national maternal death surveillance and ......national maternal death surveillance and response...
TRANSCRIPT
NationalMATERNAL DEATH
SURVEILLANCE AND RESPONSE
MYANMAR, DECEMBER 2018
2017 Report
Maternal and Reproductive Health Division Department of Public Health Ministry of Health and Sports

National MATERNAL DEATH SURVEILLANCE AND RESPONSE
2017 Report
Myanmar
December, 2018


INATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Foreword
Maternal death surveillance and response (MDSR) is one of several low cost, high impact strategies to reduce maternal mortality. The Maternal Death Surveillance and Response (MDSR) strategy aims to improve quality of care and reduce maternal deaths by investigating individual maternal deaths and taking action to avoid remediable causes.
The MDSR system was rolled-out across all states/regions in Myanmar in 2017. In addition to full national coverage, the MDSR database now receives reports and case summaries from a growing number of hospitals ensuring that the cycle of identification, notification, reporting, review, and response occurs at both community and facility levels. This is important as it will ensure that action is taken both to increase demand-side use of maternal, newborn and child health (MNCH) services and improve supply-side quality of routine and emergency obstetric and newborn care.
This report on maternal deaths is the fifth in a series of reports for Myanmar, the previous reports were on maternal death reviews (MDR). While the review (MDR) component of MDSR is well established, “surveillance” in MDSR emphasizes the need for more accurate and complete data on number of maternal deaths, and the “response” involves formulating and implementing targeted recommendations. Furthermore, the classification of deaths was in accordance with the 2018-2019 International Classification of Disease -10-CM. Post-partum haemorrhage (23 per cent) remained high in geographically remote areas; while pregnancy with abortive outcomes (16 per cent) was the leading cause in major cities. Hypertensive disorders in pregnancy (15 per cent), unanticipated complications of management (9 per cent); and indirect causes, namely pre-existing medical diseases (19 per cent) were other major contributors.
It is important to document where delays occur: deciding to seek care, reaching care and receiving care; as interventions for each type of delay are different and need to be prioritised according to identified need to accelerate further reduction in the number of preventable maternal deaths. The three delays model helps to determine where improvements can be made to save the lives of women and babies.
Myanmar’s commitment to the maternal, newborn and child health agenda remains strong and ending preventable maternal and child mortality is prominent in the National Health Plan (NHP).MDSR report will be a reliable data source that will be useful for policy, advocacy, decision making and planning action in response to identified needs and gaps.
II NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Table of Contents Foreword IList of Acronyms IVList of Tables VList of Figures V
Executive Summary 1
Chapter 1. Introduction 3Chapter 2. Objectives of MDSR Report 7Chapter 3. Methodology 9Chapter 4. Introduction of MDSR System 11
Chapter 5. MDSR Implementation 13
5.1 Surveillance 13 5.1.1 Surveillance in the community 13 5.1.2 Surveillance in the health facility 13 5.1.3 Compilation of information at State/Regional level 14 5.1.4 Review of Maternal Deaths 14 5.1.4.1 Maternal deaths by geographic areas 14 5.1.4.2 Background characteristics 18 5.1.4.3 Obstetric profile 20 5.1.4.4 Cause of death 24 5.1.5 Contributory factors: the delay model 28 5.1.6 Review Committees 315.2 Response 32 5.2.1 Specific 32 5.2.2 General 33 5.2.3 Activities conducted by MRH Division 33
Chapter 6. Benefits of Institutionalizing MDSR System 35

IIINATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 7. Challenges 37
7.1 Notification and reporting 37 7.1.1 Community 37 7.1.2 Health facilities 387.2 Transmission of forms 387.3 Analysis 387.4 Review 397.5 Response 397.6 Other issues 39
Chapter 8. Recommendations 41
8.1 Recommendations to improve the surveillance functions of the system 418.2 Recommendations to improve the Response 428.3 General recommendations 44
Chapter 9. Conclusion 45
Annexes 47
Annex 1 List of documents reviewed 47Annex 2 List of persons interviewed 48Annex 3 Definitions 49
IV NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
AMW Auxiliary MidwifeANC Antenatal CareAPH Antepartum haemorrhageBEmONC Basic Emergency Obstetric and Newborn CareBHS Basic Health StaffCBMDSR Community-based maternal death surveillance and responseCEmONC Comprehensive Emergency Obstetric and Newborn CareCensus Myanmar Population and Household CensusCSO Civil Society OrganizationDHS Demographic and Health SurveyDHIS District Health Information SystemDoPH Department of Public HealthEPMM Ending Preventable Maternal MortalityHMIS Health Management Information SystemHSS Health System StrengtheningICD-10-CM 2018-2019 International Classification of Disease-10-CMIDP Internally displaced populationIEC Information, Education and CommunicationIUD Intra-uterine DeviceMCH Maternal and Child HealthMDG Millennium Development GoalsMDSR Maternal Death Surveillance and ResponseMDR Maternal Death ReviewMMEIG Maternal Mortality Estimation Inter-Agency GroupMMR Maternal Mortality RatioMNH Maternal and Newborn HealthMoHS Ministry of Health and SportsMRH Maternal and Reproductive HealthMW MidwifePAC Post-abortion CarePMTCT Prevention of mother-to-child transmissionPPH Post-partum HaemorrhageQOC Quality of careRH Reproductive HealthRHC Rural Health CentreSBA Skilled Birth AttendantSDGs Sustainable Development Goal(s)SMO Station Medical OfficerSRHC Sub-Rural Health CentreTBA Traditional Birth AttendantTMO Township Medical OfficerUHC Universal Health CoverageUNFPA United Nations Population FundWHO World Health Organization3MDG FMO 3 Millennium Development Goal Fund Management Office
List of Acronyms
VNATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
List of Tables
List of Figures
Table 1. Review Rate of Maternal Deaths 4Table 2. Deaths from Obstetric Haemorrhage 25
Figure 1. Primary Steps of MDSR 5Figure 2. Number of MDSR Reported Deaths for 2017 (State/Region) 15Figure 3. Comparison of Maternal Deaths in 2016 and 2017 16Figure 4. MMR as per Reported MDSR Deaths 17Figure 5. Number of Maternal Deaths by Residence 17Figure 6. Number of Maternal Deaths by Age Group 18Figure 7. Number of Maternal Deaths by Education 19Figure 8. Number of Maternal Deaths by Occupation 19Figure 9. Number of Maternal Deaths by Gravida 20Figure 10. Number of Maternal Deaths by Antenatal Visits 21Figure 11. Comparison of Number of Antenatal Visits in 2016 and 2017 21Figure 12. Number of Maternal Deaths by Place of Death 22Figure 13. Maternal Mortality: Place of Delivery and Place of Death 22Figure 14. Maternal Mortality by Provider at Birth 23Figure 15. Maternal Deaths by Stage of Pregnancy 23Figure 16. Abortion-Related Deaths 24Figure 17. Classification of Cause of Deaths 24Figure 18. Cause of Deaths by Direct Group 25Figure 19. Cause of Deaths by Indirect Group 26Figure 20. Cause of Deaths by all Groups 27Figure 21. Maternal Deaths by Type of Delay 29

1NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Executive Summary
Myanmar has moved forward to transform Maternal Death Reviews (MDRs) to Maternal Death Surveillance and Response (MDSR), which was launched for nationwide implementation in January 2017.MDSR builds on MDR by stressing the importance of follow-up action (response) and of continual monitoring to ensure that recommendations are acted on. As a result, MDSR has been described as a “continuous action cycle for monitoring of maternal deaths”
As such, Myanmar has embarked on the four primary steps of the MDSR:
1. Identification and notification on an ongoing basis: Identification of suspected maternal deaths in facilities through completion of hospital forms; and verbal autopsy in communities.This is followed by immediate notification to the township, then state/regional and finally national authorities.
2. Review of maternal deaths by local (township) maternal death review committees: Examination of cause of death, medical and nonmedical contributing factors that led to the death, assessment of avoidability and development of recommendations for preventing future deaths, and immediate implementation of prioritized recommendations.
3. Analysis and interpretation of aggregated findings from reviews: Reviews conducted at the state/regional level and reported to the national level; development of critical recommendations for national action based on the aggregated data.
4. Response and monitoring of the response: Implementation of recommendations made by the review committee(s) and those based on aggregated data analyses; monitoring to ensure that recommended actions are being adequately implemented. The response/actions can address problems at the community, facility, or multi-sectoral level.
In 2017, there was a total of 949 deaths reported, of which 873 (91.9 per cent) were reviewed.
When urban-rural area of residence was calculated, 75.7 per cent of the dead women resided in rural areas, whereas 23.4 per cent were urban residents, reflecting the 2014 Census data which suggests that Myanmar is still a predominantly rural country. The deaths occurred mainly among the less-educated and lower-income groups. The highest number of deaths were in women in the 25-29 age group.
Classification of deaths was in accordance with the 2018-2019 International Classification of Disease -10-CM. Among the direct causes of deaths, post-partum haemorrhage is highest at 23 per cent, pregnancy with abortive outcomes 16 per cent, hypertensive disorders in pregnancy 15 per cent and unanticipated complications of management 9 per cent; while indirect causes, namely pre-existing medical diseases contributed to 19 per cent of the total.
When the contributory factors were analysed according to the “Three Delays” model, the decision to seek care and reach care accounted for three quarters of cases. The burden was borne mainly by geographically hard-to-reach areas and rural areas.
Review meeting at different levels could be initiated in the second half of the year. Almost all State/Regional Health Departments held two meetings in 2017. The actions taken by hospitals in response to in-patient care were immediate, i.e. improved monitoring of labour, adherence to standard operating procedures in Obstetrics and Anaesthesia. A few Health Departments organized refresher training for management of third stage of labour for midwives and prevention of post-partum haemorrhage

2 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
for auxiliary midwives. Furthermore, community health education sessions were organized by some townships on contraception and dangers of unsafe abortion when there were increasing numbers of deaths from post-abortion complications. In some areas, the sessions, covered antenatal care and birth preparedness plans.
Health staff at different administrative levels had a heightened awareness of the importance of “surveillance”. As a result, there were efforts to obtain more complete data. Early transmission of information was achieved through means such as Instant Messaging, Viber or telephone. The delays occurred in transmission of forms and holding of review meetings. While efforts were made to “Respond” to individual cases or aggregated data, the follow-up and monitoring could be strengthened at all levels. Challenges in implementation of MDSR included the transfer of staff trained on MDSR implementation, the costs for travel for verbal autopsies and for convening review meetings.
This is a report of the first year of MDSR implementation in Myanmar. While progress has been made, it is acknowledged that there is still much to be done. The “Response” to the surveillance needs to be merged with on-going strategies to end preventable maternal mortality: comprehensive emergency obstetric and newborn care, post-abortion care, sexual and reproductive health information and contraceptive service, among others.

3NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 1. Introduction
The Myanmar National Health Plan (NHP) aims to strengthen the country’s health system and pave the way towards Universal Health Coverage (UHC), choosing a path that is explicitly pro-poor.Reproductive, maternal, newborn and child health is one of the programme priority areas under NHP and the unfinished task of MDGs 4 and 5 remains of high importance in the SDG era.
According to the United Nations Inter-agency Estimates for Maternal Mortality, the maternal mortality ratio (MMR)for Myanmar, declined from 453 deaths per 100,000 live births to 178 per 100,000 live births between 1990 and 2015. 178 per 100,000 is an estimated average of a range varying from 121 (lowest) to 284 (highest) deaths per 100,000 live births. This estimate is consistent with the figure of 282 per 100,000 live births reported by the 2014 Myanmar National Housing and Population Census.
Maternal Death ReviewsIn Myanmar, data on births and deaths were collected from 1996 through the Health Management Information System (HMIS). Further, hospital-based maternal death reviews have been carried out at tertiary/university hospitals and state/regional hospitals in Myanmar for many years. The results were reported during conferences organized by the Obstetric and Gynaecological Society of the Myanmar Medical Association. Maternal death notification in the public health system was initiated in 2003 by the Maternal and Child Health (MCH) section, Department of Health. In addition to the number of deaths, information was collected on place and time of death, type of providers and cause of death. In 2005, Myanmar introduced maternal death review (MDR) as a pilot in Sagaing Region. This process introduced a community-based MDR being conducted in 30 pilot townships in Sagaing between 2005 and 2009, and facility-based MDR conducted in the three teaching/university hospitals (Universities of Medicine 1, 2 and Mandalay).
The verbal autopsy in the community-based MDR elicits information on socio-demographic variables, medical history, and past and present obstetric history and a review of the antenatal record. For hospital deaths, a review of the patient records, post mortem examination findings, and comments from the hospital doctors and other staff are noted. The completed form is then reported by the Township Health Department to State/Region level. Maternal death review team members from State/Regional level review these forms, make comments and note the actions taken, and forward it to the central level. At the central level, maternal death audit teams review the reported deaths and provide feedback.
Using this process, an increasing number (proportion) of maternal deaths were reported and reviewed. This increase in review rate was reported in previous MDR reports. In 2016, out of 823 maternal deaths reported to the MDR, review was conducted in 815 (99%), thus maintaining the high rate of review of maternal deaths reported. In the MDR 2015 report, a table showed the progress from 2011 to 2015. It was observed that there was a notable decline in the review rate in 2015. This table is reproduced below with the addition of the performance in 2016 and 2017, and it shows that the review rate has increased appreciably from 2015.
There were 823 maternal deaths reported to the MDR in 2016, out of which 815 were reviewed. The MMR for 2016 is 94.9 per 100,000 livebirths.

