nausea & vomiting in pregnancy / hyperemesis gravidarum
TRANSCRIPT

Nausea & Vomiting in Pregnancy /
Hyperemesis Gravidarum
Professor Cathy Nelson-Piercy
Consultant Obstetric Physician
KCL Division of Women’s Health

Nausea & Vomiting in Pregnancy (NVP)
• Affects 50-85% of pregnancies1.
• Symptoms usually start between 6-8 weeks of gestation
• Rise to a peak before the end of the first trimester, and in the majority of
women, resolve by 20 weeks2.
• Most women (65-70%) do not seek medical advice but attempt to manage
their symptoms with avoidance of dietary triggers and oral hydration2.
1. Niebyl JR. Clinical practice. Nausea and vomiting in pregnancy. N Engl J Med. Oct 14
2010;363(16):1544-1550.
2. Jarvis S, Nelson-Piercy C. Management of nausea and vomiting in pregnancy. BMJ. 2011;342:d3606.
1

Hyperemesis Gravidarum (HG)
• 0.3-1% of pregnancies1
• Peak occurrence 8-12 weeks gestation
• Severe end of NVP spectrum2
• intractable nausea, vomiting, dehydration
• ketosis, electrolyte imbalance
• weight loss (> 5% of body weight)
1. Niebyl JR. Clinical practice. Nausea and vomiting in pregnancy. N Engl J
Med. Oct 14 2010;363(16):1544-1550.
2. Jarvis S, Nelson-Piercy C. Management of nausea and vomiting in
pregnancy. BMJ. 2011;342:d3606.

Page 3
Nausea Vomiting in pregnancy: prevalence 80%
Hyperemesis gravidarum: prevalence 1.5%
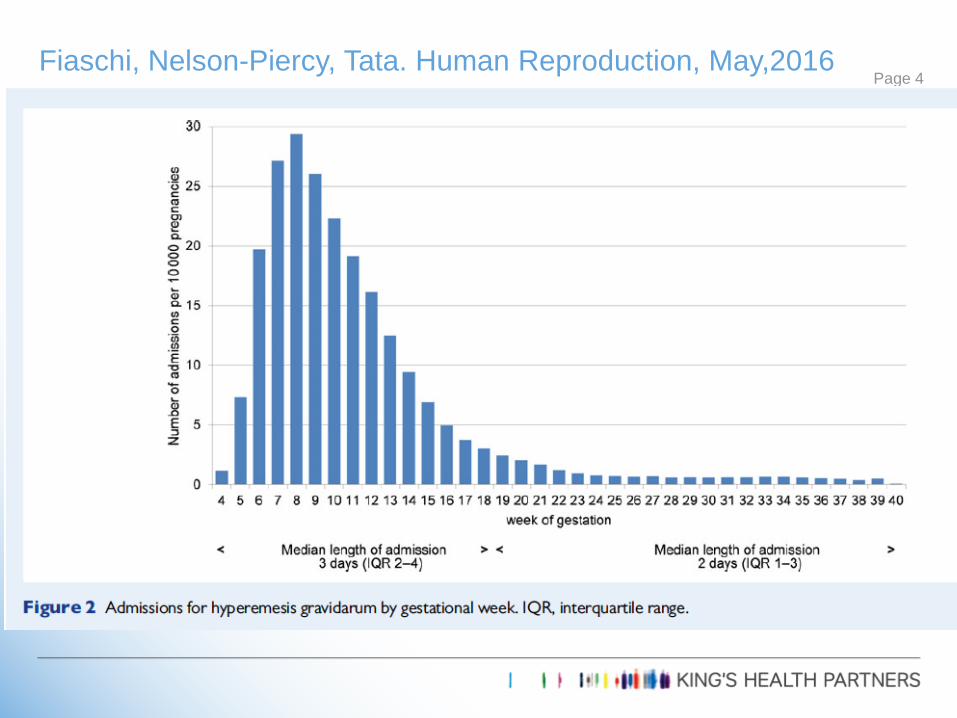
Fiaschi, Nelson-Piercy, Tata. Human Reproduction, May,2016Page 4

Page 5

HG admission and readmission (surrogate for severity) higher risk if :
• younger (<30)
• more socioeconomically deprived status
• Asian or Black ethnicity,
• carrying a female fetus
• multiple pregnancy
Page 6Fiaschi, Nelson-Piercy, Tata. Human Reproduction, May,2016

Comorbidities most strongly associated with HG were:
• parathyroid dysfunction (aOR 3.83, 95% CI 2.28–6.44),
• Hypercholesterolemia (aOR 2.54, 1.88–3.44),
• Type 1 diabetes (aOR 1.95, 1.82–2.09),
• thyroid dysfunction (aOR 1.85, 1.74–1.96).
History of HG was the strongest independent risk factor (aOR . 4.74, 4.46–5.05).
Women with higher parity had a lower risk of HG compared with
nulliparous women (aOR . 0.90, 0.89–0.91), which was not explained by
women with HG curtailing further pregnancies
Page 7Fiaschi, Nelson-Piercy, Tata. Human Reproduction, May,2016

