negotiating ict development and use: the case of a telemedicine system in the healthcare region of...
TRANSCRIPT
INFORMATION
Information and Organization 16 (2006) 27–55
www.elsevier.com/locate/infoandorg
ANDORGANIZATION
Negotiating ICT development and use: Thecase of a telemedicine system in the
healthcare region of Crete
Panos Constantinides *, Michael Barrett
The Judge Institute of Management, University of Cambridge, Trumpington Street,
Cambridge CB2 1AG, UK
Received 2 August 2004; received in revised form 4 July 2005; accepted 15 July 2005
Abstract
Recent research on the development and use of information and communication technol-ogy (ICT) has focused on the emergent use of technology in practice and the multiplicity ofoutcomes being simultaneously negotiated by different groups and individuals. In this paper,we seek to understand this emergent process by examining the interrelationship between thecontext(s) in which ICTs are introduced, the ways in which ICTs are enacted in practice,and the role of different technological artifacts. We pursue the value of these conceptual devel-opments in an interpretive case study on the introduction of a telemedicine system in thehealthcare region of Crete, Greece. Some key implications arising from the case study referto the relationship between power relationships and organizational change; the relationshipbetween existing work practices and resistance to ICT-mediated change; and the role of differ-ent artifacts in negotiations of power, as well as in processes of community formation.� 2005 Elsevier Ltd. All rights reserved.
Keywords: ICT; Organizational change; Telemedicine; Boundary objects; Process research; Interpretivecase studies
1471-7727/$ - see front matter � 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.infoandorg.2005.07.001
* Corresponding author. Tel.: +44 1223 339700; fax: +44 1223 339581.E-mail addresses: [email protected] (P. Constantinides), [email protected] (M. Barrett).
28 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
1. Introduction
Recent research on information and communication technology (ICT) develop-ment and use has focused on practice-level explanations of the interplay betweentechnology and organizational continuity and/or change (Orlikowski, 2000). Theunderlying argument is that we should move away from a view of ICT as fixed orembedded in a set of organizational and technological structures and towards a fo-cus ‘‘on human agency and the open-ended set of emergent structures that may beenacted through recurrent use of a technology’’ (Orlikowski, 2000, p. 412). More re-cent work has built on this practice perspective to also recognize the importance ofsocial influences on individual enactments of technology use over time (Boudreau &Robey, 2005). In addition, some researchers drawing from the broad field of Scienceand Technology Studies have argued that, in any given ICT project, there are severaloutcomes simultaneously being negotiated by different groups and individuals (Bow-ker & Star, 1999; Star & Ruhleder, 1996). In this view, people are members of multi-ple communities simultaneously, which produces precarious outcomes for therelationships between different groups and individuals, their practices, and choiceof technological artifacts, including ICT (Bowker & Star, 1999).
This paper seeks to contribute to a richer understanding of ICT development anduse by recognizing the value of practice-level explanations while drawing on multipleperspectives and seeking to understand the broader network of interactions betweendifferent groups and individuals. This objective is pursued by examining the interre-lationship between the context(s) in which ICTs are introduced, the ways in whichICTs are enacted in practice by different groups and individuals, and the role of dif-ferent technological artifacts in this process. First, we examine the changing role ofdifferent contextual elements, such as political reforms in the broader environmentwhere the ICT project unfolds. Second, we examine the structures of reference thatdifferent stakeholders draw upon to make sense of, and act in, their work and socialcontexts. Structures of reference refer to the underlying meanings and intentions thatpeople have about an object, action or event, which are constantly being shaped inlight of new knowledge brought into their communities, changing contextual ele-ments, and new and existing artifacts. Finally, we examine the changing role of dif-ferent artifacts such as the existing technological base and other specialized objects.These artifacts may often play a key role in ICT projects, either by reinforcing theneed for change or by being employed as a means for resistance and continuity(of existing work practices) by different groups and individuals. We argue that theinterplay between contextual elements, the structures of reference of different partic-ipants, as well as their choice of artifacts follows an ecological evolution where di-verse (and often contradicting) outcomes are simultaneously being negotiated atdifferent levels and points in time. We will pursue the value of these conceptual devel-opments in an interpretive case study on the introduction of a telecardiology collab-oration workspace between primary healthcare centers and a district hospital in thehealthcare region of Crete, Greece.
The rest of the paper is organized as follows. In Section 2, we discuss our concep-tual foundations by drawing on existing knowledge on ICT development and use.
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 29
Then, in Section 3, we describe our research approach including methods of datagathering, coding and analysis. In Section 4, we provide a brief description of thecase study, as informed by the interviewees and other secondary data. Section 5 pro-vides an analysis of the case study based on our conceptual foundations. Then, inSection 6, we return to our research questions, and discuss the findings from the casestudy in more depth. Finally, in Section 7, we conclude with some implications forresearch and practice.
2. Conceptualizing ICT development and use as a process of negotiation
The process of negotiating meanings and actions around new initiatives such asthe introduction of new ICT in existing work practices has been very difficult to ex-plain let alone manage. In an effort to understand this process, researchers have em-ployed diverse conceptual frameworks, such as structurational models (Barrett &Walsham, 1999; Orlikowski & Robey, 1991), dialectical models (Robey & Boudreau,1999; Sabherwal & Newman, 2003), practice-level approaches (Boudreau & Robey,2005; Orlikowski, 2000), and a number of approaches drawing from the broad fieldof Science and Technology Studies (Bowker & Star, 1999; Hanseth & Monteiro,1997; Star & Ruhleder, 1996). Although this variation has given birth to novel waysof examining the processes of organizational continuity and change, it has also cre-ated a theoretical diversity that often discourages constructive dialogue between dif-ferent approaches. Instead, this paper follows the argument of a growing number ofscholars that the multifaceted nature of social and organisational reality that IS re-search is often faced with can only be approached through the application of multi-ple philosophical beliefs and methods (Robey & Boudreau, 1999; Walsham, 1995).This section will draw on, and develop links between, some of the key elements ofdivergent analyses of ICT development and use to build a ground for unearthingnegotiation processes in ICT projects. Table 1 provides a summary of our conceptualfoundations.
2.1. Contextual elements of ICT development and use
The first conceptual element emerging from research on ICT development and userefers to the relationship between context and process. ICT development and use haslong been described as a social process involving users, project and senior managers,and other key stakeholders (Newman & Robey, 1992; Robey & Boudreau, 1999;Sabherwal & Newman, 2003). In turn, this social process has been linked to both in-tra-organizational and broader contexts, and emerging from a series of historical,organizational and economic circumstances (Walsham, 1993). The linkage betweencontext and process is key for understanding the impact of new ICT initiatives,‘‘which are both constrained by the context in which they are developed and, in turn,are a factor for maintaining or altering that context’’ (Walsham, 1993, p. 60).
Context is understood to refer to the broader socio-political structure in which agiven ICT project unfolds, including industry characteristics, political agendas and
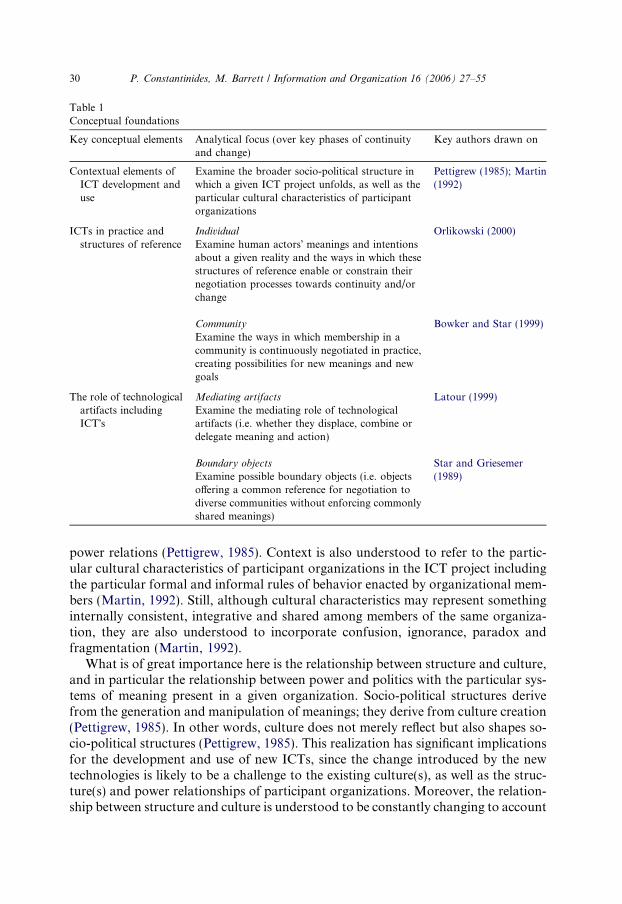
Table 1Conceptual foundations
Key conceptual elements Analytical focus (over key phases of continuityand change)
Key authors drawn on
Contextual elements ofICT development anduse
Examine the broader socio-political structure inwhich a given ICT project unfolds, as well as theparticular cultural characteristics of participantorganizations
Pettigrew (1985); Martin(1992)
ICTs in practice andstructures of reference
Individual Orlikowski (2000)Examine human actors� meanings and intentionsabout a given reality and the ways in which thesestructures of reference enable or constrain theirnegotiation processes towards continuity and/orchange
Community Bowker and Star (1999)Examine the ways in which membership in acommunity is continuously negotiated in practice,creating possibilities for new meanings and newgoals
The role of technologicalartifacts includingICT�s
Mediating artifacts Latour (1999)Examine the mediating role of technologicalartifacts (i.e. whether they displace, combine ordelegate meaning and action)
Boundary objects Star and Griesemer(1989)Examine possible boundary objects (i.e. objects
offering a common reference for negotiation todiverse communities without enforcing commonlyshared meanings)
30 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
power relations (Pettigrew, 1985). Context is also understood to refer to the partic-ular cultural characteristics of participant organizations in the ICT project includingthe particular formal and informal rules of behavior enacted by organizational mem-bers (Martin, 1992). Still, although cultural characteristics may represent somethinginternally consistent, integrative and shared among members of the same organiza-tion, they are also understood to incorporate confusion, ignorance, paradox andfragmentation (Martin, 1992).
