multiple sclerosis project
TRANSCRIPT

Rehabilitation Systems
Multiple Sclerosis Rehabilitation Program Implementation Manual

Contents
Intro Multiple Sclerosis Rehabilitation 5 1 Multiple Sclerosis Rehab Inclusion Criteria & Evaluation 7 2 Physical Activity for People with Multiple Sclerosis 13 3 Understanding Multiple Sclerosis 16
What is Multiple Sclerosis? 16 What causes Multiple Sclerosis? 17
4 Course of the Disease 19 Relapsing-Remitting MS (RRMS) 20 Secondary-Pro aggressive MS (SPMS) 21 Primary Progressive MS (PPMS) 22 Progressive-Relapsing MS (PRMS) 23 Symptoms of Multiple Sclerosis 24
5 Management of Multiple Sclerosis 26 Benefits of an Exercise Program 27 Differences: Rehabilitation versus Fitness/Wellness 29 Functional Levels: Options for Movement Modifications 30
6 MS Communication 32 Activity 33 Language 34
7 The Environment—Safety and Accessibility 35 The Americans with Disabilities Act: A Summary of Titles 36
8 Functional Assessment 39 SF-36 Health Survey 39 R P E / FT 40 Dyspnea 41 6MWT 42
9 Multiple Sclerosis Patient Education 43 10 Energy Conservation 51 11 Relaxation and Stress Management 53 12 General Dietary Guidelines for MS Patients 55 13 Quick Conversion Chart (MET) 59
Exercise Prescription and Progression 60 14 Individual Therapeutic Session 65
SOAP NOTES 68 15 Functional Capacity: Writing Functional Goals 70
The Compendium of Physical Activities Tracking Guide 73 Rehabilitation Discharge Summary 83 About the Instructor 85 Course Evaluation 86 Glossary 87
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 2

Intro Multiple Sclerosis Rehabilitation
A rehabilitation program for people with MS is designed to meet the needs of the individual patient, depending upon the type and severity of the symptoms and the amount of impairment. Active involvement of the patient and family is vital to the success of the program.
The goal of MS rehabilitation is to help the patient to return to the highest level of function and independence possible, while improving the overall quality of life - physically, emotionally, and socially.
In order to help reach these goals, MS rehabilitation programs may include the following:
• exercises and activities to help improve motor skills, restore activities of daily living (ADLs), and help the patient reach maximum independence
• exercises that promote muscle strength, endurance, and control
• management of bowel or bladder control
• use of assistive devices such as canes, braces, walkers
• methods to improve communication skills for patients who have difficulty speaking
• cognitive retraining
• vocational counseling
• adapting the home environment for ease of function, safety, accessibility, and mobility
• patient and family education
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 3

www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 4

1 Multiple Sclerosis Rehab Inclusion Criteria & Evaluation
Inclusion Criteria: • Confirmed diagnosis of MS • Known neurological and psychological deficits
Exclusion Criteria: • Those with severe cognitive problems.
Demonstrated Outcomes of Multiple Sclerosis Rehabilitation Activity...Not Rest should be encouraged to reduce the effects associated with Multiple Sclerosis. Multiple Sclerosis Rehabilitation Programs are tailored to the unique needs & interests of patients. It has been demonstrated to be safe & effective regardless of previous activity levels. Expect the following benefits from Multiple Sclerosis Rehabilitation: • Improved Quality of Life with Increased Brain Power • Reduced Fatigue, Improves Restorative Sleep • Increased Energy and Improved Muscle Tone • Greater Endurance, Stamina and Robustness • Increased Muscular Strength and Power • Decreased Anxiety and Depression • Enhanced Self-image, Self Concept • Sense of Control over Fitness • Reduction of Painful Sensations • Decreased Fear and Social Isolation • Stronger Immune System
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 5
Multiple Sclerosis Rehabilitation Patient Evaluation Patient Information: Name: _______________________________________Date:_____________________ Address: ___________________________________Phone:______________________ Emergency Contact: __________________________Phone:_____________________ Age: _____Sex:_____Occupation:_______________Retired:_______Disabled:______ Height: _____________Weight:________Marital Status: ________________________ Insurance Provider: _____________Sessions Allowed:__________________________ Diagnosis:_________________________________Date of RX:___________________ Referring Physician:__________________ Primary Care Physician:________________ Presenting symptoms(s): Circle the dot (.) if it applies:
• Vision problems: may include blurred vision, double vision, involuntary eye movements, temporary loss of sight, eye pain.
• Fatigue: may be worse at certain times of day and interfere with daily activities. • Muscle stiffness: include in your description where stiffness occurs and if anything you do relieves
it • Weakness: may include clumsiness, dropping things, inability to pick up things or hold something
in your hand, dragging a leg when you walk • Poor balance: may include changes in the way you walk, dizziness, bobbing from side-to-side
when you walk • Tingling: pins-and-needles sensations, indicate where on your body • Bowel and bladder problems: may include inability to hold urine or bowels, inability to fully
empty bladder or bowels • Pain: may include shock-like sensation, especially down the spine and legs when you bend your
neck forward • Numbness: may include loss in sense of touch as well as reduced ability to feel heat and cold • Problems concentrating: may include difficulty with memory, getting lost in places you are
usually familiar with, sense that your thinking is in a fog • Depression: may include sadness, sense of hopelessness, uncontrollable crying. • Cooling And Thermo-Regulation: Is cooling therapy associated with objectively measurable but
modest improvements in motor and visual function as well as persistent subjective benefits • Stress: positive emotions can enhance the immune system, while negative emotions can suppress
it. • Spasticity: Spasticity is a muscle control disorder characterized by tight or stiff muscles and an
inability to control muscle movement. It may cause hyperactive reflexes, which are abnormally strong and persist for too long.
Allergies: Food □ Medication □ Specify:____________________________________ # of hospitalizations in past year:______ # of days in hospital:______
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 6

Body Composition: This method is the most widely used body composition testing method for assessing percent body fat. Equipment used for this assessment includes a skinfold caliper. Take three measurements at the specified sites, then average measurements and total the averages for a score. 7 Site Skinfold: Chest_________________________________________________________________
Triceps________________________________________________________________
Subscapular____________________________________________________________
Axilla__________________________________________________________________
Suprailiac______________________________________________________________
Abdomen______________________________________________________________
Thigh_________________________________________________________________
TOTAL AVERAGES: PRE:____________________________POST:_____________________________
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 7

Sleep Hygiene: #Hours: __________Pillows Used: ___________Sleep Disturbances: _________ What Kind: ________________Do You Snore: Y/N Does Your Spouse Say You Snore: __________ Do You Wake Up To Breathe Y/N __________ Do You Need To Take Naps Daily: ___________ Do You Take Medication To Help You Sleep: __________________ Activities of Daily Life: Are You Able To Care For Yourself? ________________________________________ Are You Able To Care For Your Home?______________________________________ Do You Exercise? Y/N Type of Exercise & How Often:__________________________ Do You Have Exercise Equipment? Y/N Type:________________________________ Special Interests & Hobbies:______________________________________________ Does Cancer Keep You From Your Activities?_________________________________ Do You Live Alone? _______Do You Have Transportation?______________________ Do You Need Assistive Devices?___________________________________________ Physical Limitation (sensory, stroke, surgeries) ________________________________ Dietary History: Do You Have Trouble Eating? Y/N Why?______________________________________ Do You Have Difficulty Gaining or Losing Weight?______________________________ Special Diet?____________________________________________________________ Appetite: Good______Fair______Poor_____Is This Usual For You?_________________ Vitamins: Y/N Restaurants Per Week?________________________________________ Do You Consume Alcohol: Y/N How Much?____________________________________ Smoke Cigarettes: Y/N How Many?__________________________________________
Pack Years: Packs per day times the years of smoking Psychosocial Assessment:
Present Temperament: score each temperament from (1 to 10) (1=LOW) (10=HIGH) as they apply to you: (Angry, Worried, Sad, Impatient, Frustrated, Depressed, Anxious, Calm, Content, Cheerful, Happy) (____)(____)(___)(______)(______)(_______)(_____)(___)(_____)(_____)(____) Stressors / Fears /Concerns: _______________________________________________ Relaxation Techniques You Use:____________________________________________ You’re Most Difficult Adjustment Since MS?________________________________ Do You Forget Often? Y/N Do You Have A Support System: Y/N Who?:_____________ Do You Understand Your Diagnosis:_________________________________________
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 8

Medical History: Check ALL spaces below that apply to the patient. Explain and Date: _____High blood pressure_________________________________________________ _____Chest discomfort____________________________________________________ _____Heart Problems_____________________________________________________ _____Coughing up blood__________________________________________________ _____Stomach or intestinal problems________________________________________ _____Anemia____________________________________________________________ _____Stroke_____________________________________________________________ _____Migraine or recurrent headaches_______________________________________ _____Dizziness or fainting spells____________________________________________ _____Leg pain after walking short distances__________________________________ _____Back/neck pain/injury_______________________________________________ _____Foot/ankle problems_________________________________________________ _____Knee/hip problems__________________________________________________ _____Lymphedema_______________________________________________________ _____High cholesterol____________________________________________________ _____Diabetes__________________________________________________________ _____Respiratory problems/asthma__________________________________________ _____Increased anxiety / depression_________________________________________ _____Recurrent fatigue____________________________________________________ _____Arthritis____________________________________________________________ _____Swollen/stiff/painful joints_____________________________________________ _____Epilepsy___________________________________________________________ _____Vision/hearing problems________________________________________ Physical Assessment: 1. Range Of Motion: ______________________________________________________________________________________________________________________________________________ 2. Strength: 1RM / 3RM, ______________________________________________________________________________________________________________________________________________ 3. Functional Capacity / Independence: 6 Minute Walk Test. PRE: Distance:________Time:________HR:________RPE:________DYSP/FT:_______ POST:Distance:________Time:________HR:________RPE:________DYSP/FT:_______ List the Short Term Goals on Lines 1 – 3 for Cancer Rehabilitation. List the Long Term Goals for the Patient’s Quality of Life on Lines 4 – 5. 1. _____________________________________________________________________ 2. _____________________________________________________________________ 3. _____________________________________________________________________ 4. _____________________________________________________________________ 5. _____________________________________________________________________
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 9

(MET) to Functional Task Conversions 3.0; home activities; cleaning, wash car, wash windows, clean garage 3.5; home activities; mopping 3.0; home activities; cleaning, house or cabin, genera 3.5; home activities; vacuuming 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing - packing/unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; lawn and garden; riding snow blower 2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; music playing; conducting 2.5; music playing; piano or organ 2.5; music playing; violin 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside 2.0; home activities; standing-light (pump gas, change light bulb, etc.)
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 10

2 Physical Activity for People with Multiple Sclerosis An Education Manual for Health and Wellness Professionals
Edited by
Deborah P. Hertz, MPH National Director, Medical Programs Clinical Programs Department National Multiple Sclerosis Society New York, NY 212-476-0468
Contributors:
Helen Tilden, RN, NMSS, Georgia Chapter Clinical Advisory Committee & NMSS Special Project Consultant Miranda Mirsec MA, CES, NMSS Southern California Chapter Programs Manager, Physical Health and Recreation Brian Hutchinson, MS PT, President, Heuga Center & NMSS Clinical Consultant National Multiple Sclerosis Society, © 2004
The Professional Resource Center (PRC) of the Clinical Programs Department supports the work of health professionals by providing a range of library and literature search services, as well as information and consultation about the disease and its management, insurance and long-term care issues, and the Society’s professional education opportunities. Acknowledgements This manual has developed over time thanks to the efforts of many Society chapter staff and volunteers. Connie Divine, TRS, Patricia Finlay, McSP/PT and Helen Tilden, RN, of the Georgia Chapter, developed an aquatics manual in 1993 that was subsequently adopted as a national model. The vision for the new format, including a generic part A and a discipline specific part B came from Denise Nowak, RD (also certified by the American Council on Exercise) and Miranda Mirsec, MA, CES of the Southern California Chapter.
The manual was reviewed by Dr. Corey Ford, MD, PhD, of the National MS Society’s Professional Education Committee and Nancy Holland, EdD, RN, MSCN, Vice President, Clinical Programs Department.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 11

Overview There is strong interest, among many people with multiple sclerosis (MS) to participate in physical activity programs. Individuals with MS involved in exercise programs may experience an increased sense of well-being in addition to other benefits such as, increased muscle strength and endurance, maintained and improved joint range of motion and flexibility, improved coordination, improved balance and increased cardio-respiratory endurance. (See Benefits of Exercise for more information.) Choosing to work with this population can be a rewarding experience, both for the participant and the instructor. The National Multiple Sclerosis Society is delighted you have taken an interest in this course. This manual is meant to be a resource to you; one that provides an overview of MS the disease and offers specific strategies for working with a diverse MS population.
Course Objectives: Upon completion of the Physical Activity for People with MS: Education Program for Health and Wellness Professionals, participants will be able to:
describe basic facts about multiple sclerosis
identify MS symptoms that affect movement and activity level
apply exercise movements appropriate for people with MS
modify exercise movements to an individual's needs and abilities
develop appropriate exercise session formats for people with MS with varying functional levels.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 12

3 Understanding Multiple Sclerosis What is Multiple Sclerosis?
Multiple sclerosis (MS) is a chronic, often disabling disease of the central nervous system (CNS), which includes the brain, spinal cord and optic nerves.
It is one of the most common neurological diseases that affects young adults. Random attacks (also called relapses or exacerbations) damage myelin - the protective coating
surrounding nerve fibers that acts as insulation for the nerve impulses. This causes scarring, called plaques or lesions. The name multiple sclerosis comes from the multiple areas of scarring that characterize the disease process. The resulting inflammation, loss of myelin, scarring as well as damage to the nerve fibers (axons) themselves leads to a disruption of nerve signals with the CNS. These conduction problems produce the symptoms that characterize the disease. Until 1998, it was believed that any damage to the nerve fibers (axons) themselves was secondary and less substantial than the damage to the myelin sheath. A study (Trapp, BD, Peterson J. Ransohoff, RM, et al. “Axonal transection in the lesions of MS”. N Eng. J Med. 1998; 338:328-337) however, provided new evidence that the axons can become irreversibly damaged as a consequence of the immune system’s attacks on myelin and the inflammation that occurs during relapses. This irreversible axonal loss, which can occur even in the earliest stages of the disease, may be a major cause of the persistent neurologic deficits in multiple sclerosis. Symptoms of MS are highly variable in type and frequency from person to person. Symptoms can include abnormal fatigue, visual problems, stiffness, weakness, numbness, pain, imbalance, bladder and bowel problems, sexual dysfunction, speech and swallowing difficulties, emotional changes and problems with memory and thinking.
MS affects approximately 400,000 people in the United States. It is usually diagnosed between the ages of 20 and 50, but has been known to make its first appearance in early childhood or well after 60. MS is 2-3 times more likely to occur in women than in men. MS is most prevalent in people of northern European heritage, but it is also found among African-Americans, Hispanics and Asians. It is also more common in temperate regions than in the tropics.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 13

What causes Multiple Sclerosis? While the precise cause of MS is still unknown, decades of research indicate that multiple sclerosis may be the result of an abnormal immune (autoimmune) response to some infection or environmental trigger in a genetically susceptible individual.
An Autoimmune Disorder Under normal circumstances, the immune system of the body is activated when a foreign agent, such as a virus, enters the body. Multiple sclerosis is thought to be an autoimmune disease, in which the body’s immune system attacks apparently healthy tissues (i.e. the myelin sheath surrounding the nerve fibers and the nerve fibers themselves) in the central nervous system. The exact antigen (the target that the immune cells are sensitized to attack) remains unknown. The damage causes nerve impulses to be slowed or halted, thus producing symptoms.
An Initiating Event Although most experts believe MS begins when an abnormal immune response is first mounted against an infectious agent, no single causative virus or bacterium has yet been identified. It is possible that several viruses or bacteria are capable of triggering the response that leads to MS, though we still do not know which, if any might be the culprit.
Environment Data suggest that exposure before puberty to some environmental agent may predispose a person to develop MS. Migration patterns and epidemiologic studies (that take into account variations in geography, socioeconomics, genetics, and other factors) have shown the following: People who are born in an area of the world with a high risk of MS, and move to an area with a lower risk before 15 years of age, acquire the risk level of their new home
People who move after age 15 carry the risk associated with their old home.
All in the Family? While genetic susceptibility may play a role in the development of the disease, it is far subtler than in other diseases, such as diabetes or breast and colon cancer. MS is not directly inherited, and while persons with close relatives who have MS are at a somewhat greater chance of developing the disease, the overall risk remains relatively low. Support for this conclusion comes from the fact that an identical twin of a person with MS has only a 30 percent chance of developing MS rather than a 100 percent certainty. Scientists theorize that MS develops in individuals who are born with a genetic predisposition to react to some environmental or infectious agent. Exposure to that agent then triggers the autoimmune response. Research has demonstrated a higher prevalence of certain genes in populations with high rates of MS. Common genetic factors have also been found in some families where there is more than one person with MS.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 14

