name of the doctor :- dr. shivinijhawan
TRANSCRIPT

.
1
Name of the Doctor :-
Dr. Shivi Nijhawan
�Mast cells are primary effector cells in immunoglobulin E (lgE) mediated inflammatory reactions.
�They are implicated in:-
– both acquired and innate immune responses
– Wound healing
– Fibrosis
– Angiogenesis
– Autoimmune diseases
� First described by Ehrlich in 1871, who distinguished them from other connective tissues by their ability to stain metachromatically with basic aniline dyes.
Mast cells are bone marrow-derived cells with special secretory properties. � They are present in large numbers in the papillary
dermis, around the appendages and blood vessels.
�Mast cells are widely distributed, long lived cells found predominately in connective and mucosal tissues and often in proximity to blood vessels, nerves, and lymphatic tissues.
�Mast cells are abundant in the skin, respiratory tract, gastrointestinal tract, and genitourinary tract.
� 7000 mast cells/cubic mm in normal skin.
�All human mast cells contain tryptase , histamine, and proteoglycans, including heparin and chondroitin sulfate E.
�Mast cells are classically identified in tissue by :-
� Toluidine blue or Giemsa dye that stains the cytoplasmic granules, and
� more recently, by immunohistochemistry using an antibody that recognizes mast cell tryptase.
�Human mast cells are classically divided into two types :-( Depending on neutral protease composition)
1) TC mast cells(MCtc) –
�Mast cells that contain tryptase and chymase.
� Skin , intestinal submucosa, & synovium nearly bear MCtc.(~90%).
� Such cells tend to be located in sub mucosal tissues.
� Increased numbers of these cells are found in fibrotic disease.

.
2
2) T mast cells (MCt) –
�Mast cells that contain tryptase but not chymase.
� Found in alveolar walls & gut mucosa (>90%).
� increased in allergic and parasitic diseases.
�Mast cells are oval to spindle-shaped cells with a centrally located round to oval nucleus.
�They are 6–12 µm in diameter, resembling friedeggs.
�They contain in their cytoplasm numerous granules that do not stain with routine stains like hematoxylin-eosin.
� The granules stain with methylene blue, which is present in the Giemsa stain, with toluidineblue, and with Alcian blue.
�This is because of a high content of heparin
� Electron microscopic examination of mast cells reveals numerous large and long villi at their periphery .
�The mast cell granules appear as round, oval, or angular-shaped, membrane-bound structures.
�Mature granules measure up to 0.8µm in diameter surrounded by a perigranular membrane.
� They contain two components: lamellae and electron-dense, finely granular material .
� The lamellae appear in cross sections as thick, curved, parallel, filaments forming whorls or scrolls that may resemble finger-prints in their configuration.
� Each lamella is 7–12 nm wide, and their spacing is about 12 nm wide.
Mast cell with cytoplasmic granules andvillous projections from the cell surface. �They also contain histamine, neutrophil and
eosinophil chemotactic factors, tryptase, kininogenase and β-glucosaminidase.
�Slow-reacting substance of anaphylaxis (LTC4 and LTD4), LTB4, platelet activating factor and prostaglandin D2 are formed only after IgE mediated release of granules.

.
3
1) Mast cells are reservoirs of preformed inflammatory mediators and rapidly synthesizes others on activation.
2) Mediators contributes to the changes in anaphylaxis and delayed hypersensitivity reactions.
3) Primes B-cell for antibody formation.
4) They play a role in the defense against parasites; stimulate chemotaxis, activation and proliferation of eosinophils; promote phagocytosis.
5) stimulate connective tissue repair and angiogenesis.
�Mast cell granules contain various mediators which can be classified into:
(1) Preformed soluble mediators such as histamine, heparin, eosinophil chemotacticfactor, neutrophil chemotactic factor, platelet activating factor, tryptase and kallikreingenerating factor,
(2) Granule-associated mediators such as proteases, peroxides, proteoglycans and inflammatory factors of anaphylaxis, and
(3) Newly synthesized mediators such as prostaglandin D2; leukotrienes B4, C4, D4, E4; and thromboxanes.