Clinical Features
Nausea
Vomiting
Ptyalism
Dehydration
Weight Loss
Protein-calorie
malnutrition
Ketonuria
Hyponatraemia
Hypokalaemia
Low urea
Hypochloraemic alkylosis
Vitamin deficiency

Pathophysiology
• Genetic
• Increased risk in daughters of sufferers1
• Endocrine
• Higher levels of human chorionic gonadotrophin, (hCG) have been associated
with more severe forms of NVP/HG2
• Gastrointestinal factors
• Delayed gastric emptying
• H pylori infection3
1. Vikanes AV, et al. Recurrence of hyperemesis gravidarum across generations: population based cohort
study. BMJ. 2010;340(c2050).
2. Derbent AU, et al. First trimester maternal serum PAPP-A and free beta-HCG levels in hyperemesis
gravidarum. Prenatal Diagnosis. 2011;31:450-453.
3. Sandven I, et al. Helicobacter pylori infection and hyperemesis gravidarum: a systematic review and
meta-analysis of case-control studies. Acta Obstet Gynecol Scand. 2009;88 :1190-1200.
9

Diagnosis
• Likely if previous history of HG
• Higher risk in the second pregnancy of women with a previous history of
HG1
• Unlikely if onset after 10-12 weeks
1. Trogstad LIS, et al. Recurrence risk in hyperemesis gravidarum. BJOG 2005;112:1641-
1645.

Diagnosis of exclusion
• Infection eg. UTI
• Endocrine eg.
• Addison’s
• Thyrotoxicosis
• Hypercalcaemia
• Pancreatitis, Cholecystitis
• Peptic ulceration, gastritis
• ENT eg. labyrinthitis
• Drugs eg. iron

NVP: Potential risks
• emotional and psychological distress1,2
• reduced quality of life1,2
1. Mazzotta P, Maltepe C, Navioz Y, Magee LA, Koren G. Attitudes, management and
consequences of nausea and vomiting of pregnancy in the United States and Canada. Int
J Gynaecol Obstet. Sep 2000;70(3):359-365.
2. Smith C, Crowther C, Beilby J, Dandeaux J. The impact of nausea and vomiting on
women: a burden of early pregnancy. Aust N Z J Obstet Gynaecol. 2000;40:397-401.
12

HG: Potential Risks
Maternal
Dehydration / Malnutrition / Metabolic
Wernicke’s encephalopathy
Central Pontine Myelinolysis
Psychiatric
Venous thrombosis
Fetal
FGR
Preterm delivery
IUD

Psychological factors
• Anxiety and depression present in 57% (consequence)
• Affected women do not have antecedent psychological illness and do not
take up offer of a psychiatry appointment for assessment.
• Women with HG consider HG to have a biologic basis.
• Psychological consequences can be profound
• No quality data to support a primary psychological basis for HG.
Tan & Omar. Current Opinion in Obstetrics and Gynecology 2011, 23:87–93
Qualitative research
Highlights debilitating effects and burden of HG on patients and lack of
appreciation and interest by care providers as perceived by patients.
• Patients felt unpopular with healthcare professionals who may be
skeptical about symptom severity.
• Women left with perception they are time wasters or somebody else’s
responsibility.
• For women most severely affected, it appears that primary care support
is often lacking.
Power Z, Thomson AM, Waterman H. Understanding the stigma of
hyperemesis gravidarum: qualitative findings from an action research study.
Birth 2010; 37:237–244.

Validated measures of severity
• The Rhodes Index
• Pregnancy-Unique Quantification of Emesis/Nausea (PUQE) index.
• 3 questions, correlate with Rhodes
• Moderate – severe NVP = PUQE ≥ 7

PUQE: Validated Scoring System for NVP
Question Point Value Enter
1) In the last 24 hours for how long
have you felt nauseated or sick
to your stomach?
Not at all
(1)
1 hour or
less
(2)
2-3 hours
(3)
4-6 hours
(4)
More
than 6
hour
(5)
2) In the last 24 hours have you
vomited or thrown up?
7 or more
times
(5)
5-6
times
(4)
3-4
times
(3)
1-2
times
(2)
I did not
throw up
(1)
3) In the last 24 hours how many
times have you had retching or
dry heaves without bringing
anything up?
No time
(1)
1-2 times
(2)
3-4
times
(3)
5-6
times
(4)
7 or more
times
(5)
Sum point values for the 3 questions to find the PUQE Score PUQE Score
PUQE-24 Score ≤6 7-12 13-15
NVP Severity Mild Moderate Severe



Hospital Management
• Intravenous fluid and electrolytes
• Emotional support
• Nutritional support - Thiamine
• Antiemetic therapy
• Thromboprophylaxis

Intravenous fluids – in-patients
N Saline
KCL
Hartmanns/plasmalyte
Dextrose Saline
5% Dextrose
2 N Saline
1/5 N Saline
N Saline 1 litre + 40 mmol KCL – 3 litres /day
Check U + E daily

Problems with In-patient Mx
Costly
Disruptive to patient / work / family life
Problems with gynae elective beds
Pressures on length of stay result in premature discharge and recurrent admissions

Page 25

Page 26

Page 27

Safety Data
Cochrane review
Systematic review and metaanalyses1,2
Registry data
Sweden3
metoclopramide, (884)
prochlorperazine (145)
promethazine (4740)
cyclizine (1221)
Danish4
Ondansetron (2000)
1. Magee LA, Mazzotta P, Koren G. Am J Obst Gyn 2002;186(5 Suppl 2):S256–61.
2. Gill & Einarson. Expert Opin Drug Safety 2007; 6:685-694
3. Asker et al. Eur J Clin Pharmacol 2005; 61: 899-906
4. NEJM 2013; 368:814-23.

