myocardial infarction - case presentation and an overview
TRANSCRIPT

Clinico-pathological conference
1st
Myocardial
infarctionPresentation by
1605- Abubakkar
Raheel
1622- Haider Ali
1606- Ahmed Arsalan
1611- Amaila Anam
Final Year MBBS
27th February, 2015

Long Case
• Muhammad Shareef, a 65 year old male patient from Abbottabad, known case of Diabetes since last 12 years and Coronary Artery Disease for the last 2 years presented in King Abdullah Teaching Hospital with the complaints of Chest pain and breathlessness for the last 6 hours. Patient had an episode of vomiting. He was conscious and well oriented. Overall health state was weak and meagre.
Dept of MedicineFrontier Medical and Dental College

Dept of MedicineFrontier Medical and Dental College

Dept of MedicineFrontier Medical and Dental College
History of Patient
• Name: Muhammad Shareef
• Sex: Male
• Age: 65 years
• Marital Status: Married
• Occupation: Retired Govt. servant
• Address: Abbottabad
• D.O.A: 20th February, 2015
• T.O.A: 9:30 am
• M.O.A: OPD
Dept of MedicineFrontier Medical and Dental College
Chief Complaints
• Chest pain – 6 hrs
• Shortness of Breath – 6 hrs
• Vomiting - 5 hrs
Dept of MedicineFrontier Medical and Dental College
History of Present illness
• Known case of Diabetes - 12 yrs & Ischemic Heart Disease – 2 yrs
• Chest pain started 6 hrs back
• Sudden in onset
• Retrosternal
• Crushing in nature
• Radiating to left arm, back and neck
• Aggravated on exertion
Dept of MedicineFrontier Medical and Dental College
History of Present illness
• Shortness of breath – 6hrs
• Sudden onset
• present at rest
• Vomiting – 5hrs
• 2 episodes of vomiting
• Vomitus was yellowish
Dept of MedicineFrontier Medical and Dental College

History of Present illness
Associated symptoms:
• Moderate fever
• Sweating
• Dizziness
• Patient was completely conscious
• Palpitations
Dept of MedicineFrontier Medical and Dental College
History of Present illness
• Systemic Inquiry
1. General
a. Reduced apetite
b. Sleep disturbed
c. Weakness
2. Respiration
Cough, wheezing and hemoptysis not present
Dept of MedicineFrontier Medical and Dental College

History of Present illness
• Alimentary system: Nausea & Vomiting present
• Urinary system: No significant history
Dept of MedicineFrontier Medical and Dental College
History of Past illness
• Past Medical History
– Diabetes : 12 yrs
– IHD : 2 yrs
– HTN : Positive
– TB : Negative
– Asthma : Negative
• Past Surgical History
No significant past surgical history
Dept of MedicineFrontier Medical and Dental College

Family History
• Positive for IHD, HTN and DM
• 2 brothers died of MI
Dept of MedicineFrontier Medical and Dental College
Drug & treatment History
• Patient was taking anti diabetics and anti hypertensive drugs
• Drug compliance was poor
• No other significant drug history
Dept of MedicineFrontier Medical and Dental College

Personal History
• Chronic Smoker
• No history of drinking
• Sedentary lifestyle
Dept of MedicineFrontier Medical and Dental College

Socio-economic History
• Satisfactory
Dept of MedicineFrontier Medical and Dental College
History based Differential Diagnosis
• Acute Myocardial Infarction
• Unstable Angina
• Pleurisy
• Pericarditis
• Pneumothorax
• Pulmonary embolism
• Reflex Esophagitis
Dept of MedicineFrontier Medical and Dental College
General Physical Examination
Patients general appearance
• Pale and anxious
Dept of MedicineFrontier Medical and Dental College