� Pre–formed secretory granular mediators are released In response to aggregation Of the high-affinity IgE receptor, activation through complement receptors, or activation by cytokine.
�Mast cell tryptase is released upon activation of mast cells, along with histamine, heparin, chymase, and carboxypeptidaseA.
�Most abundant human mast cell protein and exists in two forms that show 90 percent homology, alpha and Beta tryptases.
�The biologic function of tryptase has not been completely defined, but it appears to activate protein cascade systems, enhance vasopermeability , and alter airway smooth muscle reactivity.
�Tryptase has the capability to Cleave fibronectin , vasoactive intestinal peptide, and kininogens.
�Also a growth factor for epithelial cells and fibroblast.
�The total tryptase level in Blood is used as an indirect parameter of mast cell burden and mast cell activation.
� Baseline tryptase levels are generally elevated in patients with systemic mastocytosis (SM).
� Increased serum tryptase levels are also observed within 15minutes of onset of anaphylaxis with a peak level seen at 1 to 2 hours, although this is not consistent.
�The mast cell protease chymase converts angiotensin I to angiotensin II.
�The vasoactive properties produced by angiotensinII may contribute to transient hypertension in some individuals during mast cell activation reactions.
�CarboxypeptidaseA similarly converts Angiotensin I to angiotensin II.

.
4
�Histamine is stored in all mast cells, as well as basophils and released with cell activation.
�The biological effects of histamine are mediated through activation of H1,H2, H3, and H4 receptors.
�H1 receptors are located on epithelial cells as well as vascular and perivascular cells and mediate vascular permeability and instability.
�H2 receptors are present on epithelial Cells in the gastrointestinal tract and are associated with gastric hypersecretion.
�H3 receptors are found in the brain and gastrointestinal tract and may be associated with certain neurologic effects such as headache.
�H4 receptors are present on eosinophils and mast cells but their significance Is still unknown.
�Heparin stabilizes and regulate secretory granule proteases.
� In addition, it binds to antithrombin III, inhibiting activation of the clotting cascade.
�Heparin binding also regulates and stabilizes cytokines and growth factor.
�Heparin mediated effects include bleeding diathesis, osteopenia and osteoporosis.
�Newly formed, membrane-derived Lipid mediators, produced by mast cell activation, include prostaglandin D2 (PGD2), cysteinylleukotrienes and platlet-activating factor (PAF).
�These mediators have profound effects in both the immediate and late allergic reactions.
�Receptors for PGD2, are present on vascular and perivascular cells and mediate effects including bronchospasm ,vasodilation, vasopermeability and inhibition of platelet aggregation.
� Flushing in response to niacin is mediated by PGD2.
�Cysteinyl leukotrienes increase vascular Permeability and cause bronchoconstriction.
�These mediators also are responsible for the long-lasting wheal and flare in response to injection of antigen in human skin.
� Leukotrienes are believed to contribute to abdominal Symptoms in patients with Systemic Mastocytosis.
� PAF is a potent inducer of bronchoconstrictionmediated through microvascular leakage in the airways and the subsequent development of submucosal edema.
�Various cells synthesize PAF including endothelial cells, neutrophils and macrophages.
� Functions as a chemotactic agents for eosinophils, neutrophils and mast cells.
�Mast cells similarly produce and release a number of cytokines that contribute features of mastocytosis.
�Tumor necrosis factor causes cachexia and vascular instability.
�Transforming growth factor-Beta contributes to tissue fibrosis, abnormal bone remodeling, osteopenia and eosinophilia.
� IL-4 is implicated in IgE synthesis and the development of a T helper 2 phenotype.
� IL-5 is instrumental in the recruitment and survival of eosinophils that contribute to tissue damage.
� IL-6 has been linked to the Pathogenesis of osteoporosis and is elevated in the plasma of patients with SM.

