multiple myeloma after ash 2016 - office of continuing ...cme.uthscsa.edu/courses/panao/2017/online...
TRANSCRIPT

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
EOKMultiple Myeloma after ASH 2016
Financial Disclosure
No relevant financial relationships to disclose
10% per year
1% per year
3% per year
1% per year

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Diagnosis of MyelomaRevised Definition of Multiple Myeloma
Classical Definition HyperCalcemia
Renal insufficiency
Anemia
Bone disease
Expanded Definition: Myeloma defining events
Clonal BMPC ≥ 60%
> 1 focal lesion on MRI
Involved/uninvolved serum FLC ratio > 100
Rajkumar SV, et al. Lancet Oncol. 2014;15:e538-548.
Predicts ≥ 80% probability of progression from smoldering to active disease within 2 yrs
Multiple Myeloma by the numbers
• 2nd most common hematologic malignancy
• More than 30,000 new cases in US every year
• Approximately 12,000 deaths in US every year
• African Americans 2X
• Male: Female: 1.4:1
• Age <40: 2%
• Median age at diagnosis 69 years; at death 75 years
• 5 year relative survival approximately 50% (2006‐2012)
1. American Cancer Society. Cancer facts & figures. 2014. 2. SEER stat fact sheet: myeloma. 2016.
Revised ISS Staging System
Palumbo A, et al. J Clin Oncol. 2015;33:2863-2869.
Definition
I
ISS stage I AND Normal LDH No t(4;14), t(14;16), or del(17p)
II Not stage I or III
III
ISS stage IIIAND Serum LDH > ULNOR With t(4;14), t(14;16), or del(17p)
1.0
0.8
0.6
0.4
0.2
00 12 24 36 48 60 72
R-ISS I NRR-ISS II 83R-ISS III 43
Median OS, Mos
Mos
Pro
bab
ilit
y o
f O
S
Definition
I Serum albumin ≥ 3.5 g/dL AND β2-M < 3.5 mg/L
II Not stage I or III
III β2-M ≥ 5.5 mg/dL
ISS Stage
R-ISS Stage

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
R-ISS stage: OS based on Therapy
Regardless of therapy
A. Non-autologous stem cell transplant
B. Autologous stem cell transplant
C. IMiD based therapy
D. PI based therapy
R-ISS stage differentiated patient outcomes
Revised ISS Stage Limitations
Pooled data from 3000+ patients on RCT!
- not real world patients who are not healthy enough to be on trials, frail patients
- 65% were less than 65 years old
- Majority of real world patients >70 years old
Excluded chromosome 1 abnormalities from analysis, evolving data supporting this is high risk
No host related factors: Age, performance status, comorbidities
No validation of this in an independent data set
Early deaths in high risk patientsNo plateau
Myeloma Treatment Paradigm
Induction
Induction followed by continuous therapy
Consolidation Maintenance
SC
T
Elig
ible
SC
T
Inel
igib
le
Dia
gn
osi
s an
d
Ris
k S
trat
ific
atio
n
Tumor Burden

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Myeloma Rx heading into 2017Melphalan Prednisone versus Conventional chemotherapy
Attal M, et al. N Engl J Med. 1996;335:91-97.
Transplantation vs Conventional Chemotherapy
15 30 45 60
25
50
75
100
OS
(%
)
00
High dose
Conventional dose
Mos
63%
69%
35%
61%
12%
52%
Autologous Stem Cell TransplantMaintenance

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
What is the role of upfront transplant in the era of novel agents?IFM/DFCI 2009: Phase III Study Design
Primary objective: PFS
Secondary objectives: ORR, MRD, TTP, OS, safety
Attal M, et al. ASH 2015. Abstract 391.
Pts 65 yrs of age or younger with symptomatic
measurable NDMM; ECOG PS < 2
(N = 700)
Lenalidomidemaintenance
12 mos
*RVD: bortezomib 1.3 mg/m2 IV on Days 1, 4, 8, 11 + lenalidomide 25 mg on Days 1-14 + dexamethasone 20 mg on Days 1, 2, 4, 5, 8, 9, 11, 12.†Included PBSC collection with cyclophosphamide 3 g/m2 + G-CSF after cycle 3.
RVd*†
8 cycles
RVd*3 cycles
RVd*2 cycles
consolidation
MEL200ASCT†
IFM 2009: Responses
At second interim analysis in June 2015 with median follow-up of 39 mos, the data and safety monitoring board for this trial recommended that the trial be stopped
Response, %RVD
(n = 350)Transplantation
(n = 350)P Value
CR 49 59
.02VGPR 29 29
PR 20 11
< PR 2 1
≥ VGPR 78 88 .001
Negative MRD by FCM 65 80 .001
Attal M, et al. ASH 2015. Abstract 391.
Attal M, et al. ASH 2015. Abstract 391.
IFM 2009: PFS
Pts
(%
)
Follow-up (Mos)
ASCTNo ASCT
100
80
60
40
20
00 12 24 36 48
P < .001
Pts at Risk, n
ASCTNo ASCT
350350
309296
261228
153128
2724
ParameterRVD
(n = 350)Transplantation
(n = 350)P Value
Median follow-up, mos 41 41
Progression or death, n 204 158
Median PFS, mos 34 43
4-yr PFS, % 35 47
HR (95% CI) 1 0.69 (0.56-0.84) < .001
Lenalidomide Maintenance

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
SPM risk
Is more treatment better?Role of tandem transplant or triple consolidationSTaMINA: Phase III Study Design
Primary endpoint: PFS at 38 mos
Secondary endpoints: OS, ORR, CR conversion rate, safety, infections, tx-related mortality, QoL
ASCT-eligible pts ≤ 70 yrswith symptomatic MM and ≥ 2 cycles systemic tx
initiated in past 12 mos;no prior progression;
adequate organ function(N = 758)
Single ASCTLenalidomide Maintenance until PD*
10 mg/day for 3 cycles, then 15 mg/day*(n = 257)
Bortezomib 1.3 mg/m² IV Days 1, 4, 8, 11Lenalidomide 15 mg Days 1-15
Dexamethasone 40 mg IV Days 1, 8, 15Four 28-day cycles
(n = 254)
Stadtmauer EA, et al. ASH 2016. Abstract LBA-1
Lenalidomide Maintenance until PD
10 mg/day for 3 cycles, then 15 mg/day*
Tandem ASCTMelphalan 200 mg/m² IV
Second ASCT(n = 247)
*Originally given for 3 yrs only but amended to until PD in 2014.
Stratified by risk group (high vs standard)
Melphalan 200 mg/m² IV
ASCT
STaMINA: PFS and OS for Overall Population
PFS (Primary Endpoint) OS
Stadtmauer EA, et al. ASH 2016. Abstract LBA-1. Reproduced with permission.
100
80
60
40
20
0
PF
S (
%)
0 12 24 38
38-Mo Estimate, % (95% CI)
Tandem ASCT: 56.5 (49.4-62.9)RVD consolidation: 56.7 (50.0-62.8)Single ASCT: 52.2 (45.4-58.6)
Pts at Risk, nTandem ASCT
RVD consolidation Single ASCT
247254257
200215213
153172158
879980
Mos From Randomization
100
80
60
40
20
0
OS
(%
)
0 12 24 38
38-Mo Estimate, % (95% CI)
Tandem ASCT: 82.0 (76.3-86.5)RVD consolidation: 85.7 (80.5-89.5)Single ASCT: 83.4 (77.9-87.7)
Pts at Risk, nTandem ASCT
RVD consolidation Single ASCT
247254257
231246247
204229227
147166148
Mos From Randomization
In high-risk patients, PFS was between 40% and 48% at 38 months, with no difference in OS

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
STaMINA: Secondary Primary Malignancies
Secondary Malignancy in First 38 Mos Single ASCT(n = 257)
RVD Consolidation
(n = 254)
Tandem ASCT
(n = 247)
No. of second malignancies 10 15 14
Cumulative incidence,* % (95% CI) 4.0 (1.9-7.2) 6.0 (3.4-9.6) 5.9 (3.3-9.6)
Most common malignancy, n Solid tumors, NR Leukemia, 9 Leukemia, 3
Stadtmauer EA, et al. ASH 2016. Abstract LBA-1.
*First secondary malignancy.
Non‐Transplant OptionsNovel agents
Combining agents with different mechanisms may have a synergistic effect
Integration of novel agents into myeloma management
• Target MM in the BM microenvironment to overcome conventional drug resistance in vitro, and in vivo
• Effective in relapse/refractory, relapsed, induction, consolidation, and maintenance therapy
• Median survival prolonged from 2‐4 years to approximately 6‐7 years, with additional prolongation from maintenance
• New approaches needed to create and ultimately prevent relapse

