neph ro pharmacology
TRANSCRIPT
NEPHROPHARMACOLOGY
DARMAWAN,dr.,M.Kes
Introduction• Kidney comprise only 0,5 %
BW, but receive 25% CO• So, drugs can damage the
kidney, renal disease affects responses to drugs
• The recognition of DIRD is very important because the resulting ARF & CRF pottentially reversible & preventable

Subtopics
• Drugs induced renal disease
(=DIRD)
• Drugs prescribing in renal
disorders
Mechanisms of DIRD :1) Direct biochemical effect :
Heavy metals (Hg, Au, Fe, Pb) Antimicrobials (Aminoglycosides, Cephalosporins, sulphonamides) Contrast media (biliary) Analgesics (aspirin) Solvents (CCL4, Ethylene Glycol)
2) Indirect biochemical effect : Uricosurics urate
precipitation Calciferol renal
calcification Diuretic/laxative tubular
damage Sulphonamides crystallise
in UT Anticoagulant
haemorrage into kidney:
3) Immunological effect : Penicillins, sulphonamides, isoniazid, Rifampicin Phenytoin, procainamide, hydralazine Au, Penicillamine
A drug renal disease, by > 1 mechanisms (sulphonamides)
Sites & Pathological types of RD
1.Glomerular2.Tubular
Damage proximal, medulla, distal Obstruction
3.Other DIRD
1. Glomerular : large surface area glomerular capillaries susceptible to damage from circulating immune complexes
Penicillamine: GlomerulonephritisProteinuria Nephrotic syndrome
Creatinine clearance (= CCR) a measure of glomerular filtration rate (= GFR)
Formula of Cockcroft & Gault : (140 – age ) x BW CCR = 72 x Cs
Notes : - Cs = Serum creatinine - Women = Man – 15 %

2. Tubular Tubular damage
200L/day GF 1,5 L/day urine renal tubular cells expose more than other cells to toxins Proximal, medulla, distal tubular
Tubular obstructionCertain physico chemical conditions crystal can deposit within tubular lumen

Tubular proximal toxicity By acids (salicylates,
cephalosporins), bases (aminoglycosides), heavy metals
and contrast media Urinary excretion of glucose, phosphate, HCO3, amino
acids
Medullary toxicity NSAID >< local Pg
ischaemia analgesic nephropathy

Distal tubular toxicity Under physico-chemical conditions, crystal can deposit within tubular lumen Methotrexate (relative insoluble at low Ph) can prepitate in distal tubular when urine is acid Nucleic acids (in leukemic cells) breakdown by chemotherapy insoluble urate will be prescipitate

3. Other DIRD Vasculitis by sulphonamide, allopurinol, isoniazid Allergic Interstitial Nephritis by penicillins, sulphonamides, thiazides, allopurinol, phenytoin SLE by hydralazine, procainamide ARF by aminoglycosides, cisplatin NS by penicillamine, Au, captopril CRF by NSAID, amphotericin-B Functional impairment due to impairment to dilute/concentrate urine, potassium loss, acid-base imbalance

Vulnerability factor to DIRD1) High work-load of renal
function2) Glomerural endothelial surface
area >3) Capacity to concentrate of
drugs & nephrotoxins in lumen4) Liability to immune injury5) Accumucation of drugs &
metabolites (in renal insufficiency)

