multi-site diagnosis and management of 260 patients with...
TRANSCRIPT

Original Article
International Journal of Audiology 2010; 49: 30–43
ISSN 1499-2027 print/ISSN 1708-8186 onlineDOI: 10.3109/14992020903160892© 2010 British Society of Audiology, International Society of Audiology, and Nordic Audiological Socie
Multi-site diagnosis and management of
260 patients with Auditory Neuropathy/
Dys-synchrony (Auditory Neuropathy
Spectrum Disorder *)
Charles I. Berlin1,2
Linda J. Hood1,3, Thierry Morlet1,4, Diane Wilensky1,5
Li Li1,5, Kelly Rose Mattingly1
Jennifer Taylor-Jeanfreau1,6
Bronya J.B. Keats1,8, Patti St. John5, Elizabeth Montgomery5
Jon K. Shallop7, Benjamin A. Russell2, Stefan A. Frisch2
1Formerly at Kresge Hearing Research Laboratory, LSUHSC, New Orleans, Louisiana, USA; 2University of South Florida, Tampa, Florida, USA; 3Vander-bilt University, Nashville, Tennessee, USA; 4duPont Hospital for Children, Wilmington, Delaware, USA; 5LouisianaState University Health Sciences Center, New Orleans, Louisiana, USA; 6NewOrleans Speech and Hearing Center, New Orleans, Louisiana, USA; 7MayoClinic, Rochester, Minnesota, USA; 8Australian National University, Canberra ACT, Australia
Key WordsAuditory neuropathyAuditory dys-synchronyAuditory neuropathy spectrum disorderDiagnosis, managementAuditory brainstem responseCochlear microphonicsOtoacoustic emissionsHearing aidsCochlear implantsCued speechMiddle-ear muscle refl exes
AbbreviationsABR: Auditory brainstem responseAN/AD: Auditory Neuropathy/
Dys-synchronyANSD: Auditory Neuropathy
Spectrum DisorderAVT: Auditory Verbal TherapyCI: Cochlear implantCM: Cochlear microphonicECochG: ElectrocochleographyMEMR: Middle-ear muscle refl exOAE: Otoacoustic emissions
*At the Consensus Conference on Auditory Neuropsponsored by the Bill Daniels Hearing and Speech Ce
Abstract Test results and management data are summarized for 260 patients with diagnoses of Auditory Neuropathy Spectrum Disorder (ANSD). Hearing aids were tried in 85 of these patients, and 49 patients tried cochlear implants. Approxi-mately 15% reported some benefi t from hearing aids forlanguage learning, while improvement in speech comprehen-sion and language acquisition was reported in 85% of patients who were implanted. Approximately 5% (13/260) of thetotal population developed normal speech and languagewithout intervention. Patients were diagnosed at our labo-ratory (n � 66) or referred from other sites (n � 194), and all showed absent/grossly abnormal auditory brainstem responses (ABR), often ‘ringing’ cochlear microphonics, and the presence or history of otoacoustic emissions. Etiologies and co-existing conditions included genetic (n � 41), periph-eral neuropathies (n � 20), perinatal jaundice and/or anoxia and/or prematurity (n � 74). These patients comprise 10% or more of hearing impaired patients; their language acquisi-tion trajectories are generally unpredictable from their audio-grams.
Charles I. BerlinDepartment of Otolaryngand Disorders University4202 E. Fowler Avenue, E-Mail: [email protected].
Received:July 2, 2009Accepted:July 3, 2009ty
athy/Dys-synchrony coordinated by Drs. Yvonne Sininger and nter, this nomenclature was recommended by the clinical review
SumarioSe resumen los resultados de las pruebas y los datos del tratamiento de 260 pacientes con diagnóstico de Espectro de desórdenes de la Neuropatía Auditiva (ANSD). En 85 de estos pacientes se probó el uso de auxiliares auditivos y 49 pacientes recibieron un implante coclear. Aproximadamente 15% report-aron algún benefi cio con los auxiliares auditivos para la adqui-sición del lenguaje mientras que el 85% de los que recibieron un implante reportaron una mejoría en la comprensión y la adquisición del lenguaje. Aproximadamente 5% (13/260) de la población total desarrolló lenguaje normal sin intervención. Los paciente fueron diagnosticados en nuestro laboratorio (n=66) o referidos de algún otro lado (n=194) y todos mos-traron ausencia o anormalidad importante de los potenciales evocados (ABR), frecuentemente con una microfónica coclear “timbrante” y con presencia o historia de emisiones otoacús-ticas. La etiología o las condiciones co-existentes incluidas fueron: genéticas (n=41), neuropatías periféricas (n=20), icteri-cia perinatal y/o anoxia y/o prematurez (n=74). Estos pacientes representan 10% o más de los pacientes con hipoacusia; su trayectoria en el proceso de adquisición del lenguaje es gen-eralmente impredecible a partir de sus audiogramas.
ology Head and Neck Surgery and communication Sciences of South Florida,PCD1017 Tampa, FL 33620-8200, USA.edu
Deborah Hayes (NHS, Como, Italy, June 19–21, 2008), and panel.

Introduction, Historical and Theoretical Issues
Auditory neuropathy spectrum disorder (ANSD; see terminologydiscussion in Berlin et al, 2001a, 2001b; Kraus et al, 2000; Rapin & Gravel, 2006) describes a condition in which a patient’s otoacoustic emissions (OAE) are (or were at one time) present, and auditory brain-stem responses (ABR) are abnormal or absent. In some instances, ANSD is identifi ed on the basis of present cochlear microphonics (CM) and abnormal or absent ABRs (e.g. Berlin et al, 1993 ; Starr et al, 1996 ; Deltenre et al, 1999 ; Rance et al, 1999 ) with or without abnormalities of OAEs. The patient’s pure-tone audiogram, if it can be acquired reliably, may range anywhere from essentially normal hearing sensitivity to a profound hearing loss. Speech recognition ability is generally poor, particularly in noise, although it may be good in quiet in some patients ( Rance et al, 2007 ). In addition, fl uctuant listening abilities have been reported, some associated with body temperature and others with no clear precipitant ( Starr et al, 1998 ; Berlin et al, 1999 ). Prevalence accounts vary from roughly 1% ( Foerst et al, 2006 ) to 10% in schools for the deaf ( Berlin et al, 2000 ; Lee et al, 2001 ; Cheng et al, 2005 ) and between 10% in newborns ( Sininger, 2002 ) and 40% in hearing-impaired NICU graduates ( Rea & Gibson, 2003 ).
Probably the fi rst audiological reports of ANSD came from Hinch-cliffe et al (1972) well before OAEs ( Kemp, 1978 ) were reported. Subsequent suspicions were raised by Chisin et al (1979) , Worthing-ton and Peters (1980) , Cacace et al (1983 ), Kraus et al (1984) , Prieve et al (1991 ), Berlin et al (1993 ), and (Kaga et al (1996 ). We ( Starr , Picton , Sininger , Hood & Berlin, 1996 ) labeled this disorder as ‘audi-tory neuropathy’ after collectively reviewing our fi rst 10 patients who shared a set of unique auditory problems. One had absent compound action potentials (CAP) during transtympanic electrocochleography (ECochG) recording (found by Berlin and Hood) and the others had concurrent peripheral neuropathies, which were agreed upon by the two attending neurologists (Starr and Picton). It has been suggested subsequently that the term ‘neuropathy’ presumes data that we do not always have (Berlin et al, 2003; Moser et al, 2006; Rapin & Gravel, 2006) and should be avoided or at least semantically indexed ( Korzyb-ski, 1958 2 ) to allow for the inclusion of inner hair cell losses, as suggested by Amatuzzi et al (2001 ) and Varga et al (2003 ), or inner hair cell synaptic disorder Santarelli and Arslan, 2002 ; Moser et al, 2006 ; McMahon et al, 2008 ). At the same time, we must also recog-nize the ‘neuropathy’ part of this descriptor and collaborate with our neurology and genetics colleagues to identify and categorize the peripheral neuropathies that have been reported in over one-third of our patients. These neuropathies include absent VIIIth nerves ( Buch-man et al, 2006 ), Charcot-Marie-Tooth Disease, and Mohr-Traneb-jaerg syndrome ( Starr et al, 1996 ; Merchant et al, 2001 ) as well as mitochondrial diseases ( Corley & Crabbe, 1999 ; Cerani c & Luxon, 2004 ; Forli et al, 2006 ). Additionally, Delmaghani et al (2006) reported mutations in the pejvakin gene in individuals described as having nonsyndromic deafness due to a neuronal defect.