4 Course of the Disease The course of multiple sclerosis is unpredictable and may be characterized by periods of time when symptoms intensify (relapses) or improve (remissions). In other instances MS may appear as a progressive type manifested by a continuous increase in disability. Although the following categories have come to play a significant role in MS research and management decisions, they were designed to be descriptive in nature rather than a “report card” or rating scale of a person’s disease. A particular individual may not fit neatly into one category or another. It is important to keep in mind that these disease categories serve primarily as a tool for development of clinical research protocols, and as a guide for certain types of treatment decisions.
The four categories used to classify the clinical course in persons with MS, which are the result of an international survey are:
Relapsing-remitting
Primary-progressive
Secondary-progressive
Progressive-relapsing
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 15

Relapsing-Remitting MS (RRMS)
RRMS is characterized by clearly defined acute attacks with full recovery (1a) or with residual deficit upon recovery (1b). Periods between disease relapses characterized by a lack of disease progression. Epidemiological studies indicate that approximately 85% of people are diagnosed initially with relapsing-remitting MS.
time time
increasing disability
increasing disability
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 16

Secondary-Pro aggressive MS (SPMS) SPMS begins with an initial relapsing-remitting disease course, followed by progression of variable rate (2a) that may also include occasional relapses and minor remissions and plateaus (2b). Epidemiological studies indicate that of the approximately 85% who start with relapsing-remitting disease, more than 50% will develop SPMS within 10 years; 90% within 25 years.
increasing disability
time
time
increasing disability
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 17

Primary Progressive MS (PPMS) PPMS is characterized by progression of disability from onset, without plateaus or remissions (3a) or with occasional plateaus and temporary minor improvements (3b). Epidemiological studies indicate that no more than 10% of people are diagnosed with PPMS.
time
increasing disability
time
increasing disability
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 18

Progressive-Relapsing MS (PRMS) PRMS, which is the least common disease course shows progression from onset, with the later appearance of clear acute relapses, with (4a) or without (4b) full recovery. Epidemiological studies indicate that only about 5% of people appear to have PRMS. time
increasing disability
time
increasing disability
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 19

Symptoms of Multiple Sclerosis The three categories of symptoms are primary (noted below), secondary and tertiary. Primary symptoms are a result of demyelination and/or axonal damage, secondary symptoms occur as complications of primary symptoms (e.g. pressure sores) and tertiary symptoms are the result of psychosocial complications associated with MS. Symptoms vary greatly from individual to individual and not every person with MS will experience all of the symptoms listed. The most common primary symptoms of multiple sclerosis are:
Motor Weakness Spasticity/spasms Lack of coordination Loss of balance Gait difficulties Tremors Swallowing difficulties (dysphagia) Speech disorders (dysarthria)
Sensory Numbness Tingling, "pins and needles" Burning Pain
Visual
Blurred vision Double vision Blind spots Blindness Nystagmus (lateral or circular eye
movements)
Bowel and Bladder
Urgency Frequency Nocturia Hesitation/retention Incontinence Constipation
Other Symptoms Vertigo (a sensation of spinning) Depression Sexual dysfunction Emotional lability (in-appropriate
laughing or crying)
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 20

Cognitive Approximately 50-60% of people with MS experience some degree of cognitive dysfunction, but the vast majority of these problems are mild. The types of cognitive dysfunction commonly seen in MS involve short-term memory loss, impaired concentration and difficultly in word processing. Fatigue Fatigue is probably the most common symptom experienced by people with multiple sclerosis, however the reason for the fatigue is unknown. MS fatigue is commonly described as a feeling of "exhaustion" or being "wiped out", with reported worsening in mid-to-late afternoon, and unrelated to the level of exertion. Heat Intolerance Increased environmental temperature may cause a temporary worsening of MS symptoms. Heated swimming pools, outdoor temperatures and hot baths often can lead to such problems. Increased core body temperatures associated with fever or physical exertion can have the same effects. Heat intolerance or heat sensitivity has an impact on the symptoms of the disease, not on the disease itself. Psychological Aspects of MS The psychological aspects of multiple sclerosis, and the effects on families, significant others, friends, employers, colleagues or neighbors are of major importance to the MS community. The age group of those affected, the unpredictability of the disease, and the social, financial and emotional impact of MS complicate the adaptation and coping processes.
Diagnosis There is no single test that can determine whether a person has MS. The diagnosis is a clinical one, made on the basis of medical history, signs detected by the physician during a neurologic exam, and symptoms reported. A definitive diagnosis of MS requires the following:
Evidence of plaques or lesions in two distinct areas of the central nervous system Evidence that the plaques occurred at discrete points in time The plaques in the white matter of the CNS have no explanation other than MS
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 21

5 Management of Multiple Sclerosis
Although there is no known cure for the disease, treatments for the person with MS fall into six main categories:
Management of acute attacks (also called exacerbations or episodes)
Symptom management
Modification of disease course (finding ways to reduce the number of exacerbations, reduce the accumulation of lesion area in the CNS, slow or halt disease progression, and slow progression of disability)
Rehabilitation (to enhance and maintain physical function)
Psychosocial support
Preventative health/wellness management
About the National Multiple Sclerosis Society
The National MS Society…dedicated to ending the devastating effects of MS The National Multiple Sclerosis Society (Society) was founded in 1946 by Sylvia Lawry to pursue a cure for MS. Since its inception, the Society—with its nationwide network of chapters--has worked to find a cure for MS, to improve the quality of life for people with MS and their families and to promote quality MS care through partnerships with the medical community. Nationwide, assistance is provided to over a million people annually.
The National Multiple Sclerosis Society supports more MS research, offers more services to people with MS and provides more professional education programs than any other MS organization in the world.
To contact the chapter nearest you call 1-(800) FIGHT-MS or find us on the web at www.nationalmssociety.org
The National MS Society …a nationwide resource for professionals The Professional Resource Center (PRC) of the Clinical Programs Department supports the work of health professionals by providing a range of library and literature search services, as well as information and consultation about the disease and its management, insurance and long-term care issues, and the Society’s professional education opportunities.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 22

Benefits of an Exercise Program A sedentary lifestyle, for anyone, leads to deconditioning. Exercise decreases the risk of heart disease, decreases resting blood pressure, aids sleep, strengthens bones, increases flexibility, endurance, energy and can elevate one’s sense of well being. While exercise has not been shown to slow the progression of MS, it can help decrease complications that arise from muscular fatigue, weakness, contractures, and spasticity. Additionally, exercise can serve as an outlet for stress reduction and help maximize independence, regardless of one’s ability.
Researchers at the University of Utah demonstrated the benefits of exercise for people with MS. Those people with MS who participated in an aerobic exercise program had better cardiovascular fitness, better bladder and bowel function, less fatigue and depression, a more positive attitude, and increased participation in social activities. (Petajan JH, Gappmaier E, White AT, et al. “Impact of aerobic training on fitness and quality of life in multiple sclerosis”. 1996 Ann Neurol; 39: 432-441.)
For people with MS involved in an exercise program, it is believed that:
Breathing can become deeper and more regular
Circulation can increase, bringing oxygen throughout the body
Flexibility can increase and joint range of motion can improve
Fatigue and balance issues can be addressed
Secondary complications of spasticity, muscular tension and muscle atrophy can decrease
Level of independence may increase
Skeletal structural alignment can improve
Muscles and joints can be strengthened
A general feeling of well being ensues
Swelling/edema can decrease
Isolation and depression may decrease
Weight maintenance/reduction is facilitated
Tolerance for exercise can increase
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited.
23

General teaching tips: Choosing appropriate variations and types of activities is an important step.
When planning an exercise program, it is important to incorporate flexibility, strengthening and cardiorespiratory/(aerobic) activities. The needs of the participants will dictate where emphasis needs to be placed.
Frequency, intensity and time (FIT) considerations are important – adjustments to these parameters will help individuals achieve their goals.
Activities need to be enjoyable for participants. Adherence to an exercise program is often related to the amount of enjoyment derived.
If an individual is having difficulty initiating or maintaining an exercise/physical activity program, recommend that they consult with a healthcare or fitness professional with expertise in MS. These individuals may be able to provide specific exercises that will increase success and adherence with an activity program. Always remember, of course, to recommend that a person consult with his/her physician if s/he has any questions about whether a new exercise program it is right for him/her or if symptoms change.
Differences: Rehabilitation versus Fitness/Wellness
Treatment, care, and wellness programs are all important components for maximum functional outcomes and independence. Although skills, education, and goals differ for each discipline, as a team effort, the client benefits with a complete program.
The following chart helps clarify professional roles:
Health (Rehab.) Professional Fitness/Wellness Professional
Professional meets state requirements for licensure and/or registration.
No standard requirements
Assesses neurological manifestations and evaluates quality of movement. Muscle tone, posture, joint mobility, pain, vision and balance are also evaluated to contribute to a specific individualized program.
Uses general screening techniques and assessment information provided by healthcare professional and client. It can consist of questions re: health history, and non-invasive fitness testing (strength, flexibility, etc.).
Develops treatment plan and collects data for attaining and maintaining optimal level of functional independence. Treatment-based programs usually focus on affected area.
Designs and implements fitness/wellness programs that address the body as a whole.
“Hands On”: Client may need “Hands Off”: Participant performs
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 24

Health (Rehab.) Professional Fitness/Wellness Professional
assistance to perform movement. Therapist may facilitate or assist with movement of limbs and/or add manual resistance to movement.
exercises independently - touching participant is limited to spotting and guiding/cueing.
Session objective is on improving function until a plateau or stable condition is reached.
Session objective is over-all physical and mental well-being and achieving overall fitness goals
Provision of one-on-one service. “Customers” are called patients or clients. Treatment is sometimes done in groups.
Provision of group and one-on-one services. “Customers” are called students/participants (group setting) and clients (one-on-one setting).
Settings include: hospitals, rehabilitation centers, clinics, private office or homes.
Settings include: gyms, studios, fitness centers, homes and preventative health settings (along with healthcare professionals)
Functional Levels: Options for Movement Modifications
The following levels are intended to assist the health, fitness, and wellness professional in designing exercise programs and class formats that address the needs of a group with mixed functional levels. Modifications suggested (in part B) are intended as a guide to assess participants and adapt movements and not as a means to categorize students/clients. When designing a class or one-on-one training session keep the following three levels in mind.
It is important to remember that symptoms of MS are different for each individual and may change daily or weekly. Be sure to discuss any specific limitations with each student. Whenever possible involve participants throughout the adaptation process so that they can modify a movement to best meet their needs.
Level 1 These individuals may have no symptoms or mild symptoms. (See list of symptoms on pages 9-10A). These people will walk independently or use a cane, although they may be experiencing symptoms that are not outwardly visible to the instructor.
Level 2 These Individuals have more motor-physical limitations and are more dependent on assistive devices such as walkers and wheelchairs for mobility. They have good transfer skills, but may need additional help getting into a chair, onto the floor or into the pool. They may require assistance with balance while participating in a class.
Level 3 These individuals have greater functional impairment and may experience paralysis and spend most of their time in a wheelchair. These participants may need personal attention
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 25

and may require an assistant. (Note: an exercise class is not intended to replace rehabilitation therapy or personal training.)
Equipment Usage and Analysis Equipment can enable an individual to complete a movement action or position, when range of motion, flexibility or individual symptoms would otherwise prohibit it. In this way, full benefits of the exercise or position are garnered without stress, strain or injury. Equipment can also be used to increase or decrease intensity and add challenge or variety to activities.
An important first step in selecting the appropriate exercise equipment is to determine the needs of the students. Next, evaluate specific pieces of equipment to determine which type will best address these needs. Once you have made a selection, knowing how to use it correctly is essential. Equipment that is effective as an exercise tool can also be ineffective and damaging when used inappropriately. When used correctly they can be excellent tools for modification/adaptation or intensification of movements.
Evaluate the following when determining appropriate equipment use:
Establish intended use/application
Assess for correct body mechanics during use
Identify contraindications/risks
Determine benefits
Determine the ability of the client
Identify tool limitations (cost, availability, intended ability level, etc.)
Determine desired action or benefit you wish to impart.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 26

6 MS Communication Activity Limitation 101 This is meant to encourage sensitive communication with people who have activity limitations. Etiquette
1. When introduced to a person with an activity limitation, it is okay to offer to shake hands. (If you notice the person does not have a right hand or the right hand is not functional, use your left. This is socially acceptable.)
2. Speak directly to the person with an activity limitation, not the attendant or companion.
3. If you are dealing with an adult, treat her/him as such.
4. A wheelchair is part of a person’s personal space. It is not okay to lean on it.
5. When speaking to a person who uses a wheelchair, try to place yourself at eye level to that person—however, do not lean over in a condescending manner. Sit in a chair or squat if you are going to have a long conversation.
6. Wait until you are asked for assistance. Do not assume someone wants or needs help. If you notice, however, that someone is struggling (e.g.-getting over a sidewalk lip) do not ignore the situation, simply ask if assistance is desired then wait for the reply. Assume that the person is the expert on what s/he needs, so respond accordingly.
7. When approaching a person with a visual impairment, always identify yourself immediately. Identify yourself before you speak especially if there are many voices in the room as it is difficult to know who is speaking.
8. When conversing with a person with speech problems, be patient, and let him/her speak at a comfortable pace. Never pretend you understand if you are having difficulty. It is okay to ask a person to repeat. It is also appropriate to repeat what you think you heard, and ask for confirmation or correction.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 27

Language A person with an activity limitation is a person first. Labeling implies that a disability is someone’s primary attribute and makes most people very uncomfortable. Avoid words and phrases with negative, stereotypical, or judgmental connotations.
ACCEPTABLE UNACCEPTABLE
Person with a disability
Person with multiple sclerosis/MS
People with disabilities
Person with an activity limitation
Person with a participation restriction
Crippled, afflicted, sufferer, deformed, invalid
MS client, MS patient, MS’er, victim of MS, the MS person
The disabled, the handicapped
(These are derogatory labels. Do not refer to a person in terms of a condition)
Person who uses a wheelchair
Wheelchair user
Wheelchair-bound
Confined to a wheelchair (w/c) (A w/c is a mode of transportation, like feet. A person is not tied or stuck in it permanently)
Congenital disability Birth defect, affliction
People without disability
People without activity limitations
Temporarily able bodied (TAB)
Normal person
Poor, Pitiful, Unfortunate
Do not refer to a person as courageous or brave, having a disability does not automatically make you a hero. Most importantly, all people are different and react to certain words differently. When in doubt, always ask – do not make assumptions. “Client” describes a role a person takes in relationship to a service provider, not a description of the person him/herself. Anyone who comes to the NMSS for assistance is a “client”, which is not synonymous with “person with MS.” In group settings individuals are “students” or “participants” not “patients” (unless you hold a medical or healthcare degree and the class is considered therapy/treatment i.e. not a recreation/wellness class).
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 28

7 The Environment—Safety and Accessibility
Participant Safety Precautions to remind participants of at the beginning of each class:
Encourage participants to advise instructor about medications being taken that could impact attention, balance, concentration, etc.
Each participant needs to know his/her own limitations and to exercise at his/her own pace. Classes are not competitive in nature and each participant has his or her own situation, which may change from week to week. Short breaks during the class are appropriate and recommended if needed.
Any time a person experiences new difficulty with the exercises in class or symptoms increase, recommend that he/she contact his/her physician.
Facility Accessibility An accessible facility is a must for a successful MS aquatics program. Facility accessibility is defined in Title III of the Americans with Disabilities Act (ADA)--enacted in January of 1992 to prohibit discrimination by places of public accommodation against those with disabilities.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 29