What is of great importance here is the relationship between structure and culture,and in particular the relationship between power and politics with the particular sys-tems of meaning present in a given organization. Socio-political structures derivefrom the generation and manipulation of meanings; they derive from culture creation(Pettigrew, 1985). In other words, culture does not merely reflect but also shapes so-cio-political structures (Pettigrew, 1985). This realization has significant implicationsfor the development and use of new ICTs, since the change introduced by the newtechnologies is likely to be a challenge to the existing culture(s), as well as the struc-ture(s) and power relationships of participant organizations. Moreover, the relation-ship between structure and culture is understood to be constantly changing to account

P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 31
for new individuals entering the negotiation process with new meanings and inten-tions. That is, in the same way that the underlying systems of meaning of differentgroups and individuals change over time, so does the context of their everyday workand social activities. Thus, although we may talk about the context of a given study,this context needs to be understood as dynamic and changing in nature.
2.2. ICTs in practice and structures of reference
The second conceptual element refers to the ways in which existing work practicesmay shape and be shaped by the introduction of new ICTs. This conceptual elementis closely interlinked with our discussion on context, in that, it looks at the underly-ing assumptions, knowledge and expectations that people have about ICT and whichthey draw upon to make sense of, and act in, their work and social contexts. Theo-retical approaches for examining the relationship between existing work practicesand the practices being introduced through new ICTs include dialectical modelsbased on a logic of opposition (Robey & Boudreau, 1999; Sabherwal & Newman,2003), a practice lens based on structuration theory (Orlikowski, 2000), and socio-technical analyses drawing from the broad field of Science and Technology Studies(Bowker & Star, 1999; Star & Ruhleder, 1996).
First, dialectical models pay particular attention to the ‘‘pluralistic world of col-liding events, forces, or contradictory values that compete with each other, for dom-ination or control’’ (Van de Ven & Poole, 1995, p. 517). In a dialectical sense,opposition does not necessarily mean conflict; rather it refers to the process of giveand take, of negotiating meaning and synthesizing action. Employed in research onICT development and use, dialectical models seek to explain the ways in which par-ticipants continually construct the technology and the work context in which it isintroduced through a process of give and take (Robey & Boudreau, 1999; Sabherwal& Newman, 2003). Second, building on the premises of structuration theory (Gid-dens, 1984), Orlikowski (2000) develops a �practice lens� to examine how people,as they interact with groupware technologies in their work practices, enact structureswhich shape their emergent use of the technology. Orlikowski (2000, p. 404) arguesthat viewing the use of technology as ‘‘a process of enactment’’ enables a deeperunderstanding of the role of work practices in the ongoing use and transformationof new technologies. Finally, some socio-technical analyses draw and extend onmore traditional Science and Technology Studies which argue that work practicesare intimately interconnected to a number of �constitutive� elements such as technicaldevices, forms, classifications, tools, etc., all of which mediate, and become mediatedby, the contextual configuration of work (Latour, 1991; Woolgar, 1991). In an at-tempt to further understand this socio-technical process, some researchers focusedon two sets of relationships: between people and membership in their social andwork contexts; and between artifacts and their ‘‘naturalization’’ (their taken-for-grantedness) by different communities (Bowker & Star, 1999; Star & Ruhleder,1996). These relationships are constantly torn in an interplay between ambiguous(new, strange) and naturalized (taken-for-granted) encounters with people, artifactsand classes of action involved in a given community. Moreover, in the presence of an

32 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
ever-increasing number of communities (e.g. different types of professional commu-nities, informal communities, and variations of those), not only are people membersof multiple communities, but membership to any community is constantly beingnegotiated. Likewise, the naturalization of artifacts in a given community is negoti-ated by the same and different individuals at different points in time.
In this paper, similar to Orlikowski�s (2000) �practice lens�, we acknowledge thathuman actors� meanings and intentions about a given reality – we call these struc-
tures of reference – are continuously constructed and refined in practice throughinferences of past experience, as well as the obtainment of new knowledge. Forexample, consider how in an effort to reach a conclusion on a patient�s medical con-dition, a general practitioner (GP) follows a set of standard practices, such as exam-ining the patient�s medical record and conducting a set of exams, all of which buildon the GP�s inferences of past experience and knowledge, while also being mediatedby new meanings and perhaps new practices (e.g. the use of new technologies). Thus,whether human actors engage in routine work processes or new processes in themaking, they are always drawing on their structures of reference to make sense of,and act/interact with other individuals (including the use of technological artifacts).As human actors negotiate new meanings about a given reality, they continuouslyreproduce and refine their structures of reference to account for new knowledge.
Moreover, linking our discussion to the first conceptual element, our theoreticalapproach attributes a strong relationship between context and action. Specifically,individual interpretations as to the role of new ICT in their work practices may even-tually produce a change in the activities of other individuals in the same context.That is, the success of a given ICT introduced in a given context will depend onthe collective efforts of all participants. In other words, the reality around the givenICT will continue to be negotiated until determined by a community of participants.In fact, similar to the research of Star and Ruhleder (1996) and Bowker and Star(1999), we argue that the development and use of any ICT is intimately interlinkedto the structures of reference of multiple communities of users. This argument hastwo implications. First, that meanings and actions are interwoven with work prac-tices, and second that, technological artifacts are usually interpreted independentlyof the intentions of their creators, and that what transcends these intentions is thenotion of a community. In other words, what will prevail in the long run is the realitythat builds up from the collective interpretations of a given community. Without adoubt, at any given context, the same individuals may be members of multipleand diverse communities (Bowker & Star, 1999). However, by following the historic-ity of the interpretive chain over key periods of continuity and change, we can realizewhich individuals become members of which community and what they perceive therole of technology to be in their work practices.
2.3. The role of technological artifacts including ICTs
The third and final conceptual element emerging from research on ICT develop-ment and use distinguishes between the use of the technology and its artifactual char-acter. Although the two are closely interrelated, since technology can only be

P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 33
understood when used in practice, the distinction is critical to understanding ICT asboth a physical entity and as a thing that emerges in use. In particular, we want to gobeyond an understanding of ICT as an artifact with embedded structures as intendedby the developers and as emergent in practice (Orlikowski & Iacono, 2001); we wantto understand the role of ICT as a technological artifact independent of any inten-tions or structural properties but involved in processes of negotiation.
To facilitate the discussion around the role of technological artifacts, consider thefollowing scenario. A patient visits the local primary healthcare center to inform his/her GP of some signs of a possible cardiac problem, such as dizziness and chest pain.The GP performs a series of standard practices, such as consultation of the patient�smedical record, and generation of an electrocardiograph (ECG). By this point, theGP has developed an initial understanding of the patient�s condition, based on thepatient�s description, the patient�s medical history, the ECG, and the GP�s own expe-rience with similar cases – all interacting and mediating the GP�s interpretation andnext actions. To receive a second opinion by a more specialized physician (i.e. a car-diologist), the GP connects to a district hospital through a telemedicine system. TheGP and cardiologist discuss their interpretations of the patient�s condition and makesuggestions for ways forward. The telemedicine system records this interaction andthe patient�s medical record is updated in the relevant database(s).
In the above scenario, there are a series of artifacts, including an ECG device andpaper-based medical records that are at the GP�s disposal for use towards differenttasks at different time periods in the provision of care. We can categorize these arti-facts in two broad types: those that mediate and those that bind the work of health-care professionals.
The first type is that of artifacts with a mediating role (Latour, 1999). A mediator,in Latour�s vocabulary, does not transport meaning or action without transforma-tion; a mediator displaces (i.e. distorts meanings and actions), combines (i.e. bringsmultiple meanings and actions together), or delegates (i.e. acts on behalf of some-thing or someone). For example, in our scenario, although the final diagnosis mayhave relied more on the GP�s and the cardiologist�s professional knowledge andexperience, the number of artifacts employed by the two physicians (e.g. the ECGdevice and the telemedicine system) mediated the physicians� judgment by renderinggeneral signs to specific symptoms. In other words, action should be understood as acollective effort between human actors and artifacts while exchanging competences,and offering one another new possibilities (Latour, 1999, p. 182). This is not to saythat artifacts can, by any means, act on their own in the same way as humans do,since artifacts can only mimic certain actions that have been programmed in theirrepertoire of actions by their human designers (Collins & Kusch, 1998). Nonetheless,even in their mimicking fashion, artifacts used in practice can shape their humanusers� interpretations and actions. In those instances, agency takes the form of a hu-man-artifact hybrid that is mutually and emergently transformed in practice (Jones,1998). That is, humans seek to shape technological artifacts towards particular goalsin ways that are not wholly determined either by the intentions of the human actorsor by the material properties of technology, but by the interplay of the two (Picker-ing, 1993).
34 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
The second type of artifacts refers to the concept of boundary objects (Star &Griesemer, 1989). Boundary objects are those objects that originate and continueto be negotiated in more than one community while satisfying the informationalrequirements of each of them. They have two important properties: they are looselystructured in common use, and become more tightly bound in particular locations(Bowker & Star, 1999). In this sense, boundary objects have different meanings indifferent communities but their structure is common enough to more than one com-munity to make them recognizable. For example, if we assume that, in the above sce-nario, the GP and the cardiologist have participated in negotiations towards thedevelopment and use of the telemedicine system then the telemedicine system canbe described as a boundary object. It can be described as such in that, work at dif-ferent sites (the primary health centre and the district hospital) and with differentperspectives (the GP and the cardiologist) was agreed to be conducted autonomouslywhile not necessarily enforcing any commonly shared meanings among participants.