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Therapeutic Agents in Myeloma: Old vs New
“Older” novel agents
– Bortezomib
– Lenalidomide
– Carfilzomib
– Pomalidomide
“Newer” novel agents
– Daratumumab
– Ixazomib
– Elotuzumab
– Panobinostat
Earlier lines or induction therapy, partner for
newer agents
Monoclonal antibody
Novel Myeloma Therapy DevelopmentNovel Therapies Novel Therapies
and Immunotherapy
Lenalidomide
Thalidomide
BortezomibLiposomal
Doxorubicin
Pomalidomide
Panobinostat
CAR T Investigational
VaccinesInvestigational
NivolumabInvestigational
AtezolizumabInvestigational
IsatuximabInvestigational
Elotuzumab
2003 2006 2007 2012 2013 2015 2016+
IMID
Proteasome inhibitor HDAC inhibitor
Chemotherapy
Adoptive T cell therapy
Vaccines
Checkpoint inhibitors
Carfilzomib
Ixazomib
Daratumumab
Backbone
FIRST: Lenalidomide/Dexamethasone vs MPT in NDMM SCT-Ineligible Pts
Ran
dom
ized
1:1
:1
Arm BRd18
Arm CMPT
Len + LoDex 18 cycles (72 wks) Lenalidomide 25 mg on Days 1-21/28LoDex 40 mg on Days 1, 8, 15, 22/28
Mel + Pred + Thal 12 cycles (72 wks)Melphalan 0.25 mg/kg on Days 1-4/42Prednisone 2 mg/kg on Days 1-4/42Thalidomide 200 mg on Days 1-42/42
PD
, OS
, and
subsequent anti-MM
Tx
PD
or unacceptable toxicity
Active treatment + PFS follow-up phase
Pts > 75 yrs: LoDex 20 mg on Days 1, 8, 15, 22/28; Thal 100 mg on Days 1-42/42; Mel 0.2 mg/kg on Days 1-4. Stratification: age, country, and ISS stage.
Len + LoDex ContinuouslyLenalidomide 25 mg on Days 1-21/28LoDex 40 mg on Days 1, 8, 15, 22/28
Arm AContinuous Rd
Hulin C, et al. ASH 2014. Abstract 81. Facon T, et al. Lancet. 2007;370:1209-1218. Hulin C, et al. J Clin Oncol. 2009;27:3664-3670. Benboubker L, et al. N Engl J Med. 2014;371:906-917
Phase III(N = 1623)
FIRST Trial: Rd (Continuous or Every 18 Mos) vs MPT
Pts
(%
)
100
80
60
40
20
0
HR:Continuous Rd vs MPT: 0.72; P < .001Continuous Rd vs Rd18: 0.70; P < .001
Continuous Rd (n = 535) Rd18 (n = 541)MPT (n = 547)
Median PFS, Mos
25.520.721.2
0 6 12 18 24 30 36 42 48 54 60
PFS OS
Benboubker L, et al. N Engl J Med. 2014;371:906-917.
Pts
(%
)
100
80
60
40
20
0
Continuous Rd (n = 535) Rd18 (n = 541)MPT (n = 547)
4-Yr OS, %595651
0 6 12 18 24 30 36 42 48 54 60
Mos Mos

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Combinations in the upfront treatmentDoublet Vs Triplet UpfrontSWOG S0777: Study Design
Randomized phase III trial of VRd vs Rd
Lenalidomide 25 mg/day PO Days 1-21 +Dexamethasone 40 mg/day PO Days 1, 8, 15, 22
for six 28-day cycles(eligible n = 230)
Bortezomib 1.3 mg/m2 IV Days 1, 4, 8, 11 +Lenalidomide 25 mg/day PO Days 1-14 +
Dexamethasone 20 mg/day PO Days 1, 2, 4, 5, 8, 9, 11,12 for eight 21-day cycles
(eligible n = 243)
Rd maintenance
until PD, unacceptable
AE, or withdrawal of
consent
Stratified by ISS stage I/II/III and intent to transplant at progression
Durie B, et al. ASH 2015. Abstract 25.
Previously untreated active MM
(CRAB criteria) with measurable
disease (including FLC) and
CrCl > 30 cc/min(N = 525)
All pts received aspirin 325 mg/day; pts in bortezomib arm received HSV prophylaxis
Primary endpoint: PFS
Secondary endpoints: ORR, OS, safety
Durie B, et al. ASH 2015. Abstract 25.
SWOG S0777: PFS
Pts
Wit
ho
ut
Pro
gre
ssio
n
Mos Since Registration
Median PFS, Mos
VRd (n = 242) 43Rd (n = 229) 30
HR: 0.71; P = .0018
100
80
60
40
20
00 24 48 72 96

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Durie B, et al. ASH 2015. Abstract 25.
SWOG S0777: OS
Pts
Rem
ain
ing
Ali
ve
Mos Since Registration
Median OS, Mos
VRd (n = 242) 75Rd (n = 229) 64
HR: 0.71; P = .025
100
80
60
40
20
00 24 48 72 96
S0777: VRd vs Rd
Grade ≥3 AE VRD Rd P value
Neuro 33 11 <.0001
Pain 12 4 .0002
Sensory 23 3 .004
GI 22 8 NA
20 patients experienced secondary primary malignancies, 10 (4%) on VRd and 10 (4%) on Rd
Initial Myeloma Rx: Summary
Combination of IMiD and PI should be considered standard
- RVd head-to-head winner vs Rd
Early single autologous transplant adds benefit and should be considered standard
- ORR, VGPR, PFS, MRD all better with ASCT
What’s coming?
- Rd+Carfilzomib; Rd+Dara; VRd+Elo
Relapsed/Refractory Multiple MyelomaWhen to consider retreatment
• Differences between biochemical relapse and asymptomatic relapse needs to be considered
• Does this patient really need to be treated now? Patients with asymptomatic rising M protein can be observed to determine the rate of rise and nature of the relapse
Caveat: patient with known aggressive or high risk disease should be considered for salvage even in the setting of biochemical relapse
• CRAB criteria are still listed as the indication to treat in the relapse setting. However, in patients with progression, treatment can avoid CRAB

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Basic principles of selecting a treatment
Use new agent: Use drugs the patient has not received before; class switching
Using same drug in a different combination
Using another drug in the same class: patients progressing on thalidomide may respond to lenalidomide; those progressing on lenalidomide may respond to pomalidomide; those progressing on bortezomib may respond to carfilzomib
Increase dose: Patients progressing on lenalidomide at 10 mg may respond when dose is increased to 25 mg plus dexamethasone or addition of cyclophosphamide
Adding clarithromycin to lenalidomide, thalidomide or pomalidomide can be used to achieve a temporary response
Richardson PG, et al. Blood. 2014;123:1461-1469 Berenson et. al. Leukemia (2014) 28, 1529–1536.
Nijhof IS, et al. ASH 2013. Abstract 287. Richardson P, et al. Blood. 2009;114-772-778.
Factors to consider while selecting treatment
•Diabetes
•CHF, MI
•Renal failure
•Oral, IV, subcutaneous
•How active is the patient?
•Can the patient travel to receive treatment?
•Aggressiveness of disease
•Cytogenetics
•Quality and duration of previous response?
•Pre‐existing toxicities?
Prior Treatments
Disease characteristics
Comorbid conditions
Convenience
What is new?
New drugs/combinations recently approved by the FDA for R/R myeloma
Panobinostat (Oral): Feb 28, 2015: pan-deacetylase inhibitor, in combination with bortezomib and dex
Daratumumab (IV): Nov 16, 2015: Human anti-CD138 IgG1, single agent
Ixazomib (Oral): Nov 20, 2015: PI, in combination with lenalidomide and dex
Elotuzumab (IV): Nov 30, 2015: human IgG1 immunostimulatory monoclonal Ab targeting SLAMF-7 and activates NK cell, in combination with lenalidomide and dex
3 new combinations approved
Carfilzomib/Rev/dexDara/len/dexDara/bort/dex
2 vs 3 drugs in R/R myelomaDrug Class Study arm Control arm
Carfilzomib (27 mg/m2)
Proteasome Inhibitor Carfilzomib/lenalidomide/dex Lenalidomide/dex
Ixazomib Proteasome Inhibitor Ixazomib/lenalidomide/dex Lenalidomide/dex
Elotuzumab Monoclonal Antibody Elotuzumab/lenalidomide/dex Lenalidomide/dex
Panobinostat HDAC inhibitor Panobinostat/bortezomib/dex Bortezomib/dex
Daratumumab Monoclonal Antibody Daratumumab/lenalidomide/dex Lenalidomide/dex
Daratumumab Monoclonal Antibody Daratumumab/lenalidomide/dex Bortezomib/dex
Caveat: The randomized trials with KRd, ERd, and IRd included only those patients not refractory to lenalidomide, and we do not know how active these combinations are in lenalidomide‐refractory MM