4 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Table 1. Review Rate of Maternal DeathsNumber of maternal deaths (source) Number reported Number (%) reviewed
2011 2,000 (MMEIG) 1,517 478 (31.5%)
2012 2,000 (MMEIG) 1,208 670 (55.5%)
2013 1,900 (MMEIG) 922 863 (93.6%)
2014 Not available 846 846 (100%)
2015 Not available 861 674 (78.2%)
2016 Not available 823 815 (99.0%)
2017 MDSR 949 873 (91.9%)
With respect to reporting, respondents from states and regions noted that:
“There could be underreporting of 2017 figures, especially from hard-to reach and conflict areasin terms of reporting and conduct of field investigations."
Maternal Death Surveillance and ResponseMyanmar has moved forward to transform Maternal Death Reviews (MDRs) to Maternal Death Surveillance and Response (MDSR), which was launched for nationwide implementation in September 2016.
Maternal death surveillance and response (MDSR) is a relatively new approach to investigating maternal deaths and taking action based on the findings, which has evolved from the established system of maternal death review (MDR). It builds on MDR by stressing the importance of follow-up action (response) and of continual monitoring to ensure that recommendations are acted on. As a result, MDSR has been described as a “continuous action cycle for monitoring of maternal deaths”
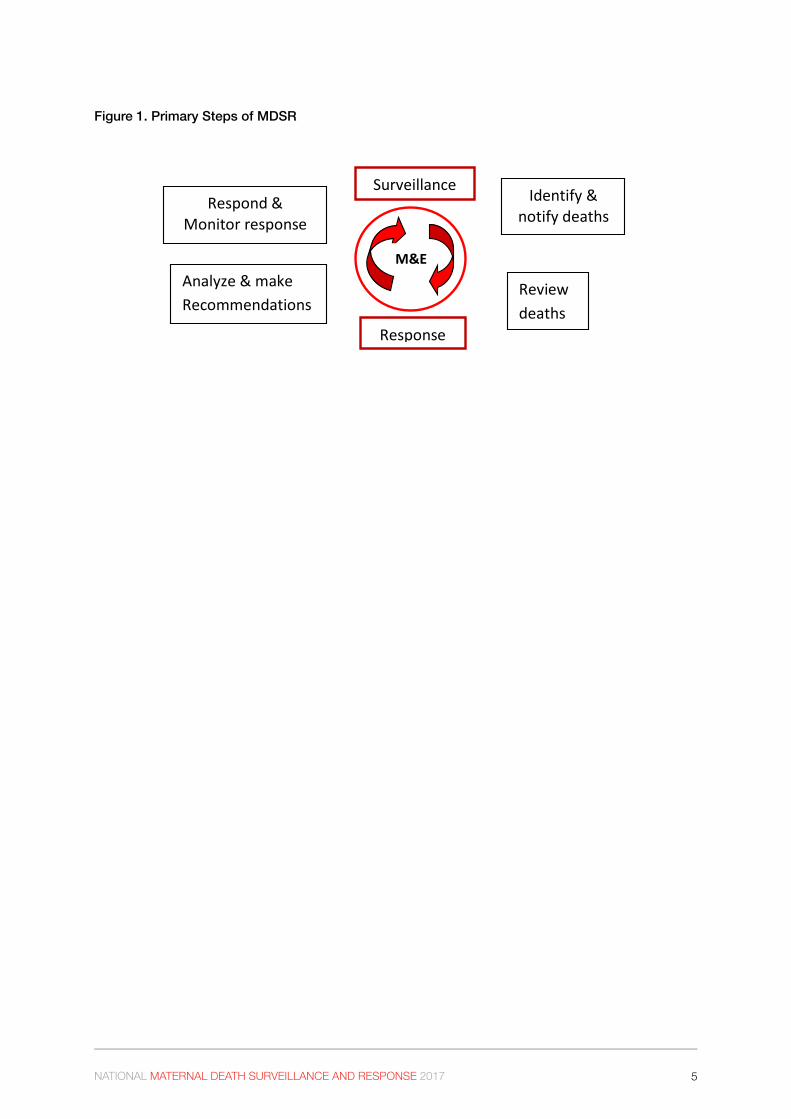
In a continuous action cycle, there are four primary steps to the MDSR:
1. Identification and notification on an ongoing basis: Identification of suspected maternal deaths in facilities and communities, followed by immediate notification to the appropriate authorities.
2. Review of maternal deaths by local (township) maternal death review committees: Examination of medical and nonmedical contributing factors that led to the death, assessment of avoidability and development of recommendations for preventing future deaths, and immediate implementation of pertinent recommendations.
3. Analysis and interpretation of aggregated findings from reviews: Reviews conducted at the state/regional level and reported to the national level; development of priority recommendations for national action based on the aggregated data.
4. Response and monitoring of the response: Implementation of recommendations made by the review committee and those based on aggregated data analyses; monitoring to ensure that recommended actions are being adequately implemented. The response/actions can address problems at the community, facility, or multi-sectoral level. (MDSR Technical Guidance, 2013 – WHO and partners)
5NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 1. Primary Steps of MDSR
Surveillance
Response
Identify & notify deaths
Review deaths
Respond & Monitor response
Analyze & make Recommendations
M&E

6 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017

7NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 2. Objectives of MDSR Report
The primary goal of MDSR is to eliminate preventable maternal mortality, with the overall objective “to provide information that effectively guides immediate as well as longer term actions to reduce maternal mortality and the impact of actions to reduce it.” MDSR emphasizes the continued importance of identification and notification of deaths, of accurate collection of information regarding cause of death and preventable or avoidable factors relating to the death, and of appropriate analysis and interpretation of the data collected. These will lead to the generation of evidence- based recommendations, and, perhaps most importantly, a measurable response to these recommendations. This surveillance approach emphasizes the need to close the loop. In addition, the process itself requires ongoing monitoring and evaluation to ensure that it is functioning effectively.
The objectives of the MDSR report (2017) are to:
• Highlight the efforts that were put in place to establish MDSR in the country. • Provide information on the current status of implementation of MDSR: notification, review,
analysis and response. • Provide an overview of maternal deaths from collated information for the period January
to December 2017. • Analyse the causes of maternal deaths based on ICD-10-CM coding which includes
ICD-10-MM.• Describe the social and behavioural determinants of maternal deaths from the providers
perspectives.• Describe the benefits of the MDSR process and the challenges.• Provide recommendations to strengthen the existing system and other measures to further
reduce maternal deaths.

8 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017

9NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 3. Methodology
Review of literatureMany documents related to the maternal and newborn health (MNH)programme, maternal death review and maternal death surveillance and response: global, regional and national were reviewed. (Annex 1).
Conducting interviewsKey informant interviews were conducted with a wide spectrum of stakeholders from the different administrative levels under the Ministry of Health and Sports: Maternal and Reproductive Health Division, Deputy State/Regional Public Health Directors and Assistant Directors, Medical Superintendents, Township Medical Officers, MRH staff officers and Health Assistants from four Regions (Ayeyawaddy, Mandalay, Magway and Yangon) and four states (Chin, Kachin, Kayah and Northern Shan). Obstetricians and Gynaecologists from tertiary/university and state/regional hospitals and district hospitals were also interviewed. UNFPA staff who were engaged throughout the process were also consulted. (The complete list of 33informants is provided in Annex 2).
Evaluation of data entry and analysisData entry from various forms had been performed on excel sheets and the collated data on Community-based MDSR (CBMDSR) and Facility based MDSR were reviewed for completeness and coherence. Data on livebirths was obtained from HMIS DHIS2 and was used to calculate MMR based on MDSR reports.
The 3MDG FMO team assisted the MRH in data cleaning and analysis of 2017 MDSR data. Firstly, the raw data file in which maternal death data which were entered by the respective state and regional teams, were processed by the 3MDG FMO team into the first clean version by preparing data into the correct format, removing unnecessary characters (such as “?”, “-“, etc.) and re-categorizing groups as per coding. This version was further processed into the second clean version in which overlapped maternal deaths were removed, obvious errors (e.g LSCS in RHC/SRHC done by Specialist), a number of variables (age group, place of delivery, antenatal visits, place of death) were re-categorized. After that, the final cleaning process was done by removing formula and unnecessary columns, and changing “not recorded and “Unknown” as “missing” in key variables. Based on the final clean version file, countrywide and state/regional MDSR analysis and graphs were prepared with reference to the 2015 and 2016 MDSR reports.
Data was analysed to obtain the number of deaths, as well as the background information and obstetric profile of the deceased. The cause of deaths and the contributory factors were also studied.
Assignment of ICD codesThe international classification of disease (ICD 10) and WHO definition of maternal deaths were used to independently code the causes of death. https://www.icd10data.com/ICD10CM/Codes. The data was corroborated by information obtained during interviews. The coding was checked with the diagnosis, the codes entered and the description of findings where the entries were contradictory. The cause of death is presented in accordance with the ICD 10 codes.
Analysis of Response and Action. The action taken by the MDSR Teams at various levels which had been recorded in the review forms were also entered in the excel sheet. Further, the key informant interviews allowed elaboration of the response mechanism including general and specific responses and follow-up.

10 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Developing RecommendationsIn addition to the recommended points noted in the excel sheets, the key informant interviews added depth to the suggestions to improve the MDSR process and ultimately lower the maternal mortality.
The social and behavioural factors described by interviewees brought about a better understanding of the underlying factors leading to the death, which is critical for preventing future mortality. While the reasons for the “Three delays” had been recorded as the type(s) of delay in the forms; discussion on the entire process allowed the analysis to go “beyond the numbers”.
11NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 4. Introduction of MDSR System
The Maternal and Reproductive Health Division, Ministry of Health and Sports, in collaboration with country offices of UNFPA and WHO, supported by 3MDG Fund, took the lead in establishing the MDSR system in 2017. The expectation was that MDSR would provide information that effectively guides actions to end preventable maternal mortality at health facilities and in the community; and by counting every maternal death permitting an assessment of the true magnitude of maternal mortality and the impact of actions taken to reduce it. An analysis of these deaths would help to identify the delays at each level that contribute to maternal deaths and this information would be used to adopt measures to improve decision making and address gaps in service.
Preparatory activitiesIn addition to in-country efforts to improve the national process, Myanmar benefitted from South-South collaboration. This included Myanmar’s participation in a regional meeting organized by the South-east Asia Regional Office of WHO to strengthen capacity on maternal and perinatal death surveillance, held in the Republic of Maldives in February 2016. This was followed by a visit to Sri Lanka to learn from their experiences and success stories on MDSR given that the system was established and considered as one of the “good practice” countries in South-east Asia. Furthermore, a joint Myanmar-Sri Lanka MDSR symposium was held in Yangon, Myanmar, in February 2017 as part of the 12th Annual Conference of the OBGYN society. At this event, a larger audience from Myanmar – comprising of national and state/regional senior officials and obstetricians and gynaecologists were able to learn from the MDSR experience in Sri Lanka.
During 2016 a series of consultations were held with key players of Ministry of Health and Sports and representatives of medical universities, Obstetric and Gynaecological society, Myanmar Medical Association, and health care providers from different levels. This led to drafting of the Myanmar MDSR guidelines, MDSR forms for community reporting as well as hospital settings and a training manual. Pilot testing for Community Notification, Community Investigation, Facility Based Notification and Facility Based Investigation Forms was undertaken in specialist hospitals, general hospitals, township hospitals and at station hospitals which is the lowest facility of the health infrastructure (25-50 beds). This process also involved engaging families in the community in terms of the forms being user-friendly and understandable. A national MDSR advocacy package was also developed through a similar process.
In September 2016, the national MDSR system was launched at the central level and in the last Quarter of 2016, State and Regional Level MDSR advocacy meetings were conducted in tandem with MDSR training in all States and Regions, involving township level health facility representatives and OBGYN focal persons. The training included identification of causes of maternal death in accordance with the International Classification of Disease ICD-10-CM coding guidelines, as well as conducting verbal autopsy. This enabled participants to explore the in-depth situation on each maternal death that occurred in both community as well as hospital settings.
12 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Application of the Three Delays modelIn addition to verbal autopsy, which involved the use of standardized interview tools to question the caretakers of recently deceased persons about the symptoms that preceded the death; non-biological factors contributing to a death, i.e. social, behavioural and health systems determinants of maternal deaths were looked into. This took into account the family’s aspect of the event. Finally, the caretaker of the deceased was interviewed in detail to establish what care was received by the deceased inside or outside the home, as well as barriers encountered during care seeking.
Interviews in the community and at health facilities focused not only on determining the clinical diagnosis and management; but also on the contributory factors that affected the outcome of emergency presentation during pregnancy. These three main factors were defined, chronologically, as the lengths of the delays in: (i) the decision to access care, (ii) the identification of – and transport to – a medical facility, and (iii) the receipt of adequate and appropriate treatment.
Setting up MDSR review committeesIn accordance with the Myanmar National MDSR guideline, MDSR teams were formed at National, State/ Regional, and Township (both public health and hospital) levels. Lines of reporting at different levels were clarified. The guidance provided was that MDSR reviews are undertaken within the MoHS as a routine and ongoing mechanism at township level (both in public health and in hospital setting) on a monthly basis, while at State/Regional level, these are undertaken on a three-monthly basis, and at central level on a six-monthly basis. This was to be an on-going mechanism. Furthermore, MDSR focal points were assigned at every level in the Health Department and at hospitals. In large university/tertiary hospitals, at least one person was selected as focal person.

13NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 5. MDSR Implementation
Myanmar has been working towards implementing a comprehensive MDSR system by building on existing approaches, particularly MDR. The rapid cycle of notification, review, analysis and response enabled by MDSR gives the opportunity to monitor maternal mortality in near real time, both at subnational and national level, and can provide early warning of problems in a health facility or locality.
5.1 Surveillance
5.1.1 Surveillance in the community
Identification and notification of deathsThe local midwife collects the information and documents in the maternal death notification form, then notifies the Township Health Department.
Township Health Department usually has to notify maternal deaths to the respective State/Regional MDSR team and Central level MDSR team within 24 hours of maternal deaths through available communication channels e.g. phone/Fax/Viber or instant messaging. However, in case of maternal deaths in hard-to-reach areas, this notification may take longer than 24 hours.
Field investigation through verbal autopsy and determination of social-behavioural factorsA team led by the Township Medical Officer (TMO) and other members: Township Health Nurse, Lady Health Visitors and local midwife undertake a visit to the home of the deceased after the customary period of mourning for that community, which is usually within seven days. The health team is accompanied by local/village health authorities and usually visits the home in an unobtrusive manner, i.e. not dressed in uniforms. The midwife brings vitamins for the family and in circumstances where the baby has survived, the midwife brings small gifts for him/her. The verbal autopsy was made and the information of events surrounding the maternal death is obtained as part of a conversation. Notes are not taken, but facts are written up afterwards.
Township level reviews Township level reviews were carried out and reviews at monthly or (two to three monthly) and specific responses were made with respect to each death within their vicinity. The Township Health Department and Hospital level MDSR team compiled the death review and response summary for each maternal death. These are then reported to State and Regional MDSR team. While the township MDSR team should ensure the completeness of investigation form and send on to the respective state/regional MDSR team within 21 days of the occurrence of maternal deaths, in actual practice it could take more than 21 days.
5.1.2 Surveillance in the health facility
Identification of deathsHealth facilities were identifying deaths and hospital MDSR focal persons and their colleagues used a variety of sources for identifying maternal deaths: labour, delivery and postnatal registers. Women who were dead on arrival were reported and documented at the emergency department and the forms being completed by MDSR focal persons. In tertiary level hospitals, state/regional or district hospitals, it was primarily the obstetricians and gynaecologists who followed up on women who were transferred out to medical or surgical wards or the intensive care units.

14 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Notification of deathsCompletion of Hospital Investigation forms and determination of socio-behavioural factors is carried out by MDSR focal persons and their colleagues. These forms are then sent to State/Regional MDSR team within 21 days, though it takes longer in reality.
In most hospitals, the information required for these forms was noted from the outset in hospital records. Were it not for this, it could be difficult and insensitive to interview the family or care providers in the event of a maternal death occurring. If the patient survived the episode, she would fall under the category of “near-miss” (severe maternal morbidity). Most hospitals record and review “near miss” cases with the objective of improving the quality of care – determining “what went right”.
Facility level reviews Hospital MDSR team would review the cases, focusing the three delays, ascertain the avoidable factors and administrative and clinical procedures that could be improved in future management of similar conditions. Summary reports are sent to the State/Regional MDSR team.
5.1.3 Compilation of information at State/Regional level
State/Regional MDSR team collected data from both community and hospital deaths and compiled and developed the case scenarios for State/Regional level MDSR review meeting which was conducted quarterly. The State/Regional MDSR focal person prepared the case summaries and presented these at review meeting(s) and identified the three delays and avoidable factors and made recommendations for remedial actions. Then, they reported to Central MDSR team with a narrative report and also shared the excel spreadsheet for further analysis of maternal deaths.
At the end of the year, MRH Division together with 3MDG Fund Management Office (FMO) carried out data cleaning and explored the geographic distribution, socio-demographic profile of women, analysis of deaths by cause of death and the three delays, etc by categorisation. The Maternal and Reproductive Health Division at the central level conducted a detailed review of the records and reports that were submitted.
Furthermore, highlights of recommendations and suggestions given by state/regional and township levels were grouped and collated.
5.1.4 Review of Maternal Deaths
The analysis of maternal deaths for 2017 builds on the previously conducted maternal death reviews. A new feature is the classification of maternal deaths in accordance with ICD -10-CM and ICD-10-MM. Furthermore, the responses at the different administrative levels and in the health facilities are reported.This review covers 91.9 per cent of reported deaths for 2017 which was 873 while total reported deaths were 949. Calculation of MMR and comparison of the numbers of maternal deaths will be based on the total number of reported deaths. The other description and diagrams are based on the results of the analysed data, which is 873 maternal deaths.
5.1.4.1 Maternal deaths by geographic areas
Maternal deaths by geographic areas for the year 2017 is shown in Figure 2. The highest number of maternal deaths were in Ayeyawaddy, Yangon, Bago, Mandalay, Sagaing and Magway Regions, the first four regions having 100 or more deaths. The same pattern of occurrence was noted in the

15NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
2016 report. The high number of deaths reflect the population of these regions. Among the States and Regions, Yangon Region has the largest population at 7.3 million, followed by Ayeyawaddy and Mandalay Regions, each with approximately 6.2 million, and Shan State, with 5.8 million. Moderately large numbers of people live in Bago Region, Magway Region, Rakhine State and Sagaing Region; large territories that are home to approximately one third of the total population. (2014 Myanmar Population and Housing Census)
Figure 2. Number of MDSR Reported Deaths for 2017 (State/Region)
152
119
103 100
8579
51 4939 36 35
23 22 18 17 156
0
20
40
60
80
100
120
140
160
Ayeyarw
addy
Yango
nBag
o
Manda
lay
Sagain
g
Magway
Shan (
South
)
Rakhin
e
Shan (
North)
Kayin
Mon
Tanin
tharyi
Nay Pyi T
aw ChinKac
hin
Shan (
East)
Kayah
Num
ber o
f Mat
erna
l Dea
ths
2017
Source: Maternal Death Surveillance and Response, Maternal and Reproductive Health Division, Ministry of Health and Sports
The number of maternal deaths remained the highest in Ayeyawaddy Region in 2017. Geographical barriers as well as transportation difficulties affect access to health care by the resident population and migrants. A study conducted in two townships in the Region indicated that seasonal migration was high and that migrant mothers had less access to antenatal care and delivery by a skilled health professional. (Wai Wai Han, Saw Saw et al 2015). https://www.iom.int/sites/default/files/country/docs/myanmar/IOM-Myanmar-Migrant-MCH-folder.pdf
The number of deaths in Yangon was the second highest in 2017. This can be partly attributable to deaths among the large peri-urban population, most of whom are migrants. The direction of the main migration streams between districts or between states/regions was towards Yangon and in particular North and East Yangon. The major origins of the flows were other districts within Yangon or districts in Ayeyawady. On account of this, Yangon has an urban population of 5.2 million which far exceeds the sum of the population of the next three cities, (i.e. Mandalay, Nay Pyi Taw, and Bago). Of the 41 industrial zones sites approved by 2010, 23 were located in the Yangon Region. A high proportion of migrants to Yangon were employed in the manufacturing sector, half of whom were females. (2014 Myanmar Population and Housing Census – Policy Brief on Migration and Urbanization).The high number of deaths in Yangon was followed by two other urban hubs: Bago and Mandalay.