.
5
�Mast cells arise from a CD34*, KIT+ pleuripotentprogenitor stem cell.
�Cross linking KIT by stem cell factor (SCF) is essential for these precursor cells to differentiate into mast cell.
�Mature mast cells require SCF for survival.
�KIT (CD117) expressed on haematopoeitic stem cell, is transmembrane tyrosine kinase receptor for SCF.
� It remains highly expressed on mast cells and is critical for many mast cell functions such as survival, chemotaxis and enhancement of signalling events.
�Other cytokines that regulate SCF-dependent mast cell differentiation and proliferation include interleukin 13 (IL-13), IL-4,5, and interferon-gamma (IFN-y).
�Antigen-dependent aggregation of FceRl bound IgEon the surface of mast cells is a primary mechanism of activation of Mast cells and subsequent release of preformed proinflammatorymediators, as well as of newly synthesized mediators.
�Non-IgE-driven signals that activate mast cells include Toll-like receptor ligands such as lipopolysaccharide and nucleic acids, the anaphylatoxins C3a and C5a, and certain chemokines and cytokines.
�Whenever the specific antigen gets bound to the Fab portion of the corresponding molecules of IgE, there is further bridging of these antigens.
�This leads to a disturbance in the balance between cyclic AMP and cyclic GMP, leading to a decrease in cyclic AMP, with the result that the mast cell granules move towards the cell surface, fuse with the cell wall and release their contents into the surrounding tissue.
� Mast cell degranulation occurs after cross-linkage with IgE on its cell surface in response to neuropeptides like substance P and mechanical or other exogenous agents.
�Mast cell degranulation can also occur by:-other stimuli such as C5a and C3a, macrophage-derived cytokines (e.g. IL-8),
�some drugs such as codeine and morphine, adenosine, melitin (present in bee venom), and physical stimuli (e.g. heat, cold, sunlight).
�Allergen detection leads to mast cell histamine release.
� In skin, this leads to wheal and flare reactions.
� In the gut ,leads to intestinal hyper-permeability, smooth muscle contraction, altered water and ion transport, and intestinal symptoms.
� In the lungs, this leads to smooth muscle contraction, mucus production, and airway remodeling.

.
6
�Mast cells offer a first line of defense against parasitic pathogens.
�They are preferentially located in organs targeted by parasites, where they release proteases, recruit neutrophils, and regulate vessel permeability.
�Mast cells release antimicrobial peptides.
�Helminth infection
�MCs are activated by helminth & MC hyperplasia is observed in helminth infection.
�Mast cells express most TLRs on their membrane surfaces.
�TLR binding triggers distinctive patterns of mast cell activation including the release of antimicrobial peptides and the production of complement-mediated membrane attack complexes.
� Bacterial infection
�MC-derived TNF, together with LTC4 & LTB4 contributed to recruitment neutrophils to clearance Klebsiella pneumoniae, Listeria
monocytogenes, Pseudomonas aeruginosa
� Parasite antigen stimulation of TLRs and C-type lectin receptors (CLRs) initiates a wide range of mast cell.
� IgE receptors resulting in the release of proinflammatory cytokines, chemokines, and other pre-stored mediators of inflammation.
� Fungal infection
�Human MCs respond to zymosan, but not peptidoglycan,
�Trichoderma viridae, indoor fungus, induce
MC degranulation (high dose) but low dose enhance histamine secretion from MCs
�Aspergillus fumigatus induce IgE-
independent MC degranulation
�Upper respiratory viral infections worsen allergic asthma, suggesting increased activation of mast cells during infection.
�Mast cells recognize the presence of double-stranded viral RNA and respond by releasing:
IL-29, interferon alpha, interferon-beta, and tumor necrosis factor alpha.
�Virally infected mast cells respond by releasing the anti-viral proteins.
� Stimulation of mast cell TLR3 induces mast cell
�Viral infection
�Report from HIV-infected patients
� Increased serum IgE predict worse prognosis

.