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Doublet Vs Triplet (ORR, ≥ VGPR, PFS)
Pubmed, Cochrane database, ASH, ASCO conference proceedings from 1/200 through 01/2016 to identify phase 3 RCTs that have randomized early relapsed myeloma patients (≤ 3 prior lines) to receive a triplet vs a doublet salvage regimen
Nooka et. al. ASCO 2016 oral abstract
Slide 7
Meta‐analysis of 5 RCT (PANORAMA‐1, MMVAR, ASPIRE, ELOQUENT‐2, TOURMALINE‐MM1)
Nooka et. al. ASCO 2016 oral abstract
Randomized phase II trial evaluating VDC, VDR, and VDCR in previously untreated MM
Four drug combination had similar efficacy, but with increased toxicity
EVOLUTION: 3 vs 4 Agents in Combination
Kumar S, et al. Blood. 2012;119:4375-4382.
Patients categorized as VGPR include those who have no measurable M-protein but have not yet had bone marrow assessments to confirm CR/nCR status.Response determined according to automated computer algorithm.
Response, n (%) VDCR (n = 48)
VDR (n = 42)
VDC (n = 33)
VDC-Mod (n = 17)
CR 10 (25) 10 (24) 7 (22) 8 (47)
≥ VGPR 23 (58) 21 (51) 13 (41) 9 (53)
ORR (≥ PR) 35 (88) 35 (85) 24 (75) 17 (100)
Should we aspire to use 3 drugs in R/R myeloma?ASPIRE: Addition of Carfilzomib to Rd in Relapsed/Progressive Myeloma
Randomized, open-label phase III trial
Pts with relapsed or progressive MM,
1-3 prior treatments with ≥ PR in
≥ 1 prior regimen, ECOG PS 0-2, and CrCl ≥ 50 mL/min
(N = 792)
Until PD or unacceptable
toxicity
KRdCarfilzomib Days 1, 2, 8, 9, 15, 16 for cycles 1-12,
Days 1, 2, 15, 16 for cycles 13-18,and discontinued after cycle 18 +
Lenalidomide Days 1-21 +Dexamethasone Days 1, 8, 15, 22
28-day cycle(n = 396)
RdLenalidomide Days 1-21 +
Dexamethasone Days 1, 8, 15, 2228-day cycle
(n = 396)
Stratified by β2-microglobulin, prior bortezomib, and prior lenalidomide
Carfilzomib: 20 mg/m2 Days 1, 2 of cycle 1; 27 mg/m2 thereafter. Lenalidomide: 25 mg. Dexamethasone: 40 mg.
Stewart AK, et al. N Engl J Med. 2015;372:142-152.

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
ASPIRE: PFS Significant improvement in PFS in KRd arm vs Rd arm
Stewart AK, et al. N Engl J Med. 2015;372:142-152.
KRd Rd(n = 396) (n = 396)
Median PFS, mos 26.3 17.6HR (95% CI) 0.69 (0.57-0.83)
P < .0001
100
80
60
40
20
0
PF
S (
%)
KRdRd
0 6 12 18 24 30 36 42 48Mos Since Randomization
Pts at Risk, nKRd
Rd396 332 279 222 179 112 24 1396 287 206 151 117 72 18 1
KRd in Pts With MM and Early Progression: Efficacy
ORR and median PFS better in KRd vs Rd arms in both subgroups
Ludwig H, et al. ASCO 2016. Abstract 8045.
Outcome Early Relapse Posttransplant Early Relapse
KRd(n = 87)
Rd(n = 72)
KRd(n = 48)
Rd(n = 49)
ORR, % (95% CI) 79.3 (69.3-87.3)
61.1 (48.9-72.4)
83.3 (69.8-92.5)
61.2 (46.2-74.8)
Best overall response, n (%) CR or better VGPR PR
19 (21.8)32 (36.8) 18 (20.7)
3 (4.2)24 (33.3) 17 (23.6)
6 (12.5)25 (52.1) 9 (18.8)
2 (4.1)13 (26.5) 15 (30.6)
Median DoR, mos (95% CI) 24.9 (17.5-30.4)
17.0 (9.7-NE)
18.5 (14.3-23.1)
19.6 (8.3-27.3)
Median PFS, mos 24.1 12.5 17.3 11.1
HR (95% CI) 0.750 (0.500-1.125) 0.870 (0.536-1.411)
Slide credit: clinicaloptions.com
Side effects
Stewart AK, et al. N Engl J Med. 2015;372:142-152
AE % Carfilzomib/len/dex Len/dexAll grades Grade >3 All grades Grade >3
Any grade 3/4 AE 83.7 80.7
Nonhematologic AE
Diarrhea 42.3 3.8 33.7 4.1
Fatigue 32.9 7.7 30.6 6.4
Cough 28.8 0.3 17.2 0
Pyrexia 28.6 1.8 20.8 0.5
Upper respiratory tract infection
28.6 1.8 19.3 1.0
Hypokalemia 27.6 9.4 13.4 4.9
Muscle spasms 26.5 1.0 21.1 0.8
Other AEs of interest
Peripheral neuropathy
17.1 NR 17.0NR
Dyspnea 19.4 2.8 14.9 1.8
Hypertension 14.3 4.3 6.9 1.8
Acute renal failure 8.4 3.3 7.23.1
Cardiac failure 6.4 3.8 4.1 1.8
Ischemic heart disease
5.9 3.3 4.62.1
Response and Safety
>PR Complete Response
Duration of Response(months)
Len/dex 67 9 21.2
Carfilzomib/Len/dex 87 32 28.6
Stewart AK, et al. N Engl J Med. 2015;372:142-152
Twice a week IntravenousRelatively safe in renal failureMonitor for dyspnea, HTN, cytopeniasNew onset or worsening of heart failure can occur, especially in >75 yrs oldDose 27mg/m2 in triplet (10 min); 56mg/m2 in doublet or monotherapy (30 min)Carfilzomib in combination with dex or with lenalidomide/dex approved in patients who have received 1‐3 prior lines of therapyMultiple ongoing trials in the upfront and relapsed setting

