myoelectric pattern recognition and augmented reality for ... · myoelectric pattern recognition...
TRANSCRIPT

14TH ANNUAL DELSYS PRIZE ENTRY # [ WINNER ] PAGE 1 OF 2
TITLE OF ENTRY
INNOVATION
DESCRIPTION
In the proposed technology myoelectric activity at the residual limb of amputees is used to predict complex phantom
limb movements. These phantom movements are then feedback to the patient in real-time via Augmented and Virtual
Reality. The purpose of engaging patients in Phantom Motor Execution is to eliminate Phantom Limb Pain (PLP) by
normalizing maladapted brain circuitry and exploiting competitive plasticity. This novel and non-invasive approach has
been shown effective in chronic suffers from whom no other treatment worked previously (chronic intractable PLP).
EMG signal processing and pattern recognition are used to predict motor volition of distal joints (several degrees of
freedom simultaneously). This technology overcomes the limitations of previous PLP treatments such as mirror therapy
or VR approaches based on sensorized gloves or motion capture systems. In addition, this approach is suitable for
bilateral amputates, home-use, is non-invasive and more engaging as it involves serious gaming.
Myoelectric pattern recognition and augmented reality for the treatment of Phantom Limb Pain
Over 130,000 amputation-related hospital discharges occur each year in the USA alone. This number is expected to rise
with aging population as the prevalence of diabetes increases. Phantom limb pain (PLP) is a chronic and debilitating
condition that affects the majority of amputees. Over 60 treatments have been proposed in the literature to alleviate PLP.
However, no treatment had been proven successful for all patients, thus leaving a considerable portion of patients in a
permanent painful condition.
The proponent developed a novel approach in which a virtual limb responds directly to phantom motions (decoded using
myoelectric pattern recognition), while the illusion of a restored limb is enhanced via augmented reality (AR).
Furthermore, phantom motions are facilitated and encouraged via serious gaming and virtual reality (VR). Figure 1
illustrates the approach.
Figure 1. a) Surface electrodes and a fiduciary marker placed at the stump. b) Environment captured by the webcam and displayed on a
computer screen with the addition of the virtual limb superimposed on the fiduciary marker. c) Patient playing a racing game in which he drives
the car by phantom movements (simultaneous control of two degrees of freedom). d) Patient using the Target Achievement Control tests as a
rehabilitation tool (originally designed for the prosthetic field).
The use of EMG capturing the synergistic activation of remaining muscles lies at the heart of this technology. It allows
to verify and promote the engagement of central and peripheral circuitry involved in motor execution. Th emphasis in
the affected limb differs from the conventional mirror therapy and VR approaches, which rely on the presence of a
healthy contralateral limb. This distinction also allows to treat patients with bilateral amputations.
Decoding motor volition using myoelectric pattern recognition is also an important component, as it allows to control
considerably more movements that using the conventional one-to-one approach (one EMG signal to control one
movement). This means that much more of the relevant brain circuitry can be engaged and thus returned to the non-
painful perceptive state. In a trans-humeral amputation, up to 8 phantom movements can be decoded reliably (hand
open/close, pro/supination, hand flexion/extension, and elbow flexion/extension), and in a transradial amputation
movement of individual fingers can also be achieved.
14TH ANNUAL DELSYS PRIZE ENTRY # [ WINNER ] PAGE 2 OF 2
TITLE OF ENTRY
SUPPORTING MATERIAL
Myoelectric pattern recognition and augmented reality for the treatment of Phantom Limb Pain
This approach was initially reported in a case study of a 72 years old male who had suffered from chronic PLP for 48
years. This subject reported constant painful sensations at a moderate intensity with periods of intense pain occurring
through the day and night. Intense pain episodes hindered his sleep and daily activities. He showed no improvement
after several medical and non-medical treatments such as mirror therapy, medicaments, TENS, acupuncture, and self-
hypnosis. However, continuous improvement was observed through 18 sessions with the approach described here. At
the end of the treatment, PLP practically disappeared and only sporadic and short pain episodes remained. Sleep and
daily activities were no longer interrupted, and closer relatives reported a perceived improvement on the patient’s quality
of life and emotional state. The technology and this study was published in Frontiers in Neuroscience.