Thus, ANSD may be part of a continuum in which a mosaic of present and functioning inner and outer hair cells and pre- and
260 patients with ANSD
2Korzybski’s work on semantic indexing teaches that the labels which we use affect our actions. Thus calling this a “neuropathy” may misguide us into believing that the neurons are irreparably damaged or unavailable, and block us from even considering implantation. Hence our suggestion (Berlin et al., 2003) that the term “dys-synchrony” be added to “index” the basic term of “neuropathy” and remind us that, if this might also be “dys-synchrony”, implantation is likely to be useful. McMahon et al (2008) and Santarelli et al (2008) later showed physiologically that this is a valid construct, when they separated pre-synaptic from post-synaptic pathology using ECochG.
post-ganglionic single units of the auditory nerve may lead to various combinations of temporal disruption ( Berlin et al, 1993 ; Zeng et al, 1999 , 2005 ; Starr et al, 2000 , 2008 ; Amatuzzi et al, 2001 ; Varga et al, 2003 ; Rance et al, 2004 ; McMahon et al, 2008 ). In addition, ANSD patients may differ greatly from one another in their ability to use temporal cues. These factors affect both the methods utilized in evaluation and the issues that must be considered in recommend-ing management for both the patient and family. They also underlie our motivation for this retrospective review of how patients have been treated in the fi eld so far. This paper is written from the his-torical perspective of the fi rst author (CIB) who saw the fi rst patient in our series in the early 1980s.
Methods
The database at the core of this report is composed of material from patients evaluated at the Kresge Hearing Research Laboratory and the associated Audiology Clinics at LSU Health Sciences Center (n � 66)and data submitted by professional colleagues (n � 194). No data were submitted or accepted directly from patients without confi rmation and clearance from their professional referring agents. Compilation of this database began in 1982 with our fi rst patient and became systematized in 1994 after our fi rst public reports ( Berlin et al, 1993 ). The 260 patients included in this database met strict diagnostic criteria based on acquired copies of the ABR and OAE tracings, which were suf-fi ciently valid to confi rm a diagnosis of ANSD. The criteria at the time required a de-synchronized or absent ABR, in the presence of (or one time history of) normal otoacoustic emissions. We would now add elevated or absent middle-ear muscle refl exes, which are incon-gruent with normal emissions. In order to be included in this database, the test data, including tracings of all OAEs, CMs, and ABRs, were reviewed, and categorization was agreed upon by a team of four of the author-audiologists and researchers who had studied ANSD patients for fi ve or more years (CIB, LJH, TM, and DW). In order to acquire these 260 patients, more than 300 patient fi les were reviewed. Patients who may actually have had ANSD were excluded where there was insuffi cient corroborating evidence, for example, just a narrative from others of normal OAEs and/or an abnormal ABR with no trac-ings. We also excluded patients with a diagnosis of Friedreich’s Ataxia (FA) because all of our FA patients had a robust Wave I and normal middle-ear refl exes. This suggested to us that their abnormal ABRs were more traceable to brainstem anomalies than to primary auditory nerve or inner hair cell disorders. Other respected colleagues (e.g. ( Cacace et al, 1983; Miyamoto et al 1999 ; Rance et al, 2008 ) have categorized and treated some FA patients as having ANSD. We remain uncertain in part because of the presence of middle-ear muscle refl exes in our patients and the report of the failure of CI in one FA patient ( Miyamoto et al, 1999 ).
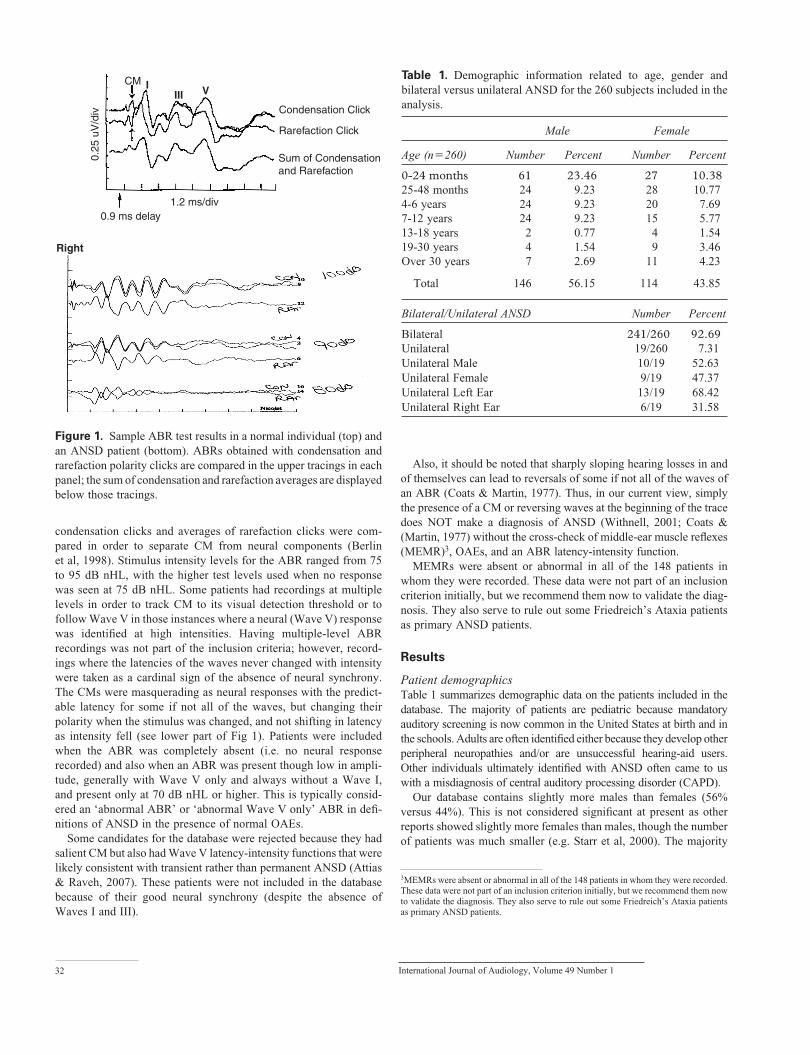
A sample of data from an ANSD patient, which qualifi ed this patient for inclusion in the database, is shown in Figure 1 (bottom). Note the long ringing CM, which could easily masquerade as a nor-mal ABR until or unless tracings to stimuli with polarity reversal were compared. This is contrasted with an ABR from a normal indi-vidual shown in the top portion of Figure 1 .
OAE data were either transient evoked OAEs (TEOAEs) collected using default test levels and procedures (80 dB peak SPL, non-linear clicks) or distortion product OAEs (DPOAE) typically collected using stimulus levels of L1 � 65/L2� 55 dB SPL. ABRs were obtained using click stimuli, where replicated averages of
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
31
Condensation Click
Rarefaction Click
Sum of Condensationand Rarefaction
1.2 ms/div
CMIII VI
0.9 ms delay
Right
0.25
uV
/div
Table 1. Demographic information related to age, gender and bilateral versus unilateral ANSD for the 260 subjects included in the analysis.
Male Female
Age (n � 260) Number Percent Number Percent
0-24 months 61 23.46 27 10.3825-48 months 24 9.23 28 10.774-6 years 24 9.23 20 7.697-12 years 24 9.23 15 5.7713-18 years 2 0.77 4 1.5419-30 years 4 1.54 9 3.46Over 30 years 7 2.69 11 4.23
Total 146 56.15 114 43.85
Bilateral/Unilateral ANSD Number Percent
Bilateral 241/260 92.69Unilateral 19/260 7.31Unilateral Male 10/19 52.63Unilateral Female 9/19 47.37Unilateral Left Ear 13/19 68.42Unilateral Right Ear 6/19 31.58
3MEMRs were absent or abnormal in all of the 148 patients in whom they were recorded. These data were not part of an inclusion criterion initially, but we recommend them now to validate the diagnosis. They also serve to rule out some Friedreich’s Ataxia patients
condensation clicks and averages of rarefaction clicks were com-pared in order to separate CM from neural components ( Berlin et al, 1998 ). Stimulus intensity levels for the ABR ranged from 75 to 95 dB nHL, with the higher test levels used when no response was seen at 75 dB nHL. Some patients had recordings at multiple levels in order to track CM to its visual detection threshold or to follow Wave V in those instances where a neural (Wave V) response was identifi ed at high intensities. Having multiple-level ABR recordings was not part of the inclusion criteria; however, record-ings where the latencies of the waves never changed with intensity were taken as a cardinal sign of the absence of neural synchrony. The CMs were masquerading as neural responses with the predict-able latency for some if not all of the waves, but changing their polarity when the stimulus was changed, and not shifting in latency as intensity fell (see lower part of Fig 1). Patients were included when the ABR was completely absent (i.e. no neural response recorded) and also when an ABR was present though low in ampli-tude, generally with Wave V only and always without a Wave I, and present only at 70 dB nHL or higher. This is typically consid-ered an ‘abnormal ABR’ or ‘abnormal Wave V only’ ABR in defi -nitions of ANSD in the presence of normal OAEs.
Some candidates for the database were rejected because they had salient CM but also had Wave V latency-intensity functions that were likely consistent with transient rather than permanent ANSD ( Attias & Raveh, 2007 ). These patients were not included in the database because of their good neural synchrony (despite the absence of
32 I
Waves I and III).
Also, it should be noted that sharply sloping hearing losses in and of themselves can lead to reversals of some if not all of the waves of an ABR ( Coats & Martin, 1977 ). Thus, in our current view, simply the presence of a CM or reversing waves at the beginning of the trace does NOT make a diagnosis of ANSD ( Withnell, 2001 ; Coats & ( Martin, 1977 ) without the cross-check of middle-ear muscle refl exes (MEMR)3 , OAEs, and an ABR latency-intensity function.