Both mediating artifacts and boundary objects have a distinct role to play in thechange and/or continuity wrought by ICT development and use. In practice, bound-ary objects will either become �grounded� as formal representations of work (i.e. be-come ‘‘naturalized’’), at which point they will contribute to the process of change orthey will continue to be negotiated until they eventually become grounded or dis-carded by participants. As soon as a boundary object becomes grounded as a formalrepresentation of work, it will stop being negotiated since a consensus has beenreached as to its role in practice; at this moment, it will be transformed into a medi-ating artifact that is used for a collectively agreed task, a standard (Hanseth &Monteiro, 1997). Of course, as new members and new meanings enter the negotia-tion process, even these standards will be challenged and transformed; a standarddoes not remain a standard for too long (Monteiro, 1998; Star, 1991). Rather, justlike the broader context, as well as the particular structures of reference of differentgroups and individuals, technological artifacts are continuously constructed and re-fined. Nonetheless, by explicitly theorizing the role of different technological artifactsin the work practices of different groups and individuals, the processes of change andcontinuity can be better informed.
2.4. Summary
The conceptual foundations elaborated here examine the interrelationship be-tween the context(s) in which ICTs are introduced, the ways in which ICTs are en-acted in practice by different groups and individuals through their structures ofreference, and the role of different technological artifacts in this process. In this re-spect, while sharing many of the insights of past research we differentiate our ap-proach as encompassing and multi-layered, offering more opportunities for aricher understanding of ICT development and use. To this end, the level of analysisis not restricted to a single focal organization or group of participants rather it ismultilayered, seeking to understand the broader network of interactions between dif-ferent groups and individuals, as well as their relationships to different artifacts andpractices.
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 35
3. Research approach
In our field study, we sought to examine the ongoing negotiation processes be-tween different groups and individuals in an attempt to introduce a telecardiologycollaboration workspace (TCW) in the regional healthcare sector of Crete, Greece.
3.1. Key research questions
Our central research focus involves the development and use of ICT with a par-ticular focus on telecardiology services. Our key research questions aim at examin-ing: (1) the role of ICT in the work and social contexts of different groups andindividuals; and (2) the way(s) ICT development and use is negotiated in practiceover time.
3.2. Methods
The overall approach was qualitative, which is recommended for studying conti-nuity and change in ICT development (Robey & Boudreau, 1999). An in-depth lon-gitudinal case study method was adopted as the appropriate research design, as itenabled us to understand how the process evolved over time and why it evolved incertain ways and not otherwise (Langley, 1999; Pettigrew, 1990). Further, it is widelyaccepted that case studies are the preferred research strategy when �how� or �why�questions are being posed regarding a process study and when an in-depth under-standing of phenomena in the IS field is needed (Klein & Myers, 1999; Walsham,1995).
The principal method of data collection was through in-depth semi-structuredinterviews of senior management, IT professionals, and healthcare professionals ofvarious participating organizations in the project. The main focus of the interviewswas around the meaning of ICT to the different individuals or groups and theirexpectations around its use, particularly with respect to their work contexts. Thesemi-structured design of the interviews allowed for questions to be adapted to thecharacteristics and position of each interviewee. For example, more detailed ques-tions on the strategy and design of the TCW were directed to senior managementand IT personnel from the private institute that initiated the project. Similarly, moredetailed questions on the changing nature of their work wrought by the introductionof the TCW were directed to participating healthcare professionals. The questionsdirected to the Regional Health Authorities focused on socio-political issues shapingcollaboration with the private institute, as well as the potential integration of theTCW in the healthcare region�s future plans.
The longitudinal nature of the study also meant that interview questions wouldfocus on how actions and expectations changed over time. For example, in additionto being asked to discuss current events, the interviewees were encouraged to com-ment on major historical events concerning the TCW project which helped producea concurrent and reconstructed account of key events that happened prior to andduring our fieldtrips. In addition, a repeat interview method was adopted with a
36 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
number of key informants being interviewed at each phase of research, which furtherhelped us to understand their perceptions over time.
Interviews were supplemented by real-time observation of the use of the TCW,study of publications, press reports, and various other sources regarding the keyevents in the project timeline, as well as social interactions with different membersfrom the private institute that initiated the project. The aim of this multiple data col-lection method was to account for issues and concerns outside formal interviews andto gain a clearer picture of emerging themes.
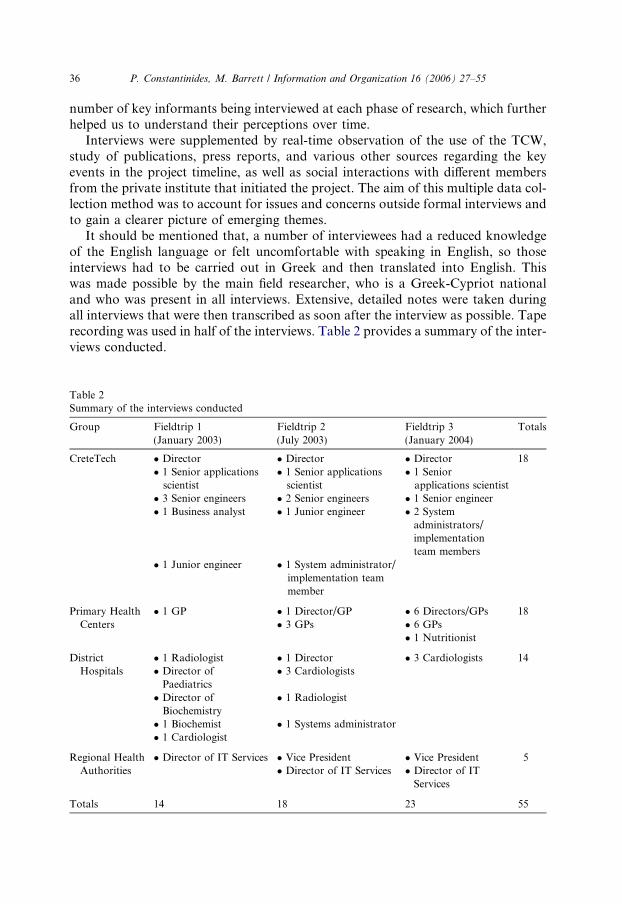
It should be mentioned that, a number of interviewees had a reduced knowledgeof the English language or felt uncomfortable with speaking in English, so thoseinterviews had to be carried out in Greek and then translated into English. Thiswas made possible by the main field researcher, who is a Greek-Cypriot nationaland who was present in all interviews. Extensive, detailed notes were taken duringall interviews that were then transcribed as soon after the interview as possible. Taperecording was used in half of the interviews. Table 2 provides a summary of the inter-views conducted.
Table 2Summary of the interviews conducted
Group Fieldtrip 1(January 2003)
Fieldtrip 2(July 2003)
Fieldtrip 3(January 2004)
Totals
CreteTech � Director � Director � Director 18� 1 Senior applicationsscientist
� 1 Senior applicationsscientist
� 1 Seniorapplications scientist
� 3 Senior engineers � 2 Senior engineers � 1 Senior engineer� 1 Business analyst � 1 Junior engineer � 2 System
administrators/implementationteam members
� 1 Junior engineer � 1 System administrator/implementation teammember
Primary HealthCenters
� 1 GP � 1 Director/GP � 6 Directors/GPs 18� 3 GPs � 6 GPs
� 1 Nutritionist
DistrictHospitals
� 1 Radiologist � 1 Director � 3 Cardiologists 14� Director ofPaediatrics
� 3 Cardiologists
� Director ofBiochemistry
� 1 Radiologist
� 1 Biochemist � 1 Systems administrator� 1 Cardiologist
Regional HealthAuthorities
� Director of IT Services � Vice President � Vice President 5� Director of IT Services � Director of IT
Services
Totals 14 18 23 55

P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 37
Data gathering and analysis was conducted in a process of continuous refinement,moving to different levels of abstraction from the field notes toward more generaltheoretical inferences. To accommodate this process, detailed case study write-ups,including interview transcripts and field notes, were prepared at the end of each field-trip (Eisenhardt, 1989), which were then discussed and analyzed in meetings betweenthe two researchers. In this sense, the conceptual foundations and research focusemerged and were adjusted through a continuous interaction with the data fromthe field. These adjustments allowed us to probe emergent themes while eliminatingbias towards preordained theoretical perspectives (Langley, 1999).
In this context, the data were first separated into three main groups in respect towhether they reflected statements or actions of the IT providers, the users, and keypolitical stakeholders. These data included interviews, as well as secondary historicaldata generated by each group focusing on key events and broad themes in the casestudy (Langley, 1999; Pettigrew, 1990). This step was followed by intra-group analysisfor similarities and/or differences on answers to particular issues. For example, all userswere asked to describe whether they found the technology to be useful in their workpractices and whether the introduction of new technology tried to introduce new prac-tices. Thirdly, inter-group analysis followed, which consisted of comparing the catego-ries generated by each group�s data to determine whether it reflected common themes(Eisenhardt, 1989; Langley, 1999). Having identified these themes, all field data werethen re-examined to determine whether the proposed set of themes and categories cov-ered as much of the data as possible. This iterative examination was aimed at generat-ing a final set of themes while recognizing the presence of multilayered and changingcontexts contributing to multiple levels of analysis (Langley, 1999).
Theoretical analysis proceeded within the conceptual foundations developed inSection 2 and according to key phases of continuity and change. In particular, inan attempt to follow the historicity of the interpretive chain in ICT developmentand use, the analysis focused on three key phases. The first phase involves the initia-tion and development of the technology as negotiated between an initial group ofindividuals. The second phase involves the implementation and initial use of the tech-nology, as negotiated between the IT providers, the group(s) of users and other par-ticipants. Finally, the third phase involves the efforts to scale-up the technology andthe implications such a scale-up (or collapse) might have on the different participants.
The decision to focus on these key phases is directly related to our commitment toprocess research, as well as an effort to identify and discuss key periods of continuityor change in the ICT project�s history (Pettigrew, 1990). Defining such periods ofcontinuity and change is neither new in the literature on organizational changeand development (e.g. Van de Ven & Poole, 1995) nor in the literature on ICT designand implementation (e.g. Cooper & Zmud, 1990). For example, Van de Ven andPoole (1995) provide an extensive analysis on different process models of organiza-tional change and development employed by researchers from diverse fields, whichinvolves an identification of key periods in an organization�s history. In this paper,the three key phases of initiation, implementation & use, and scale up, will be used asanalytical directions with which to examine emergent change or continuity duringthe focal ICT project. These phases are purely used as analytical reference points,
38 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
a structure for describing and analyzing the historicity of developments in the casestudy and not for defining a set of predictable events.