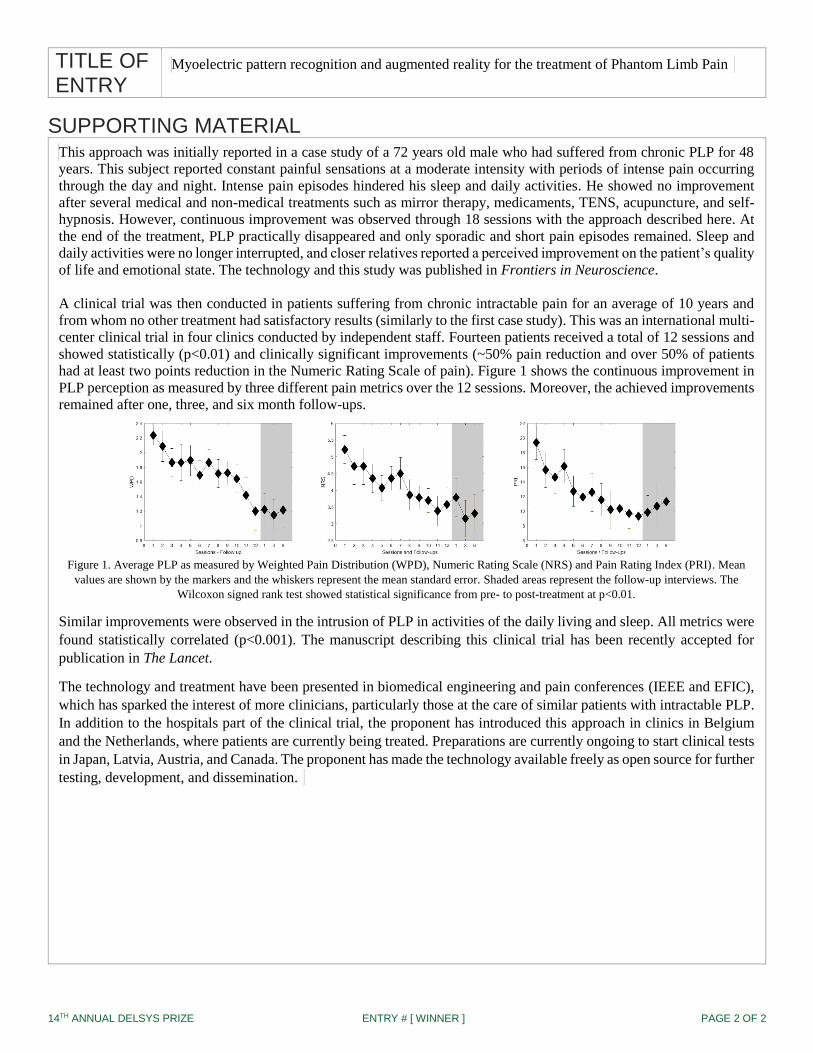
A clinical trial was then conducted in patients suffering from chronic intractable pain for an average of 10 years and
from whom no other treatment had satisfactory results (similarly to the first case study). This was an international multi-
center clinical trial in four clinics conducted by independent staff. Fourteen patients received a total of 12 sessions and
showed statistically (p<0.01) and clinically significant improvements (~50% pain reduction and over 50% of patients
had at least two points reduction in the Numeric Rating Scale of pain). Figure 1 shows the continuous improvement in
PLP perception as measured by three different pain metrics over the 12 sessions. Moreover, the achieved improvements
remained after one, three, and six month follow-ups.
Figure 1. Average PLP as measured by Weighted Pain Distribution (WPD), Numeric Rating Scale (NRS) and Pain Rating Index (PRI). Mean
values are shown by the markers and the whiskers represent the mean standard error. Shaded areas represent the follow-up interviews. The
Wilcoxon signed rank test showed statistical significance from pre- to post-treatment at p<0.01.
Similar improvements were observed in the intrusion of PLP in activities of the daily living and sleep. All metrics were
found statistically correlated (p<0.001). The manuscript describing this clinical trial has been recently accepted for
publication in The Lancet.
The technology and treatment have been presented in biomedical engineering and pain conferences (IEEE and EFIC),
which has sparked the interest of more clinicians, particularly those at the care of similar patients with intractable PLP.
In addition to the hospitals part of the clinical trial, the proponent has introduced this approach in clinics in Belgium
and the Netherlands, where patients are currently being treated. Preparations are currently ongoing to start clinical tests
in Japan, Latvia, Austria, and Canada. The proponent has made the technology available freely as open source for further
testing, development, and dissemination.