The Americans with Disabilities Act: A Summary of Titles EMPLOYMENT (Title I) Employers may not discriminate against a person with a disability in hiring or promotion if the person is other wise qualified for the job. Employers must provide “reasonable accommodation” to persons with disabilities, including such steps as job restructuring and modification. PUBLIC SERVICES AND TRANSPORTATION (Title II) State and local governments may not discriminate against persons with disabilities and accessibility must be provided for public transit buses, rail lines, and bus and train stations. PUBLIC ACCOMMODATION (Title III) Persons with disabilities are to be provided accommodations and access equal to, or similar to, that available to the public…barriers are to be removed when readily achievable…easily accomplished with minimal difficulty or expense. TELECOMMUNICATIONS (Title IV) Companies offering telephone service to the public must offer telephone relay service to persons who use telecommunications devices for the deaf (TDDs) or similar devices.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 30

Accessibility Checklist for Facilities Entrances and Doors
Is there an approach path without stairs? (Y/N)
Is the path stable, firm and slip-resistant? (Y/N)
Is the path at least 36” wide? (Y/N)
Is the main entrance free of barriers/steps, etc.? (Y/N)
If there are barriers, is there another accommodation such as a ramp, lift, or alternative accessibly entrance? (Y/N)
Are there accessible entrance doors? (Y/N)
___ Clear opening of at least 32” wide
___ Door handles are no higher than 48”
___ Can be operated with a closed first
___ Interior doors do not require more than 5 pounds of force to operate (local fire regulations may pre-empt this)
___ Doors with closers take at least 3 seconds to close
___ Doors have a level threshold (less than ¼” high) or beveled (no more than ½” high)
___ Doormats are no higher than ½” and be secured to the floor at all edges
Ramps Do ramps have slopes no greater than 1:12 (which means that for every one inch of
height or rise, there are 12 inches (one foot) of ramp “length” or “run.” (Y/N)
Do ramps longer than 6 feet have railings on both sides? (Y/N)
Do ramps have a non-slip surface? (Y/N)
Lockers and Showers Do entrances and doors to locker rooms have a clear opening of at least 32”? (Y/N)
Do entrances, and doors to locker rooms provide necessary clearances for guests with restricted mobility? (Y/N)
Do locker rooms include accessible lavatories, urinals, water closets, showers, dressing booth, and lockers as well as provide an accessible route from the entrance to these fixtures? (Y/N)
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 31

Swimming Pool
At least one pool entry/exit is provided for people with restricted mobility. (Y/N)
Do steps into swimming pools have slip-resistant treads or finish? (Y/N)
Are there handrails at steps to provide support to the user on both the right and left side? (Y/N)
Is the pool temperature between 80-84? (Y/N)
Is there a lift available? (Y/N)
Miscellaneous
• Are staff members available to assist with mobility needs, if necessary? (Y/N)
• Are there accessible fire exits/emergency procedures for people with limited mobility? (Y/N) If so, where are they located?
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 32

8 Functional Assessment SF-36 Health Survey
Physical Functioning Score (PFS)
Example of processing a score of 21 from the question above: A Physical Functioning raw score of (21) is converted as follows: (21 – 10) ---------------- X 100 = 55 20 PRE PROGRAM: SF 36 PFScore:_________ POST PROGRAM: SF 36 PFScore:_________
The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much? (Please circle one number on each line.)
Activities Yes, limited a lot
Yes, limited a little
Not limited at all
1. Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports.
1 2 3
2. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf.
1 2 3
3. Lifting or carrying groceries. 1 2 3 4. Climbing several flights of
stairs. 1 2 3
5. Climbing one flight of stairs. 1 2 3 6. Bending, kneeling, or stooping. 1 2 3 7. Walking more than a mile. 1 2 3 8. Walking several blocks. 1 2 3 9. Walking one block. 1 2 3 10. Bathing or dressing yourself. 1 2 3
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 33

R P E / FT Ratings of Perceived Exertion
Ratings of Fatigue Threshold
How much are you (working / fatigued?)
MODIFIED 10 POINT BORG SCALE
0 Nothing at all 0.5 Very, very slight (just noticeable) 1 Very slight 2 Slight (light) 3 Moderate 4 Somewhat severe 5 Severe (heavy) 6 7 Very severe 8 9 10 Very, very severe (maximal)
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 34

DYSPNEA SHORTNESS OF BREATH (SOBr)
How much are you breathing?
MODIFIED 10 POINT BORG SCALE
0 Nothing at all 0.5 Very, very slight (just noticeable)
1 Very slight 2 Slight (light) 3 Moderate 4 Somewhat severe 5 Severe (heavy) 6 7 Very severe 8 9 10 Very, very severe (maximal)
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 35

6 - MINUTE WALK TEST (6MWT)
Resting Data: Name: ___________________________ Date: _________
HR RPE SOBr % Spo2 FiO2/ LPM
6MWT HR RPE SOBr %Sp02 FiO2/LPM
Distance Walked
1 MIN Checkmark
2 MIN Checkmark
3 MIN Checkmark
4 MIN Checkmark
5 MIN Checkmark
6 MIN Checkmark Feet:
TOTALS Checkmarks = 100ft
100ft = one length. Total feet:
Comments: i.e., signs and symptoms, angina, dizziness, stopped/paused before 6 minutes, reason why, etc. Therapist: Date:
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 36

9 Multiple Sclerosis Patient Education
Introduction Among the first things people are told after being diagnosed with multiple sclerosis are that the course of the disease is unpredictable and there is no cure. These statements are true at the present time, but they do not mean that there is nothing you can do. A disease modifying therapy that reduces the number of attacks and may slow the disease course and delay onset of permanent disability may be right for you. In addition, people live well with MS by making the most of what they have and using a variety of strategies to maintain function even if problems develop. In short, they manage MS with a rehabilitation approach in order to prevent MS symptoms from shutting them off from life.
What is Rehabilitation? Rehabilitation addresses maintaining and restoring function in order to maximize your abilities at work, at home, and in the community. Rehab can address problems with walking, dressing and personal care, performing tasks at work, and can teach the appropriate use of mobility aids such as a cane or wheelchair. It also addresses speech and memory problems, sexual difficulties, bladder and bowel needs, and overall fitness. Restorative rehabilitation aims to restore lost function. This usually involves strengthening and retraining muscles as well as adapting to decreased function with new techniques. Restorative rehabilitation is especially useful following an exacerbation or acute attack of MS symptoms. Maintenance or preventive rehabilitation aims to preserve function even as the disease worsens. Preventive rehab may also help slow down losses of ability and prevent unnecessary problems or complications.
Who Can Benefit? Everyone with MS, whether their symptoms are mild or severe, can benefit from rehabilitation! Recently published scientific studies have demonstrated sustained functional benefit for persons with MS who participated in supervised rehabilitation programs. For those people with mild or “invisible” symptoms, a rehab approach stresses education, energy management, and physical fitness. Doing a rehab program early on can establish positive behavior patterns that will come in handy should other problems surface later. When disabilities are more severe, rehab focuses on making the most of existing strengths and abilities. Rehab also has something to offer friends and family. Part of a rehab program may well involve learning how to deal with changes, modify environments to reduce restrictions, and teach other people how to give assistance in ways that are physically and emotionally beneficial to you. A program can also help people protect their important personal relationships by helping individuals recognize the impact of their MS on other people. In other words, rehab may help you keep your perspective.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 37

Home Based Rehabilitation Your neurologist, family doctor, nurse, or other healthcare professional may refer you to a rehab clinic or to therapists in private practice. However, Applegate Homecare is a home based rehabilitation program. Integrated programs not solely devoted to MS can be found in physical medicine and rehabilitation (physiatry) departments of many major hospitals. They may be offered on an inpatient or outpatient basis and are usually run by a neurologist or physiatrist (an MD who specializes in physical medicine and rehabilitation). Each person with MS has a unique set of symptoms and circumstances that requires a personalized combination of rehab techniques. Evaluation is the first step. In addition to assessing your physical abilities, cognition, and personal goals, your evaluation may also include an assessment of your environment to see if modifications to your home or workplace would be useful. Whether or not you go to an MS center, it is important to be an educated consumer. You should consider the expertise and experience with MS of prospective therapists. The nearest chapter of the National MS Society is an excellent source of referrals. A good source of information on assistive devices for people with disabilities is ABLEDATA. (The National MS Society does not evaluate assistive devices, so we cannot endorse or recommend any of the products listed in their database.) For information, contact: ABLEDATA, 8630 Fenton Street, Suite 930, Silver Spring, MD 20910, 1-800-227-0216. Web site: www.abledata.com.
Who are the specialists and what do they do? Physical Therapists (PTs) work primarily with large motor skills—standing, walking, lifting, or moving about in a wheelchair, for example. Mobility To keep mobile, a person with MS may need both gait (walking) training and training in the effective use of a number of different mobility aids. Professional help from an MD or PT is essential to get good results from an aid. The wrong equipment or incorrect use of the right equipment are both potentially harmful! Since walking requires balance, coordination, upper body control, strength, and endurance, rehab for walking requires evaluation of all of these areas. MS symptoms that affect walking include weakness, tremor, visual disturbances, sensory changes, spasticity, or problems with balance and coordination. Physical therapy, medications, walking aids, and/or appropriate footwear may be needed. You may also need to adapt your home, workplace, or habits to maximize your mobility and safety. Mobility aids keep people mobile, but accepting this concept can be difficult. Many people see aids as symbols of disability and as a sign of “giving in” to the disease. They are afraid that using an aid will lead to greater weakness, and so they refrain from using devices that actually enhance independence and prevent fatigue. It may help a bit to look on mobility devices as tools. A carpenter can’t work without proper tools, and some people with MS can’t move about easily on their own without the proper tools. The tools for mobility are now lighter, easier to handle, more attractive, and more comfortable than ever. A PT can determine which mobility tools are appropriate to your needs and teach you the skills you need to use them well. The mobility “tool chest” includes: ∫ Orthotics (lightweight shoe inserts) to position a spastic foot properly or to brace the foot and compensate for foot drop (a symptom that causes the toe of your shoe to scrape the
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 38

ground when you walk and may cause you to trip or fall). Wearing orthotics decreases fatigue and increases stability. Ankle-foot orthoses or AFOs to compensate for weakness of the legs. They decrease fatigue and help prevent injury from misuse or overuse of joints. Canes to provide support when balance and/or weakness of the legs are problems. If one leg is weak, the cane is used in the hand opposite the weak leg. Two canes can be used if both legs are weak. Crutches to give greater stability when weakness is more severe and canes cannot do the job. Forearm crutches, called Canadian or Lofstrand crutches, are especially stable and require less muscle strength than canes. Walkers to offer stability when the lower body is weak or balance is impaired. Wheeled walkers in bright colors with baskets, brakes, and pull-down seats are available. Wheelchairs or three-wheel scooters to provide mobility when walking, even with an aid, is fatiguing or impossible. These aids are often used by people who are able to walk but need to conserve their energy. People who use scooters must have trunk control. Balance A PT can provide balance retraining through exercises that emphasize strengthening and flexibility. Balance can be improved through use of visual cues or techniques to reduce upper-extremity tremors. Relaxation training is often used as therapy. Weakness Weakness is addressed through specific exercises and various types of assistive devices. Spasticity Normal movements require a coordinated sequence: As one muscle contracts, an opposing muscle must relax. MS can disrupt this process, resulting in the simultaneous contraction of opposing muscles. This is called spasticity. It may also be described as “increased tone.” The affected body part becomes stiff or difficult to move and tends to feel very tight. Spastic sensations may range from neutral to mildly unpleasant to very painful. In severe cases, spasticity can even cause a limb to become “frozen” in a bent position, requiring immediate medical attention. Spasticity can be managed with the help of a physician and a PT. A combination of medication, exercises, adaptive devices, and relaxation techniques may be prescribed. Exercise programs will likely include stretching and range-of-motion exercises. Exercise in a cool swimming pool is helpful because the buoyancy of the water makes smooth movements easier. Passive exercise (when someone else moves your body) is particularly effective for managing spasticity. Specific positioning can also help to decrease spasticity. Physical fitness Appropriately designed exercise programs are of enormous benefit to people with MS. Exercise helps maintain or even build endurance. After a flare-up of MS symptoms, exercise can help restore function and reenergize a person. A PT, physiatrist, or exercise physiologist can provide the best advice on a good program that includes aerobic and non-aerobic exercises. It is best to seek help from someone familiar with MS.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 39

Pain from awkward positions The medical term is “musculoskeletal dysfunction.” It results from unusual positioning of the body caused by MS symptoms. For example, hip, knee, or low back pain can stem from an odd standing position that a person has developed in an attempt to maintain balance. Fatigue can make this kind of pain even worse. Overuse of certain muscles to compensate for other muscles can also lead to pain. A physician will need to determine whether your pain is caused by nerve damage or by musculoskeletal dysfunction. If the latter has occurred, a PT can devise a program of strengthening and stretching exercises, practice of proper positioning, and compensatory techniques, such as bracing or use of an assistive device, to prevent awkward or excessive use of joints or muscles. Pressure sores Many changes in the body may occur if mobility is severely impaired. A person who is immobile runs the risk of developing pressure sores. These occur when the skin breaks down from constant pressure caused by sitting or lying in one position. This pressure cuts off the blood supply to the underlying skin, fat, and muscle. These sores usually occur over bony prominences such as the tailbone, buttock, heel, shoulder blade, elbow, and possibly the back of the head. Sores may also develop from friction to the skin. This is called shear and may result from sliding across a bed or wheelchair. The skin is much more likely to break down if it is moist or infected. Thus incontinence (not being able to control urine or bowel movements, or both) can add to the problem. The best way to treat a pressure sore is to avoid developing one in the first place. Pressure sores can be prevented in the following ways: Get up or change positions frequently, or have someone assist you to change your position at least every two hours. Keep the skin clean and dry. Check skin for reddened areas or sores during self-care routines. And make sure nutrition and fluid intake is adequate. The treatment of pressure sores becomes more difficult as the sore advances. It is imperative to see your physician if you suspect that a pressure sore has begun. Occupational Therapists (OTs) focus on skills that require upper-body strength, coordination, and fine motor control. These include all the “occupations” of daily life, such as bathing, toileting, household chores, and working at a job. OTs also focus on cognitive problems, and can assist with cognitive retraining and strategies to compensate for poor memory. Most important, OTs can help with energy conservation. Fatigue Fatigue is one of the most common symptoms of MS, and sometimes the most disabling one. It affects everything you do. Your physician may prescribe medications and regular rest periods. Fatigue is also managed by conserving energy and working efficiently. OTs are the experts on laborsaving and energy-conservation techniques. Ask your physician for a referral if fatigue is disrupting your life. Upper body function An OT can recommend exercises to improve the strength and coordination of your arms and hands. Doing so can improve independence and function in your daily activities.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 40