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Which Proteasome Inhibitor is superior?ENDEAVOR: Kd vs Vd in Relapsed MM
Randomized, open-label, multicenter phase III trial
Primary endpoint: PFS
Secondary endpoints: OS, ORR, DoR, grade ≥ 2 peripheral neuropathy, safety
Dimopoulos MA, et al. Lancet Oncol. 2016;17:27-38.
Relapsed MM with 1-3 prior lines of therapy; prior V or K if
response occurred with no discontinuation due to toxicity
(N = 929)
Kd* (n = 464)
Vd†
(n = 465)
Until PD or unacceptable
toxicity
Stratified by prior PI therapy, prior lines of treatment, ISS stage, and route of V administration (IV vs SC)
*Carfilzomib: cycle 1 only, 20 mg/m2 IV on Days 1, 2 followed by 56 mg/m2 on Days 8, 9, 15, 16, then 56 mg/m2 on Days 1, 2, 8, 9, 15, 16 of a 28-day cycles; dexamethasone: 20 mg on Days 1, 2, 8, 9, 15, 16, 22, 23 of a 28-day cycle. On days when carfilzomib is administered, dexamethasone given 30 mins to 4 hrs prior to carfilzomib. †Bortezomib: 1.3 mg/m2 IV bolus or SC on Days 1, 4, 8, 11 of a 21-day cycle; dexamethasone: 20 mg on Days 1, 2, 4, 5, 8, 9, 11, 12 of a 21-day cycle.
100
80
60
40
20
0
PF
S (
%)
0
Mos Since Randomization
KdVd
Kd(n = 464)
171 (37)18.7
Vd(n = 465)
243 (52)9.4
0.53 (0.44–0.65)1-sided P < .0001
Disease progression or death, n (%)Median PFS, mosHR for Kd vs Vd (95% CI)
Median follow-up: 11.2 mos
6 12 18 24 30
ENDEAVOR: PFS
Dimopoulos MA, et al. Lancet Oncol. 2016;17:27-38.
Kd (n = 214)
Vd (n = 213)
1-SidedP Value
Kd (n=250)
Vd (n=252)
1-SidedP Value
Median PFS, mos NE 11.2 Median PFS, mos 15.6 8.1ORR, % (95% CI) 84 (78–88) 65 (59–72) < .0001 ORR, % (95% CI) 71 (65–77) 60 (54–66) .005
No Prior Bortezomib Prior Bortezomib100
80
60
40
20
0
PF
S (
%)
0 6 12 18 24 30
Mos Since Randomization
KdVd
100
80
60
40
20
0
PF
S (
%)
Mos Since Randomization
KdVd
0 6 12 18 24 30
ENDEAVOR: PFS by Prior Bortezomib
Dimopoulos MA, et al. Lancet Oncol. 2016;17:27-38.
Survival and Response ratesCarfilzomib/dex Bortezomib/dex
>CR 13% 6%
>VGPR 54% 29%
>PR(Overallresponse)
77% 63%
Duration ofResponse
21.3 months 10.4 months
PFS 18.7 months 9.4 months
Serious side effects
48% 36%
Anemia 14 10
High BP 9 3
Low platelets 8 9
Peripheral neuropathy
2 8
Pneumonia 7 8
Longer follow up needed to ascertain if this translates in superior survivalCarfilzomib with dexamethasone could be considered in cases in which bortezomib with dexamethasone is a potential treatment option
Dimopoulos et. Al. Lancet Oncol 2016; 17: 27–38 Moreau P, et al. ASH 2015. Abstract 729.
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
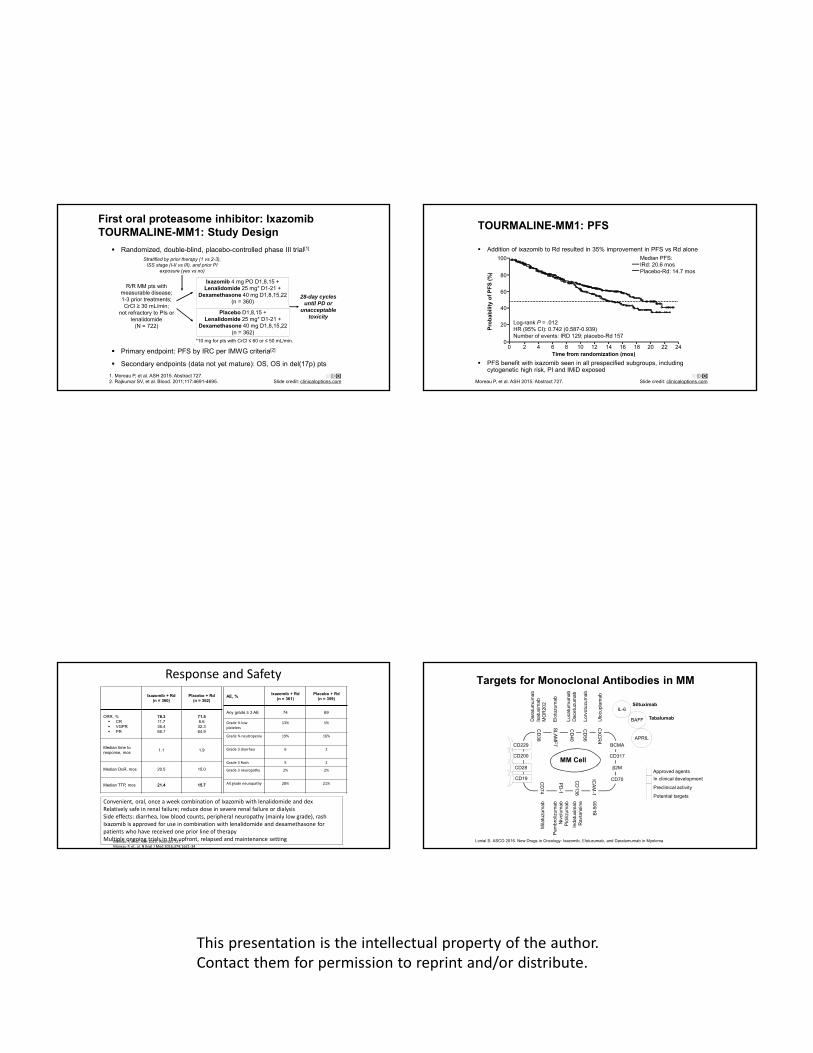
First oral proteasome inhibitor: IxazomibTOURMALINE-MM1: Study Design
Randomized, double-blind, placebo-controlled phase III trial[1]
Primary endpoint: PFS by IRC per IMWG criteria[2]
Secondary endpoints (data not yet mature): OS, OS in del(17p) pts
1. Moreau P, et al. ASH 2015. Abstract 727. 2. Rajkumar SV, et al. Blood. 2011;117:4691-4695.
Ixazomib 4 mg PO D1,8,15 +Lenalidomide 25 mg* D1-21 +
Dexamethasone 40 mg D1,8,15,22(n = 360)
R/R MM pts with measurable disease; 1-3 prior treatments; CrCl ≥ 30 mL/min;
not refractory to PIs or lenalidomide
(N = 722)
Placebo D1,8,15 +Lenalidomide 25 mg* D1-21 +
Dexamethasone 40 mg D1,8,15,22(n = 362)
28-day cyclesuntil PD or
unacceptable toxicity
Stratified by prior therapy (1 vs 2-3), ISS stage (I-II vs III), and prior PI
exposure (yes vs no)
*10 mg for pts with CrCl ≤ 60 or ≤ 50 mL/min.
Slide credit: clinicaloptions.com
TOURMALINE-MM1: PFS
Moreau P, et al. ASH 2015. Abstract 727. Slide credit: clinicaloptions.com
Addition of ixazomib to Rd resulted in 35% improvement in PFS vs Rd alone
PFS benefit with ixazomib seen in all prespecified subgroups, including cytogenetic high risk, PI and IMiD exposed
100
80
60
40
20
0
Log-rank P = .012HR (95% CI): 0.742 (0.587-0.939)Number of events: IRD 129; placebo-Rd 157
Median PFS:IRd: 20.6 mosPlacebo-Rd: 14.7 mos
0 2 4 6 8 10 12 14 16 18 20 22 24Time from randomization (mos)
Pro
ba
bili
ty o
f P
FS
(%
)
Response and Safety
Ixazomib + Rd(n = 360)
Placebo + Rd(n = 362)
ORR, % CR VGPR PR
78.311.736.466.7
71.56.632.364.9
Median time to response, mos
1.1 1.9
Median DoR, mos 20.5 15.0
Median TTP, mos 21.4 15.7
Moreau P, et al. ASH 2015. Abstract 727.Moreau P, et. al. N Engl J Med 2016;374:1621‐34
Convenient, oral, once a week combination of Ixazomib with lenalidomide and dexRelatively safe in renal failure; reduce dose in severe renal failure or dialysisSide effects: diarrhea, low blood counts, peripheral neuropathy (mainly low grade), rashIxazomib is approved for use in combination with lenalidomide and dexamethasone for patients who have received one prior line of therapyMultiple ongoing trials in the upfront, relapsed and maintenance setting
AE, %Ixazomib + Rd
(n = 361)Placebo + Rd
(n = 359)
Any grade ≥ 3 AE 74 69
Grade ¾ low platelets
13% 5%
Grade ¾ neutropenia 19% 16%
Grade 3 diarrhea 6 2
Grade 3 Rash 5 2
Grade 3 neuropathy 2% 2%
All grade neuropathy 28% 21%
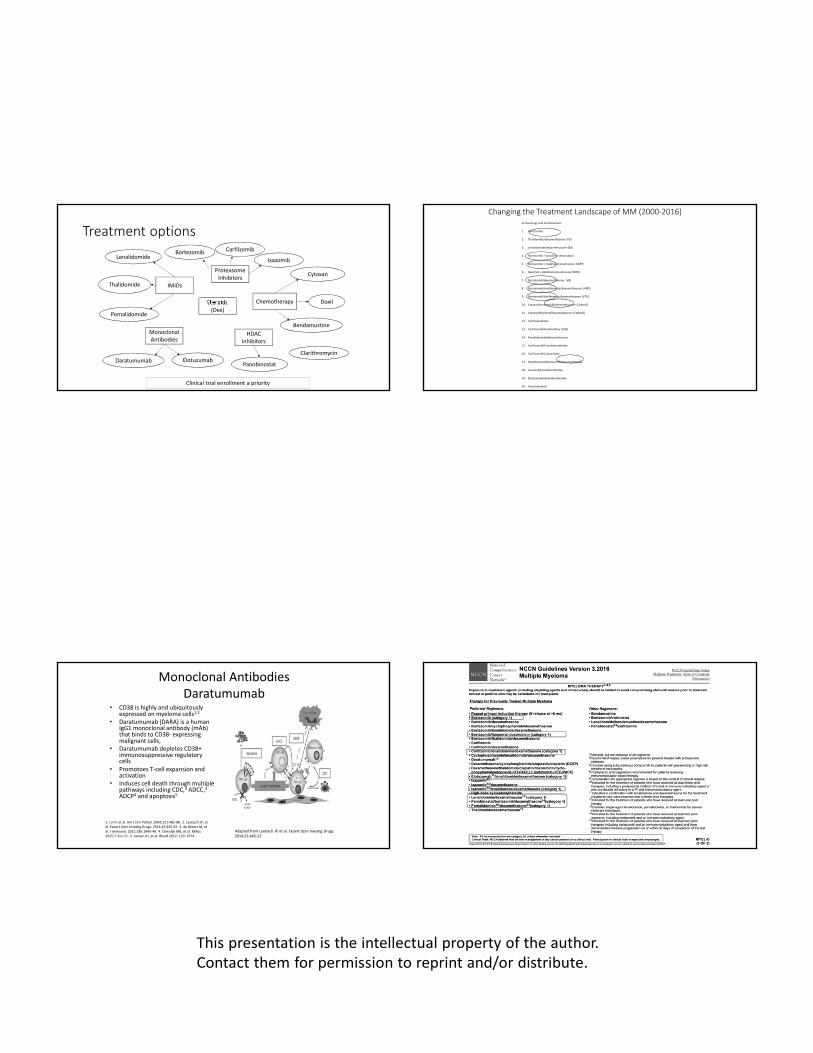
Targets for Monoclonal Antibodies in MM
CD229
CD200
CD28
CD19
BCMA
CD317
CD70
β2M
CD
74
PD
-1
CD
138
ICA
M-1
CD
38
CD
40
CD
56
CX
CR
4
SL
AM
F7
IL-6
BAFF
APRIL
In clinical development
Preclinical activity
Potential targets
Siltuximab
Tabalumab
Mila
tuzu
mab
Pem
brol
izum
abN
ivol
umab
Pid
ilizu
mab
Inda
tuxi
mab
Rav
tans
ine
BI-
50
5
Dar
atum
umab
Isat
uxim
abM
OR
202
Elo
tuzu
mab
Luca
tum
umab
Dac
etuz
umab
Lorv
otuz
umab
Ulo
cupl
umab
Lonial S. ASCO 2016. New Drugs in Oncology: Ixazomib, Elotuzumab, and Daratumumab in Myeloma
Approved agents
MM Cell