General Physical Examination
• Vitals
– B.P: 160/90mmHg in lying position
– Pulse: 115 b/m, regular, tachycardia
– Temp: 101 F
– Resp: 30/m
Dept of MedicineFrontier Medical and Dental College
General Physical Examination
• No Clubbing, pallor, splinter hemorrhages koilonychias or leconichia
• Mild tobacco staining observed
• Xanthomas present on extensor surface of hands
• Carotid pulse: thin
• JVP: Not raised
• Eyes: Anemia not present
Dept of MedicineFrontier Medical and Dental College
General Physical Examination
• Jaundice not present
• Dental hygiene good
• Carotid briut not audible
• No abnormality on fundoscopy
• No abnormality seen on thyroid examination
• Lymph nodes not palpable
• Pedal and Sacral edema absent
• No other significant findings
Dept of MedicineFrontier Medical and Dental College

Systemic Examination
1. CVS Systemic Examination
a. Inspection:
• No Chest deformity
• No sternotomy or any other surgical scar
b. Palpation:
• Apex beat: Lateralized from mid clavicular line at 6th intercoastal spacecedue to LVH
Dept of MedicineFrontier Medical and Dental College

General Physical Examination
• Heave: well sustained (at apex)
• No left parasternal lift
c. Auscultation:
Mitral, Tricuspid, Aortic, Pulmonary
Dept of MedicineFrontier Medical and Dental College
General Physical Examination
• S1- Normal (Apex)
• S2- Audible (Left sternal edge)
• No added sounds
• No murmurs
Dept of MedicineFrontier Medical and Dental College

General Physical Examination
c. GIT:
• Liver not palpable
• Spleen not palpable
• Ascites not present
d. Respiration:
• Chest clear
• No tracheal shift
• No remarkable findings
Dept of MedicineFrontier Medical and Dental College

General Physical Examination
e. CNS:
No remarkable findings
Dept of MedicineFrontier Medical and Dental College

Examination based Differential Diagnosis
• Myocardial Infarction
• Unstable Angina
Dept of MedicineFrontier Medical and Dental College

Investigations - ECG
Dept of MedicineFrontier Medical and Dental College
Investigations
ECG:
Done within 25 mins of patient arrival
Findings:
• Rate: 78.9
• Rhythm: Sinus Rhythm
Dept of MedicineFrontier Medical and Dental College
Investigations
Leads showing ECG Changes:
• V1 to V6, AvL
• Changes include:
• ST Segment Elevation
• Q wave development
• Loss of R Wave
• T wave inversion
Dept of MedicineFrontier Medical and Dental College

Investigations
• Left Axis deviation seen by thumb rule on Lead 1 and AvF
(For inferior wall MI, changes are seen in: Leads 2, 3 and AvF)
Dept of MedicineFrontier Medical and Dental College

Investigations
Cardiac biomarkers
• Trop T raised
• CK-MB raised
Chest Xray
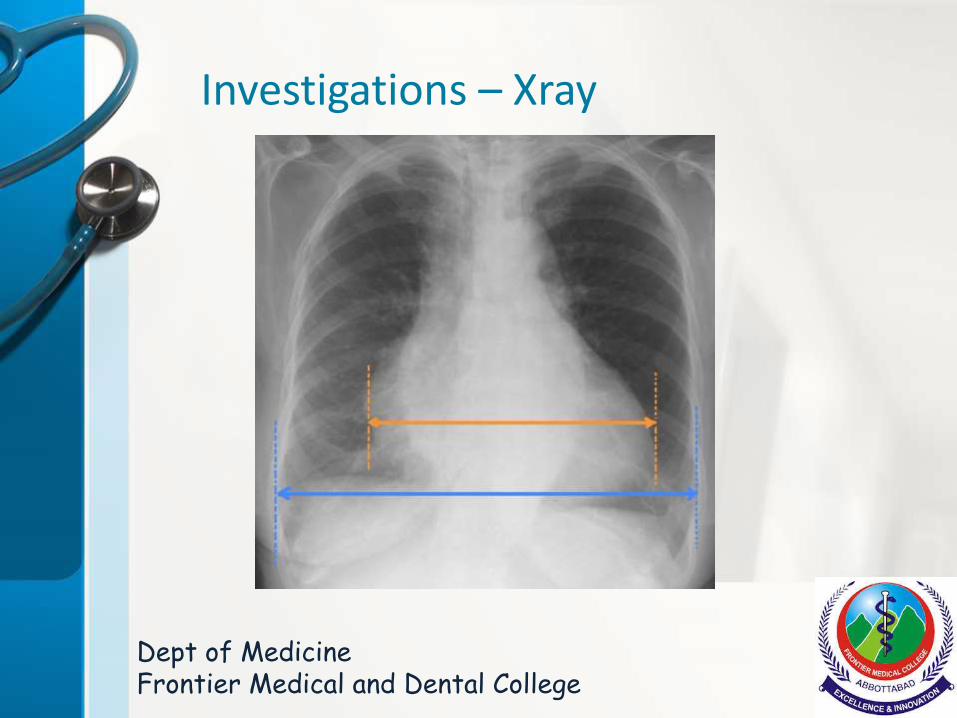
• Cardiothoracic ratio increased showing LV Dilatation
• Pulmonary edema not evident
Dept of MedicineFrontier Medical and Dental College
Investigations – Xray
Dept of MedicineFrontier Medical and Dental College
Investigations
Other Blood Tests
• ESR and CRP raised
Echocardiography could not be done due to the non availablity of facility.
Dept of MedicineFrontier Medical and Dental College