Driving Driving can be affected by many MS-related disabilities. An OT can assess your driving skills and determine whether the available adaptations will work for you. Testing should be conducted both in the OT’s office and on the road. Bear in mind that the laws regarding what kinds of testing and reporting are necessary vary from state to state. Hand controls for braking and acceleration are available for people who cannot rely on their legs. Steering knobs can help people who have the use of only one arm. And wheelchair lifts can be installed in certain cars and vans for drivers and passengers who use scooters or wheelchairs. Computers and electronic equipment Computers open a world of recreation and job-related activities, but MS symptoms may require special adaptations. For example, people with vision problems can use computers with enlarged keyboards, magnifying displays, or text-to-speech programs that read aloud the material onscreen. Visit www.MyMSMyWay.com for useful information on how you can use accessible technology to live better with MS. Electronic remote controls can be used for virtually all the appliances in an environment—lights, radios, telephones, televisions, air conditioners, even doors. An OT can help you determine which devices are most appropriate, and where you can get any training that’s needed. Daily occupations The “occupations” of occupational therapy include the everyday things you do—caring for yourself and your household, holding a job, recreation. Bathing, toileting, dressing, eating, and household chores may become hard to do in the presence of certain impairments. An OT can advise you about techniques and adaptive devices to compensate for particular disabilities. The table on the next page illustrates some everyday activities. Vocational Rehabilitation Specialists focus on retraining or use of adaptations and accommodations on the job. They may work independently or in consultation with your OT. Psychologists help people learn ways to handle their emotional and cognitive problems and deal with the impact of MS on the family. Sexuality Neurologists, urologists, sex therapists, specialized nurses, and psychologists may all play a role in addressing sexual problems caused by MS. Men may have difficulty achieving or maintaining erections, or reaching orgasm; women may experience impaired sensation, numbness or tingling in the genital area, insufficient lubrication, or difficulty reaching orgasm. MS also affects sexual responses indirectly. Fatigue, pain, bowel or bladder problems, and the emotional impact of having MS can dampen sexual desire. Spasticity may prevent using certain positions. Taking an active approach to sexual problems means that both partners explore adaptations in sexual expression. If you find these conversations difficult, a psychologist can help start this process. Medical treatment to manage symptoms is part of the solution. So is attention to the emotional concerns of both partners. Neuropsychologists specialize in memory, problem solving, and other cognitive problems, and can assess individuals for the most precise diagnosis of these difficulties.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 41
Memory loss and other cognitive difficulties Poor recent memory is the most commonly reported cognitive symptom in MS. Psychologists, speech pathologists, and OTs can recommend teach simple compensatory strategies, such as making lists, writing notes, learning memory tricks, and keeping a “memory” notebook. People with MS can also experience problems with concentration, reasoning, judgment, and the ability to learn. A neuropsychologist may be recommended for evaluation and design of the best therapy. Restructuring daily activities and providing supervision may be needed in rare situations. Even very mild cognitive problems can increase fear, anxiety, and depression—emotions that in themselves are disabling. A psychologist can provide supportive counseling. Speech/Language Therapists (or Speech/Language Pathologists) work with speech when MS makes talking difficult or causes swallowing problems. They can also help with problems in cognitive functioning, memory problems, and using language, which may stem from MS-related injury in the “thinking” part of the brain. If it’s hard to speak or swallow When MS affects parts of the brain that control muscles in the mouth, throat, or voice box, speech and/or swallowing difficulties may result. To improve speech, the therapist may teach breath control techniques or how to speak more slowly with emphasis on key words. Voice amplifiers can help when a person cannot generate volume. If speech is severely impaired, other communication devices are available. Swallowing problems may be helped by exercises, altering mealtime routines to promote relaxation, or by making changes in the diet, or the position of the body while eating. If the words are wrong Common language symptoms involve not being able to find the right word or using an inappropriate substitute word. These problems can be handled with compensatory techniques. Urologists treat urinary infections, bladder problems, and sexual problems. Bladder problems Many people with MS experience bladder problems at one time or another. The most common problems are increased frequency or urgency, leakage, difficulty urinating despite having the urge to do so, and the inability to hold urine in the bladder. Sometimes the bladder does not empty completely, which can set the stage for urinary tract infections. Diagnosis is the first step. Symptoms may then be managed by medications, diet changes, and in some cases self-catheterization, in which a small tube, or catheter, is inserted through the urethra into the bladder so urine can drain out. (This sounds difficult and painful, but most people can learn to do it easily and comfortably.) There are also exercises involving the pelvic floor muscles that may be appropriate. Bowel problems Constipation may occur because of MS-related neurological damage, or lack of exercise, inadequate fluids, or poor diet. The first line of therapy usually involves modifying the diet to include more fruits, vegetables, and whole grains, and six to eight glasses of water each day. If these measures don’t solve the problem, consult your physician or nurse. A gastroenterologist will be needed in difficult situations. Incontinence, or loss of bowel control, is a much less frequent complication and may result from leakage around impacted stool. Stool
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 42

bulkers, a regular “bowel program,” and medication may also be prescribed. A physiatrist may also be very helpful with both bowel and bladder problems. Nurses—First and Last. A nurse can be the linchpin of your rehab program. If your physician is an MS specialist, the chances are so is your nurse. But even if this isn’t the case, nurses are trained to identify health problems, do assessments, and connect people to appropriate specialists. “Patient education” is on their job description and nurses will make time to listen to your questions and teach you self-help techniques.
Reference
Lisa J. Bain is a professional science and medical writer. Randall T. Schapiro, MD, is director of the Schapiro Center for Multiple Sclerosis at the Minneapolis Clinic of Neurology in Minneapolis, MN. This publication is supported by contributions to the National MS Society from its members and friends. Reviewed by members of the Client Education Committee of the National Multiple Sclerosis Society’s Clinical Advisory Board.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 43

10 Energy Conservation Principle Energy conservation consists of tasks that are utilized to minimize energy expenditure in the patient with low or no reserves for maintaining basic life support. Conservation methods can be used with patients who struggle with daily tasks due to a chronic condition such as COPD or CHF. Methods can be used when a patient is unable to breathe within normal limits for that patient, and is using alternative breathing techniques that will further drain reserves and lead to distress or exacerbation.
Purpose Rehabilitation and nursing personnel can assist the patient in performing energy conservation tasks to relieve expenditure of reserves when a patient is working hard to breathe. Assisting the patient to conserve energy will bring control back to the patient, prevent exacerbation, and diminish the need for emergency care.
Procedure
Activity intolerance Decreased tolerance is evident when a patient is unable to complete ADL’s without assistance.
Interventions
1. Assist patients to avoid excessive tiring by combining activities when possible to shorten time involved to complete tasks.
2. Locate needed items for personal grooming within easy reach such as on a bedside table, to avoid standing for long periods of time.
3. Stop activities or exercise that produce excessive shortness of breath or tachycardia.
4. Allow for adequate rest periods between activities. 5. Make use of comfort measures that promote rest, such as massage,
encouraging personal items of comfort, changing locations away from drafts, improving lighting, etc.
6. Teach the patient to rate fatigue level on a scale of 0-10. See Modified 10 Point Borg Scale.
7. Save large tasks for when the patient has a low level of fatigue such as a score of 0-2.
8. Small tasks can be accomplished with monitoring during medium levels of fatigue such as from 3-6.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 44

9. For greater fatigue levels rating 7 or higher, provide rest opportunities and monitor for potential breathing difficulties (see Five-Finger Fly-By Assessment and Exacerbation Interventions).
10. Continually identify priorities and eliminate non-essential activities. Anxiety and irritability Low oxygen levels can cause a patient to become anxious and/or irritable. The change in disposition from calm to irritable increases energy expenditure and can lead to distress.
Interventions
1. Make an effort to reduce anxiety and irritability that can drain reserves. 2. Reduce stressors and respond promptly to patient’s concerns. 3. Accept irritability without provoking further aggressive responses. 4. Provide appropriate encouragement for progress.
Altered Body Positioning while effective for mild or moderate respiratory distress, tripod positions are not encouraged for severe respiratory distress. When the patient has to support the body in an upright position using arm strength, fatigue will occur quickly and the patient will lose valuable energy needed for basic survival.
Interventions Use a High Fowler’s position or dangle at the bedside with arms folded across a bedside table. Use of these positions will decrease the amount of work it takes to stay upright with the chest expanded for better lung efficiency.
Altered secretion clearance the elderly, and those with chronic respiratory conditions, have decreased ability to mobilize secretions. This can lead to infection and can quickly tire a person already struggling to breathe. Interventions Energy conservation methods can be applied to coughing, called stage-controlled coughing, (see Exacerbation Interventions). Teach the patient to use a huff-cough method, by huffing several times with exhalation to promote secretion movement and then one strong cough. (See Exacerbation Interventions and Breathing Retraining procedures for details.)
References Carpenito, L.J., (2002), Handbook of Nursing Diagnosis and Nursing Diagnosis, Application to Clinical Practice, J.B. Lippincott Co. Lewis, S.M., Heitkemper, M.M., Dirksen, S.R., (2004), Medical Surgical Nursing, Mosby Co. Linton, A. D., Matteson, Maebius, N. K., (2000), Nursing Care of Adults, W. B. Saunders Co.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 45

11 Relaxation and Stress Management Principle Relaxation and stress management will help increase the quality of life. Stress can have negative effects on the body, such as decreased energy, hypertension, blood sugar imbalances, and impaired cognitive function. Purpose The purpose of this module is to help educate and incorporate stress and relaxation techniques into our patient’s lives. Procedure The word stress is derived from the Latin work stringer which means to “draw tight.” Long term or prolonged stress is a serious threat to a person’s emotional and physical health. As stress increases or the number of stressors increase a person’s ability to effectively adapt is decreases. Stress can be defined as any type of change that causes physical, emotional or psychological strain. Stress causes the body to release a hormone called cortisol. Prolonged high levels of cortisol can lead to heart disease and other health problems. Cortisol is an important hormone in the body, secreted by the adrenal glands and is involved in the following functions:
• Glucose metabolism • Regulation of blood pressure • Insulin release for blood sugar maintenance • Immune function • Inflammatory response
Cortisol normally is present in the body at higher levels in the morning and at its lowest at night. Although stress isn’t the only reason that cortisol is secreted into the bloodstream, it is termed “the stress hormone” because it’s also secreted in higher levels during the body’s ‘fight or flight’ response to stress. Cortisol is accountable for several stress-related changes in the body. While cortisol is important and a helpful part of the body’s response to stress, it’s important that the body’s relaxation response be activated so the body’s functions can return to homeostasis. Higher and more prolonged levels of cortisol in the bloodstream have been shown to have negative effects, such as:
• Impaired cognitive performance • Suppressed thyroid function • Blood sugar imbalances such as hyperglycemia
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 46

• Decreased bone density • Decrease in muscle tissue • Higher blood pressure
Lowered immunity and inflammatory responses in the body To keep cortisol levels healthy and under control, the body’s relaxation response should be activated after the fight or flight response occurs. You can learn to relax your body with various stress management techniques, and you can encourage lifestyle changes in order to keep the body from reacting to stress in the first place. The following have been found by many to be very helpful in relaxing the body and mind, aiding the body in maintaining healthy cortisol levels:
• Guided Imagery • Self-Hypnosis • Exercise • Yoga • Listening to Music • Breathing Exercises • Meditation • Anti-anxiety Medications
Relaxation is a form of control. Cortisol secretion varies among individuals. Studies have shown that people who secrete higher levels of cortisol in response to stress also tend to eat more food, and food that is higher in carbohydrates than people who secrete less cortisol. If you’re more sensitive to stress, it’s especially important for you to learn stress management techniques and maintain a low-stress lifestyle. References Linton, D. K., Matteson, M. A. & Maebuis, N. K. (2000). Introductory Nursing Care of Adults. (2nd Ed.). W.B. Saunders Company: Philadelphia. Lewis, S. K., Heitkemper, M. M. & Dirkesen, S.R. (2004). Medical Surgical Nursing. Assessment and Management of Clinical Problems.(6th ed.). Mosby, INC. St. Louis. Mountain Land Rehabilitation. (1996). Physical COPD Rehabilitation. Aspen Publishers Inc.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 47

12 General Dietary Guidelines for MS Patients Nutrition Basics for Healthy Living with MS Just as life with MS is a balancing act, so is eating right. The key to nutritional success means making choices that fit your lifestyle. Here are a few tips to start down that road of living well by eating well. 1. Choose your fats wisely. About Unhealthy Saturated Fats Saturated fats have long been associated with a wide range of negative health effects including high blood pressure, heart disease, stroke and some forms of cancer. These fats are usually solid at room temperature and most often come from the animal foods in our diets. Saturated fats can be found in highly-marbled meats, the skin on poultry, rich, creamy cheeses, butter and whole milk dairy products. There are also plant sources high in saturated fats including coconut oil, palm oil and palm kernel oil (often called tropical oils), and cocoa butter. Trans fats act like saturated fats and are typically found in shortening, margarine, cookies, crackers, snack foods, and fried foods. Most trans fats are man-made through a process called hydrogenation—where a liquid oil-like corn oil is made into a more solid form, like margarine or shortening. Understanding the Food Label Information about unhealthy saturated fats has been on food labels since 1993. Until now, the only way to tell if a food contained trans fats was to check the ingredients list for the words “hydrogenated” or “partially hydrogenated.” With the addition of trans fats on the food panel, you not only have information about the total fat found in a product, but the total amount of unhealthy saturated fat and trans fat. Here’s how it works. When comparing like food products, add the grams (g) of saturated fat and trans fat on a food label and choose the lowest in the combined amount. You can find more information on trans fats and the food label by visiting the website of the U.S. Food and Drug Administration at www.cfsan.fda.gov Healthy Unsaturated Fats Unsaturated fats play a very important role in our diet and support many essential functions in the body: ∫ They promote growth and healthy skin. ∫ They help the body make hormone-like substances. ∫ They help in the absorption of vitamins A, D, E & K. ∫ They help regulate blood pressure and the immune system. ∫ They are important components of myelin and the central nervous system. They include both monounsaturated fats—found in olive, canola and peanut oils; avocados, and nuts including almonds, hazelnuts, peanuts, and polyunsaturated fats—found in other vegetable www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited.
48

oils such as safflower, sunflower seed, corn and soybean oils, seeds and nuts including walnuts and brazil nuts. When these fats replace saturated fats in the diet, they can help to lower blood cholesterol and the risk of heart disease. There is some evidence that certain types of polyunsaturated fats in the diet—specifically omega-3 fatty acids and omega-6 fatty acids—could actually have a beneficial effect on MS. While the research is limited, there have been a few studies that demonstrated that a low-fat diet rich in these types of fatty acids might decrease severity and duration of MS attacks. Some of the best sources of omega-3 fats can be found in fatty fish like mackerel, herring, sardines, albacore tuna and salmon. These fish contain two omega-3 fatty acids—EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid). The American Medical Association suggests that the benefits of eating fish outweigh the risk of mercury when consumed according to FDA recommendations. Children and pregnant women are recommended to avoid high-risk fi sh. See website resources at the end of the booklet for further information. Plant sources (soybeans, canola oil, walnuts and flaxseeds) contain ALA (alpha-linolenic acid), a less potent form of omega-3. Good sources of omega-6 fatty acids are the oils of seeds and nuts, such as safflower oil, sunflower oil, and sesame seed oil. Fitting in Fat While fat is an important part of a healthy diet, moderation is key. Leading health agencies recommend that less than 30% of your total daily calories come from fat and that unhealthy saturated & trans fats be limited (less than 7% of total calories) and replaced with healthier unsaturated fats. Here are some ideas to help bring these strategies to life in your diet: ∫ Keep your protein choices lean— lean meats and poultry without skin and prepare them without added saturated and trans fat. ∫ Choose low fat, 1% or nonfat dairy—including milk and yogurt. Cheeses and frozen desserts should have less than 3 grams of fat per serving. ∫ Include omega-3 rich seafood—two to three 3 oz. servings/week. ∫ Experiment with more beans, peas & lentils—a great source of protein without the saturated fat. ∫ Substitute packaged snack foods with nuts or seeds—to cut the trans fats and increase healthy omega-3 and omega-6 fats. ∫ Use fats and oils sparingly—choose liquid vegetable oils like safflower or sunflower and liquid or tub margarines that are low in saturated and trans fats. 2. Include 5 servings of antioxidant-rich fruits and vegetables. Color may be your best clue to spotting foods that are rich in antioxidants—a substance that may protect the cells in our body from the damage caused by free radicals. The damage caused by free radicals may contribute to a host of health issues like aging, cancer, and heart disease—and preliminary evidence suggests that it may be involved in the disease process in MS. Antioxidants and MS A few studies using an animal model of MS suggest that There is an important theoretical risk to consider. Antioxidant vitamins (e.g., Vitamin C, Vitamin E and beta-carotene) stimulate the immune system. In MS, where an overactive immune system appears to be part of the disease process, stimulation may be dangerous.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 49

Look for the Colors of the Rainbow When it comes to antioxidants, food sources appear to be preferred to supplements (foods rich in Vitamin C, Vitamin E and beta-carotene). An added benefit is that foods are packed with other complementary nutrients that help you absorb them in the right form and right amount. Let the color be your guide—red, yellow, orange, blue and green fruits and vegetables are your best choices for these antioxidants. Fill your plate with the colors of the rainbow and include 4–6 servings in your diet each day. 3. Aim for Fitness. Make a healthy weight your target. There are many reasons why a person with MS may gain or lose weight, but controlling weight is the same story for everyone. Watch the calories and do regular physical activity. Calories are a measure of the energy locked inside the carbohydrates, fats, and proteins found in foods. This energy fuels our body, but what we don’t use gets stored as fat, and over time results in extra weight. Physical activity and good nutrition are perfect partners in managing weight. Not only does physical activity burn calories, it can help you: antioxidants may even be therapeutic. There are no well documented published studies of people with MS that show a clinical benefit related to antioxidant supplements, and the safety of taking antioxidants for people with MS has not been established. ∫ Make the most of your potential muscle strength, or even build strength, depending on your program. ∫ Increase your endurance. ∫ Maximize range of motion and joint flexibility. ∫ Strengthen your heart. ∫ Decrease feelings of fatigue. (Really. Even with MS.) ∫ Decrease symptoms of depression. ∫ Maintain regular bowel and bladder functions. ∫ Minimize the risk of skin breakdown and irritation. ∫ Protect your weight-bearing bone mass. ∫ Improve cognition. 4. Be aware of the impact of different symptoms. Since the course of MS is often unpredictable, focusing on those aspects of health you can control becomes even more meaningful. Working to improve your diet to maximize the positive effects it can have on MS symptoms is one area where you’re in charge!
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 50

