m.slam.nhs.uk · • this option means that you will be able to see other participants (and be...
TRANSCRIPT

A meeting of the Council of Governors Tuesday 15 September 2020 from 15.00 to 17.00
Held via Microsoft Teams AGENDA
COG 20
ITEM PRESENTER TIME PAGES
STANDING ITEMS 20 Introductions and welcome, apologies for
absence, declarations of interest.
Chair 15.00 (5)
21
Minutes of the meeting of the Council of Governors, 10 June 2020. Action log.
Chair 15.05 (5)
1 - 9
22 Chair’s Report and Diary
Chair 15.10 (5)
10 - 19
PRESENTATION 23 External Auditor’s Report Sarah Ironmonger,
Grant Thornton LLP 15.15 (10)
20 - 51
24 Audit Committee Report
Duncan Hames 15.25 (10)
52 - 62
EXECUTIVE REPORTS 25 CEO Report David Bradley 15.35
(5)
26 Finance Report Gus Heafield / Andy Bell
15.40 (10)
63 - 66
27 Performance and Quality Report Vanessa Smith Michael Holland Neil Robertson
15.50 (10)
67 - 114
FOR INFORMATION 28 Lead / deputy lead governor report
Jenny Cobley
Sue Scarsbrook Brian Lumsden
16.00 (5)
115 - 116
29 Working group reports • Quality Working Group • Planning and Strategy Working Group • Membership and Planning Working Group • Bids Steering Group
Gill Sharpe
Angela Flood Ermias Alemu Simon Darnley
16.05 (15)
117 - 121
Q&A FOR ANSWER BY THE NEDs AND EXECUTIVE 30 In the interests of time, Governors are
requested to submit questions in advance for the Q&A portion of this meeting to [email protected]. Questions submitted in advance will be prioritised on the day.
Chair 16.20 (25)
FOR DECISION 31 Appointment of external auditor
Gus Heafield 16.45
(10) 122 - 128
FOR NOTING

32 Presentation of Annual Report and Accounts Chair 16.55 (5)
33 Governor / NED meeting notes • 28 July 2020
Chair - 129 - 131
WRAP-UP 34 Date of next meeting:
• 10 December 2020, 11.00 – 13.00 This meeting is likely to be held online and in person (social distancing allowing).
Chair -
How to join a virtual Governors’ meeting on Microsoft Teams
To join a Microsoft Teams meeting on a desktop / laptop • This option means that you will be able to see other participants (and be seen, if you choose to). • Please see the attached document showing you how to join a Teams meeting. If you choose to
use the app, please allow a few minutes to get the app loaded and make sure you are familiar with it the first time.
• When joining via Teams you do not need phone or PIN numbers. To join a Microsoft Teams meeting on a smartphone • This option also means that you will be able to see other participants (and be seen, if you
choose to). • Click the link on the invite email. You will be directed to download the app. • Once downloaded, you will need to register for free. • Once downloaded and registered, you can then open the meeting through the Teams app. To join a Microsoft Teams meeting using a phone • This option is just like joining a conference call. • If you do not want other people to see your phone number, dial 141 first. • Ring the phone number given on the email invitation you will be sent. • You will then be asked to enter PIN number (given on invitation) . • There may be a short pause as other people ahead of you join. • You will be asked to state your name, and will then be linked into the meeting. Note: if you wish to see the meeting but do not have a microphone on your computer, you may join both by phone and by Teams. Meeting etiquette • Please bear with us, we are all learning how best to administrate and organise virtual meetings. • Virtual meetings are, by necessity, a slightly more stilted format than meeting in person due to
delays in the signal; the meeting will work better if attendees allow space for others to speak. • If you are able, please routinely mute your microphone, to minimise the ‘noise’ or interference in
the meeting. Turning off your camera may improve connection difficulties • There are multiple ways to highlight if you wish to contribute (there are pictures in the
accompanying : o Attendees using Microsoft Teams submit a question to the organiser using the chat function
(the square speech bubble), or use this to state that you wish to say something. The symbol is a square speech bubble and can be found either in the top right corner of your screen if you are on an iPad, or if you hover over the screen on a laptop / desktop.
o There is also the ‘raise hand’ button (not show on the panel below, but it is a picture of a hand), though not every version has this functionality. This alerts the virtual room that you wish to say something. Please put your hand down when you have finished.

o If you have joined the meeting over the phone, the Chair will invite phone participants if they would wish to make a point; when this happens, please state your name.
• Please then wait for the Chair or administrator to ask you to speak. • Please respect the Governor Group Agreement, included below for reference.
Left to right: Camera on / off; microphone on / off; share screen; other options; chat screen; other people in the meeting; hang up. Tips for Teams on the phone • If you have been muted and are then invited to speak, please press * then 6 to unmute.
Reclaiming the cost of your call • The call will be charged at a local rate, and we are happy to reimburse you on production of the
phone bill and the standard claim form (Carol can let you have a claim form).
Governor Group Agreement
1. We will treat others with courtesy & respect. We will not raise our voices, make personal criticisms or behave in a threatening manner.
2. We will be kind, caring and polite:
• We will support and encourage participation from quieter members of the group. • There is no such thing as a stupid question. If we are unsure we will ask.
3. We will work within agreed timeframes – valuing the time of others:
• We will start the meeting on time. • We will set mobile phones to silent and take calls only in an emergency. • We will help to keep discussions within the allocated time frame.
4. We will respect our differences, challenging the statement not the person:
• We will not personalise differences of opinion. 5. We will listen to others:
• In discussions, we will indicate to the person chairing the meeting that we would like to speak and wait to be invited.
• We will give other people the chance to speak. 6. Wherever possible, we will do what we say we will do 7. We will not discriminate against anyone on the grounds of their age, gender, gender re-
assignment, marriage, civil partnership, pregnancy, maternity, race, religion and belief or sexual orientation
8. We will not share personal information about other people without their permission.

Minutes of a meeting of the Council of Governors of the South London and Maudsley NHS Foundation Trust
Held on 11 June 2020, 17.00 to 18.15, via Microsoft Teams and telephone
Present Sir Norman Lamb Trust Chair Ermias Alemu Maggie Browning
Staff Governor Southwark Council
James Canning David Clugston
Public Governor Service user Governor
Jenny Cobley Public Governor Giles Constable Staff Governor Rhoda Dakar Service user Governor Ed Davie Lambeth Council Charles Gostling Lewisham Clinical Commissioning Group (CCG) Bert Johnson Rethink Mental Illness Nancy Kuchemann Michael Kopelman
Southwark CCG Public Governor
Brian Lumsden Public Governor Susan Scarsbrook Carer Governor Gill Sharpe Public Governor Luke Sorba Tutiette Thomas
Lewisham Council Service user Governor
Emma Williamson Staff Governor
In attendance Andy Bell Director of Finance Rod Booth Director of Performance, Contracts and Operational
Assurance David Bradley Helen Edwards Ian Everall Mike Franklin Duncan Hames Michael Holland
Chief Executive Non-Executive Director Non-Executive Director Non-Executive Director Non-Executive Director Medical Director
Charlotte Hudson Paul Gibson Renuka Jeyarajah-Dent June Mulroy Norbert Lieckfeldt
Ian Rothwell
Interim Director of Corporate Affairs Corporate Governance Manager NeXt Director Non-Executive Director Observer (Corporate Governance Manager, East London NHS Foundation Trust) Interim Deputy Director of Corporate Affairs
Vanessa Smith Interim Director of Nursing Carol Stevenson Membership Officer Geraldine Strathdee Non-Executive Director Anna Walker Non-Executive Director
Page 1 of 131

Apologies Jane Avis Croydon Council Tim Dee Service user Governor Angela Flood Carer Governor Philippa Lalor Service user Governor Vaishali Shetty Croydon CCG
Did not attend Maisie Barrett Abraham Blay Handsen Chikowore Simon Darnley Heather Gilmour
Carer Governor Staff Governor Public Governor Staff Governor Kings College Hospital (KCH)
Harpal Harrar Ian Norman Jann Oliver
Lambeth CCG Kings College Hospital (KCH) Public Governor
Modupe Oluwapowale Rawle Ragoobar Ingrid Tennessee
Service user Governor Staff Governor Public Governor
COG /20
Item Action
12 Introductions and welcome, apologies for absence, declarations of interest, action log
Sir Norman Lamb welcomed Governors to the meeting and thanked them for embracing the virtual meeting format and reminded them to observe the protocols that had been sent out in advance. He advised that two Governors have stepped down since the last meeting (Adam Black and Ray Baker) and placed on record his thanks for their contributions. Apologies were taken as above. There were no new declarations of interest or matters arising from the action log. There were no minutes to approve as the previous meeting on 12 March 2020 was cancelled due to the onset of the Covid-19 pandemic.
13 Finance report Andy Bell introduced this report and advised Governors that the Trust has met its
breakeven total for the 2019-20 financial year (with £14.3m of central NHS Improvement funding included) and this had been aided by a reduction of private bed usage and the recovery of income debts. The Trust’s cash position remains robust; capital spend in-year was reduced from the planned £25m to £18m following delays in major schemes. The Trust had fully allocated approximately half of its planned Cost Improvement Programme (CIP) savings. He also provided an update to Governors on the impact Covid-19 has had on Trust finances, advising that the normal funding and contracting process with commissioners has been suspended and replaced by emergency funding measures. These include a block (lump sum) payment each month based on the Trust’s spending pattern in 2019/20, plus 2.8% inflation. This payment will be monitored throughout the year and funding can be increased or decreased depending on either over or under funding through the block payment. In addition,
Page 2 of 131

SLaM receives separate funding for COVID 19 specific costs based on a monthly return. In advance of the meeting Governors had submitted questions relating to this item, the first of which was as follows: I read in the May Board papers that there is £9 million debt from local authorities owed to SLAM, £6.5 million of the £9 million budget from Southwark owed in debt, which is mainly reimbursement for placements. Is this for 2019/ 2020? Has SLAM received any further information on this debt and when it will be settled? Andy Bell responded that not all of the debt related to 2019/20, with some of it relating to previous years. Assurances are being sought around the repayment of the full amount within the Integrated Care System (ICS). Norman Lamb asked what the justification was for non-payment. Andy Bell advised that repayments are complicated by an ongoing dispute between the South East London Clinical Commissioning Group (CCG) and Southwark Council over the allocation of payments. SLaM has invoiced in good faith and has escalated as appropriate with David Bradley meeting with Southwark Council’s Chief Executive Officer and Director of Social Care to raise the issue. Tutiette Thomas voiced her concern that with Southwark having the largest African and Afro-Caribbean diaspora in the country, there is a significant risk that these communities will be disproportionally affected again in the provision of mental health services to them. Nancy Kuchemann acknowledged that there are challenging legacy issues to work through and that it is hoped that the move towards an Integrated Care System and pooled budgets across the SLaM boroughs will help prevent such problems occurring in the future. In response to a Governor question regarding other local authority models that could be adopted in the meantime, the Lambeth Alliance was suggested as an example where the consolidation of resources between the local CCG and Council is working effectively. The second question submitted under the finance item was as follows: Post services - community teams are continuing to send fit notes and other correspondence to service users via second class mail. Given that it can now take more than 2 weeks for second class mail to arrive, could the Trust switch to using first class mail by default, until Royal Mail services have returned to their pre-covid levels? Could this incremental expense be considered a covid-19 cost and then be reclaimed? Andy Bell advised that this change can be implemented as it represents a modest cost and could be reclaimed under Covid-19 arrangements.
14 Reshaping services: the journey out of Covid-19 and working in partnership Rod Booth, Director of Performance, Contracts and Operational Performance,
introduced this item providing Governors with an overview of the Trust’s work to move into a ‘post-Covid’ era and the partnership arrangements that are being established to achieve this. He began by outlining some of the drivers behind this work including:
• Enabling effective demand and capacity planning, particularly as there remains the risk of second wave of the Covid-19 pandemic;
Page 3 of 131

• Freeing up acute care pathways across the Integrated Care Systems (ICS) and South London Partnership (SLP);
• Reducing administrative obstacles to enable a more agile crisis response; • Collaborating with partners on population health initiatives; • Supporting members of staff, especially those returning to work following
Covid-related absence. He then shared with Governors the five key principles established across the Integrated Care Systems that are guiding reshaping work. These are:
• The front door/crisis offer – learning and building on what was successful during our Covid-19 response and delivering a best in class mind and body offer on the crisis pathway;
• Housing/welfare/employment/education – picking up the NHS Long Term Plan ambitions for our community rehabilitation offer;
• Pharmacy and prescribing – focus on psychosis and schizophrenia • Primary care network therapies offer – meeting the post Covid-19 demand
to support local communities and staff; • Reducing health inequalities – roll out the Mind and Body programme across
all services to strengthen the link between good physical and mental health. Governors were then appraised of some the initiatives that have already commenced within the reshaping programme. These include:
• Working with SLP partners on sharing bed space to free up acute pathways and the establishment of new and innovative all-age Crisis Assessment Centres to alleviate pressure on acute emergency departments;
• Increased Home Treatment Team service to manage patients post-discharge and therefore enable faster discharge;
• Moving Improving Access to Psychological Therapies (IAPT) from face to face to predominantly virtual appointments (approximately 80%)
• Arrangement of an SEL System Summit on 2 June 2020 jointly hosted between NHS and Local Authority partners to address how we can work together to protect our communities’ mental health as a result of Covid-19 culminating in a set of six agreed high level actions;
• Further roll-out of our housing and community rehabilitation model developed via the Lambeth Alliance to support independent living – this has included two step-down housing projects progressed during the pandemic;
• New ICS Mental Health System Governance across the SEL and SLP with the establishment of an ICS Mental Health Leadership Group
There had been several Governor questions submitted for this item and these included: In the ICS Action Programme, the expectation on how the Integrated Care System will address health inequalities, meet need and prioritise patients who are not currently or historically accessing services, one of the suggestions is ‘Working with Local Authority, Voluntary Sector and Health partners via Alliance and partnership governance to meet population health needs and ensure our hard to reach communities are aware of and can access services’. Can I have some more information on how SLaM would like to work with the Local Authority (specifically Southwark but presumably also Lambeth) and what steps have already been taken to put this in place?
Page 4 of 131

Rod Booth advised that the ICS Action Programme has a 12-24 month integration timeline and that partnership working will be progressed through a number of networks including: the ICS Mental Health Leadership Group (see above); established (Lambeth) and emerging alliance arrangements; new alignments arising from the SEL System Summit and the adoption of a multi-agency approach. Engagement and collaboration with local authorities with be incorporated within all these initiatives. Could you give us the latest thinking on environments – how to accommodate face-to-face meetings for those who need it? I have seen that psychologists are particularly concerned about this. Michael Holland advised that SLaM psychologists have been provided with guidance in this area and that accompanying risk assessments will follow. Could you tell us more about how Consultant Connect works? Governors were advised that Consultant Connect is a digital application designed to enable direct contact between Primary Care (GPs) and Trust Consultants – providing advice and support to optimise the patient pathway and get support in early to prevent admission. Emma Williamson wished to highlight that there needs to be some careful thinking on how elements of the reshaping plans might have an adverse impact on vulnerable communities such as the homeless who might become excluded if virtual interactions with mental health services become predominant. Michael Holland responded that SLaM is mindful of the challenges facing this particular community and their needs will be identified and monitored as part of the reshaping plans.
15 Performance and Quality (P&Q) Report Michael Holland introduced this item and Governors were advised that due to the
Covid-19 pandemic and the subsequent prioritisation of some workstreams, some of the most recent data has not been readily available and there has been an understandable focus on freeing up critical care capacity and serving wider population health requirements. Attention was drawn to a new indicator on patient discharge rates. The report was taken as read and the item moved on to the Governor questions that had been submitted in advance including: I note that the P&Q report is not up-to-date, due to Covid. It is good to see that Out of Area beds were down to zero in March and there had been a reduction in Mental Health Act assessment cancellations. However, I am concerned that Child and Adolescent Mental Health Services were not accepting new referrals (except in crisis) – how long will this continue, or has the situation improved? Michael Holland advised that the Child and Adolescent Mental Health Service (CAMHS) had continued to accept referrals during the current pandemic and that it was only specialist services in this area that had been stepped down due to a specific request from NHS England and these are now restarting. How is the discharge of patients with combined brain injury and psychiatric problems being managed?
Page 5 of 131
Michael Holland advised that these instances are being treated exactly as they were before the pandemic, bar shielding where necessary and with no changes to discharge processes. Giles Constable asked what the plans are to re-open inpatient wards as the Trust emerges from the pandemic. Michael Holland explained that this is being done in increments (with some staff capacity challenges) and that while the Trust is working towards a pre-pandemic complement of beds, there needs to be contingency planning to cope with a potential second wave of the virus with capacity built-in for infection control.
16 Q&A FOR ANSWER BY THE NEDs AND EXECUTIVE There were several questions submitted by Governors under this item; responses
to these from the Non-Executive Directors and members of the Executive are outlined below: At a recent briefing from NHS Providers at a Governwell event for Governors I learned that Centralised Procurement had become an issue particularly concerning Personal Protective Equipment (PPE). There was then on going distribution problems as the orders tended to go to a centralised store rather than individual trusts causing delay. I was wanting to know if this could happen here in SLAM for anything else not just PPE? Andy Bell advised that PPE receipt from a central source has not been a significant issue and that the Trust has benefitted from a proactive approach to procurement as part of shared service agreement with other Trusts (Guy’s and St Thomas’ Foundation Trust leading) and also by securing access to a National Hub of resources. This applies to other equipment and supplies and is not restricted to PPE. What demonstrable, accountable assurances can the NEDs give that the Executive will demonstrate will, and leadership, by the implementation of policies and programmes which address Black, Asian and Minority Ethnic (BAME) inequity? Sir Norman Lamb emphasised that it is a central priority for the Trust to enshrine within its working practices equality of opportunity for BAME staff progression and equality of access and provision for BAME service users. He pointed to important work already underway concerning the increased recording of ethnicity data that is designed to provide further insight into areas such as restraint, detentions under the Mental Health Act and length of stay which have been identified as concerns for the BAME community. The recent Mental Health Prevention Summit held in conjunction with South London and Local Authority partners has also resulted in a set of agreed actions including a mental health community capacity building programme that seeks to reach out, listen and act upon the concerns of as many communities as possible across the boroughs that the Trust serves. Anna Walker added that as Chair of the Quality Committee and as a member of the Equalities and Workforce Committee, redressing inequality is a top priority and she echoed the importance of improving data collection procedures so that they can also inform activity in other areas such bullying and harassment. She welcomed the introduction of the Listening into Action initiative for significantly moving engagement with BAME staff in a more positive direction and the substantial progress made on the Integrated Equalities Action Plan.
Page 6 of 131

Geraldine Strathdee reaffirmed that addressing inequalities is a principal focus for Non-Executive Directors and that not only is more comprehensive, intelligent data collection necessary as a step towards achieving this, but the follow-up analysis on this information needs to be both robust and incisive if it is to enable greater understanding of the particular challenges facing the different cultural groups within the BAME communities that the Trust serves. As Chair of the Mental Health Law Committee, a key objective is to secure greater representation BAME service user representation to provide input and drive change; she is also delighted to be welcoming Non-Executive Directors Mike Franklin and Renuka Jeyarajah-Dent to the group. Mike Franklin stated that he is delighted to be joining the Mental Health Law Committee and supported Geraldine Strathdee’s assertion that more robust data gathering and analysis is needed if long-standing issues for the BAME community in areas such as restraint and other restrictive practices are to be better understood and consequently addressed. He added the pandemic has disproportionately affected members of the BAME community and that this naturally includes SLaM staff; while he is pleased to see the introduction of risk assessments to provide an important layer of protection, he feels that these should include in-built mitigation ideas where possible. Governors welcomed the necessary focus on and improvements to, the recording of ethnicity data and hope that this will be supported by sufficient resources. They are excited to see the proposals emerging from the Mental Health Prevention Summit and hope this will include input from as wide a group of community, faith and third-sector organisations as possible. In addition it is hoped that the Trust’s reshaping work will look at whether its services are culturally competent in catering for as many of SLaM’s diverse communities as possible. How have the SLaM staff in the Middle East been getting on during the pandemic, and are they OK? Governors were advised that Maudsley Health staff based in Abu Dhabi have been observing guidelines on working at home where possible and maintaining safe social distancing in medical environs. Would it not be a good idea if both the Chief Executive and the Medical Director were to offer exit interviews to Consultants who leave the Trust to work elsewhere? Michael Holland advised that both inductions and exit interviews are conducted with new and departing consultants. Issues raised are escalated to the Medical Director to take forward with clinical services. The Trust uses a lot of Bank staff from NHS Professionals. Could SLaM, possibly in conjunction with the South London Partnership LP or Integrated Care Systems, set up their own Bank? Governors were advised that the Trust is investigating whether a shared bank option with other Trusts might be feasible. David Bradley added that there is large recruitment drive currently being undertaken across the Trust.
Page 7 of 131

17 Engaging Governors during the pandemic and plans going forward Sir Norman Lamb thanked Charlotte Hudson for her work in maintaining Governor
engagement during the pandemic and this was echoed by Governors who have appreciated the bespoke update and Q&A sessions that have been arranged with Executive and Non-Executive Directors (see below). Charlotte Hudson stated that she feels the Trust is incredibly fortunate to have such an engaged group of Governors. She wished to highlight the forthcoming Governor elections and in an effort to encourage a greater breadth and diversity of candidates, requested volunteers from the Governor group to participate in a possible video/social media promotion on the role of a Governor and its importance.
18 Governor/Board meeting minutes and Governor/NED meeting notes The Council of Governors noted the minutes of the bespoke Governor/Board
meetings held on the 5 and 21 May 2020 and the notes of the Governor/NED meeting held on 19 May 2020.
19 Date of next meeting The next meeting is due to be held on 15 September 2020 from 15.00 – 17.00.
Depending on the public safety arrangements in place in September, this meeting is likely to be held online and in person (social distancing allowing). Arrangements for the Annual Members Meeting which is due to be held on the same day will also be revisited.
Page 8 of 131

Council of Governors Action Tracker – September 2020
Meeting date
Item ref Description of action Lead Date for completion
Status / Notes / Evidence RAG
14/03/19 MC1906 Add Community Development Design Programme to the Council of Governors’ forward workplan.
Corporate Affairs
Mar-20 Community Redesign is incorporated into Reshaping our Services programme; Council of Governors and Quality Working Group will receive regular updates from this programme.
G
14/03/19 MC1908 Membership and Involvement Working Group to revisit Council membership under the constitution with a view to making recommendations for revision.
Corporate Affairs
Jan-20 A Task & Finish Group will produce revisions for consideration by the Council and the Board. Deferred due to COVID-19, will reschedule.
A
10/09/19 MC1939 An item explaining the different types of audits and their functions to be included on a future CoG agenda.
Corporate Affairs
Mar-20 Audit report at the September Council of Governors, but different types of audit not referred to in the written report. Potentially a verbal update, otherwise it will be listed for a subsequent meeting.
A
RAG ratings Green = action complete Amber = action on schedule for completion Red = action not on schedule for completion / overdue
Page 9 of 131

Council of Governors 15 September 2020
Name of Report Diary Summary
Author
Sir Norman Lamb, Trust Chair
Presented by
Sir Norman Lamb, Trust Chair
Purpose
For information
Period: March 2020 to September 2020
Date Meeting/Event 2nd March Introductory meeting - Interim SLaM Chair Introductory Meeting - PA to Chair Introductory Meeting - Director of Corporate Affairs (Interim) Introductory Meeting - Chief Financial Officer Centre for Society and Mental Health - Craig Morgan, Nikolas Rose,
Benedict Wilkinson – Co Directors Introductory Meeting – Chief Executive 3rd March Introductory Meeting - Geraldine Strathdee – Non-Executive Director Introductory Meeting and briefing for Staff Conference – Communications
Team 4th March Leadership Forum – Executive Members 5th March Staff Conference Kings Fund Mental Health Network Annual Conference and Exhibition
2020 9th March Executive Leadership Team meeting – Trust Executive Introductory meeting - Chief Operating Officer (Interim) Visit to PALS, Patient Safety and Complaints - Deputy Director of Nursing Introductory Meeting - Lead Governors and Deputy Introduction meeting – Chair South West London and St Georges Hospital 11th March Introductory Meeting - Director of Communications Trust values Day Introductory meeting - Prof Ian Everall – Non-Executive Director Introductory Meeting - Director Strategy and Commercial 12th March Introductory Meeting - Anna Walker – Non-Executive Director Introductory Meeting - Medical Director SLaM Board Development – Board Members 18th March SLAM/South West London and St Georges Chair, CEO and SID meeting Introductory Meeting - Mike Franklin - Non-Executive Director Introductory Meeting - Director of Human Resources Introductory Meeting – Béatrice Butsana-Sita – Non-Executive Director 19th March Chief Executive and Director of Corporate Affairs (Interim) – Catch up
Page 10 of 131