4. Case description
In this section, we will provide a brief description of the case study. Extensiveanalysis and discussion will follow in Sections 5 and 6.
4.1. Historical developments in the healthcare region of Crete
Crete is one of the 13 healthcare regions of Greece. After the foundation of the firstprimary healthcare centre in Greece in 1986 at the mountain village of Spili, as well asthe establishment of a University Hospital/Medical School in 1989 at Heraklion, Cretewas declared amodel region for healthcare services within theGreek national health sys-tem (NHS). Since then, the regional government has assigned high priority to further de-velop Crete as a model region for healthcare services, including science and technology.
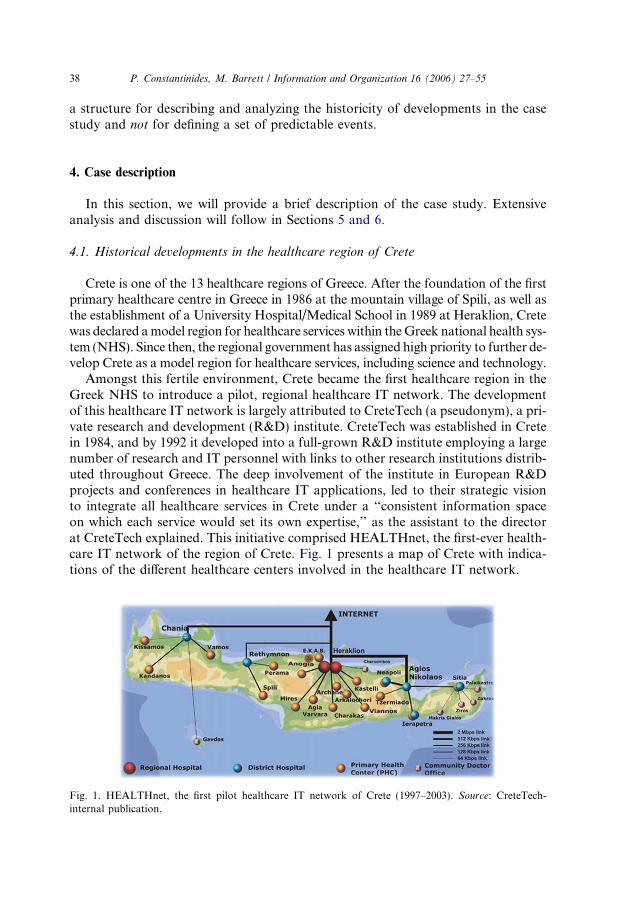
Amongst this fertile environment, Crete became the first healthcare region in theGreek NHS to introduce a pilot, regional healthcare IT network. The developmentof this healthcare IT network is largely attributed to CreteTech (a pseudonym), a pri-vate research and development (R&D) institute. CreteTech was established in Cretein 1984, and by 1992 it developed into a full-grown R&D institute employing a largenumber of research and IT personnel with links to other research institutions distrib-uted throughout Greece. The deep involvement of the institute in European R&Dprojects and conferences in healthcare IT applications, led to their strategic visionto integrate all healthcare services in Crete under a ‘‘consistent information spaceon which each service would set its own expertise,’’ as the assistant to the directorat CreteTech explained. This initiative comprised HEALTHnet, the first-ever health-care IT network of the region of Crete. Fig. 1 presents a map of Crete with indica-tions of the different healthcare centers involved in the healthcare IT network.
Fig. 1. HEALTHnet, the first pilot healthcare IT network of Crete (1997–2003). Source: CreteTech-internal publication.
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 39
4.2. Initiation and development of the TCW project
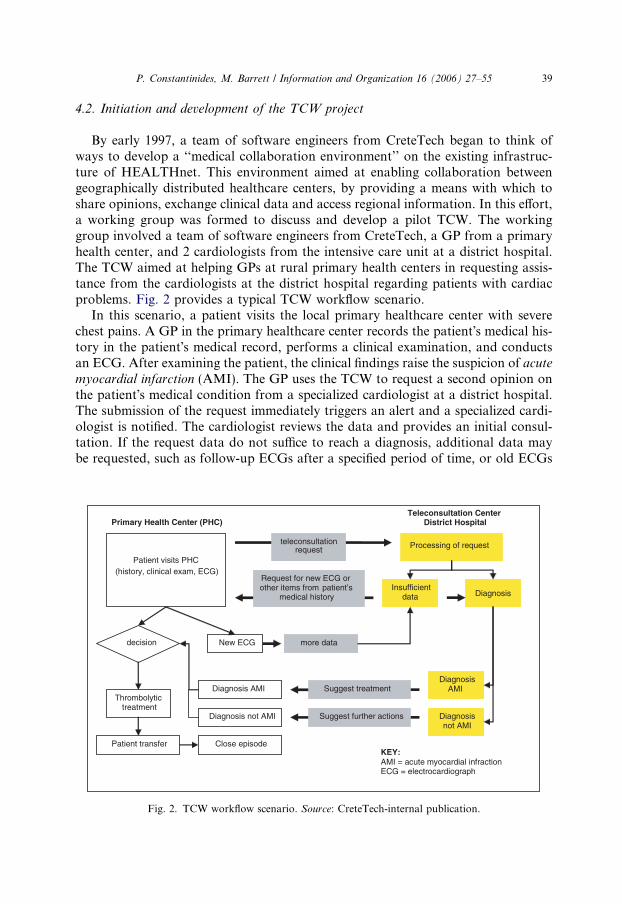
By early 1997, a team of software engineers from CreteTech began to think ofways to develop a ‘‘medical collaboration environment’’ on the existing infrastruc-ture of HEALTHnet. This environment aimed at enabling collaboration betweengeographically distributed healthcare centers, by providing a means with which toshare opinions, exchange clinical data and access regional information. In this effort,a working group was formed to discuss and develop a pilot TCW. The workinggroup involved a team of software engineers from CreteTech, a GP from a primaryhealth center, and 2 cardiologists from the intensive care unit at a district hospital.The TCW aimed at helping GPs at rural primary health centers in requesting assis-tance from the cardiologists at the district hospital regarding patients with cardiacproblems. Fig. 2 provides a typical TCW workflow scenario.
In this scenario, a patient visits the local primary healthcare center with severechest pains. A GP in the primary healthcare center records the patient�s medical his-tory in the patient�s medical record, performs a clinical examination, and conductsan ECG. After examining the patient, the clinical findings raise the suspicion of acutemyocardial infarction (AMI). The GP uses the TCW to request a second opinion onthe patient�s medical condition from a specialized cardiologist at a district hospital.The submission of the request immediately triggers an alert and a specialized cardi-ologist is notified. The cardiologist reviews the data and provides an initial consul-tation. If the request data do not suffice to reach a diagnosis, additional data maybe requested, such as follow-up ECGs after a specified period of time, or old ECGs
Patient visits PHC (history, clinical exam, ECG)
teleconsultation request
decision
Primary Health Center (PHC)Teleconsultation Center
District Hospital
Processing of request
Insufficient data
Request for new ECG or other items from patient’s
medical history Diagnosis
New ECG more data
Thrombolytic treatment
Patient transfer
Diagnosis AMI
Close episode
Diagnosis AMI
Diagnosisnot AMI
Suggest treatment
Diagnosis not AMI Suggest further actions
KEY: AMI = acute myocardial infraction ECG = electrocardiograph
Fig. 2. TCW workflow scenario. Source: CreteTech-internal publication.
40 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
of the same patient if available. Alternatively, if the patient is diagnosed with AMI, arecommendation that includes a prescription for thrombolysis treatment may be re-turned. If the patient is given thrombolytic therapy, the cardiologist may request tobe regularly updated on the condition of the patient so as to be alert for possiblearrhythmias. Alternatively, if the patient�s condition is diagnosed as critical the pa-tient is immediately transferred to the intensive care unit of the district hospital, atwhich point the teleconsultation session is closed and all data become part of the pa-tient�s electronic medical record.
Even though CreteTech had managed to secure the support of a team of health-care professionals, the institute still had to depend on its own resources for fundingthe development of the TCW. In fact, although, 25% of CreteTech�s regular budgetcomes from the government, 75% of that budget has to be earned ‘‘on a competitivebasis or from industry,’’ as explained by the director of CreteTech. At this point intime, however, the Greek Ministry of Health held an indifferent position to Crete-Tech�s vision for the region, primarily due to ‘‘strong affiliations’’ of ministerial offi-cers to GreekSoft (a pseudonym), a private group of software companies. This wasan explanation provided by interviewees at both CreteTech and the Regional HealthAuthorities. The ‘‘strong affiliations’’ of GreekSoft to the Ministry of Health were, atthe time, influencing the way in which funds were being allocated in the publichealthcare sector. However, by building on the motivational support of the RegionalSecretary and by securing funding in other R&D projects, CreteTech was able toproceed with its vision towards the implementation of the TCW.
4.3. Implementation and initial use of the TCW
In December 2000, the TCW was installed connecting a GP at a rural primaryhealthcare center with two cardiologists at the intensive care unit of a district hospi-tal. Some preliminary evaluations of the TCW conducted by this initial group ofusers in 2002 demonstrated significant financial benefits and improvements to thequality of care provided. In brief, the findings reported that over a 14-month period,teleconsultation was applied in 40 cases (23 men and 17 women) representing 10% ofthe total number of cardiac patients seen at the participating primary healthcare cen-tre. On average, the contacted cardiologist needed approximately 13 min for dataevaluation and diagnosis and proposed hospital referral for 19 patients (47.5%).Based on these findings, the report made the following claims: (a) the TCW canbe easily used by all involved physicians, (b) the TCW provides a short response timeappropriate for emergencies, (c) teleconsultation provides GPs with confidence intheir decision making, being at the same time an education tool, (d) unnecessarytransfers to the district hospital can be avoided, and finally, (e) there can be an a pri-ori knowledge of a pending emergency hospital admission.