Investigations based Diagnosis
Anterolateral ST Segment Elevation Myocardial Infarction with Left Axis Deviation
Dept of MedicineFrontier Medical and Dental College
Management
• Patient was immediately admitted in ICU. Within 10 mins, ECG was performed and based upon diagnosis, following treatment was given.
• Oxygen + Cardiac rhythm monitoring
Dept of MedicineFrontier Medical and Dental College
Management
• Aspirin 300mg PO
• (Therapy should be continued indefinitely if there are no side affects)
• Clopidogrel 600mg PO followed by 150mg daily for 1 week and 75mg daily thereafter.
• Streptokinase 1.5ml I.V in 100ml sol at 6ml/hr
• Inj Morphine
• Inj Metoclopromide I.V Stat
Dept of MedicineFrontier Medical and Dental College

Late Management
• Patient advised on the following:
• Lifestyle Modification:
• Lipid Lowering diet
• Cessation of Smoking
• Regular exercise
Dept of MedicineFrontier Medical and Dental College
Late Management
• Secondary Drug therapy:
• Aspirin
• B blocker
• Ace Inhibitor/ARB
• Statin
• Additional therapy for DM and HTN
Dept of MedicineFrontier Medical and Dental College
The patient was given Streptokinase (Thrombolysis) within 8 hours of his arrival. He is still in the ICU undergoing 24/7 observation and treatment. He was advised angiography due to the unavailability of the facility at the Hospital. We wish him a speedy recovery.
Dept of MedicineFrontier Medical and Dental College

What is MI ?
• Detection of rise and/or fall of cardiac biomarker values (preferably cardiac troponin) with atleast one of the following:
• Symptoms of Ischemia
• Significant ST segment-T wave changes or new LBBB
• Development of pathological Q waves
• Imaging evidence of new loss of viable myocardium
• Angiographic identification of Intra coronary thrombus
Dept of MedicineFrontier Medical and Dental College
Types of MI
On the basis of ECG, there are two main types of MI
• STEMI (major coronary artery complete obstruction)
• Non-STEMI (Complete occlusion of a minor vessel or partial occlusion of a major coronary vessel
Dept of MedicineFrontier Medical and Dental College