Introductory Meeting - Director of Nursing (Interim) 23rd March Human Resource Director - Remuneration Committee Briefing Introductory Meeting – Duncan Hames - Non-Executive Director 24th March Remuneration Committee Meeting 25th March Joint Introductory Meeting – Chief Executive and - Directorate Leadership
– CAMHS 26th March NHS Confed - COVID-19 - Conference Call Introductory Meeting - Chair Camden and Islington Geraldine Strathdee – Non-Executive Director Chief Executive - Trust Live Broadcast Introductory Meeting - Renuka Jeyarajah-Dent - NeXT Director Director of Corporate Affairs (Interim) - Board Briefing Board Meeting preparation 30th March Chief Executive – Catch up 31st March Cavendish Square Group Chairs' Zoom Meeting Chief Executive - Trust Live Broadcast Trust Board Meeting – Part II Trust Board Meeting – Part I 1st April Chief Executive – Catch up 2nd April NHS Confed COVID-19 – Conference Call Chief Executive – Trust Live Broadcast 3rd April Chief Executive – Catch up 6th April Introductory Meeting - Director Performance and Contracts Chief Executive – Catch up 7th April Director of Corporate Affairs (Interim) – 1-2-1 Chief Executive – Trust Live Broadcast Introductory Meeting - Chair, Oxleas NHS Foundation Trust Chief Executive – 1-2-1 Introductory Meeting - Trust Director of Psychology and Psychotherapy 8th April Introductory Meeting - Chair Guy's and St Thomas's NHS Foundation
Trust Medical Director – Catch up Service Delivery Board Chief Executive – Catch up Introductory Meeting – Clinical Director, Mind and Body Programme,
King’s Health Partners Managing Director, Maudsley Learning 9th April Joint Introductory Meeting – Chief Executive and Croydon and BDP Introductory Meeting - HeLived Experience Network - Helen Edwards –
Non-Executive Director Chief Executive – Trust Live Broadcast 14th April Chief Executive – Trust Live Broadcast Chief Executive, Vice Dean of Research, Institute of Psychiatry - to look at
Research and Modelling Joint Introductory Meeting – Chief Executive, Non-Executive Directors -
Directorate Leadership – Lambeth Joint Introductory Meeting – Chief Executive, Non-Executive Directors -
Directorate Leadership - Southwark and Addictions 15th April Introductory Meeting - Project Manager - Supported Employment Services BAME Meeting
Page 11 of 131

Introductory Meeting – Non-Executive Directors, Head of Inclusion, Recovery, Professional Head of Occupational Therapy and AHPs
No.10's interest in our Patient and Carer Race Equality Framework - Director of Organisation and Community and Freedom to Speak Up Guardian and Consultant Psychiatrist
Matt Quinton - BBC - follow up interview 16th April Governance and Covid-19 Conference Call Chief Financial Officer – Catch up Chief Executive – Trust Live Broadcast 17th April Chief Officer Lambeth CCG - Lambeth Living Well Network 20th April Introductory Meeting - with HeLived Experience Network Hayes MP and
Andy Simmons, Research Manager Chief Financial Officer – Catch up 21st April Chief Executive – Trust Live Broadcast Quality Committee June Mulroy – Non-Executive Director Catch up Chief Executive – Catch up Virtual Board Meeting - HCAS Payment and Succession Planning 22nd April Introductory Meeting - Deputy Medical Director and NED's Introductory Meeting - Director QI and SLaM Partners and Non-Executive
Director Introductory Meeting - Chief Executive, Maudsley Charity, Chair, Maudsley
Charity and Non-Executive Director 23rd April Governance and Covid-19 Conference Call Weekly Update Meeting - Non-Executive Directors, Executive Directors,
and Director of Corporate Affairs (Interim) Chief Executive – Trust Live Broadcast Introductory Meeting - Florence Eshalomi MP Mental Health Champions Meeting 24th April Introductory Meeting - Harriet Harman, MP 28th April Chief Executive – Trust Live Broadcast Cavendish Square Group Chairs' Meeting Introductory meeting - Chair Lewisham and Greenwich NHS Trust Chief Executive – Catch up 29th April South West London Health Provider Chairs Introductory Meeting - Chief Information Officer Meeting to discuss Future Modelling Introductory Meeting - Neil Coyle MP 30th April Chief Executive – Catch up Introductory Meeting - Associate Director of Strategy and Non Executive
Directors Weekly Update Meeting - Non-Executive Directors, and Director of
Corporate Affairs (Interim) Chief Executive – Live Trust Broadcast Governance and Covid-19 Conference Call Introductory Meeting - Chair of Croydon Health Services NHS Trust 1st May London Chairs and Sir David Sloman briefing meeting Good Governance in times of crisis: The NHS Non-Executive Director
Meeting Strategy Approach Meeting
Page 12 of 131

Director of Corporate Affairs (Interim) - Catch up Mike Franklin – Non-Executive Director – Catch up Duncan Hames – Non-Executive Director – Catch up 4th May Introductory Meeting - Jill Lockett, Managing Director King's Health
Partners, Robert Lechler, Executive Director, King's Health Partners 5th May Chief Executive – Live Trust Broadcast Mental Health Research - and The Royal Foundation Chief Executive – Catch up Governor / Board meeting Introductory Meeting - Lead, South East London Integrated Care System Director of Communications - Mental Health Summit 6th May BRC Strategy Development Workshop - Prevention Introductory Meeting - London Regional Director Chair South West London and St Georges - Catch up Meeting 7th May Governance and Covid-19 Chairs Conference Call Béatrice Butsana-Sita, Non-Executive Director – Catch up Good Governance - Staff Wellbeing and Reflections Non-Executive Directors and Director of Corporate Affairs (Interim) –
Catch up Chief Executive – Live Trust Broadcast SLaM STAR Presentation – Lewisham Anna Walker, Non-Executive Director - SLaM Strategy Chief Executive – Catch up Leader of the Southwark Council - Covid-19 Mental Health Prevention
Summit 11th May ICS COVID Recovery - Chair meeting 12th May Chief Executive – Live Trust Broadcast Quality Centre Meeting Equalities and Workforce Committee Director of Corporate Affairs (Interim) – 1-2-1 Chief Executive – Catch up 13th May Renuka Jeyarajah-Dent, Non-Executive Director – Board Strategy Service Delivery Board Covid-19 Mental Health Prevention Summit - Leader of LAMBETH
Council, Cabinet Member for health and Social Care Ian Everall, Non-Executive Director – Board Strategy 14th May Social Minds, Chief Executive – Board Work Governance and Covid-19 Chairs Conference Call Covid-19 Mental Health Prevention Summit - Deputy Mayor and cabinet
member for health and adult social care Lewisham Director of Corporate Affairs (Interim) – Board Briefing Chief Executive – Live Trust Broadcast Chief Executive – 1-2-1 NEDs and Director of Corporate Affairs (Interim) – Catch up Covid-19 Mental Health Prevention Summit - Leader of the Council
Croydon and Boroughs Mental Health Champion Board Meeting preparation Cavendish Square Group: CEO meeting 18th May Chief Operating Officer (Interim) – Catch up
Page 13 of 131

19th May Chief Executive – Live Trust Broadcast Director of Corporate Affairs (Interim) – Board Briefing Non-Executive Director /Governor meeting Trust Board Meeting – Part II Trust Board Meeting – Part I 20th May Lambeth Alliance - Denis O'Rouke Introductory Meeting - Chair, South East London Integrated Care System
and Norman Lamb Joint NHS and Council Commissioner for Mental Health Croydon Services
- Developments in Croydon BME Network Meeting 21st May Governance and Covid-19 Chairs Conference Call Governor/Board meeting NEDs and Director of Corporate Affairs (Interim) – Catch up Chief Executive – Live Trust Broadcast King’s Health Partners - Joint Boards meeting Chief Executive – Catch up 22nd May Director of Communications – Summit Agenda setting 26th May Board Development Chief Executive – Live Trust Broadcast Jacqui Dyer Preparation for Mental Health Prevention Summit 27th May Cavendish Square Group - Chairs monthly meeting The Pears Maudsley Centre For Children And Young People – Briefing Team Time - Coping with Work during COVID-19 Introductory meeting - South London Partners (SLP) Director and Non-
Executive Directors Natalie Creary – Black Thrive 28th May Introductory meeting - Director of Research and Development and Non-
Executive Directors Governance and Covid-19 Chairs Conference Call Chief Executive – Catch up Local Strategic Partnership - Weekly Coivd-19 Update NEDs and Director of Corporate Affairs (Interim) – Catch up Chief Executive – Live Trust Broadcast London Chairs Meeting with Sir David Sloman Geraldine Strathdee, Non-Executive Director – Catch up 29th May Good Governance in times of crisis: The NHS Non-Executive Director
Meeting 2nd June Ian Everall, Non-Executive Director – Catch up Chief Executive – Live Trust Broadcast Chief Executive – Catch up Urgent South London Mental Health Prevention Summit 2020 Breakout session 2: Covid-19 mental health and community resilience 3rd June Non-Executive Directors and Director of Corporate Affairs (Interim) –
Catch up Introductory Meeting - Director of Children's Services, and Non-Executive
Directors Introductory Meeting - Executive Director leading on Croydon collaborative
approach to localities
Page 14 of 131

4th June Director of Performance, Contracts and Operational Assurance – Catch up Governance and Covid-19 MH Chairs Conference Call Chief Executive – Catch up Chief Executive – Live Trust Broadcast Introductory Meeting - Chair NHS South East London CCG Provost and Senior Vice President (Health) Kings College London -
Stakeholder panel 5th June Strategy Discussion – Chief Executive and Social Minds Good Governance - Engage, Engage, Engage - Patient and Communities Chair – Guys and St Thomas Foundation Trust – Catch up 9th June ICS COVID Recovery - Chair meeting Chief Executive – Live Trust Broadcast Lewisham MP – Catch up Director of Corporate Affairs (Interim) – 1-2-1 Chief Executive – Catch up The Policy Institute - King's LBC / NHS Meeting 10th June Introductory Meeting - Interim Chief Operating Officer Croydon Health Services Chair – Catch up Director of Corporate Affairs (Interim) – Council of Governors Briefing Jonathan Campion, Consultant Psychiatrist, Croydon – catch up Virtual Lived Experience Network Teams Meeting 11th June NEDs and Director of Corporate Affairs (Interim) – Catch up SLaM's Dragons' Den Chief Executive – Live Trust Broadcasts Introduction/briefing - Lead for Inclusion, Recovery, Occupational Therapy
and AHP and the two co-Chairs of the Trust Service User Involvement Committee
Chief Executive – Catch up Council of Governors meeting 12th June Mental health in Lambeth and Southwark 15th June Cavendish Square Group Trust Chairs' Meeting 16th June Dr Michael Sanders, Reader in Public Policy, The Policy Institute at King’s CoG - Lead Governor, Deputy Meeting and Director of Corporate Affairs
(Interim) – Catch up Charity Commission - Alzheimer's Society – Jeremy Hughes 17th June Al Beck - Director of Psychology and Psychotherapy, Psychology – Catch
up Rachel Eborall - Deputy Head, Inclusion and Peer Worker Development Ermias Alemu - Project and Training Services Manager Alice Debelle - ST (Specialty Training Doctor), Bethlem Adolescent Unit Introductory Meeting - Millie Banerjee, Chair, NHS Blood and Transplant
and Norman Lamb, Chair 18th June Social Work in Community Recovery and Resilience Chief Executive – Catch up NEDs and Director of Corporate Affairs (Interim) – Catch up Chief Executive – Live Trust Broadcast Mental Health Law Committee Meeting Renuka Jeyarajah-Dent – NED – Catch up
Page 15 of 131
19th June Mike Franklin – Non-Executive Director – Catch up 23rd June Chief Executive – Catch up Performance Indicator Review Meeting – Chief Executive, Non-Executive
Directors, Director of Corporate Affairs (Interim) and Interim Chief Operating Officer
Introductory Meeting - Faisil Sethi – Consultant Psychiatrist Chief Executive and Chair – South West London and St Georges, Chief
Executive SLaM. 25th June Chief Executive – Catch up Non-Executive Directors and Director of Corporate Affairs (Interim) –
Catch up Social Minds, Chief Executive - Strategy Catch up SLaM and LGT Chairs and Chief Executive - Meeting Chief Executive – Live Trust Broadcast London Chairs Meeting – David Sloman 30th June Ian Everall – NED – Catch up Chief Executive – Catch up Anna Walker – NED – Catch up Tutiette Thomas and Barbara Lindsay Non-Executive Meeting Board Development Meeting – Board Members 1st July Director of Performance, Contracts and Operational Assurance – Catch up 2nd July Governance and Covid-19 MH Chairs Conference Call Chief Executive – Catch up CAMHS - Ruth Kennedy, Perrie Ballantyne and Director of Performance,
Contracts and Operational Assurance (Interim) 7th July Quality Committee Equalities and Workforce Committee Director of Corporate Affairs (Interim) – 1-2-1 8th July Social Minds, Chief Executive - Strategy Catch up Joe Rafferty, Chief Executive, Beatrice Fraenkel, Chair - Merseycare,
Chief Executive, SLAM – Meeting 9th July Governance and Covid-19 MH Chairs Conference Call Chief Executive – Live Trust Broadcast Chairs Briefing with Mark Britnell – Global Health of Heathcare KPMG 10th July Medical Director – Catch up 13th July Chief Financial Officer – Catch up 14th July Helen Edwards- Non-Executive - Catch up Discussion - Mental Health in South London Karin Orman - Assistant Director- Professional Practice - Royal College of
Occupational Therapists Business Development Investment Committee and Financial Performance
Committee Non-Executive Directors and Director of Corporate Affairs (Interim) –
Catch up 15th July Renuka Jeyarajah-Dent – Non-Executive Director – Catch up Sophie Browning - Consultant Clinical Psychologist/Lead Psychologist for
Inpatients CAMHS Jessie Emilion - Principal Adult CAT Psychotherapist
Page 16 of 131

Ethnicity Data – Board Members, Non-Executive Directors and Chief Executive
Introductory Meeting - John Palmer - Deputy Chief Executive King College Hospital
16th July Mike Franklin – Non-Executive Director – Catch up Family and Careers Committee Chief Executive – Catch up Ian Everall – Non-Executive Director – Catch up 17th July Anna Walker – Non-Executive Director – Catch up 20th July London Transition Board - Education Sub-Group South East Focused Support Team Meeting Mental Health Research Group 21st July June Mulroy – Non-Executive Director – Catch up King’s Health Partners Board Meeting LGBT+ staff network 22nd July Trust Strategy and Commercial Director - Estates Commercialisation London Regional Roadshow Fergus Kane, Lee Roach, Jonathan Burns Non-Executive Director Training for AHM role 23rd July Chief Executive – Catch up Social Minds, Chief Executive – Strategy Update Chief Executive – Live Trust Broadcast Director of Corporate Affairs (Interim) - Board Briefing 24th July NExT Non-Executive Director scheme 28th July Board Development – Board Members Non-Executive Members and Governors Meeting Trust Board Meeting – Part II Trust Board Meeting – Part I ICS Chairs meeting 29th July South West London Provider Chair's Meeting Chief Executive – Catch up Time to Talk Jenny Drift - Consultant Psychiatrist, Homeless Outreach Team (START) Julian Onwumere, Senior Lecturer and Consultant Clinical Psychologist,
IoPPN 30th July Beatrice Butansa-Sita – Non-Executive Director – Catch up Governance and Covid-19 MH Chairs Conference Call Non-Executive Directors and Director of Corporate Affairs (Interim) –
Catch up South London Covid-19 Mental Health Crisis Prevention Taskforce Chief Executive – Live Trust Broadcast Introductory Meeting - Tim Dee, SLaM Governor 3rd August London Transition Board - Education Sub Group 4th August Remuneration Committee Social Minds, Non-Executive Directors – Strategy update Chair – South West London and St Georges Anna Walker – Non-Executive Director – Appraisal 5th August Duncan Hames – Non-Executive Director – Appraisal
Page 17 of 131

Sean Cross - Consultant Psychiatrist, Mental Health Liaison Service (King's College Hospital) – Catch up
Louise Edwards - Director of Strategy, Beatrice Fraenkel, Chair – Merseycare – Meeting
6th August Director of Performance, Contracts and Operational Assurance – Catch up Governance and Covid-19 MH Chairs Conference Call Chief Executive – Trust Live Broadcast Virtual Team Visit - CAMHS Response Team and Chief Executive Chief Executive – Catch up 7th August Social Minds, Chief Executive – Strategy update Annual Leave 20th August – 6th September 10th August Introductory Meeting - Neil Jackson- Director of Capital, Estates and
Facilities Strategy Discussion - Social Minds, Board Members and Non-Executive
Directors 11th August Estates commercialisation - Sub group of the Board Béatrice Butsana-Sita – Non-Executive Director – Appraisal 12th August Chief Executive – Catch up The Impact of Covid-19 and Psychological Distress NHS Providers - Chair induction Cavendish Square Group Chairs' Monthly Meeting 13th August Director of Corporate Affairs (Interim) – Catch up Governance and Covid-19 MH Chairs Conference Call Kate Lillywhite - Programme Director – King’s Health Partners Institute of
Diabetes, Endocrinology and Obesity Chief Executive – Live Trust Broadcast
14th August Chief Executive – Catch up 17th August Transition Board - Education Sub Group 18th August Ian Everall – Non-Executive Director – Appraisal Valsraj Koravangattu - Consultant Psychiatrist and Associate Clinical
Director, Croydon, Trust Ambitions update – Social Minds and Non-Executive Directors Mike Franklin – Non-Executive Director - Appraisal Renuka Jeyarajah-Dent – Non-Executive Director - Reflections and Setting
Objectives 19th August Chief Executive – Catch up HeLived Experience Network Edwards – Non-Executive Director –
Reflections and Setting Objectives Introductory Meeting - Paul Jenkins – Chief Executive Tavistock and
Portman Social Minds, Chief Executive – Strategy Update 20th August – 6th September – Annual Leave 8th September Quality Committee Equalities and Workforce Committee Director of Corporate Affairs (Interim) – 1-2-1 ICS Chair Meeting 9th September Governor Luke Sorba – introductory meeting June Mulroy – Non-Executive Director – Catch up Geraldine Strathdee – Non-Executive Director – Appraisal Director of Corporate Affairs (Interim) – Risk Assessment
Page 18 of 131

Chief Executive – Catch up Council of Governors - Lead Governor and Deputy, Director of Corporate
Affairs (Interim) – Meeting 10th September Governance and Covid-19 MH Chairs Conference Call World Suicide Prevention Day conference and Service of Remembrance 11th September Cavendish Square Group CEO Meeting, with London ICS Chairs Board Introduction Session – Children Young Programme and Douglas
Bennet House 14th September Cavendish Square Group - Chairs' Meeting PMOA Involvement and participation Team Meeting 15th September Anna Walker – NED – Catch up Béatrice Butsana-Sita – Non-Executive Director – Catch up Chief Executive, Vice Dean of Research Institute of Psychiatry – BRC in
Progress Chief Executive – Catch up Director of Corporate Affairs (Interim) – Council of Governors Briefing Council of Governors Meeting Annual Members Meeting 16th September Mandatory Training Non-Executive Directors Meeting 17th September Social Minds, Chief Executive – Strategy Update Governance and Covid-19 MH Chairs Conference Call Chief Executive – Catch up Director of Corporate Affairs (Interim) – Board Briefing NIHR Maudsley BRC Trainees’ Conference Invitation: Showcasing 21st September Maudsley Charity Board of Trustees Away Day Session 22nd September Governor Jim Canning – introductory meeting Audit Committee Non-Executive Directors and Governors Meeting Trust Board Part II Trust Board Part I 23rd September Chief Executive – Catch up 24th September NHS Provider – Non-Executive Director Induction 25th September NHS Provider – Non-Executive Director Induction 28th September Kings Health Partners Board Meeting 29th September Ian Everall – NED – Catch up Introductory Meeting - Stephani Hatch - Professor of Sociology and
Epidemiology Department of Psychological Medicine - Institute of Psychiatry
Mike Franklin – Non-Executive Director – Catch up Introductory Meeting – John Jenkins Partnership Committees in Common 30th September Lived Experience Network Edwards – Non-Executive Director – Catch up Chief Executive – Catch up Director of Performance, Contracts and Operational Assurance – Catch up Director of Corporate Affairs (Interim) – Catch up
Page 19 of 131