• Review by the European Medicines Agency’s Committee for Medicinal
Products for Human Use, confirmed risks of short-term extrapyramidal
disorders and tardive dyskinesia, particularly in young people.
• should only be prescribed for short-term use (maximum dose of 30 mg in 24
hours and maximum duration of 5 days)
• intravenous doses should be administered by slow bolus injection over at least
3 minutes to help minimise these risks.
• Dystonic reactions have been shown to be significantly less common in non
pregnant patients receiving a slow infusion as opposed to a bolus injection of
10 mg of metoclopramide.
Metoclopramide – second line therapy Page 29

Studies on the safety of ondansetron are mixed.
• Large retrospective analysis of data from the Danish birth registry of 608 385
pregnancies found no increased risk of major birth defect, stillbirth, preterm
labour or small-for-gestational age.
• Case–control study with 4524 cases and 5859 controls found a two-fold
increased risk of cleft palate (adjusted OR 2.37, 95% CI 1.18–4.76)
• Data from the Swedish Medical and Birth Register demonstrated a small
increased risk of cardiovascular defects and cardiac septal defects (OR 1.62,
95% CI 1.04–2.14, and risk ratio 2.05, 95% CI 1.19–3.28, respectively).
Ondansetron – second line therapy Page 30

Reproductive toxicology 2016; 62: 87-91 Page 31
Ondansetron
1070
HG / No
ondansetron
771
No HG / No
ondansetron
1555
Malformations 3.47% 3.4%
VSD 2/952 0 4/1286
Cleft palate 1/952 0 2/1286
Terminations 2.52% 8.69%

Page 32

Hviid A, Molgaard-Nielsen D. CMAJ 2011;183(7):796-804.
• Cohort study of all live births in Denmark 1996 to 2008.
• 832 636 live births
• 51 973 exposures to corticosteroids during the first trimester
• 1232 isolated orofacial clefts (i.e., cleft lip, cleft palate, or cleft lip
and cleft palate) diagnosed within first year of life
84 in which the infant had been exposed to corticosteroids
during the first trimester

Hviid A, Molgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacialclefts. CMAJ 2011;183(7):796-804.

Iron supplements
Two-thirds of 97 women who discontinued iron supplements reported
improvement in their severe NVP in a Canadian prospective cohort
study.
Gill SK, Maltepe C, Koren G.
The effectiveness of discontinuing iron-containing prenatal
multivitamins on reducing the severity of nausea and vomiting
of pregnancy. J Obs Gyn 2009; 29: 13-16.

Page 36

Pre-emptive treatment
Canadian study comparing women with NVP [PUQE ≥ 13] who took pre-
emptive antiemetics before pregnancy or before the onset of symptoms
with those who did not
• lower recurrence rate of HG
• significant improvement in the PUQE score of NVP severity compared
to the previous pregnancy in the pre-emptive group.
• Women who have experienced severe NVP in a previous pregnancy
may benefit from taking antiemetics before or immediately at the start
of symptoms in a subsequent pregnancy.
Koren G, Maltepe C. Pre-emptive therapy for severe nausea and
vomiting of pregnancy and hyperemesis gravidarum. J Obstet Gynaecol
2004;24:530–3. 37

Jarvis & Nelson-Piercy. BMJ 2011;342

Jarvis & Nelson-Piercy. BMJ 2011;342

Page 40
I visited my GP who said he would prescribe the ondansetron on repeat only
because you had authorised it 'because GPs aren't allowed to prescribe
high risk medications during pregnancy.'
I politely mentioned that the UK guidelines recommend ondansetron for HG.
He was of the view that NVP is very normal so I should 'keep eating and
keep vomiting' because something will stay down eventually!
Thank you once again for seeing me at short notice and for making the
nausea and vomiting bearable!
I feel so much better and it's all thanks to you! I have been able to eat small
meals after weeks of surviving on 2 crackers a day.
Of course you could use my GPs quote - whatever it takes to get GPs to
understand that HG is more than a touch of morning sickness!

• Pre-eclampsia
• Acute fatty liver of pregnancy
Not specific to pregnancy:
• UTI
• Gastoenteritis
• Cholecystitis
• Appendicitis
• Pancreatitis
• Metabolic / Endocrine – DKA, hyperparathyroidism
Other pregnancy causes of nausea and vomiting Page 41

H2 blockers
Proton pump inhibitors
H pylori eradication therapy
OGD / endoscopy
ARE ALL SAFE IN PREGNANCY !!
Drugs Page 42