Arterial Supply of the Heart
Dept of MedicineFrontier Medical and Dental College
Arterial Supply of the Heart
Dept of MedicineFrontier Medical and Dental College
Arterial Supply of the Heart
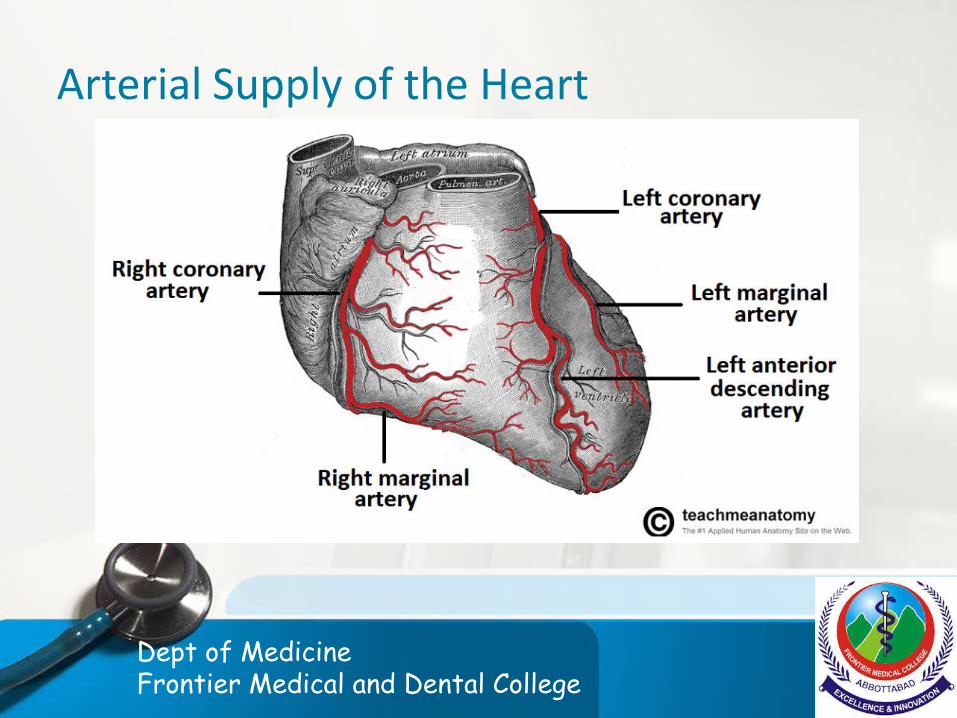
There are two major arteries which supply the heart
• Left coronary artery
• Right coronary artery
1. Left Coronary Artery:
It is further divided into two main branches:
LAD (I/V septum, Ant. Wall of LV and Apex)
LCx (Lateral, Posterior and Inferior Walls)
Dept of MedicineFrontier Medical and Dental College
Arterial Supply of the Heart
2. Right Coronary Artery
It supplies RA, RV and inferio-posterior part of LV
Branches include:
PDA (supplies I/V septum inferior part) In 90% individuals PDA is a branch of RCA. (Right Dominant people)
In 10% individuals PDA is a branch of LCA (Left Dominant)
Dept of MedicineFrontier Medical and Dental College

Arterial Supply of SA & AV Node
• SA Node: RCA in 60% individuals
• AV Node: RCA in 90% individuals
Clinical Significance:
• Proximal RCA occlusion may result in Sinus Bradycardia and may also cause AV Nodal block
• Abrupt occlusion of RCA may lead to infarction of inferior part of LV
Dept of MedicineFrontier Medical and Dental College

Conducting system of Heart
Dept of MedicineFrontier Medical and Dental College
Nerve Supply of Heart
• Adrenergic Nerves from the Cervical Sympathetic chain supply atria and ventricles
• Parasympathetic: Vagus nerve
Dept of MedicineFrontier Medical and Dental College
Pathophysiology of MI
Atheromatous plaque formation
Interplaque haemorrhages
Exposure of Subendothelialcollagen fibers
Formation of micro thrombi
Full blown thrombus
vasospasm
Dept of MedicineFrontier Medical and Dental College

