na- 147 (h) k- 3.0 (l) creat- 1.24 (h) ca - 8.4 (l)...
TRANSCRIPT

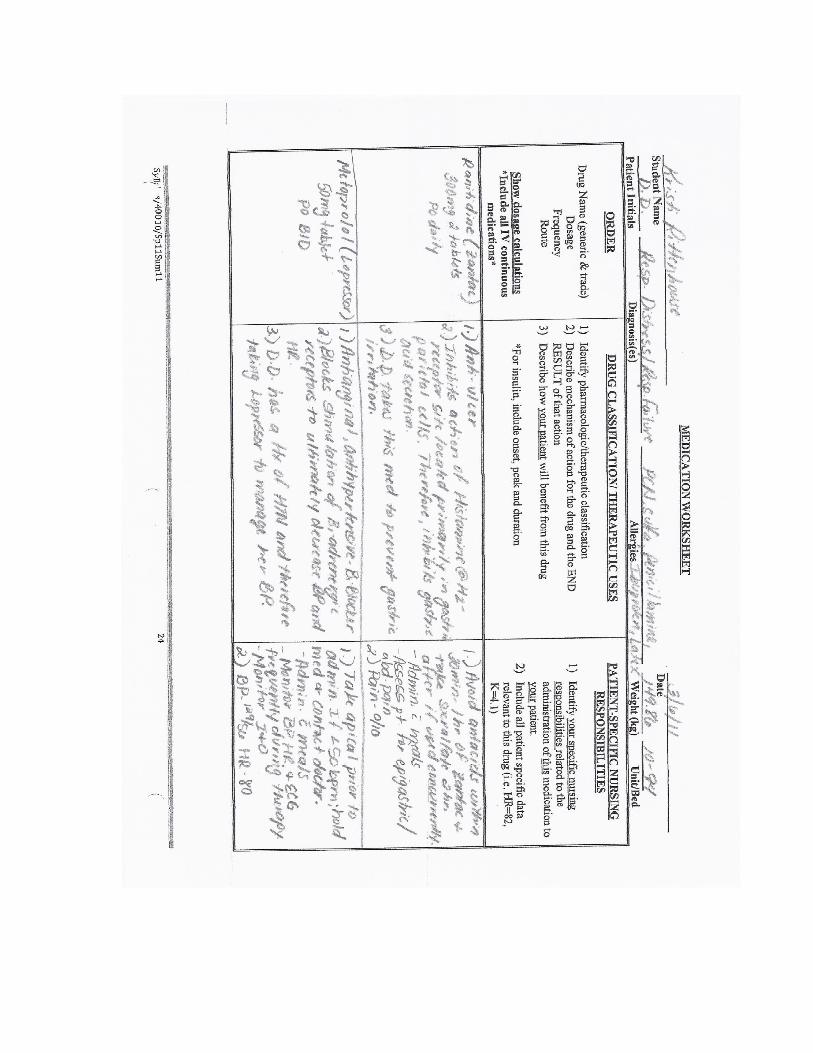
Medications
(see attached paper)
Student Name Kristi Rittenhouse Client Initials D.D. Date 03/6/11
Age 55 Gender Female Room # Floor 10- #94 Admit Date 02/22/11
CODE Status FULL Allergies PCN, Sulfa, Penicillamine, Codeine, Ibuprofen, and Latex
Diet Reg. Activity BRP as tol. And HOB eleveated 30-40 o Braden Score 20
State lab values and identify abnormal
results relevant to this admission
Identify other diagnostic test results
relevant to this admission
2/21/11
o Na- 147 (H)
o K- 3.0 (L)
o Cl- 93 (L)
o Carbon Dioxide- 36 (H)
o BUN- 24
o CREAT- 1.24 (H)
o Ca 2+- 8.4 (L)
o Mg- 2.0
o WBC- 11.8 (H)
o RBC- 3.27
o Hemoglobin- 9.2
o Hematocrit- 29.9
o Platelet- 295
o BS- 152 (H)
IV Sites/Fluids/Rate
#22 L FA Adapted
- Dated 3/5
Monitoring: Invasive/Non-Invasive
State specific monitoring device and
specific values with each device
o ECG- see paper from clinical
rotation
o Tele monitor
Chief Complaint: Difficulty breathing, Trach occluded
Admitting Diagnosis: Respiratory Distress/Respiratory Failure
Medical Diagnosis: Respiratory Distress/Respiratory Failure
ECG Interpretation
(see paper from clinical rotation)
- D.D. has a history of chronic respiratory failure status post tracheostomy secondary to
recent cardiopulmonary arrest on 2/6/11. D.D. presented to the ED with SOB and eventually
went into acute respiratory distress. The ED found with acute respiratory failure and trach
block with blood debris and phlegm. An ENT consult was obtained in the ED along with a
bronchoscopy which revealed trach tube was in good condition with moderate amount of
tracheomalacia distal to the trach. When D.D. was in the ED, there was som suspicion that the
patient probably had some obstruction from the bloody secretions. This may be the case
because D.D. was on Coumadin due to her history of chronic A-fib and she came into the ED
with an INR of 2.6.