Council of Governors 15 September 2020
Name of Report External Auditor’s report
Author
Sarah Ironmonger, Key Audit Partner, Grant Thornton LLP
Presented by
Sarah Ironmonger, Key Audit Partner, Grant Thornton LLP
Purpose
For information
Page 20 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
The Audit Findings Reportfor South London and Maudsley NHS Foundation Trust Year ended 31 March 2020
16 June 2020
Page 21 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
2
Contents
Section Page
1. Headlines 3
2. Financial statements 5
3. Value for money 15
4. Independence and ethics 18
Appendices
A. Action plan 19
B. Follow up of prior year recommendations 21
C. Audit adjustments 23
D. Fees 25
E. Audit Opinion 26
The contents of this report relate only to those matters which came to our attention during the conduct of our normal audit procedures which are designed for the purpose of expressing our opinion on the financial statements. Our audit is not designed to test all internal controls or identify all areas of control weakness. However, where, as part of our testing, we identify control weaknesses, we will report these to you. In consequence, our work cannot be relied upon to disclose all defalcations or other irregularities, or to include all possible improvements in internal control that a more extensive special examination might identify. This report has been prepared solely for your benefit and should not be quoted in whole or in part without our prior written consent. We do not accept any responsibility for any loss occasioned to any third party acting, or refraining from acting on the basis of the content of this report, as this report was not prepared for, nor intended for, any other purpose.
Grant Thornton UK LLP is a limited liability partnership registered in England and Wales: No.OC307742. Registered office: 30 Finsbury Square, London, EC2A 1AG. A list of members is available from our registered office. Grant Thornton UK LLP is authorised and regulated by the Financial Conduct Authority. Grant Thornton UK LLP is a member firm of Grant Thornton International Ltd (GTIL). GTIL and the member firms are not a worldwide partnership. Services are delivered by the member firms. GTIL and its member firms are not agents of, and do not obligate, one another and are not liable for one another’s acts or omissions.
Your key Grant Thornton team members are:
Sarah Ironmonger
Key Audit Partner
T: 020 7865 2997
Matt Dean
Senior Audit Manager
T: 020 7728 3181
Kit Bissell
In-Charge Accountant
T: 020 7728 2992
Page 22 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
3
1. HeadlinesThis table summarises the key findings and other matters arising from the statutory audit of South London and Maudsley NHS Foundation Trust (‘the Trust’) and the preparation of the Trust's financial statements for the year ended 31 March 2020 for those charged with governance.
Covid-19 The outbreak of the Covid-19 coronavirus pandemic has had a significant impact on the normal operations of the Trust in terms of dealing with the impact of the pandemic, which has impacted mental health providers as much as acute trusts, albeit in different ways.
Given the unprecedented operational challenge for Trusts, the Department of Health and Social Care (DHSC) extended the deadline for preparation of the financial statements up to 27 April 2020, with flexibility to extend to 11 May 2020, and the date for audited financial statements to 25 June 2020.
We have considered emerging guidance issued by the Financial Reporting Council, NHS Improvement and NHS England and actively contributed to audit firm and NAO technical meetings where the impact of the virus on the financial reporting disclosures and audit approach has been discussed.
We updated our audit risk assessment to consider the impact of the pandemic on our audit and issued an audit plan addendum on 5 May 2020. In that addendum we reported an additional financial statement risk in respect of Covid-19 and highlighted the impact on our VfM approach. Further detail is set out on page 7.
Restrictions for non-essential travel has meant both you and us have had to deliver the audit via remote access working arrangements, which has included accessing financial systems remotely, video calling, physical verification of completeness and accuracy of information produced by the entity. However we have been able to work well with you to keep the overall impact on the audit to a minimum, as evidenced by the progress made and documented within this Report.
FinancialStatements
Under International Standards of Audit (UK) (ISAs) and theNational Audit Office (NAO) Code of Audit Practice ('theCode'), we are required to report whether, in our opinion:
• the Trust's financial statements give a true and fair view of the financial position of the Trust and its income and expenditure for the year; and
• the Trust’s financial statements, and the parts of the Remuneration and Staff Report to be audited, have been properly prepared in accordance with International Financial Reporting Standards, as interpreted and adapted by the Department of Health and Social Care (DHSC) and the DHSC group accounting manual 2019/20 (GAM).
We are also required to report whether other information published together with the audited financial statements in the Annual Report, is materially inconsistent with the financial statements or our knowledge obtained in the audit or otherwise appears to be materially misstated.
Our audit work was completed on remotely during April to June 2020. Our findings are summarised on pages 5 to 14. To date, we have not identified any adjustments to the financial statements that impact on your retained surplus position, but have identified some disclosure amendments. These amendments are detailed in Appendix C. We have also raised recommendations for management as a result of our audit work in Appendix A. Our follow up of recommendations from the prior year’s audit are detailed in Appendix B.
Our work is substantially complete and we have not identified any matters of which we are aware that would require modification of our audit opinion, shown at Appendix E, or material changes to the financial statements.
We have concluded that the other information to be published with the financial statements, is consistent with our knowledge of your organisation and the financial statements we have audited.
Our audit report opinion was unqualified.
Page 23 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
4
AcknowledgementsWe would like to take this opportunity to record our appreciation for the assistance provided by the finance team and other staff amidst the pressure they were under during these unprecedented times.
Value for Money arrangements
Under the National Audit Office (NAO) Code of Audit Practice ('the Code'), we are required to report if, in our opinion, the Trust has not made proper arrangements to secure economy, efficiency and effectiveness in its use of resources ('the value for money (VFM) conclusion’).
We have completed our risk based review of the Trust’s value for money arrangements. We have concluded that South London and Maudsley NHS Foundation Trust has proper arrangements to secure economy, efficiency and effectiveness in its use of resources.
We have nothing to report by exception - our findings are summarised on pages 15 to 17.
Statutory duties The National Health Service Act 2006 (‘the Act’) also requires us to:
• report to you if we have applied any of the additional powers and duties ascribed to us under the Act; and
• to certify the closure of the audit.
We have not exercised any of our additional statutory powers or duties.
We have completed the majority of work under the Code and expect to be able to certify the completion of the audit when we give our audit opinion.
1. Headlines
Page 24 of 131
Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20 5
Overview of the scope of our audit
This Audit Findings Report presents the observations arising from the audit that are significant to the responsibility of those charged with governance to oversee the financial reporting process, as required by International Standard on Auditing (UK) 260 and the Code of Audit Practice (‘the Code’). Its contents have been discussed with management.
As auditor we are responsible for performing the audit, in accordance with International Standards on Auditing (UK) and the Code, which is directed towards forming and expressing an opinion on the financial statements that have been prepared by management with the oversight of those charged with governance. The audit of the financial statements does not relieve management or those charged with governance of their responsibilities for the preparation of the financial statements.
Audit approach
Our audit approach was based on a thorough understanding of the Trust's business and is risk based, and in particular included:
• An evaluation of your internal control environment, including your IT systems and controls;
• Substantive testing on significant transactions and material account balances, including the procedures outlined in this report in relation to the key audit risks
We have had to alter our audit plan, as communicated to you on 5 May 2020, to reflect our response to the Covid-19 pandemic. The main change was the identification of an additional Significant Risk in respect of our accounts audit due to the impact of Covid-19 across the accounts, further detail on which can be seen on page 8.
Conclusion
We have completed our audit of your financial statements, and have issued an unqualified audit opinion following the Audit Committee meeting on 16 June 2020, as detailed in Appendix E.
Financial statements
2. Summary
Page 25 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20 6
2. SummaryFinancial statements
.
Our approach to materiality
The concept of materiality is fundamental to the preparation of the financial statements and the audit process and applies not only to the monetary misstatements but also to disclosure requirements and adherence to acceptable accounting practice and applicable law.
Materiality levels remain the same as reported in our Audit Plan.
We detail in the table below our determination of materiality for you.
Trust Amount (£) Qualitative factors considered
Materiality for the financial statements 8,000,000 Overall Materiality is based on your Gross Expenditure over the year, which has not moved significantly from the prior year, hence why we left overall Materiality unchanged from our planning assessment.
Performance materiality 6,000,000 Performance Materiality is based on a percentage of the overall materiality.
Trivial matters 300,000 This balance is set at £300k as this is the reporting threshold for any errors identified as part of our work on the National Audit Office’s Whole of Government Accounts (WGA) exercise.
Materiality for Senior Manager Salaries 100,000 We selected a value of £100,000 for this area as an error of this size would impact on the banding within which these Managers would sit, which we have determined is something that the users of the Accounts would be interested in.
Page 26 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20 7
Risks identified in our Audit Plan Addendum Commentary
Covid–19
The global outbreak of the Covid-19 virus pandemic has led to unprecedented uncertainty for all organisations, requiring urgent business continuity arrangements to be implemented. We expect current circumstances will have an impact on the production and audit of the financial statements for the year ended 31 March 2020, including and not limited to;
• Remote working arrangements and redeployment of staff to critical front line duties may impact on the quality and timing of the production of the financial statements, and the evidence we can obtain through physical observation
• Volatility of financial and property markets will increase the uncertainty of assumptions applied by management to asset valuation and receivable recovery estimates, and the reliability of evidence we can obtain to corroborate management estimates
• Financial uncertainty will require management to reconsider financial forecasts supporting their going concern assessment and whether material uncertainties have arisen; and
• Disclosures within the financial statements will require significant revision to reflect the unprecedented situation and its impact on the preparation of the financial statements as at 31 March 2020 in accordance with IAS1.
We therefore identified the global outbreak of the Covid-19 virus as a significant risk, which was one of the most significant assessed risks of material misstatement, and a key audit matter.
As part of our audit work we have completed the following:
• We worked with management to understand the implications the response to the Covid-19 pandemic has on the organisation’s ability to prepare the financial statements and update financial forecasts and assess the implications for our materiality calculations
• We liaised with other audit suppliers, regulators and government departments to co-ordinate practical cross sector responses to issues as and when they arise
• Evaluated the adequacy of the disclosures in the financial statements that arose in light of the Covid-19 pandemic.
• Evaluated whether sufficient audit evidence can be obtained in the absence of physical verification of assets through remote technology
• Evaluated whether sufficient audit evidence can be obtained to corroborate significant management estimates such as asset valuations and recovery of receivable balances
• Evaluated management’s assumptions that underpin the revised financial forecasts and the impact on management’s going concern assessment
• Discussed with management any potential implications for our audit report if we have been unable to obtain sufficient audit evidence
From the work performed to date, we have identified that your Property Valuations have been provided with a ‘material uncertainty’ attached to them, following the guidance issued by RICS to all valuers following the Covid-19 outbreak. As a result, you have now included a material uncertainty in your accounts relating your valuation, which leads to us disclosing an Emphasis of Matter in our audit opinion. An Emphasis of Matter paragraph is not a qualification, it is used to highlight the facts in a particular area to the reader of the accounts where this is significant to the overall understanding of the financial statements.
We have also been unable to obtain the evidence supporting the approval of some of the journals selected for testing, due to the remote working arrangements which have been in place since the outbreak. We have obtained sufficient assurance that the journals are proper and appropriate, but due to the authorisations being held in paper form, we have been unable to confirm whether the correct approval process was followed for these journals. We have however obtained assurance from you over the appropriateness of these journals outside of the normal process.
Financial statements
This section provides commentary on the significant audit risks communicated in the Audit Plan and the Addendum.
2. Significant risks
Page 27 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20 8
Risks identified in our Audit Plan Commentary
Management override of controls
Under ISA (UK) 240 there is a non-rebuttable presumed risk that the risk of management over-ride of controls is present in all entities. You face external pressures to meet agreed targets, and this could potentially place management under undue pressure in terms of how they report performance.
We therefore identified management override of control, in particular journals, management estimates and transactions outside the course of business as a significant risk, which was one of the most significant assessed risks of material misstatement.
As part of our audit work we have completed the following:
• evaluated the design effectiveness of management controls over journals
• analysed the journals listing and determined the criteria for selecting high risk unusual journals
• tested unusual journals made during the year and the accounts production stage for appropriateness and corroboration
• gained an understanding of the accounting estimates and critical judgements applied by management and considered their reasonableness
As mentioned on the previous page, we have been unable to confirm that the correct approval process has been followed for some of the detailed journals selected for testing due to the remote working arrangements which have been in place since the Covid-19 outbreak. We have obtained sufficient assurance that the journals in question are proper and appropriate, but due to the authorisations being held in paper form, we have been unable to confirm whether the correct approval process was followed for these journals. We have however obtained assurance from you over the appropriateness of these journals outside of the normal process
Our audit work has not identified any further issues in respect of this risk.
Financial statements
2. Significant risks (continued)
Page 28 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20 9
Risks identified in our Audit Plan Commentary
Improper revenue recognition
Trusts are facing significant external pressure to restrain budget overspends and meet externally set financial targets, coupled with increasing patient demand and cost pressures. In this environment, we have considered the rebuttable presumed risk under ISA (UK) 240 that revenue may be misstated due to the improper recognition of revenue.
We have rebutted this presumed risk for the revenue streams of the Trust that areprincipally derived from contracts that are agreed in advance at a fixed price. Wehave determined these to be income from:
• Block contract income element of patient care revenues
• Education & training income
We have not deemed it appropriate to rebut this presumed risk for all other material streams of patient care income and other operating revenue.
We have therefore identified the occurrence and accuracy of these income streams and the existence of associated receivable balances as a significant risk, which was one of the most significant assessed risks of material misstatement, and a key audit matter.
As part of our audit work we have completed the following:
• evaluated the Trust’s accounting policy for recognition income from patient care activities and other operating revenue for appropriateness and compliance with the DHSC Group Accounting Manual 2019/20;
• updated our understanding of the Trust's system for accounting for income from patient care activities and other operating revenue, and evaluated the design of the associated controls;
Patient Care Income
• using the DHSC mismatch report, we have investigated unmatched revenue and receivable balances over the NAO £0.3 million threshold, corroborating the unmatched balances used to your supporting evidence;
• agreed, on a sample basis, income from contract variations and year end receivables to signed contract variations, invoices or other supporting evidence such as correspondence from your commissioners
• evaluated your estimates and the judgments made by management in respect of significantcontract variations with regard to corroborating evidence in order to arrive at the total income from contract variations recorded in the financial statements.
Other Operating Revenue
• agreed, on a sample basis, income and year end receivables from other operating revenue to invoices and cash payment or other supporting evidence
• for the Provider Sustainability Funding, we have agreed income recognised in Q1 – Q3 to NHS Improvement notifications;
• for Quarter 4, we have obtained supporting evidence to confirm whether you have met NHS Improvement requirements for recognising Q4 income.
From the testing performed to date, we have identified that the Trust is currently holding an allowance for credit losses of £1.6 million against its intra-NHS receivables balances, despite this being contrary to NHS business rules. Whilst we understand your rationale for this treatment, as it is against NHS business rules we are required to report this as an unadjusted misstatement in the accounts.
Our audit work has not identified any further issues in respect of this risk.
Financial statements
2. Significant risks (continued)
Page 29 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20 10
Risks identified in our Audit Plan Commentary
Valuation of land and buildings
You revalue your land and buildings on an annual basis to ensure that the carrying value is not materially different from the current value at the financial statements date. This valuation represents a significant estimate by management in the financial statements.
Management has engaged the services of a valuer to estimate the current value as at 31 March 2020.
The valuation of land and buildings is a key accounting estimate which is sensitive to changes in assumptions and market conditions.
We therefore identified valuation of land and buildings, particularly revaluationsand impairments, as a significant risk, which was one of the most significant assessed risks of material misstatement, and a key audit matter.
As part of our audit work we have completed the following:
• evaluated management's processes and assumptions for the calculation of the estimate, the instructions issued to the valuation experts and the scope of their work
• evaluated the competence, capabilities and objectivity of the valuation expert
• we have obtained an understanding from the valuer of the basis on which the valuations were carried out
• challenged the information and assumptions used by the valuer to assess completeness and consistency with our understanding
• tested, on a sample basis, revaluations made during the year to ensure they have been input correctly into your asset register
• evaluated the assumptions made by management for any assets not revalued during the year and how management has satisfied themselves that these are not materially different to current value.
From the work performed to date, we have identified that your Property Valuations have been provided with a ‘material uncertainty’ attached to them, following the guidance issued by RICS to all valuers following the Covid-19 outbreak. As a result, you have included a material uncertainty in your accounts relating to this area, which leads to us disclosing an Emphasis of Matter in our audit opinion covering this area. An Emphasis of Matter paragraph is not a qualification, it is used to highlight the facts in a particular area to the reader of the accounts where this is significant to the overall understanding of the financial statements.
Our work has also identified that you are currently holding £10.5 million of fully depreciated assets held on your Property, Plant and Equipment Register, which has no overall impact on the value of these Assets in the Accounts. You should look to undertake an exercise to determine whether these assets are still in use, or are now obsolete and can be removed from the Register.
Our audit work has not identified any further issues in respect of this risk.
Financial statements
2. Significant risks (continued)
Page 30 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for [ANOTHER] Trust | 2019/20 11
Financial statements
This section provides commentary on additional issues and risks which were identified during the course of the audit that were not previously communicated in the Audit Plan and a summary of any significant deficiencies identified during the year.
Issue Commentary Auditor view
IFRS 16 implementation has been delayed by one year
Although the implementation of IFRS 16 has been delayed to 1 April 2021, audited bodies still need to include disclosure in their 2019/2020 statements to comply with the requirement of IAS 8 para 31. As a minimum, we would expect audited bodies to disclose the title of the standard, the date of initial application and the nature of the changes in accounting policy for leases.
As a result of the work you have undertaken to prepare for IFRS16, you identified that one of your existing leases had been treated incorrectly, which had led to an understatement of the future minimum lease commitments for 2018/19 by £18.4 million. The prior year figures have also been adjusted to ensure comparability between the current and prior year figures. Given this item is just a disclosure it has no impact on your reported financial position for the year.
Refer to the disclosure adjustments table later in the Report for the full detail of this adjustment. However the work you have undertaken in year will make the transition to IFRS16 more straight forward for the 2020/21 accounts.
Processing of Starters, Leavers and Changes in Circumstances
Our walkthrough of your payroll processes identified that all starters, leavers and changes in circumstances forms have to be manually printed and sent to SBS in hard copy format, due to SBS not having electronic access to these.
This generates additional manual input into the process, which increases the chance of forms going missing and not being processed correctly or in a timely manner. You should look to allow these forms to be shared electronically to reduce the risk of human error and to make the process more efficient.
Refer to the recommendation raised within the Action Plan section of the Report for confirmation of the issue raised along with management’s response.
2. Significant findings
Page 31 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
12
2. Significant findings – judgements and estimatesFinancial statements
Significant judgement or estimate Summary of management’s approach Audit Comments Assessment
Land and Buildings –£226 million
Other land and buildings comprises £190 million of specialised assets such as such as the main Maudsley and Bethlem Hospital Sites which are required to be valued at depreciated replacement cost (DRC) at year end, on a modern equivalent asset basis. Management has determined the amount of space and location required for ongoing service delivery in the light of their current and projected service needs and have instructed the valuer accordingly. The remainder of land and buildings (£36 million) are not specialised in nature and are required to be valued in existing use (EUV) at year end. You engaged the District Valuer to complete the valuation of properties as at 31 March 2020 on a yearly cyclical basis. 98% of total land and buildings were revalued at 31 March 2020. The revaluation of properties has resulted in a net increase of £4 million.
Management has considered the year end value of non-valued properties/and the potential valuation change in the assets revalued at 31 March 2019, which relates to £4.2 million of Land and Buildings which have not been revalued in year. The reason these assets have not been revalued is because they are held on short term leases, where the fit-out works have been capitalised, and thus would not fit within the normal revaluation assumptions and routines applied by the District Valuer
The total year end valuation of land and buildings was £226 million, a net increase of £4 million from 2018/19 (£222 million).
• We reviewed the work undertaken by the District Valuer in respect of their valuation of the your Assets, and are comfortable with the assumptions applied in respect of these valuations.
• The main item to note in this area is that the valuations provided by the District Valuer have been provided with a material uncertainty attached to them. This is on the basis of guidance issued by RICS to all valuers, on the back of the Covid-19 pandemic.
• The material uncertainty reflects that future market conditions are likely to be significantly different to those conditions which have gone before, and hence values derived using these previous conditions are less likely to reflect future values.
• You have now added a material uncertainty to your accounts in respect of this area, which we will reference in our Opinion via an Emphasis of Matter paragraph.
• We have confirmed the rationale behind the small element of Land and Buildings which have not been revalued, and have obtained sufficient assurance that the carrying value as at the 31st of March 2020 is not materially different to its Fair Value at this date.
Green
Assessment
- Red - We disagree with the estimation process or judgements that underpin the estimate and consider the estimate to be potentially materially misstated
- Amber - We consider the estimate is unlikely to be materially misstated however management’s estimation process contains assumptions we consider optimistic
- Yellow - We consider the estimate is unlikely to be materially misstated however management’s estimation process contains assumptions we consider cautious
- Green - We consider management’s process is appropriate and key assumptions are neither optimistic or cautious
Page 32 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
13
2. Other communication requirementsFinancial statements
We set out below details of other matters which we, as auditors, are required by auditing standards and the Code to communicate to those charged with governance.
Issue Commentary
Matters in relation to fraud We have previously discussed the risk of fraud with the Audit Committee. We have not been made aware of any other incidents in the period and no other issues have been identified during the course of our audit procedures.
Matters in relation to related parties
We are not aware of any related parties or related party transactions which have not been disclosed. You have also amended the disclosures included within the accounts to ensure these comply with the requirements of the NHS Group Accounting Manual.
Matters in relation to laws and regulations
You have not made us aware of any significant incidences of non-compliance with relevant laws and regulations and we have not identified any incidences from our audit work.
Written representations A letter of representation has been requested from the Trust, which is appended at Appendix F.
Confirmation requests from third parties
We obtained direct confirmation from NatWest for the bank balances held under the Government Banking Scheme.
Accounting practices We have evaluated the appropriateness of the Trust’s accounting policies, accounting estimates and financial statement disclosures. As mentioned earlier in the report, we identified that the draft accounts did not include a material uncertainty disclosure in respect of the your Property, Plant and Equipment Valuations, which has subsequently been included in the revised accounts. We have also identified a number of minor disclosure amendments, which management has also agreed to amend. Further detail on these amendments can be seen withinAppendix C.
Audit evidence and explanations/significant difficulties
All information and explanations requested from management was provided, with the exception of the physical evidence supporting the authorisation of a small number of journals, which as they were held in paper form were unable to be provided due to the impact of Covid-19.
The draft Annual Report was provided to audit later than anticipated, with the Remuneration Report received on 5 June 2020 and the remainder of the Report received on 9 June. Within this version there were still a number of areas which required further work. At the current date our work in this area is still in progress, but we are hopeful of bringing this to a conclusion in advance of the formal deadline for submission.
Page 33 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
14
2. Other responsibilities under the Code
Financial statements
Issue Commentary
Other information We are required to give an opinion on whether the other information published together with the audited financial statements (including the Annual Report), is materially inconsistent with the financial statements or our knowledge obtained in the audit or otherwise appears to be materially misstated.
No inconsistencies have been identified. We plan to issue an unmodified opinion in this respect – refer to Appendix E
Auditable elements of Remuneration Report and Staff Report
We are required to give an opinion on whether the parts of the Remuneration Report and Staff Report subject to audit have been prepared properly in accordance with the requirements of the Act, directed by the Secretary of State with the consent of the Treasury.
We have audited the elements of the Remuneration Report and Staff Report, as required by the NHS Group Accounting Manual.
To date, we have nothing to report on these matters, but we will provide an update to Management and the Audit Committee should any issues be identified in our remaining work.
Matters on which we report by exception
We are required to report on a number of matters by exception in a number of areas:
• If the Annual Governance Statement does not meet the disclosure requirements set out in the NHS Foundation Trust Annual Reporting Manual 2019/20 is misleading or inconsistent with the information of which we are aware from our audit
• The information in the annual report is materially inconsistent with the information in the audited financial statements or apparently materially incorrect based on, or materially inconsistent with, our knowledge of the Trust acquired in the course of performing our audit, or otherwise misleading.
• If we have applied any of our statutory powers or duties.
To date, we have nothing to report on these matters, but we will provide an update to Management and the Audit Committee should any issues be identified in our remaining work.
Review of accounts consolidation schedules and specified procedures on behalf of the group auditor
We are required to give a separate audit opinion on the Trust accounts’ consolidation schedules and to carry out specified procedures (on behalf of the NAO) on these schedules under group audit instructions. In the group audit instructions the Trust was selected as a sampled component.
At the current date we are yet to complete our work in this area, and will provide an update to the Audit Committee following the completion of this work where appropriate.
Certification of the closure of the audit
We intend to certify the closure of the 2019/20 audit of the South London and Maudsley NHS Foundation Trust in the audit report, as detailed in Appendix E.
Page 34 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
15
Value for Money
Risk assessment
We carried out an initial risk assessment in March 2020 and identified a significant risk in respect of specific areas of proper arrangements using the guidance contained in AGN03. We communicated these risks to you in our Audit Plan dated 31 March 2020.
We have updated our VFM risk assessment to document our understanding of your arrangements to ensure critical business continuity in the current environment. We have not identified any new VFM risks in relation to the Covid-19 pandemic.
We have continued our review of relevant documents up to the date of giving our report, and have not identified any further significant risks where we need to perform further work.
We carried out further work only in respect of the significant risks we identified from our initial and ongoing risk assessment. Where our consideration of the significant risks determined that arrangements were not operating effectively, we have used the examples of proper arrangements from AGN 03 to explain the gaps in proper arrangements that we have reported in our VFM conclusion.
3. Value for MoneyBackground to our VFM approach
We are required to satisfy ourselves that the Trust has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources and report by exception where we are not satisfied. This is known as the Value for Money (VFM) conclusion.
We are required to carry out sufficient work to satisfy ourselves that proper arrangements are in place at the Trust. In carrying out this work, we are required to follow the NAO's Auditor Guidance Note 3 (AGN 03) issued in November 2019. AGN 03 identifies one single criterion for auditors to evaluate:
“In all significant respects, the audited body takes properly informed decisions and deploysresources to achieve planned and sustainable outcomes for taxpayers and local people.”
This is supported by three sub-criteria, as set out below:
Informed decision making
Value for Money
arrangements criteria
Sustainable resource
deployment
Working with partners & other third
parties
Page 35 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
16
Our work
AGN 03 requires us to disclose our views on significant qualitative aspects of the Trust's arrangements for delivering economy, efficiency and effectiveness.
We have focused our work on the significant risks that we identified in the Trust's arrangements. In arriving at our conclusion, our main considerations were:
• You have achieved a deficit for the year of £14.3 million, which was in line with your Control Total agreed with NHS Improvement (NHSI), and thus unlocked £14.3 million of Provider Sustainability Funding (PSF) and Financial Recovery Funding (FRF) during the course of the year. This meant you achieved your breakeven position at year end once the additional funding from NHSI was taken into account. This position looked under threat during the course of the year, particularly at Month 9, but a strong performance in Q4 brought you back to the planned position.
• Within this position there was a considerable overspend on Agency Staff, with you breaching the NHSI ceiling by £8.1 million, spending £23.3 million in total. This was £5.9 million above your plan for the year as well.
• Linked to this, you delivered £5 million of CIPs, which was less than half of the planned level, which was £11.7 million. A further £6.4 million of savings were being explored, reviewed and recovered as year end approached to help manage the pressure being transferred into 2020/21.
• For 2020/21 your draft Operational Plan is to achieve a Control Total of a £12 million deficit before the receipt of PSF and FRF. In order to support the wider South East London Integrated Care System (ICS) you also have a stretch target to exceed the control total by £8.9 million to help close the financial gap across the system in year.
• However, the impact of Covid-19 has meant that the planning process for 2020/21 has been paused, with NHS England having agreed block contract arrangements between Trusts and Commissioners for the first half of 2020-21 to help manage the pandemic. At this stage it is unclear what arrangements will be in place for the second half of the year, but it is clear this will be sufficient to sustain delivery of healthcare across the sector.
We have set out more detail on the risks we identified, the results of the work we performed, and the conclusions we drew from this work on the following page.
Overall conclusion
Based on the work we performed to address the significant risks, we are satisfied that the Trust had proper arrangements for securing economy, efficiency and effectiveness in its use of resources.
The text of our report, which confirms this can be found at Appendix E.
Recommendations for improvement
We discussed findings arising from our work with management and have agreed recommendations for improvement.
• You should look to reduce your reliance on Agency Staff and other one-off savings to help support a more sustainable financial position moving forward.
Our recommendations and management's response to these can be found in the Action Plan at Appendix A
Significant difficulties in undertaking our work
We did not identify any significant difficulties in undertaking our work on your arrangements which we wish to draw to your attention.
Significant matters discussed with management
There were no matters where no other evidence was available or matters of such significance to our conclusion or that we required written representation from management or those charged with governance.
Value for Money
3. Value for Money
Page 36 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
17
Value for Money
Significant risk Work to address Findings and conclusions
The continuing financial challenges of the Sector
In 2018/19, you delivered a deficit position of £658k, along with delivering £14.138 million of Cost Improvement Plans (CIPs). The deficit position was in line with plan, and hence unlocked the planned Provider Sustainability Funding (PSF), which returned the Trust to a surplus position at the end of the year. However you delivered £2.3 million less of CIP than planned.
For 2019/20, you have agreed to deliver a breakeven position, which includes £3.5 million of PSF, along with a further £11.1 million from the new Financial Recovery Fund (FRF), which is being used by NHS Improvement to support Trusts who are in an underlying deficit position. At the end of December 2019, you are currently forecasting unmitigated pressures of £4.4 million, which indicates that there may be a weakness in your arrangements for ensuring sustainable resource deployment across the Trust.
This year we will update our understanding of your financial position and the underlying arrangements, including gaining an understanding for the movement in the planned financial position during the course of the year. We will also look to understand the financial plans for the year ahead and determine whether this has any impact on our overall Value for Money Conclusion.
As documented within our Audit Plan, you faced some potentially significant financial challenges during the course of the year, which was in part the reason we raised a significant risk in this area for our VfM Conclusion. At the end of Month 9, whilst you were forecasting the delivery of the planned breakeven position, you had identified £4.4 million of unmitigated pressures which if the pressures had not been addressed would have impacted on your year-end financial position, with the potential of not receiving the expected PSF and FRF.
However by Month 12, you had been able to return to your original planned position, achieving an deficit of £14.3 million, which subsequently unlocked the planned PSF and FRF funding per the plan agreed with NHS Improvement at the start of the year. The impact was you achieved your planned breakeven position once the funding from NHS Improvement had been considered. Management has confirmed that the improved performance over the course of the last three months of the financial year was due to a number of the potential risk areas being resolved in the favour of the Trust. These included savings of £2.0 million due to operational efficiencies identified during the period, along with £1.4 million of funding received from CCGs over and above that which was originally expected in this period.
In respect of CIPs, you managed to deliver £5 million of CIPs, which was less than half of the planned level of £11.7 million. As highlighted on the previous page, you had a further £6.4 million of savings being explored at year end, which will help offset some of the one-off non recurrent savings which were utilised to ensure your overall financial position delivered to plan. Clearly the Trust should be focusing on delivering recurrent savings moving forward as these then generate benefits in future years, whereas non-recurrent savings will only ever deliver benefit in one year, and are not always the most sustainable options. One area where considerable focus is needed is the level of Agency spend you incurred, which was £8.1 million over the ceiling set by NHS Improvement, and £5.9 million above your plan, with the total spend ending up at £23.3 million.
In terms of plans for 2020/21, you had been proposing to agree a £12 million deficit position with NHS Improvement, prior to the receipt of PSF and FRF funding from the centre. You were also being set a stretch target of achieving a position £8.9 million above your control total to help support the underlying financial challenge across the South East London Integrated Care System (ICS). However the impact of the Covid-19 pandemic has meant the whole planning process across the NHS has been paused, with NHS England taking over commissioning arrangements and agreeing block contracts between CCGs and Providers for the first half of the financial year to help support arrangements to tackle the pandemic.
At this stage it is unclear what the financial landscape will look like for the second half of the year, but it is clear that there is a commitment from NHS Improvement that funding will be made available to support the level of health services required to the end of the financial year whether this is a continuation of the block contract arrangement or a return to the previous arrangement. Either way, you are on a sound footing to be able to manage these challenges and be able to move forward once normal business rules reappear.
Page 37 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
18
4. Independence and ethics We confirm that there are no significant facts or matters that impact on our independence as auditors that we are required or wish to draw to your attention. We have complied with the Financial Reporting Council's Ethical Standard and confirm that we, as a firm, and each covered person, are independent and are able to express an objective opinion on the financial statements
We confirm that we have implemented policies and procedures to meet the requirements of the Financial Reporting Council’s Ethical Standard and we as a firm, and each covered person, confirm that we are independent and are able to express an objective opinion on the financial statements.
Further, we have complied with the requirements of the National Audit Office’s Auditor Guidance Note 01 issued in December 2019 which sets out supplementary guidance on ethical requirements for auditors of local public bodies.
Details of fees charged are detailed in Appendix D
Audit and non-audit services
For the purposes of our audit we have made enquiries of all Grant Thornton UK LLP teams providing services to the Trust. The following non-audit services were identified which were charged from the beginning of the financial year to the current date, as well as the threats to our independence and safeguards that have been applied to mitigate these threats.
These services are consistent with the Trust’s policy on the allotment of non-audit work to your auditors. All services have been approved by the Audit Committee. None of the services provided are subject to contingent fees.
Independence and ethics
Fees £ Threats identified Safeguards
Audit related
Assurance on your Quality Report
6,600 Self-Interest (because this is a recurring fee)
The level of this recurring fee taken on its own is not considered a significant threat to independence as the fee for this work is £6,600 in comparison to the total fee for the audit of £68,650 and in particular relative to Grant Thornton UK LLP’s turnover overall. Further, it is a fixed fee and there is no contingent element to it. These factors all mitigate the perceived self-interest threat to an acceptable level.
Non-audit related
None N/A N/A N/A
Page 38 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
19
Action planWe have identified three recommendations for you as a result of issues identified during the course of our audit. We have agreed our recommendations with management and we will report on progress on these recommendations during the course of the 2020/21 audit. The matters reported here are limited to those issues that we have identified during the course of our audit and that we have concluded are of sufficient importance to merit being reported to you in accordance with auditing standards.
Controls
- Red - High – Significant effect on control system
- Amber - Medium – Effect on control system
- Green - Low – Best practice
Appendix A
Assessment Issue and risk Recommendations
Amber
Manual processing of Starters, Leavers and Changes in Circumstances due to access issues
Our walkthrough of your payroll processes identified that all starters, leavers and changes in circumstances forms have to be manually printed and sent to SBS in hard copy format, due to SBS not having electronic access to these. This generates additional manual input into the process, which increases the chance of forms going missing and not being processed correctly or in a timely manner.
Ensure that these forms can be shared electronically with SBS to reduce the level of manual intervention needed, and thus reduce the likelihood of any errors occurring.
Management response
***To be added***
Amber
Review of Fully Depreciated Assets held on the Property, Plant and Equipment (PPE) Register
Our work on your Assets identified £10.5 million of fully depreciated assets still being held on the PPE Register. When Assets are fully depreciated this usually indicates that they are no longer in use, but we understand this isn’t the case for some of the Assets which are being held in this manner on the Register. Thus there is a risk that Assets are being depreciated over incorrect timeframes which do not fully reflect their availability for use for you, however we have noted that the Trust’s Asset Lives are in line with the standard assumptions across the NHS.
You should look to undertake an exercise to review all fully depreciated assets held on the PPE Register to confirm whether they are still operational, or whether they are obsolete. Where items are still in use, there should be a consideration as to whether they still have a value to you which should be reflected within the Accounts.
Management response
***To be added***
Page 39 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
20
Action planWe have identified three recommendations for you as a result of issues identified during the course of our audit. We have agreed our recommendations with management and we will report on progress on these recommendations during the course of the 2020/21 audit. The matters reported here are limited to those issues that we have identified during the course of our audit and that we have concluded are of sufficient importance to merit being reported to you in accordance with auditing standards.
Controls
- Red - High – Significant effect on control system
- Amber - Medium – Effect on control system
- Green - Low – Best practice
Appendix A
Assessment Issue and risk Recommendations
Amber
Reduce the reliance on Agency Staff and one-off savings to support your financial position
The work performed on our Value for Money Conclusion has identified that you incurred a considerable overspend on Agency Staff during the course of the year, which required several one-off savings to be identified to support your overall financial position. Managing your financial position in this manner is not sustainable over the longer term, and thus you should look to try to reduce the level of Agency spend and one-off savings to make your financial position more sustainable moving forward.
Ensure that your Agency spend is tightly managed to reduce the impact on your overall financial position, which will help reduce the level of one-off savings required to manage your financial position.
Management response
***To be added***
Page 40 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
21
Follow up of prior year recommendationsWe identified the following issues in the audit of South London and Maudsley NHS Foundation Trust’s 2018/19 financial statements, which resulted in four recommendations being reported in our 2018/19 Audit Findings Report. We have followed up on the implementation of our recommendations and note two are still to be completed.
Appendix B
Assessment Issue and risk previously communicated Update on actions taken to address the issue
X Lack of automation to prepare and authorise Journals
In the previous year, we identified you still use paper records to prepare and authorise Journals, which provided challenges in providing the audit trails for our testing at year end, along with making it more difficult to trace and monitor Journals during the course of the year, which would be easier and quicker if Journals were prepared and authorised using electronic files, as is the case at a number of other Trusts across London. We recommended that you moved to a system of electronic preparation and authorization of journals to enable more timely and accurate bookkeeping.
As mentioned previously in the Report, limited progress has been made in this area, which led to us being unable to obtain evidence to support the authorization of a small number of journals selected as part of our testing at year end. The move to remote working due to the impact of Covid-19 has led to small changes in this area for Month 12, but further work is needed to implement a fully electronic system in this area.
Ensure that Journal Adjustments are adequately documented
We also identified two Journals where there were differences between the balances shown on the General Ledger, in comparison to those shown on the paper backing for the Journal. Now whilst we were able to obtain explanations for these adjustments, there is a risk that you would not be able to explain these fully if they are not documented clearly at the time of posting. We recommended that any adjustments made to Journals between preparing and posting are clearly documented to ensure there is a clear audit trail for the adjustments made.
No similar issues have been identified from the testing performed in 2019/20, and thus we are satisfied this recommendation has been cleared.
X Lack of clear trail for the Payables Balance
Our testing of your Payables balance at year end was particularly challenging, largely due to challenges in getting the relevant transactions in a listing suitable for audit sampling. Whilst this held up the audit of this area, this would also pose a challenge for you should you need to be obtain a listing of your outstanding payments at a given point in time. We recommended that you develop a method of obtaining all of your Payables balances in one Report, which will not only make the year end audit of this area more straight forward, but it will also be beneficial to your internal financial monitoring as well.
Whilst we were able to make quicker progress with our testing in this area this year, it still required us to pull various listings together to select our initial sample, which was at a code level. We then had to select a sample of transactions from these codes, which adds an extra level of complexity to what is already a challenging area to audit. Developing an approach to show all of your Payables balances in one report would be beneficial both for you and for the audit process and should be explored further in the future.
Assessment
Action completed
X Not yet addressed
Page 41 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
22
Follow up of prior year recommendationsWe identified the following issues in the audit of South London and Maudsley NHS Foundation Trust’s 2018/19 financial statements, which resulted in three recommendations being reported in our 2018/19 Audit Findings Report. We have followed up on the implementation of our recommendations and note two are still to be completed.
Appendix B
Assessment Issue and risk previously communicated Update on actions taken to address the issue
Ensure Related Party Declarations are up to date
During our testing of the Related Parties included within the Accounts, we identified that a number of the declarations from the Directors were out of date and had not been updated for 2018-19. Whilst this may have been appropriate if the status of these individual’s Related Party Transactions had remained consistent, without obtaining a formal return from the relevant individuals there is no formal way of confirming this. We recommended that these Declarations are obtained as part of the final accounts process, ensuring up to date declarations are held ahead of the audit process.
We have discussed the Trust’s process in this area and have confirmed that Declarations are only required where changes are made, which is sufficient given the circumstances and thus we have closed the issue on this basis.
Assessment
Action completed
X Not yet addressed
Page 42 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
23
Audit AdjustmentsWe are required to report all non trivial misstatements to those charged with governance, whether or not the accounts have been adjusted by management.
Impact of adjusted misstatements
At the date of preparing this Report, no adjusted misstatements have been identified from our audit work. Should any be identified from our remaining audit work, then we will bring them to the attention of Management and the Audit Committee as soon as possible.
Impact of unadjusted misstatements
The table below provides details of the adjustments identified during the 2019/20 audit which have not been made within the final set of financial statements. The Audit Committee is required to approve management's proposed treatment of all items recorded within the table below.
Appendix C
Detail
Statement of Comprehensive Net Income
£‘000Statement of Financial
Position £’ 000Impact on adjusted net
surplus/(deficit) £’000 Reason for not adjusting
Allowance for Credit Losses – NHS Receivables
As mentioned earlier in the Report, we identified that you are holding an allowance for credit losses against your NHS Receivables balance, effectively understating the receivables balance included within the Accounts. Whilst we understand the rationale for this treatment, it is not in line with NHS business rules and hence we are required to report as an unadjusted misstatement.
Cr Income 1,606 Dr Receivables 1,606 • Increase by 1,606 We have not amended for this balance as it is immaterial to the overall financial standing of the Trust. In our experience NHS Commissioners often do not pay full amounts and seek credit notes against legitimate invoices without having raised a dispute as part of the agreement of balances exercise
Overall impact £1,606 £1,606 £1,606
Page 43 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
24
Audit Adjustments
Appendix C
Disclosure omission Detail Auditor recommendations Adjusted?
Note 1 – Accounting Policies
Critical Judgements – Property Valuations
We identified that no material uncertainty had been provided in the draft accounts in respect of your Property Valuations. Adequate disclosures have now been provided about this uncertainty in the revised Accounts.
Note 3 – Operating Income
Additional Income to fund increase in Pensions Contributions of £11,191k
Our testing identified that the notional income received to fund the increase in NHS pension contributions of £11,191k had been incorrectly removed from the ‘Other Clinical Income’ line in Note 3.1 instead of the ‘Cost and Volume Contract Income’ line. This has been adjusted in the revised Accounts to show the correct analysis of income.
Note 4 – Operating Expenses
Audit Fees The draft Note did not include the correct external audit fees for 2019-20, which has subsequently been updated by you in the revised Accounts.
Note 10 – Property, Plant and Equipment
2019/20 Capital Commitments The draft Note did not include a value for your Capital Commitments as at the 31 March 2020, which has subsequently been provided in the revised Accounts.
Note 19 – Lease Commitments
Minimum lease payments under Operating Leases
As mentioned earlier in the Report, a number of amendments were identified to the Operating Leases disclosure to reflect the correct value of minimum lease payments due in future years. The total value of minimum lease payments was updated by £18,440k and the analysis of when the payments were due was also updated as well.
Note 21 – Related Party Transactions
Disclosures of 2019-20 Balances You have streamlined your Related Party Disclosures to ensure compliance with the GAM, as the disclosures initially provided were in excess of the requirements in this area.
Minor Disclosure Issues Accounting Policies
Note 17 – Provisions
A number of other minor disclosure amendments have been processed by you in the areas mentioned. None of these are individually significant enough to warrant separate disclosure.
Misclassification and disclosure changesThe table below provides details of misclassification and disclosure changes identified during the audit which have been made in the final set of financial statements.
Page 44 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
25
We confirm below our final fees charged for the audit and provision of non-audit services.
The fees reconcile to the financial statements. The breakdown of the additional fee charged is as follows:
The reason for reduction in the Quality Report fee is due to the fact that the requirement for Trusts to obtain external assurance over this area was removed in March 2020 as part of the response to the Covid-19 pandemic. We have only charged a small fee to reflect the cost of the work that was undertaken before the requirement to obtain this assurance was removed.
Fees
Audit fees Proposed fee Final fee
Trust Audit 75,150 84,750
Total audit fees (excluding VAT) £75,150 £84,750
Non-audit fees for other services Proposed fee Final fee
Quality Report 6,600 1,000
Total non-audit fees (excluding VAT) £6,600 £1,000
Appendix D
Original Contract Fee (excluding VAT) £68,650
Raising the Bar 2,500
PPE Valuations – Work of Experts 2,000
Impact of Covid-19 on Audit Procedures 7,600
Work on Maudsley Commercial 4,000
Revised Fee for 2019-20 (excluding VAT) £84,750
Page 45 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
26
Audit OpinionWe anticipate we will provide the Trust with an unmodified audit report, with an Emphasis of Matter Paragraph for the Material Uncertainty relating to Property Valuations
Appendix E
Page 46 of 131
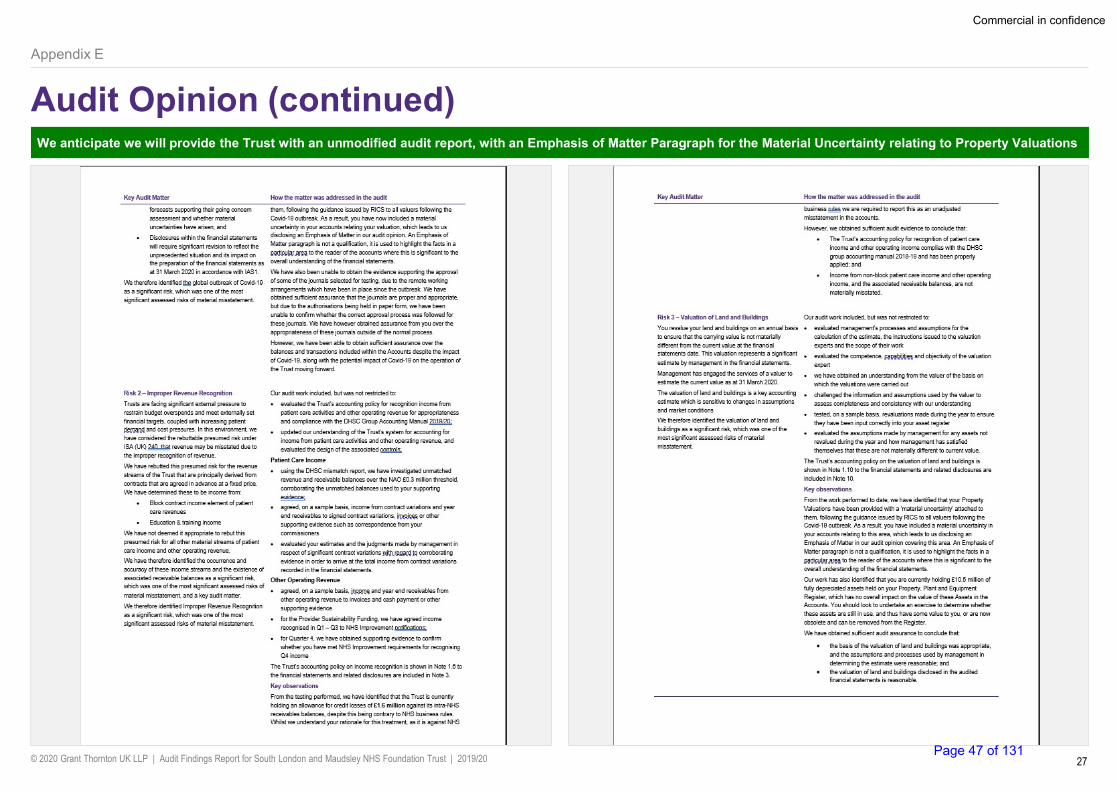
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
27
Audit Opinion (continued)We anticipate we will provide the Trust with an unmodified audit report, with an Emphasis of Matter Paragraph for the Material Uncertainty relating to Property Valuations
Appendix E
Page 47 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
28
Audit Opinion (continued)We anticipate we will provide the Trust with an unmodified audit report, with an Emphasis of Matter Paragraph for the Material Uncertainty relating to Property Valuations
Appendix E
Page 48 of 131
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
29
Audit Opinion (continued)We anticipate we will provide the Trust with an unmodified audit report, with an Emphasis of Matter Paragraph for the Material Uncertainty relating to Property Valuations
Appendix E
Page 49 of 131

© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
Commercial in confidence
30
Audit Opinion (continued)We anticipate we will provide the Trust with an unmodified audit report, with an Emphasis of Matter Paragraph for the Material Uncertainty relating to Property Valuations
Appendix E
Page 50 of 131

Commercial in confidence
© 2020 Grant Thornton UK LLP | Audit Findings Report for South London and Maudsley NHS Foundation Trust | 2019/20
© 2020 Grant Thornton UK LLP. All rights reserved.
‘Grant Thornton’ refers to the brand under which the Grant Thornton member firms provide assurance, tax and advisory services to their clients and/or refers to one or more member firms, as the context requires.
Grant Thornton UK LLP is a member firm of Grant Thornton International Ltd (GTIL). GTIL and the member firms are not a worldwide partnership. GTIL and each member firm is a separate legal entity. Services are delivered by the member firms. GTIL does not provide services to clients. GTIL and its member firms are not agents of, and do not obligate, one another and are not liable for one another’s acts or omissions.
grantthornton.co.ukPage 51 of 131

Council of Governors Tuesday 15 September 2020
Name of Report Audit Committee 2019/20 Annual Report to the Council of Governors
Author
Steven Thomas (Audit Committee Secretary)
Presented by
Duncan Hames (Audit Committee Chair)
Purpose
The Council of Governors (‘the Council’) is asked to note this report; Background The Audit Committee (‘the Committee’) is required report annually to the Council on: • the Committee’s work for the year and (if the Committee considers
it necessary) matters needing action or improvement, and the corrective steps to be taken; and
• external audit as regards their performance for the year. The Committee is also required to make recommendations to the Council as to the appointment, reappointment, termination of appointment and fees of the external auditor. This is dealt with in a separate paper. These requirements all flow from the Committee’s terms of reference (paras 2.8 and 3.2)
Summary The Committee met for 2019/20 in line with its terms of reference, and after these meetings highlighted a number of key issues/actions to the Trust Board and Council. Ongoing evaluation of Committee meetings indicated that the Committee has been working effectively, with no significant points for improvement. Ongoing evaluations also flagged a number of ways in which the Committee is making positive contributions to the Trust and the lives of the people and communities that the Trust serves. The Committee has reviewed the performance of the Trust’s current external auditor (Grant Thornton). The Committee is satisfied with the external auditor’s performance, the quality and value of their work, the timeliness of their reporting and the external audit fee.
1. The Committee and its work for 2019/20 1.1. The Committee’s purpose. The overall purpose of the Committee is to support the Board to implement Board strategy effectively: by promoting efficient and effective management of risk and excellent financial management and governance within the Trust; and by acting as the committee with prime oversight of these matters (Committee’s terms of reference refer). Ultimately, the Committee seeks to play its part in supporting improvement of the mental health and wellbeing of the people and communities served by the Trust.
Page 52 of 131

1.2. Committee membership. The Committee comprises 3 Non-Executive Directors (‘NEDs’ – Chair: Duncan Hames). Membership remain unchanged throughout the year. Regular attendees include the Chief Financial Officer (‘CFO’), Chief Operating Officer (‘COO’) and other senior Trust management, internal audit, counter fraud, external audit and a Governor Observer. This arrangement ensures that the Committee receives information and assurances from a balanced range of sources. 1.3. Committee meetings. To achieve its goal, in line with its terms of reference and practice in previous years, the Committee held meetings as follows. All were quorate: • four quarterly meetings at which the Committee considered reports it had requested from Trust
management, external audit, internal audit and counter fraud specialists. In line with the Committee’s rolling work programme, regular reports include progress reports from these groups, the Board Assurance Framework, and an exception report on breaches of the Trust’s Standing Financial Instructions/tender requirements. The Committee also requests ‘one off’ reports as necessary; and
• one special meeting (May 2019) to consider the Trust’s 2018/19 annual report and accounts. The Committee reviewed annual reports from external audit, internal audit and counter fraud providing assurance supporting the Committee’s consideration of the Trust’s annual report and accounts. The Committee held a similar meeting in June 2020 to consider the Trust’s 2019/20 accounts.
1.4. Integration with other committees/partnership groups. To help ensure that it has a rounded overview of issues affecting the Trust, at each meeting the Committee reviews current key issues discussed at other key Trust committees, namely: the Business Development and Investment Committee (‘BDIC’); the Finance and Performance Committee (‘FPC’); and the Quality Committee (‘QC’). The Committee also has a standing request to the South London Mental Health and Community Partnership (‘SLP’) to be advised of any relevant key issues. In addition, the Quality Committee Chair is a Committee member and regularly flags issues discussed at the Quality Committee 1.5. Key Committee achievements: issues/actions reported. After each Committee meeting the Trust Board and Council of Governors receive summary reports on key issues/actions arising from that meeting. Appendix 1 shows all the key issues/actions reported to the Trust Board for 2019/20. Of these, the following issues/actions are considered the most important (covered in more detail in Appendix 1, and flagged there with an asterisk *). The Committee draws a distinction between key issues escalated to the Trust Board (these are issues which the Committee considers require decisions or actions from the Trust Board) and key issues flagged for the attention of the Trust Board (these are issues of which the Committee considers the Trust Board should be aware): • (June 2019 meeting – escalated to the Board) Revisions to the Trust’s framework of organisational
and financial rules (for subsequent Board approval) should resolve inconsistencies between actual current practice and the existing framework;
• (June 2019 meeting – escalated to the Board) non-executive directors and executive directors will screen the Board Assurance Framework (‘BAF’) and will take account of 3 potential Mental Health Act/regulatory breach areas noted in the meeting;
• (June 2019 meeting – escalated to the Board) The Board should discuss the waiting time issues referred to in the Quality Committee recent key issues reports to the Board;
• (September 2019 meeting) Internal Audit will consider planning an audit of Trust grievance procedures, further to Board discussion on BME staff experience;
• (September 2019 meeting) Trust management will follow up of recommendations from internal audit reviews of 2 major Trust projects (Ascom safety alarm system and Children and Young People (‘CYP’) project);
• (December 2019 meeting) Permissible but potentially excessive staff working hours – the Human Resources team will look into this. (March 2020) The Committee was advised that this was partly a ‘one off’ response to unusually large staffing gaps, and Human Resources has subsequently contacted managers to resolve this issue; and
Page 53 of 131