13 Quick Conversion Chart (MET)
Speed, Distance, Energy Conversion Chart. MPH Ft Per Min 6MWT / Ft (MET) kcal / min Notes:
0.1 8.8 52.8 1.07 5.35
0.2 17.6 105.6 1.15 5.75
0.3 26.4 158.4 1.22 6.1
0.4 35.2 211.2 1.3 6.5
0.5 44 264 1.38 6.9
0.6 52.8 316.8 1.45 7.25
0.7 61.6 369.6 1.53 7.65
0.8 70.4 422.4 1.61 8.05
0.9 79.2 475.2 1.68 8.4
1 88 528 1.76 8.8
1.1 96.8 580.8 1.84 9.2
1.2 105.6 633.6 1.91 9.55
1.3 114.4 686.4 1.99 9.95
1.4 123.2 739.2 2.07 10.35
1.5 132 792 2.14 10.7
1.6 140.8 844.8 2.22 11.1
1.7 149.6 897.6 2.3 11.5
1.8 158.4 950.4 2.37 11.85
1.9 167.2 1003.2 2.45 12.25
2 176 1056 2.52 12.6
2.1 184.8 1108.8 2.6 13
2.2 193.6 1161.6 2.68 13.4
2.3 202.4 1214.4 2.76 13.8
2.4 211.2 1267.2 2.83 14.15
2.5 220 1320 2.91 14.55
2.6 228.8 1372.8 2.99 14.95
2.7 237.6 1425.6 3.06 15.3
2.8 246.4 1478.4 3.14 15.7
2.9 255.2 1531.2 3.22 16.1
3 264 1584 3.29 16.45
MPH Ft Per Min 6MWT / Ft (MET) kcal / min References:
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett DR Jr, Schmitz KH, Emplaincourt PO, Jacobs DR Jr, Leon AS. Compendium of Physical Activities: An update of activity codes and MET intensities. Medicine and Science in Sports and Exercise, 2000;32 (Suppl):S498-S516. http://prevention.sph.sc.edu/tools/docs/documents_compendium.pdf
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 51

Exercise Prescription and Progression
Principle In patients with MS, disability is primarily a result of progressive deconditioning. As the disease progresses, limited capacity makes exertion unpleasant and leads to an increasingly sedentary lifestyle. Exercise intolerance are the most incapacitating symptoms patients develop. A counter-measure to progressive functional decline in patients with MS is exercise training. Purpose It has clearly been demonstrated that exercise is beneficial for patients who have MS. Structured exercise protocols and less demanding protocols alike produced significant improvement in exercise tolerance, and decreased dyspnea. Although exercise may not lengthen life expectancy, it has been shown to improve the quality of life and therefore should be an integral treatment for all MS patients. Components of an exercise prescription An exercise prescription generally includes the following specific recommendations:
• Type of exercise or activity (i.e. strength training, walking, cycling, swimming, chopping wood, fishing, showering, cleaning house)
• Specific workloads (i.e. MPH, MET, FPM-walking speed, Kcal/min, ) • Duration-(variable) and frequency-(fixed:3 X Wk) of the activity or exercise session • Intensity guidelines – Target heart rate (THR) range and estimated rate of (RPE),
(SOBr), (Fatigue). Precautions or contraindications regarding oxygen saturation such as: Keep oxygen saturation > 88% Sp02 at all times during the therapeutic exercise session or an orthopedic, cardiac or co-morbidity concern. The 6 Minute Walk Test (6MWT) is used to establish the exercise prescription of the patient in both the in & out patient setting. Many MS patients will not likely complete the full (6MWT). However, the information collected from the test is valuable. Special attention should be paid to Oxygen Saturation (%Sp02), Ratings of Perceived Exertion (RPE), Dyspnea (SOBr), Heart Rate (HR), when identifying exercise intensity. Subjective V. Objective Measurements. Subjective measurements are (RPE), (SOBr) (Fatigue) Objective measurements are (HR), (%Sp02), (Distance) (MPH). Low stress threshold V. High stress threshold. Low stress threshold is categorized by high subjective ratings with low objective measurements. High stress threshold is categorized by low subjective ratings with high objective measurements. If the Heart Rate remains low 80 to 100 and RPR-FT/SOBr are high between 6 and 7, one may conclude that the patient has a lower stress threshold or deconditioned functional capacity and is appropriate to start at a lower intensity level of RPR/SOBr of 2 to 3. Conversely, if the patient achieves a Heart Rate of 100 to 120 and reports an RPE-FT/SOBr of
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 52

3 to 4, this patient has a higher stress threshold and is appropriate to start at a moderate intensity level of RPE-FT/SOBr of 3 to 4. Procedure Sure and safe progression is consistently achieved in the MS diseased population with incremental increases in prescriptive exercise intensity, type, and duration. Start Low and Go Slow
Moderate Intensity Low Intensity
Exercise to promote functional independence Activity to maintain function or prevent deconditioning
Accumulate 30 minutes three to five days per week. RPE 4-6 on 10 point scale.
Accumulate 10 minutes of activity that is well-tolerated three times a week and gradually increase exercise time and intensity, RPE 2-4 on 10 point scale.
Gathering information from the 6MWT The amount of time completed on the 6 Minute Walk Test (6MWT) sets the starting point for exercise duration for the first session and to progress through interval training onto continuous exercise with multiple types of exercise equipment as an exercise progression methodology. The patient completed 3 minutes on the (6MWT), this patient starts with an exercise duration of 3 minutes the first session, then as soon as the patient can tolerate it, work to perform 3 minutes of low intensity work, with a 3 minute rest period followed by 3 more minutes of exercise, this is “interval training” and is a standard starting method for patients with low functional levels. Below is an example of incremental exercise progression. Each patient will progress differently depending on type, stage and grade of disease or exacerbation; therefore, therapist must individualize prescriptive exercise based on the individual’s adaptability, resiliency, tolerance, knowledge, skills, abilities, and eagerness to perform therapeutic exercise.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 53

Incremental Increase in Aerobic Exercise & Strength Training Session WORK REST INTERVAL WORK 50-70% - 1RM
Session 1 3 MIN Tread Mill 1 x 8 Session 2 3 MIN 3:00 3 MIN 1 x 8 Session 3 3 MIN 2:30 3 MIN 1 x 8 Session 4 3 MIN 2:00 3 MIN 1 x 10 Session 5 3 MIN 1:30 3 MIN 1 x 10 Session 6 3 MIN 1:00 3 MIN 1 x 10 Session 7 3 MIN 0:30 3 MIN 1 X 12 Session 8 6 MIN End of Rest Inter 0:00 0 MIN 1 X 12 Session 9 7 MIN Tread Mill 1 X 12 Session 10 8 MIN Tread Mill 2 x 8 Session 11 6 MIN ADD: CE, NS, UBE 3 MIN 2 x 8 Session 12 6 MIN CE or NS or UBE 4 MIN 2 x 8 Session 13 7 MIN CE or NS or UBE 4 MIN 2 x 10 Session 14 7 MIN CE or NS or UBE 5 MIN 2 x 10 Session 15 7 MIN CE or NS or UBE 6 MIN 2 x 10 Session 16 7 MIN CE or NS or UBE 7 MIN 2 X 12 Session 17 8 MIN CE or NS or UBE 7 MIN 2 X 12 Session 18 8 MIN CE or NS or UBE 8 MIN 2 X 12 Session 19 9 MIN CE or NS or UBE 8 MIN 3 X 8 Session 20 9 MIN CE or NS or UBE 9 MIN 3 X 8 Session 21 10 MIN CE or NS or UBE 9 MIN 3 X 10 Session 22 10 MIN CE or NS or UBE 10 MIN 3 X 10 Session 23 11 MIN CE or NS or UBE 10 MIN 3 X 12 Session 24 11 MIN CE or NS or UBE 11 MIN 3 X 12 Legend:
CE: Cycle Ergometer NS: NuStep
UBE: Upper Body Ergometer
Work-Rest Ratio The Work-Rest-Ratio (WRR) as a method of interval training serves best at the beginning of the low level patients program and should follow the One-to-One (1:1) (WRR) rule, i.e., Work 3 minutes: Rest 3 minutes: Work 3 minutes. The Work-Rest-Ratio-Interval (WRRI) should decrease in 30 second increments from threptic session to therapeutic session or as the patient tolerates without fatigue hangovers. Once the (WRRI) has been closed, the therapist may add one (1) minute of exercise duration per exercise session or as the patient tolerates without fatigue hangovers. (Causing a “Fatigue Hangover” is a cardinal sin) The optimal aerobic activity segment should seek to reach the following “Best Case Scenario”.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 54

GOAL: Best Case Scenario; 15 minutes walking/treadmill, 15 minutes cycling, with 20 minutes of upper and lower extremity strength training exercises. Prescribing exercise in the chronic diseased population requires a significant amount of planning and encouragement. The exercise prescription should proceed gradually since most individuals are extremely limited in the amount of exercise tolerated secondary to deconditioning, dyspnea, exertional distress or hypersensitivity to exertion. References United States Army Center for Health Promotion and Preventive Medicine 5158 Blackhawk Road. Aberdeen Proving Ground, Maryland 21010-5403 MAJ Robert L. Gauer, MD, FACSM LTC Francis G. O.Connor, MD, FACSM F. Edward Hébert School of Medicine Uniformed Services University of the Health Sciences Department of Family, Sports and Preventative Medicine 4301 Jones Bridge Road Bethesda, Maryland 20814 COL Willis B. Campbell, MD, Ph.D., MPH, FACSM Larry W. Laughlin, M.D., Ph.D. FCCP
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 55

General Aerobic Exercise Recommendations Parameter Recommendation and Comment Mode
Most exercises involving large muscle groups are appropriate, but walking, cycling, and NuStep, are especially recommended. The key is to modify exercise mode based on acute or chronic treatment effects of pulmonary exacerbations.
Frequency At least 3 times/wk, but daily exercise may be preferable for severely deconditioned inpatients performing lighter-intensity and shorter-duration exercises.
Intensity Moderate intensity, depending on patient's current fitness level and severity of side effects from treatments. Guidelines include 50%-75% VO2max or HRreserve, 60%-70% HRmax, or an RPE of 4-6. HRreserve is the best guideline if HRmax is estimated rather than measured.*
Duration At least 20-30 min of continuous activity, but this goal may require multiple intermittent shorter bouts (eg, 5-10 min) with rest intervals in deconditioned patients or those experiencing severe side effects of treatment.
Progression Initial progression should be in frequency and duration. Only when these goals are met should intensity be increased. Progression should be slower and more gradual for deconditioned patients.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 56

14 Individual Therapeutic Session
Principle Each therapeutic session is an opportunity to provide exercise in a controlled and monitored environment, and education that not only enhances exercise, but also improves all aspects of function. Each session will build on the previous session in both fitness and knowledge. Purpose Exercise sessions should focus on individual needs and aim to progress the patient to a higher level of functioning. Patient goals should be discussed and reviewed at various points throughout the sessions to assist in measuring progress. Documentation during each session also helps both therapists and patients measure success.
Procedure
Subjective Record subjective information that the patient reports, such how they are feeling or sleeping.
Objective Record a productive chough, or sleep disturbance such as waking up to breathe.
Measurements • HR (Heart Rate) • BP (Blood Pressure) • % spO2 • RPE/SOBr/Fatigue
Physiological Changes During Exercise
What do these measurements mean? You expect the heart rate to increase with exertion. You should also see an increase in blood pressure with exercise. Oxygen usage will increase, but the % sp O2 should remain above 88% at all times during exercise. Any sudden change in any of the baseline measurements or subjective reporting indicates a need to decrease or even stop the exercise. Monitoring changes will allow you to determine whether to increase or decrease the intensity of the therapeutic session or seek medical attention from the patient’s physician.
Aerobic Exercise There are various modes that can be used for aerobic exercise. Ideally two modes of aerobic exercise will provide variety if the patient can tolerate the
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 57

exercise duration. The treadmill is the most important mode of aerobic training as it easily translates into ADL's and functional independence.
• All aerobic exercise must begin with a 3 min warm up and conclude with a 3 min cool down at minimal loads.
• Aerobic training requires only one warm up and one cool down. Transitioning between equipment is exempt from WU & CD workloads.
• COPD patients often have balance and falls-risk issues so they must be monitored for safety while on exercise equipment. As a rule, most COPD patients will require balance and gait training to counter the lean tissue waisting that occurs from chronic corticoid steroid use.
Resistance Exercise Resistance exercise is patient dependent; therefore, adjusting intensity, and volume should be considered based on patient needs, ability, and history.
• Resistance exercise is very important for LE & UE as it translates into ADL's.
• Resistance exercise is an emerging research focus for COPD patients as it’s revealing functional outcomes equivalent to aerobic exercise training.
• Resistance exercise progression is outlined in the following guidelines: o Sets & Reps:
1x8, 1x10, 1x12, 2x8, 2x10, 2x12, 3x8, 3x10, 3x12.
• ROM exercise may be “medically necessary”, thus, ROM therapy should be carefully attended to.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 58

Patient Education Exercise sessions will include education associated with your condition. Successive education will build on previous education. You will be asked to read about the benefits of exercise and proper exercise, and you will be given tips for making everyday tasks easier.
• 8 sessions should be taught and documented. • Patient education is a partnership, ask the patient to pre-read, and then
cover the section & answer questions once a week in a 15-minute lesson session.
Follow-up Complete SOAP notes and documentation.
Assessment
Document how the patient tolerated the exercise session using intensity, duration, frequency, and mode (IDFM).
Plan Document goals and/or changes for the next session using IDFM.
Measurements
Allow the patient to cool down, and then collect final measurements and compare to baseline measurements. The resting heart rate should be within 8 beats of the baseline.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 59

SOAP NOTES
Session # Patient Name: Date:
Subjective: Patient feels (check one) О Good О Fair О Poor
Objective:
Resting Measurements Aerobic Exercise
Start Tx End Tx Requirement Type Duration Int HR BP %
spO2 FiO2
HR HR <100 to DC Warm up (3 Min)
BP BP <200/110
%spO2 %spO2 >88%
FiO2 FiO2 Keep % spO2 >88
Education: Notes:
Cool Down (3 Min) RPE/DYSP/Fatigue (1-10)
Strength Training Sets (1-3) Reps (8-12) Load (lbs)
Leg Press Chest Press Overhead Press Pull Downs Rowing
Assessment:
Planning:
Therapist
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 60