- WBCs are high at 11.8 indicating there is an infection somewhere. I am speculating here
that it may be at D.D.’s trach. However, upon assessment no signs or symptoms were present
of infection. Mupirocin, an anti-infective, was being applied to the trach site twice a day. D.D.
presents upon assessment 2+ edema bilaterally in lower legs, ankles, and feet. This could be a
result of the excess sodium of 147. The potassium-3.0 and chloride- 93 are both low. D.D. is
receiving Potassium Chloride pills to help increase these levels.
- D.D. has a history of COPD, chronic obstructive pulmonary disease which refers to
several disorders that affect the movement of air in and out of the lungs (Black & Hawks,
2009). This could be the reason why the carbon dioxide is high at 36.
- High Blood sugar of 152 r/t insufficient carbohydrate metabolism plus high creatine level
of 1.24 leads me to question her kidney function. However the high blood sugar could also be a
result of the steroid-induced DM. DM adds to complications associated with D.D.’s
diagnosis. Diabetes Mellitus is a disorder in which beta-cells no longer respond to high glucose
levels which results in no insulin production, or the body no longer responds to the insulin
being secreted (Black & Hawks, 2009). This results in decreased glucose utilization, increased
fat mobilation and increased protein utilization (Black & Hawks, 2009). Diabetes Mellitus
potentially caused a multitude of D.D.’s signs and symptoms. The incidence of infections is
increased due to diabetes mellitus and an infection can cause an increase in blood sugar
(hyperglycemia), which was 152. Her other complications that Diabetes Mellitus adds to is the
HTN, and the peripheral neuropathy. Which D.D. complained of numbness and tingling in
her fingers and toes.
Past Medical/Surgical History
Relevant to this admission
Past Medical Hx
o Cor pulmonale
o Chronic Resp. Failure, status
post Right tracheostomy
o Tracheomalacia
o Recent cardiopulmonary arrest
o COPD
o Steroid-induced DM
o Chronic A-fib, on Coumadin
o CHF from diastolic
dysfunction
o HTN
o Peripheral neuropathy
o Chronic anemia
o Smoked until up to 2 months
ago: 50 packs/year
Past surgical Hx
o Recent tracheostomy
o Cholecystectomy
o Hysterectomy
Treatments
Medical and Nursing Interventions
Relevant to this admission
o O2 via Trach Mask 35%
o Trach care q shift
o Suction PRN
o BSC PRN
o Daily Weights
o I&O
o Respiratory therapy
o Ammonium Lactate 1Gm TP
BID to legs
o Mupirocin 1Gm TP BID to
trach site
o Encouraged elevation of legs
for edema

Primary Nursing Diagnosis with Relational Statement
Risk for impaired skin integrity r/t decreased blood and
nutrients to tissues secondary to 2+ edema bilaterally in
lower extremities.
Short Term Goal Relevant to Nursing Diagnosis
D.D. will demonstrate skin integrity free of pressure
ulcers by the end of my shift on 3/6/11.
6 Nursing Diagnosis with Relational Statement
1. Risk for impaired skin integrity r/t decreased blood
and nutrients to tissues secondary to 2+ edema bilaterally
in lower extremities, hx of DM and anemia, hx of
numbness and tingling in fingers and toes, and obesity.
2. Risk for infection r/t compromised host defenses
secondary to history of infections, increased hospital stay,
DM, an IV site AEB increased WBC count.