• (March 2020 meeting) Covid-19 cost management and related breaches of Trust Standing Financial Instructions, and Trust response to Covid pandemic: Trust management outlined the issues and mitigations, including internal audit review.
1.6. Matters needing action or improvement at the Trust. The Committee confirms that for 2019/20: • no matters arose which it considers need to be raised with the Council; • (as noted in para 1.5 above) three matters arose from the June 2019 Committee meeting which
needed to be escalated to the Trust Board. These related to: revisions to the Trust’s framework of organisational and financial rules; review of the Board Assurance Framework by Trust Board members and subsequent update; and Trust Board consideration of waiting time issues;
• the Committee has discussed the Board Assurance Framework regularly, and considers that the framework is a good one enabling the Trust to identify key risks and to ensure that these reflect emerging issues. The Committee has noted the importance of all Board Assurance Framework risks clearly identifying any gaps in assurance and control, identifying the mitigating actions as a result, and then ensuring actions are being taken to minimise these risks. The Committee notes that all the Board Assurance Framework risks are currently being reviewed by their executive team owners, and by relevant Board committees, to ensure that these mitigating actions have been identified and are being acted on.
1.7. Committee performance: themes from ongoing evaluations. At the end of each meeting the Committee conducts an informal meeting evaluation taking account of a standard checklist developed by Corporate Affairs management. The Committee has reflected on the evaluations for 2019/20. No adverse comments were noted. Key themes identified included: • the Committee’s input supports improvement of the mental health and wellbeing of the people and
communities served by the Trust, for example through discussion of the Trust’s 2018/19 quality report and consideration of use of the Trust’s cash balances;
• there has been a good balance in the nature of the issues discussed. This is generally difficult for Audit Committees to achieve as the temptation is to be drawn into discussion of matters of detail rather than seeking to identify systemic themes in the detailed information presented; and
• the Committee adds value to the presenting teams. For instance, the Chief Financial Officer and Chief Operating Officer advised that they had found discussions with the Committee helpful.
1.8. Committee performance: annual review. Currently, given other priorities arising from the Covid-19 pandemic, the usual Board/committee annual reviews are on hold. Until these annual reviews take place, Committee members are using the informal meeting evaluations (see above) as an alternative means of assessment/improvement. 2. External auditor 2.1. Appointment of current external auditor (September 2017 for 3 years). Following a tender exercise, at its meeting in September 2017 the Council of Governors appointed Grant Thornton as the Trust’s external auditor on a three year contract, starting September 2017. The tender process was conducted on behalf of the Trust and Oxleas NHS Foundation Trust by a group of representatives from both Trusts, including representatives from the Council of Governors, the Audit Committee Chairs and the Chief Financial Officers. The group reviewed tenders received from the Trust’s then current external auditor (Deloitte), Grant Thornton and one other external audit provider. 2.2. Review of external auditor’s performance 2019/20. The Committee has reviewed the performance of the external auditors for 2019/20, taking account of the reports received from external audit, and other parties, considered at each Committee meeting. Based on this the Committee is satisfied with the performance of the Trust’s external auditors, the quality and value of their work, the timeliness of their reporting and the external audit fee.
Page 54 of 131

APPENDIX 1: KEY ISSUES REPORTED TO THE TRUST BOARD BY THE COMMITTEE Listed below are the key issues reported to the Trust Board by the Committee arising from the Committee’s meetings during 2019/20 on the dates shown. Except for the 3 issues flagged at the June 2019 Committee meeting, these are not matters of escalation, but rather are key issues or concerns that the Committee considered the Trust Board should be aware of. The Committee draws a distinction between key issues escalated to the Trust Board (these are issues which the Committee considers require decisions or actions from the Trust Board) and key issues flagged for the attention of the Trust Board (these are issues of which the Committee considers the Trust Board should be aware For the purpose of this report to Council of Governors, issues considered as more important have been flagged with an asterisk * and are summarised in section 1 of this annual report to the Council. Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
20 May 2019 special accounts review meeting No matters for escalation to the Board 1. Assurance reports received at the meeting. The Committee received and discussed the following: • internal audit 2018/19 annual report and
opinion • counter fraud 2018/19 annual report and
outline plan for 2019/20 • external audit 2018/19 reports/opinions on
the Trust’s accounts, annual report and quality report
Note only
2. Items reviewed at the meeting. The Committee received and reviewed the following: • draft 2018/19 Trust accounts • draft 2018/19 Trust Annual Report • draft 2018/19 Trust Quality Report • Audit Committee 2018/19 annual review and
Terms of Reference … • Audit Committee annual report to the Council
of Governors 2018/19 (not presented at the meeting – Audit Committee agreed this would subsequently be reviewed/finalised with the Audit Committee Chair outside of the meeting)
The Committee approved these reports subject to appropriate resolution of points raised at the meeting. The Committee agreed a process for managing changes to the accounts after the Committee meeting
25 June 2019 meeting Items 2, 5 and 6 only were escalated to the Board
1. Increasing the Audit Committee membership The meeting heard that, further to suggestions at a recent meeting of the Trust’s Council of Governors, the Trust is seeking to identify and appoint an additional Audit Committee member who is not a Trust Board member. The intention is that this new member would bring an additional ‘external’ perspective to the Audit Committee’s work
Noted for information only
Page 55 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
*2. Update of SFIs, SoD and BRDP (escalated to the Board) The meeting discussed progress on the refresh/update of the following key documents: Standing Financial Instructions (‘SFIs’); Scheme of Delegation (‘SoD’); and Board Reservation and Delegation of Powers (‘BRDP’). These documents, together with the Standing Orders (‘SOs’), codify the organisational and financial rules that staff must follow, and describe what decisions the Board delegates (and to what party) and what decisions it reserves to itself. One specific point discussed was whether internal audit should report to the Director of Corporate Affairs, or to the Chief Financial Officer. On balance, the Committee agreed it best to retain accountability with the Chief Financial Officer
The Director of Finance will present final drafts of the SFIs, SoD and BRDP to the Trust Board for review and approval, together with a clear proposal on addressing any major inconsistencies between actual current practice, the current SFIs, SoD and BRDP, and the proposed updated SFIs, SoD and BRDP (Sep 2019)
3. Quality Impact Assessments (‘QIAs’): production and review The meeting discussed this paper, which had been produced for another purpose – namely to provide assurance to the quality leads in the 4 borough Clinical Commissioning Groups (‘CCGs’ – Croydon, Lambeth, Lewisham and Southwark) that the quality impacts of the Trust’s Cost Improvement Programme (‘CIP’) and Quality Innovation and Productivity Programme (‘QIPP’) were assessed, mitigated and authorised before the schemes could proceed. In addition, the paper addressed several supplementary queries raised by Clinical Commissioning Groups, and details of the Trust’s Quality Impact Assessment methodology were included. The Committee noted that the paper was comprehensive and informative
The Committee suggested that the Quality Committee would find it useful to receive such a paper regularly
4. CAMHS performance indicator criteria The Head of Internal Audit advised that a recent internal audit had identified that the Trust’s Child and Adolescent Mental Health Services (‘CAMHS’) performance return may not be compliant with the national guidance, and updated the meeting as to progress in addressing this: • there has been ongoing communication
between the Trust’s service and NHS Improvement concerning the issues; and
• NHS Improvement is committed to identifying a national lead who can engage on the issue
In the interim the Trust’s service will prepare local guidance aligned to its own interpretation of the indicator (the Trust now employs the relevant national expert in this area). Also the Chief Operating Officer will arrange: (a) for the Trust to benchmark its methodology against other mental health trusts; (b) to present an appropriate report to the Quality Committee; and (c) to report back to the Audit Committee (Sep 2019)
Page 56 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
although, so far, they have been unable to do so
*5. Board Assurance Framework (‘BAF’) (escalated to the Board) The Committee noted in discussion: • that Board Assurance Framework (‘BAF’) risk
7 (quality and statutory compliance) should respond to Mental Health Act issues and other regulatory breach issues, as well as CQC-related issues. The Director of Nursing advised that the Quality Committee is leading a ‘deep dive’ into flow-related issues and problems at Boroughs;
• the need to have regard to breaches of ‘place of safety’ requirements in law and regulation; and
• a further potential area of breach – provision to detained patients, within the required timeframes, of information about their rights
The Director of Nursing will arrange for NEDs and executive directors to discuss and screen the BAF risks, and will update the next Audit Committee meeting on progress (Sep 2019)
*6. Waiting time issues (escalated to the Board) The Committee noted the waiting time issues referred to in the Quality Committee key issues reports to the Board meetings held in April and June 2019. The Audit Committee Chair considered that the Board should discuss these matters further
Hereby flagged for the Board’s attention
September 2019 meeting No escalation points – FAO board only *1. Experience of staff from BME backgrounds. The Committee heard that non-executive director Mike Franklin had suggested that the Trust should conduct an audit of Trust grievance procedures and the experience of BME staff.
The Head of Internal Audit will consider whether/how to include an audit of Trust grievance procedures in internal audit plans and will update the Audit Committee (Dec 2019)
*2. Ascom project: internal audit report. Internal audit advised that: • the contract with Ascom (contractor re the
safety alarm system at the Ladywell Unit) lacked information about key deliverables, thereby, passing much of the design change risk to the Trust; and
• although the contract was based on the formalised contracting process developed by the Institution of Civil Engineers (‘NEC’ contracts) the compensation event process was not properly managed and appeared not to be well understood. This pointed to issues with capability of the Estates team, choice of contract type and independent scrutiny and challenge.
The Chief Financial Officer will, with the Director of Strategy and Commercial, review Trust management’s progress in addressing issues identified following internal audit’s review of the Ascom security alarm system at the Ladywell Unit. The Chief Financial Officer will report on this to the next Committee meeting (Dec 2019)
Page 57 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
The Committee noted that, together with the results of the internal audit reports on the DBH (‘Douglas Bennett House’) and CYP (‘Children and Young People’) projects (see below), this indicated systemic underlying issues – in particular with the Estates team and its need to work together with clinical teams. *3. Children and Young People (‘CYP’) project: internal audit report. The Committee noted that several Board members had expressed concerns about the CYP project at Board meetings, in particular about whether it will benefit/improve the service provided by the Trust – there seems to be no clear link with the Trust’s services and little clarity over the project objectives. The Chief Financial Officer advised that the Trust had a vision on these matters but had experienced difficulties in converting this into a project action plan with measurable outcomes. The Chief Financial Officer flagged that the CYP project depended on (amongst other things) sign off by King’s College London management of an agreement involving significant funding. The Chief Financial Officer advised that Trust management was working on the basis that such agreement would be obtained in November 2019 as planned.
The Director of Strategy and Commercial confirmed that: • there was no conflict of interest arising from
the method of funding the CYP project (charitable contributions);
• there was no indication that the Trust’s current services would be affected adversely by delivery of the CYP project (albeit that significant resources are/will be used in its delivery); and
• Trust management had accepted all recommendations in the internal audit report, and would complete them as soon as possible (the Committee had noted that the planned implementation dates for most of the audit recommendations were current or past).
4. Review of BAF. The Committee reviewed the Board Assurance Framework (‘BAF’) and discussed it with Trust management. The Committee noted that the quarterly BAF reports were most helpful, evidencing the Trust’s active use of the BAF as a tool for managing the Trust’s operations. The Committee noted that it was content with the BAF review process and with closure of BAF 2 (operational delivery structure) and replacement with a new BAF risk for community redesign
Noted for information only
5. Risk Management Policy. The Committee reviewed the draft policy and commended its clarity, in particular as regards its definitions of terms relating to the Board Assurance Framework (‘BAF’) such as ‘gaps in control’. As a point for future consideration, the Committee Chair queried how the risk management/BAF regime would deal with collaborative services – for instance whether each service would have its own BAF.
Noted for information only. After due discussion the Committee ratified the policy and approved its immediate implementation
6. SFI breach. The Director of Strategy and Commercial:
After due discussion (including consideration of internal audit’s related report – key issue 3
Page 58 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
• gave a verbal report about a breach of the Trust’s Standing Financial Instructions (‘SFIs’) relating to engagement of an NHS body to work on the Trust’s Alternative Delivery Model (‘ADM’) project. The potential issue was a lack of evidence of competition in the engagement, the underlying reason for this being the dearth of candidate organisations with appropriate capability; and
• advised that the Trust has subsequently been testing the prices cited by the engaged NHS body, and has control mechanisms in place to verify other information cited by it, including involvement of the Regulator.
The Committee Chair noted that the NHS body might at some future time become a partner with the Trust in the ADM initiative, and flagged that this could represent a conflict of interest. The Chief Financial Officer advised that the other NHS body was likely to be a minority partner (< 10% shareholding)
refers) the Committee agreed that the Trust should adopt a prudent approach to managing potential conflicts of interest that arise as the project proceeds, albeit that the other NHS body’s shareholding may be prove to be less than 10%
17 December 2019 meeting No escalations 1. CAMHS performance indicators. Child and Adolescent Mental Health Services (‘CAMHS’) faces a number of significant challenges, such as waiting time performance, but is doing its best in difficult circumstances. The Care Quality Commission’s (CQC’s) next annual ‘well led’ inspection is likely to be in July 2020 and CAMHS may be an area of interest for them either as part of any visit in July 2020 or before that (given that CAMHS units around the UK are tending to close
The Committee concluded that the Trust is making progress in resolving problems with quality of service (although this is not yet complete), and the Trust awaits a CQC inspection and is preparing for this. For example, the Trust is conducting ‘mock CQC’ inspections – in particular a Croydon-based team has inspected the Trust’s CAMHS.
2. Counter fraud service. The meeting discussed 2 cases concerning suspected falsified job applications and job offers based thereon. These indicate some serious learning points for the HR team to reflect upon, for example the need to cross check job applications with previous applications/roles irrespective of whether job applicants list the Trust as a previous employer (Human Resources’ records may well have improved since the time of the original weaknesses in Human Resources’ records) .
The Head of Counter Fraud advised that there were no very significant matters to note as regards the current caseload A draft 2019/20 internal audit report on ‘Payroll and Pensions’ is relevant and with Trust management for comment, and internal audit will report thereon to the March 2020 Committee meeting The Director of Human Resources and Organisational Development will report to the March 2020 Committee meeting on any lessons learned from these 2 cases, and any steps planned to prevent or mitigate future cases
*3. Internal audit service (a). LoS. The Head of Internal Audit confirmed that (as from Sep 2019) Trust management
Page 59 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
(a). Length of Stay (‘LoS’). Internal audit has issued five reports since the previous Committee meeting, comprising: • 1 ‘Limited assurance’ audit report on ‘LoS’.
Key issues related to calculation of the LoS indicator, in particular start/finish times; and
• 4 ‘substantial assurance’ reports *(b). Working hours. There is no Trustwide policy on Temporary Staffing. Some staff are working 70 hour weeks for periods of up to 7 weeks. This may lead to quality/safety issues. (c). ASCOM. The meeting discussed issues around the Trust’s ASCOM security alarm
had addressed the key issues identified by the LoS audit, so length of stay figures might well increase as a result *(b). Working hours. The Director of Human Resources (‘HR’) will arrange for the HR team to look into the issue of staff working hours, will advise staff accordingly and will update the next Committee meeting. ASCOM. Internal audit will update the annual audit plan to cover issues around the ASCOM security alarm system. The 4 ‘substantial assurance’ audit reports issued were: • Serious Incidents: implementing lessons
learnt, actions and recommendations • Temporary Staffing – NHS Professionals • Medicines management • General ledger
4. Board Assurance Framework (‘BAF’). Issues noted included: • the quality of the estate links closely with
quality of service, yet the risk scores differ significantly (16 and 9 respectively);
• there is more to ‘Right Care’ than monitoring LoS and Out Of Area numbers, yet BAF risk 14 focuses on these; and
• the BAF is very detailed, which can inhibit review and focus.
The Chief Operating Officer will ensure that these issues are reviewed and implemented as appropriate. In particular, to aid BAF review and focus, the relevant executive director risk owners should flag the 2 or 3 key mitigating actions for each risk (the Trust Finance and Performance Committee’s recent meeting had noted the same issue and resolution)
(5). External audit work on ‘VfM’ and ‘going concern’ The Trust’s circumstances and financial performance may well affect the external audit work required (and possibly also the wording of the external audit report) as regards Value for Money (‘VfM’) and Going Concern
External audit will keep the Committee updated at future Committee meetings
31 March 2020 meeting No escalations *1. Potentially excessive staff working hours: follow up. At a previous Committee meeting, internal audit had reported that there was no Trustwide policy on Temporary Staffing, and some staff had (within the rules in force) been working 70 hour weeks for periods of up to 7 weeks, which may be of concern for several reasons. The Committee noted this as an action point. At the current Committee meeting the Committee Chair reiterated that the Committee’s prime
The Deputy Director of Human Resources advised that: • this was in part a ‘one off’ response to
unusually large staffing gaps; and • Human Resources has subsequently
emailed managers to resolve this issue. The Committee agreed that the action should be closed as resolved.
Page 60 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
concern had been to ensure that staff wellbeing and the quality of care to service users were maintained. 2. Counter Fraud across the UK: benchmarking exercise performed by NHSCFA. This exercise shows that the Trust is performing relatively well, but the collation process adopted by NHS Counter Fraud Authority (‘NHSCFA’) means that benchmarking data is somewhat out-of-date and so some caution needs to be applied in interpretation. The Trust’s Head of Counter Fraud advised that the NHSCFA is concerned at the large drop off in fraud sanctions/prosecutions at Trusts around the UK
To address this: • the NHSCFA is implementing a national
proactive exercise. Based on his experience of previous similar exercises, on cost/benefit grounds the Trust’s Head of Counter Fraud proposed that the Trust should provide the minimum dataset requested by NHSCFA. The Committee concurred; and
• the NHSCFA has suggested that each Trust appoints a further Fraud Champion (in addition to the current requirement for a Local Counter Fraud Specialist, a non-executive director Fraud Champion and an executive director Fraud Champion). The Trust’s Head of Counter Fraud suggested that the Trust’s current Fraud Champion arrangements were sufficient. The Committee concurred
3. Trust’s Counter Fraud Self Review Tool (‘SRT’). The Committee noted the results of the self-assessment of performance for 2019/20 against the NHS Counter Fraud Authority’s standards
The Committee noted that of the NHS Counter Fraud Authority’s 23 standards, 19 were scored ‘full compliance’ 4 were scored ‘partial compliance’ and 0 were scored ‘non compliance’, with action plans for addressing the 4 areas of partial compliance.
4. Review of quality governance. The Committee noted a recent, concise review of Trust quality governance processes by Northumberland Tyne and Wear NHS Foundation Trust, and noted that it included a number of recommendations which Trust management could usefully consider for relevance.
The Head of Internal Audit will report to the Autumn 2020 Committee meeting on implications of the Tyne and Wear report for the audit plan. Trust management may also wish to refer to the report to identify possible improvements to Trust arrangements.
*5. SFI breaches and COVID cost management. The Committee discussed the risks, mitigations and justifications for the placing of a £180k contract with a health consultancy firm, and the learnings gained from this. The Chief Financial Officer advised that this was also related to the issue of COVID cost management, and the Executive Leadership Team (‘ELT’) had also discussed these matters.
The Chief Financial Officer confirmed that he would continue to scrutinise this area and would keep the Committee updated as appropriate. The Head of Internal Audit advised that internal audit review of procurement processes (including COVID cost management) was included in the draft 2020/21 plan covered separately in the Committee’s agenda papers. The Committee noted that SFI breaches appeared not to be restricted to specific departments/services and so learning points were applicable across the Trust
Page 61 of 131

Key potential issues (as at the date of the Audit Committee meeting)
Actions proposed to address key issues (as at the date of the Audit Committee meeting)
*6. Trust’s response to COVID pandemic. The Chief Operating Officer outlined key issues and Trust responses including: • the steps taken by Trust management,
including risk reviews, provision of Personal Protective Equipment (‘PPE’) and modelling of implications;
• the system of bronze, silver and gold calls/meetings used by Trust management to manage developments; and
• Trust management’s current key priorities – including the aim of keeping services closed for as long as appropriately possible.
The Chief Operating Officer advised that to date she was not aware of any unsafe practices at the Trust The Chief Financial Officer advised that some trusts are revising their Standing Financial Instructions (‘SFIs’) to take account of COVID-19 implications. The Head of Internal Audit concurred that some relaxation of SFI processes would be appropriate, and stressed the need to document appropriate justifications
16 June 2020 special accounts review meeting
1. Assurance reports received at the meeting. The Committee received and discussed the following: • internal audit 2019/20 annual report and
opinion • counter fraud 2019/20 annual report • external audit 2019/20 reports/opinions on
the Trust’s accounts and annual report (the 2019/20 Quality Report was not presented as it is not required to be submitted until later in 2020/21)
Internal audit’s opinion for 2019/20 was that internal controls within the organisation are operating effectively with the exception of those areas identified within 3 limited assurance reports: (1) Datix incident reporting; (2) Bridge House – Ascom security; and (3) Data Quality – length of stay. In those areas, Trust management is taking appropriate remedial action Counter fraud work identified no significant issues remaining unresolved going forward, and there are no matters of concern relevant for the Trust’s Annual Governance Statement. At the time of the Committee meeting, external audit work was not quite complete. External audit confirmed that they proposed to issue unqualified (‘clean’) audit reports/opinions on the Trust’s 2019/20 accounts and the other matters they were required to consider;
2. Other reports reviewed at the meeting. The Committee received and reviewed the following: • draft 2019/20 Trust accounts • draft 2019/20 Trust Annual Report
The Committee was content for these reports to be approved subject to appropriate resolution of points raised at the meeting. The Committee agreed a process for managing changes to the accounts after the Committee meeting
3. Audit Committee annual report to the Council of Governors. The report for 2018/19 was presented as a basis for discussion as to the form/content for the 2019/20 report. The final report will be presented at the Governors’ meeting in September 2020, subject to prior approval at the next Committee meeting.
Note only
Page 62 of 131

COUNCIL OF GOVERNORS – SUMMARY REPORT
Date of meeting: 15 September 2020
Name of Report: Finance Report – July (Month 4), Covid costs and 20/21 funding update
Author: Andy Bell, Director of Finance
Presented by: Gus Heafield, Chief Financial Officer / Andy Bell, Director of Finance
Purpose of the report:
For Governors to note. This paper is intended to inform Governor’s about:
• How well the Trust has performed financially against its plan in the four key financial areas SLaM is measured against:
o Income and Expenditure (day to day spending e.g. paying staff each month)
o Cost Improvement (achieving SLaM’s agreed savings plan) o Cash (readily available funds, physical money in the Trust’s bank accounts) o Capital (spend on long term investments like buildings, equipment and IT
infrastructure) • What has caused any major variation in the four key areas (referred to as Key
Drivers) • What risks (or opportunities) have been identified in any of the four key financial
areas. These will be items that are not yet fully reflected in the Trust’s current financial position but could be if certain things happen or conditions are met.
In addition, this report also covers:
• A summary of Covid related and Top Up costs and associated funding for the 4 months from April 20 to July 20 (Months 1 to 4)
• An update on NHS funding for the remainder of 20/21 during the Covid-19 emergency.
Page 63 of 131