Pathophysiology of MI
Dept of MedicineFrontier Medical and Dental College

Pathophysiology of MI
Dept of MedicineFrontier Medical and Dental College

Pathophysiology of MI
• LCA Occlusion:
LAD occlusion (40-50) leads to
Anterior wall infarction of LV
Anterior portion of ventricular septum
Apex
LCx Occlusion 15-20%
Lateral wall of LV
Dept of MedicineFrontier Medical and Dental College
Pathophysiology of MI
RCA Occlusion (30-40%)
RCA occlusion leads to infarction of
• Posterior wall of RV
• Inferior wall of LV
• Posterior 1/3rd of I/V septum
Dept of MedicineFrontier Medical and Dental College
Clinical features
Symptoms:
• Pain: Crushing, retrosternal chest pain radiating to back, left arm, neck or jaw
• Anxiety and fear of impending death
• Nausea and Vomiting
• Breathlessness
• Diaphoresis
Dept of MedicineFrontier Medical and Dental College
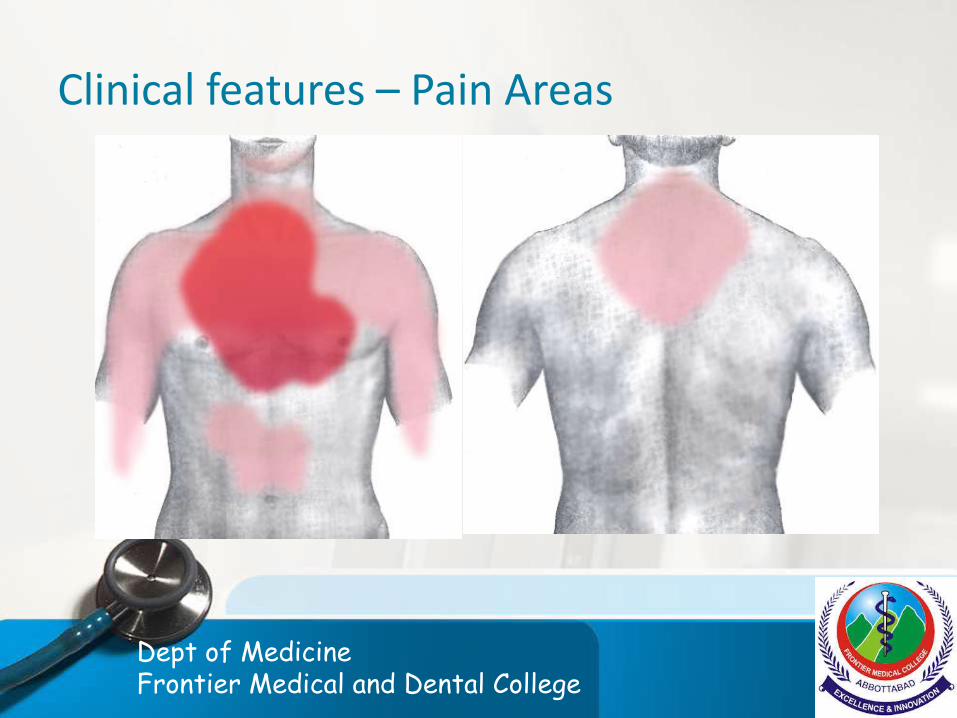
Clinical features – Pain Areas
Dept of MedicineFrontier Medical and Dental College

Clinical features
• Signs
Sympathetic activation:
- pallor
- sweating
- tachycardia
Vagal activation:
-bradycardia
Dept of MedicineFrontier Medical and Dental College
Clinical features
vomiting
• Signs of impaired myocardial function:
Hypotention
Narrow pulse pressure
JVP may be raised
Dept of MedicineFrontier Medical and Dental College

Clinical features
3rd heart sound
Quiet 1st heart sound
Diffuse apical impulse
Lung crepitations
Dept of MedicineFrontier Medical and Dental College
Clinical features
• Signs of tissue damage
fever
• Signs of complications e.g Mitral regurgitation, pericarditis etc
Dept of MedicineFrontier Medical and Dental College

Clinical features
• Silent MI
diabetic patients
Older individuals
Dept of MedicineFrontier Medical and Dental College

Investigations
• ECG
• Cardiac biomarkers
• Chest X-Ray
• Echocardiography
• ESR & CRP
• Angiography
Dept of MedicineFrontier Medical and Dental College