4.4. Attempts to scale-up the TCW project
In early 2003, the TCW received an �honorable mention� for its ‘‘technologicallyadvanced design’’ at the European eHealth awards. The award was received by both
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 41
CreteTech and the district hospital that was the main supporter of the TCW. By late2003, in light of these developments, CreteTech and the participating district hospitalentered a negotiation process with the Ministry of Health towards securing the nec-essary financial support to develop a health telematics centre based on the TCWtechnology. This center would support teleconsultation services between the special-ized cardiologists at the district hospital and the GPs of six more primary healthcarecenters in the district of Heraklion, the capital of Crete.
Despite these positive developments, the fate of the TCW project was soon sub-jected to a number of inhibiting factors that eventually caused its collapse. These in-cluded issues of technology adoption including the relatively limited IT knowledgebase of the new group of users compared to that of the initial group of users, as wellas the limited amount of technical support provided by CreteTech due to insufficientfunds. In addition, a number of reforms introduced at the national level since 2000 –the last time new technologies were introduced in the region – also played a negativerole in the efforts to scale up the TCW project. Specifically, in late 2001, the new gov-ernment decentralized the Greek NHS by dividing it into 13 autonomous healthcareregions. In spite of the overall success of HEALTHnet and the TCW, the newlyestablished Regional Health Authorities of Crete had never been very enthusiasticabout CreteTech�s involvement in the region. This lack of enthusiasm is mostlyattributed to an intellectual property (IP) rights dispute between a GP and the direc-tor of CreteTech, which ensued after the former was promoted to a high position atthe newly established Regional Health Authorities. The IP rights dispute involvedthe development of electronic patient records in the region, which brought the oncecollaborating parties into conflict. To make things even worse, in 2003, a nationalinitiative urged all healthcare regions in Greece to declare their own regional IT com-petition. This initiative further alienated the relationship between CreteTech and theRegional Health Authorities and contributed to the collapse of the TCW project andthe broader HEALTHnet pilot.
5. Case analysis
In this section, we will draw on the conceptual foundations developed in Section 2to examine in more detail the negotiations behind the initial success and subsequentcollapse of the TCW project. Table 3 provides a summary of key themes in the TCWproject.
5.1. Initiation and development of the TCW project: Forming an initial community of
participants
Notwithstanding a number of political power relations that have long been foundto influence the allocation of funds in the public healthcare sector in Greece (Toun-tas, Karnaki, & Pavi, 2002), CreteTech�s senior management (led by the director ofthe institute) managed to gain the support of the Regional Secretary and a group ofkey healthcare professionals for initiating the TCW project. In fact, the choice of the
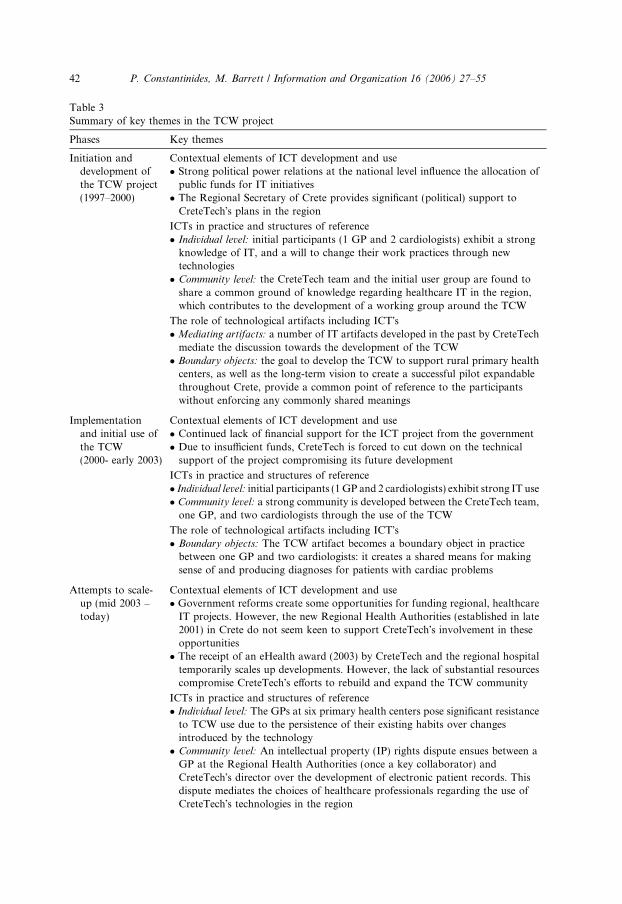
Table 3Summary of key themes in the TCW project
Phases Key themes
Initiation anddevelopment ofthe TCW project(1997–2000)
Contextual elements of ICT development and use� Strong political power relations at the national level influence the allocation ofpublic funds for IT initiatives
� The Regional Secretary of Crete provides significant (political) support toCreteTech�s plans in the region
ICTs in practice and structures of reference� Individual level: initial participants (1 GP and 2 cardiologists) exhibit a strongknowledge of IT, and a will to change their work practices through newtechnologies
� Community level: the CreteTech team and the initial user group are found toshare a common ground of knowledge regarding healthcare IT in the region,which contributes to the development of a working group around the TCW
The role of technological artifacts including ICT�s� Mediating artifacts: a number of IT artifacts developed in the past by CreteTechmediate the discussion towards the development of the TCW
� Boundary objects: the goal to develop the TCW to support rural primary healthcenters, as well as the long-term vision to create a successful pilot expandablethroughout Crete, provide a common point of reference to the participantswithout enforcing any commonly shared meanings
Implementationand initial use ofthe TCW(2000- early 2003)
Contextual elements of ICT development and use� Continued lack of financial support for the ICT project from the government� Due to insufficient funds, CreteTech is forced to cut down on the technicalsupport of the project compromising its future development
ICTs in practice and structures of reference� Individual level: initial participants (1GP and 2 cardiologists) exhibit strong IT use� Community level: a strong community is developed between the CreteTech team,one GP, and two cardiologists through the use of the TCW
The role of technological artifacts including ICT�s� Boundary objects: The TCW artifact becomes a boundary object in practicebetween one GP and two cardiologists: it creates a shared means for makingsense of and producing diagnoses for patients with cardiac problems
Attempts to scale-up (mid 2003 –today)
Contextual elements of ICT development and use� Government reforms create some opportunities for funding regional, healthcareIT projects. However, the new Regional Health Authorities (established in late2001) in Crete do not seem keen to support CreteTech�s involvement in theseopportunities
� The receipt of an eHealth award (2003) by CreteTech and the regional hospitaltemporarily scales up developments. However, the lack of substantial resourcescompromise CreteTech�s efforts to rebuild and expand the TCW community
ICTs in practice and structures of reference� Individual level: The GPs at six primary health centers pose significant resistanceto TCW use due to the persistence of their existing habits over changesintroduced by the technology
� Community level: An intellectual property (IP) rights dispute ensues between aGP at the Regional Health Authorities (once a key collaborator) andCreteTech�s director over the development of electronic patient records. Thisdispute mediates the choices of healthcare professionals regarding the use ofCreteTech�s technologies in the region
42 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
Table 3 (continued)
Phases Key themes
The role of technological artifacts including ICT�s� Mediating artifacts: Existing artifacts, such as paper-based records, are stronglyembedded in the work practices of the new group of users. This embeddednesscreates a lot of resistance to TCW-mediated change
� From boundary object to disputable artifact: The use of the TCW is challenged bythe series of government reforms as well as an IP rights dispute; the TCW isabandoned even by the initial group of users
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 43
initial TCW working group of healthcare professionals was not random. These indi-viduals – a GP at a rural primary health centre and two cardiologists at a districthospital – had been in close collaboration with CreteTech during the developmentof the pilot healthcare IT network throughout the 1990s, which had contributedto a level of trust between the two parties. Further, the intensive care unit at the dis-trict hospital has always stood as a highly respectable cardiology unit in the region ofCrete, something which was critical in securing collaboration between the two cardi-ologists and the GP at the rural primary health centre.
The strategy of selectively approaching key self-motivated healthcare profession-als was found to be highly effective in this first phase in the project since it graduallyled to the formation of an initial community around the TCW. This community wasformed between the director, his assistant, and a senior engineer from CreteTech, aGP at a rural primary healthcare centre, and two cardiologists at a major districthospital. These parties were brought together through (a) an immediate goal to de-velop a system that would provide medically standardized, telecardiology services torural primary healthcare centers, which are usually cut off from immediate medicalsupport; and (b) a common vision to develop a successful pilot with proven benefits,in order to expand the service throughout the whole region – providing an educationtool for GPs and eventually reimbursing the cardiologists for their services.
First, there was a common understanding that the TCW would provide substan-tial support to rural primary healthcare centres. The TCW system would provide ashared means for storing and accessing medically standardised patient data andinformation between rural primary healthcare centres and the participating hospital.The director of the intensive care unit (senior cardiologist) at the participating hos-pital reflected on this vision:
. . .we think that telemedicine is very important and in particular for telecardi-ology, but also for other aspects that would enable doctors and general prac-titioners to have specific advice for specific problems. . . we [also] think that bycollaborating with primary healthcare centres we provide more benefits to thepatients.