Drugs may :1. Exacerbate renal diseases2. Accumulate, due to failure of renal excretion/changes in protein binding3. Be ineffective, e.g thiazide in moderate/severe renal failure, uricosurics
Problem: RF patients must be treated with nephrotoxic drugs & largelly eliminated by the kidney
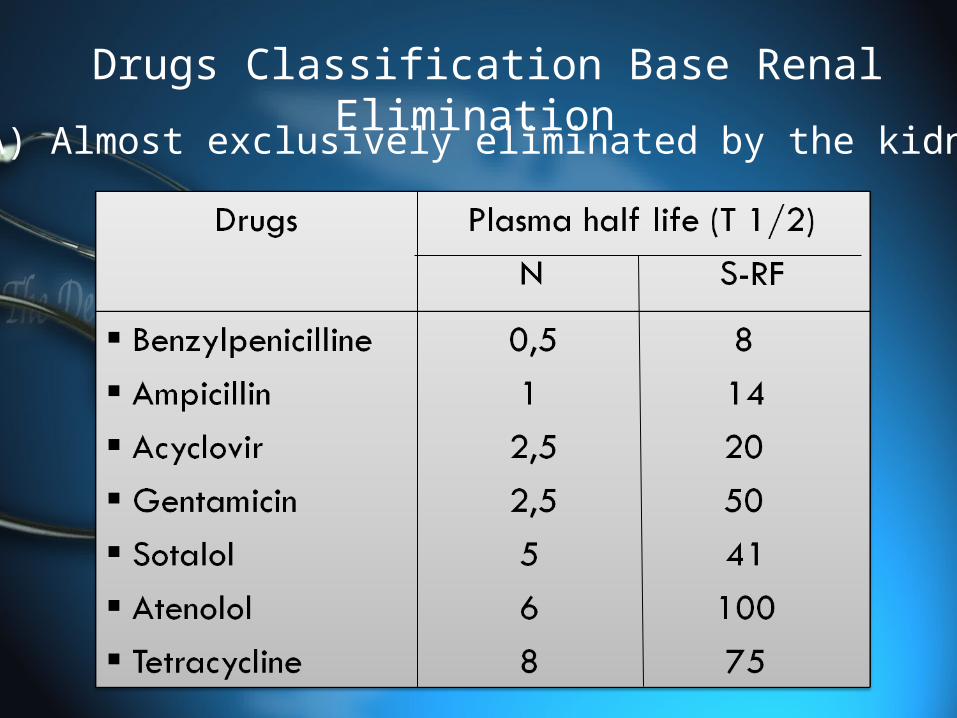
Drugs Classification Base Renal Elimination(A) Almost exclusively eliminated by the kidney

(B1) Almost entirely metabolised
(B2) Drugs produce pharmacologically active metabolites (water-soluble) renal elimination
In RF accumulate e.g. - Acebutolol, hydralazine, Isosorbide dinitrate - Allopurinol, carbamazepine - Chordiazepoxide, diazepam, clobazam, flurazepam - Metronidazole, 5-FU
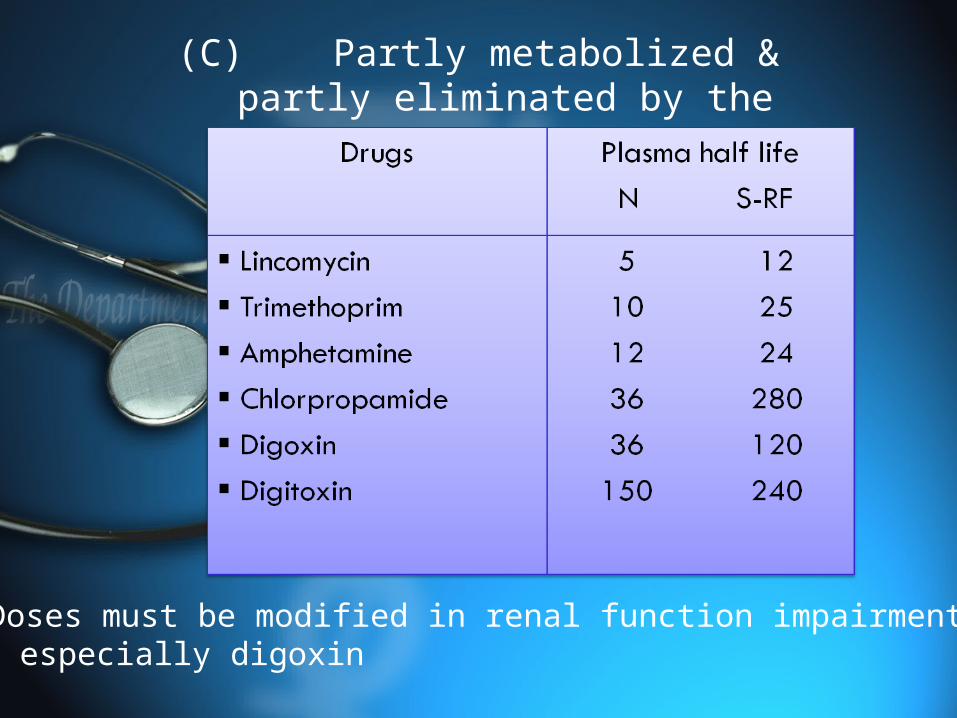
(C)Partly metabolized & partly eliminated by the kidney
- Doses must be modified in renal function impairment especially digoxin