16 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 3. Comparison of Maternal Deaths in 2016 and 2017
Source: Maternal Death Surveillance and Response (2016) and Maternal Death Surveillance and Response (2017) reported deaths, Maternal and Reproductive Health Division, Ministry of Health and Sports
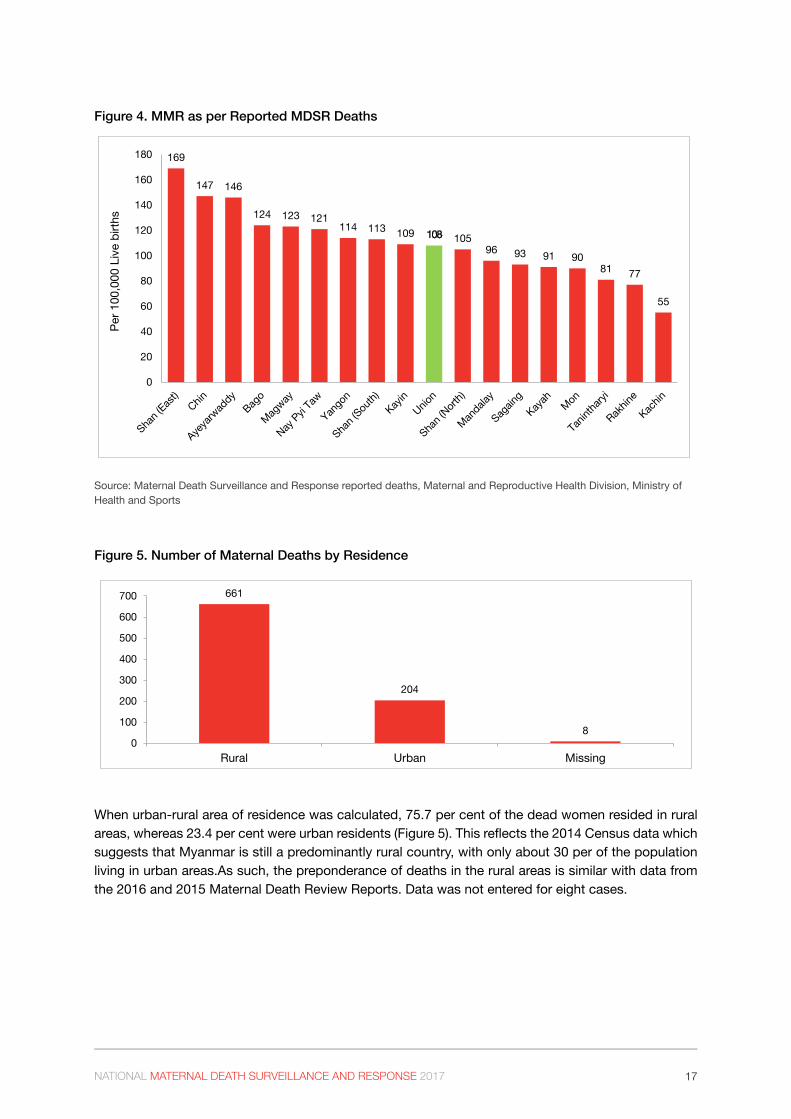
When MMR was calculated as per MDSR reported deaths with data on livebirths from HMIS DHIS2; the highest among the State/Regions in descending order are: Shan East (169 per 100,000 live births), Chin (147 per 100,000 live births), Ayeyawaddy (146 per 100,000 live births), Bago (124 per 100,000 live births) and Magway (124 per 100,000 live births). While the absolute numbers for these states: Shan East and Chin were less than 20, the population base is also smaller. The figure for Nay Pyi Taw is 121 per 100,000 live births. Nay Pyi Taw has a small number of deaths, but the resident population base is quite small 1,160,242 as it is an administrative area occupying a small land area. Moreover, the Nay Pyi Taw Hospital recieves referrals from townships such as Lae Wae, Pyinmana and Tutkone. In terms of both high absolute number and maternal mortality, Ayerwaddy ranked highest (152 maternal deaths and MMR-146 per 100,000 live births).
There are several hard-to-reach areas in Chin State and conflict-affected areas in the mountainous Shan East and Kachin States. During interviews, it was reported that there could be maternal deaths that were not reported due to the prevailing situation. As a result, further investigations could not be carried out.
122
86 84 79 77 7155
4837 36 32
25 22 22 171 1
152
103
119
100
7985
51 49
36 3517
39
18 23 2215
60
20
40
60
80
100
120
140
160
Num
ber o
f Mat
erna
l Dea
ths
2016 2017
17NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 4. MMR as per Reported MDSR Deaths
169
147 146
124 123 121114 113 109 108 105
96 93 91 9081 77
55
0
20
40
60
80
100
120
140
160
180
Per 1
00,0
00 L
ive b
irths
Source: Maternal Death Surveillance and Response reported deaths, Maternal and Reproductive Health Division, Ministry of Health and Sports
Figure 5. Number of Maternal Deaths by Residence
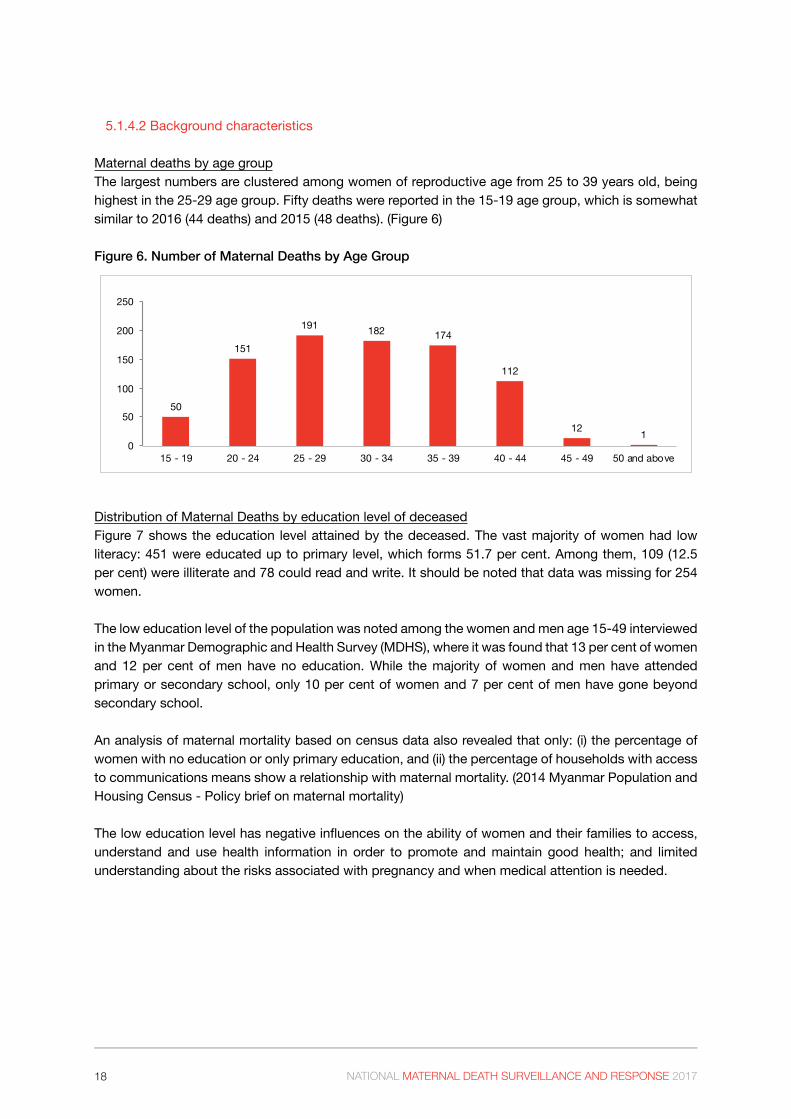
When urban-rural area of residence was calculated, 75.7 per cent of the dead women resided in rural areas, whereas 23.4 per cent were urban residents (Figure 5). This reflects the 2014 Census data which suggests that Myanmar is still a predominantly rural country, with only about 30 per of the population living in urban areas.As such, the preponderance of deaths in the rural areas is similar with data from the 2016 and 2015 Maternal Death Review Reports. Data was not entered for eight cases.
661
204
80
100
200
300
400
500
600
700
Rural Urban Missing
18 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
5.1.4.2 Background characteristics
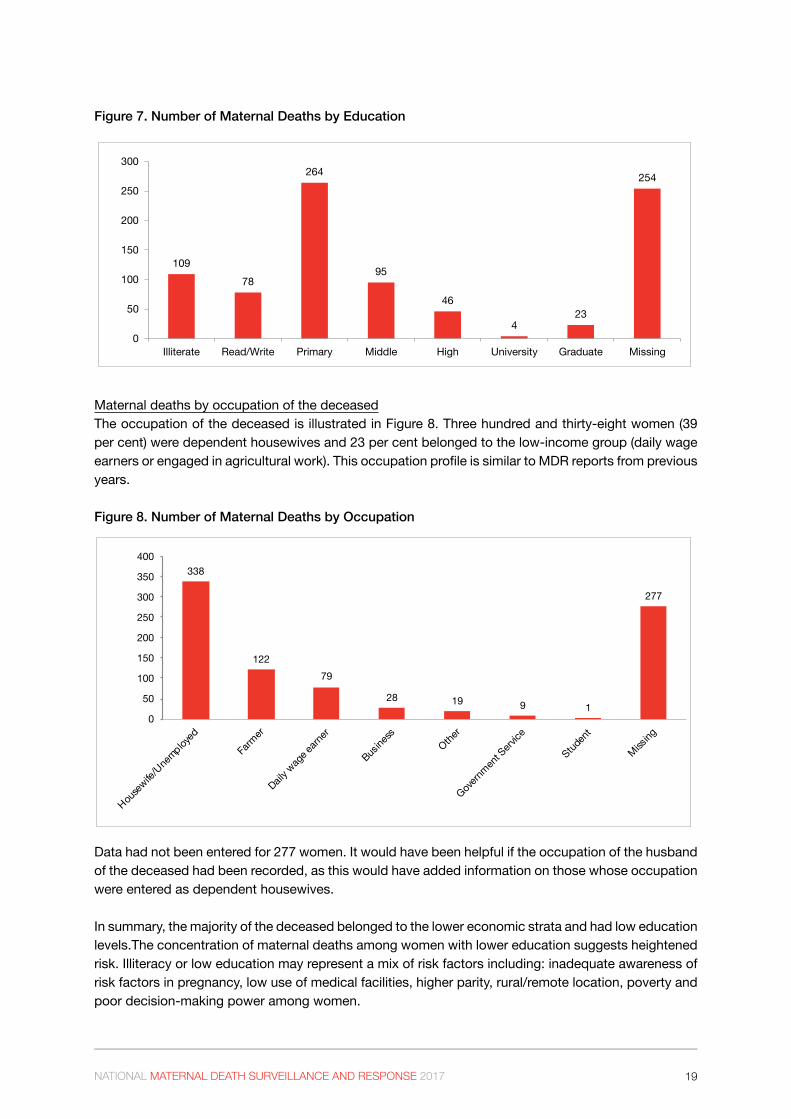
Maternal deaths by age groupThe largest numbers are clustered among women of reproductive age from 25 to 39 years old, being highest in the 25-29 age group. Fifty deaths were reported in the 15-19 age group, which is somewhat similar to 2016 (44 deaths) and 2015 (48 deaths). (Figure 6)
Figure 6. Number of Maternal Deaths by Age Group
50
151
191 182 174
112
12 10
50
100
150
200
250
15 - 19 20 - 24 25 - 29 30 - 34 35 - 39 40 - 44 45 - 49 50 and above
Distribution of Maternal Deaths by education level of deceasedFigure 7 shows the education level attained by the deceased. The vast majority of women had low literacy: 451 were educated up to primary level, which forms 51.7 per cent. Among them, 109 (12.5 per cent) were illiterate and 78 could read and write. It should be noted that data was missing for 254 women.
The low education level of the population was noted among the women and men age 15-49 interviewed in the Myanmar Demographic and Health Survey (MDHS), where it was found that 13 per cent of women and 12 per cent of men have no education. While the majority of women and men have attended primary or secondary school, only 10 per cent of women and 7 per cent of men have gone beyond secondary school.
An analysis of maternal mortality based on census data also revealed that only: (i) the percentage of women with no education or only primary education, and (ii) the percentage of households with access to communications means show a relationship with maternal mortality. (2014 Myanmar Population and Housing Census - Policy brief on maternal mortality)
The low education level has negative influences on the ability of women and their families to access, understand and use health information in order to promote and maintain good health; and limited understanding about the risks associated with pregnancy and when medical attention is needed.
19NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 7. Number of Maternal Deaths by Education
Maternal deaths by occupation of the deceasedThe occupation of the deceased is illustrated in Figure 8. Three hundred and thirty-eight women (39 per cent) were dependent housewives and 23 per cent belonged to the low-income group (daily wage earners or engaged in agricultural work). This occupation profile is similar to MDR reports from previous years.
Figure 8. Number of Maternal Deaths by Occupation
338
12279
28 19 9 1
277
0
50
100
150
200
250
300
350
400
Housew
ife/Une
mployed
Farm
er
Daily wag
e earn
er
Busine
ssOthe
r
Governm
ent S
ervice
Studen
t
Missing
Data had not been entered for 277 women. It would have been helpful if the occupation of the husband of the deceased had been recorded, as this would have added information on those whose occupation were entered as dependent housewives.
In summary, the majority of the deceased belonged to the lower economic strata and had low education levels.The concentration of maternal deaths among women with lower education suggests heightened risk. Illiteracy or low education may represent a mix of risk factors including: inadequate awareness of risk factors in pregnancy, low use of medical facilities, higher parity, rural/remote location, poverty and poor decision-making power among women.
10978
264
95
46
423
254
0
50
100
150
200
250
300
Illiterate Read/Write Primary Middle High University Graduate Missing
20 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
5.1.4.3 Obstetric profile
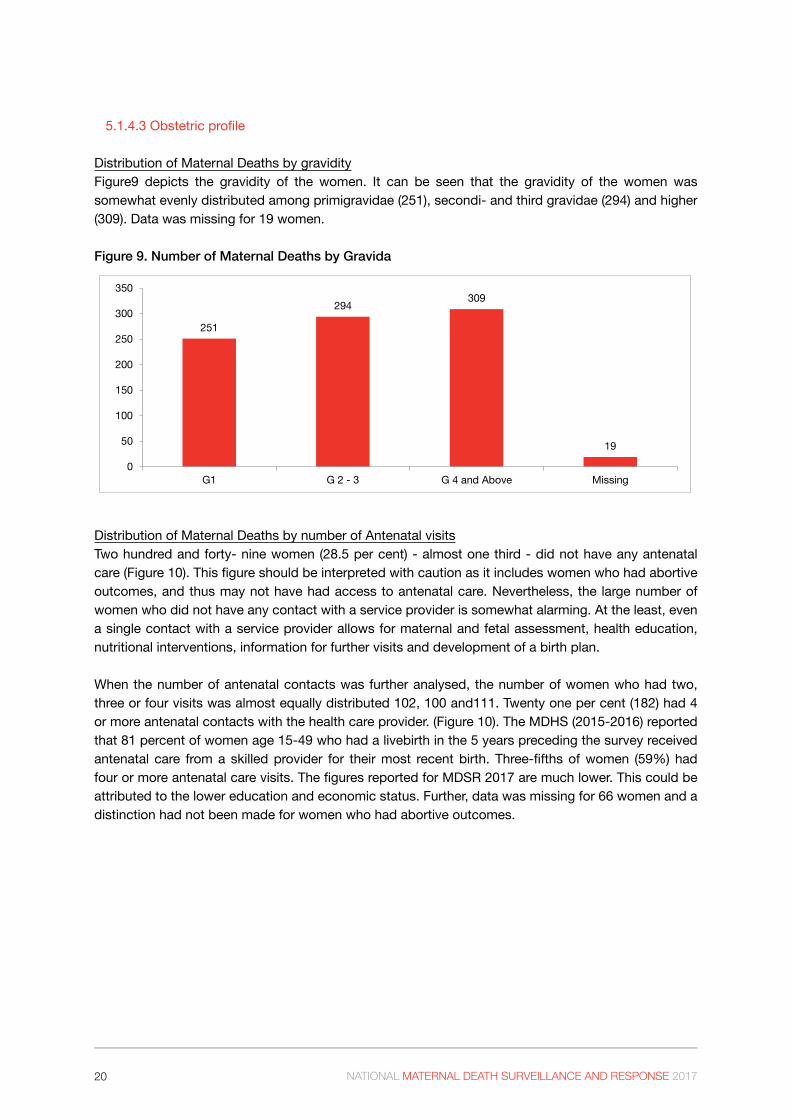
Distribution of Maternal Deaths by gravidityFigure9 depicts the gravidity of the women. It can be seen that the gravidity of the women was somewhat evenly distributed among primigravidae (251), secondi- and third gravidae (294) and higher (309). Data was missing for 19 women.
Figure 9. Number of Maternal Deaths by Gravida
251
294 309
19
0
50
100
150
200
250
300
350
G1 G 2 - 3 G 4 and Above Missing
Distribution of Maternal Deaths by number of Antenatal visitsTwo hundred and forty- nine women (28.5 per cent) - almost one third - did not have any antenatal care (Figure 10). This figure should be interpreted with caution as it includes women who had abortive outcomes, and thus may not have had access to antenatal care. Nevertheless, the large number of women who did not have any contact with a service provider is somewhat alarming. At the least, even a single contact with a service provider allows for maternal and fetal assessment, health education, nutritional interventions, information for further visits and development of a birth plan.
When the number of antenatal contacts was further analysed, the number of women who had two, three or four visits was almost equally distributed 102, 100 and111. Twenty one per cent (182) had 4 or more antenatal contacts with the health care provider. (Figure 10). The MDHS (2015-2016) reported that 81 percent of women age 15-49 who had a livebirth in the 5 years preceding the survey received antenatal care from a skilled provider for their most recent birth. Three-fifths of women (59%) had four or more antenatal care visits. The figures reported for MDSR 2017 are much lower. This could be attributed to the lower education and economic status. Further, data was missing for 66 women and a distinction had not been made for women who had abortive outcomes.

21NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 10. Number of Maternal Deaths by Antenatal Visits
249
63
102 100 111
182
66
0
50
100
150
200
250
300
No AN 1 2 3 4 More than 4 Missing
Figure 11 compares the number of antenatal visits in the years 2016 and 2017. There were 815 maternal deaths that were reviewed in 2016 and 873 in 2017. The data demonstrates a general trend that in 2017, the antenatal visits by deceased women are less. However, the comparison is between the number of visits. There is no information on the content of antenatal care, whether heath education was given or birth plans discussed.
Figure 11. Comparison of Number of Antenatal Visits in 2016 and 2017
128
54
11699
163 160
95
249
63
102 100 111
182
66
0
50
100
150
200
250
300
No AN 1 2 3 4 More than 4 Missing
Num
ber o
f Mat
erna
l Dea
ths
2016 2017

22 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Distribution of Maternal Deaths by Place of DeathFigure 12 shows that the distribution of maternal deaths by place of death is 190 at home and 133 on the way. The number of women who died at a public facility was 520. The number of women who died on the way could be surmised as affected by the first or second delay or a combination. It can also be construed that the high number of facility deaths are as a result of women reaching health facilities but at a very late stage. (See section on “delays”). Information had not been collected on whether the death occurred on transit from home to health facility or transit from health facility to health facility.
Figure 12. Number of Maternal Deaths by Place of Death
190133
1
520
15 4 100
100
200
300
400
500
600
Home On the way RHC/SC Public Hospital Private Hospital Other Missing
When the place of delivery and place of death were computed, among 258 who delivered, 190 died at home. There were women who died on the way indicating delays due to decision making and referral or transportation. When death in the health facility was analysed, 267 delivered at a health facility but 536 expired there. (Figure 13). This difference is probably due to third stage complications or late arrival. Figure 13. Maternal Mortality: Place of Delivery and Place of Death
258
6
267241
101
190133
536
4 100
100
200
300
400
500
600
Home On the way Facility Other/NA Missing
Place of Delivery Place of Death
23NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 14. Maternal Mortality by Provider at Birth
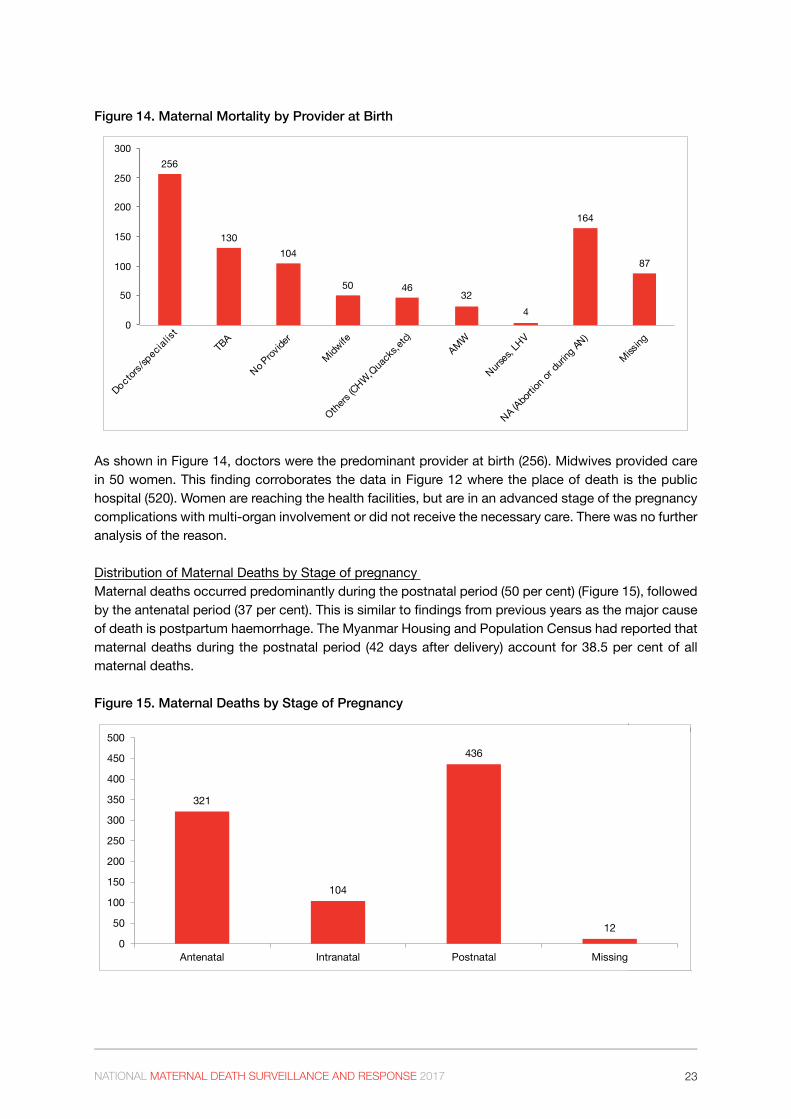
As shown in Figure 14, doctors were the predominant provider at birth (256). Midwives provided care in 50 women. This finding corroborates the data in Figure 12 where the place of death is the public hospital (520). Women are reaching the health facilities, but are in an advanced stage of the pregnancy complications with multi-organ involvement or did not receive the necessary care. There was no further analysis of the reason.
Distribution of Maternal Deaths by Stage of pregnancy Maternal deaths occurred predominantly during the postnatal period (50 per cent) (Figure 15), followed by the antenatal period (37 per cent). This is similar to findings from previous years as the major cause of death is postpartum haemorrhage. The Myanmar Housing and Population Census had reported that maternal deaths during the postnatal period (42 days after delivery) account for 38.5 per cent of all maternal deaths.
Figure 15. Maternal Deaths by Stage of Pregnancy
256
130104
50 4632
4
164
87
0
50
100
150
200
250
300
Doctors/s
pecialist
TBA
No Prov
ider
Midwife
Others
(CHW,Qua
cks,e
tc)AMW
Nurses,
LHV
NA (Abo
rtion o
r duri
ng AN
)
Missing
Percentage of Maternal Death by time
321
104
436
120
50
100
150
200
250
300
350
400
450
500
Antenatal Intranatal Postnatal Missing
24 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 16. Abortion-Related Deaths
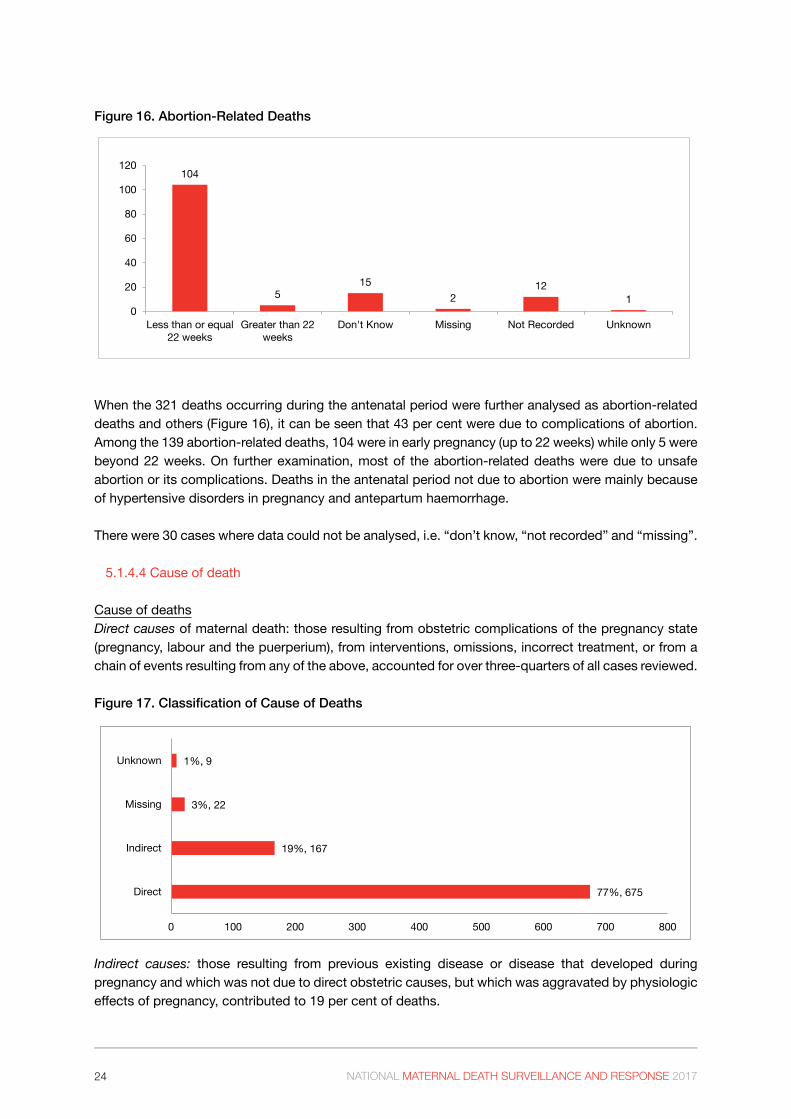
When the 321 deaths occurring during the antenatal period were further analysed as abortion-related deaths and others (Figure 16), it can be seen that 43 per cent were due to complications of abortion. Among the 139 abortion-related deaths, 104 were in early pregnancy (up to 22 weeks) while only 5 were beyond 22 weeks. On further examination, most of the abortion-related deaths were due to unsafe abortion or its complications. Deaths in the antenatal period not due to abortion were mainly because of hypertensive disorders in pregnancy and antepartum haemorrhage.
There were 30 cases where data could not be analysed, i.e. “don’t know, “not recorded” and “missing”.
5.1.4.4 Cause of death
Cause of deathsDirect causes of maternal death: those resulting from obstetric complications of the pregnancy state (pregnancy, labour and the puerperium), from interventions, omissions, incorrect treatment, or from a chain of events resulting from any of the above, accounted for over three-quarters of all cases reviewed.
Figure 17. Classification of Cause of Deaths
Indirect causes: those resulting from previous existing disease or disease that developed during pregnancy and which was not due to direct obstetric causes, but which was aggravated by physiologic effects of pregnancy, contributed to 19 per cent of deaths.
104
515
212
10
20
40
60
80
100
120
Less than or equal22 weeks
Greater than 22weeks
Don't Know Missing Not Recorded Unknown
77%, 675
19%, 167
3%, 22
1%, 9
0 100 200 300 400 500 600 700 800
Direct
Indirect
Missing
Unknown

25NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Direct causes of deathWhen the direct causes of death were further analysed in accordance with ICD-10-MM coding, obstetric haemorrhage was the commonest followed by pregnancy with abortive outcomes and hypertensive disease in pregnancy (Figure 18).
PPH, abortion, HDP and medical diseases complicating pregnancy are the major causes of maternal deaths. Interviews with key informants from states and regions corroborated this analysis. Their major concern was PPH in which a woman’s condition can deteriorate rapidly before she can be transferred to a health facility. Mismanagement of the third stage of labour during home deliveries leading to uterine inversion was also mentioned.
Figure 18. Cause of Deaths by Direct Group
Out of a total of 235 cases who succumbed from obstetric haemorrhage, a large number - 197 (84 per cent) were due to postpartum haemorrhage (Table 2). While this has been a consistent finding in the previous maternal death reviews, the number has declined, comprising 23 per cent compared to figures reported from previous years as 30 per cent (2015) and 29 per cent (2016).
Unanticipated complications of management accounted for 11 per cent – mainly due to anaesthetic accidents during pregnancy and labour or from cardiovascular or neurological complications.
Table 2. Deaths from Obstetric Haemorrhage
Group 3 – Obstetric haemorrhage # TOTAL %
Postpartum haemorrhage 197 84%
Antepartum haemorrhage 19 8%
Other obstetric causes 19 8%
235 100%
21%, 139
19%, 130
35%, 235
5%, 35
8%, 56
11%, 77
0%, 3
0 50 100 150 200 250
Group 1 - Pregnancy with abortive outcome
Group 2 - Hypertensive disorders in pregnancy, childbirthand the puerperium
Group 3 – Obstetric haemorrhage
Group 4 – Pregnancy-related infection
Group 5 – Other obstetric complications
Group 6 – Unanticipated complications of management
Others

26 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Indirect deathsPre-existing medical diseases, other maternal diseases, diseases of the respiratory and circulatory systems were the commonest among the indirect causes. In 2017, H1N1 contributed to deaths due to superimposed pneumonia. Malignant neoplasms and diseases of the blood and blood-forming organs together contributed to other medical causes of indirect deaths.
Figure 19. Cause of Deaths by Indirect Group
Many women are not aware that they have an underlying medical condition which became worse during pregnancy.
Other maternal diseases include anaemia in pregnancy. While the level of anaemia was not determined, Myanmar DHS (2015-2016) reported that just under half (47 per cent) of women age 15-49 are anaemic; most of these women have mild anemia. Pregnant women are more likely than non-pregnant women to be anaemic (57 per cent versus 46 per cent). Thus, they cannot withstand even a small amount of blood loss during pregnancy, delivery or the postpartum period.
Indirect causes, attributable mainly to medical diseases were considered in detail according to ICD-10-CM codes for the 2017 MDSR report. The analysis highlighted the inherent risks faced by many women with severe cardiac or pulmonary diseases or malignant neoplasms as a result of an untimely pregnancy.
Myanmar is going through a phase in the obstetric transition where the mortality is still high, fertility is variable and direct causes of mortality still predominate. This is a complex stage because access remains an issue for a much of the population, but as a greater proportion of pregnant women start reaching health facilities, quality of care becomes a major determinant of health outcomes, especially with regard to overloaded health facilities. In order to further reduce maternal mortality, addressing quality of care issues and eliminating delays within health systems are critical measures.
3735
28
24
128
6 5
12
0
5
10
15
20
25
30
35
40
OthersOther maternal diseases
classifiable elsewhere but complicating pregnancy,
childbirth and the puerperium
Pre-existing medical diseases
Diseases of the respiratory
system
Diseases of the circulatory
system
Diseases of the digestive
system
Malignancies Infections Diseases of the blood

27NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 20. Cause of Deaths by all Groups
Figure 20 summarizes all the causes of death as classified by ICD-10. Among all deaths, PPH remains high, followed by Indirect causes at 19 per cent. Pregnancy with abortive outcomes form 16 per cent and Hypertensive disorders in pregnancy, childbirth and the puerperium 15 per cent.
Pregnancy with abortive outcome
(139)15.9%
Hypertensive disorders in pregnancy, childbirth and
the puerperium(130)
14.9%
Postpartum haemorrhage(197)
22.6%
Antepartum haemorrhage & others
(38)4.4%
Pregnancy-related infection
(35)4.0%
Other obstetric complications
(56)6.4%
Unanticipated complications of
management(77)
8.8%
Other direct causes(3)
0.3%
Indirect causes(167)
19.1%
Missing (22)
2.5%Unknown
(9)1.0%