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Daratumumab: Mechanism of Action
Anti-CD38 IgGκ monoclonal antibody
Direct and indirect antimyeloma activity[1-5]
Depletes CD38+ immunosuppressive regulatory cells[5]
Promotes T-cell expansion and activation[5]
1. Lammerts van Bueren J, et al. ASH 2014. Abstract 3474.2. Jansen JMH, et al. Blood. ASH 2012. Abstract 2974.3. de Weers M, et al. J Immunol. 2011;186:1840-1848.4. Overdijk MB, et al. MAbs. 2015;7:311-321.5. Krejcik J, et al. Blood. 2016;[Epub ahead of print].
Sanchez L, et al. J Hematol Oncol. 2016;30:51.
Daratumumab
106 patients heavily pretreated myeloma patientsMedian time since diagnosis was 4.8. yearsMedian number of prior therapies was 597% of the patient’s refractory to their last line of therapy and 95% were double refractoryORR 29%; >VGPR 12%; PFS 3.7 months
Lonial S, et al. Lancet. 2016;387:1551-1660.Lonial S, et al. ASCO 2015. Abstract LBA8512.
Side effects
>90% of Infusion reactions occurred during the first infusion. Most common included nasal congestion (12%); throat irritation (7%); cough, dyspnea, chills, and vomiting (6%)
Lonial et. al. Lancet 2016 Jan 6. pii: S0140‐6736(15)01120‐4
Other grade ¾ AE included anemia 24%; thrombocytopenia 19%; neutropenia 12%
Daratumumab (infusion)
Schedule Weeks
Weekly Weeks 1 to 8
Every 2 weeks Weeks 9 to 24
Every 4 weeks Week 25 onwards until progression
Almost a third of the patients benefited from getting the drug It was reasonably well tolerated and has impressive single agent activity Responses were rapid, durable, and deepened over time
Lonial et. al. Lancet 2016 Jan 6. pii: S0140‐6736(15)01120‐4

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Daratumumab Combinations in Myeloma: ORR With Rd vs Pd
ORR in double-refractory patients: 67%
Clinical benefit rate (ORR + minimal response): 74%
Dara + Rd[1] Dara + Pd[2]
Clinical benefit rate (ORR + minimal response): 88%
1. Plesner T, et al. ASH 2015. Abstract 507.2. Chari A, et al. ASH 2015. Abstract 508.
100
80
60
40
20
0
OR
R (
%)
16 mg/kg
ORR: 81%
34%CR orbetter 63%
VGPR orbetter
sCR CR VGPR PR
19%
28%
9%
25%
100
80
60
40
20
0
OR
R (
%)
16 mg/kg
ORR: 71%
9%CR orbetter
43%VGPR or
better
sCR CR VGPR PR
28%
33%
4%5%
CASTOR: PFS With Addition of Daratumumab to Vd
Palumbo A, et al. ASCO 2016. Abstract LBA4. Reproduced with permission.
PF
S (
%)
0
20
40
60
80
100
0 3 6 9 12 15
Mos
1-yr PFS
60.7%
26.9%DVdVd
Median PFS, MosNR7.2HR: 0.39 (95% CI: 0.28-0.53; P < .0001)
POLLUX: PFS with Addition of Daratumumab to Rd
63% reduction in the risk of disease progression or death for DRd vs Rd
Dimopoulos M, et al. EHA 2016. Abstract LB238.
PF
S (
%)
0
20
40
60
80
100
0 3 6 9 12 15 18 21Mos
Rd
DRd
12-mo PFS*
83%
60%
18-mo PFS*
78%
52%
HR: 0.37 (95% CI: 0.27-0.52; P < .0001)
Median PFS: 18.4 mos
Daratumumab in R/R MM: MRD Negativity
Daratumumab + Rd or Vd significantly improved MRD negativity rate vs Rd or Vd alone
MRD-negative events accumulated rapidly and increased over time (within 3-18 mos)
Avet-Loiseau H, et al. ASH 2016. Abstract 246.
MRD Negative, %POLLUX (N = 286) CASTOR (N = 251)
Dara + Rd Rd P Value Dara + Vd Vd P Value
All pts 10-4
10-5
10-6
31.824.811.9
8.85.72.5
< .0001< .0001< .0001
18.310.44.4
3.62.40.8
< .0001< .005< .05
Patients with ≥ CR 10-4
10-5
10-6
655226
422713
< .005< .005< .05
603716
35229
< .05----
By cytogenetic risk High* Standard
1830
010
< .005< .0001
1412
02
< .005< .005
*Includes pts with t(4;14), t(14;16), or del(17p).