Having previously participated in the efforts to introduce HEALTHnet in the re-gion of Crete, this initial group of users saw the TCW as a means with which to fur-ther enhance collaboration between diverse regional centres. Thus, it can be saidthat, the existing base of ICT artifacts mediated the discussion around the develop-ment of the TCW and created possibilities for new goals (Latour, 1999). In a process

44 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
of continuous refinement of their knowledge and past experience on existing ICTartifacts, these key participants gradually realised that their efforts could be furtherenhanced through a common ‘‘medical collaboration workspace’’: the TCW. In thissense, the TCW stood as a boundary object (Star & Griesemer, 1989) between theCreteTech team and the participant group of healthcare professionals. Originatingfrom multiple and diverse communities, the TCW provided a shared means for sensemaking and negotiation between participants without enforcing common meanings.It is unclear whether the development of this boundary object was intentional. How-ever, it is clear that, CreteTech�s senior management�s intentional strategy was to ap-proach a more receptive group of participant healthcare professionals. Thus, it canbe argued that, in this initial conceptualization of the TCW, CreteTech�s senior man-agement was sensitive to the particular structures of reference of the participantgroup. This is not to say that the two groups shared a similar set of meanings,but rather that they shared a common ground of knowledge. This common ground�allowed� for the creation of the TCW as a boundary object, and contributed to theformation of an initial community of collaborators. This observation further sub-stantiates that the construction of boundary objects is highly relational to the partic-ular ground of knowledge of participating communities (Boland & Tenkasi, 1995).
Secondly, there was a common long-term vision to create a successful pilot withproven benefits, in order to attract the attention of more healthcare professionalsand to expand the service throughout the region. The agreement towards this com-mon vision between the group of participant healthcare professionals and the Crete-Tech team was attributed to a number of factors. First, there was a strong level ofcommitment between the involved parties due to their similar interests and intentionsin creating the TCW and becoming advocates of the use of technology in the region.Second, there was a level of trust between the participant healthcare professionalsthemselves due to personal relationships, as well as between the healthcare profes-sionals and the CreteTech team. The private institute had, by then, already shownsigns of strong R&D activities with active participation in European projects inthe field of healthcare services. The institute�s experience along with the fact thatits members are all locals with good familiarity of the cultural characteristics ofthe region contributed to them gaining membership to the community of participanthealthcare professionals. Again, as with the goal to develop the TCW, the long-termvision to expand the pilot throughout the region came about through the partici-pants� common ground of knowledge. Their common ground �allowed� the creationof this long-term regional vision as another boundary object that provided a com-mon reference for negotiation processes among the different participants.
In summary, in this first phase in the pilot project, there were a number of differ-ent bodies negotiating developments: the team at CreteTech, the indifferent GreekMinistry of Health, the supportive Regional Secretary, and the self-motivated groupof key healthcare professionals. The negotiations between these parties were shapedby a number of contextual elements such as the lack of financial support from thegovernment in contrast to the motivational support of the Regional Secretary to-wards the development of Crete as a model region, as well as the existing regionalbase of ICT artifacts developed in the past by the CreteTech team. The coherence
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 45
of these sets of negotiations depended on the extent to which the entrepreneurial ef-forts of each of the interested parties could coexist, whatever the nature of the pro-cesses that produced them (Star & Griesemer, 1989). In this first phase, it was thecommon long-term vision for Crete and the immediate goal to develop the TCWartifact that brought these diverse entrepreneurial efforts together and helped toovercome the indifference of the government while not enforcing any shared mean-ings among participants.
5.2. Implementation and initial use of the TCW artifact: Appropriating the technology
to existing work practices
In the initial implementation of the TCW in a district hospital and a primaryhealthcare center, the TCW had proved to be a boundary object in practice: it offereda shared means with which to make sense of and produce diagnoses for patients withcardiac problems. The participating GP explained:
In some conditions, I could have sent the patient to the hospital but I didn�t. . .if I have the notes of the cardiologist I can design a more appropriate therapyfor my patient, and so it�s safer. . . .I am not alone here. I have the cardiologistnear me.
In this sense, the TCW bridged existing work practices by expanding the means ofprior interaction and communication by allowing the exchange of medical data (e.g.electrocardiographs, X-rays) between the rural primary healthcare center and thedistrict hospital.
The initial group of users was not only quick to realize the potential of the tech-nology and employ it in their work practices, but to also become advocates of thetechnology in the region. This can be observed in the participation of this initialgroup of users in the production of some preliminary evaluations of the technology,which were presented in formal reports and medical conferences in the region. Infact, these preliminary evaluations had purposely scaled up some of the benefits ofthe TCW in an attempt to rationalize the need to integrate the TCW in regionalhealthcare practices, as well as to justify the need for financial support from the Re-gional Health Authorities and the Greek government. However, interviews with theusers had shed light on other issues not reported in the preliminary evaluations.These issues referred to some reservations about the added value of the TCW. A par-ticipating cardiologist, reflecting on different periods of use, explained:
At this stage, we check the system, as often as our hospital responsibilitiesallow us to. . . For example, now we have a very young boy with severe arrhyth-mia and the whole ICU is monitoring his condition. I wouldn�t even think ofchecking the system to see if there�s an unanswered request. . . it takes a fewdays before we find the time to answer back to the primary healthcare centre.. . .in the first stages of installation, CreteTech installed a system that wouldsend me a message on my mobile saying that a request was sent to me viathe teleconsultation system. But because of network problems and because
46 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
the requests weren�t as many at the time, this service was cancelled. . . So, thesystem, as it is now, is not very practical.
In this sense, not only did the use of the TCW appropriate the users� meaningsand intentions about the technology to emergent practices, but also the TCW artifacthad been transformed by the conventions of practice of collaborating communities.That is, unlike the first phase, after the implementation and initial use of the TCW,interpretations around the TCW had begun to differ, something that eventually gaverise to more expectations, reservations and somewhat disappointments around theuse of the technology. This unintentional mediation was primarily attributable toa lack of substantial resources including time and available cardiologists to respondto teleconsultation requests, as well as financial resources with which to providearound the clock technical support to the network. This observation resonates keyempirical research, which indicates that the evolution of new ICT is often subjectto unexpected and unintentional developments (Barrett & Walsham, 1999; Orlikow-ski, 2000). Still, this unintentional development was not far from the original strategybehind the project, which aimed at developing a pilot technology with the prospectof eventually transforming it into a ‘‘real service’’ that would be self-funded, as thedirector of CreteTech noted. A senior engineer at CreteTech reflecting on the broaderHEALTHnet project explained:
The overall effort was a pilot project that was developed and implemented, butunlike other government and private projects wasn�t expected to be used on aroutine basis. It was just there, ready for use for those who felt comfortableusing it. Doctors or other users weren�t obliged to use it; they could eitheruse it or not. Since we are not part of the Ministry of Health we don�t havethe authority to demand the use of the system and there wasn�t such an issueanyway since this was an R&D project.
In summary, in this phase in the project, there was strong evidence of use and anestablished community of participants around the TCW. However, the TCW stillhad to be subjected to the underlying structures of reference of the users, which in-volved their distinct set of work practices as well as their membership into multiplecommunities (e.g. in addition to being members of the community around the TCW,the two cardiologists were also members of the community of consultant physiciansat the district hospital who also had to attend to their own patients). Coupled withCreteTech�s lack of substantial �authority� to secure the necessary resources for theproject (e.g. mobile messaging support), the TCW�s initial success was seriouslychallenged.
5.3. Attempts to scale-up the TCW project: Conflict of interest and community
break-up
The receipt of an eHealth award, in early 2003, not only amplified the reputationcapital of CreteTech and the technology, but also attracted a lot of interest from dif-ferent stakeholders to transform the TCW pilot project into a round-the-clock ‘‘real
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 47
service’’. In an attempt to take full advantage of the opportunity, CreteTech decidednot to wait for the funding to be secured and to try to build commitment to technol-ogy use by installing the TCW at the six newly integrated primary healthcare centers,essentially providing early exposure to the technology. The assistant to the directorat CreteTech gave his thoughts on this strategy:
. . .a lot of things depend on the personal contact and being able to develop acommunity of users around a given concept. . . .at least in the beginning, youmake sure the system is utilized hoping that during that time they are moti-vated and convinced regarding the benefits of the system, because. . . [when]you introduce the system it�s not obvious to the doctors what the benefits are.
This comment was made clearer when we talked to the GPs at the six newly inte-grated primary healthcare centers. This new group of users did not exhibit the sameenthusiasm around the use of the TCW as the initial user group, because of theirinherent, unique structures of reference. For example, a GP belonging to the newgroup of users explained:
We are part of a generation that is not very familiar with computers. . . For tel-ematics applications to solve my problems a lot of years will have to passbefore I become skilful and fast enough to use the system as it should beused. . . if I have an emergency here, there�s no way I will use the telematics sys-tem, because it will be too slow of a response. . . Doctors are not used to typingon the computer. . . .This cannot be done; it�s too laborious.
This response is representative of these GPs� limited knowledge and experience ofIT systems in comparison to the initial group of users. Moreover, unlike the initialgroup of users, these GPs had appeared to be more loyal to the strategic intentionsof the newly established Regional Health Authorities, which were in conflict with theintentions of CreteTech�s senior management. The head of the IT implementationteam at CreteTech, who had spent a lot of time with a number of GPs at differentprimary healthcare centers during the HEALTHnet and TCW projects gave his viewon the increasing �silent opposition� against CreteTech�s involvement in the region:
. . .lately the relationship between the Regional Health Authorities and Crete-Tech has not been the best. . . although we have installed the technology insix more primary health centers, due to the change of politics, most of thesecenters find it very hard to go against the will of the Regional Health Author-ities, because they simply depend on them. . . they [the Regional HealthAuthorities] are basically encouraging them not to use our system because soonthey will declare their regional IT competition and they strongly believe that adifferent vendor will win and offer a new system. The fact is that right nowthere is a lot of resistance from the primary healthcare centers.