15 Functional Capacity: Writing Functional Goals Purpose Physical and Occupational Therapists are required to document patient outcomes on the Department of Health and Human Services Plan of Treatment, 700 & 701, etc. Human physiological outcomes at rest and during activity are well known, translating measurements (MET) allows therapists to apply scientific principles to the assessment of everyday functional capacity. The validity of metabolic equivalents (MET) and it’s relationship to functional capacity or physical activity is central to the Compendium of Physical Activities Tracking Guide. The compendium was developed for use in epidemiologic studies to standardize the assignment of MET intensities in physical activity. The compendium has been used in studies worldwide to assign intensity units MET to physical activity, and to develop innovative ways to assess energy expenditure in physical activity.
Procedure Knowing where to find MET provides the therapist with validated information for this MET to functional capacity translation method.
Most aerobic exercise equipment includes an instrument panel for test, measurement and control. This panel will be the source of MET or Kcal measurement during therapeutic exercise. Take the time to locate the MET/Kcal read out display. The conversion method consists of taking the MET data from the instrument panel just before ending steady state exercise. Use the MET value and compare it to the physical activity tracking guide to reveal equivalent “every day” functional tasks or Activities of Daily Living (ADL). www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited.
61
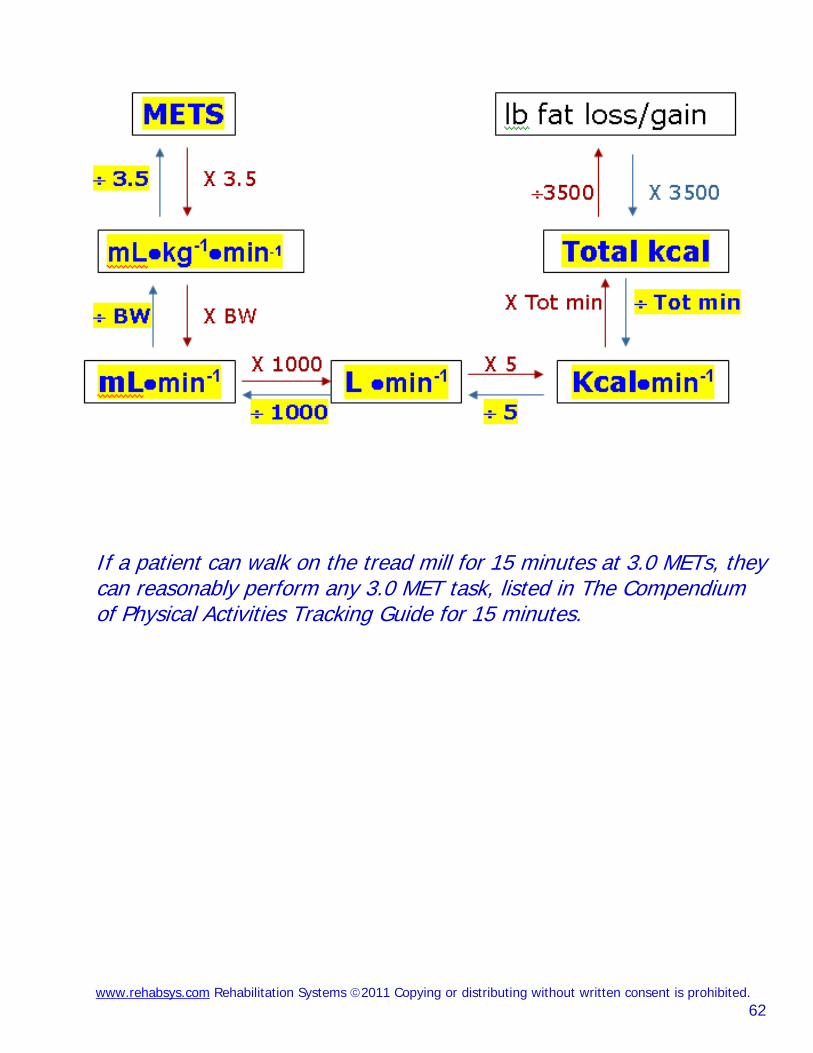
If a patient can walk on the tread mill for 15 minutes at 3.0 METs, they can reasonably perform any 3.0 MET task, listed in The Compendium of Physical Activities Tracking Guide for 15 minutes.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 62

www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 63

The Compendium of Physical Activities Tracking Guide
MET LEVEL / CATEGORY / FUNCTIONAL TASK EQUIVALENT 1 to 2 MET LEVEL 0.9; inactivity; quiet sleeping 1.5; home activities; reclining with baby 1.0; inactivity; lying quietly, watching television 1.0; inactivity; lying quietly, doing nothing, lying in bed awake 1.0; inactivity; sitting quietly and watching television 1.0; inactivity; sitting quietly, sitting smoking, listening to music 1.2; inactivity; standing quietly (standing in a line) 1.0; inactivity; reclining in a chair - talking or talking on phone 1.0; inactivity; reclining in a chair – reading 1.0; inactivity; meditating 1.5; lawn and garden; watering lawn or garden, standing or walking 1.5; miscellaneous; sitting - card playing, playing board games 1.8; miscellaneous; sitting - writing, desk work, typing 1.8; miscellaneous; standing - talking or talking on the phone 1.5; miscellaneous; sitting - talking or talking on the phone 1.8; miscellaneous; sitting - studying, general, including reading - writing 1.8; miscellaneous; sitting - class, note-taking or class discussion 1.8; miscellaneous; standing – reading new paper waiting for bus 1.5; miscellaneous; sitting - arts and crafts, light effort 1.8; miscellaneous; standing - arts and crafts, light effort 1.5; miscellaneous; family reunion, genealogy, sitting, talking, eating 1.8; music playing; accordion 1.5; occupation; farming, milking by machine, light effort 1.3; occupation; police, riding in a squad car (sitting) 1.5; occupation; sitting - light office work, general 1.5; occupation; sitting meetings, general, and/or with talking involved 1.5; occupation; typing, electric, manual or computer 1.0; self care; sitting on toilet 1.5; self care; bathing (sitting) 1.5; self care; eating (sitting) 1.0; self care; taking medication, sitting or standing
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 64

MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 1.0; self care; having hair or nails done by someone else, sitting 1.5; sexual activity; active, vigorous effort 1.3; sexual activity; general, moderate effort 1.0; sexual activity; passive, light effort, kissing, hugging 1.0; transportation; riding in a car or truck 1.0; transportation; riding in a bus 1.0; religious activities; sitting in church, attending a ceremony 1.5; religious activities; sitting in church, talking or singing 1.3; religious activities; sitting, reading religious materials at home 1.2; religious activities; standing in church (quietly), standing quietly 1.0; religious activities; kneeling in church/at home (praying) 1.8; religious activities; standing, talking in church 1.5; religious activities; eating at church 1.5; religious activities; typing, electric, manual, or computer 1.5; volunteer activities; sitting - meeting, general 1.5; volunteer activities; sitting - light office work, in general 1.5; volunteer activities; typing, electric, manual, or computer 2 to 3 MET LEVEL
2.5; conditioning exercise; stretching, hatha yoga 2.5; conditioning exercise; mild stretching 2.5; fishing and hunting; fishing from boat, sitting 2.0; fishing and hunting; fishing, ice, sitting 2.5; fishing and hunting; hunting, bow and arrow or crossbow 2.5; fishing and hunting; hunting, duck, wading 2.5; fishing and hunting; pistol shooting or trap shooting, standing 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen, taking out trash 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; non-food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 65

2.5; home activities; building a fire inside 2.0; home activities; standing - light (pump gas, change light bulb, etc.) 2.5; home activities; sitting-playing with children–light, only active periods 2.8; home activities; standing - playing with children – light, active periods 2.5; home activities; child care: sitting/kneeling - dressing, bathing 2.5; home activities; sit, playing with animals, light, only active periods 2.8; home activities; stand, playing with animals, light, only active periods 2.8; home activities; walk/run, playing w/animals, light, only active periods 2.5; lawn and garden; mowing lawn, riding mower 2.5; lawn and garden; walking, applying fertilizer or seeding a lawn 2.3; miscellaneous; standing - drawing (writing), casino gambling 2.0; miscellaneous; standing, with movement – miscellaneous 2.0; miscellaneous; sitting - arts and crafts, moderate effort 2.0; miscellaneous; touring/traveling/vacation involving walking and riding 2.5; miscellaneous; camping involving standing, walking, sitting 2.0; music playing; cello 2.5; music playing; conducting 2.0; music playing; flute (sitting) 2.0; music playing; horn 2.5; music playing; piano or organ 2.5; music playing; trumpet 2.5; music playing; violin 2.0; music playing; woodwind 2.0; music playing; guitar, classical, folk (sitting) 2.5; occupation; bakery, light effort 2.3; occupation; bookbinding 2.0; occupation; directing traffic (standing) MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 2.5; occupation; chambermaid, making bed (nursing) 2.5; occupation; custodial work - cleaning sink and toilet, light effort 2.5; occupation; custodial work - dusting, light effort 2.5; occupation; custodial work - vacuuming, light effort 2.0; occupation; farming, moving animals, driving, light effort 2.5; occupation; farming, driving harvester, cutting hay, open irrigation 2.5; occupation; farming, driving tractor 2.6; occupation; horse racing, walking speed 2.3; occupation; printing (standing) 2.5; occupation; police, directing traffic, shouting commands (standing) 2.0; occupation; police, driving a squad car (sitting) 2.5; occupation; shoe repair, general 2.5; occupation; sitting; moderate (riding mower/forklift, crane operation) 2.5; occupation; tailoring, cutting 2.5; occupation; tailoring, general 2.0; occupation; tailoring, hand sewing 2.5; occupation; tailoring, machine sewing 2.0; occupation; walking on job, less than 2.0 mph, very slow
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 66

2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; sports; billiards 2.5; sports; croquet 2.5; sports; darts, wall or lawn 2.5; sports; football or baseball, playing catch 2.5; sports; horseback riding, walking 2.0; transportation; automobile or light truck (not a semi) driving 2.0; transportation; flying airplane 2.5; transportation; motor scooter, motorcycle 2.5; walking; bird watching 2.5; walking; pushing or pulling stroller with child or walking with children 2.0; walking; household walking from room to room MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 2.0; walking; walking, less than 2.0 mph, level ground, strolling, very slow 2.5; walking; walking, 2.0 mph, level, slow pace, firm surface 2.5; walking; walking from house to car or bus, from car or bus to go places 2.5; walking; walking to neighbor’s house to socialize, visit, or teach 2.8; walking; walking, 2.5 mph, downhill 2.5; water activities; boating, power 2.5; religious activities; sitting, playing an instrument at church 2.0; religious activities; standing, singing in church, active participation 2.0; religious activities; walk/stand to usher for religious purposes 2.5; religious activities; serving food at church 2.0; religious activities; preparing food at church 2.3; religious activities; washing dishes/cleaning kitchen at church 2.5; religious activities; standing - moderate (lifting 50 lbs) 2.5; volunteer activities; sitting - moderate work 2.3; volunteer activities; standing - light work (filing, talking, assembling) 3 to 4 MET LEVEL 3.0; conditioning exercise; bicycling, stationary, 50 watts, very light effort 3.5; conditioning exercise; calisthenics, home exercise, general 3.5; conditioning exercise; rowing, stationary, 50 watts, light effort 3.0; conditioning exercise; weight lifting 3.0; dancing; ballroom, slow (e.g. waltz, foxtrot, slow dancing) 3.0; fishing and hunting; fishing, general 3.5; fishing and hunting; fishing from river bank, standing 3.3; home activities; carpet sweeping, sweeping floors 3.0; home activities; cleaning, wash car, wash windows, clean garage 3.5; home activities; mopping
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 67

3.0; home activities; cleaning, house or cabin, genera 3.5; home activities; vacuuming 3.0; home activities; cooking Indian bread on an outside stove 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing - packing/unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 3.0; home activities; carrying small children 3.0; home activities; child care: standing - dressing, bathing, grooming 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; home repair; wiring, plumbing 3.0; lawn and garden; riding snow blower 3.5; lawn and garden; trimming shrubs or trees, power cutter 3.0; lawn and garden; picking fruit off trees, picking fruits/vegetables 3.0; lawn and garden; walking/standing - picking up yard, light 3.0; lawn and garden; walking, gathering gardening tools 3.0; miscellaneous; standing - arts and crafts, moderate effort 3.5; miscellaneous; standing - arts and crafts, vigorous effort 3.5; music playing; trombone 3.0; music playing; guitar, rock and roll band (standing) 3.5; music playing; marching band, drum major (walking) 3.5; occupation; carpentry, general 3.0; occupation; custodial work - buffing the floor with electric buffer 3.5; occupation; custodial work - general cleaning, moderate effort 3.5; occupation; custodial work - mopping, moderate effort 3.0; occupation; custodial work - take out trash, moderate effort 3.0; occupation; custodial work - vacuuming, moderate effort 3.5; occupation; electrical work, plumbing work 3.5; occupation; farming, chasing cattle, non-strenuous (walking) 3.0; occupation; farming, milking by hand, moderate effort 3.5; occupation; locksmith 3.0; occupation; machine tooling, welding 3.0; occupation; standing; light/moderate, assemble/repair heavy parts 3.5; occupation; standing; moderate, assembling at fast rate, lifting 50 lbs 3.5; occupation; tailoring, weaving 3.3; occupation; walking on job, 3.0 mph, in office, moderate speed 3.8; occupation; walking on job, 3.5 mph, in office, brisk speed 3.0; occupation; walking, 2.5 mph, slowly and carrying 25 pounds MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 68

3.0; occupation; walking, gathering things at work, ready to leave 3.0; occupation; working in scene shop, theater actor, backstage employee 3.5; sports; archery (non-hunting) 3.0; sports; frisbee playing, general 3.0; sports; golf, miniature, driving range 3.5; sports; golf, using power cart 3.5; sports; horseback riding, saddling horse 3.0; sports; horseshoe pitching, quoits 3.0; sports; shuffleboard, lawn bowling 3.5; sports; trampoline 3.0; sports; volleyball, non-competitive 3.0; transportation; driving heavy truck, tractor, bus 3.5; walking; carrying infant or 15 pound load 3.0; walking; loading /unloading a car 3.0; walking; downstairs 3.0; walking; loading /unloading a car 3.0; walking; walking, 2.5 mph, firm surface 3.3; walking; walking, 3.0 mph, level, moderate pace, 3.8; walking; walking, 3.5 mph, level, brisk, firm surface 3.0; water activities; sailing, boat sailing, windsurfing, ice sailing, general 3.0; water activities; surfing, body or board 3.0; water activities; water volleyball 3.5; winter activities; snowmobiling 3.3; religious activities; walking, 3.0 mph, moderate speed 3.8; religious activities; walking, 3.5 mph, not carrying anything 3.0; religious activities; cleaning church 4 to 5 MET LEVEL 4.0; bicycling; bicycling, <10 mph, leisure, to work or for pleasure 4.8; dancing; ballet or modern, twist, jazz, tap, jitterbug 4.5; dancing; general 4.5; dancing; ballroom, fast (disco, folk, square), line dancing 4.0; fishing and hunting; digging worms, with shovel 4.0; fishing and hunting; fishing from river bank and walking
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 69

MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 4.0; home activities; multiple household tasks all at once, vigorous effort 4.0; home activities; sweeping garage, sidewalk or outside of house 4.0; home activities; walk/run - playing with children – moderate 4.0; home activities; elder care, disabled adult, only active periods 4.0; home activities; walk/run, playing with animals, moderate 4.0; home repair; automobile body work 4.5; home repair; carpentry, finishing or refinishing cabinets or furniture 4.5; home repair; caulking, except log cabin 4.5; home repair; laying or removing carpet 4.5; home repair; laying tile or linoleum, repairing appliances 4.5; home repair; painting 4.5; home repair; sanding floors with a power sander 4.5; home repair; scraping and painting 4.5; home repair; washing fence, painting fence 4.5; lawn and garden; mowing lawn, power mower 4.5; lawn and garden; operating snow blower, walking 4.5; lawn and garden; planting seedlings, shrubs 4.5; lawn and garden; planting trees 4.3; lawn and garden; raking lawn 4.0; lawn and garden; raking roof with snow rake 4.0; lawn and garden; sacking grass, leaves 4.5; lawn and garden; trimming shrubs or trees, manual cutter 4.5; lawn and garden; weeding, cultivating garden 4.0; lawn and garden; gardening, general 4.0; music playing; drums 4.0; music playing; marching band, playing an instrument (walking) 4.0; occupation; bakery, general, moderate effort 4.0; occupation; custodial work – feathering arena floor, moderate effort 4.0; occupation; farming, chasing cattle or other livestock on horseback 4.0; occupation; farming, feeding small animals, milk bottle for calf, goat 4.5; occupation; farming, feeding cattle, horses 4.5; occupation; farming, hauling water for animals, general hauling water 4.5; occupation; forestry, sawing, power 4.0; occupation; forestry, weeding 4.5; occupation; furriery – raise mink for fur coats MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 4.0; occupation; machine tooling, tapping and drilling 4.0; occupation; masseur, masseuse, manual therapy (standing) 4.5; occupation; orange grove work 4.0; occupation; police, making an arrest, taking command (standing) 4.0; occupation; lifting items continuously, 10 – 20 lbs, with limited walking 4.0; occupation; tailoring, pressing, starching 4.0; occupation; walking, 3.0 mph, moderately and carrying 25 lbs 4.0; occupation; walking, pushing a wheelchair
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 70