Dosing regimens in renal impairment (general rule)
Group A/B2 : Initial dose-normal/slightly Maintenance dose or interval dose
Group B1 :Initial dose-normal or in advanced-RD,Hypoproteinemia, drugs with highly protein binding
Group C : Initial dose-normal Maintenance dose/interval dose will be modified
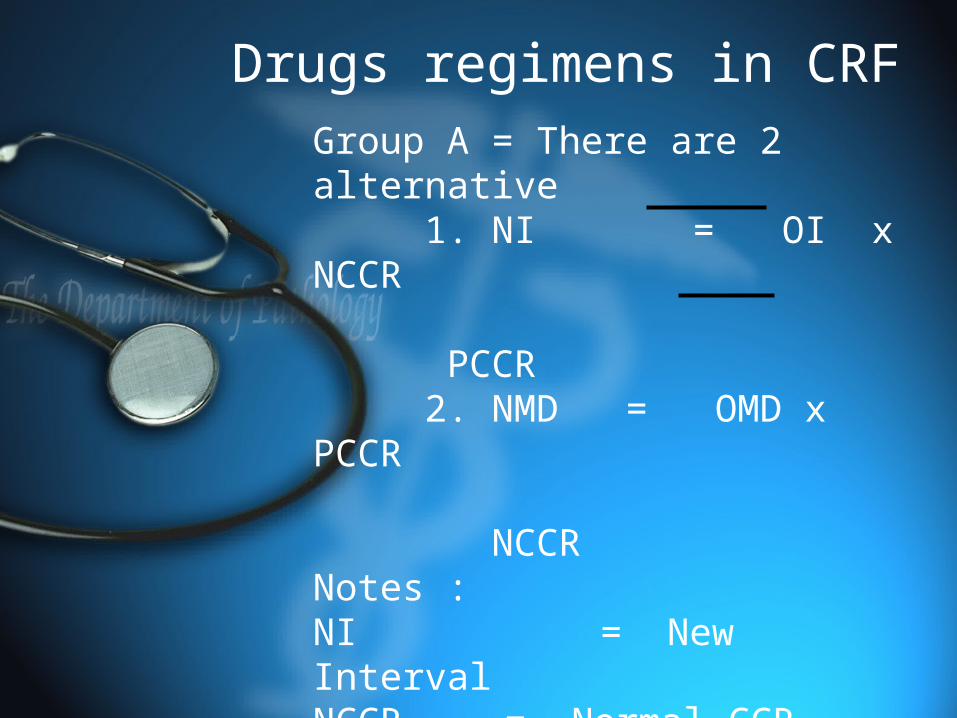
Drugs regimens in CRFGroup A = There are 2 alternative 1. NI = OI x NCCR PCCR 2. NMD = OMD x PCCR NCCRNotes :NI = New IntervalNCCR = Normal CCRNMD = New Maintenance doseOI = Old intervalPCCR = Patient CCROMD = Old maintenance dose
Group C : Calculate correction factor (CF) CF = 1 F(KF – 1 ) +1 F = Unchanged drug fraction in urine KF = Ratio of PCR /NCR
There are 2 alternative 1. NI = OI x CF 2. NMD = OMD x 1 CF

Drugs prescribing guidelines in RF1. Use a drug in define indications2. Choose a drug with minimal
nephrotoxics effect3. Use plasma level to adjust the dose4. Use recommended dosage regimens
for RF5. Avoid prolonged courses of
potentially toxic drugs6. Avoid potentially nephrotoxic
combination of drugs7. Monitor the patient carefully for
clinical efficacy & evidence of toxicity