Investigations
• ECG
It is central to confirming the diagnosis but may be difficult to interpret if there is bundle branch block or previous MI. so repeated ECGs are very important.
Dept of MedicineFrontier Medical and Dental College
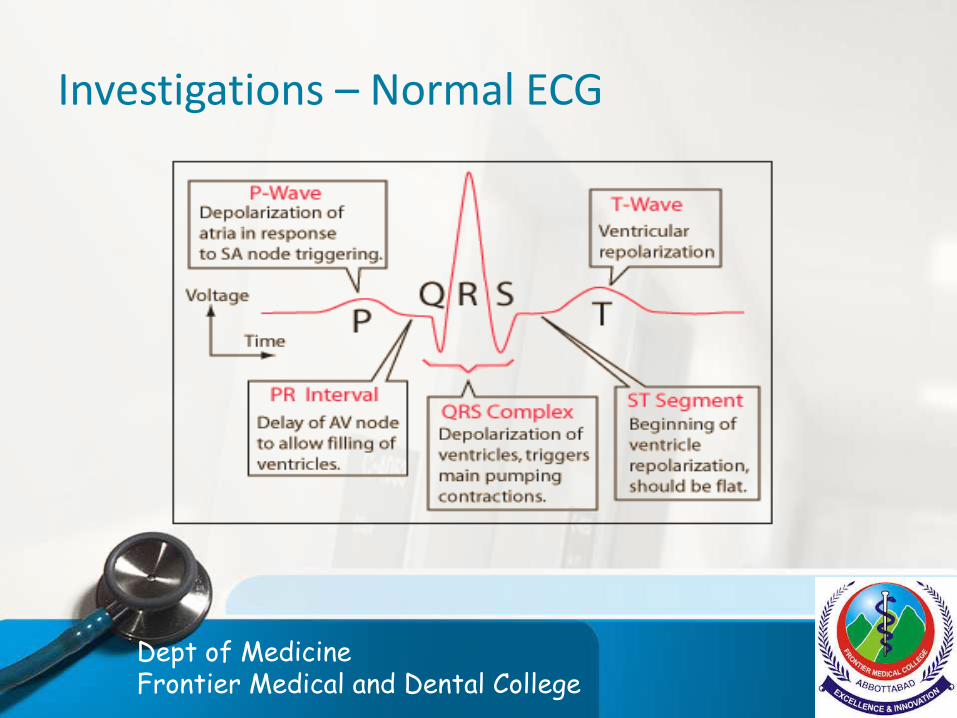
Investigations – Normal ECG
Dept of MedicineFrontier Medical and Dental College
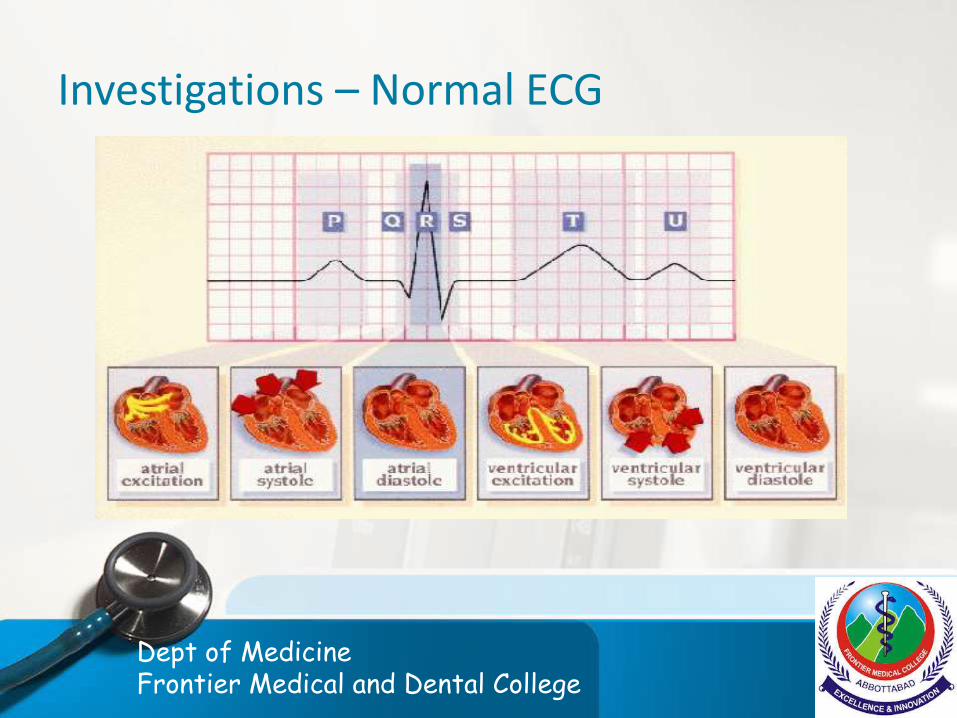
Investigations – Normal ECG
Dept of MedicineFrontier Medical and Dental College

