis: An empirical study of withdrawal oflife-supporting treatment. N Engl J Med 1986;314: 14-20.
2. Port FK, Wolfe RA, Hawthorne V, FergusonCW: Discontinuation of dialysis therapy as acause of death. Am J Neprol 1989;9:145-149.
3. Rodin GM, Chmara J, Ennis J, Fenton S. LocingH, Steinhouse K: Stopping life-sustaining med-Icab treatment: Psychiatric considerations in thetermination of renal dialysis. Can J Psychol1981 ;26:540-544.
4. U.S. Renal Data System. USRDS 1990 AnnualReport. The National Institutes of Health. Na-tional Institute of Diabetes and Digestive andKidney Diseases, Bethesda MD, August 1990.
5. President’s Commission for the Study of Ethi-cal Problems in Medicine and Biomedical andBehavioral Research. Deciding to Forego Life-Sustaining Treatment: Ethical, Medical, and Le-gal Issues in Treatment Decisions. Washington,DC: U.S. Government Printing Office; 1983.
6. The Hastings Center. Guidelines on the Termi-nation of Life-Sustaining Treatment and theCare of the Dying. Bniarcbiff Manor, New York:The Hastings Center; 1987.
7. Emanuel EJ: A review of the ethical and legalaspects of terminating medical care. Am J Med1988;84:291-301.
8. Singer PA, Siegler M.: Elective use of life-sus-taming treatments. In: Stobberman GH, ed. Ad-
vances in Internal Medicine. Vol. 36. New York:Year Book; 1991:57-79.
9. Singer PA, Siegler M.: Decisions to forego life-sustaining treatment. In: Kassirer JP, ed. Cur-rent Therapy in Internal Medicine. 3rd Ed. Phil-adebphia: BC Decker; 1991:98-103.
10. Singer PA, Siegler M: Forum commentary. In:Lowance DC. Withdrawal from dialysis: An eth-ical perspective. Kidney Int 1 988;34: 124-35.
1 1 . Singer PA: Withdrawal from Dialysis. AmericanKidney Fund Newsletter for Health Professionals1 989;6:2-4.
12. Harvey LK, Shubat SC. Physician and PublicAttitudes on Health Care Issues. Chicago: Amen-ican Medical Association; 1989:13.
13. Uhlmann RF, Pearlman PA, Cain KC: Physi-cians’ and spouses’ predictions of elderly pa-tients’ resuscitation preferences. J Genontol1988;43:M1 15-Mi 121.
1 4. Lo B, McLeod GA, Saika G: Patient attitudes todiscussing life-sustaining treatment. Arch In-tern Med t986;146:16i3-1615.
1 5. Finucane TE, Shumway JM, Powers RL, D’A-lessandri RM: Planning with elderly outpatientsfor contingencies of severe illness: A survey andclinical trial. J Gen Intern Med 1 988;3:322-325.
1 6. Shmerling RH, Bedell SE, Lilienfeld A, Del-banco TL: Discussing cardiopulmonary resus-citation: A study of elderly outpatients. J GenIntern Med 1988;3:317-32i.
1 7. Frankl D, Oye RK, Bellamy PE: Attitudes ofhospitalized patients towards life support: A sun-vey of 200 medical inpatients. Am J Med1 989;86:645-648.
1 8. Teno J, Fleishman J, Brock DW, Mor V: Theuse of formal prior directives among patientswith HIV-related diseases. J Gen Intern Med1 990;5:490-494.
19. Hare J, Nelson C: Will outpatients complete liv-ing wills? A comparison of two interventions. JGen Intern Med 199i;6:41-46.
20. Emanuel LL, Barry MJ, Stoeckle JD, EttelsonLM, Emanuel EJ: Advance directives for medicalcare-a case for greater use. N Engb J Med1 99 1 ;324:889-895.
2 1 . Danis M, Southerland LI, Garrett JM, et al.: Aprospective study of advance directives for life-sustaining cane. N Engb J Med 1 99 1 ;324:882-888.