7
� It is a heterogeneous group of disorders.
� Characterized by mast cell hyperplasia in one or more of following organs: bone marrow, liver, spleen, lymph node, gastroinstinal tract & skin.
� Clinically, disease accompanied by constitutive mast cell activation & anatomical distribution of mast cells.
�The original description of mastocytosis was given by Nettleship and Tay on a 2 yr old girl with hyper pigmented papules that spontaneously urticated in 1869.
� Later in 1877, Paul Ehrlich discovered the mast cell.
�Unna was the first to demonstrate the mast cells were responsible for the cutaneous eruption in mastocytosis patients.
� In 1949, Ellis reported the first patient with systemic disease
�Term ‘mastocytosis’ was proposed by Sezary to describe skin and systemic involvement together.
�Term ‘mastocytosis in skin’ can be used when patients present with skin lesions but have not been investigated for systemic disease (e.g. an adult who does not want a bone marrow biopsy or has low blood tryptase)
�Hannaford et al describe fifth type-pseudoxanthomatous mastocytosis.
�There are 2 main categories:
1. CUTANEOUS MASTOCYTOSIS(CM):
�MC infiltrate is confined to one or more lesions on the skin
2. SYSTEMIC MASTOCYTOSIS(SM):
�MC infiltration of at least one extracutaneousorgan with or without evidence of skin involvement
� The symptoms of mastocytosis are primarily due to mast cell mediator release.
� Somatic mutations involving codon 816 of the c-KIT gene represent the most common genetic
abnormality in patients with sporadic mastocytosis.
�The result is a substitution of the amino acid aspartic acid (D) with valine (V) or another amino acid; examples include D816V, D816Y, D816F and D816H.
� Extracellular, transmembrane and juxtamembranemutations reported- in childhood mastocytosis.
�KIT is also expressed on haemopoietic stem cells and melanocytes,
�which might be relevant to the development of myeloproliferative and myelodysplastic disorders in mastocytosis and the hyperpigmentation that often accompanies lesions of urticaria pigmentosa.
.
8
� Age: can present at the time of birth or develop anytime thereafter into late adulthood (aged 30-49 years.)
� Sex: Males and females equally affected.
� Diseases incidence varies from 0.1% to 0.8%.
Uncommon disorder.
� Mostly sporadic ,but some familial cases with
dominant pattern of inheritance may occur.
�Maculopapular cutaneous mastocytosis
1. Urticaria pigmentosa (UP)/maculopapularcutaneous mastocytosis (MPCM)
2. Diffuse cutaneous mastocytosis (DCM)
3. Solitary mastocytoma of the skin
4. Telangiectasia macularis eruptivaperstans(TMEP)
�Commonest form of mastocytosis (70-90%)
� Incidence – one in 8000.
�Onset: is generally before 2 years of age and a few infants born with few skin lesions, also seen in adults (20-40 years) where it is more chronic and associated with systemic involvement.