Investigations - ECG
Earliest changes are seen in ST-segment
1. STEMI
• ST-segment elevation
• progressive loss of R wave .
• Development of Q wave .
• Resolution of ST-segment
• T-wave inversion
Dept of MedicineFrontier Medical and Dental College
Investigations - ECG
2. NSTEMI
• St-segment depression
• T-wave changes
• Loss of R-wave
• Absence of Q-wave
Dept of MedicineFrontier Medical and Dental College

Investigations – ECG - STEMI
Dept of MedicineFrontier Medical and Dental College
Investigations - ECG
Significance of chest leads
Antero-septal infarct
v1 ,v2,v3,v4
Antero-lateral
v4,v5,v6 and AVL and 1
Dept of MedicineFrontier Medical and Dental College

Investigations - ECG
Inferior infarction
leads II , III and AvF
Posterior wall infarction doesn’t cause ST elevation or Q-waves in the standad leads but can be diagnosed by the reciprocal changes that is stdepression and a tall R-wave and leads V1-V4.
Dept of MedicineFrontier Medical and Dental College
Cardiac Biomarkers
1. Troponins
2. Creatinine kinases
3. LDH
4. AST
5. Myoglobins
6. Most specific are troponins and CK-MB
Dept of MedicineFrontier Medical and Dental College
Cardiac Biomarkers
1. CK-MB
Rises in 4-6 hours and peaks a 12 hours and falls to normal within 48-72 hours . It is very important. For diagnosis of recurrent MI’s.
2. Troponins: Trop-T and trop-I are gold standards for diagnosis of MI, Troponins rise in 4 to 6 hours and remains elevated for 2 weeks
Dept of MedicineFrontier Medical and Dental College

Investigations- Chest Xray
• Chest Xray to determine cardiomegaly and pulmonary edema
Dept of MedicineFrontier Medical and Dental College
Investigations - Echocardiography
• Useful for assessing ventricular function and determining complications
Eg. Mural thrombus, cardiac rupture , VSD and pericardial effusion etc
Dept of MedicineFrontier Medical and Dental College
Investigations - Other blood tests
1. ESR raised
2. Leucocytosis
3. CRP raised
Dept of MedicineFrontier Medical and Dental College
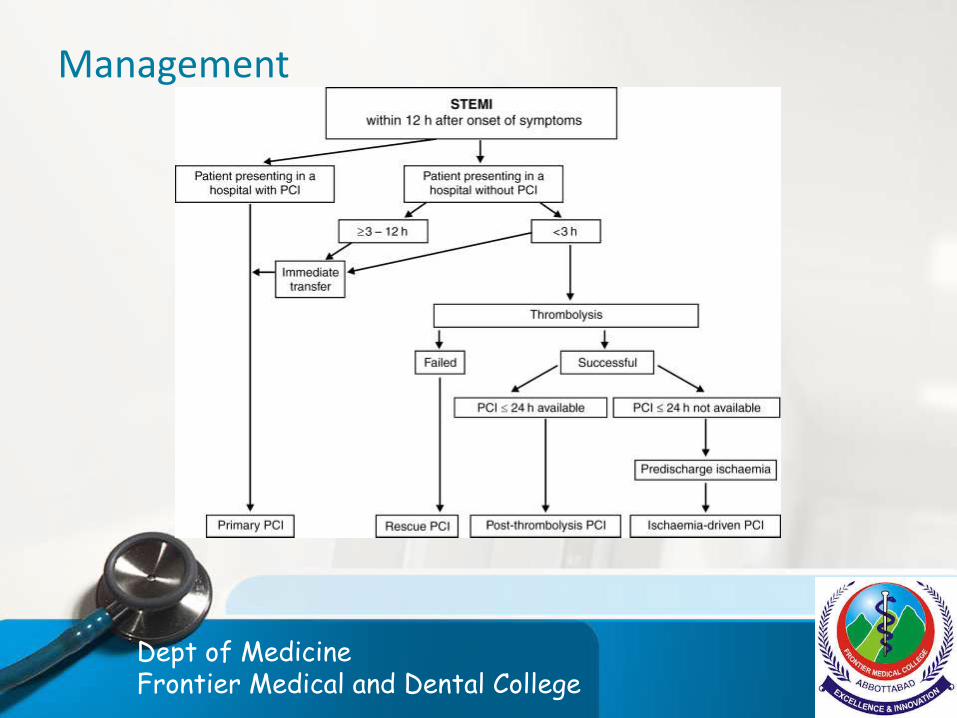
Management
Dept of MedicineFrontier Medical and Dental College