3. Risk for falls r/t altered mobility secondary to
generalized weakness, 2+ edema bilaterally in lower
extremities, and medications.
4. Risk for Aspiration r/t depressed laryngeal and glottis
reflexes secondary to presence of tracheostomy.
5. Fluid Volume excess r/t sodium and water retention,
impaired venous return secondary to peripheral
neuropathy,
6. Activity intolerance r/t compromised oxygen
transport system secondary to CHF, COPD, Anemia,
Obesity, dyspnea, and O2 via trach mask 35%.
Definition (State definition and source)
“The state in which an individual experiences or is at risk
for altered epidermis and/or dermis” (Carpenito-Moyet,
2008, p. 339).
Outcome Criteria (Must be specific and measurable)
- D.D.’s fluid intake will be sufficient. (Met- During my
shift D.D.’s intake was 500mL)
- D.D. will stay off pressure points and keep turning
every hour to two hours. (Met- D.D. completed this
intervention as she either walked around the room or lay
down or sat up on the side of the bed.)
- D.D. will stay free of pressure ulcers and I as the nurse
will assess her skin qs and prn. (Met- I checked her skin
when I assisted her with her bed bath and put lotion on
her back and legs. (see assessment below)
- D.D.’s skin will remain moistened and clean. (Met- I
assisted D.D. with her bath and applied lotion to her
back and Ammonium lactate to her legs).
-Avoid massage over bony prominences. (Met- I only
massaged her back when I assisted D.D. with her bed
bath).
AEB: Defining characteristics specifically exhibited by
your patient that support primary nursing diagnosis
o 2+ edema bilaterally in lower extremities
o Hx of DM
o Hx of anemia
o Numbness and tingling in fingers and toes
o Obesity
o Hx of CHF
o LOS
Identify nursing interventions that you implemented with this patient.
Evaluate patient progress towards achieving outcome criteria as a result of nursing interventions.
1. Encourage D.D. to maintain sufficient fluid intake for adequate hydration to keep the skin healthy (Hess,
1998).
2. Instruct D.D. to turn or shift weight every hour to two hours to stimulate circulation and reduce pressure
points (Hess, 1998).
3. Assess skin qs and prn to provide a baseline of the skin (Hess, 1998).
4. Keep D.D.’s skin clean and moistened by applying moisturizers to maintain skin suppleness and pliability
(Hess, 1998).
5. Avoid massage over bony prominences at all times because this may destroy underlying skin and traumatize
blood vessels (Hess, 1998)
What I Would Do Differently
- D.D. was choking on a Potassium Chloride pill and I
asked the visitor to go and get a nurse while I stayed with
the patient. She could still breathe, so I was rubbing her
back to calm her until the nurse got there. The nurse
suctioned her right away. This came to my mind at first,
but then I wondered how it would work because the pill
was so big and the suction tubing was small. However,
this did work because the pill ended up dissolving. I wish
I would have known what to do in this case and I would
have known how to set up the suction.

Assessment:
o A&O X3; numbness and tingling in fingers and toes due to hx of peripheral neuropathy
o Skin: warm, slightly moist, normal capillary refill <3 seconds, normal turgor, Braden
Score- 20, +2 edema bilateral lower legs, dry lower legs bilateral
o Musculoskeletal: standards not met: mild generalized weakness,
o Respiratory: clear to course, and diminished throughout lobes; occasional, weak cough to
clear yellowish green secretions
o GI: Soft, obese, non-tender abdomen, BS present X4
o Pulses: Radial +2, Dorsalis pedis +1, Posterior tibial +1
o Pt. states she gets dizzy often
Vital Signs
3/6/2011
Temperature 98.7 degrees- oral
Heart Rate 80 bpm
B/P 129/56 Monitor
Respirations 20
O2 saturation 97% on Trach Mask 35%
Pain 0/10



References
Black, J.M., & Hawks, J.H. (2009). Medical-surgical nursing: Clinical management of positive
outcomes (8th
ed.). St. Louis, MS: Saunders.
Carpenito-Moyet, L.J. (2008). Nursing diagnosis: Application to clinical practice (12th
ed.).
Pittsburg, PA: Lippincott Williams &Wilkins.
Hess, C. (1998). Preventing skin breakdown. Nursing, 28(7), 28-29. Retrieved from Health
Source: Nursing/Academic Edition database.