MEMRs were absent or abnormal in all of the 148 patients in whom they were recorded. These data were not part of an inclusion criterion initially, but we recommend them now to validate the diag-nosis. They also serve to rule out some Friedreich’s Ataxia patients as primary ANSD patients.
Results
Patient demographics Table 1 summarizes demographic data on the patients included in the database. The majority of patients are pediatric because mandatory auditory screening is now common in the United States at birth and in the schools. Adults are often identifi ed either because they develop other peripheral neuropathies and/or are unsuccessful hearing-aid users. Other individuals ultimately identifi ed with ANSD often came to us with a misdiagnosis of central auditory processing disorder (CAPD).
Our database contains slightly more males than females (56% versus 44%). This is not considered signifi cant at present as other reports showed slightly more females than males, though the number of patients was much smaller (e.g. Starr et al, 2000 ). The majority
Figure 1. Sample ABR test results in a normal individual (top) and an ANSD patient (bottom). ABRs obtained with condensation and rarefaction polarity clicks are compared in the upper tracings in each panel; the sum of condensation and rarefaction averages are displayed below those tracings.
nternational Journal of Audiology, Volume 49 Number 1
as primary ANSD patients.
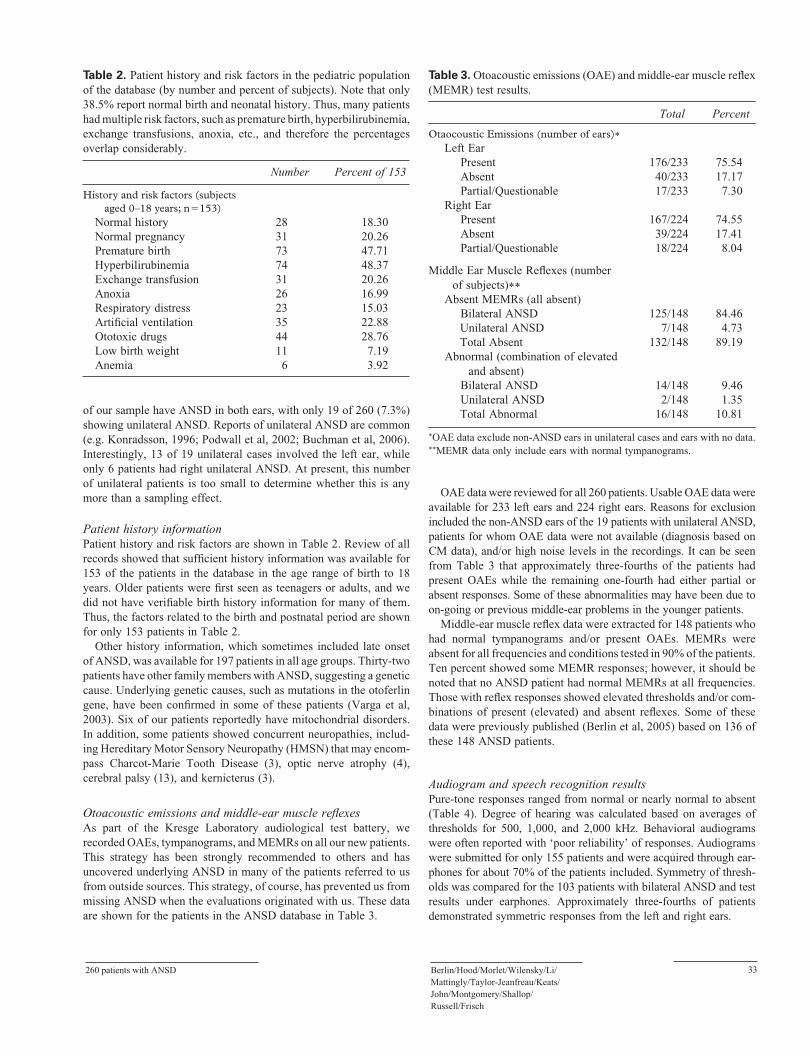
Table 2. Patient history and risk factors in the pediatric population of the database (by number and percent of subjects). Note that only 38.5% report normal birth and neonatal history. Thus, many patients had multiple risk factors, such as premature birth, hyperbilirubinemia, exchange transfusions, anoxia, etc., and therefore the percentages overlap considerably.
Number Percent of 153
History and risk factors (subjects aged 0–18 years; n � 153)
Normal history 28 18.30Normal pregnancy 31 20.26Premature birth 73 47.71Hyperbilirubinemia 74 48.37Exchange transfusion 31 20.26Anoxia 26 16.99Respiratory distress 23 15.03Artifi cial ventilation 35 22.88Ototoxic drugs 44 28.76Low birth weight 11 7.19Anemia 6 3.92
Table 3. Otoacoustic emissions (OAE) and middle-ear muscle refl ex (MEMR) test results.
Total Percent
Otaocoustic Emissions (number of ears)Left Ear
Present 176/233 75.54Absent 40/233 17.17Partial/Questionable 17/233 7.30
Right EarPresent 167/224 74.55Absent 39/224 17.41Partial/Questionable 18/224 8.04
Middle Ear Muscle Refl exes (number of subjects)
Absent MEMRs (all absent)Bilateral ANSD 125/148 84.46
Unilateral ANSD 7/148 4.73 Total Absent 132/148 89.19Abnormal (combination of elevated and absent)
Bilateral ANSD 14/148 9.46Unilateral ANSD 2/148 1.35
Total Abnormal 16/148 10.81
OAE data exclude non-ANSD ears in unilateral cases and ears with no data. MEMR data only include ears with normal tympanograms.
of our sample have ANSD in both ears, with only 19 of 260 (7.3%) showing unilateral ANSD. Reports of unilateral ANSD are common (e.g. Konradsson, 1996; Podwall et al, 2002; Buchman et al, 2006). Interestingly, 13 of 19 unilateral cases involved the left ear, while only 6 patients had right unilateral ANSD. At present, this number of unilateral patients is too small to determine whether this is any more than a sampling effect.
Patient history information Patient history and risk factors are shown in Table 2 . Review of all records showed that suffi cient history information was available for 153 of the patients in the database in the age range of birth to 18 years. Older patients were fi rst seen as teenagers or adults, and we did not have verifi able birth history information for many of them. Thus, the factors related to the birth and postnatal period are shown for only 153 patients in Table 2 .
Other history information, which sometimes included late onset of ANSD, was available for 197 patients in all age groups. Thirty-two patients have other family members with ANSD, suggesting a genetic cause. Underlying genetic causes, such as mutations in the otoferlin gene, have been confi rmed in some of these patients ( Varga et al, 2003 ). Six of our patients reportedly have mitochondrial disorders. In addition, some patients showed concurrent neuropathies, includ-ing Hereditary Motor Sensory Neuropathy (HMSN) that may encom-pass Charcot-Marie Tooth Disease (3), optic nerve atrophy (4), cerebral palsy (13), and kernicterus (3).
Otoacoustic emissions and middle-ear muscle refl exes As part of the Kresge Laboratory audiological test battery, we recorded OAEs, tympanograms, and MEMRs on all our new patients. This strategy has been strongly recommended to others and has uncovered underlying ANSD in many of the patients referred to us from outside sources. This strategy, of course, has prevented us from missing ANSD when the evaluations originated with us. These data are shown for the patients in the ANSD database in Table 3 .
260 patients with ANSD
OAE data were reviewed for all 260 patients. Usable OAE data were available for 233 left ears and 224 right ears. Reasons for exclusion included the non-ANSD ears of the 19 patients with unilateral ANSD, patients for whom OAE data were not available (diagnosis based on CM data), and/or high noise levels in the recordings. It can be seen from Table 3 that approximately three-fourths of the patients had present OAEs while the remaining one-fourth had either partial or absent responses. Some of these abnormalities may have been due to on-going or previous middle-ear problems in the younger patients.
Middle-ear muscle refl ex data were extracted for 148 patients who had normal tympanograms and/or present OAEs. MEMRs were absent for all frequencies and conditions tested in 90% of the patients. Ten percent showed some MEMR responses; however, it should be noted that no ANSD patient had normal MEMRs at all frequencies. Those with refl ex responses showed elevated thresholds and/or com-binations of present (elevated) and absent refl exes. Some of these data were previously published ( Berlin et al, 2005 ) based on 136 of these 148 ANSD patients.
Audiogram and speech recognition results Pure-tone responses ranged from normal or nearly normal to absent ( Table 4 ). Degree of hearing was calculated based on averages of thresholds for 500, 1,000, and 2,000 kHz. Behavioral audiograms were often reported with ‘poor reliability’ of responses. Audiograms were submitted for only 155 patients and were acquired through ear-phones for about 70% of the patients included. Symmetry of thresh-olds was compared for the 103 patients with bilateral ANSD and test results under earphones. Approximately three-fourths of patients demonstrated symmetric responses from the left and right ears.
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
33

Table 4. Audiometric test results, based on data from 155 subjects. Degree of pure tone behavioral hearing loss is based on pure-tone averages for 500, 1,000 and 2,000 kHz.
