myra lalas pitt. refers to a group of clinical and laboratory features of renal disease: 1. heavy...
TRANSCRIPT

Myra Lalas Pitt

Refers to a group of clinical and laboratory features of renal disease:1. heavy proteinuria (protein excretion greater than 3.5 g/24 hours)2. hypoalbuminemia (less than 3.0 g/dL)3. Edema4. Hyperlipidemia


Primary Renal Disorders Minimal change disease
Focal segmental glomerulosclerosis
Membranoproliferative glomerulonephritis
Membranous glomerulonephritis
Intoxication Heroin, mercury, probenicid, silver
Allergic Reaction Poison ivy, bee sting, snake venom
Infection Bacterial
Viral: Hep B, CMV, EBV
Protozoa: Malaria, Toxoplasmosis
Neoplasm Hodgkin's disease, Wilms' tumor, etc.
Autoimmune SLEHSP
Metabolic DM
Cardiac CHF, Pericarditis

Accounts for 90% of cases of the nephrotic syndrome in children under the age of 10, and > 50% of cases in older children. Electron micrograph in
minimal change disease showing a normal glomerular basement membrane (GBM), no immune deposits, and the characteristic widespread fusion of the epithelial cell foot processes (arrows).
Courtesy of Helmut Rennke, MD. (www.uptodate.com)

Usual clinical features: hematuria, hypertension, and decreased renal function.
Steroid-resistance in a patient considered to have minimal change disease should raise suspicion about FSGS.
Px: CKD in 50%–80% at 10 yr
Tx: Only 1/3 respond to steroids
Light micrograph in focal segmental glomerulosclerosis shows a moderately large segmental area of sclerosis with capillary collapse on the upper left side of the glomerular tuft; the lower right segment is relatively normal. Focal deposition of hyaline material (arrow) is also seen. Courtesy of Helmut Rennke, MD. www.uptodate.com
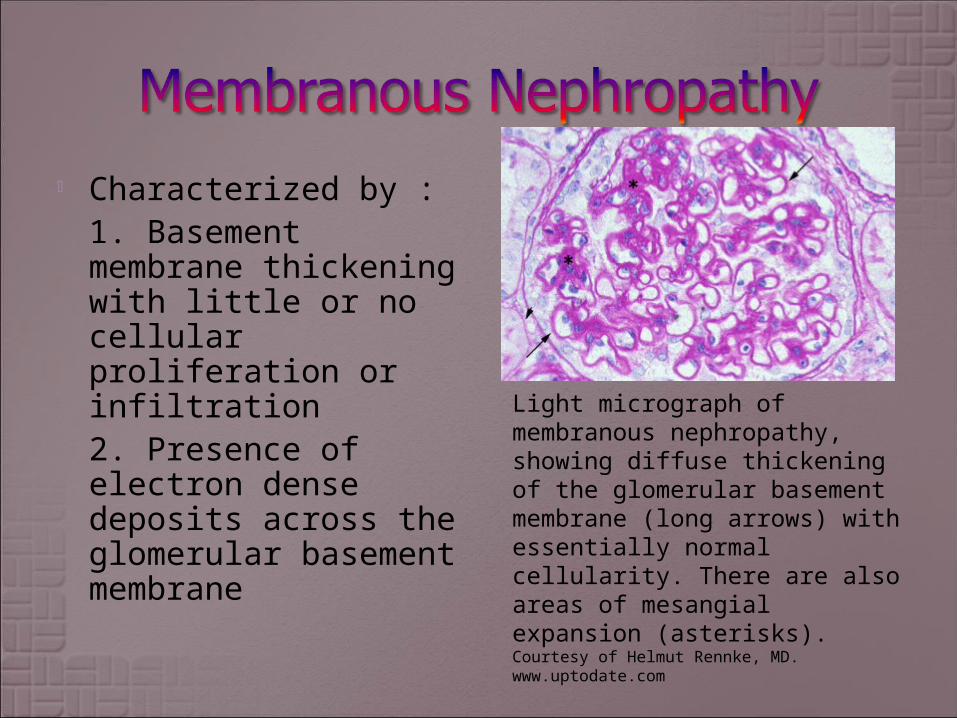
Characterized by : 1. Basement membrane thickening with little or no cellular proliferation or infiltration 2. Presence of electron dense deposits across the glomerular basement membrane
Light micrograph of membranous nephropathy, showing diffuse thickening of the glomerular basement membrane (long arrows) with essentially normal cellularity. There are also areas of mesangial expansion (asterisks). Courtesy of Helmut Rennke, MD. www.uptodate.com

Immunofluorescence microscopy in membranous nephropathy showing diffuse, granular IgG deposition along the capillary walls. Courtesy of Helmut Rennke, MD. www.uptodate.com

HTN frequent; hematuria 80%
Prognosis: ESRD common at 10 yr
Tx: Variable steroid response
Light micrograph of membranoproliferative glomerulonephritis (MPGN) showing thickening of all capillary walls with double contours (long arrows) and focal areas of cellular proliferation (short arrow). The double-contour or tram-track appearance represents interposition of mesangial cell elements with new glomerular basement membrane synthesis. Courtesy of Helmut Rennke, MD.www.uptodate.com

Immunofluorescence microscopy in membranoproliferative glomerulonephritis reveals complement deposition in a rim pattern outlining the glomerular capillary wall. Courtesy of Helmut Rennke, MD. www.uptodate.com

The majority of patients should be hospitalized initially, with input from Renal
For hypovolemia: treat with albumin and fluids.
Monitor closely and treat hypertension if it occurs.
After diagnosis and stabilization, patients without complications are started on prednisone at a dose of 2 mg/kg per 24 hours up to 80 mg per 24 hours and tapered once a response is noted.
Nearly 75% of patients will respond within 14 days.
If with limited response: predictive of poor outcome.
Treatment continues for approximately 2 months but is reinstituted if relapse is noted.
If with worsening congestion (resp distress, pulmonary edema): may give Lasix

Urine protein Urine creatinine ANA C3/ C4 Syphilis serology Hepatitis B, C serologies Renal biopsy

Age more than 10 years Azotemia Decreased complement Hematuria Persistent hypertension No response to steroids
Consider doing a renal biopsy.

Barkin Roger M, "Chapter 84. Specific Renal Syndromes" (Chapter). Gary R. Strange,
William R. Ahrens, Robert W. Schafermeyer, Robert A. Wiebe: Pediatric Emergency Medicine,
3e: http://www.accesspediatrics.com/content/5344076.
Eddy Allison A, "Chapter 472. Glomerular Diseases" (Chapter). Colin D. Rudolph, Abraham
M. Rudolph, George E. Lister, Lewis R. First, Anne A. Gershon: Rudolph's Pediatrics, 22e:
http://www.accesspediatrics.com/content/7045367.
Lowry AW, Bhakta KY, Nag PK, "Chapter 21. Nephrology" (Chapter). Lowry AW, Bhakta KY,
Nag PK: Texas Children's Hospital Handbook of Pediatrics and Neonatology:http://www.accesspediatrics.com/content/7442753.
www.uptodate.com