In addition, influenced by the negative stance of other healthcare professionals toCreteTech�s technology, the initial group of users had also developed reservations asto the role of the TCW in practice, gradually distancing themselves from using thetechnology. These reservations were attributed to a number of contextual elements,
48 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
such as an IP rights dispute between CreteTech and the Regional Health Authoritiesover the development of electronic patient records; a lack of support (financial orotherwise) to CreteTech�s IT initiatives in the region by the Greek Ministry ofHealth, which restricted CreteTech�s efforts to expand training support around theTCW; and the announcement of healthcare reforms involving government-led IT ini-tiatives and cornering the TCW project. Although the director of CreteTech in-formed us that the private institute will be bidding at the regional IT competitionin Crete and may gain the opportunity to scale-up both the broader HEALTHnetproject and the TCW technology, based on discussions with the Regional HealthAuthorities, this looks like a distant possibility. The director of IT services at the Re-gional Health Authorities reflected on the situation:
They [CreteTech] have done extensive work on HL7 standards, which is a veryimportant aspect of the evaluation process.. . .[however] a lot of the things thatCreteTech introduced in their systems do not correspond to the actual needs ofthe users and so the users don�t use them because they don�t find the systemsvery useful. Second, CreteTech never had the necessary authority or powerto enforce the use of its systems. . . all CreteTech could do was to ask the userswhether they wanted free computers and free systems, but could never askthem to start using it on a regular basis, and so at some point when the usersdecided not to use the systems installed, the whole project went bust. . . it�s ablessing, after all, that CreteTech�s efforts did not evolve to the extent theywanted because we would then have to tie our hopes to CreteTech�s chariot.
In summary, the TCW project suffered an uneven development due to a numberof contextual elements such as a series of political reforms contributing to insufficientresources and power conflicts, as well as differences between distinct structures of ref-erence, including diverse meanings around the role of the TCW between the initialgroup of users and other groups of GPs, and diverse (and opposing) intentionsaround the development of electronic patient records between CreteTech and the Re-gional Health Authorities. In addition, the development and use of the TCW alsoinvolved a number of artifacts that had a distinct role to play in negotiation pro-cesses between different parties including the existing base of medical and IT artifactsand the TCW itself. These negotiations are now explored in more depth.
6. Discussion
In this section we will further elaborate on the findings from the case study. Thediscussion will be structured in relation to the three conceptual elements developed inSection 2, namely, contextual elements of ICT development and use, ICTs in practiceand structures of reference, and the role of technological artifacts in negotiation pro-cesses. Although presented independently to give depth to the discussion, the threesubsections that follow are closely interrelated – as is the relationship between thethree elements of our conceptual foundations – and together aim to contribute toa richer understanding of negotiation processes in ICT development and use.

P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 49
6.1. Contextual elements of ICT development and use: Negotiations of power and
politics
We start the discussion by looking at contextual elements of ICT developmentand use with a particular focus on negotiations of power and politics. As Walsham(2001, p. 56) notes, ‘‘it is of fundamental importance to analyze such issues, whichcan be considered to underlie all individual, organizational and societal practices,since power is endemic to all human activities.’’ In agreement with Walsham(2001), power is hereby conceived as manifested in shifting relationships with otherswhile gaining access to different resources. In consequence, politics is viewed as at-tempts to use such resources as knowledge, funds, the existing technological base,and time availability, to achieve particular ends. In short, power and politics are un-ique but intimately interdependent in an ongoing cycle of negotiation: people em-ploy politics (attempts to use different resources) to gain power, but withoutpower (establishment of strong relationships) they cannot gain access to the neces-sary resources.
Issues of power and politics have been a common theme in the literature on ITimplementation in healthcare organizations. For example, in an extensive reviewof the literature on IT implementation in healthcare organizations, Berg (2001) citesa number of examples of failed implementations due to resistance to power, includ-ing incompatibility between the designers� inscriptions in system processes and theusers� working routines, as well as conflicts of interest among diverse groups ofhealthcare professionals as to the role of IT in their work contexts. Similar findingshave been reported elsewhere (e.g. Bloomfield, Coombs, Cooper, & Rea, 1992).
Evidence of such negotiations of power and politics are supported in findingsfrom the case study, where collaborative efforts towards the development anduse of the TCW were seriously compromised by ongoing negotiations to protectthe interests of dominant groups. Specifically, although initially a key collaboratorof CreteTech during the HEALTHnet project, a GP later questioned the involve-ment of CreteTech in the development of electronic patient records in the publicsector once he had been appointed to a high position in the newly establishedRegional Health Authorities. The IP rights dispute that ensued between the GPand the director of CreteTech contributed to the uncertainty of the pilot natureof the TCW and to the resistance posed by different healthcare professionals inthe region. Further, challenged by the continuous lack of financial support fromthe government leading to a lack of adequate technical support of the TCW, Crete-Tech had no power or �authority� to gain the commitment of the majority ofhealthcare professionals in the region. In turn, this lack of adequate resourcesmeant that healthcare professionals had no incentives to �make time� to use Crete-Tech�s technologies. Even the strong collaborators of the project (e.g. the initialgroup of TCW users and co-receivers of the eHealth award) soon became unableto salvage the use of the TCW from these cascading events. The collapse of thepilot was primarily attributed to negotiations of power between key political stake-holders in the region and the implications those negotiations had to gaining accessto necessary resources.

50 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
6.2. ICTs in practice and structures of reference: Negotiating meanings around
ICT-mediated change
There have been many studies in the literature on IT implementation in healthcareservices with an emphasis on the relationship between existing work practices andresistance to ICT-mediated change. For example, the UK NHS has suffered a seriesof high-profile IT failures, including the Wessex Health Authority Regional Infor-mation Systems Plan, which was abandoned after six years of infertile efforts andmore than £20 million spent, and the London Ambulance Service Computer AidedDispatch project, which was scrapped within 48 h of going live (Jeffcott & Johnson,2002; Jones, 2003). Although there were multiple issues involved, one of the mainreasons behind all of these IT failures was the damaging effect of new ICT-mediatedchange on the existing work environments in which they were introduced (Jeffcott &Johnson, 2002). Similar findings have also been reported in studies in the US health-care sector, where physicians are often ‘‘reticent to leave the familiar paper chart’’due to their unfamiliarity with computer systems, which also contributes to theirtechnophobia that the information collected could be used to critique their perfor-mance and the outcomes of their patients (Treister, 1998, p. 21). As a result, ‘‘phy-sicians are reluctant to change traditional long-standing practice patterns’’ refrainingfrom any IT use altogether (Anderson, 1997, p. 84).
Evidence of the relationship between existing work practices and resistance toICT-mediated change is also found in the Crete case study. For example, althoughthe initial group of users exhibited strong knowledge and experience of ICT, themajority of potential users (GPs at six primary healthcare centers) resisted Crete-Tech�s technologies. Their resistance can be attributed to the fact that the newtechnologies challenged their structures of reference, including both their knowl-edge of ICT and their existing work practices. Even the group of healthcare pro-fessionals using the TCW, who exhibited a relatively quick adoption of technologyin their work practices, were later found to have reservations as to the practicalityof the system in their work practices. These instances of non-use of ICT link to thefact that actions (including the action of interpretation) towards a shared realitycan only take place against a ground of common knowledge and practices. Inthe absence of a common ground the possibility of resistance and diversificationbecomes stronger. Of course, there was no possible way that every healthcare pro-fessional in the region could share the same knowledge of IT as some of the moreadvanced users. Nor was it simple and easy to turn a pilot project into a real-timeregional network with the endowment of the government. Such collective effortsrequired the formation of collaborating communities, which is often directly impli-cated in the development and sustainability of power relationships. For example,as discussed earlier, by succumbing to an IP rights dispute, CreteTech lost a keypolitical relationship and the chance of gaining enough �authority� to help buildand expand the initial community of participants throughout the region. Certainly,power relationships are not the sole reason for building commitment among di-verse groups. The relationship between new technologies and the individual cul-tures of the different user groups is equally important for building commitment
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 51
to IT use. As the responses of participant healthcare professionals suggest, thetechnology did not correspond to their structures of reference and especially tothe medical practice of responding quickly to critically ill patients. For example,when asked to explain why the TCW was not used by the GPs in his primaryhealthcare centre, a GP categorically stated that the technology ‘‘will be too slowof a response for emergency situations’’ and therefore there is no point of using it.This example stresses the fact that participants� structures of reference (includingtheir knowledge of ICT and their existing work practices) may equally contributeto resistance to ICT-mediated change as power relationships. Initiating possibilitiesfor change must, therefore, involve an understanding of both the structures of ref-erence of participants (cf. Heracleous & Barrett, 2001), as well as the power rela-tionships between them.
6.3. The role of technological artifacts including ICT�s in negotiation processes
The third and final focus of discussion refers to the role of technological arti-facts in processes of negotiation around ICT development and use. First, regard-ing the mediating role of technological artifacts (Latour, 1999), in the Crete casestudy, the TCW was found to combine the efforts of the GP and the cardio-logists towards the production of diagnoses at the primary care level and theminimization of patient admission at the hospital level. In addition, the TCWwas also found to delegate each of the users� individual actions: it carried theGP�s request to the cardiologist and the latter�s response back to the GP,whereas this was once done through paper orders in an ambulance or throughthe telephone. Furthermore, electronic patient records were found to displace
the goals of both CreteTech and the Regional Health Authorities, by becomingan artifact of intense conflict between the two parties. Second, a number ofboundary objects were found to be negotiated in the Crete case study, eventhough it is unclear whether they were intentionally created or not. However,the succession through the different phases in the pilot project seemed to involveobjects, which originated and, for some time period, continued to inhabit multi-ple communities. These boundary objects included a long-term vision to createsuccessful pilots expandable throughout Crete and the TCW artifact itself, whichaimed to provide medically standardized, telecardiology services to rural primaryhealthcare centers. These boundary objects offered a shared means for actingupon, at least for some time period, for some groups and individuals; they of-fered a modus operandi for negotiation without enforcing commonly sharedmeanings (cf. Bowker & Star, 1999; Star & Griesemer, 1989). However, as withany object, the status of these boundary objects did not remain static for toolong. In fact, as negotiations progressed in the project, these objects were trans-formed from a center of collaborative work to a center of intense conflict (cf.Boland & Tenkasi, 1995). Reaching a more complete view of ICT developmentand use may, thus, involve an understanding of the structures of reference ofparticipants, the power relationships between them, as well as the role of differ-ent technological artifacts in the process.