Total Percent
Pure Tone Test Data (number of subjects)Bilateral ANSD—Left and Right EarsUnilateral ANSD—Left EarUnilateral ANSD—Right EarSound fi eld
103/155
6/1552/155
44/155
66.45
3.871.29
28.39
Left and Right Ear Symmetry (number of subjects)*
Symmetric ThresholdsAsymmetric Thresholds
79/10324/103
76.7023.30
Degree of Pure Tone Behavioral Hearing Loss (number of ears)**
Within Normal LimitsNormal-Moderate
8/2586/258
3.102.33
Mild 10/258 3.88Mild-Moderate 42/258 16.28Mild-SevereMild-ProfoundModerateModerate-SevereModerate-ProfoundSevereSevere-ProfoundProfound
19/2588/258
25/25837/25811/25816/25837/25839/258
7.363.109.69
14.344.266.20
14.3415.12
Based on bilateral ANSD subjects tested via earphones.Based on data from left ears, right ears and sound fi eld.
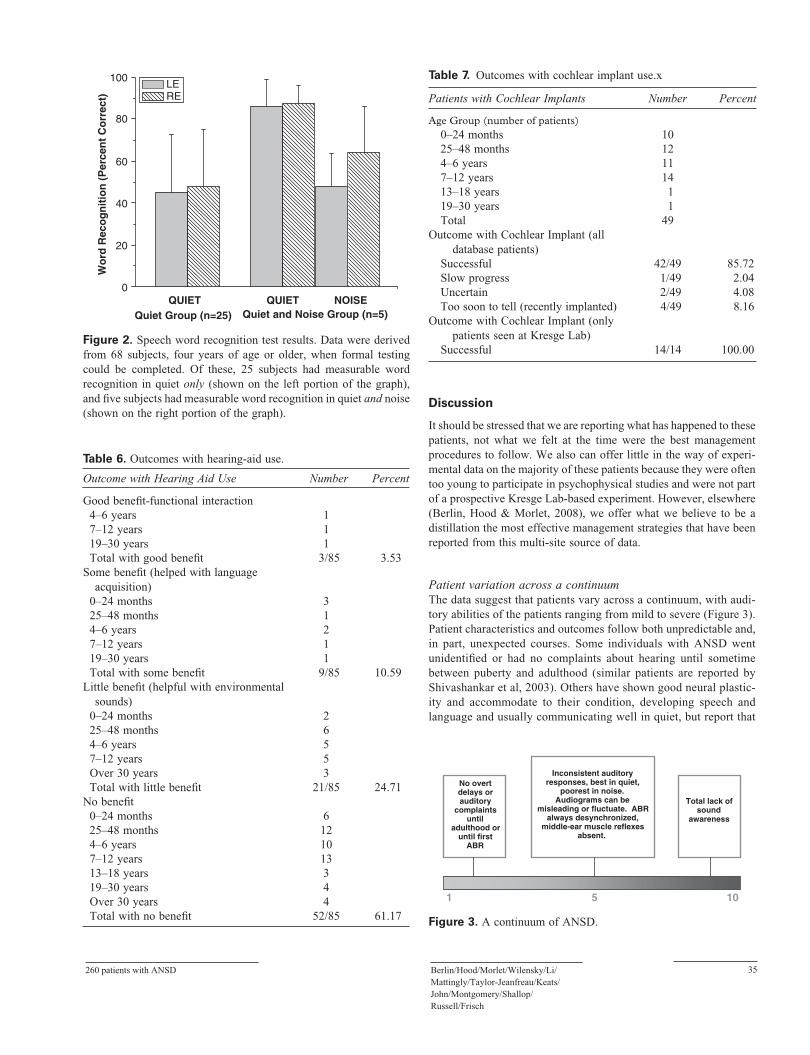
Speech recognition scores for monosyllables in quiet were avail-able from only 25 patients in the database aged four years and older. It should be noted that speech audiometry was attempted in 95 patients in this age range; only 25 had word recognition ability in
34
Table 5. Speech awareness, reception, and recognition test results, basehad word recognition ability in quiet greater than 0%, and only 5 subj
Results for Subjects with Measurable Word Recognition in Quiet OnlyNumber of subjects over 4 years of ageLeft ear mean score (Quiet)Right ear mean score (Quiet)
Results for Subjects with Measurable Word Recognition in Quiet and Number of subjects over 4 years of ageLeft ear mean score (Quiet)Right ear mean score (Quiet)Left ear mean score (Noise )Right ear mean score (Noise )
SRTs were typically obtained using a very limited set of spondees. Speech in noise testing was typically at a +8 or 10 signal-to-noise ratio.
3Four patients came from other clinics initially.
quiet and only 5 in noise. Word recognition in quiet was 0% in the remaining patients ( Table 5 and Figure 2 ). For the 25 patients with speech recognition ability only in quiet, their scores averaged 45.1% for the left ear and 47.8% for the right ear. Five subjects had word recognition ability both in quiet and in noise. These subjects represent our ‘best performers’ in relation to ability to utilize auditory informa-tion, and this is also refl ected in their recognition scores, averaging 86–87% in quiet and 48–64% in noise tested by us with 25-word PB lists at a S/N ratio of +10 for four of the patients and +8 for the remaining patient. The background noise was white noise.
Hearing aids and cochlear implants Hearing-aid outcome data were provided on 85 patients, while CI data came from 49 patients ( Tables 6 and 7 ). Hearing aids, verifi ed with real-ear measurement for our patients at Kresge Lab, were fi t by just one of us (CIB) using an audibility criterion. That is to say, the most stable and repeatable behavioral audiogram was used and fi rst converted to SPL. Then a 40 dB input signal was amplifi ed by the program until the real-ear measures or DSL with RECD showed the output to exceed the target threshold by 5 dB or more. Then the input was changed to 60 and fi nally 75 dB to assure compression and output levels matched the expected maxima predicted from the curves. Aids were tried in 27 of our patients, to establish candidacy for cochlear implantation. In retrospect, it is clear that hearing aids alone helped language acquisition in relatively few of those patients in our sample.
A total of 11 of the 94 patients who tried hearing aids in this sample learned language with hearing aids suffi cient to reach second and third grade, and reportedly compete successfully with normal-hearing peers. The categories were established by parent and audi-ologist’s report (see Table 6 ). Thus we should not be quoted as suggesting that hearing aids will not work with these patients, but only that they have not in the past been salutary for the majority of this limited sample.
This observation should be viewed in context with 13 patients in this sample (13/260 � 5%) whose ANSD was so mild as to require no intervention for hearing or developing speech and language 3 , although all reported trouble hearing in noise.
International Journal of Audiology, Volume 49 Number 1
d on data from 95 subjects. Note that only 25 subjects of this numberects had any word recognition ability in quiet and noise.
25Mean: 45.1% St. Dev.: 27.5%Mean: 47.8% St. Dev.: 27.4%
Noise5Mean: 86.0% St. Dev.: 12.8%Mean: 87.2% St. Dev.: 8.7%Mean: 48.0% St. Dev.: 15.8%Mean: 64.0% St. Dev.: 22.1%
260 patients with ANSD
Table 7. Outcomes with cochlear implant use.x
Patients with Cochlear Implants Number Percent
Age Group (number of patients) 0–24 months 10 25–48 months 12 4–6 years 11 7–12 years 14 13–18 years 1 19–30 years 1 Total 49Outcome with Cochlear Implant (all
database patients) Successful 42/49 85.72 Slow progress 1/49 2.04 Uncertain 2/49 4.08 Too soon to tell (recently implanted) 4/49 8.16Outcome with Cochlear Implant (only
patients seen at Kresge Lab) Successful 14/14 100.00
0
20
40
60
80
100
Wo
rd R
eco
gn
itio
n (
Per
cen
t C
orr
ect)
Quiet Group (n=25) Quiet and Noise Group (n=5)
LERE
QUIET QUIET NOISE
Table 6. Outcomes with hearing-aid use.
Outcome with Hearing Aid Use Number Percent
Good benefi t-functional interaction4–6 years 17–12 years 119–30 years 1Total with good benefi t 3/85 3.53
Some benefi t (helped with language acquisition)
0–24 months 325–48 months 14–6 years 27–12 years 119–30 years 1Total with some benefi t 9/85 10.59
Little benefi t (helpful with environmental sounds)
0–24 months 225–48 months 64–6 years 57–12 years 5Over 30 years 3Total with little benefi t 21/85 24.71
No benefi t0–24 months 625–48 months 124–6 years 107–12 years 1313–18 years 319–30 years 4Over 30 years 4Total with no benefi t 52/85 61.17
Discussion
It should be stressed that we are reporting what has happened to these patients, not what we felt at the time were the best management procedures to follow. We also can offer little in the way of experi-mental data on the majority of these patients because they were often too young to participate in psychophysical studies and were not part of a prospective Kresge Lab-based experiment. However, elsewhere ( Berlin , Hood & Morlet, 2008 ), we offer what we believe to be a distillation the most effective management strategies that have been reported from this multi-site source of data.