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Lower risk of progression in pts who achieve MRD negativity, regardless of therapy
– DRd MRD-negative pts (n = 71); estimated 12-mo PFS > 90%
– DVd MRD-negative pts (26); estimated 12-mo PFS > 90%
– Rd MRD-negative pts (n = 16 in POLLUX and n = 6 in CASTOR); estimated 12-mo PFS > 90%
Daratumumab + Rd or Vd shows PFS benefit in MRD-positive pts over doublets alone
– POLLUX: estimated median PFS NR vs 17 months for DRd MRD-positive (n = 215) vs Rd MRD-positive pts (n = 267)
– CASTOR: estimated median PFS NR vs 7 months for DVd MRD-positive (n = 225) vs Vd MRD-positive pts (n = 241)
Daratumumab in R/R MM: PFS
Avet-Loiseau H, et al. ASH 2016. Abstract 246.
Daratumumab
Anti‐CD38 mAb, approved as combination in patients that have received 1 prior line of therapy and as monotherapy who have had at least 3 prior lines of therapy containing a PI and an IMiD (or who are double refractory)
Intravenous infusion
Pre‐meds required
Interferes with RBC compatibility testing • Dithiothreitol (DTT) prevents this • Talk to blood bank
Subcutaneous daratumumab studies ongoing (prelim efficacy similar and no new safety signals)
Multiple ongoing studies in combinations
Panobinostat/bortezomib/dex Vs Bortezomib/dex
• Randomized, multicenter, placebo‐controlled, double‐blind phase III trial
Pts with symptomatic
RRMM after 1-3 prior treatments
(bortezomib-refractory excluded)(N = 768)
Panobinostat20 mg Days 1, 3, 5 of Wks 1, 2
Bortezomib1.3 mg/m2 IV Days 1, 4 of Wks 1, 2
Dexamethasone 20 mg Days 1, 2, 4, 5 of Wks 1, 2
(n = 387)
Placebo Days 1, 3, 5 of Wks 1,2
Bortezomib 1.3 mg/m2 IV Days 1, 4 of Wks 1, 2
Dexamethasone 20 mg Days 1, 2, 4, 5 of Wks 1, 2
(n = 381)
San-Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206.
Panobinostat 20 mg Days 1, 3, 5 of Wks 1, 2, 4, 5
Bortezomib 1.3 mg/m2 IV Day 1 of Wks 1, 2, 4, 5
Dexamethasone 20 mg Days 1, 2 of Wks 1, 2, 4, 5
Phase I: Eight 3-wk cycles Phase II: Four 6-wk cycles
Placebo Days 1,3,5 of Wks 1, 2, 4, 5
Bortezomib 1.3 mg/m2 IV Day 1 of Wks 1, 2, 4, 5
Dexamethasone 20 mg Day 1 of Wks 1, 2, 4, 5
≥ SD
≥ SD
Phase III PANORAMA-1 Trial: PFS, OS With Addition of Panobinostat to Vd
Primary endpoint reached: median PFS ↑ by 3.9 mos
Median OS ↑ by 4.5 mos: NS
1. San-Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206.2. San-Miguel JF, et al. ASH 2015. Abstract 3026.
100
80
60
40
20
0Pro
bab
ility
of
PF
S (
%)
0 4 8 12 16 20 24 28 32 36
Mos
Pan + Vd
Placebo + Vd
12.0 (10.3-12.9)
8.1 (7.6-9.2)
0.63(0.52-0.76)
< .0001
P ValueHR
(95% CI)Median PFS, Mos (95% CI)Arm
Pan + VdPlacebo + Vd
PFS[1]
Pro
bab
ility
of
OS
(%
)
Mos
0.94(0.78-1.14) .5435
P ValueHR
(95% CI)Median OS,
Mos (95% CI)Arm
40.3 (35.0-44.8)
35.8 (29.0-40.6)
OS[2]
100
80
60
40
20
0
Pan + VdPlacebo + Vd
0 8 16 24 32 40 48 56 64
Pan + Vd
Placebo + Vd

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Survival and Response ratesAE, %
Panobinostat
(n = 381)
Placebo
(n = 377)
Any grade 3/4 AE 96 82
Grade 3/4 nonhematologic AEs
Diarrhea 25 8
Asthenia or fatigue 24 12
Grade 3/4 hematologic AEs
Thrombocytopenia 68 31
Neutropenia 35 11
Serious AE 60 42
Discontinuation due to AE 24 12
Boxed Warning: increased risk of serious and potentially fatal diarrhea, cardiac ischemic events, and severe arrhythmiasApproved by the FDA for patients with MM who have received at least two prior therapies, including bortezomib and an immunomodulatory agent
San-Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206.
New Novel Agents
Selinexor Mechanism of Action
XPO1 is the nuclear exporter for the majority of TSPs, the GR, and eIF4E-bound oncoprotein mRNAs
Selinexor is a first-in-class XPO1 inhibitor that induces nuclear retention and activation of TSPs and the GR in the presence of steroids and suppresses oncoprotein expression
CYTOSOL
NUCLEUS
Nuclear pore complex
Nuclear envelope Tumor
suppressors
SINE
XPO1
Tumor suppressors
p53Par-4PP2ApRB
p21IkBBRACA1p27
eIF4E
XPO1
Tumor suppressors
Vogl DT, et al. ASH 2016. Abstract 491. Reproduced with permission.
STORM (Selinexor Treatment of Refractory Myeloma): Study Design
Phase II clinical trial: selinexor plus low-dose dexamethasone for heavily pretreated patients with MM refractory to most recent treatment (N = 79; median age: 68 yrs)
– Quad: refractory to bortezomib, carfilzomib, lenalidomide, and pomalidomide
– Penta: quad refractory and also daratumumab or isatuximab (anti-CD38 antibodies)
Treatment: selinexor 80 mg plus dexamethasone 20 mg twice weekly; reductions or interruption as needed for toxicity
– Group 1: 6 doses/28-day cycle (3 wks on/1 wk off)
– Group 2: 8 doses/28-day cycle (4 wks continuously)
Primary endpoints: ORR and DoR (IRC assessed)
Secondary endpoints: PFS and OS
Vogl DT, et al. ASH 2016. Abstract 491.

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
ORR: 21%CBR: 33%
515
13
35
12
21
417
8
44
8
19
713
20
20
17
23
614
10
41
8
22
419
19
22
19
19
STORM: Efficacy
Median time to response: 1 mo
Median DoR: 5 mos
Vogl DT, et al. ASH 2016. Abstract 491.
100
80
60
40
20
0Overall(n = 78)
Quad(n = 48)
Penta(n = 30)
6 Doses per mo(n = 51)
8 Doses per mo(n = 27)
VGPRPRMRSDPDNE
Pts
(%
)
ORR: 21%CBR: 29%
ORR: 20%CBR: 40%
ORR: 20%CBR: 29%
ORR: 22%CBR: 41%
ORR: 38%CBR: 63%
STORM: Responses by Cytogenetic Risk
Vogl DT, et al. ASH 2016. Abstract 491.
*1 pt with t(14;16) achieved PR; 1 pt with del(17p) and t(14;16) had PD (not included in graph).
514
23
50
9
6
29
18
35
12
13
25
25
25
13
50
50
33
67
100
80
60
40
20
0Standard
Risk(n = 22)
All High Risk*
(n = 17)
Del (17p)(n = 8)
t(4;14)(n = 4)
Del(17p) and
t(4;14) (n = 3)
VGPRPRMRSDPD
Pts
(%
)
ORR: 18%CBR: 41%
CBR: 33%
ORR: 35%CBR: 53%
ORR: 50%
STORM: OS and PFS
Median OS for all pts: 9.3 mos, ≥ MR: not reached
Median PFS for all pts: 2.3 mos, ≥ MR: 5.5 mos
OS and PFS: All Pts
OS (all)PFS (all)
N = 78Su
rviv
al (
%)
100
50
0200 5 10 15
Mos Following Initiation of Selinexor Treatment
OS and PFS: Pts with ≥ MR
OS ( ≥ MR)PFS ( ≥ MR)
N = 26Su
rviv
al (
%)
100
50
0200 5 10 15
Mos Following Initiation of Selinexor Treatment
Vogl DT, et al. ASH 2016. Abstract 491. Reproduced with permission.
Selinexor
Ongoing study with an expansion phase to include >100 penta-refractory patients
? Possibly the next agent to get approval