Management
Dept of MedicineFrontier Medical and Dental College
Drugs used in treatment of MI
1. Analgesics
- Opiates: Morphine Sulphate dimorphine
2. Anti-emetics: metoclopromide
3. Anti-thrombotic drugs
a. Anti platelets: Aspirin
- Clopidogrel
- Ticagrelor
- Gycoprotien 2b and 3a receptor antagonists: Abciximab
Dept of MedicineFrontier Medical and Dental College
Drugs used in treatment of MI
b. Anticoagulants :
– LMW Heparin, HMW Heparin, pentasaccharide - fondaparinux
– Warfarin
Dept of MedicineFrontier Medical and Dental College
Drugs used in treatment of MI
4. Anti anginal drugs
- Nitrates: GTN, isosorbide dinitrate
- B blockers: metoprolol and atenolol
5. Dihydropyridine CCBs:
- Nifedipine, amlodipine
6. Thrombolytics:
- Alteplase, streptokinase, retiplase, tenecteplase
Dept of MedicineFrontier Medical and Dental College

Invasive modalities used in the treatment of MI
• PCI (Percutaneous Intervention)
• CABG (Coronary Artery Bypass graft) Surgery
Dept of MedicineFrontier Medical and Dental College
Late Management of MI
Lifestyle modifications
Diet
Cessation of smoking
Weight control
Reguar exercise
Dept of MedicineFrontier Medical and Dental College

Late Management of MI- Sec prevention
• Anti platelet therapy
• B blockers
• Ace inhibitors
• Statins
• Additional therapy for diabetes and HTN control
• Mineralocorticoid receptor antagonist
• Devices: Implantable Cardiac Defibrillators
Dept of MedicineFrontier Medical and Dental College

Complications
• Arrythmias
• Bradycardia
• Acute Circulatory failure
• Pericarditis
Dept of MedicineFrontier Medical and Dental College

Complications - Mechanical
• Rupture of papillary muscle
• Rupture of I/V septum
• Rupture of ventricle which can lead to fatal cardiac temponade
• Embolism
• Impaired ventricular function, remodeling and ventricular aneurysm
Dept of MedicineFrontier Medical and Dental College

Prognosis
• If medical care is not provided, death occurs in almost 1/4th of the cases. Half of the death occurs within 24nhours of the onset of symptoms and about 40% of all affected patients die within the first month.
• Patients who reach the hospital and survive have much better prognosis with a 28 day survival of more than 85%. The prognosis of anterior infarcts is worse as compared to inferior infarcts.
Dept of MedicineFrontier Medical and Dental College
Prognosis
OF THOSE WHO SURVIVE AN ACUTE ATTACK, MORE THAN 80% LIVE FOR A FURTHER YEAR. ABOUT 75% FOR 5 YEARS.
50% FOR 10 YEARS & 25% FOR 20 YEARS.
Dept of MedicineFrontier Medical and Dental College

Thankyou everyone
Dept of MedicineFrontier Medical and Dental Collegev