Patient variation across a continuum The data suggest that patients vary across a continuum, with audi-tory abilities of the patients ranging from mild to severe ( Figure 3 ). Patient characteristics and outcomes follow both unpredictable and, in part, unexpected courses. Some individuals with ANSD went unidentifi ed or had no complaints about hearing until sometime between puberty and adulthood (similar patients are reported by Shivashankar et al, 2003). Others have shown good neural plastic-ity and accommodate to their condition, developing speech and language and usually communicating well in quiet, but report that
Figure 2. Speech word recognition test results. Data were derived from 68 subjects, four years of age or older, when formal testing could be completed. Of these, 25 subjects had measurable word recognition in quiet only (shown on the left portion of the graph), and fi ve subjects had measurable word recognition in quiet and noise (shown on the right portion of the graph) .
Inconsistent auditory responses, best in quiet,
poorest in noise.Audiograms can be
misleading or fluctuate. ABRalways desynchronized,
middle-ear muscle reflexes absent.
No overtdelays orauditory
complaintsuntil
adulthood oruntil first
ABR
Total lack ofsound
awareness
1 5 10
Figure 3. A continuum of ANSD.
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
35

they hear poorly in even the slightest background noise. At the other extreme, some patients have very poor or non-existent sound awareness and never develop auditory abilities, auditory based lan-guage, or speech. Some patients have missing VIIIth nerves that may remain undiscovered until after a failed CI ( Buchman et al, 2006 ). By contrast, some of these patients and/or their parents report that they are comfortable and well served in Deaf Culture if they neither benefi t from nor respond well to hearing aids or Audi-tory Verbal Therapy, while others say they do well with just lip-reading and/or cued speech. Others, whose parents desire verbal communication, have become ideal candidates for cochlear implan-tation, which usually promotes neural synchrony. In some cases, there may be a combination of ANSD and more central hearing losses (particularly in patients with other conditions in addition to ANSD); this increases the diffi culty of predicting success of man-agement and outcomes. We continue to learn about many, but not all, of these patients and monitor their concerns and issues, albeit informally.4
Underlying mechanisms in ANSD An outstanding and admirable review of underlying mechanisms in ANSD has recently been published by Starr et al (2008) . Our current understanding of inner-ear physiology suggests that the outer hair cells are low-level pre-amplifi ers rather than fully sensory cells (e.g. Dallos & ( Fakler, 2002 ; Dallos et al, 2006 ). The inner hair cells, which have a limited 65–70 dB dynamic range, are the drivers for the primary neural elements. Thus, the presence of normal OAEs and a ‘corner’ audiogram in the presence of an MRI showing a normal VIIIth nerve, would suggest serious impairment of at least inner hair cells with possible concomitant anterograde loss of afferents and synaptic connections. This type of patient might be classifi ed as hav-ing total dys-synchrony fi rst, which might accompany a genetic cause (e.g. otoferlin) or neonatal anoxia ( Amatuzzi et al, 2001 ) with inoperative inner hair cells. Spontaneous language learning in con-genital non-temperature-sensitive otoferlin patients has not been documented. Thus, cochlear implantation, as soon as the parents wish, seems wise to prevent anterograde neural degeneration trace-able to the lack of afferent stimulation.
Separating neural from inner hair cell dysfunction Trans-tympanic electrocochleography, which can separate pre-syn-aptic from post-synaptic dysfunction, is now our most powerful clinical tool. Despite our having promulgated ECochG in the 1970s (e.g. Cullen et al, 1972 ), we have not used it on more than a few of our own ANSD patients, including one patient we presented in the Starr et al (1996) paper. Pre-synaptic dysfunction implicates the inner hair cell and its environs, while post-synaptic dysfunction implicates neural elements themselves. Gibson ) and Sanli (2007 ), ( McMahon et al (2008) , and Santarelli and Arslan (2002) have shown that pre- and post-ganglionic disorders might be separated from one another. These are essential data and might be ultimately collected on all new patients to understand the nature of their auditory disorder and provide more accurately targeted management.
36
4through a Parent’s List Serve owned by Elaine Blackford, RN at [email protected]. Nurse Blackford’s son was among the fi rst 16 ANSD patients we diagnosed at LSUHSC, and she established this List Serve to supply parent-friendly information to other families who receive the ANSD diagnosis.
Speculations on what, if anything, the audiogram might tell us about the underlying pathophysiology? This section presents speculations based on literature reports of true neuropathy patients (e.g. Starr et al, 2003 ), studies of post anoxia patients ( Amatuzzi et al, 2001 ), and the experiences of some of our own patients with confi rmed otoferlin mutations (e.g. Varga et al, 2003 , 2006 ). All of these speculations depend upon a stable behavioral audio-gram, which is often diffi cult to acquire on ANSD patients.
We suspect, based on our data and the literature, that very poor audiograms indicate that inner hair cells are generally absent ormalfunctioning ( Amatuzzi et al, 2001 ; Moore, 2004 ; Rance, 2005 ; Rapin and Gravel, 2006 ) or the V IIIth nerve is absent ( Buchmanet al, 2006 ). The better the audiogram, the more likely we are to have some functioning inner hair cells and some compromised neuralelements ( Starr et al, 2008 ). Combinations and mosaics no doubt abound, but, at the extremes, ANSD and normal OAEs in the presence of a ‘corner’ audiogram are most probably associated with complete inner hair cell loss ( Amatuzzi et al 2001 ; Varga et al 2003 , 2006 ) or absent auditory nerves ( Buchman et al, 2006 ). In contrast Starr et al (1996) and Merchant et al (2001) have shown that a mild-to-moderate audiometric loss has been associated with considerable residual inner hair cells but compromised nerve fi bers. This constellation has been predicted by Rapin and Gravel (2006 ) from most of the same literature.
Possible relationships between clinical characteristics and underlying mechanisms We present two case examples highlighting the variation in clinical characteristics and possible relationships to underlying mechanisms.
Patient A . This patient, who has mutations in the otoferlin gene, was part of the Varga et al (2003) study. She presented with a corner audiogram ( Figure 4 ), which we now associate with completely absent or malfunctioning inner hair cells. Of course one might argue that she might have absent endocochlear potentials (e.g. Loundon et al, 2005 ), but this argument does not hold in view of her normal OAEs ( Figure 5 ). She is also patient A in the Shallop et al (2001 ) paper on CIs in ANSD. Her brother inherited the same gene muta-tions and also has ANSD. Her CI, originally done at age four years and recently upgraded to bilateral implants, has been very successful in part because of her pre-implant language education with cued speech. She now shows excellent speech and language and is main-streamed in a normal school, outperforming virtually all of her normal-hearing peers in reading levels and vocabulary.
From the temporal bones Starr et al (2003) studied, we reason that along with good audiograms come more usable inner hair cells and that only a small number of healthy nerve fi bers are needed to trans-mit that information ( Kiang et al, 1986 ; Burkard et al, 1997 ). How-ever, these conditions need not be mutually exclusive, and it is probable that, in some mild-to-moderate losses, a mosaic of prob-lems might co-exist. Thus, as Amatuzzi et al (2001 ) have already shown in the temporal bones of anoxic infants, there can be parts of the cochlea that show normal outer hair cells and absent inner hair cells, and within just a few millimeters the condition can reverse, with normal-looking inner hair cells and absent outer hair cells. In support of the notion that as long as there are viable inner hair cells there will be some audiometric sensitivity, we again cite Starr et al (2000 , 2003 ), who show the temporal bones of patients with a familial neural disease, intact inner hair cells, and sparsely
International Journal of Audiology, Volume 49 Number 1

Speech Audiometry
R Threshold : NR L Threshold : NR
R Discrim (Q): NR L Discrim (Q): NR
Middle-Ear Muscle Reflex Thresholds
500 1k 2k 4kHz R Contra NR NR NR NR L Contra NR NR NR NR
R Ipsi NR NR NR NR L Ipsi NR NR NR NR
120
110
100
90
80
70
60
50
40
30
20
10
0
�100.25 0.5 0.75 1 1.5 2 3 4 6 8
Frequency in kHz
Hea
rin
g L
evel
in d
B
Right EarLeft Ear
NR above 2kHz
myelinated auditory nerve fi bers. CIs have already been shownto be effective in such patients despite the neuropathies, probablyby synchronizing the available neural elements. As we cited earlier, ( McMahon et al (2008) have shown that pre-synaptic and post-
260 patients with ANSD
synaptic ANSD can be differentiated by ECochG and aid in the separation of what we called ‘dys-synchrony’ from ‘neuropathy’.
Patient B. Success with CIs in such patients is supported by our observations in another ANSD patient (Patient B) with the
Figure 4. Test results for ANSD patient A. Pure-tone thresholds were consistent with a profound hearing loss in the lower frequencies bilaterally and no response in the higher frequencies. No speech reception (threshold) or recognition (discrim) ability was demonstrated.Middle-ear muscle refl exes were absent for ipsilateral and contralateral stimulation at the usual clinical test limits (90–95 dB HL ipsi and 100–110 dB HL contra). NR � no response.
Figure 5. Transient OAE right-ear test results for ANSD patient A. OAEs were present with good reproducibility, particularly in the 1–3 kHz range. Similar results were obtained for the left ear.