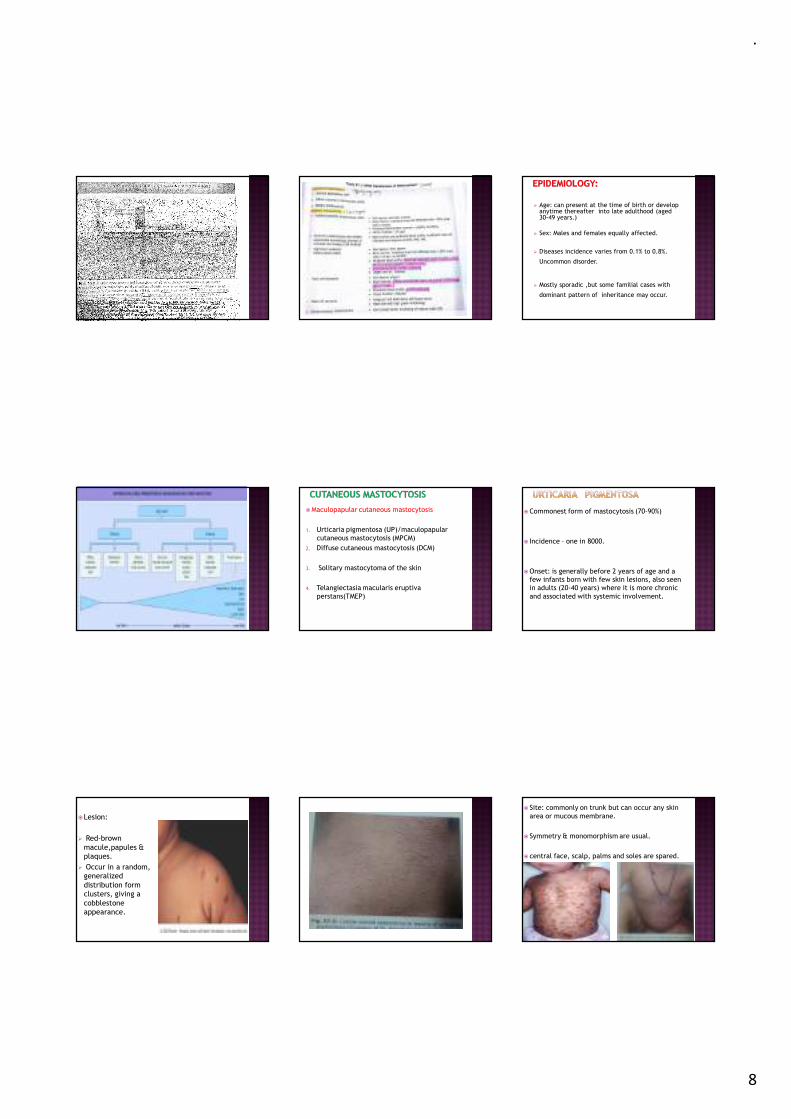
�Lesion:
� Red-brown macule,papules & plaques.
� Occur in a random, generalized distribution form clusters, giving a cobblestone appearance.
� Site: commonly on trunk but can occur any skin area or mucous membrane.
� Symmetry & monomorphism are usual.
� central face, scalp, palms and soles are spared.

.
9
� Telengiectasia , petechiae, or echymoses may occur.
� Nodules and plaques are less common.
� A generalized blistering variety has been reported in
patients less than 2 years which subsides
spontaneously by 3-5 years.
� Lesions heal without scarring.
� Systemic involvement in about 10% of patients with
urticaria pigmentosa presenting after age of 5 years
reported.
�Darier’s sign :
Rubbing of the lesions usually leads to urticationand erythema over and around the macules( due to local release of histamine from mast cells )
�UP is sometimes associated with pruritus that is exacerbated by :-
1. Changes in temperature
2. Local friction
3. Ingestion of hot beverages
4. Spicy foods
5. Ethanol
6. Certain drugs- NSAIDS, OPIODS
� Extremely rare form of CM.
�Onset : children younger than 3 years , but also in adults.
�Characterized by diffuse infiltration of virtually the entire skin by mast cells.
� Lesions: Skin appear normal or have red-yellow-brown color.
�Numerous erythematous to yellow tan papules and plaques with areas of confluence that have a leather grain appearance.
�Dermographismwith formation of hemorrhagic blisters is common.
� Large blisters may develop on apparently normal skin spontaneously or following pressure or mild trauma.
� Usually resolves spontaneously between age of 15 months & 5 years.
� Sometimes large bullae which rupture easily to form
erosions, with surrounding infiltration of skin-
Bullous mastocytosis.
� Numerous ill defined yellowish papules
(Pseudoxanthoma) may be seen.
� Generalized erythroderma may occur-
Erythrodermic DCM
� Because of enormous mast cell load, serious
complications such as hypotension, shock, GI
bleeding( due to high level of serum
histamine) and severe diarrhea may occur.

.
10
�Onset: may present at birth or more commonly appear within first 3 months of life (extremely rare in adults).