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Venetoclax Monotherapy for Relapsed/Refractory MM: Phase I Study Design
Pts with previously treated MM with measurable disease;
ECOG PS 0/1 and adequate organ function (N = 66)
Venetoclax 50 mg*Venetoclax 300 mg*Venetoclax 100 mg*
Venetoclax 100 mg*Venetoclax 600 mg*Venetoclax 300 mg*
Venetoclax 300 mg*Venetoclax 900 mg*Venetoclax 600 mg*
Venetoclax 400 mg*Venetoclax 1200 mg*Venetoclax 800 mg*
Venetoclax 400 mg*Venetoclax 1200 mg*Venetoclax 800 mg*
Accelerating lead-inTest dose cycle 1+
21 days/cycle
Kumar S, et al. ASH 2016. Abstract 488.
(Safety cohort; n = 36)
*Pts who progressed on venetoclax could add dexamethasone and continue on study.
(n = 9)
(n = 6)
(n = 9)
(n = 6)
Primary objectives: safety, tolerability, MTD, recommended phase 2 dose, PK
Secondary objectives: ORR, TTP, DoR, pharmacodynamics, predictive biomarker analysis
Venetoclax Monotherapy for Relapsed/Refractory MM: TTP and DoR
Kumar S, et al. ASH 2016. Abstract 488. Reproduced with permission.
No. at riskNo. at riskNo. at risk
663036
332013
27198
20173
16133
972
321
11
11
11
11
11
TTP
No
t P
rog
ress
ed (
%)
100
80
60
40
20
00 2 4 6 8 10 12 14 16 18 20 22 24
Mos Since First Dose
All ptst(11;14)Non-t(11;14)
No. at riskNo. at risk
915
911
911
98
95
62
3 2 2 2 2 1
TTP
No
t P
rog
ress
ed (
%)
100
80
60
40
20
00 2 4 6 8 10 12 14 16 18 20 22 24
Mos Since First Dose
High BCL2:BCL2L1Low BCL2:BCL2L1
Gene expression ratioamong t(11;14) pts
Pembrolizumab/Pomalidomide/Dexamethasone for R/R MM: Background PD-1/PD-L1 pathway blockade being exploited in several cancers to
restore cytotoxic T-cell activity and anticancer immunity[1]
Pembrolizumab: humanized anti–PD-1 monoclonal antibody
Pomalidomide: immunomodulatory thalidomide analogue indicated in combination with dexamethasone for pts with MM and ≥ 2 previous treatments including lenalidomide and a PI with progression ≤ 60 days of last regimen
Current study evaluates the safety and efficacy of pembrolizumab combined with pomalidomide and dexamethasone in pts with R/R MM[2]
1. Boussiotis VA. N Engl J Med. 2016;375:1767-1778. 2. Badros AZ, et al. ASH 2016. Abstract 490.
Pembrolizumab/Pomalidomide/Dexamethasone for R/R MM: Study Design Exploratory trial
Primary endpoint: safety
Secondary endpoints: ORR, PFS, OS
Exploratory endpoints: correlation of BL levels of PD-1 and PD-L1 in BM with response
Badros AZ, et al. ASH 2016. Abstract 490.
Pts with R/R MM and 2 lines of previous tx including IMiD and
PI; ECOG PS < 2 and adequate organ function;
no active autoimmune disease requiring treatment or history of
severe autoimmune disease(N = 48)
Pembrolizumab* 200 mg IV Days 1, 14 +Pomalidomide 4 mg PO Days 1-21 +
Dexamethasone 40 mg† PO Days 1, 7, 14, 21Q28D
Mo 24
Pembrolizumab 200 mg IV/mo +Pomalidomide 4 mg PO +
Dexamethasone 40 mg† PO
*First 6 pts received pembrolizumab on Day 1 only.
Responders
†Pts > 70 yrs of age received 20 mg.

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Pembrolizumab/Pomalidomide/Dexamethasone for R/R MM: Efficacy
Badros AZ, et al. ASH 2016. Abstract 490.
Response, % Full Efficacy Population
(N = 45)
Refractory to 2 Classes(n = 32)
High-Risk Cytogenetics
(n = 27)
ORR 65 68 56
Clinical benefit 72 69 60
Best response sCR CR VGPR PR MR SD PD
72
20367
235
33
18443
224
744
414
317
sCR + CR + VGPR, % 29 24 15
Pembrolizumab/Pomalidomide/Dexamethasone for R/R MM: Duration of Response and Survival
PFS significantly longer in low-risk vs high-risk subgroups (P = .0366)
Badros AZ, et al. ASH 2016. Abstract 490.
Outcome, Mos (95% CI) Full Efficacy Population(N = 45)
Median duration of response 16.3 (9.9-19.1)
Median PFS 17.4 (11.7-18.8)
Median OS Not reached (18.8-not reached)
The ‘Iceberg Hypothesis’ of multiple myeloma

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Multiple Myeloma Clinical Trials at CTRC
Relapsed/Refractory Multiple Myeloma• An Open-Label, Randomized Phase 3 Trial of
Combinations of Nivolumab, Elotuzumab, Pomalidomide and Dexamethasone in Relapsed and Refractory Multiple Myeloma
• ACY-241: A selective oral HDAC6 inhibitor given with Pomalidomide and dexamethasone. All oral regimen.
Untreated Multiple Myeloma • Phase III trial Daratumumab in combination with
Revlimid/dexamethasone vs. Revlimid/ dexamethasone.
• E1A11 Endurance (VRd vs CRd) – A study comparing VRd vs. CRd followed by lenalidomidemaintenance for up to 24 cycles or until progressive disease or excessive toxicities in newly diagnosed MM of standard risk
Thank you for your attention!
ELOQUENT-2: Background
Elotuzumab: anti-SLAMF7 monoclonal antibody that acts via dual mechanism
– Directly activates natural killer cells
– Myeloma cell destruction by ADCC
In primary study analysis, elotuzumab + len/dex reduced risk of progression or death by 30% vs len/dex[1]
Elotuzumab approved November 30, 2015, for use with len/dex in pts with MM and 1-3 prior therapies[2]
Current analysis presents extended 3-yr safety and efficacy follow-up[3]
1. Lonial S, et al. N Engl J Med. 2015;373:621-631. 2. FDA.gov. Accessed December 5, 2015. 3. Dimopoulos MA, et al. ASH 2015. Abstract 28.
ELOQUENT-2: Background
Elotuzumab: anti-SLAMF7 monoclonal antibody that acts via dual mechanism
– Directly activates natural killer cells
– Myeloma cell destruction by ADCC
In primary study analysis, elotuzumab + len/dex reduced risk of progression or death by 30% vs len/dex[1]
Elotuzumab approved November 30, 2015, for use with len/dex in pts with MM and 1-3 prior therapies[2]
Current analysis presents extended 3-yr safety and efficacy follow-up[3]
1. Lonial S, et al. N Engl J Med. 2015;373:621-631. 2. FDA.gov. Accessed December 5, 2015. 3. Dimopoulos MA, et al. ASH 2015. Abstract 28.