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
37

110
100
90
80
70
60
50
40
30
20
10
250 500 1000 2000Frequency (KHz)
dB
Hea
rin
g L
evel
4000 8000
0
�10
Tymps: Type A R&LMEMRs: Ipsi and contra absent R&L
Pre-operative test results: Speech Recognition (recorded stimuli) Quiet (R 60, L 65 dB HL): W22: 8% R / 10% L CID Sentences: 19% R/36% L Noise (+10 S/N): W22: 0% R / 0% L SIN: 0% R / 0% L
Post-operative test results Speech Recognition (CID Sentences 65 dB HL) Quiet: 94% Noise (+10 S/N): 70%
audiogram shown in Figure 6 , normal OAEs, absent MEMRs, and de-synchronized ABR ( Figure 7 ). Initially, we were reluctant to implant this patient because of her nearly normal audiogram for 1 kHz and higher frequencies, but she was losing useful vision due to optic nerve atrophy and systemic peripheral neuropathy. Her post-implant results were, to say the least, excellent, wherein she showed 8–10% word recognition in quiet before her implant and 70% in noise after her implant.
In this case, cochlear implantation was so successful for the 16-year-old daughter that she encouraged her similarly-affl icted father to have the surgery. The CI was equally successful for him. This father and daughter clearly demonstrate a systemic neuropathy, presumably in the auditory system as well, with reduction in axonal function rather than totally inoperative inner hair cells. Such patients, who often have neurological disorders such as Charcot-Marie-Tooth disease, or sometimes hyperbilirubinemia and kernicterus, have not shown ‘corner’ audiograms in our sample. Other patients have audio-grams that fl uctuate with body temperature, a common report in multiple sclerosis for example, again supporting a primarily neural locus for them ( Varga et al, 2006 ).
38
There are clearly cases in the literature that suggest cochlear implantation is not always successful. Miyamoto et al (1999) , for example, showed an unsuccessful implant in a patient with Friedre-ich’s ataxia, and Buchman et al (2006 ) showed why MRIs are critical in evaluating ANSD patients. Many of their patients exhibited either no VIIIth nerve or morphologically small or sparse innervation. This would presumably lead to poorer cochlear implant results than in patients with abnormal inner hair cells for example. Having studies of pre- and post-synaptic responses to sound as McMahon et al (2008) and Santarelli et al (2008) have proposed, might better predict success in ANSD patients.
Issues in evaluation of ANSD We face an increased incidence of the diagnosis ANSD because of the widespread use of screening programs at birth and because of the increased survival of premature infants under 30 weeks gestation. If only one test is used for screening, two errors will occur. OAE screening programs or programs that screen for hearing loss with OAEs will miss ANSD. For such programs locked in to OAEs, we have recommended elsewhere ( Berlin et al, 2005 ) the addition of MEMRs to screening programs if possible and follow up with ABRs on any patient who has normal OAEs and absent MEMRs. Programs that only use ABRs for both screening and diagnosis, and do not add OAEs, have in the past and will continue to miss normal outer hair cell function ( Hall et al, 2004 ). It has been argued that more norms are needed before we can rely on immittance audiometry to aid in the diagnosis of ANSD in infants ( Sutton, 2007 ). However, the pres-ence of refl exes at levels near 90 dB HL per se in neonates and infants up to six months of age would seriously question a diagnosis of ANSD. See Hall et al (2004 ) for a full discussion. Sutton himself may be modifying his criticism (2009).
Undetected mild forms of ANSD Some forms of ANSD are so mild as to need no intervention; our very fi rst patient in 1982 is just such a patient (see next paragraph). Other combinations, in which pure-tone hearing loss generally exceeds 70 dB HL on the audiogram, lead to conditions currently called ‘dead zones’ in the cochlea and suggest that amplifi cation in that zone will not be helpful (Turner et al, 1999; Moore et al, 2000, 2004). Thus we should consider that many of the patients who have, in the past, failed to progress well with hearing aids and auditory verbal therapy (AVT) may have all along been unidentifi ed ANSD patients. In those who have been implanted unilaterally, we have already found some with residual normal OAEs in the unimplanted ear, and there are likely others where emissions have disappeared with time (Deltenre et al, 1999; Rance et al, 1999; Starr et al, 2000; Berlin et al, 2001a). Using a pre-hearing aid triage with positive and negative polarity clicks included in the ABR, plus OAEs and MEMRs, to rule out ANSD might be considered for CI teams that currently require hearing-aid trials before implantation. Currently, hearing aids are often used and recommended as a requirement before implants can be considered; our data show this practice should be monitored carefully because it has sometimes served to delay the ability to eavesdrop on language. Cued speech or signs to aid visual eavesdropping have been a powerful adjunct to avoid language delays, especially if hearing aids are chosen or used for any length of time.
Figure 6. Test results for ANSD patient B. Pure-tone thresholds were consistent with a moderate hearing loss in the lower frequencies bilaterally rising to the normal hearing range in the higher frequencies. Middle-ear muscle refl exes were absent for ipsilateral and contralateral stimulation at 90–95 dB HL ipsi and 100–110 dB HL contra. Speech audiometric test results in quiet and in noise are shown before and after obtaining a cochlear implant.
International Journal of Audiology, Volume 49 Number 1

Some patients (5% in our current sample) develop adequate speech and language with little or no intervention needed. The fi rst patient (Patient C) we ever saw with this syndrome had a normal audiogram with absent MEMRs (which at the time we considered
260 patients with ANSD
to be an insignifi cant variant; Silman and Gelfand, 1981) and had no complaints at all . He was a volunteer ‘normal’ subject for an ABR normative study carried out by one of our colleagues. We saw him again 22 years later to confi rm the presumptive diagnosis of
Figure 7. Transient OAE and ABR test results for ANSD patient B. Robust OAE responses were obtained for each ear (left top, right below).ABRs display only cochlear microphonics, shown by comparison of condensation and rarefaction polarity clicks at two intensities (left top, right below).
Figure 8. Transient OAE left ear test results for ANSD patient C. OAEs were recorded only for the lower frequency bands.
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
39

ANSD, at which time we found normal OAEs ( Figure 8 ), no ABR ( Figure 9 ), and this new audiogram ( Figure 10 ), for which he told us hearing aids suggested by others were never satisfactory.
40
Middle-Ear Muscle Reflex Thresho
500 1k 2k 4kH R Contra 110 105 110 NR L Contra 100 110 115 115
R Ipsi NR NR NR NR L Ipsi NR NR NR NR
110
100
90
80
70
60
50
40
30
20
10
0
-100.25 0.5 0.75 1 1.5 2 3
Frequency in kHz
Hea
rin
g L
evel
in
dB
Right EarLeft Ear
The other 95% of ANSD patients have constituted potential enigmas for management groups that depend primarily (as we did initially) upon the pure-tone audiogram for their guidance.
Figure 9. ABR Test results for ANSD patient C. ABRs show cochlear microphonics, defi ned by comparison of condensation and rarefaction polarity clicks for each ear and no synchronous neural responses.
Speech Audiometry
R Threshold: 20 dB HL L Threshold: 25 dB HL
R Discrim (Q): 78%L Discrim (Q): 72%
lds
z
4 6 8
Figure 10. Test results for ANSD patient C. Pure-tone thresholds were consistent with normal hearing in the lower frequencies bilaterallysloping to a mild-to-moderate hearing loss in the higher frequencies. Speech-reception thresholds were in the borderline normal range, and word recognition (discrim) ability was 78% in the right ear and 72% in the left ear. Middle-ear muscle refl exes were present at elevated threshold levels for contralateral stimulation and absent for ipsilateral stimularion. NR=no response.
International Journal of Audiology, Volume 49 Number 1

Potential weakness of multi-site reports Much can be learned from careful compilation of information such as we have here, but some potential weaknesses must be recognized. First, because of confi dentiality rules, and the 23-year period of our data acquisition from 1982 to 2005, we have little idea of how many of these patients have also been reported in the literature by our col-leagues who published their papers before this paper was accepted for publication.
Second, there are no experimentally controlled or collected data here on the psychophysical or perceptual nature of ANSD. The data obtained from our database provide a view of practices and experiences in our purview, using information about outcomes obtained through case reviews and collaborations. Reports with more extensive direct experience will come, as the number of identifi ed patients continues to grow and from countries (e.g. India and China) with large populations.
Another weakness of reports such as these is always in thepaucity of population data and the failure to control all the testing methods. The few patients we report here by no means constitute the majority of the patients in the population. The data alsoaddress what has happened in the past and been reported to us, and are not presented as harbingers of what will happen in the future with any individual patient. While these patients have been withus for years, the life-saving methods with some premature and medi cally compromised infants likely will be producing more such newborns.
Note also that some patients who have already been implanted because of failure to develop adequate speech and language by ‘tra-ditional methods’, including AVT and hearing aids, may well be unrecognized ANSD patients. In those who have had only one CI, we have already found some with residual normal OAEs in the unimplanted ear, and there are likely others where emissions have disappeared with time ( Deltenre et al, 1999 ; ( Rance et al, 1999 ; Starr et al, 2000 ; Berlin et al, 2001a ).