� Lesions: few in numbers, may be solitary or multiple,& present as macule, plaque or nodule.
� Bullae may be present.
� Site: often appear at distal extremities but rare on palms & soles.
�Often asymptomatic, associated with severe pruritus, blister (31%) & flushing (29%).
� Systemic manifestations –rare
� It has highest concentrations of mast cells nearly 150 times of normal skin.
� Surface may have an orange peelappearance/ peau d’orange.
�Darier’s sign is positive.
�A rare form of mastocytosis seen < 1% of cases.
�Age: usually appears in the adults.
� Pruritus, purpura & blister formation are not associated.
� Lesion: generalized, red, telangiectacticmacules have a background color ranging from tan to brown.
�Individual lesions are 2-6 mm in diameter & without sharply defined outlines.
� Site: primarily on the trunk(especially the chest), but also on the extremities.
� Longstanding lesions develop hyperpigmentation
�The site become edematous when rubbed.
� It may co exist with Urticaria pigmentosa
�Darier’s sign is absent in most cases.
�On dermatoscopic examination, telangiectasias are alignedd in a reticular pattern.
� In isolated cases, splenomegaly, increased numbers of mast cells in bone marrow, & abnormal skeletal radiographs reported.
Diffuse or localized hyperpigmented macules
• Café –au-lait spots.• Neurofibromatosis.• Albright synndrome.• Multiple cutaneous lentiginosis.
Bullous lesions
• Chronic bullous disease of childhood.• Linear immunoglobulin A dermatosis.
Solitary or multiple papules or nodules
• Congenital nevus• Juvenile xanthogranuloma.
�Refers to the condition in which patients have an abnormal increase in mast cells in non cutaneoustissues.
�Usual sites affected: bone marrow, liver, spleen, lymph nodes, GIT, skeletal system but any tissue can be affected.
�CNS is not effected.
�Usually seen in adults but rarely seen in children.

.
11
�The symptoms of SM are usually grouped into 4 categories:
(1) constitutional symptoms : fatigue, weight loss, sweats, and fever
(2) skin symptoms
(3) MC mediator-related symptoms
(4) musculoskeletal symptoms, which include bone, muscle, and joint pain
� If the age of onset of mastocytosis is below 5 years,
then skin biopsy is sufficient to determine the diagnosis
� If systemic signs are present or later age of onset, then
1. A complete blood count (anemia, leukocytosis, thrombocytopenia)
2. Serum tryptase levels (elevated in mastocytosis)
3. Bone marrow biopsy
4. USG Abdomen/CT Scan abdomen ( to rule out liver and spleen pathology).
5.Radiologic and endoscopic studies of GIT (if GI symptoms are present)
6.Radiological skeletal survey (if bone pain or h/o of fracture is present)
7. Liver Function tests
8. Urinary levels of major histamine metabolites (methylimidazoleaceticacid,MIAA)
9. Plasma or urinary histamine levels (2-3 times more in pts with mastocytosis)
�Normal range is 1-15ng/ml
� It is slightly elevated in patients with CM’s and isolated bone marrow mastocytosis.
� It is significantly elevated(>20ng/ml) in case of multi organ involvement.
� show multifocal, sharply demarcated, compact infiltrates of mast cells.
�Mast cells are a mixture of both round and spindle shaped forms.
� Immunohistochemical and molecular studies are recommended to distinguish reactive from malignant mast cell infiltrates.

.
12
�MIAA(1,4-methylimidazoleacetic acid) in urine.
�Markedly increased, especially in TMEP and SM.
�They correlate well with the extent of systemic involvment and their periodic measurement can be used to monitor disease activity
�Other indicators of mast cell degranulation are the mast cell granule associated tryptase, chronologically elevated urinary metabolite pfprostaglandin D2 and a prolonged PTT immediately after an attack.
� Mast cells are oval or spindle-shaped and have
granules that stain metachromatically with toluidine
blue.