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Bahlis NJ Blood 2012;120(5);927-928
Myeloma evolution and alternating clonal dominanceClonal heterogeneity
Keats JJ et. Al. Blood 2012;120(5);1067-76
How close is a cure?
MRD
Attal M, et al. ASH 2015. Abstract 391. Slide credit: clinicaloptions.com
IFM 2009: OS
Pts (%)
Follow‐up (Mos)
ASCTNo ASCT
100
80
60
40
20
00 12 24 36 48
P = NS
350350
328338
309320
226244
5556
Pts at Risk, nASCT
No ASCT

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Retreatment with Immunomodulatory drugs
Madan et. al. Blood 2011 Aug 18;118(7):1763-5
Len
LenN=48
Thal
LenN=58
Len
ThalN=11
Thal
ThalN=23
>Partial Response
54% 48% 20% 30%
Retrospective study in 140 patients treated with first line Len/dex (59; 42%) or Thal/dex (81; 58%)Retreatment with a regimen containing Lenalidomide (76%) and Thalidomide (24%)# of treatments before retreatment – median 2 (range 1‐6)Median time from diagnosis to repeat exposure was 28 months
Overall Survival has Improved in the Past Decade
<65 yrs >65 yrs
2006‐2010 73 56
2001‐2005 63 31
6 yr survival, %age
Meta‐analysis of 5 RCT (PANORAMA‐1, MMVAR, ASPIRE, ELOQUENT‐2, TOURMALINE‐MM1)
Nooka et. al. ASCO 2016 oral abstract

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Aim of treatment is to prevent organ damage and it’s complications
Courtesy Rafael Fonseca MD
High Calcium, Renal (kidney) failure, Anemia, Bone lesions
‘CRAB’ criteria
IMWG ultra high‐risk that is now MM
GEM SMM trial ‘high‐
risk’
Low risk smoldering myeloma
(MGUS like)
Improved PFS and OS with Novel agents (thalidomide, lenalidomide, bortezomib) compared to conventional chemotherapy and improvement with maintenance
Old Regimen New regimen with novel agents
ORR 50‐60 80‐100
CR 16‐25 40‐60
VGPR 5‐10 20‐30
PFS 15 months 25‐30 mos (improved to >48 months with maintenance)
5 year OS 30‐35 50‐70
• Palumbo et al Lancet, 2006; Mateos Blood 2010; McCarthy NEJM 2012; Attal NEJM, 2012

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Natural history of myeloma: the cycle of response, remission and relapse
Response
RemissionRelapse
Durie B; concise review of the disease and treatment options 2011/2012
What does relapsed, refractory mean?
• Relapsed and Refractory: progressing on therapy or within 60 days of last therapy
• Relapsed: progressing while off therapy
• How do we define disease progression?
‐ 25% increase from nadir in the monoclonal protein
‐ New bone abnormalities
‐ High calcium
‐ Kidney failure
‐Worsening blood counts (anemia)
Bahlis NJ Blood 2012;120(5);927-928
Patterns of Relapse
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Treatment options
Steroids(Dex)
Chemotherapy
IMiDs
ProteasomeInhibitors
Monoclonal Antibodies
Lenalidomide
Bendamustine
Pomalidomide
Thalidomide
Cytoxan
ElotuzumabDaratumumab
Bortezomib Carfilzomib
Ixazomib
HDAC inhibitors
Panobinostat
Clarithromycin
Clinical trial enrollment a priority
Doxil
Changing the Treatment Landscape of MM (2000‐2016)Active Drugs and Combinations
1. Bortezomib
2. Thalidomide/dexamethasone (TD)
3. Lenalidomide/dexamethasone (Rd)
4. Bortezomib + liposomal doxorubicin
5. Bortezomib + melphalan/prednisone (VMP)
6. Revlimid + Melphalan/prednisone (MPR)
7. Bortezomib/dexamethasone (Vd)
8. Bortezomib/lenalidomide/dexamethasone (VRD)
9. Bortezomib/thalidomide/dexamethasone (VTD)
10. Cytoxan/bortezomib/dexamethasone (CyBorD)
11. Cytoxan/Revlimid/Dexamethasone (CyRevD)
12. Carfilzomib/Dex
13. Carfilzomib/Revlimid/dex (KRd)
14. Pomalidomide/dexamethasone
15. Carfilzomib/Pomalidomide/dex
16. Carfilzomib/Cytoxan/dex
17. Panobinostat/bortezomib/dexamethasone
18. Ixazomib/lenalidomide/dex
19. Elotuzumab/lenalidomide/dex
20. Daratumumab
Monoclonal AntibodiesDaratumumab
• CD38 is highly and ubiquitously expressed on myeloma cells1,2
• Daratumumab (DARA) is a human IgG1 monoclonal antibody (mAb) that binds to CD38‐ expressing malignant cells,
• Daratumumab depletes CD38+ immunosuppressive regulatory cells
• Promotoes T‐cell expansion and activation
• Induces cell death through multiple pathways including CDC,3 ADCC,3
ADCP4 and apoptosis5
1. Lin P, et al. Am J Clin Pathol. 2004;121:482‐88. 2. Laubach JP, et al. Expert Opin Investig Drugs. 2014;23:445‐52. 3. de Weers M, et al. J Immunol. 2011;186:1840‐48. 4. Overdijk MB, et al. MAbs. 2015;7:311‐21. 5. Jansen JH, et al. Blood.2012; 120. 2974
Adapted from Laubach JP, et al. Expert Opin Investig Drugs. 2014;23:445‐52

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Dual mechanism of action of Elotuzumab
• Elotuzumab is a first‐in‐class humanized immunoglobulin G1 immunostimulatorymonoclonal antibody
• It targets signaling lymphocytic activation molecule F7 (SLAMF7, also called CS1, a glycoprotein expressed on myeloma and natural killer cells)
• It causes myeloma cell death via dual mechanism (NK cell activation and Tagging for Recognition)
Lonial et. al. N Engl J Med 2015; 373:621‐631
CASTOR: Study Design
Presented By Antonio Palumbo at 2016 ASCO Annual Meeting
Progression-free Survival
Presented By Antonio Palumbo at 2016 ASCO Annual Meeting
PFS: Subgroup Analysis
Presented By Antonio Palumbo at 2016 ASCO Annual Meeting

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Where do we go from here?
Presented By Rafael Fonseca at 2016 ASCO Annual Meeting
Basic principles of selecting a treatment
Use new agent: Use drugs the patient has not received before
Using same drug in a different combination
Using another drug in the same class: patients progressing on thalidomide may respond to lenalidomide; those progressing on lenalidomide may respond to pomalidomide; those progressing on bortezomib may respond to carfilzomib
Increase dose: Patients progressing on lenalidomide at 10 mg may respond when dose is increased to 25 mg plus dexamethasone or addition of cyclophosphamide
Adding clarithromycin to lenalidomide, thalidomide or pomalidomide can be used to achieve a response
Richardson PG, et al. Blood. 2014;123:1461-1469 Berenson et. al. Leukemia (2014) 28, 1529–1536.
Nijhof IS, et al. ASH 2013. Abstract 287. Richardson P, et al. Blood. 2009;114-772-778.
• Calcium elevation (> 11.5 mg/L or ULN)
• Renal dysfunction, (serum creatinine >2 mg/dL)
• Anemia (Hb < 10 g/dL or 2g <normal)
• Bone disease (lytic lesions or osteoporosis)
Retreatment with Immunomodulatory drugs
Madan et. al. Blood 2011 Aug 18;118(7):1763-5
Len
LenN=48
Thal
LenN=58
Len
ThalN=11
Thal
ThalN=23
>Partial Response
54% 48% 20% 30%
Retrospective study in 140 patients treated with first line Len/dex (59; 42%) or Thal/dex (81; 58%)Retreatment with a regimen containing Lenalidomide (76%) and Thalidomide (24%)# of treatments before retreatment – median 2 (range 1‐6)Median time from diagnosis to repeat exposure was 28 months

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
What is new?
4 new drugs approved by the FDA in 2015 for relapsed myeloma
Panobinostat (Oral)
Ixazomib (Oral)
Daratumumab (IV)
Elotuzumab (IV)
Major drug categoriesImmunomodulatory drugs (IMiDs)
Proteasome Inhibitors (PI)
Steroids
Monoclonal Antibody (MoAb)
HDAC inhibitors
Conventional Chemotherapy
Treatment options in relapsed myeloma
Steroids(Dex)
Chemotherapy
IMiDs
ProteasomeInhibitors
Monoclonal Antibodies
Lenalidomide
Bendamustine
Pomalidomide
Thalidomide
Cytoxan
ElotuzumabDaratumumab
Bortezomib Carfilzomib
Ixazomib
HDAC inhibitors
Panobinostat
Clarithromycin
Clinical trial enrollment a priority
Doxil
3 vs 2 drugs in relapsed myeloma
Drug Class Study arm Control arm
Carfilzomib (27 mg/m2)
Proteasome Inhibitor Carfilzomib/lenalidomide/dex Lenalidomide/dex
Ixazomib Proteasome Inhibitor Ixazomib/lenalidomide/dex Lenalidomide/dex
Elotuzumab Monoclonal Antibody Elotuzumab/lenalidomide/dex Lenalidomide/dex
Panobinostat HDAC inhibitor Panobinostat/bortezomib/dex Bortezomib/dex

This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
Natural history of myeloma: the cycle of response, remission and relapse
Response
RemissionRelapse
Durie B; concise review of the disease and treatment options 2011/2012