The finance team is continuing to work with Governors to ensure that the financials presented are more easily understood. Therefore, this paper sets out to:
• Ensure technical references, jargon or terminology have been explained or simplified.
• Focus on the most important areas of finance • Encourage Governors to ask any and all questions they have to help us improve
the reports. In future iterations more visual, co-designed reports remain the ambition
Headlines (key financial figures you need to be aware of)
RAG Rating Risk Key (what do the Red Amber and Green colours mean in the graphic):
Red: significant risk that planned position will not be fully delivered.
Amber: Risk that planned position will not be fully delivered but with reasonable mitigation
Green: Minimal risk that the planned position will not be achieved
PositionThe Trust has met on target Year to Date. This includes £7.2m of Covid
related Costs and £10.8m of central top up funding. Going forward the Trust is
planning to break even for the year.
CIP (Savings)Due to the suspension of the annual
planning process and the requirements of the Covid emergency the Trust has not made efficiencies so far in 20/21
CashCash is increasingly robust at £125.1mdue to the central support Covid and
Top Up payments being made in advance to minimize risks during the
Covid emergency.
CapitalThe Trust has a planned spend of
£38.7m the current forecast suggests this will be spent. £20.8m relates to the
approval of DBH and Pears Maudsley cases
Key Financial AreasAs at 31st July 2020
Page 64 of 131

2020/21 (Month 4) Position (Financial performance from April 20 to July 20)
Due to the ongoing Covid-19 emergency annual business planning was suspended for 2020/21. In place of an annual plan the Trust has been issued a financial ‘plan’ based on previous year’s income and spend in 2019/20 for the first 4 months of the year. On top of this the Trust has been able to claim for any additional Covid-19 costs (£7.2m) and a further central top up for any other unavoidable costs or income losses (£10.8m) for example, research income.
Key points to note:
• As a result of this new regime the Trust has broken even each month. • Due to Covid requirements and the subsequent suspension of annual planning no CIP
has been achieved to date. • As Cash is provided in advance to support the Covid crisis cash balances have
increased from what was already a healthy position to £125.1m • The Trust has a planned spend of £38.7m the current forecast suggests this will be
spent. £20.8m relates to the approval of Douglas Bennett House and Pears Maudsley Centre for Children and Young People cases.
Key Risks in SLaM’s ongoing financial position (what are the potential financial issues that could emerge that are not currently included in the financial forecast)
• Southwark Local Authority fail to fund Complex Placements
• SLaM are unable to mitigate longer term Overspill pressure
• SLaM are unable to mitigate longer term Ward cost pressure
• SlaM are unable to mitigate longer term agency pressure
• Surge in patient demand Costs Post Covid-19
• SLaM are unable to deliver full Cost Improvement Programme (CIP) requirement
• Uncertainty in financial settlement for the last 6 months of 20/21 as no agreement with the Treasury.
Page 65 of 131

Covid-19 related costs and funding beyond the initial COVID emergency period
Covid-19 Specific Funding
The trust has been able to recover all reasonable costs related to Covid-19. The main areas of costs so far are highlighted below. In total, SLaM received £7.2m of Covid funding for the 4 months from April to July 2020.
Overall SLaM Funding and Planning 2020/21
The impact of Covid-19 has meant that the normal funding and contracting process with commissioners has been suspended and replaced by emergency funding measures. Currently, these measures are expected to stay in place until the end of September 2020.
The emergency funding and planning regime update:
• SLaM receives a block (lump sum) payment each month based on the Trust’s spending pattern in 2019/20 (the previous financial year) plus 2.8% inflation.
• SLaM receives separate funding for Covid 19 specific costs based on a monthly return. • SLaM receives a top up (increase) or top slice (decrease) of funding to adjust for over or
under funding through the block payment. • Some funding sits outside the block and is dealt with separately (e.g. costs funded by
local authority) • It has been confirmed that Month 5 and 6 (August and September) will be funded in a
similar way to Month 1 to 4. • Beyond Month 6 there remains material uncertainty over financials for the last 6 months
of the year with no final agreement from the Treasury for the NHS as at the time of reporting.
• The Trust is currently developing plans with its Commissioners and system leads based on full receipt of Mental Health Investment Standard (MHIS) funding and reasonable ongoing Covid costs and cost pressures.
• The current expectation is that SLaM will be required to breakeven by the end of 20/21.
£000Backfill for higher sickness absence 921 COVID 19 virus testing 296 Plans to release bed capacity 127 Existing workforce additional shifts 2,042 Expand NHS workforce 1,750 National procurement areas 87 Remote management of patients 4 Remote working for non patient activities 263 Support for stay at home models 82 Segregation of patient pathways 804 Other 822 TOTAL 7,195
Page 66 of 131

Council of Governors 15 September 2020
Name of Report Performance and Quality Report M8 Author
Mary O’Donovan, Head of Quality Rod Booth, Director of Performance, Contracts & Operational Assurance
Presented by
Neil Robertson, Interim Chief Operating Officer Vanessa Smith, Interim Director of Nursing Michael Holland, Medical Director
Purpose
To ensure the Council of Governors is fully sighted on the Trust’s quality and performance against a range of key regulated indicators and constitutional standards and identify areas for improvement This is a refreshed version of the Trust-wide Performance and Quality (P&Q) report with the purpose of providing Quality Committee with: 1. A Trust-wide overview of Performance, Quality and Workforce delivery with risks and mitigations clearly set out; and 2. An updated suite of performance indicators to support measuring the impact of our Right Care: Community Transformation Programme. These indicators will be further developed for next month based on new guidance from NHSE/I on outcome measures for community services (linked to national community transformation funding which we are in the process of planning a bid for with 4 Borough Alliance / community partners) 3. This iteration of the P&Q report will be further developed and refined folliwng review of the specific indicator definitions aligning with other indicator definition reviews in various workstreams across the Trust. Ie. Safety workstream.
Page 67 of 131

Trust Wide Performance and Quality Report:Month 4 (includes August data where available)
Page 68 of 131
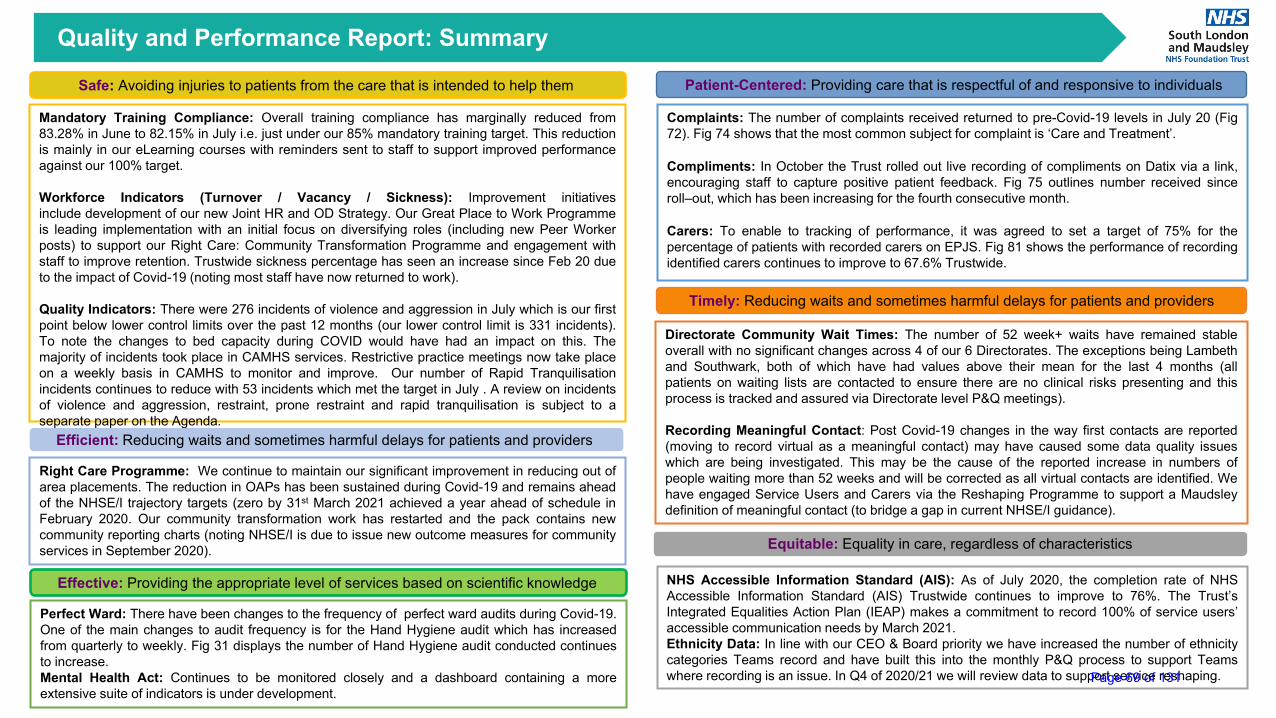
Quality and Performance Report: Summary
Safe: Avoiding injuries to patients from the care that is intended to help them Patient-Centered: Providing care that is respectful of and responsive to individuals
Mandatory Training Compliance: Overall training compliance has marginally reduced from83.28% in June to 82.15% in July i.e. just under our 85% mandatory training target. This reductionis mainly in our eLearning courses with reminders sent to staff to support improved performanceagainst our 100% target.
Workforce Indicators (Turnover / Vacancy / Sickness): Improvement initiativesinclude development of our new Joint HR and OD Strategy. Our Great Place to Work Programmeis leading implementation with an initial focus on diversifying roles (including new Peer Workerposts) to support our Right Care: Community Transformation Programme and engagement withstaff to improve retention. Trustwide sickness percentage has seen an increase since Feb 20 dueto the impact of Covid-19 (noting most staff have now returned to work).
Quality Indicators: There were 276 incidents of violence and aggression in July which is our firstpoint below lower control limits over the past 12 months (our lower control limit is 331 incidents).To note the changes to bed capacity during COVID would have had an impact on this. Themajority of incidents took place in CAMHS services. Restrictive practice meetings now take placeon a weekly basis in CAMHS to monitor and improve. Our number of Rapid Tranquilisationincidents continues to reduce with 53 incidents which met the target in July . A review on incidentsof violence and aggression, restraint, prone restraint and rapid tranquilisation is subject to aseparate paper on the Agenda.
Complaints: The number of complaints received returned to pre-Covid-19 levels in July 20 (Fig72). Fig 74 shows that the most common subject for complaint is ‘Care and Treatment’.
Compliments: In October the Trust rolled out live recording of compliments on Datix via a link,encouraging staff to capture positive patient feedback. Fig 75 outlines number received sinceroll–out, which has been increasing for the fourth consecutive month.
Carers: To enable to tracking of performance, it was agreed to set a target of 75% for thepercentage of patients with recorded carers on EPJS. Fig 81 shows the performance of recordingidentified carers continues to improve to 67.6% Trustwide.
Effective: Providing the appropriate level of services based on scientific knowledge
Perfect Ward: There have been changes to the frequency of perfect ward audits during Covid-19.One of the main changes to audit frequency is for the Hand Hygiene audit which has increasedfrom quarterly to weekly. Fig 31 displays the number of Hand Hygiene audit conducted continuesto increase.Mental Health Act: Continues to be monitored closely and a dashboard containing a moreextensive suite of indicators is under development.
Timely: Reducing waits and sometimes harmful delays for patients and providers
Directorate Community Wait Times: The number of 52 week+ waits have remained stableoverall with no significant changes across 4 of our 6 Directorates. The exceptions being Lambethand Southwark, both of which have had values above their mean for the last 4 months (allpatients on waiting lists are contacted to ensure there are no clinical risks presenting and thisprocess is tracked and assured via Directorate level P&Q meetings).
Recording Meaningful Contact: Post Covid-19 changes in the way first contacts are reported(moving to record virtual as a meaningful contact) may have caused some data quality issueswhich are being investigated. This may be the cause of the reported increase in numbers ofpeople waiting more than 52 weeks and will be corrected as all virtual contacts are identified. Wehave engaged Service Users and Carers via the Reshaping Programme to support a Maudsleydefinition of meaningful contact (to bridge a gap in current NHSE/I guidance).
Efficient: Reducing waits and sometimes harmful delays for patients and providers
Right Care Programme: We continue to maintain our significant improvement in reducing out ofarea placements. The reduction in OAPs has been sustained during Covid-19 and remains aheadof the NHSE/I trajectory targets (zero by 31st March 2021 achieved a year ahead of schedule inFebruary 2020. Our community transformation work has restarted and the pack contains newcommunity reporting charts (noting NHSE/I is due to issue new outcome measures for communityservices in September 2020). Equitable: Equality in care, regardless of characteristics
NHS Accessible Information Standard (AIS): As of July 2020, the completion rate of NHSAccessible Information Standard (AIS) Trustwide continues to improve to 76%. The Trust’sIntegrated Equalities Action Plan (IEAP) makes a commitment to record 100% of service users’accessible communication needs by March 2021.Ethnicity Data: In line with our CEO & Board priority we have increased the number of ethnicitycategories Teams record and have built this into the monthly P&Q process to support Teamswhere recording is an issue. In Q4 of 2020/21 we will review data to support service reshaping.Page 69 of 131

www.slam.nhs.uk
Section 1: Right Care - Community Services
Page 70 of 131

Directorate Community Waiting TimesTi
mel
yPerformance and Quality Indicators
Background: Wait times remain on agenda atDirectorates’ local team meetings, with all staff fullyengaged in the work to reduce waiting times, mitigatechallenges and oversee actions agreed. Overall thenumber of 52 week+ waits is reducing marginally.Directorates will continue to monitor closely andimprove data quality.The Chief Operating Officer is working with each ODto develop a plan for eradicating all 52 week waits.
What the Charts tell Us:Fig 1 Shows waiting times for Borough directorates
Figs 2 to 8: show the number of 52 week + waits bydirectorate ( Excluding BDP and Addictions)
Number of 52 week+ waits have remained stable withno significant changes across most ofthe Directorates. The exceptions being Lambeth andSouthwark both of which have had values above theirmean for the last 4 months
Post Covid-19 changes in the way first contacts arereported have caused some data quality issues whichare being investigated and may be the cause of thereported increase in waiting times.
Lewisham and PMOA have maintained their goodperformance with only 1 person waiting over 52weeks in PMOA and 0 in Lewisham
Fig 2: CAMHS 52 + week waiting has continued toreduce from a peak of 95 in October 2019 to 27 InJune 2020
Fig 1: Community Patient Wait Times by Directorate. Source: Power BI Performance and Contracts Workspace
Fig 2: Community Patient Wait Times (CAMHS). Source: Power BI P&C Workspace
Fig 3: Community Patient Wait Times (Croydon). Source: Power BI P&C Workspace
Fig 4: Community Patient Wait Times (Lambeth). Source: Power BI P&C Workspace
Fig 5: Community Patient Wait Times (Lewisham). Source: Power BI P&C Workspace
Fig 6: Community Patient Wait Times (Southwark). Source: Power BI P&C Workspace
Fig 7: Community Patient Wait Times (MHOA). Source: Power BI P&C Workspace
Fig 8: Community Patient Wait Times (PMIC). Source: Power BI P&C Workspace
Reporting Month 4
Page 71 of 131

Discharges & Follow-ups Ef
ficie
ntPerformance and Quality Indicators
Fig. 9
Fig. 10
Reporting month 4
Page 72 of 131
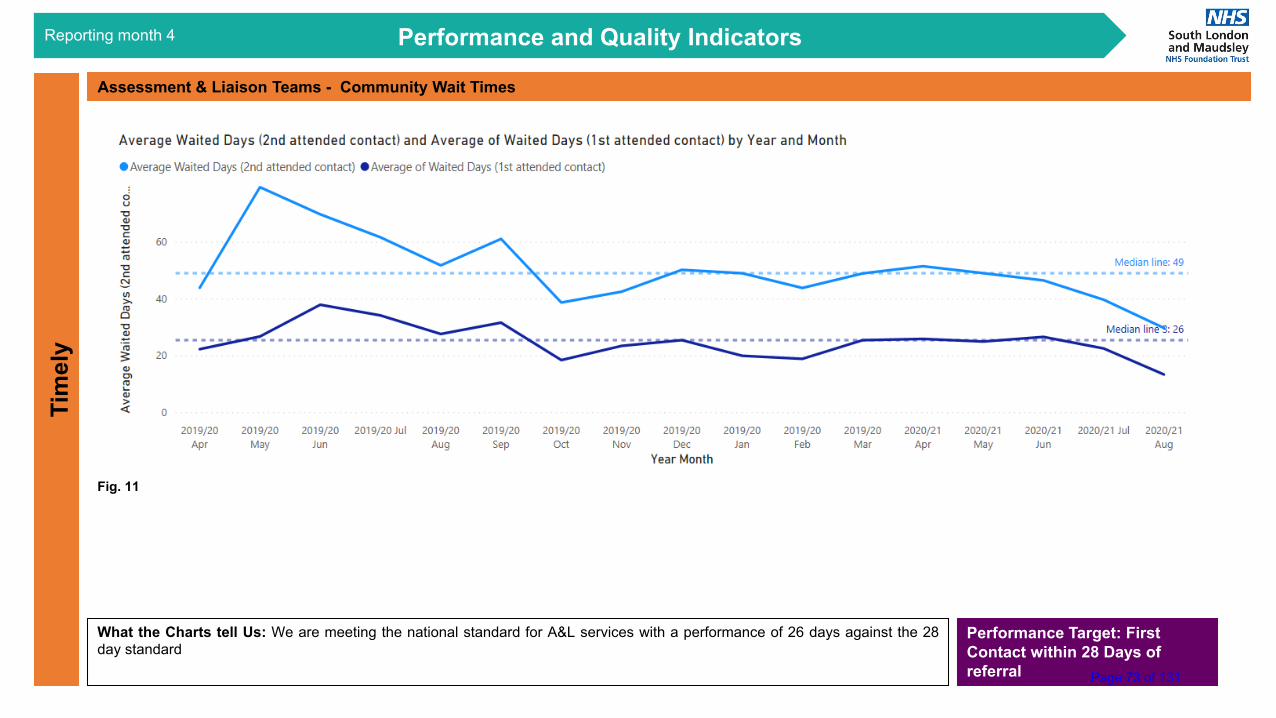
Assessment & Liaison Teams - Community Wait TimesTi
mel
yPerformance and Quality Indicators
What the Charts tell Us: We are meeting the national standard for A&L services with a performance of 26 days against the 28day standard
Reporting month 4
Performance Target: First Contact within 28 Days of referral
Fig. 11
Page 73 of 131

Community Metrics Assessment & Liaison TeamsTi
mel
yPerformance and Quality Indicators
What the charts are telling us:
• Numbers of referrals have returned to pre-Covid-19 levels in the past 2 weeks
• Treatment duration levels on closed cases are stable
• Discharge levels are stable (but subject to monthly fluctuation – potentially as a result of data uploads)
Reporting month 4
Fig. 12
Fig. 13
Fig. 14 Page 74 of 131

Community Metrics Home Treatment TeamsTi
mel
yPerformance and Quality Indicators
What the charts are telling us:
• Numbers of referrals have returned to pre-Covid-19 levels
• Average treatment duration on closed cases is 16 days
• Discharges remain stable at 55 service users per week Trust Wide
Reporting month 4
Fig. 15
Fig. 16
Fig. 17Page 75 of 131
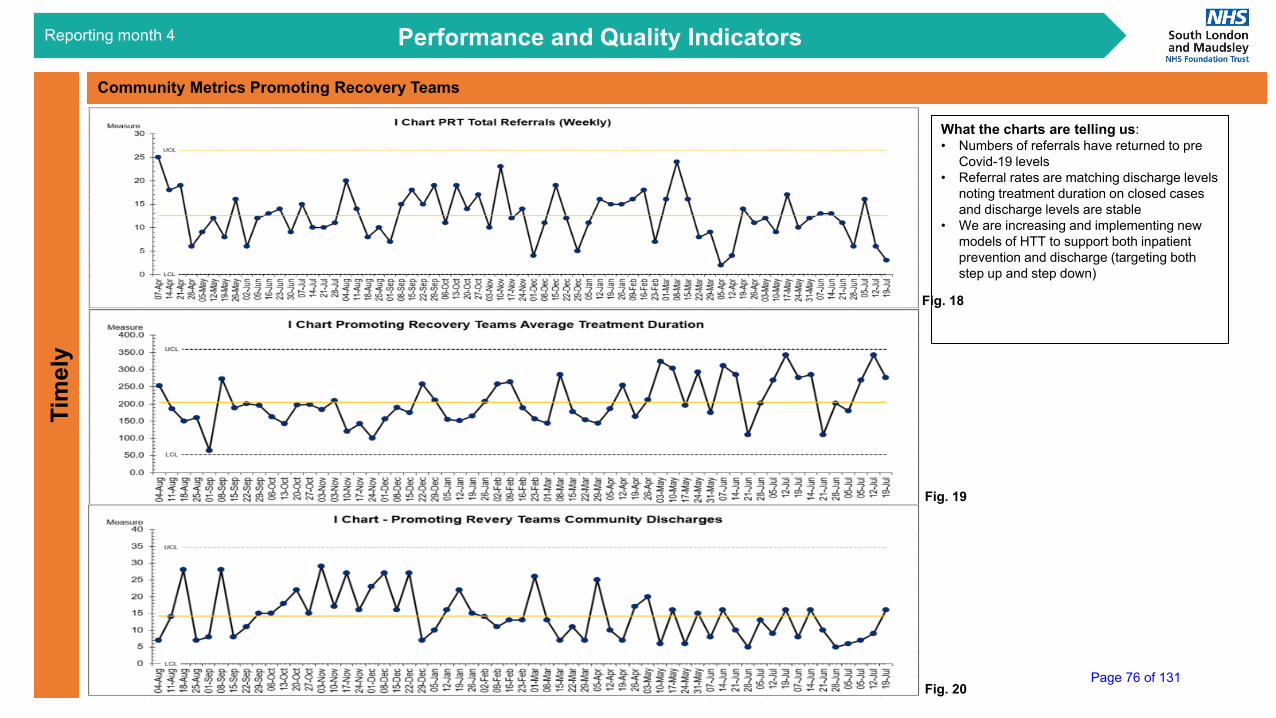
Community Metrics Promoting Recovery TeamsTi
mel
yPerformance and Quality Indicators
What the charts are telling us:• Numbers of referrals have returned to pre
Covid-19 levels• Referral rates are matching discharge levels
noting treatment duration on closed cases and discharge levels are stable
• We are increasing and implementing new models of HTT to support both inpatient prevention and discharge (targeting both step up and step down)
Reporting month 4
Fig. 18
Fig. 19
Fig. 20Page 76 of 131

Community Metrics Caseload EOMTi
mel
yPerformance and Quality Indicators
What the charts are telling us:• Numbers of referrals have returned
to pre Covid-19 levels• There has been an increase on
A&L caseload levels which reflectsthe increase in referrals - notingtreatment duration and dischargelevels are stable. This mayindication a need for increasedcapacity which is being reviewed aspart of our Communitytransformation plans
• HTT caseloads are back tobusiness as usual levels
Reporting month 4
Fig. 21
Fig. 22
Fig. 23 & 24Page 77 of 131

Performance and Quality IndicatorsPa
tient
-Cen
tred
How we are connecting with patients
Reporting month 4
To provide an updateon work underway onhow we areconnecting withpatients a dashboardhas been developedto show:
• Numbers ofcontacts
• Contact method• Gender and
ethnicitybreakdown
For next month thiswill be broken downinto community teams(currently all Trustcontacts)
We can see the largeshift to telephone andvideo contact from 1st
March.
Our new ethnicitycategories will alsoimprove on the datareported here for nextmonth.
Fig. 25Page 78 of 131

www.slam.nhs.uk
Section 2: Right Care - Acute Pathway
Page 79 of 131

Right Care (Acute Pathway)Ef
ficie
ntPerformance and Quality Indicators
Fig 26: Trust Total MHAA Cancellations – Source: Performance and Contracts
Right Care Programme: We continue to maintain our significant improvement in reducing out of area placements. The reduction in OAPs has been sustained during Covid-19 and remains ahead of the NHSE/I trajectory targets (zero by 31st March 2021 achieved a year ahead of schedule in February 2020. Our community transformation workhas restarted and the pack contains new community reporting charts (noting NHSE/I is due to issue new outcome measures for community services in September 2020. Inaddition to achieving zero out of area placement we have also achieved and sustained a 30% reduction in 12 hour ED breaches since Feb 2020.
Reporting month 4
Fig 27: I Chart LSLC 12 hour ED Breaches – Source: Performance and Contracts
Fig 28: I Chart Trust Total External Overspill –Source: Performance and Contracts
Page 80 of 131