4.5; occupation; walking, 3.5 mph, briskly and carrying 25 pounds 4.5; running; jogging on a mini-tramp 4.5; sports; badminton, social singles and doubles, general 4.5; sports; basketball, shooting baskets 4.0; sports; coaching: football, soccer, basketball, baseball, swimming, etc. 4.0; sports; curling 4.5; sports; golf, general 4.5; sports; golf, walking and carrying clubs 4.3; sports; golf, walking and pulling clubs 4.0; sports; gymnastics, general 4.0; sports; softball, officiating 4.0; sports; table tennis, ping pong 4.0; sports; tai chi 4.0; walking; pushing a wheelchair, non-occupational setting 4.0; water activities; swimming, treading water, moderate effort, general 5 to 6 MET LEVEL 5.5; conditioning exercise; health club exercise, general 5.0; dancing; aerobic, low impact 5.5; dancing; ballroom, dancing fast 5.0; fishing and hunting; hunting, general 5.0; home activities; maple syruping/sugar bushing 5.0; home activities; walk/run-playing with children–vigorous 5.0; home activities; walk/run, playing with animals, vigorous 5.0; home repair; caulking, chinking log cabin 5.0; home repair; cleaning gutters MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 5.0; home repair; hanging storm windows 5.0; home repair; painting the outside of the house 5.0; home repair; spreading dirt with a shovel 5.0; lawn and garden; carrying, loading or stacking wood 5.0; lawn and garden; clearing land, hauling branches 5.0; lawn and garden; digging sandbox 5.0; lawn and garden; digging, spading, filling garden with compost 5.0; lawn and garden; laying sod 5.5; lawn and garden; mowing lawn, general 5.5; lawn and garden; mowing lawn, walk, power mower 5.5; occupation; construction, outside, remodeling 5.5; occupation; farming, shoveling grain 5.0; occupation; forestry, ax chopping, (SLOW) 5.0; occupation; forestry, hoeing 5.0; occupation; walking, carrying objects about 25 to 49 pounds 5.0; sports; cricket (batting, bowling) 5.0; sports; softball or baseball, fast or slow pitch, general 5.0; sports; tennis, doubles
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 71

5.0; walking; using crutches 5.0; walking; walking, 4.0 mph, level, firm surface 5.0; walking; walking, grass track 5.0; water activities; snorkeling 5.5; winter activities; ice skating, moderate effort 5.0; winter activities; skiing, downhill, light effort 6 to 7 MET LEVEL 6.0; bicycling; 10-12 mph 6.0; fishing and hunting; fishing in stream, in waders 6.0; fishing and hunting; hunting, deer, elk, large game 6.0; fishing and hunting; hunting, pheasants or grouse 6.0; home activities; butchering animals 6.0; home activities; moving furniture, household items 6.0; home repair; carpentry, outside house, installing rain gutters 6.0; lawn and garden; chopping wood, splitting logs MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 6.0; lawn and garden; gardening with heavy power tools, tilling a garden 6.0; lawn and garden; mowing lawn, walk, hand mower 6.0; lawn and garden; shoveling snow, by hand 6.0; occupation; coal mining, general 6.0; occupation; farming, care of animals (grooming, brushing, shearing) 6.0; occupation; forestry, planting by hand 6.0; occupation; horse grooming 6.5; occupation; horse racing, trotting 6.5; occupation; truck driving, loading and unloading truck 6.0; occupation; using heavy power tools such jackhammers 6.0; sports; boxing, punching bag 6.0; walking; carrying 16 to 24 lb load, upstairs 6.0; walking; hiking, cross country 6.5; walking; marching, rapidly, military 6.0; walking; walking, 3.5 mph, uphill 6.3; walking; walking, 4.5 mph, level, firm surface 6.0; water activities; swimming, leisurely, not lap swimming, general 7 to 8 MET LEVEL 7.5; home activities; carrying groceries upstairs 7.5; home repair; carpentry, sawing hardwood 7.0; occupation; forestry, sawing by hand 7.0; occupation; masonry, concrete 7.0; running; jogging, general 7.0; sports; basketball, officiating 7.0; sports; racquetball, casual, general 7.0; sports; tennis, general
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 72

7.0; walking; backpacking 8 to 9 MET LEVEL 8.0; walking; up stairs 8.0; bicycling; bicycling, general 8.0; occupation; carrying heavy loads, such as bricks MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 8.0; occupation; farming, baling hay, cleaning barn, vigorous effort 8.0; occupation; fire fighter, hauling hoses on ground 8.5; occupation; shoveling, digging ditches 8.0; running; running, 5 mph (12 min/mile) 8.0; sports; basketball, game References
1. Barbara Ainsworth, William Haskell, Arthur Leon, David Jacobs, Jr., Henry Montoye, James Sallis & Ralph Paffenbarger, Jr. Compendium of physical activities: classification of energy costs of human physical activities. Medicine and Science in Sports and Exercise 25: 71-80, 1993.
2. Wasserman K, Hansen JE, Sue DY, Whipp BJ, Casaburi R. Principles of exercise testing and interpretation, 3rd ed. Baltimore: Lippincott Williams & Wilkins; 1999.
3. Wasserman K. Cardiopulmonary exercise testing and cardiovascular health. Armonk, NY: Futura; 2002.
4. Principles of Exercise Testing and Interpretation; Including Pathophysiology. Karlman Wasserman, James E. Hansen, Darryl Y. Sue, Brian J. Whipp, William W. Stringer, M.D. - 2005 - 585 pages.
5. 5. Sue DY. Integrative cardiopulmonary testing: basis and application. Medicine, Exercise, Nutrition and Health 1994;3:32-35.
6. Whipp BJ, Davis JA, Torres F, et al. A test to determine parameters of aerobic function during exercise. J Appl Physiol: Resp Environ Exerc Physiol 1981;50:217-221
7. Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 1986;60:2020-2027
8. Cohen-Solal A. Cardiopulmonary exercise testing in chronic heart failure. In: Wasserman K, ed. Exercise gas exchange in heart disease. Armonk, NY: Futura Publishing Co, 1996:17-35.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited.
73

DATE: October 14, 2009. TO: J. Doe M.D. RE: John Doe
Rehabilitation Discharge Summary OVERALL PROGRESS: POOR FAIR GOOD EXCELLENT Compliance: Good. We worked with Mr Doe for Home Bases MS Rehabilitation three times a week and he became a participant in improving his health. Six minute walk test: Pt able to make improvements with 6 min walk test improving from 350 ft and terminating test at 2 min 37 sec to 740 ft and completing test. Pt required no supplemental oxygen and was able to maintain %SPO2 at 97 and above. Patient Education: Pt received education on medications and equipment for self-care, physical fitness, work – rest ratios, stress management, relaxation, nutrition. Home Exercise Program: Pt needs further instructions and pictures to understand his home exercise program. Pt instructed to walk 3-5 times per week Additional Comments: Pt took encouragement during treatment to push himself. Pt motivation was at first poor, but really took off after session 9 which resulted in good overall progress. Thank you for this referral, John Doe
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 74

www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited.
75

About the Instructor
Roger Campbell, M.S., CET, MFT-c. Patient Care Coordinator
Applegate HomeCare & Hospice www.rehabsys.com/about-us
Mr. Campbell started his exercise science career in 1985 as an Army Master Fitness Trainer, where he physically prepared troops for combat deployments. With the GI Bill, Campbell obtained his Bachelor of Science Degree in Exercise Science from Utah State University, followed by a Master of Science Degree from the University of Utah, in Clinical Exercise Physiology. Campbell's greatest passion is working for the physical restoration of medically complex individuals. While serving on the University of Utah's Lung Transplant program, Campbell realized that greater restorative measures could, and should, be implemented to improve functional abilities of patients, and has set his focus on their rehabilitation pathway. Campbell spends his best energies devoted to building rehabilitation programs. Additionally, Campbell is committed to the development of health care professionals as a serving panel member of the industries-first, accredited Cancer Specialist certification prepared by the American College of Sports Medicine (ACSM) and the American Cancer Society (ACS).
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 76

Course Evaluation
Roger Campbell, M.S., CET, MFT-c. The purpose of this evaluation is to gather input so that we may improve this course and how it is taught and therefore help you improve your learning. We are the only ones looking at your responses, and we will report back to you on the feedback received if you desire, you may email us at: [email protected] 1. What are the strongest features of this course and of our teaching? In other words, what contributes most to your learning experience? 2. What specific suggestions do you have for changes that we can make to improve the course or how it is taught? 3. Is the pace of the course: (Too Fast) (Just Right) (Too Slow)
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 77

Multiple Sclerosis Glossary of Terms Abdomen: The belly , that part of the body that contains all of the structures between the chest and the pelvis . The abdomen is separated anatomically from the chest by the diaphragm , the powerful muscle spanning the body cavity below the lungs . Abnormal: Not normal. Deviating from the usual structure, position, condition, or behavior. In referring to a growth, abnormal may mean that it is cancerous or premalignant (likely to become cancer ). Acetaminophen: A pain reliever and fever reducer. Brand name: Tylenol. The exact mechanism of action of acetaminophen is not known. Acetaminophen relieves pain by elevating the pain threshold (that is, by requiring a greater amount of pain to develop before it is felt by a person). Acetaminophen reduces fever through its action on the heat-regulating center (the "thermostat") of the brain. Generic is available. Acetate: A molecular ion derived from acetic acid. The formula of acetate is CH3COO-. Amitriptyline: An antidepressant medication. In some patients with depression, abnormal levels of brain chemicals called neurotransmitters may relate to the depression. Amitriptyline elevates mood by raising the level of neurotransmitters in brain tissue. Amitriptyline is also a sedative that is useful for depressed patients with insomnia, restlessness, and nervousness. It is sometimes used to treat fibromyalgia and symptoms related to chronic pain. Brand names are Elavil and Endep. A generic version is available. Anxiety: A feeling of apprehension and fear characterized by physical symptoms such as palpitations , sweating, and feelings of stress . Anxiety disorders are serious medical illnesses that affect approximately 19 million American adults. These disorders fill people's lives with overwhelming anxiety and fear. Unlike the relatively mild, brief anxiety caused by a stressful event such as a business presentation or a first date, anxiety disorders are chronic, relentless, and can grow progressively worse if not treated. Arms: An appendage in anatomy and in clinical trials. See: Arm. Aspirin: A good example of a tradename that entered into the language, Aspirin was once the Bayer trademark for acetylsalicylic acid . See the entire definition of Aspirin Attention: The ability to focus selectively on a selected stimulus, sustaining that focus and shifting it at will. The ability to concentrate. Back pain: Pain felt in the low or upper back. There are many causes of back pain.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 78

Balance: A biological system that enables us to know where our bodies are in the environment and to maintain a desired position. Normal balance depends on information from the inner ear, other senses (such as sight and touch) and muscle movement. Benign: Not cancer. Not malignant . A benign tumor does not invade surrounding tissue or spread to other parts of the body. A benign tumor may grow but it stays put (in the same place). Bladder: Any pouch or other flexible enclosure that can hold liquids or gases but usually refers to the hollow organ in the lower abdomen that stores urine -- the urinary bladder. The kidneys filter waste from the blood and produce urine, which enters the bladder through two tubes called ureters. Urine leaves the bladder through another tube, the urethra . In women, the urethra is a short tube that opens just in front of the vagina . In men, it is longer, passing through the prostate gland and then the penis . Infection of the bladder is called cystitis . Blindness: Loss of useful sight. Blindness can be temporary or permanent. Damage to any portion of the eye, the optic nerve, or the area of the brain responsible for vision can lead to blindness. There are numerous (actually, innumerable) causes of blindness. The current politically correct terms for blindness include visually handicapped and visually challenged. Blood: The familiar red fluid in the body that contains white and red blood cells, platelets, proteins, and other elements. The blood is transported throughout the body by the circulatory system. Blood functions in two directions: arterial and venous. Arterial blood is the means by which oxygen and nutrients are transported to tissues while venous blood is the means by which carbon dioxide and metabolic by-products are transported to the lungs and kidneys, respectively, for removal from the body. Blood pressure: The blood pressure is the pressure of the blood within the arteries. It is produced primarily by the contraction of the heart muscle. It's measurement is recorded by two numbers. The first (systolic pressure) is measured after the heart contracts and is highest. The second (diastolic pressure) is measured before the heart contracts and lowest. A blood pressure cuff is used to measure the pressure. Elevation of blood pressure is called "hypertension". Bowel: Another name for the intestine . The small bowel and the large bowel are the small intestine and large intestine , respectively. Brain: That part of the central nervous system that is located within the cranium ( skull ). The brain functions as the primary receiver, organizer and distributor of information for the body. It has two (right and left) halves called "hemispheres." Breast : The breast refers to the front of the chest or, more specifically, to the mammary gland. The mammary gland is a milk producing gland. It is composed largely of fat. Within the mammary gland is a complex network of branching ducts. These ducts exit from sac-like structures called lobules, which can produce milk in females. The ducts exit the breast at the nipple.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 79

Catheter: A thin, flexible tube . For example, a catheter placed in a vein provides a pathway for giving drugs, nutrients, fluids, or blood products. Samples of blood can also be withdrawn through the catheter. Chest: The area of the body located between the neck and the abdomen . The chest contains the lungs , the heart and part of the aorta . The walls of the chest are supported by the dorsal vertebrae , the ribs , and the sternum . Chest pain: There are many causes of chest pain. One is angina which results from inadequate oxygen supply to the heart muscle. Angina can be caused by coronary artery disease or spasm of the coronary arteries. Chest pain can also be due to a heart attack (coronary occlusion) and other important diseases such as, for example, dissection of the aorta and a pulmonary embolism. Do not try to ignore chest pain and "work (or play) though it." Chest pain is a warning to seek medical attention. Complication: In medicine, an additional problem that arises following a procedure, treatment or illness and is secondary to it. A complication complicates the situation. Constipation: Infrequent (and frequently incomplete) bowel movements. The opposite of diarrhea, constipation is commonly caused by irritable bowel syndrome, diverticulosis, and medications (constipation can paradoxically be caused by overuse of laxatives). Colon cancer can narrow the colon and thereby cause constipation. The large bowel (colon) can be visualized by barium enema x-rays, sigmoidoscopy, and colonoscopy. Barring a condition such as cancer, high-fiber diets can frequently relieve the constipation. Corticosteroid: Any of the steroid hormones made by the cortex (outer layer) of the adrenal gland. Cortisol is a corticosteroid. Depression : An illness that involves the body, mood, and thoughts, that affects the way a person eats and sleeps, the way one feels about oneself, and the way one thinks about things. A depressive disorder is not the same as a passing blue mood. It is not a sign of personal weakness or a condition that can be wished away. People with a depressive disease cannot merely "pull themselves together" and get better. Without treatment, symptoms can last for weeks, months, or years. Appropriate treatment, however, can help most people with depression. Diagnosis: 1 The nature of a disease ; the identification of an illness. 2 A conclusion or decision reached by diagnosis. The diagnosis is rabies . 3 The identification of any problem. The diagnosis was a plugged IV. Diarrhea : A familiar phenomenon with unusually frequent or unusually liquid bowel movements, excessive watery evacuations of fecal material. The opposite of constipation . The word "diarrhea" with its odd spelling is a near steal from the Greek "diarrhoia" meaning "a flowing through." Plato and Aristotle may have had diarrhoia while today we have diarrhea. There are myriad infectious and noninfectious causes of diarrhea.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 80

Disease: Illness or sickness often characterized by typical patient problems (symptoms) and physical findings (signs). Disruption sequence: The events that occur when a fetus that is developing normally is subjected to a destructive agent such as the rubella (German measles) virus. Dizziness : Painless head discomfort with many possible causes including disturbances of vision, the brain, balance (vestibular) system of the inner ear, and gastrointestinal system. Dizziness is a medically indistinct term which laypersons use to describe a variety of conditions ranging from lightheadedness, unsteadiness to vertigo. Dysfunction: Difficult function or abnormal function. Exacerbation: A worsening. In medicine, exacerbation may refer to an increase in the severity of a disease or its signs and symptoms. For example, exacerbation of asthma is one of the serious effects of air pollution.. Eye: The organ of sight. The eye has a number of components. These components include but are not limited to the cornea, iris, pupil, lens, retina, macula, optic nerve, choroid and vitreous. Fatigue: A condition characterized by a lessened capacity for work and reduced efficiency of accomplishment, usually accompanied by a feeling of weariness and tiredness. Fatigue can be acute and come on suddenly or chronic and persist. FDA: The Food and Drug Administration, an agency within the U.S. Public Health Service, which is a part of the Department of Health and Human Services. Fever : Although a fever technically is any body temperature above the normal of 98.6 degrees F. (37 degrees C.), in practice a person is usually not considered to have a significant fever until the temperature is above 100.4 degrees F (38 degrees C.). Fiber : The parts of plants that cannot be digested, namely complex carbohydrates. Also known as bulk or roughage. Foot: The end of the leg on which a person normally stands and walks. The foot is an extremely complex anatomic structure made up of 26 bones and 33 joints that must work together with 19 muscles and 107 ligaments to execute highly precise movements. At the same time the foot must be strong to support more than 100,000 pounds of pressure for every mile walked. Even small changes in the foot can unexpectedly undermine its structural integrity and cause pain with every step. Gene: The basic biological unit of heredity . A segment of deoxyribonucleic acid (DNA) needed to contribute to a function. Genetic: Having to do with genes and genetic information.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 81