� Well demonstrated by Giemsa or chloroacetate
esterase stains in formalin-fixed biopsies.
� In urticaria pigmentosa
� Characterized by accumulation of mast cells in
dermis particularly around the blood vessels.
� Mast cells are basophilic, granular and they may
appear elongated like fibroblast or cuboidal.
� In the bullous variety the blister is sub epidermal
and the blister cavity often contains numerous
eosinophils.
� The epidemis shows increased melanization
In Mastocytomas and diffuse cutaneous
mastocytosis
� Epidermis shows increased melanization.
� Diffuse, dense interstitial infiltrate of mast cells around blood vessels are seen.
Telangiectasia macularis eruptiva perstans
(TMEP)
� Mast cells are confined to superficial
capillaries and dilated venules.
�Counseling the patient regarding the nature of the disease.
�Avoidance of factors provoking mediator release.
�Management of chronic symptoms like pruritis and gastric hypersecretion (mast cell mediator release symptoms).
�Treatment of acute episodes of vascular collapse.
�Cytoreductive therapy to address the sequelae of disabling organ infiltration by mast cells.
�Alcohol intake
�Anticholinergic medications
�Aspirin
�NSAID’S
�Heat
� Friction
�Narcotics (morphine and codeine)
� Polymyxin B sulfate
�Thiamine
�Quinine
�Opiates
�D-tubocurarine
.
13
�Antihistamines
�Corticosteroid
�Disodium cromolyn (cromolyn sodium)
� Bisphosphonates
�UV light irradiation
� Epinephrine
�H1 receptor antagonists:
� potent or non-sedating antihistamines
� reduce pruritus and flushing
�H2 receptor antagonists:
� If H1 is insufficient, especially in cases of gastric hypersecretion
� Ex :ranitidine , cimetidine , famotidine
�Ketotifen fumarate:(dose :- 1-2 mg/day)
� has both antihistamine and mast cell stabilisingproperties.
� Effective when combined with ranitidine.
� Disodium cromoglycate (oral cromolyn sodium):� Inhibits mast cell degranulation
� may reduce Gastrointestinal symptoms - abdominal
pain, nausea and diarrhoea , cutaneous and CNS
symptoms.
� Available as an oral concentrate solution in 5-mL ampules .
� low dose Aspirin improve prostaglandin-dependent
flushing, tachycardia ,syncope.
�Oral psoralen plus UVA (PUVA) can be given 4 times per week reduces no. of mast cells, leukotriene, histamine level.
�Helps in controlling the pruritis and cutaneouswhealing but does not alter other symptoms associated with this disorder.
� Photochemotherapy should be used only in instances of extensive cutaneous disease unresponsive to other forms of therapy.
�Topical steroids under occlusion(0.05% betamethasone dipropionate ointment) for 6 weeks or more eliminates pruritis, cutaneouswhealing , histamine levels and the no of lesional skin mast cells.
� Intralesional injection of Triamcinoloneacetonide can also be given to clear mast cell infiltrates in the skin of mastocytosis patients.
� Systemic corticosteroids can be used in combination with cyclosporine in patients with aggressive mastocytosis.
�Treated with self administered premeasured epinephrine preparations.
�Oral Prednisone(20-40mg/day for 2-4 days) can be given to prevent recurrence of episodes.
�Given for aggressive SM, SM-AHNMD, MCL
1. interferon-α-2b(IFN-α-2b) has been used in treating more aggressive forms (dose -0.5×106 U/day)
� side effects include hypothyroidism, thrombocytopenia, depression
2. Cladribine (2-chlorodeoxyadenosine) IV was effective in eliminating skin lesions and markedly reducing the no of bone marrow mast cells in patients with advanced systemic disease.
�Treatment option for patients with advanced categories of mastocytosis associated with poor survival in only a few reported instances
�may yield a better prognosis if mast cell suppression is attempted prior to the transplantation.
�Nd:YAG laser in the treatment of a patient with urticaria pigmentosa.

.
14