Medically Fit for Discharge (MFFD)
Effic
ient
Performance and Quality Indicators
Fig 29 : Trust Total MFFD Days
Fig 30: Trust Total Patients MFFD & DToC)
Reporting month 4
What the Charts tell Us:
Trust wide MFFD days reducedfrom 2993 in Jan 2020 to 615 inMay, a reduction ofapproximately 80%.
This lower level has beenmaintained reducing further to493 this month.
Our ongoing focus on medicallyfit for transfer is resulting in apositive change.
Page 81 of 131
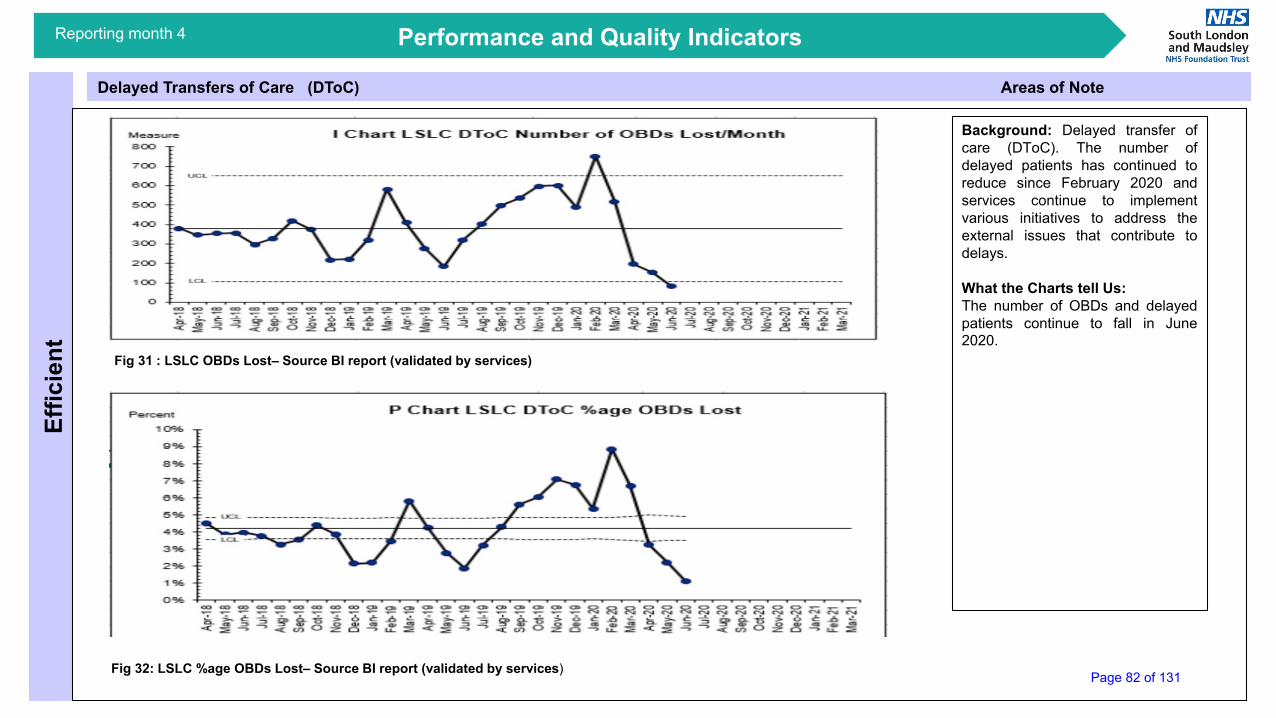
Delayed Transfers of Care (DToC) Areas of Note
Effic
ient
Performance and Quality Indicators
Fig 31 : LSLC OBDs Lost– Source BI report (validated by services)
Fig 32: LSLC %age OBDs Lost– Source BI report (validated by services)
Reporting month 4
Background: Delayed transfer ofcare (DToC). The number ofdelayed patients has continued toreduce since February 2020 andservices continue to implementvarious initiatives to address theexternal issues that contribute todelays.
What the Charts tell Us:The number of OBDs and delayedpatients continue to fall in June2020.
Page 82 of 131

MHLT A&E Breaches and ActivityEf
ficie
ntPerformance and Quality Indicators
Fig 33: LSLC A&E Total Breaches due to MHLT (All over 4 hours
Fig 34: LSLC Total A&E Assessments Source: A&E Monthly Returns
Reporting month 4
Background: ED liaison teams are a keycomponent in the crisis care pathway.
What the Charts tell Us:Our 4 hour plus breaches reduced in Marchand April linked to an overall reduction inactivity levels (Mental Health presentations inour acute partner ED departments). Sincethen breaches and activity levels havesteadily increased to above average levels inJuly. The increase in breaches in July reflectsa significant increase in the number ofpatients waiting between 4 and six hours – inthe main driven by a delay in referral to ourliaison team from acute partner colleagues.The number of patients waiting over 6 hoursdid not change significantly demonstratingonce alerted our teams are able to get thereand assess patients quicky.
Total attendances dipped during the lockdownperiod but have now recovered to pre Covid-19 levels.
Page 83 of 131

Length of Stay Ef
ficie
ntPerformance and Quality IndicatorsReporting month 4
What the Charts tell Us:
To note:
• 1st April 2018 to31st March 2019Benchmarking showsus at 49 days LoSTrust Wide againstnational performanceof 35 days
• 1st April 2019 to 31st
March 2019/20Deming data showsan improved 43.57position for LoS
Fig. 35
Page 84 of 131

www.slam.nhs.uk
Section 3: National Standards - Delivering the NHS Long Term Plan
Page 85 of 131

National standards - IAPT Access targetsTi
mel
yPerformance and Quality Indicators
Background
NHS England has suspended the IAPT performance targets during the Covid-19 outbreak.
Underlying Issues
Croydon IAPT Rreferrals for May 2020 were muchmore than seen in April 2020 due to Covid-19 andtargets are suspended for Q1 20/21.
Lambeth IAPT Referrals have increased in Mayand June 2020 and over the last few weeks, toaround 80% of normal levels
Southwark IAPT Referral number for May 2020has increased by 40% compared to April, but theMay figure was still only at 50% of normal rate.
Lewisham IAPT The level of referral to IAPT hasbeen much lower in Q1 but is returning to expectedlevels, of around 1,000 plus. Focus has been onreducing therapy waiting lists and with thetransformation to a step 4 IAPT+ service..
Reporting month 4
Performance Target:50% Recovery Rate75% Treatment start within 6 weeks95% Treatment start within 18 weeks
Fig. 36
Page 86 of 131

National standards – Dementia DiagnosisTi
mel
y
BackgroundThe national standard is that all services meetat least 67% of the expected population (trajectory) to have access to the right diagnosisof dementia.
What the Charts are Telling UsDementia data performance exceeded thenational ambition for a dementia diagnosis rateof 67%, with the Trust’s 4 main CCGsexceeding the national two thirds diagnosistargets in June 2020.
Underlying Issues: None to note
Performance and Quality IndicatorsReporting month 4
Fig 37: Dementia Diagnosis Rate for LSLC . Source: Performance & Contracts
Performance Target: 67% + of expected population receive a diagnosis
Page 87 of 131
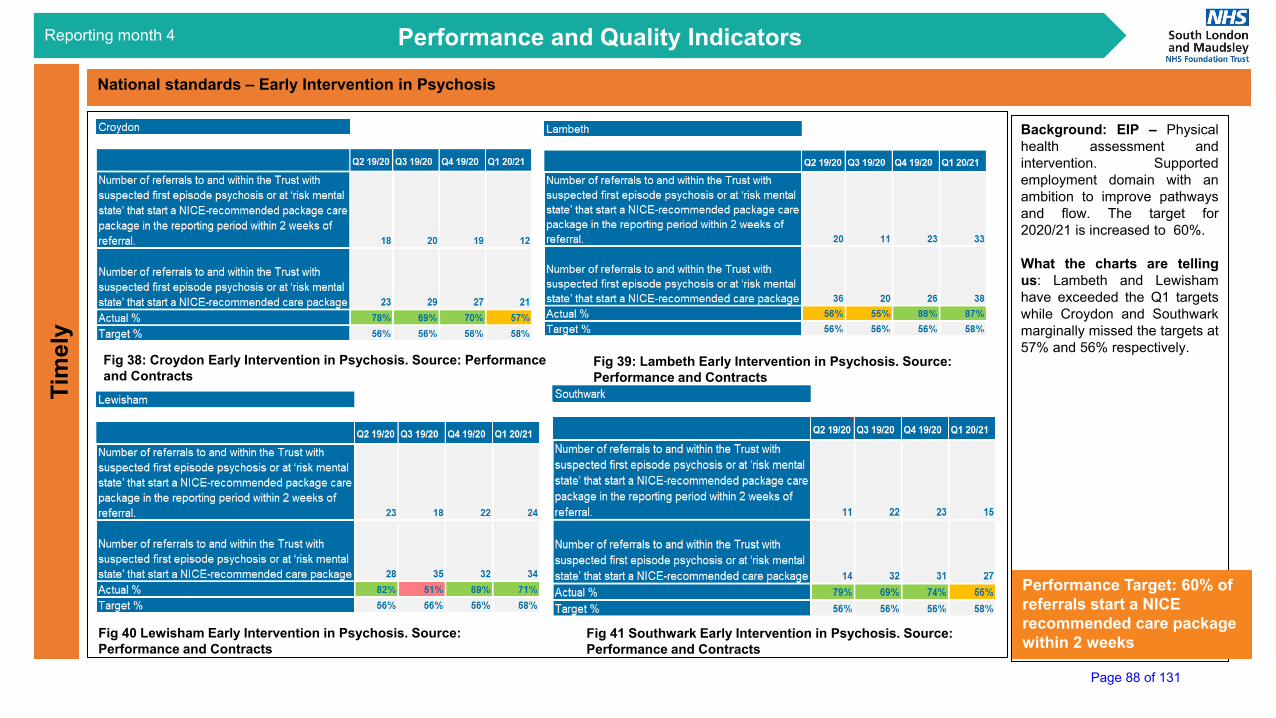
National standards – Early Intervention in PsychosisTi
mel
yPerformance and Quality Indicators
Fig 38: Croydon Early Intervention in Psychosis. Source: Performance and Contracts
Fig 39: Lambeth Early Intervention in Psychosis. Source: Performance and Contracts
Fig 40 Lewisham Early Intervention in Psychosis. Source: Performance and Contracts
Fig 41 Southwark Early Intervention in Psychosis. Source: Performance and Contracts
Background: EIP – Physicalhealth assessment andintervention. Supportedemployment domain with anambition to improve pathwaysand flow. The target for2020/21 is increased to 60%.
What the charts are tellingus: Lambeth and Lewishamhave exceeded the Q1 targetswhile Croydon and Southwarkmarginally missed the targets at57% and 56% respectively.
Reporting month 4
Performance Target: 60% of referrals start a NICE recommended care package within 2 weeks
Page 88 of 131

National Standards - CAMHS Waiting Times (LSLC borough Combined Data)
Tim
ely
Performance and Quality Indicators
Fig 43: LSLC combined data and National & Specialist - Young people waiting over 39 weeks at the end of the month Apr 2019 – July 2020.Source: Power BI CAMHS App
Fig 42: LSLC combined data and National &Specialist - Young people waiting over 52 weeks at the end of the month Apr 2019 – July 2020. Source: Power BI CAMHS App
Reporting month 4
BackgroundAll 52 week and over waiters have a plan and havebeen offered appointments. The remaining people are thosewho have DNAd or cancelled, or who have chosen not toaccept a remote appointment but who don’t fit criteria for aFace to Face one ( i.e. urgent/complex/ at risk). Effort in allservices is directed at long waiters , especially those over 39weeks, to try to ensure they do not become 52-week waiters.
What the Charts are Telling UsThe number of 52 weeks waits has remained stable duringCovid-19 with nobody waiting in N&S, except for increasingnumber of long waits in Croydon, due to the issue with theADOS diagnostic tool which is not compatible with remoteassessments. Croydon is the only borough where ASDdiagnostic assessment for all 5-18-year olds is commissionedfrom CAMHS ( elsewhere this is with community paediatricservices).
Underlying IssuesThere is difficulty with Croydon ASD diagnosticassessments because ADOS, the diagnostic tool generallyused, is not valid if used remotely or with PPE. A Quality Impactassessment has been completed on the ASD issue for allrelevant Trust services, and consideration is being given as towhat could be done to mitigate the issues. A senior clinicalworking group is preparing a Safer Working paper on this.
The planned opening of a temporary Tyson East Adolescent uniton the Acorn Lodge site at Bethlem Royal Hospital, has been puton hold until further notice. NHSE have been informed of delay.
Page 89 of 131

www.slam.nhs.uk
Section 4: Month Three Performance & Quality Data
Page 90 of 131

IncidentsSa
fePerformance and Quality Indicators
Fig 45: Total Deaths reported by week Source: Datix
Fig 44: Total Incidents reported by week. Source: Datix
Reporting month 4
What the chart tell us:The weekly numbers of total incidents and deaths are within the control limits in July 20.
UCL
LCL0
5
10
15
20
25
30
35
31/1
2/20
1714
/01/
2018
28/0
1/20
1802
/11/
2018
25/0
2/20
1803
/11/
2018
25/0
3/20
1804
/08/
2018
22/0
4/20
1805
/06/
2018
20/0
5/20
1806
/03/
2018
17/0
6/20
1807
/01/
2018
15/0
7/20
1829
/07/
2018
08/1
2/20
1826
/08/
2018
09/0
9/20
1823
/09/
2018
10/0
7/20
1821
/10/
2018
11/0
4/20
1818
/11/
2018
12/0
2/20
1816
/12/
2018
30/1
2/20
1813
/01/
2019
27/0
1/20
1902
/10/
2019
24/0
2/20
1903
/10/
2019
24/0
3/20
1904
/07/
2019
21/0
4/20
1905
/05/
2019
19/0
5/20
1906
/02/
2019
16/0
6/20
1930
/06/
2019
14/0
7/20
1928
/07/
2019
08/1
1/20
1925
/08/
2019
09/0
8/20
1922
/09/
2019
10/0
6/20
1920
/10/
2019
11/0
3/20
1917
/11/
2019
12/0
1/20
1915
/12/
2019
29/1
2/20
1901
/12/
2020
26/0
1/20
2002
/09/
2020
23/0
2/20
2003
/08/
2020
22/0
3/20
2004
/05/
2020
19/0
4/20
2005
/03/
2020
17/0
5/20
2031
/05/
2020
14/0
6/20
2028
/06/
2020
07/1
2/20
2026
/07/
2020
C Chart - Total deaths reported by weekCount
UCL
LCL
0
50
100
150
200
250
300
350
400
450
31/1
2/20
1714
/01/
2018
28/0
1/20
1802
/11/
2018
25/0
2/20
1803
/11/
2018
25/0
3/20
1804
/08/
2018
22/0
4/20
1805
/06/
2018
20/0
5/20
1806
/03/
2018
17/0
6/20
1807
/01/
2018
15/0
7/20
1829
/07/
2018
08/1
2/20
1826
/08/
2018
09/0
9/20
1823
/09/
2018
10/0
7/20
1821
/10/
2018
11/0
4/20
1818
/11/
2018
12/0
2/20
1816
/12/
2018
30/1
2/20
1813
/01/
2019
27/0
1/20
1902
/10/
2019
24/0
2/20
1903
/10/
2019
24/0
3/20
1904
/07/
2019
21/0
4/20
1905
/05/
2019
19/0
5/20
1906
/02/
2019
16/0
6/20
1930
/06/
2019
14/0
7/20
1928
/07/
2019
08/1
1/20
1925
/08/
2019
09/0
8/20
1922
/09/
2019
10/0
6/20
1920
/10/
2019
11/0
3/20
1917
/11/
2019
12/0
1/20
1915
/12/
2019
29/1
2/20
1901
/12/
2020
26/0
1/20
2002
/09/
2020
23/0
2/20
2003
/08/
2020
22/0
3/20
2004
/05/
2020
19/0
4/20
2005
/03/
2020
17/0
5/20
2031
/05/
2020
14/0
6/20
2028
/06/
2020
07/1
2/20
2026
/07/
2020
C Chart - Total incidents reported by weekCount
CAMHS PICU
Peak WardNG Feeding
Page 91 of 131

Violence and AggressionSa
fe
Background: One of the Quality Priorities of is reducing all types of restrictive practice by 50% over 2018-2021.
What the chart tell us: There were 276 incident of violence and aggression Trustwide in July 20. It fell below the lower control limit for the first time this month. CAMHS has the highest number of V&A incidents, with most of them from BAU.
Actions being taken: Restrictive practice meetings will take place on a weekly basis in CAMHS to monitor and improve. A deep dive in violence and aggression, restraint, prone restraint an rapid tranquilisation is scheduled for Quality Committee in September 2020 to look at our current position and how we are going to reach the target.
Note: The safety workstream including Deputy Head of Nursing, Deputy Medical Director, members of the QI team (including a Service User Coordinator) and the Lead Nurse for Reducing Practice have been meeting at least weekly since April to review data, share progress and obstacles, and drive forward the testing and implementation of the following initiatives related to violence reduction. This has included a review of the definitions set two years ago around these quality priorities. Following the safety deep dive at the next quality committee the definitions may be refined further.
Quality Priority: Reducing violence by 50% over 3 yearsAim 20/21: 173 per month• The above target was agreed before the opening of CAMHS PICU and
Peak Ward, hence it is not applicable to the Trustwide trend
Performance and Quality Indicators
Fig 46: Total V&A Incidents. Source: Datix
Fig 48: V&A Incidents in July 2020 by Directorates. Source: Datix
Data extracted on 3.8.2020
Reporting month 4
Fig 47: Total V&A (excluding CAMHS PICU, Peak Ward and EDU) Incidents. Source: Datix
12.50%20.39%
14.14%17.76%
2.96%5.59%
10.86%15.46%
BDPCAMHSCroydonLambeth
LewishamSouthwark
Older AdultsSpecialist
Violence and Aggression by Directorates - Jul 20(% of Trustwide Total)
Special cause concernSpecial cause improvement
UCL
LCL
0
100
200
300
400
500
600
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide incidents of violence and aggressionCount
CAMHS PICU NG Feeding Peak Ward
UCL
LCL
0
100
200
300
400
500
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide (excluding CAMHS PICU, Peak Ward) incidents of violence and aggression
Target
Count
2017/18 2018/19 2019/20 2020/21Baseline 4158
Yearly Target 3464 2769 2079
Yearly Actual 4372 4185 1268(Apr-Jul)
Page 92 of 131

Safe
Performance and Quality Indicators
Fig 49: Total Incidents of Restraint Trust wide. Source: Datix
Use of restraint
Data extracted on 3.8.2020
Reporting month 4
Background: One of the Quality Priorities of is reducing all types of restrictive practice by 50% over 2018-2021.
What the chart tell us:There were 222 incident of restraint Trustwide in July 20, with most of them from CAMHS PICU and CAMHS BAU.
Actions being taken: Restrictive practice meetings will take place on a weekly basis in CAMHS to monitor and improve. A deep dive in violence and aggression, restraint, prone restraint and rapid tranquilisation Trustwide is scheduled for Quality Committee in September 2020 to look at our current position and how we are going to reach the target.
Quality Priority: Reduction in restraint by 50% over 3 years – Trust Deming DashboardAim 20/21: 71.5 per month• The above target was agreed before the opening of CAMHS
PICU and Peak Ward, hence it is not applicable to the Trustwide trend
Special cause concernSpecial cause improvement
3.68%37.13%
14.34%11.40%
12.50%15.44%
3.31%2.21%
BDPCAMHSCroydonLambeth
LewishamSouthwark
Older AdultsSpecialist
Restraint by Directorates - Jul 20(% of Trustwide Total)
Fig 51: Restraint Incidents in July 2020 by Directorates. Source: Datix. Source: Datix
Fig 50: Total Incidents of Restraint Trust wide (excluding CAMHS PICU, Peak Ward, EDU. Source: Datix
UCL
LCL
0
100
200
300
400
500
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide incidents of restraintCount
CAMHS PICUNG Feeding Peak Ward
UCL
LCL
0
100
200
300
400
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide (excluding CAMHS PICU, Peak Ward) incidents of restraint
Target
Count
2017/18 2018/19 2019/20 2020/21Baseline 1716
Yearly Target 1429 1142 858
Yearly Actual 1789 2973926
(Apr-Jul)
Page 93 of 131

Use of prone restraintSa
fePerformance and Quality Indicators
Fig 52: Total Incidents of Prone Restraint Trust wide. Source: Datix
Fig 53: Total Incidents of Prone Restraint Trust wide excluding CAMHS PICU and Peak Ward. Source: Datix
Data extracted on 3.8.2020
Reporting month 4
Background: One of the Quality Priorities of is reducing prone restraint to zero over 2018-2021.
What the chart tell us:The number of prone restraint Trustwide is within the normal variation in July 20. Southwark has the highest number of prone restraint incidents (14), with most of them in ES1.
Actions being taken: Performance is monitored in the monthly directorate Performance and Quality meetings. Plan is in place in Southwark to reduce rapid tranquilisation incidents. A deep dive in violence and aggression, restraint, prone restraint and rapid tranquilisation Trustwide is scheduled for Quality Committee in September 2020 to look at our current position and how we are going to reach the target.
Quality Priority: Reduction in prone restraint by zero by 3 yearsAim 20/21: 0 per month• The above target was agreed before the opening of CAMHS PICU
and Peak Ward, hence it is not applicable to the Trustwide trend
2.17%21.74%
17.39%17.39%
15.22%26.09%
BDPCAMHSCroydonLambeth
LewishamSouthwark
Prone Restraint by Directorates - Jul 20
Special cause concernSpecial cause improvement
Fig 54: Prone restraint Incidents in July 2020 by Directorates. Source: Datix
UCL
LCL
020406080
100120
Aug-
17Se
p-17
Oct
-17
Nov
-17
Dec
-17
Jan-
18Fe
b-18
Mar
-18
Apr-1
8M
ay-1
8Ju
n-18
Jul-1
8Au
g-18
Sep-
18O
ct-1
8N
ov-1
8D
ec-1
8Ja
n-19
Feb-
19M
ar-1
9Ap
r-19
May
-19
Jun-
19Ju
l-19
Aug-
19Se
p-19
Oct
-19
Nov
-19
Dec
-19
Jan-
20Fe
b-20
Mar
-20
Apr-2
0M
ay-2
0Ju
n-20
Jul-2
0
C Chart - Trustwide all incidents of prone restraintCount
CAMHS PICU
NG feeding Peak Ward
UCL
LCL
0
50
100
150
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide (excluding CAMHS PICU, Peak Ward) all incidents of prone restraint
Count
2017/18 2018/19 2019/20 2020/21Baseline 708
Yearly Target 472 236 0
Yearly Actual 549 574206
(Apr - Jul)
Page 94 of 131

Safe
Performance and Quality Indicators
Rapid Tranquilisation
Fig 55: Total Incidents of Rapid Tranquilisation Trust wide. Source: Datix
Fig 56: Total Incidents of Rapid Tranquilisation (Trustwide excluding CAMHS PICU, Peak Ward and EDU). Source: Datix
Data extracted on 3.8.2020
Reporting month 4
3.92%
17.65%
29.41%
49.02%
CAMHS
Croydon
Lewisham
Southwark
Rapid Tranquilisation by Directorates - Jul 20(% of Trustwide Total)
Background: One of the Quality Priorities of is reducing the use of rapid tranquilisation by 25% over 2018-2021.
What the chart tell us:The Trustwide number of incidents of rapid tranquilisation was 53 in July 20, which met the target. Most of the incidents were in Southwark Directorate (27), in ES1 and Ruskin.
Actions being taken: Performance is monitored in the monthly directorate Performance and Quality meetings. Plan is in place in Southwark to reduce rapid tranquilisation incidents. A deep dive in violence and aggression, restraint, prone restraint and rapid tranquilisation Trustwide is scheduled for Quality Committee in September 2020 to look at our current position and how we are going to reach the target.
Quality Priority: Reduce the use of rapid tranquilisation by 25% over the next 3 yearsAim 20/21: 53 per month• The above target was agreed before the opening of
CAMHS PICU and Peak Ward, hence it is not applicable to the Trustwide trend
Special cause concernSpecial cause improvement
Fig 57: Rapid Tranquilisation Incidents in July 2020 by Directorates. Source: Datix
UCL
LCL
0
50
100
150
200
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide incidents of rapid tranquilisationCount
CAMHS PICU NG feedingPeak Ward
UCL
LCL
0
50
100
150
Aug-
17
Sep-
17
Oct
-17
Nov
-17
Dec
-17
Jan-
18
Feb-
18
Mar
-18
Apr-1
8
May
-18
Jun-
18
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec
-18
Jan-
19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
C Chart - Trustwide excluding (CAMHS PICU, Peak Ward) incidents of rapid tranquilisation
Target
Count
2017/18 2018/19 2019/20 2020/21Baseline 840Yearly Target 770 700 630
Yearly Actual 772 995259
(Apr-Jul)
Page 95 of 131