Genetics: The scientific study of heredity . Genetics pertains to humans and all other organisms. So, for example, there is human genetics, mouse genetics, fruitfly genetics, etc. See Health: As officially defined by the World Health Organization, a state of complete physical, mental, and social well-being, not merely the absence of disease or infirmity. High blood pressure : Also known as hypertension, high blood pressure is, by definition, a repeatedly elevated blood pressure exceeding 140 over 90 mmHg -- a systolic pressure above 140 with a diastolic pressure above 90. Hives: A raised, itchy area of skin that is usually a sign of an allergic reaction. It can be rounded or flat-topped but is always elevated above the surrounding skin. It reflects circumscribed dermal edema (local swelling of the skin). The hives are usually well circumscribed but may be coalescent and will blanch with pressure. They typically last less than 4 hours but they may stay for days or weeks. Approximately 20% of the population has experienced a bout of hives. Immune: Protected against infection. The Latin immunis means free, exempt. Immune system: A complex system that is responsible for distinguishing us from everything foreign to us, and for protecting us against infections and foreign substances. The immune system works to seek and kill invaders. Implant: 1. To embed; to set in firmly. In embryology, the fertilized egg implants in the uterine lining 6 or 7 days after conception (fertilization). In medicine today, many things may be implanted. 2. That which is embedded. For example: lens implants, breast implants, cochlear implants, defibrillator implants, pacemaker implants, etc. Incidence: The frequency with which something, such as a disease, appears in a particular population or area. In disease epidemiology, the incidence is the number of newly diagnosed cases during a specific time period. The incidence is distinct from the prevalence which refers to the number of cases alive on a certain date. Inflammation: A basic way in which the body reacts to infection , irritation or other injury, the key feature being redness, warmth, swelling and pain . Inflammation is now recognized as a type of nonspecific immune response . Injury: Harm or hurt. The term "injury" may be applied in medicine to damage inflicted upon oneself as in a hamstring injury or by an external agent on as in a cold injury. The injury may be accidental or deliberate, as with a needlestick injury. The term "injury" may be synonymous (depending on the context) with a wound or with trauma. Interferon : A naturally occurring substance that interferes with the ability of viruses to reproduce. Interferon also boosts the immune system.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 82

Joint: A joint is the area where two bones are attached for the purpose of motion of body parts. A joint is usually formed of fibrous connective tissue and cartilage. An articulation or an arthrosis is the same as a joint. Liver: An organ in the upper abdomen that aids in digestion and removes waste products and worn-out cells from the blood. The liver is the largest solid organ in the body. The liver weighs about three and a half pounds (1.6 kilograms). It measures about 8 inches (20 cm) horizontally (across) and 6.5 inches (17 cm) vertically (down) and is 4.5 inches (12 cm) thick. Magnetic resonance imaging : A special radiology technique designed to image internal structures of the body using magnetism, radio waves, and a computer to produce the images of body structures. In magnetic resonance imaging (MRI), the scanner is a tube surrounded by a giant circular magnet. The patient is placed on a moveable bed that is inserted into the magnet. The magnet creates a strong magnetic field that aligns the protons of hydrogen atoms, which are then exposed to a beam of radio waves. This spins the various protons of the body, and they produce a faint signal that is detected by the receiver portion of the MRI scanner. A computer processes the receiver information, and an image is produced. The image and resolution is quite detailed and can detect tiny changes of structures within the body, particularly in the soft tissue, brain and spinal cord, abdomen and joints. Malignant: 1. Tending to be severe and become progressively worse, as in malignant hypertension. 2. In regard to a tumor, having the properties of a malignancy that can invade and destroy nearby tissue and that may spread (metastasize) to other parts of the body. Manic: Refers to a mood disorder in which a person seems "high", euphoric, expansive, sometimes agitated, hyperexcitable, with flights of ideas and speech. Memory: 1. The ability to recover information about past events or knowledge. 2. The process of recovering information about past events or knowledge. 3. Cognitive reconstruction. The brain engages in a remarkable reshuffling process in an attempt to extract what is general and what is particular about each passing moment. Migraine: Usually, periodic attacks of headaches on one or both sides of the head. These may be accompanied by nausea, vomiting, increased sensitivity of the eyes to light (photophobia), increased sensitivity to sound (phonophobia), dizziness , blurred vision, cognitive disturbances, and other symptoms. Some migraines do not include headache, and migraines may or may not be preceded by an aura. See the entire definition of Migraine Motor: In medicine, having to do with the movement of a part of the body. Something that produces motion or refers to motion. For example, a motor neuron is a nerve cell that conveys an impulse to a muscle causing it to contract. The term "motor" today is also applied to a nerve that signals a gland to secrete. Motor is as opposed to sensory.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 83

Mouth: 1. The upper opening of the digestive tract, beginning with the lips and containing the teeth, gums, and tongue. Foodstuffs are broken down mechanically in the mouth by chewing and saliva is added as a lubricant. Saliva contains amylase, an enzyme that digests starch. 2. Any opening or aperture in the body. The mouth in both senses of the word is also called the os, the Latin word for an opening, or mouth. The o in os is pronounced as in hope. The genitive form of os is oris from which comes the word oral. MRI: Abbreviation and nickname for magnetic resonance imaging. For more information, see: Magnetic Resonance Imaging; Paul C. Lauterbur; Peter Mansfield. Multiple sclerosis : Abbreviated MS. A disease of the central nervous system (CNS) marked by numbness, weakness, loss of muscle coordination, and problems with vision, speech, and bladder control. MS is an autoimmune disease in which the body's immune system attacks myelin, a key substance that serves as a nerve insulator and helps in the transmission of nerve signals. The progress, severity and specific symptoms in MS are unpredictable. One never knows when attacks will occur, how long they will last, or how severe they will be. Most people with MS are between the ages of 20 and 40 at the time of diagnosis. The term "multiple" refers to the multiple places in the CNS that are affected and to the multiple relapses and remissions characteristic of MS. Muscle: Muscle is the tissue of the body which primarily functions as a source of power. There are three types of muscle in the body. Muscle which is responsible for moving extremities and external areas of the body is called "skeletal muscle." Heart muscle is called "cardiac muscle." Muscle that is in the walls of arteries and bowel is called "smooth muscle." Muscular: Having to do with the muscles. Also, endowed with above average muscle development. Muscular system refers to all of the muscles of the body collectively. Myelin: The fatty substance that covers and protects nerves. Myelin is a layered tissue that sheathes the axons (nerve fibers). This sheath around the axon acts like a conduit in an electrical system, ensuring that messages sent by axons are not lost en route. It allows efficient conduction of action potentials down the axon. Myelin consists of 70% lipids (cholesterol and phospholipid) and 30% proteins. It is produced by oligodendrocytes in the central nervous system. Nerve: A bundle of fibers that uses chemical and electrical signals to transmit sensory and motor information from one body part to another. See: Nervous system. Neurological: Having to do with the nerves or the nervous system. Onset: In medicine, the first appearance of the signs or symptoms of an illness as, for example, the onset of rheumatoid arthritis . There is always an onset to a disease but never to the return to good health. The default setting is good health.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 84

Organ: A relatively independent part of the body that carries out one or more special functions. The organs of the human body include the eye, ear, heart, lungs, and liver. Pain: An unpleasant sensation that can range from mild, localized discomfort to agony. Pain has both physical and emotional components. The physical part of pain results from nerve stimulation. Pain may be contained to a discrete area, as in an injury, or it can be more diffuse, as in disorders like fibromyalgia . Pain is mediated by specific nerve fibers that carry the pain impulses to the brain where their conscious appreciation may be modified by many factors. Palpitations: Unpleasant sensations of irregular and/or forceful beating of the heart. In some patients with palpitations, no heart disease or abnormal heart rhythms can be found. In others, palpitations result from abnormal heart rhythms (arrhythmias). Arrhythmias refer to heartbeats that are too slow, too rapid, irregular, or too early. Penile: Of or pertaining to the penis. Phenol: 1. A poisonous corrosive compound obtained by the distillation of coal tar that, in dilute solution, is an antimicrobial agent. Also called carbolic acid. 2. A generic term for any compound similar in structure to phenol (an organic compound with one or more hydroxyl groups attached to an aromatic or carbon ring). Physical therapy: A branch of rehabilitative health that uses specially designed exercises and equipment to help patients regain or improve their physical abilities. Physical therapists work with many types of patients, from infants born with musculoskeletal birth defects, to adults suffering from sciatica or the after- effects of injury, to elderly post-stroke patients. Placebo: A "sugar pill" or any dummy medication or treatment. Plasma: The liquid part of the blood and lymphatic fluid, which makes up about half of its volume. Plasma is devoid of cells and, unlike serum, has not clotted. Blood plasma contains antibodies and other proteins. It is taken from donors and made into medications for a variety of blood-related conditions. Some blood plasma is also used in non-medical products. Plasmapheresis: A procedure designed to deplete the body of blood plasma (the liquid part of the blood) without depleting the body of its blood cells. Whole blood is removed from the body, the plasma is separated from the cells, the cells are suspended in saline, a plasma substitute or donor plasma), and the reconstituted solution may be returned to the patient. The procedure is used to remove excess antibodies from the blood in lupus, multiple sclerosis, multiple myeloma, etc. Plasmapheresis carries with it the same risks as any intravenous procedure. The risk of infection increases with the use of donor plasma, which may carry viral particles despite screening procedures. The procedure is done in a clinic or hospital. Pregnancy: The state of carrying a developing embryo or fetus within the female body. This condition can be indicated by positive results on an over-the-counter urine test, and confirmed through a blood test, ultrasound, detection of fetal heartbeat, or an X-ray. Pregnancy lasts for about nine months, measured from the date of the woman's last menstrual period (LMP). It is conventionally divided into three trimesters, each roughly three months long.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 85

Primary: First or foremost in time or development. The primary teeth (the baby teeth) are those that come first. Primary may also refer to symptoms or a disease to which others are secondary. Progressive: Increasing in scope or severity. Advancing. Going forward. In medicine, a disease that is progressive is going from bad to worse. Protein: A large molecule composed of one or more chains of amino acids in a specific order determined by the base sequence of nucleotides in the DNA coding for the protein. Range: In medicine and statistics, the difference between the lowest and highest numerical values. For example, if five premature infants are born weighing two, three, four, four, and five pounds respectively, the range of their birth weights is two to five pounds. Relapse: The return of signs and symptoms of a disease after a patient has enjoyed a remission . For example, after treatment a patient with cancer of the colon went into remission with no sign or symptom of the tumor, remained in remission for 4 years, but then suffered a relapse and had to be treated once again for colon cancer. Remission: Disappearance of the signs and symptoms of cancer or other disease. When this happens, the disease is said to be "in remission." A remission can be temporary or permanent. Sclerosis: Localized hardening of skin. Sensation: In medicine and physiology , sensation refers to the registration of an incoming ( afferent ) nerve impulse in that part of the brain called the sensorium , which is capable of such perception. Therefore, the awareness of a stimulus as a result of its perception by sensory receptors. (Sensory is here synonymous with sensation.) Sensitivity: 1. In psychology, the quality of being sensitive. As, for example, sensitivity training, training in small groups to develop a sensitive awareness and understanding of oneself and of ones relationships with others. 2. In disease epidemiology, the ability of a system to detect epidemics and other changes in disease occurrence. 3. In screening for a disease, the proportion of persons with the disease who are correctly identified by a screening test. 4. In the definition of a disease, the proportion of persons with the disease who are correctly identified by defined criteria. Sensory: Relating to sensation , to the perception of a stimulus and the voyage made by incoming ( afferent ) nerve impulses from the sense organs to the nerve centers. Side effects: Problems that occur when treatment goes beyond the desired effect. Or problems that occur in addition to the desired therapeutic effect. Sinusitis: Sinusitis is inflammation of the lining membrane of any of the hollow areas (sinuses) of the bone of the skull around the nose. The sinuses are directly connected to the nasal cavities.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 86

Skin: The skin is the body's outer covering. It protects us against heat and light, injury, and infection. It regulates body temperature and stores water, fat, and vitamin D. Weighing about 6 pounds, the skin is the body's largest organ. It is made up of two main layers; the outer epidermis and the inner dermis. Spasticity: A state of increased tone of a muscle (and an increase in the deep tendon reflexes). For example, with spasticity of the legs (spastic paraplegia) there is an increase in tone of the leg muscles so they feel tight and rigid and the knee jerk reflex is exaggerated. SPF (sun protection factor): A number on a scale for rating sunscreens. SPF stands for Sun Protection Factor. Spinal cord: The major column of nerve tissue that is connected to the brain and lies within the vertebral canal and from which the spinal nerves emerge. Thirty-one pairs of spinal nerves originate in the spinal cord: 8 cervical , 12 thoracic , 5 lumbar, 5 sacral, and 1 coccygeal. The spinal cord and the brain constitute the central nervous system ( CNS ). The spinal cord consists of nerve fibers that transmit impulses to and from the brain. Like the brain, the spinal cord is covered by three connective-tissue envelopes called the meninges . The space between the outer and middle envelopes is filled with cerebrospinal fluid ( CSF ), a clear colorless fluid that cushions the spinal cord against jarring shock. Also known simply as the cord. Surgery: The word "surgery" has multiple meanings. It is the branch of medicine concerned with diseases and conditions which require or are amenable to operative procedures. Surgery is the work done by a surgeon. By analogy, the work of an editor wielding his pen as a scalpel is s form of surgery. A surgery in England (and some other countries) is a physician's or dentist's office. Syndrome: A set of signs and symptoms that tend to occur together and which reflect the presence of a particular disease or an increased chance of developing a particular disease. Therapy: The treatment of disease . Throat: The throat is the anterior (front) portion of the neck beginning at the back of the mouth , consisting anatomically of the pharynx and larynx . The throat contains the trachea and a portion of the esophagus . Tiredness: See: Tired. Tissue: A tissue in medicine is not like a piece of tissue paper. It is a broad term that is applied to any group of cells that perform specific functions. A tissue in medicine need not form a layer. Thus,
• The bone marrow is a tissue; • Connective tissue consists of cells that make up fibers in the framework supporting
other body tissues; and • Lymphoid tissue is the part of the body's immune system that helps protect it from
bacteria and other foreign entities.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 87

Twin: One of two children produced in the same pregnancy and born during the same birth process. Urine: Liquid waste. The urine is a clear, transparent fluid. It normally has an amber color. The average amount of urine excreted in 24 hours is from 40 to 60 ounces (about 1,200 cubic centimeters). Chemically, the urine is mainly an aqueous (watery) solution of salt (sodium chloride) and substances called urea and uric acid. Normally, it contains about 960 parts of water to 40 parts of solid matter. Abnormally, it may contain sugar (in diabetes), albumen (a protein) (as in some forms of kidney disease), bile pigments (as in jaundice), or abnormal quantities of one or another of its normal components. Virus: A microorganism smaller than a bacteria, which cannot grow or reproduce apart from a living cell. A virus invades living cells and uses their chemical machinery to keep itself alive and to replicate itself. It may reproduce with fidelity or with errors (mutations)-this ability to mutate is responsible for the ability of some viruses to change slightly in each infected person, making treatment more difficult. Viruses: Small living particles that can infect cells and change how the cells function. Infection with a virus can cause a person to develop symptoms. The disease and symptoms that are caused depend on the type of virus and the type of cells that are infected. Vitamin C: An essential nutrient found mainly in fruits and vegetables. The body requires vitamin C to form and maintain bones, blood vessels, and skin.
www.rehabsys.com Rehabilitation Systems 2011 Copying or distributing without written consent is prohibited. 88