28 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
5.1.5 Contributory factors: the delay model
Delays in seeking, accessing and receiving care during obstetric emergencies are usually classified into three categories.
• Delay 1 refers to the time from the start of a woman’s illness to the time the problem is recognized as requiring care;
• Delay 2 refers to the time from acknowledging a problem to reaching an appropriate health facility; and
• Delay 3 refers to the time from arrival at a care facility to receiving the requisite treatment (Thaddeus and Maine, 1994).
Delay 1 was reported for 367 (42 per cent), a combination of Delays 1 and 2 for 159 (18.2 per cent) and Delay 3 for 68 (7.8 per cent) cases. While Delay 1 and Delay 2 can potentially occur for any death (due to poor recognition of the problem and difficulties in accessing a facility), Delay 3 can only be recorded for deaths while (or after) the woman has reached a facility and thus by definition will occur among a smaller proportion of all reported deaths.
When the type of delay was analysed, the first delay or a combination thereof, was the commonest.
The first delay - the decision to access careInformants communicated additional information during interviews regarding why the decision to “wait and see” was made.
“If the woman has delivered before, she and her family have a false sense of security that the delivery will proceed without major issues.”
“In women who have induced abortion, they are worried about the possible punitive measures and fear of repercussions by the community. Furthermore, they have faith in the traditional birth attendant who has reassured them that after some bleeding, spontaneous expulsion will occur.”
“Even though most of the care is free in the hospitals, there is still some out-of-pocket expenditure as you still need to buy medicines.”
“In remote areas, the family first seeks the help of the Traditional Birth Attendant, then if there is no progress, the auxiliary midwife is consulted. Some AMWs were trained a long time ago with no further refresher training so their skills are just a little better than the Traditional Birth Attendant. When the woman’s condition does not improve, then the family looks for the midwife or for transport.”
An inability to recognize an emergency may extend the delay in the decision to seek care. While the ability of the patient or a caregiver to recognize an emergency is partially dependent upon the patient’s or caregiver’s level of health literacy, often true obstetric emergencies may not be perceived as emergencies in areas where they commonly occur. A woman can be influenced by the elders or caregivers who have traditional or cultural beliefs which will affect both the ability of women to decide to seek care and their subsequent ability to reach care.
In summary, lack of information and inadequate knowledge about danger signs during pregnancy and labour; social hierarchy that restricts women from seeking health care; and limited resources/family poverty attributed to the first delay.

29NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Figure 21. Maternal Deaths by Type of Delay
The second delay - the identification of - and transport to - a medical facilityGeographical remoteness of some communities led to difficulty in reaching health facilities due to poor road infrastructure (especially in the rainy season), communication networks and community support mechanisms. Limited or lack of public transportation, was highlighted as a barrier in access.While there are vehicles organized by volunteer organizations, a nominal fee is charged for gasoline and remuneration for the driver, which the family might not be able to afford. Time and opportunity costs and in some places, security concerns may prevent a woman from reaching a facility in time.
The following are excerpts from interviews with key informants:
“Among the low-income population, costs of transfer to hospital and costs of hospitalisation and loss of income leads to hesitancy to seek care at hospitals”.
“Sometimes the vehicle is there, but the ‘driver’ is working in the hills”
“Often there is no facility within a reasonable distance. It takes a long time to reach a health facility ”
Difficult access remains an issue in certain areas in Ayeyawaddy region and Chin, Shan and Kachin States and women cannot get to facilities in a reliable or affordable way.Being the front-line health worker, it was felt that some midwives need to play a more leading role: they are in a position to recognise complications and persuade the family of the importance of referral to a health facility at a higher level. However, it was also acknowledged by the Township Health Department that the midwife needs to cover a number of villages and is often not in a position to attend to all deliveries.
An example was given during interviews that good road access will reduce maternal mortality which then becomes recorded as a “maternal near miss”. Arrangements were to transfer a complicated obstetric case from Yamethin (Mandalay region) to Nay Pyi Taw where overall travel time takes one hour instead of referring her to Mandalay (which takes three hours or more). The access to tertiary level care saved the woman’s life.
367
159
2250
20 8
68 76 6241
0
50
100
150
200
250
300
350
400
30 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
The third delay - the receipt of adequate and appropriate treatmentThe facility readiness or otherwise of Station or Township hospitals, in particular Station Hospitals, was identified as an area to be improved on, in the recommendations/responses and mentioned during interviews. With respect to human resources, there are vacant posts of medical officers. It was also mentioned that surgical skills were lacking (e.g. for caesarean section) and unanticipated complications can result. Further, the timely recognition and referral of complicated cases was wanting, leading to delayed arrival at the next level facility. For blood transfusions, there is still a reliance on living donors. Anaesthetic accidents were also noted. During interviews, it was mentioned that although spinal anaesthesia was the preferred method for emergency LSCS, not all medical officers have the skills to perform it.
Emergency medical officers in district or tertiary level facilities need to be vigilant that women of reproductive age who are admitted for other symptoms e.g. diarrhoea could have pelvic abscess following abortion.
Respondents from a few tertiary/university hospital noted that:
“In the past year, we have had medical officers who have completed three years training in acute medicine – the A&E doctors who are based in the emergency department of our hospital. Since their placement, we have had early recognition of obstetric emergencies, rapid resuscitation and prompt referrals which has improved the situation dramatically.”
For medical officers in maternity Ob-Gyn wards, the choice of (less potent) antibiotics for severe sepsis and(delayed) timing of surgical intervention which compromises the care received by patients.
Respondents from Southern Shan State mentioned the need for a constant supply of emergency medicines.
In tertiary level facilities where problematical cases end up, the limited number of beds in the Intensive Care Unit and nursing staff trained in providing such care affected the patient’s outcome.

31NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
5.1.6 Review Committees
Membership on regional/state, tertiary hospital and central MDSR committees ranged from ten to 14 providers. Nearly all MDSR committees were interdisciplinary in their composition, including hospital administrators, paediatricians, obstetricians, nurses or midwives, forensic medicine specialists, and pathologists. In addition, the committee invites the attending doctor or nurse at the time of death to the meeting. After completing the background data and obstetric characteristics, the committee discussed the cause of death and classification and the contributing factors. Suggestions to improve the quality of management at facilities and address the three delays were made and action planned.
Across the health facilities the frequency of mortality audit meetings differed. While an attempt was made to hold meetings within the suggested time frame, factors such as natural disasters, public health emergencies and competing priorities led to deferring meetings. Further, MDSR meetings had to be held in conjunction with other meetings as there were no financial resources for travel or for convening review meetings. As such, meetings were often focused to discuss on a few selected cases that were particularly problematical in terms of classification of delays or cause of death. Common challenges were incomplete forms with respect to socio-demographic and obstetric parameters and entries regarding cause of deaths at home. Often, hospital case records, antenatal records and post-mortem findings were not sent together with the reporting forms. The output of the meetings is to recommend solutions and implement recommendations (see Section 5.2).
The states/regions could hold more meetings in the second half of the year. In 2017, at least one review meeting was held in all states and regions. Seven of the states/regions held two meetings and one state held three meetings. There were two states where review meetings could not be held due to prevailing local circumstances – internal conflict. Furthermore, additional review meetings were held in the first quarter of 2018 as part of the MDSR review for 2017.
32 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
5.2 ResponseWhile aggregated data from annual reports provide information shared by many facilities or communities, analysis of individual cases lead to more specific responses. A summary of some of the action-oriented responses are given below.
5.2.1 Specific
Human resourcesImprove knowledge and skills of midwives with additional training – this has taken place in a few townships, particularly for prevention and management of PPH. When a case of uterine inversion occurred, refresher training was arranged on third stage management and BEmONC for midwives.Reinforce auxiliary midwives performance with refresher training – this has taken place in a few areas for prevention and management of PPH, namely conduct of the third stage of labour (e.g. Southern Shan State).
Linking BEmONC with MDSR – some townships have addressed preventable causes of maternal mortality by linking MDSR with BEmONC training.
Staffing levels - The issue of staff vacancies was addressed by local administrators/Health Departments e.g. a medical officer was deployed to a township hospital (Northern Shan State). Organisation of AMW training took place at Nam Khan Hospital with state/regional funds with the objective that all villages have an AMW in place.
Health facilityInterventions at health facilities were on improving quality of care for women with obstetric emergencies and promoting adherence to evidence-based guidelines.
Stringent monitoring of labour was reinforced after a death from intrapartum shock.
Ensuring that clinical guidelines were strictly followed for pre-eclampsia/eclampsia and severe sepsis.
Joint care by physician and obstetrician instituted for management of medical disease in pregnancy in tertiary level facilities.
Anaesthesia training – while having an anaesthetist on-site would prevent the complications from anaesthesia, in the meantime medical officers who will be posted to township or station hospitals will need training on anaesthesia. This has been arranged previously by the Ministry of Health and Sports.
Community levelImproving community knowledge and health education including risk factors and dangers signs during antenatal care and the need to improve health seeking behavior.
Conducting outreach antenatal care in camps for internally displaced persons in certain states.
Ensuring iron supplements are provided to all women attending AN care.
Encouraging uptake of ANC and having birth preparedness and complication readiness plans in place.
Improving referral mechanism where delays were observed. An example was given by respondents
33NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
following a death due to antepartum haemorrhage where a revolving fund was set up to provide support for transportation to health facilities during labour. In Mon State, co-ordination with local authorities helped to set up a self-help referral system.
Information on and availability of contraceptive services, particularly for young women working in garment factories in peri-urban areas.
5.2.2 General
Health education and promotion programmes on sexual and reproductive health, contraception for healthy spacing and timing of pregnancy, nutrition, antenatal care, changing traditional practices at home, birth planning-advice on danger signs and emergency preparedness, came out strongly from all states and regions, both in the recommendations from the MDSR reviews as well as key informant interviews. A few townships have co-ordinated with Village Health Committees to conduct these programmes.
Induced abortion remains a major problem in all states and regions. While medical officers and midwives received basic training on family planning, not all have received refresher training and are not familiar with newer methods such as implants and emergency contraception. Furthermore, community support for transport and identification and prompt referral of women with complications of unsafe abortion would have an impact on preventing deaths from unsafe abortion.
Information on the dangers of unsafe abortion, the need for timely referral and post-abortion care and contraception is critical in urban and peri-urban areas of large cities. Interviewees from these areas reported that women use misoprostol tablets to initiate the abortion process and are then admitted to hospital. These women have a better outcome and become “near miss” cases. However, in rural areas, the use of intravaginal chemicals and mechanical means lead to injury to the genital tract, pelvic infection and other serious complications such as Adult Respiratory Distress Syndrome (ARDS) or renal failure.
5.2.3 Activities conducted by MRH Division
There are ongoing activities conducted by MRH Division that are contributing to the response to improve quality of care and reduce maternal deaths: training on BEmONC and CEmONC for doctors and midwives, family planning, management of post-abortion complications, among others. To prevent postpartum haemorrhage, auxiliary midwives are now allowed to dispense oral misoprostol for third stage management. Further, the section on contraception has been expanded in the AMW manual (2018) and in addition to dispensing oral contraceptive pills and condoms, they can now provide subcutaneous injection depot provera.
Recently MRH Division has convened a technical meeting to review and amend the medical indications for female sterilization and the administrative procedures required. The outcome of the meeting was a relaxation of medical indications for female sterilization and elimination of a few of the administrative procedures required. This is particularly relevant for mothers who died of indirect causes which account for approximately one-fifth of all deaths. These women with underlying medical diseases, (cardiovascular and respiratory conditions) malignant neoplasms, diseases of blood and blood forming organs for whom physiological changes in pregnancy will tip the scales against them.