Conclusions
ANSD patients make up at least 10–15% of children in schools for the deaf, although some report a much lower incidence. There are likely to be many patients who have already been implanted because of failure to succeed with hearing aids and AVT. Only in retrospect, after years of depending upon it, can we see that the audiogram has not generally been valuable in these patients as a management tool for hearing-aid fi tting. Success with hearing aids in quiet as reported by others ( Deltenre et al, 1999 ; Rance et al, 2008 ) has not led to age-appropriate language acquisition in the majority of patients in our report. We recommend obtaining tympanometry, MEMRs and OAEs as a pre-audiometric screening to see if the audiogram can and should be trusted as a valid picture of ‘hearing’ for patients like these. If OAEs are normal and MEMRS are absent, an ABR will help disam-biguate the results and clarify the diagnosis. In audiograms that imply hearing loss of more than 40 dB but accompany normal OAEs word recognition in noise has not been well predicted from the audiogram. Collaboration with speech-language pathologists, neurologists, and teachers of the deaf is of great value to the patients and their families. Although the audiologist is likely to be among the fi rst professionals to encounter a patient with ANSD, management should focus on the global communication skills and abilities of the patient to acquire language, become literate, and be self-suffi cient.
260 patients with ANSD
Acknowledgements
We appreciate the help of grants and support from: NIH NIDCD, BMDR 1549; the Oberkotter, Marriott, Lions, and Deafness Research Foundations; Kam’s Fund for Hearing Research as part of the LSUHSC Foundation; The Kenneth and Frances Barnes Bullington Professorship to Dr. Berlin; and help from the donors who established the Charles I. Berlin PhD Chair in Molecular and Genetic Hearing Science. This Chair was most recently occupied at LSUHSC by Dr. Bronya JB Keats. We appreciate the patients and their families who came for testing and stayed for coffee. Data were collected and shared by many audiologists too numerous to mention, but among the most diligent and steadfast were Harriet L. Berlin, Shanda Brashears Morlet, and Melanie Thibo-deaux. Thanks are due to Annette Hurley, Ph.D., and Robert Turner, Ph.D., for valuable editorial suggestions. Administrative support through the many years of data collection came from Sue Mason, Nan-cie Roark, and Frances Billes. At Vanderbilt University, Andrea Hill-ock, Christopher Spankovich, Rita Anelli, and Christine Williams assisted with recent data review and compilation.
Declaration of interest: We have no fi nancial or related ownership of Parents List Serve on yahoo.com
References
Amatuzzi , M.G., Northrop, C., Liberman, M.C., Thornton , A., Halpin, C. et al. 2001. Selective inner hair cell loss in premature infants and cochlea pathological patterns from neonatal intensive care unit autopsies. ArchOtolaryngol Head Neck Surg, 127: 629– 636 .
Attias , J. & Raveh , E. 2007, Transient deafness in young candidates for co-chlear implants. Audiol Neuro-otol, 12, 325– 333 .
Berlin, C.I., Hood , L.J., Cecola, R.P., Jackson, D.F. & Szabo, P. 1993. Does type I afferent neuron dysfunction reveal itself through lack of efferent suppression? Hear Res, 65, 40– 50 .
Berlin , C.I., Bordelon, J., St John P., Wilensky , D., Hurley, A., et al. 1998. Reversing click polarity may uncover auditory neuropathy in infants. EarHear, 19, 37– 41.
Berlin , C.I., Hood, L.J., Goforth-Barter, L. & Bordelon, J. 1999. Auditory neurop-athy: three time courses after early identifi cation. ARO Abstracts, 22, 169.
Berlin, C.I., Hood , L.J., Morlet, T., Den Z., Goforth , L. et al. 2000. The search for auditory neuropathy patients and connexin 26 patients in schools for the deaf. ARO Abstracts, 23, 23.
Berlin, C.I., Hood , L.J. & Rose, K. 2001a. On renaming auditory neuropathy as auditory dys-synchrony. Audiol Today, 13, 15– 17 .
Berlin, C.I., Jeanfreau, J., Hood , L.J., Morlet, T. & Keats , B. 2001b. Managing and renaming auditory neuropathy as part of a continuum of auditory dys-synchrony. ARO Abstracts, 24, 137.
Berlin , C.I., Morlet, T. & Hood, L.J. 2008. Management of individuals with auditory neuropathy spectrum disorder . In: D. Hayes. & Y.S. Sininger (eds). Identifi cation and Management of Infants and Young Children with Auditory Neuropathy Apectrum Disorder. Aurora, CO: The Chil-dren’s Hospital . pp. 35–40.
Berlin, C.I., Hood, L., Morlet , T., Rose, K. & Brashears, S. 2003. Auditory neuropathy/dys-synchrony: diagnosis and management. Ment Retard Dev Disabil Res Rev, 9, 225– 231 .
Berlin, C.I., Hood, L.J., Morlet , T., Wilensky, D., St John, P. et al. 2005. Absent or elevated middle ear muscle refl exes in the presence of normal otoacoustic emissions: a universal fi nding in 136 cases of auditory neu-ropathy/dys-synchrony. J Am Acad Audiol, 16, 546– 553 .
Buchman , C.A., Roush, P.A., Teagle, H.F., Brown, C.J., Zdanski , C.J.. et al. 2006. Auditory neuropathy characteristics in children with cochlear nerve defi ciency. Ear Hear, 27, 399– 408.
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
41

Burkard, R., Trautwein , P., Salvi, R. 1997. The effects of click level, click rate, and level of background masking noise on the inferior colliculus potential (ICP) in the normal and carboplatin-treated chinchilla. J Acoust Soc Am, 102, 3620– 3627.
Cacace, A.T., Satya-Murti , S. & Grimes, C.T. 1983.; Frequency selectivity and temporal processing in Friedreich’s ataxia. Clinical aspects in two pa-tients. Ann Otol Rhinol Laryngol, 92, 276– 280.
Ceranic, B. & Luxon, L.M. 2004. Progressive auditory neuropathy in patients with Leber’s hereditary optic neuropathy. J Neurol Neurosurg Psychia-try, 75, 626– 630 .
Cheng , X., Li, L., Brashears, S., Morlet, T., Ng , S.S., et al. 2005. Connexin 26 variants and auditory neuropathy/dys-synchrony among children in schools for the deaf. Am J Med Genet, 139, 13– 18 .
Chisin , R., Perlman , M. Sohmer H. 1979. Cochlear and brainstem responses in hearing loss following neonatal hyperbilirubinemia. Ann Otol Rhinol.Laryngol, 88, 352– 357 .
Coats, A.C. & Martin, J.L. 1977. Human auditory nerve action potentials and brain stem evoked responses. Effects of audiogram shape and lesion locations. Arch Otolaryngol, 103, 605– 622 .
Corley, V.M. & Crabbe, L.S. 1999. Auditory neuropathy and a mitochondrial disorder in a child: case study. J Am Acad Audiol, 10, 484– 488 .
Cullen, J.K. Jr, Ellis, M.S. & Berlin , C.I. 1972. Lousteau , R.J. Human acoustic nerve action potential recordings from the tympanic membrane without anesthesia. Acta Otolaryngol, 74, 15– 22 .
Dallos, P. & Fakler, B. 2002. Prestin, a new type of motor protein. Nat Rev Mol Cell Biol, 3, 104– 111 .
Dallos , P., Zheng , J. & Cheatham, M.A. 2006. Prestin and the cochlear amplifi er. J Physiol, 576, 37– 42.
Delmaghani, S., del Castillo, F.J., Michel V., Leibovici M., Aghaie, A. et al. 2006. Mutations in the gene encoding pejvakin, a newly identifi ed protein of the afferent auditory pathway, cause DFNB59 auditory neuro-pathy. Nat Genet, 38, 770– 778 .
Deltenre, P., Mansbach , A.L., Bozet , C., Christiaens, F., Barthelemy, P., et al. 1999. Auditory neuropathy with preserved cochlear microphonics and secondary loss of otoacoustic emissions. Audiol, 38, 187– 195.
Foerst , A., Beutner , D., Lang-Roth , R., Huttenbrink K.B., von Wedel , H. et al. 2006. Prevalence of auditory neuropathy/synaptopathy in apopulation of children with profound hearing loss. Int J Pediatr Otorhi-nolaryngol, 70, 1415– 1422 .
Forli, F., Mancuso, M., Santoro, A., Dotti, M.T., Siciliano , G. et al. 2006. Auditory neuropathy in a patient with mitochondrial myopathy and multiple mtDNA deletions. J Laryngol Otol, 120, 888– 891 .
Gibson, W.P. Sanli , H. 2007. Auditory neuropathy: an update. Ear Hear. 28, 52: 102S– 106S .
Hall , J.W. 3rd, Smith, S.D. & Popelka , G.R. 2004. Newborn hearing screening with combined otoacoustic emissions and auditory brain-stem responses. J Am Acad Audiol, 15, 414–425.
Hinchcliffe , R., Osuntokun , B.O. & Adeuja, A.O. 1972. Hearing levels in Nigerian ataxic neuropathy. Audiol. 11: 218– 230 .
Kaga, K., Nakamura , M., Shinogami , M., Tsuzuku ,T., Yamada , K. et al. 1996. Auditory nerve disease of both ears revealed by auditory brain-stem responses, electrocochleography and otoacoustic emissions. Scand. Audiol, 25, 233– 238.
Kemp, D.T. 1978. Stimulated acoustic emissions from within the human auditory system. J Acoust Soc Am, 64, 1386– 1391 .