52 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
7. Conclusion
In this paper, we have examined the development and use of a healthcare-relatedICT in the region of Crete, Greece. As evident from the analysis and discussion ofthe case study, the ICT project was negotiated at multiple levels and points in timeemerging through a complex network of socio-technical interactions. At each leveland point in time, different groups and individuals enacted their distinct structuresof reference and shaped the development and use of the focal ICT in relation to tech-nological choices offered to them and within the constraints of their social and workcontext. For example, the initial group of participants (i.e. 1 GP, 2 cardiologists, andthe CreteTech team) enacted (and shared) their knowledge and interests in the tech-nology, which enabled them to construct the focal ICT as a boundary object. In turn,this boundary object offered the initial group of participants flexibility of interpreta-tion, thus enabling enactments of work practices that satisfied individual meaningsand intentions (structures of reference) while serving as a tool in negotiations. Onthe other hand, however, other groups of healthcare professionals did not shareany of the interests and knowledge of the initial group of participants in the projectand enacted their own (opposing) structures of reference, believing that the focal ICTdisrupted their existing work practices. Further, grasping the opportunity offered bypolitical reforms at the national level, a once key collaborator in the project em-ployed politics (efforts towards the accumulation of different resources) and man-aged to build further resistance against the focal ICT, with the role of thetechnology shifting from a boundary object to an object of intense dispute.
A key theoretical implication is that the development and use of ICT do not ema-nate solely through the intentions of a select few individuals (e.g. the designers or se-nior management), but through an ongoing process of negotiation between multipleactors and their technological choices within their changing work and social con-texts. Greater emphasis should, therefore, be placed on gaining an understandingof how the process of ICT development and use is shaped and configured at differentlevels over time.
Conceptualizing ICT development and use as an ecological process where diverse(and often contradicting) outcomes are simultaneously being negotiated at differentlevels and points in time has implications for addressing issues of collaboration andresistance (and subsequently of change vs. continuity). Certainly, as evident from theanalysis of the case study, the formation of communities of collaborators around agiven ICT project is no simple task; communities may be initially formed but sustain-ing participation among community members and resolving potential conflicts be-tween them cannot be controlled. The same individuals may be members ofmultiple communities simultaneously and membership to any of these communitiesis constantly being negotiated within the changing strength of emergent socio-tech-nical relations. It is in the shifting strength of these socio-technical relations that weshould seek to understand issues of collaboration and resistance. Our researchshould be concerned with the processes by which different groups of participantscoordinate their efforts, including the ways in which they attempt to mobilize (spreadand extend) their structures of reference and technological choices in opposition to
P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 53
other groups, as well as the ways in which they may choose to collaborate withoutany agreement, often within the constraints of their social and work context.
With this conclusion, we challenge research that tends to pay attention to individ-ual events but fails to consider the ongoing process of ICT development and use; re-search that employs a single level of analysis but fails to consider multiple levels orviews of the process; and research that fails to account for the changing socio-tech-nical context in which the given ICT project unfolds including the changing relation-ship between people and their technological choices. The importance of theseepistemological choices suggests the need to recognize that all ICTs are necessarilysuffused with socio-political negotiations and modulated by socio-technical relation-ships. ICTs are active participants in the changes that they help bring about, as wellas simulators of existing practices and relationships. Keeping this in mind, we keepopen and can explore spaces of change and continuity that are otherwise lost (Bow-ker & Star, 1999).
Acknowledgments
We are grateful to the Cambridge-MIT Institute for their financial support inmaking this research project a reality. We would also like to thank CreteTech forgranting us access to the site as well as for their invaluable insights in helping usto understand strategic issues around the development of a telecardiology systemin Crete. Finally, we would like to thank all those who have accepted a requestfor an interview, whose responses have provided many insights to the objectives ofthis study and have helped prepare the ground for further research.
References
Anderson, J. G. (1997). Clearing the way for physicians� use of clinical information systems.Communications of the ACM, 40(8), 83–90.
Barrett, M., & Walsham, G. (1999). Electronic trading and work transformation in the London insurancemarket. Information Systems Research, 10(1), 1–22.
Berg, M. (2001). Implementing information systems in health care organisations: Myths and challenges.International Journal of Medical Informatics, 64, 143–156.
Bloomfield, B. P., Coombs, R., Cooper, D. J., & Rea, D. (1992). Machines and manoeuvres:Responsibility accounting and the construction of hospital information systems. Accounting,
Management & Information Technology, 2(4), 197–219.Boland, R. J., & Tenkasi, R. V. (1995). Perspective making and perspective taking in communities of
knowing. Organization Science, 6(4), 350–372.Boudreau, M.-C., & Robey, D. (2005). Enacting integrated information technology: A human agency
perspective. Organization Science, 16(1), 3–18.Bowker, G., & Star, S. L. (1999). Sorting things out – classification and its consequences. Cambridge, MA:
MIT Press.Collins, H. M., & Kusch, M. (1998). The shape of actions: What humans and machines can do. Cambridge,
MA: MIT Press.Cooper, R. B., & Zmud, R. W. (1990). Information technology implementation research: A technological
diffusion approach. Management Science, 36(2), 123–139.
54 P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55
Eisenhardt, K. M. (1989). Building theories from case study research. Academy of Management Review,
14(4), 532–550.Giddens, A. (1984). The constitution of society. Cambridge: Polity Press.Hanseth, O., & Monteiro, E. (1997). Inscribing behaviour in information infrastructure standards.
Accounting, Management and Information Technology, 7(4), 183–211.Heracleous, L., & Barrett, M. (2001). Organisational change as discourse: Communicative actions and
deep structures in the context of information technology implementation. Academy of Management
Journal, 44(4), 755–778.Jeffcott, M. A., & Johnson, C. W. (2002). The use of a formalised risk model in NHS information system
development. Cognition, Technology & Work, 4(2), 120–136.Jones, M. (1998). Information systems and the double mangle: Steering a course between the Scylla of
embedded structure and the Charybdis of strong symmetry. In T. Larsen, L. Levine, J.I. DeGross,(eds.) Information systems: Current issues and future challenges: Proceedings of the IFIP WG8.2 and 8.6
Joint Working Conference, Helsinki, pp. 287–302.Jones, M. R. (2003). ‘‘Computers can land people on Mars, why can�t they get them to work in a
hospital?’’ Implementation of an electronic patient record system in a UK hospital. Methods of
Information in Medicine, 42, 410–415.Klein, H., & Myers, M. (1999). A set of principles for conducting and evaluating interpretive field studies
in information systems. MIS Quarterly, 27(1), 67–88.Langley, A. (1999). Strategies for theorizing from process data. Academy of Management Review, 24(4),
691–710.Latour, B. (1991). Technology is society made durable. In J. Law (Ed.), A sociology of monsters: Essays on
power, technology & domination (pp. 103–131). London: Routledge Press.Latour, B. (1999). Pandora�s hope: Essays on the reality of science studies. Cambridge: Harvard University
Press.Martin, J. (1992). Cultures in organisation: Three perspectives. Oxford: Oxford University Press.Monteiro, E. (1998). Scaling information infrastructure: The case of the next generation IP in Internet.
Information Society, 14(3), 229–245.Newman, M., & Robey, D. (1992). A social process model of user–analyst relationships. MIS Quarterly,
16(2), 249–265.Orlikowski, W. J. (2000). Using technology and constituting structures: A practice lens for studying
technology in organizations. Organization Science, 11(4), 404–428.Orlikowski, W. J., & Iacono, S. (2001). Desperately seeking the �IT� in IT research: A call to theorizing the
IT artifact. Information Systems Research, 12(2), 121–134.Orlikowski, W. J., & Robey, D. (1991). Information technology and the structuring of organizations.
Information Systems Research, 2(2), 143–169.Pettigrew, A. M. (1985). The awakening giant: Continuity and change in imperial chemical industries.
Oxford: Blackwell Press.Pettigrew, A. M. (1990). Longitudinal field research on change: Theory and practice. Organization Science,
1(3), 267–292.Pickering, A. (1993). The mangle of practice: Agency and emergency in the sociology. American Journal of
Sociology, 99(3), 559–589.Robey, D., & Boudreau, M.-C. (1999). Accounting for the contradictory organizational consequences of
information technology: Theoretical directions and methodological implications. Information Systems
Research, 10(2), 167–185.Sabherwal, R., & Newman, M. (2003). Persistence and change in system development: A dialectical view.
Journal of Information Technology, 18(2), 69–92.Star, S. L. (1991). Power, technologies and the phenomenology of conventions: On being allergic to
onions. In J. Law (Ed.), A sociology of monsters: Essays on power, technology & domination (pp.103–131). London: Routledge Press.
Star, S. L., & Griesemer, J. R. (1989). Institutional ecology, �translations� and boundary objects: Amateursand professionals in Berkeley�s museum of vertebrate zoology, 1907–39. Social Studies of Science,
19(3), 387–420.

P. Constantinides, M. Barrett / Information and Organization 16 (2006) 27–55 55
Star, S. L., & Ruhleder, K. (1996). Steps toward an ecology of infrastructure: Design and access for largeinformation spaces. Information Systems Research, 7(1), 111–134.
Tountas, Y., Karnaki, P., & Pavi, E. (2002). Reforming the reform: The Greek national health system intrasition. Health Policy, 62, 15–29.
Treister, N. W. (1998). Physician acceptance of new medical information systems: The field of dreams.Physician Executive, 24(3), 20–25.
Van de Ven, A. H., & Poole, M. S. (1995). Explaining development and change in organizations. Academy
of Management Review, 20(3), 510–540.Walsham, G. (1993). Interpreting information systems in organizations. New York: Wiley.Walsham, G. (1995). Interpretive case studies in IS research: Nature and method. European Journal of
Information Systems, 4(2), 74–81.Walsham, G. (2001). Making a world of difference: IT in a global context. Chichester: Wiley.Woolgar, S. (1991). The turn to technology in social studies of science. Science, Technology & Human
Values, 16(1), 20–50.