34 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017

35NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 6. Benefits of Institutionalizing MDSR SystemThe following quotes and observations were based on interviews with representatives from Maternal and Reproductive Health Division, Department of Public Health; Health Departments of States and Regions from different levels - state/region and township - including MDSR focal persons; professors and staff from university/teaching hospitals; and representatives of United Nations agencies involved in the MDSR process (See Annex 2 for List of Persons interviewed).
Awareness of MDSR processAll respondents reported a high level of awareness of the MDSR process and Technical Guideline for Action to End Preventable Maternal Deaths in Myanmar (referred to henceforth as “Guideline”) among themselves and their staff. The state/region and township health teams and hospital staff were more aware of the importance of collecting mortality data and notifying authorities regarding maternal deaths. Most teams had a systematic practice of reviewing the causes and avoidable factors related to maternal deaths in the community and facilities and developing recommendations based on the reviews. One or two MDSR focal points/persons were assigned in state/region or township health departments and hospitals to notify and follow-up on each maternal death.
The stark reality of issues faced by patients were seen at first-hand by the township teams conducting verbal autopsies and community-based reviews and central level teams on their monitoring visits.
“Families move to the paddy fields during the planting season and live in huts in the fields. It is impossible for any vehicle to navigate through the fields to reach a woman who has an obstetric emergency and then take her to hospital”. (Ayeyawaddy region)
“The woman had to be brought to the main road by a bullock cart, and then transferred to a car so it takes a long time for her to reach a hospital”. (Magway region)
Township Health Departments have made positive progress in reporting maternal deaths. They notified the deaths through Instant Messaging and communicate and exchange information on Instant Messaging platforms within which there are interest groups. State/regional authorities used mobile phones to follow-up on data in incomplete forms.
The MDSR teams put in persistent efforts to understand who, where, why, and when maternal deaths were occurring. This was of particular importance as the deaths are required to be reported from the residence of the deceased. In addition, when a woman is transported from one hospital to another and subsequently dies and communication between hospitals may be limited, diligence of the individual collecting data is of particular importance.
“The deceased woman was from a village in Amarapura. She first went to Sagaing Township Hospital, then Amarapura Township Hospital when she was assessed and transferred to Mandalay Central Women’s Hospital. From there, she was moved to the neurological ward where she passed away. The Township Health Nurse from Amarapura traced her steps to get a complete picture of what led to her death.”
At township level, the teams compiled all relevant information and produced a summary report of each maternal death investigated, before the state/regional level MDSR team maternal death reviews.
36 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Review and analysis of the cause of deathDuring the reviews, a culture of “no name, no blame” and “no fault-finding” was encouraged. As a result, more precise information was obtained for the cause of death compared to previous years.
ResponseResponses to MDSR reviews has taken place at all levels of the health system, all health facilities and all administrative levels as well as in the community. Some of the specific response measures for human resources, health facility and community have been detailed in the section 5.2.
Standardised guidance for identifying high risk obstetric cases, social determinants and actions that might prevent the same chain of events occurring in future was appreciated by interview respondents. Linking responses directly to every death gave staff confidence that they were acting appropriately, based on empirical evidence.
In addition to the on-going activities/responses mentioned in Section 5.2 Response, the MRH Division in collaboration with respective state/region and township health departments have initiated specific measures based on preliminary findings of the data. For example, in periurban Yangon, as a result of high number of deaths in young women from unsafe abortion complicated by sepsis, sexual and reproductive health information was intensified together with availability of contraceptive services.
37NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 7. Challenges
This section discusses on the experiences and critical challenges faced thus far, and suggests improvements to overcome them.
7.1 Notification and reporting
7.1.1 Community
The notification and reporting of maternal deaths from the community was one of the biggest challenges identified. Although the guideline clearly stipulates that all facility and community level maternal deaths should be reported within 24 and 48 hours of occurrence respectively, several challenges like communication, hindered timely reporting of deaths to districts. This was partly overcome by the use of Instant Messaging and mobile phones.
The wrong address is often given when maternal death occurs in women living in peri-urban areas in large cities or migrants in these areas. This is particularly for women who had induced abortion as the family fear consequences of being found out and action taken for induced abortion. Often, the woman’s family cannot be traced. In the Ayeyawaddy delta, families cannot give permanent addresses as they live on boats and are very mobile and thus difficult to locate. Verbal autopsy cannot be conducted as the families cannot be contacted after the funeral.
In conflict areas it is very difficult to get precise numbers or to conduct verbal autopsy to complete forms.
The township teams found out through experience that verbal autopsy and enquiry into socio-cultural and behavioral factors have to be conducted in a sensitive manner. It is difficult to get the precise diagnosis for the cause of death of women who died in the community as the description of events occurring around the time of death can be rather vague and could be attributed to different causes. Often, the individual who is responding to the team might not have been the care-giver. While the expectation is for the Township Medical Officer (TMO) to lead the field investigation, this does not always occur due to competing work priorities. The Township Health Nurse or midwife may not always be able to arrive at the precise diagnosis. This is partly because the forms are in the English language and the midwives may not understand the forms.1 To overcome this, some midwives completed the forms in Burmese. The TMO does review the completed forms.
ICD codes: The MDSR teams at township level found the assignment of ICD codes challenging. In tertiary hospitals, more details could be obtained: e.g. whether PPH was third-stage hemorrhage or other immediate postpartum hemorrhage or delayed and secondary postpartum hemorrhage or postpartum coagulation defects. They were following instructions that were short on details. While the detailed codes could be accessed from the website they could not give sufficient time to be familiar with them.
1 A Burmese translation of Form A has been made by MRH Division and will be put to use soon.
38 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
7.1.2 Health facilities
Women who were dead on arrival at health facilities pose a particular problem in collecting data, for compassionate reasons. While forms are completed to the extent possible, follow-up visits are necessary and pose problems with incorrect addresses or family’s reluctance to give interviews.
In tertiary hospitals where there are sufficient numbers of staff, all women who are in-patients, and are in serious condition have the information collected during admission. Eventually, some women may fall into the “maternal near miss” category: a woman who nearly died but survived a complication that occurred during pregnancy, childbirth or within 42 days of termination of pregnancy; whereas others would be maternal deaths. This procedure ensures that the pertinent facts are collected for all maternal deaths.
In some cities, collecting data across tertiary facilities can be challenging as the staff in wards in the General Hospital to which the woman is transferred out are not aware of MDSR process. On a few occasions, women are sent home in a moribund state.
Incomplete notes that contained limited details of the background data of the women, minimal information on case management, and missing antenatal and referral notes affected the quality of data available for analysis.
Post-mortem is usually not carried out at station and township hospitals for the main reason of “relatives deny permission”.
There is change of staff and there are medical superintendents (MS) and TMOs and MOs in hospitals who are not fully aware of the MDSR system and their respective roles. State/Regional administrators said that newly appointed medical officers are not aware of the MDSR process nor how to report.
7.2 Transmission of forms
A misunderstanding exists regarding when the forms should be transmitted, i.e. while Form B should be returned within 21 days to state/region offices; some hospitals wait till the hospital review meetings have been conducted. If these meetings occur at the end of the month as planned, the transmission is not delayed. However, if the meetings take place only in three months time, there is a delay in receiving forms at the state/region level, which leads to delay in reviews.
Zero reportingA key feature of active reporting means that there is “zero reporting” even when there are no deaths to be reported. Zero reporting was not mentioned in the reports.
7.3 Analysis
The causes of deaths were not accurately stated on reporting forms. As such, the MRH Division and Trainers should consider providing additional training on cause-of-death classification, aligned with the ICD-10-CM (which includes ICD-10-MM), because accurate classification informs the type and quality of responses developed by audit committees.

39NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
7.4 Review
At different levels, meetings could not be conducted as planned. This has been elaborated in Section 5.1.5. As a result, there are often a surplus of cases that need to be reviewed and which limits discussion on preventable or avoidable factors relating to the death, and of appropriate analysis and interpretation of the data collected; which should lead to the generation of evidence- based recommendations.
All Townships level and Hospital Level MDSR teams could not submit reports at the stipulated time to State and Region Department of Health because some did not have the quorum number of members nor was there a head of department to endorse and complete the process due to competing or emergency tasks. State and Regional-led teams began formal review meetings as of June 2017 though it was meant to hold them every three months. The reasons for delay in reviewing at State and Regional level were similar to those at township and hospital setting. Nevertheless, almost all states and regions could hold two meetings in the second half of 2017.
A central level MDSR review meeting was held in December 2017 where all State and Regional Level MDSR focal persons presented on their experiences on MDSR in their respective areas. All States and Regions could provide updates for different periods during 2017.
7.5 Response
As the “Response” of MDSR has been emphasized, there were efforts at different levels from both the Department of Public Health and the Department of Medical Care to act on the findings and recommendations. Committees should craft recommendations for immediate action that are specific, possible to carry out, and measurable. Actions need to be prioritized and delegated to individuals according to their skills.
Most respondents mentioned that there was not a formal process for follow-up of recommendations apart from reviewing minutes at the next mortality audit meeting, i.e. the follow-up of the extent of implementation of recommendations is still weak. This surveillance approach emphasizes the need to close the “loop”. The process itself requires ongoing monitoring and evaluation to ensure that it is functioning effectively. As 2017 is the first year of roll-out and implementation of MDSR in Myanmar, 2018 and 2019 will allow for the review of recommendations from the previous year and lessons learned including implementation challenges; which have been presented in this report.
7.6 Other issues
Representatives from states/regions and townships mentioned that Traditional Birth Attendants (TBA) were still performing inappropriate and harmful practices for women in labour. Thesepractices led to cases of uterine inversion, uterine rupture and introduction of infection. Similarly, interference in early pregnancy by mechanical methods led to abortion with severe sepsis. This community-related factor cannot be ignored and needs to be addressed in a sensitive and locally appropriate manner.
In a few townships, TBAs were asked to join community education sessions, particularly in relation to “Do’s” and “Don’ts” during labour and using harmful practices to procure abortion. It is not yet clear what the outcome was.

40 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017

41NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 8. Recommendations
8.1 Recommendations to improve the surveillance functions of the system
While the Departments of Public Health and Medical Care in collaboration with the MRH Division has advanced in implementing the MDSR system, there is still room for improvement. In general, timeliness of reporting, improving the data quality and coverage and analysis will need to be reinforced.
Re-sensitisation and re-training of administrators and others engaged in MDSR processAs there has been transfers among the Medical Superintendents and staff, and new medical officers and midwives have been recruited, there is still a need for training on the process, notification, completing forms and ICD-10-CMand ICD-MM coding. The correct assignment of cause of death using ICD-MM Guidelines should include clear direction on standards for classifying maternal and perinatal deaths, such as The WHO Application of ICD-10 [International Classification of Diseases, 10th revision] to Deaths during Pregnancy, Childbirth and the Puerperium (ICD-MM).
This classification ensures that there is only one underlying cause of death. The underlying cause is the disease or condition that initiated the chain of events that led to the death. Contributing factors are then identified that may have increased the risk of dying. The immediate cause is the condition that directly resulted in death.
The organizational set-up and administrators of MDSR and focal persons/implementers of MDSR have not always been the same. For example, Assistant Directors are members of the MDSR team and together with TMOs, need to be trained on MDSR.
Analysis at township levelsThe preventability of the index maternal death, encompassing social-behavioural factors and medical care is critical at this level which is close to the communities. Analysis at township levels will also stress on the actionable factors at Township and Station health facilities. In addition, as the TMOs, MOs, Township Health Nurses and midwives are familiar with the communities they serve, processes for reviewing community deaths, providing feedback to community as well as for sharing and tracking recommendations with community health workers (CHWs) and at health centres will need to be reinforced.
Conduct regular reviewsIn addition to township reviews, ensuring regular audits and feedback opportunities at referral hospitals will lead to continuous quality improvement. It is recommended that a committee to review a maternal death should meet shortly after the death has occurred, while the events that took place are still fresh in the memories of all relevant parties.
Convene knowledge and experience sharing meetingsSharing of positive and negative experiences and good practices among different levels in same State and Region followed by national level.
Allocate a dedicated budgetAt the moment, doctors, midwives and other personnel participate, without extra pay, in the intensive process of assessing cause of death, preventable conditions and contributing factors. Travel costs are “out-of-pocket” and a dedicated budget will be needed to conduct verbal autopsies and to conduct regular reviews at every level of the health system.
42 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Attention to missing dataA number of forms did not have data entered for education, occupation and antenatal visits. Efforts must be made to obtain complete data sets when the data collector (midwife, township health nurse or doctor) contacts the bereaved family for verbal autopsy or for completion of the Hospital Form.
Zero reportingMaternal Death Reporting should be an active process whether or not a death has occurred. If no maternal death has occurred a ‘zero’ should be captured to demonstrate attention has been paid to the tracking of maternal deaths.
8.2 Recommendations to improve the Response
Implementing MDSR will contribute to the Strategic Objectives (SO) of the Ending Preventable Maternal Mortality Strategy (EPMM) Strategy. The data and information generated will contribute directly to the objective of “Ensure accountability to improve quality of care and equity” by strengthening MDSR and perinatal death surveillance. The findings of MDSR will play a significant role in the strategic objective to “Address causes of maternal mortality and morbidities and related disabilities”.
When MDSR review committees identified local determinants of deaths, they could put into place responses that fit into existing and budgeted annual plans, for example, improving transportation and referral systems, increasing community awareness, promoting institutional delivery, and strengthening service quality. MDSR will thus be perceived as synergistic with ongoing activities, facilitating prioritisation rather than introducing new demands.
There are several on-going activities organized by MRH Division which have direct applicability to the findings from MDSR reviews. However, the coverage needs to be broadened particularly to reach underserved areas and an emphasis on quality of care reinforced.
It will add to accountability if the responses suggested are time-bound withsystematic processes for tracking implementation of action plansand monitoring outcomes.
CommunityAs most of the maternal deaths occurred in families with low education level and low socio-economic status and poor health literacy, almost all respondents underlined the fact that the population needs increased awareness on how to maintain general health, nutrition and screen for specific medical conditions especially cardiac disease. In addition, health education of the community regarding antenatal care, delivery with Skilled Birth Attendant or institutional delivery where possible, detection of high-risk cases –Hypertensive Diseases in Pregnancy, danger signs in pregnancy and postnatal care, should be enhanced.
Birth preparedness and complication readiness will need to be reinforced by midwives during the antenatal period. This includes four major components: 1) saving money; 2) arranging transport; 3) identifying a blood donor; and 4) identifying a skilled provider. It is not only the woman and her husband with whom these discussions need to take place but also friends, neighbours and other family members who are information sources.
Sexual and reproductive health information and contraception to prevent unsafe abortion should continue to be part of MRH Division’s annual plans. While the method mix will be expanded, the availability of long acting reversible contraception (LARC) – IUDs and contraceptive implants and post-
43NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
partum family planning will be enhanced. Commodity security will be ensured through strengthening the logistics management information system for medicines, equipment and other supplies for MNH care. However, it is vital that remote and underserved areas are reached through locally appropriate means.
Improved referral mechanisms using conditional cash transfers or community-based transport systems will need to be further explored to address the barriers due to the first and second delays. A communication system needs to be set up between the field care givers (MW or AMW) and the facility staff to streamline referral.
Human resourcesImproving competencies– An ongoing activity ensures that maternity care providers receive regular mandatory updates in emergency obstetric care, including adequate training at lower levels of care to improve capacity to resuscitate women and adhere to protocols for transfer of critically ill women. It is imperative the training links MDSR with BEmONC.
Training of a new batch of auxiliary midwives will take place using an improved curriculum. The management of PPH, the recognition of danger signs and referral of women, family planning and nutrition have been underscored. The AMWs will be posted as a temporary measure to villages where there are currently no midwives.
Training of newly appointed and newly deployed Station Medical Officers (SMO) on BEmONC, surgical and anaesthetic skills and early recognition of cases for referral to the next level health facility, before they are in position as SMOs, was stressed by state/regional and tertiary level respondents. Additionally, they need to be conversant with MDSR system. This action will need to be acted on by central level or by state/regional health authorities.
Adherence to updated treatment guidelines, i.e. evidence-based guidelines for PPH, hypertensive disease in pregnancy and severe sepsis is a requisite in all health facilities.
FacilitiesCEmONC facilities with the capacity to provide 24/7 services need to be expanded in underserved and remote areas under the leadership of the central and/or state/regional authorities.
Measures to improve blood banking facilities which depends on the availability of electricity will need the co-ordination with and co-operation of township administrative authorities.
A well-equipped Intensive Care Unit (ICU) with optimal nursing care at tertiary and university hospitals for women with ARDS, pulmonary embolism, heart disease etc is a necessity to reduce maternal deaths.
Pregnancy in women with pre-existing medical disease is becoming increasingly common as the treatment of many chronic conditions improve. Women with underlying medical conditions are at increased risk of developing complications in pregnancy which may be associated with significant maternal and fetal morbidity.Joint care by an Ob Gyn and Physician team for medical diseases in pregnancy will improve their outcome.
44 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
8.3 General recommendations
Since September 2016, maternal deaths have been declared a notifiable event in Myanmar within 24 hours from the death.This data collection runs parallel to vital statistics, and ideally one should feed into the other. Maternal death as a notifiable event should be integrated with disease surveillance and response.
The MDSR report should be used to raise awareness among senior officials and policy-makers, as well as community leaders and members so that a coordinated local and national response to prevent future deaths can be developed. It is essential that those persons with the ability to promote and effect the necessary changes be involved in the process of national review. Recommendations that are realistic and can be done locally are an important element of the “Response”
In addition, the MDSR report can inform hospital administrators to improve the quality of maternity care, identify areas for skills building and refresher training. The report can be used to strengthen referral networks and assist in developing health promotion messages.
As newly posted medical officers and midwives are not familiar with MDSR system, it should be included in undergraduate medical curriculum in discussions on maternal mortality reduction. Similarly, it needs to be included in undergraduate nursing/midwifery curriculum in discussions on maternal mortality reduction.
In future MDSR Reports, real-time examples of actions taken in facilities and communities and a measurable response to these will be invaluable. During the preparation of this report, key informant interviews with officials and clinicians from different administrative levels of states and regions added a depth of understanding to the MDSR system. In future reports, it would be valuable to include the perspectives of the community.

45NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Chapter 9. Conclusion
The nationwide initiative to conduct death audits, the national MDSR guideline, and nationwide use of MDSR tools for all cases of maternal deaths in the community and health facilities demonstrate strong political will to improve maternal and newborn health. The commitment of the MRH Division and representatives from state/region, township Health Departments and staff from health facilities was notable during the interviews. There has been an overall improvement in notification and reporting of maternal deaths from previous years, reviews have been conducted and actions/responses taken both at the community and facility levels.
Health staff are aware of the causes and determinants of death, and analysing these data to select responses that will prevent similar events in future. Immediate action has been taken at facility levels and for human resources to the extent possible.
The primary goal of MDSR is to eliminate preventable maternal mortality, with the overall objective “to provide information that effectively guides immediate as well as longer term actions to reduce maternal mortality and the impact of actions to reduce it”.MRH Division has developed the Ending Preventable Maternal Mortality Strategy 2017-2021 (EPMM)with the following Goals:
• To reduce maternal mortality ratio from 282 per 100,000 live births (2014) to less than 91 per 100,000 live births by 2030
• To reduce neonatal mortality rate from 26 per 1000 live births (2015) to less than 12 per 1000 live births by 2030
• To reduce the stillbirth rate from 20 per 1000 births (2009) to less than 10 per 1000 births by 2035
• To reduce the prevalence of anaemia in pregnant women from 57 percent to 28 percent • To reduce the adolescent birth rate from 33/1000 births (2015) to less than10/1000births
by 2020
As part of its commitment to FP 2020, Myanmar will endeavor to increase Contraceptive Prevalence Rate from 41 per cent to above 60 per cent by 2020.
All these Goals are interlinked with MDSR implementation.
It is acknowledged in countries that have moved from MDR to MDSR that the first 3-5 years of a national MDSR system the data will reflect the fact that implementation of the system is still being established and strengthened. In 2017, in Myanmar, reporting increased and expanded, from the community and facilities, with more complete reports from tertiary facilities.
While overall progress has taken place, there is still more to do such as improving processes at the subnational level, such as capacity to accurately classify cause of death, more efficient case record retrieval, monitoring of responses and targeted budget allocation.
MDSR will contribute to the Sustainable Development Goals that have sought to capture the need for ongoing improvements in maternal and child health, calling for a global target MMR of less than 70 maternal deaths per 100 000 live births by 2030.

46 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
47NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
AnnexesAnnex 1 List of documents reviewed
2018 International Classification of Disease 10 CM Codes https://www.icd10data.com/ICD10CM/Codes
MRH, 2014. Maternal Death Review (MDR) in Myanmar (2013). Myanmar: Maternal and Reproductive Health Division, Department of Health.
MRH, 2015. Maternal Death Review (MDR) Towards Maternal Death Surveillance and Response (MDSR) In Myanmar
MRH, 2017. Maternal Death Review (MDR) in Myanmar (2015). Myanmar: Maternal and Reproductive Health Division, Department of Health.
MRH, 2018. Maternal Death Review (MDR) in Myanmar (2016).
Maternal Death Surveillance and Response (MDSR) - Technical Guideline for Action to End Preventable Maternal Deaths in Myanmar (September, 2016) (3MDG, WHO, MoHS, UNFPA)
Ministry of Health and Sports - DHS Program - Myanmar Demographic and Health Survey 2015-2016
Souza JP, Tuncalp O, Vogel JP, Bohren M, Widmer M, Oladapo OT, Say L, Gulmezoglu AM, Temmerman M. Obstetric transition: the pathway towards ending preventable maternal deaths. BJOG 2014; 121 (Suppl. 1): 1–4.
Thaddeus, S. & Maine, D., 1994. Too far to walk: maternal mortality in context. Social Science and Medicine, 38(8), 1090-1110.
WHO, 2004. World Health Organization, Beyond the numbers: reviewing maternal deaths and complications to make pregnancy safer. 1st ed. Geneva. WHO Press.
WHO, 2015. Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: WHO Press.
WHO, 2012. The WHO application of ICD-10 to deaths during pregnancy, childbirth and puerperium: ICD MM. 10th ed. Geneva: WHO Press.
WHO, 2014.Study on the implementation of Maternal Death Review in five countries in the South-East Asia Region of WHO
2014 Myanmar Population and Housing Census
2014 Myanmar Population and Housing Census - Policy brief on maternal mortality
2014 Myanmar Population and Housing Census - Policy brief on urbanization and migration
Wai Wai Han, Saw Saw, TheingiMyint, Zayar Lynn (2015) - Access and utilization of maternal and child health care services among migrants in Bogale and Mawlamyainggyun townships https://www.iom.int/sites/default/files/country/docs/myanmar/IOM-Myanmar-Migrant-MCH-folder.pdf
The WHO Application of ICD-10 to deaths during pregnancy, childbirth and the puerperium: ICD-MM

48 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Annex 2 List of persons interviewed
Department Name Designation Comment
Maternal and Reproductive Health Unit
Dr Hla Mya Thway Einda Director
Dr Hnin Hnin Lwin Deputy Director
Dr Khaing Nwe Tin Deputy Director
Dr Myo Myo Mon Assistant Director
Obstetricians and Gynaecologists
Dr Nwe Mar Tun Professor/Head, University of Medicine Mandalay
(previously University of Medicine Magway)
Dr Tin Tin Cho Clinical Professor, Central Women’s Hospital
(previously North Okkalapa General Hospital)
Dr Aye Aye Tint Professor, University of Medicine 2 –North Okkalapa General Hospital
(previously Magway Teaching Hospital)
Dr Hla Myat Mo Mo Senior Consultant, North Okkalapa General Hospital
Dr Moe Nwe Senior Consultant, Central Women’s Hospital
Ob Gyn Society, Myanmar Medical Association
Dr Yin Yin Soe Professor (retired) Central Women’s Hospital
(previously University of Medicine 1, Yangon)
Anaesthetist Dr Nilar Nyein Senior Consultant retired
Mandalay Region Dr Yu Yu Wai Dy Regional Public Health Director
Dr Wah Wah Win Hlaing Ob Gyn Yamethin
Dr Thet Oo TMO Amarapura
Dr Hla Hla Htay MS Yamethin
Magway Region Dr Mon Mon Myint Dy Regional Public Health Director
Dr San San Moe TMO Min Hla
Dr Toe Toe Aung Ob Gyn Magway Hospital(previously Ayeyawaddy)
Ayeyawaddy Region
Dr Thet Su Mon Assistant Director
Dr Zeyar Min Team Leader
Yangon Region Dr Kyaw Zin Htut Staff Officer, MRH
Kayah State Dr Aye Thawda Mon Assistant Director, MCH
Shan State (North) Dr Ye Thiha Staff Officer, MRH
Chin State Daw Aye Par Township Health Assistant
Daw Lain Young Health Assistant
Kachin State Dr Tin Nyo Nyo Dy State Public Health Director
Dr Kyu Kyu Moe Assistant Director
UNFPA Ms Janet Jackson Country Representative
Dr Tin Maung Chit Former MDSR focal person
Dr Yin Yin Htun Ngwe Assistant Representative
Dr Carla Desiree Lichtenstein
Programme Analyst, Gender Equality and Women’s Empowerment
Note: Owing to limitations in the time available for preparing the report, the number of persons interviewed was somewhat restricted.
The National Maternal Death Surveillance and Response ( 2017 Report ) was developed with the technical assistance of Consultant, Dr Katherine Ba Thike.

49NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Annex 3 Definitions
There are standardized definitions which are universally adopted, and which are used by the UN Maternal Mortality Estimation Interagency group (MMEIG)
Pregnancy-related death - A pregnancy related death is the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death. This includes all maternal deaths and the deaths due to accidental or incidental causes.( Note : There is also the concept of deaths of women in reproductive age (WRA) group, regardless of their pregnancy status, often referred to as WRA-death).
Maternal death - A maternal death is the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. Maternal deaths are subdivided into two groups by cause:
Direct obstetric deaths - Direct obstetric deaths are those resulting from obstetric complications of the pregnancy state (pregnancy, labour and the puerperium), from interventions, omissions, incorrect treatment, or from a chain of events resulting from any of the above.
Indirect obstetric deaths - Indirect obstetric deaths are those resulting from previous existing disease or disease that developed during pregnancy and which was not due to direct obstetric causes, but which was aggravated by physiologic effects of pregnancy.
Incidental maternal deaths - These are deaths from unrelated or incidental/accidental causes that happen to occur in pregnancy or the puerperium. These deaths therefore will be included in pregnancy-related deaths, but not in maternal deaths.
Note :Information obtained from census and surveys (such as DHS) can only be obtained on pregnancy-related deaths (derived from the number of deaths of females of reproductive age), and not maternal deaths. But generally for all intent and purpose, and as practiced universally the number obtained is cited as maternal deaths (and it is a valid proxy for maternal deaths). In the Myanmar case, the Census 2014 report clearly explains this, and it uses the figure as “maternal death”. On the other hand, the DHS 2015 - 2016 report cites this as “pregnancy-related deaths”
Late maternal death - There is universal agreement that the puerperium ends 42 days after childbirth. There are countries that also conduct review on maternal deaths beyond this period. These are late maternal deaths - the death of a woman from direct or indirect causes more than 42 days but less than one year after termination of pregnancy. These are not included in the calculation of maternal mortality ratio for which there is international agreement to limit it to 42 days. The DHS 2015-2016 counts pregnancy-related deaths from pregnancy to 60 days after childbirth.
There is another concept Lifetime Risk (LTR) of a maternal death, which is the risk that a woman who survives age of 15 will die of maternal death at some point during her reproductive lifespan (which ends at age 49), given the current rates of maternal mortality and morbidity. (Note : In previous MDR reports, this measure was not included because it is a measure that cannot be derived from MDR, and when it is available from other sources, it is seldom used.

50 NATIONAL MATERNAL DEATH SURVEILLANCE AND RESPONSE 2017
Arising out of these definitions, there are the relevant measures used in describing maternal mortality
• Maternal Mortality Ratio (MMR) which is the number of maternal deaths divided by the number of livebirths (LB) expressed as per 100,000 LB. This is the measure that is universally used for assessing and comparing the magnitude of maternal mortality
• Maternal Mortality Rate (MMRate) is the number of maternal deaths divided by the number of women aged 15-49, usually expressed as per 1,000. This is seldom used, although it is a more valid measure of risk compared to MMR.
• Pregnancy-related Mortality Rate - As for MMRate above, the same can be calculated for pregnancy related mortality rate; the number of pregnancy related deaths divided by the number of women aged 15-49 (Both the Census 2014 and the DHS 2105-2016 report have this measure)
• Proportion of adult female deaths due to maternal causes (PMFD), which is the number of maternal deaths divided by the number of deaths among women aged 15-49, most conveniently expressed as %. This is comparable to “case fatality” in other diseases (The Census 2014 report has this measure)