Kiang , N.Y., Liberman , M.C., Sewell , W.F., Guinan , J.J. 1986. Single unit clues to cochlear mechanisms. Hear Res, 22, 171– 182.
Konrádsson, K.S. 1996. Bilaterally, preserved otoacoustic emissions in four children with profound idiopathic unilateral sensorineural hearing loss. Audiol, 35, 217– 227 .
Korzybski, A. 1958. Science and Sanity: An Introduction to Non-Aristotelian Systems and General Semantics . Connecticut: EngleWood, No, The International Non-Aristotelian Library Publishing Company.
42
Kraus , N., Ozdamar, O., Stein , L. & Reed , N. 1984. Absent auditory brain stem response: peripheral hearing loss or brain stem dysfunction? Laryngoscope, 94, 400– 406.
Kraus, N., Bradlow, A.R., Cheatham , M.A., Cunningham , J., King , C.D., et al. Consequences of neural asynchrony: a case of auditory neuropathy. 2000. J Assoc Res Otolaryngol, 1, 33– 33 .
Lee , J.S.M., McPherson, B., Yuen, K.C.P. & Wong L.L.N. 2001. Screening for auditory neuropathy in a school for hearing impaired children. Int J Pediatr Otorhinolaryngol, 61, 39– 46.
Loundon , N., Marcolla, A., Roux, I., Rouillon, I., Denoyelle, F. et al. 2005. Auditory neuropathy or endocochlear hearing loss?. Otol Neurotol, 26, 748– 754.
McMahon , C.M., Patuzzi, R.B., Gibson, W.P. & Sanli, H. 2008. Frequency-specifi c electrocochleography indicates that presynaptic and postsynaptic mechanisms of auditory neuropathy exist. Ear Hear, 29, 314– 325.
Merchant, S.N., McKenna , M.J., Nadol , J.B., Jr Kristiansen , A.G., Tropitzsch, A. et al. 2001. Temporal bone histopathologic and genetic studies in Mohr-Tranebjaerg syndrome (DFN-1). Otol Neurotol, 22, 506– 511 .
Miyamoto, R.T., Kirk, K.I., Renshaw, J. & Hussain, D. 1999. Cochlear im-plantation in auditory neuropathy. Laryngoscope, 109, 181– 185 .
Moore, B.C., Huss, M., Vickers, D.A., Glasberg, B.R. & Alcántara, J.I. 2000. A test for the diagnosis of dead regions in the cochlea. Br J Audiol, 34, 205– 224 .
Moore, B.C. 2004. Dead regions in the cochlea: conceptual foundations, diagnosis, and clinical applications. Ear Hear, 25, 98– 116 .
Moser, T., Strenzke, N., Meyer, A., Lesinski-Schiedat A., Lenarz, T, et al. 2006. Diagnosis and therapy of auditory synaptopathy/neuropathy. HNO, 54, 833– 839 .
Podwall , A., Podwall , D., Gordon , T.G., Lamendola, P. & Gold, A.P. 2002. Unilateral auditory neuropathy: case study. J Child Neurol, 17, 306– 309.
Prieve , B.A., Gorga , M.P. & Neely, S.T. 1991. Otoacoustic emissions in an adult with severe hearing loss. J Speech Hear Res, 34, 379– 385.
Rance , G., Beer , D.E., Cone-Wesson, B., Shepherd , R.K., Dowell, R.C. et al. 1999. Clinical fi ndings for a group of infants and young children with auditory neuropathy. Ear Hear, 20, 238– 252.
Rance, G., McKay, C. & Grayden, D. 2004. Perceptual characterization of children with auditory neuropathy. Ear Hear, 25, 34– 46 .
Rance , G. 2005. Auditory neuropathy/dys-synchrony and its perceptual con-sequences. Trends Amplif, 9, 1– 43.
Rance, G., Barker , E.J., Sarant , J.Z. & Ching, T.Y. 2007. Receptive language and speech production in children with auditory neuropathy/dyssynchro-ny type hearing loss. Ear Hear, 28, 694– 702.
Rance , G. & Barker , E.J. 2008;. Speech perception in children with Auditory Neuropathy/Dyssynchrony managed with either hearing aids or cochlear implants. Otol Neurotol, 29: 179– 182.
Rance, G., Fava , R., Baldock, H., Chong , A., Barker , E., Corben, L. & Delatycki , MB. 2008. Speech perception ability in individuals with Fried reich ataxia. Brain, 131: (Pt 8 ), 2002– 2012 .
Rapin , I. & Gravel, J.S. 2006. Auditory neuropathy: a biologically inappro-priate label unless acoustic nerve involvement is documented. J Am Acad Audiol, 17, 147– 150 .
Rea , P.A. & Gibson , W.P.R. 2003. Evidence for surviving outer hair cell function in congenitally deaf ears. Laryngoscope, 113, 230– 234.
Santarelli , R., Arslan, E. 2002. Electrocochleography in auditory neuropathy. Hear Res, 170, 32– 47.
Santarelli, R., Starr , A., Michalewski, H.J. & Arslan , E. (2008). Neural and receptor cochlear potentials obtained by transtympanic electrocochleog-raphy in auditory neuropathy. Clin Neurophysiol, 119 (5 ), 1028– 1041 .
Shallop, J.K., Peterson , A., Facer, G.W., Fabry , L.B. & Driscoll, C.L. 2001. Cochlear implants in fi ve cases of auditory neuropathy: postoperative fi ndings and progress. Laryngoscope, 111, 555– 562.
Shivashankar, N., Satishchandra , P., Shashikala , H.R. & Gore, M. 2003. Pri-mary, auditory neuropathy—an enigma. Acta Neurol Scand, 108, 130– 135.
International Journal of Audiology, Volume 49 Number 1

Silman , S. & Gelfand , S.A. 1981;. The relationship between magnitude of hearing loss and acoustic refl ex threshold levels. J Speech Hear Disord, 46, 312– 316.
Sininger, Y.S. 2002. Identifi cation of auditory neuropathy in infants and children. Sem Hear, 23, 193– 200.
Starr, A., Picton, T.W., Sininger, Y., Hood, L.J. & Berlin, C.I. 1996. Auditory neuropathy. Brain, 119, 741– 753 .
Starr, A., Sininger , Y., Winter , M., Derebery, M.J., Oba, S. et al. 1998 . Transient deafness due to temperature-sensitive auditory neuropathy. Ear Hear, 19, 169– 179.
Starr , A., Sininger , Y.S. & Pratt, H. 2000. The varieties of auditory neuropa-thy. J Basic Clin. Physiol Pharmacol, 11, 215– 230.
Starr , A., Michalewski , H.J., Zeng, F.G., Fujikawa-Brooks, S., Linthicum, F. et al. 2003. Pathology and physiology of auditory neuropathy with a novel mutation in the MPZ gene (Tyr145- � Ser). Brain, 126, 1604– 1619 .
Starr , A., Zeng, F.G., Michalewski , H.J. & Moser, T. 2008. Perspectives on auditory neuropathy: Disorders of inner hair cell, auditory nerve, and their synapse . In: A.I. Basbaum, A. Kaneko, G.M. Shepherd, G. & Wes-theimer (eds.). The Senses: A Comprehensive Reference. P. Dallos, D. Oertel (eds.) Vol 3: Audition. San Diego: Academic Press, 3 97– 412 .
260 patients with ANSD
Sutton , G.J. 2007. Usefulness of acoustic refl exes still unproven in newborns and young infants. Letter to the Editor. J Amer Acad Audiol. 18, 187– 189.
Turner, C.W., Chi, S.L. & Flock , S. 1999. Limiting spectral resolution in speech for listeners with sensorineural hearing loss. J Speech Lang Hear Res, 42, 773– 784.
Varga, R., Kelley , P.M., Keats, B.J., Starr, A., Leal , S.M. et al. 2003. Non-syndromic recessive auditory neuropathy is the result of mutations in the otoferlin (OTOF) gene. J Med Genet, 40, 45– 50 .
Varga, R., Avenarius, M.R., Kelley, P.M., Keats , B.J., Berlin, C.I. et al. 2006. OTOF mutations revealed by genetic analysis of hearing loss families including a potential temperature sensitive auditory neuropathy allele. J Med Genet, 43, 576– 581 .
Withnell, R.H. 2001. Brief report: the cochlear microphonic as an indication of outer hair cell function. Ear Hear, 22, 75– 77 .
Worthington , D.W., Peters , J.F. 1980. Quantifi able hearing and no ABR: paradox or error?. Ear Hear , 1, 281– 285.
Zeng, F.G., Oba , S., Garde, S., Sininger , Y. & Starr , A. 1999. Temporal and speech processing defi cits in auditory neuropathy. Neuroreport, 10, 3429– 3435 .
Zeng , F.G., Kong, Y.Y., Michalewski, H.J. & Starr , A. 2005. Perceptual consequences of disrupted auditory nerve activity. J Neurophysiol, 93, 3050– 3063 .
Berlin/Hood/Morlet/Wilensky/Li/Mattingly/Taylor-Jeanfreau/Keats/John/Montgomery/Shallop/Russell/Frisch
43