Care PlansEf
fect
ivePerformance and Quality Indicators
Fig 58:–Average score and number of audits of ‘Is there evidence of patient involvement in their care plan?’ for Jul 2020 Source: Perfect Ward
Reporting month 4
Background: Perfect Ward audit tool has been used to report audit results on the Quality Priority of care plans being devised collaboratively. The service areas that have scored red will have received feedback from the relevant clinical service lead to aid as a learning tool.The target frequency for each ward/team has been reduced from 12 to 6 since March due to Covid-19.
What the chart tell us:The number of audits undertaken by the Trust exceeded the target frequency. The average score of the care plan audit is at 83%
Actions being taken: Performance is continually being monitored via the Directorate P&Q meetings.
Quality Priority: Increase the number of care plans devised collaboratively over the next 3 years
Page 96 of 131

Effe
ctiv
ePerformance and Quality Indicators
Perfect Ward Average Score (Inpatient) Areas of Note
Fig 59: Perfect Ward Audit Average Score by Inspection Type in Jul 20. Source: Clinical Audit Team and PMO
Reporting month 4
Background: The trust introduced Perfect Ward to replace local paper audits and provide a systematic local clinical audit programme across the trust. This system has amalgamated and reduced the local clinical audits that were carried out by teams on a regular basis to allow easier data collection and a better function to review and improve upon results in a timely and responsive manner.
What the chart tell us: The majority of Directorates achieve a Green average score across all audits in inpatient services. Southwark and Addictions scored 64% in Patient Experience audits in July.
Actions being taken: Audit compliance and results are monitored in the monthly directorate Performance and Quality meetings.
Page 97 of 131

Effe
ctiv
ePerformance and Quality Indicators
Perfect Ward – Hand Hygiene Areas of Note
Fig 60: Perfect Ward Number of Hand Hygiene Audit Completed by Inspection Type. Source: Clinical Audit Team and PMO
Reporting month 4
513
27 32
51 45 51 50
30
70 71
127
172
271
0
50
100
150
200
250
300
Number of Audits Completed - Hand Hygiene Audit Background: There have been increased number of Perfect Ward audits carried out in since March 20 relating to hand hygiene. This is in response to the Covid pandemic and the expectation to carry out increased audits in this area.
What the chart tell us:The number of Hand Hygiene audit continue to increase in July 20.
Actions being taken: The compliance of hand hygiene audits by ward/ are monitored in the monthly directorate Performance and Quality meetings.
Page 98 of 131
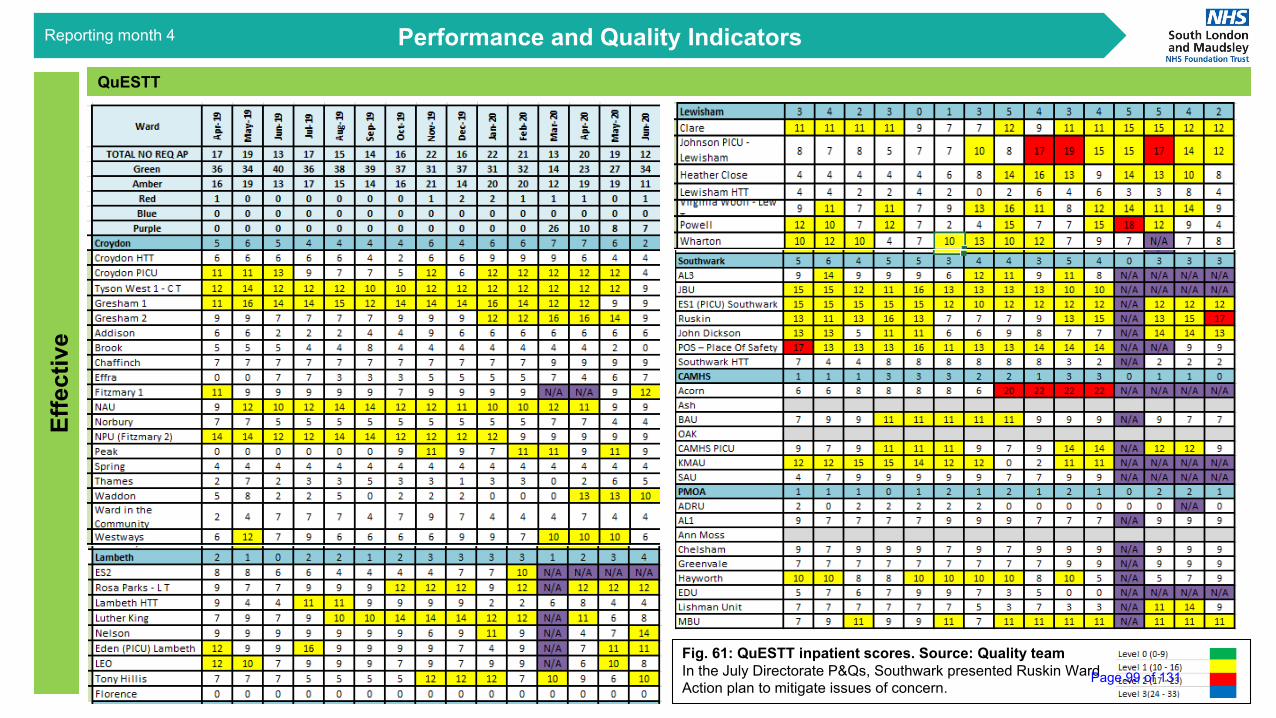
QuESTTEf
fect
ive
Performance and Quality Indicators
Fig. 61: QuESTT inpatient scores. Source: Quality teamIn the July Directorate P&Qs, Southwark presented Ruskin WardAction plan to mitigate issues of concern.
Performance and Quality IndicatorsReporting month 4
Page 99 of 131

Mental Health Act – Use of SectionEf
fect
ive
Performance and Quality Indicators
Performance and Quality Indicators
Fig. 62 Trustwide – Use of Section (Weekly)
Fig. 63 Trustwide – Number of patients who were sectioned (Weekly) Data source: Mental Health Act BI Dashboard
Reporting month 4
Background:The trust monitors useof the MHA to ensurecompliance with legalrequirements and rightcare principles.
What the chart tell us:The use of section andnumber of patientsnewly detainedreduced during thepandemic due to anumber of wardclosures during thattime. As wards havereopened the numbershave started to riseagain.
Actions being taken:Continues to bemonitored closely anda dashboard containinga more extensive suiteof indicators is underdevelopment.
Page 100 of 131

Mental Health Act – Ethnicity of Detained PatientsEf
fect
ive
Performance and Quality Indicators
Performance and Quality Indicators
Fig. 64 Trustwide – Ethnicity of Detained Patients (since April 2020)
Fig. 65 Majority Ethnic Group of Detained Patients by Directorates (since April 2020)Data source: Mental Health Act BI Dashboard
Reporting month 4
What the chart tell us: Around23% of detained patientsTrustwide since April 2020were ‘White – White British’.
Underlying issues:Following the review of thisdata in both the recentoperational directorate MH lawcommittees and the TrustwideMH law committee attentionwas drawn to the number ofblanks recorded in the ethnicityEPJS field.
Actions being taken:Performance in this area isbeing monitored in theDirectorates P&Q meetings.
Directorate Majority Ethnic Group of Detained Patients (Highest %) %BDP White British 38.46%
CAMHS White British 22.94%Croydon Black - Other 22.26%Lambeth Black - Other 19.34%
Lewisham Black - Other 24.39%Southwark White British 23.65%
Older Adults White British 50.00%
SpecialistBlack African 21.43%White - Other 21.43%Not specified 21.43%
Page 101 of 131

Mental Health Act – Section 135 and Section 136 Breaches Ef
fect
ive
Performance and Quality Indicators
Performance and Quality Indicators
Data source: Health-based Place of Safety Overstay Report
Fig. 66 s135 and s136 Breaches by month Fig. 67 s135 Breaches by Borough of Residence
Fig. 68 s136 Breaches by Borough of Residence
Reporting month 4
Background: The nationallegal standard is for the MentalHealth Act assessment whenthe person is on s135 or s136to be completed within 24hours. More than this is abreach and can mean that theperson is held ‘illegally’ in theHealth Based Place of Safety(HBPOS).
What the chart tell us: Fig 66shows that, since COVID thenumber of 24 hour breachesduring March reduced buthave begun to rise again sinceApril.. The reasons foroverstays for the same periodcan be seen at Fig. 69 on thenext page.
0
5
10
15
20
25
30
35
Jan Feb March April May June July
S135 and S136 Breaches since Jan 2020
Section 135 Section 1360
2
4
6
8
10
Croydon Lambeth Lewisham Southwark
S135 Breaches by Borough of Residence
since Jan 2020
July
June
May
April
March
Feb
Jan
05
101520253035404550
S136 Breaches by Borough of Residence since Jan 2020
July
June
May
April
March
Feb
Jan
Page 102 of 131

Mental Health Act – Section 135 and Section 136 Breaches Ef
fect
ive
Performance and Quality Indicators
Performance and Quality Indicators
Data source: Health-based Place of Safety Overstay Report
Fig. 69 Reason of Breach
Reporting month 4
0
5
10
15
20
25
30
35
Jan Feb March April May June July
Reason for Breach since Jan 2020
Expired Before MHA Assessment CompleteS136 Expired Before MHA Assessment CompleteS136 Expired, MHA Assessment Complete, No SLAM Bed AvailableSection 135 expired waiting for AMHP to complete S3Section 136 expired and it was extendedSection 136 was RescindedSection ExtendedSection RescindedSection was extended before it expiredSection was extendedWaiting for Inpatient bed
Background: The national legal standard is for the Mental Health Act assessment when the person is on s135 or s136 to be completed within 24 hours. More than this is a breach and can mean that the person is held ‘illegally’ in the Health Based Place of Safety (HBPOS).
What the chart tell us: Fig 69 shows that the largest cause of legal breaches is ‘Waiting for an inpatient bed’.
Underlying issues: This may be exacerbated during Covid-19 but it needs to be explored and an agreed pathway comparable to that in A/E agreed.
Actions being taken: Continues to be monitored closely and a dashboard containing a more extensive suite of indicators is under development.
Page 103 of 131

NHS Accessible Information StandardEq
uita
blePerformance and Quality Indicators
Fig 70: Trustwide NHS AIS field Completion Rate Source: MyCAMHS Teams, My Team, My Ward
Reporting month 4
Background: The Trust has a contractual obligation, in the Standard NHS Contract, to comply with the NHS Accessible Information Standard (AIS). The Trust’s Integrated Equalities Action Plan (IEAP) makes a commitment to record 100% of service users’ accessible communication needs by March 2021 with the aim of improving care planning with disabled service users.
MyCAMHS Teams, MyTeam and MyWard reports are used to produce the data on the percentage of AIS recorded for seen service users in July 2020 to provide more consistent data
What the chart tell us: As of Jul 2020, the completion rate Trustwide is at 76%
Actions being taken: The performance is continually being monitored via the Directorate P&Q meetings.
0%10%20%30%40%50%60%70%80%90%
100%Ja
n-19
Feb-
19
Mar
-19
Apr-1
9
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec
-19
Jan-
20
Feb-
20
Mar
-20
Apr-2
0
May
-20
Jun-
20
Jul-2
0
Run Chart: Trustwide NHS Accessible Information Standard field Completion Rate
MedianTarget 20/21
MeasureMeasure
86.3% 93.1%71.8%
20.4%
84.4%96.7%
37.6%
75.1%88.0% 95.3% 90.3%
69.4%
0.0%20.0%40.0%60.0%80.0%
100.0%120.0%
NHS Accessisble Information Standard field complete rate - Jul 20
Target 20/21
Fig 71: NHS AIS field Completion Rate by Directorate Source: MyCAMHS Teams, My Team, My WardPage 104 of 131

Performance and Quality Indicators
Fig 72: Total Number of Formal Complaints Trust wide. Source: Datix
Patie
nt-C
entr
edComplaints and Compliments
Fig 73: Number of complaints received by Directorates Source: Datix
Reporting month 4
UCL
LCL
0
10
20
30
40
50
60
70
80
Jul-1
6Au
g-16
Sep-
16O
ct-1
6N
ov-1
6D
ec-1
6Ja
n-17
Feb-
17M
ar-1
7Ap
r-17
May
-17
Jun-
17Ju
l-17
Aug-
17Se
p-17
Oct
-17
Nov
-17
Dec
-17
Jan-
18Fe
b-18
Mar
-18
Apr-1
8M
ay-1
8Ju
n-18
Jul-1
8Au
g-18
Sep-
18O
ct-1
8N
ov-1
8D
ec-1
8Ja
n-19
Feb-
19M
ar-1
9Ap
r-19
May
-19
Jun-
19Ju
l-19
Aug-
19Se
p-19
Oct
-19
Nov
-19
Dec
-19
Jan-
20Fe
b-20
Mar
-20
Apr-2
0M
ay-2
0Ju
n-20
Jul-2
0
C Chart - Trustwide Number of Complaints ReceivedCount
3.8%
9.6%
5.8%
25.0%
30.8%
5.8%
13.5%
5.8%
Addictions
BDP
CAMHS
Croydon
Lambeth
Lewisham
Southwark
PMOA
Number of complaints received by Directorates - Jul 20
1.9%
19.2%
50.0%
9.6%
1.9%
3.8%
1.9%
5.8%
5.8%
Admission/Transfer…
Attitude/Behaviour
Care and Treatment
Communication
Detention under the Mental…
Discharge
Patient…
Patient's property
Other
Primary Subject of Complaints - Jul 20
What the charts tell us: There was a decrease in the number of complaints received during Covid but it returned to pre-Covid level in July 20.
Actions being taken: Complaints and relevant learning are reviewed in detail at Directorate governance meetings
Special cause concern
Special cause improvementFig 74: Primary Subject of Complaints Source: Datix
Page 105 of 131
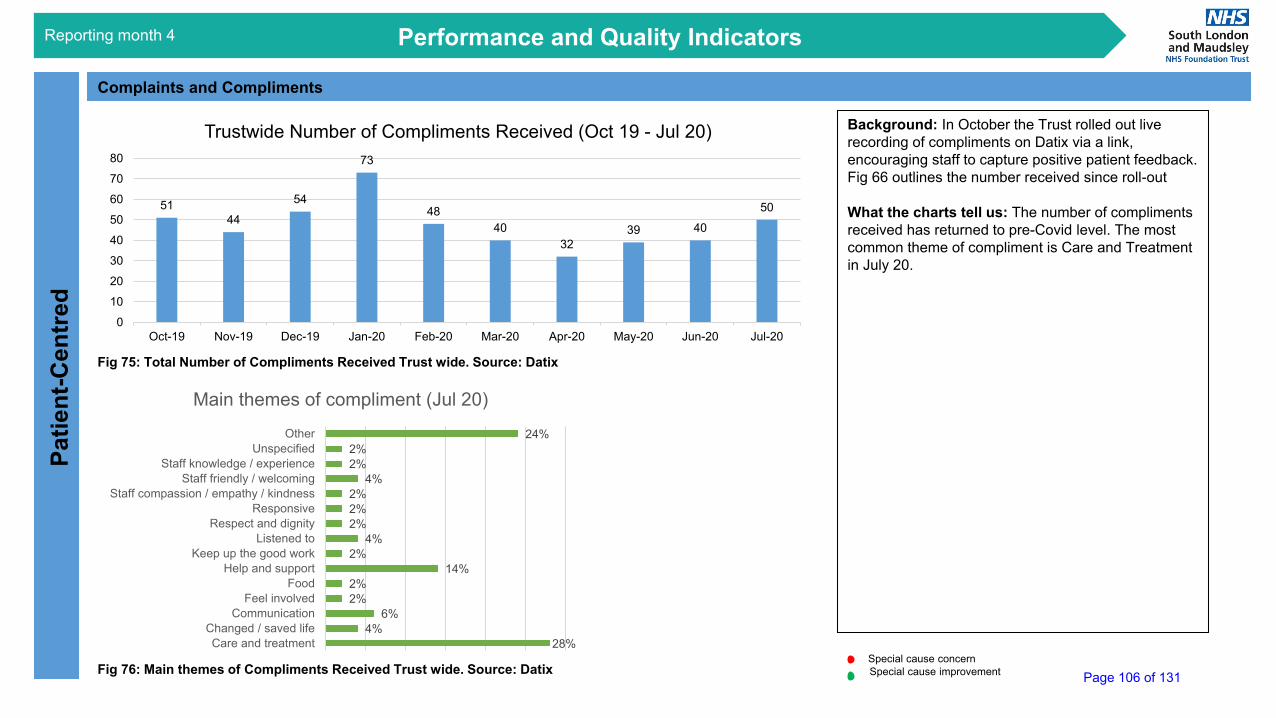
Performance and Quality IndicatorsPa
tient
-Cen
tred
Complaints and Compliments
Fig 75: Total Number of Compliments Received Trust wide. Source: Datix
Reporting month 4
5144
54
73
4840
3239 40
50
0
10
20
30
40
50
60
70
80
Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20 May-20 Jun-20 Jul-20
Trustwide Number of Compliments Received (Oct 19 - Jul 20)
28%4%
6%2%2%
14%2%
4%2%2%2%
4%2%2%
24%
Care and treatmentChanged / saved life
CommunicationFeel involved
FoodHelp and support
Keep up the good workListened to
Respect and dignityResponsive
Staff compassion / empathy / kindnessStaff friendly / welcoming
Staff knowledge / experienceUnspecified
Other
Main themes of compliment (Jul 20)
Fig 76: Main themes of Compliments Received Trust wide. Source: Datix
Background: In October the Trust rolled out live recording of compliments on Datix via a link, encouraging staff to capture positive patient feedback. Fig 66 outlines the number received since roll-out
What the charts tell us: The number of compliments received has returned to pre-Covid level. The most common theme of compliment is Care and Treatment in July 20.
Special cause concernSpecial cause improvement Page 106 of 131

PEDIC/Friends and Family Test (FFT)Pa
tient
-Cen
tredPerformance and Quality Indicators
Fig 77: Trust wide PEDIC scores.Source: PowerBI PEDIC Dashboard
Reporting month 4
Background: PEDIC surveys enable us to measure how people are experiencing our services over time so that we can continually work to improve the services we provide. They include the national indicator for patient experience, the Friends and Family Test (FFT). The trust is working to NHS England and Improvement COVID-19/FFT guidance issued in March 2020 and has therefore temporarily suspended data collection via paper and device methods; all teams are able to provide online survey links as necessary. There are no penalties for non-compliance with any part of the FFT guidance to reduce burden and release operational capacity.
What the chart tell us: The score for ‘Are staff kind and caring’ remains the highest amongst all questions, while that of ‘Do you know how to make a complaint?’ remains the lowest.
Actions being taken: The performance is continuously monitored in Directorate P&Q meetings.
Quality Priority: Increase to 90% the number of patients who would recommend the service to friends or family if they needed similar care or treatment
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
Jul-1
8
Aug-
18
Sep-
18
Oct
-18
Nov
-18
Dec-
18
Jan-
19
Feb-
19
Mar
-19
Apr-
19
May
-19
Jun-
19
Jul-1
9
Aug-
19
Sep-
19
Oct
-19
Nov
-19
Dec-
19
Jan-
20
Feb-
20
Mar
-20
Apr-
20
May
-20
Jun-
20
Jul-2
0
Trustwide PEDIC scores (% positive)
Do you feel involved in your own care?Are staff kind & caring?Do you know how to make a complaint?Do we treat you as an individual?Do you feel safe here?Has the purpose and side effects of your medication been explained to you?Do you know what to do in an emergency or mental health crisis?
Page 107 of 131

PEDIC/Friends and Family Test (FFT)Pa
tient
-Cen
tredPerformance and Quality Indicators
Fig 78: Trust wide FFT scores (Positive). Source: PowerBI PEDIC Dashboard
Fig 79: National, Regional (London) and Trustwide FFT scoresSource: NHS England
Reporting month 4
Background: PEDIC surveys enable us to measure how people are experiencing our services over time so that we can continually work to improve the services we provide. They include the national indicator for patient experience, the Friends and Family Test (FFT). NHSE has launched a new analysis tool to show FFT performance over time, as shown in Fig 79.
The trust is working to NHS England and Improvement COVID-19/FFT guidance issued in March 2020 and has therefore temporarily suspended data collection via paper and device methods; all teams are able to provide online survey links as necessary. There are no penalties for non-compliance with any part of the FFT guidance to reduce burden and release operational capacity.
What the chart tell us: The Trust FFT is at 88%; Addictions, CAMHS, Specialist and Older Adults reached the target of 90% in July 20.
Actions being taken: The performance is continuously monitored in Directorate P&Q meetings.
Quality Priority: Increase to 90% the number of patients who would recommend the service to friends or family if they needed similar care or treatment
97%88% 93% 91% 90%
81% 86%75%
84%
FFT by Directorates - Jul 20
Target
Fig 80: FFT Scores by DirectorateSource: PowerBI PEDIC Dashboard Special cause concern
Special cause improvement
0%10%20%30%40%50%60%70%80%90%
100%Ju
l-18
Aug-
18Se
p-18
Oct
-18
Nov
-18
Dec
-18
Jan-
19Fe
b-19
Mar
-19
Apr-1
9M
ay-1
9Ju
n-19
Jul-1
9Au
g-19
Sep-
19O
ct-1
9N
ov-1
9D
ec-1
9Ja
n-20
Feb-
20M
ar-2
0Ap
r-20
May
-20
Jun-
20Ju
l-20
Trustwide FFT Scores (% positive)Measure
Page 108 of 131

Identification of carers, friends and familyPa
tient
-Cen
tred
Performance and Quality Indicators
Fig 81: % Patients with identified carers Trust wide as of Jul 20. Source: Trust Dashboard
Fig 82: % Patients with identified carers by Directorate as of Jul 20. Source: Trust Dashboard
Reporting month 4
0%
10%
20%
30%
40%
50%
60%
70%
80%Ap
r-18
May
-18
Jun-
18Ju
l-18
Aug-
18Se
p-18
Oct
-18
Nov
-18
Dec
-18
Jan-
19Fe
b-19
Mar
-19
Apr-1
9M
ay-1
9Ju
n-19
Jul-1
9Au
g-19
Sep-
19O
ct-1
9N
ov-1
9D
ec-1
9Ja
n-20
Feb-
20M
ar-2
0Ap
r-20
May
-20
Jun-
20Ju
l-20
Trustwide % of patients with recorded carer
Target
Measure Background: To enable to tracking of performance, it was agreed to set a target of 75% for the percentage of patients with recorded carers on EPJS.
What the chart tell us: The performance of this indicator has been improving with the Trustwide position at 67.6% in July 20. CAMHS and Lewisham have exceeded the target this month.
Actions being taken: The performance is continuously monitored in Directorate P&Q meetings.
Quality Priority: Increase the proportion of service users underthe care of SLaM services who have at leastone carer, partner, relative or friend identified,with their contact details recorded on the CoreInfo section of EPJs
Target 20/21: 75%
Special cause concernSpecial cause improvement
76.8%
55.6%74.2% 66.7%
80.2%
53.4%67.1%
46.1%
73.9% 72.4%
0.0%10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%90.0%
% of patients with recorded carers by Directorate – Jul 20
Target
Page 109 of 131

Safe
Performance and Quality IndicatorsWorkforce Indicators – All Staff Turnover, Vacancies (Rolling Year %) and Sickness (Monthly)
Fig 83: Trustwide All Staff Turnover (Rolling Year %)Source: Workforce BI Dashboard
Reporting month 4
Fig 84: Trustwide All Staff Vacancy %Source: Workforce BI Dashboard
Fig 85: Trust wide Sickness % Source: Workforce BI Dashboard
Background:Trustwide Workforce Datahas remained stable duringthe Covid-19 period.
What the Charts are TellingUsThe turnover of all staffTrustwide has decreased tobelow the lower control limitin June 2020, at 13.5%.Vacancies for all staff grouphas fallen below lower controllimit to 17.5% in June 2020and the sickness rate isbelow the lower control limitat 2.5% at the end of June2020.
Underlying Issues andActions Being Taken:None Noted
Page 110 of 131

Safe
Performance and Quality IndicatorsWorkforce Indicators – Non Registered/Registered Nurses Vacancy Trend
Reporting month 4
Fig 86: Trust wide Monthly Unregistered Nursing Vacancy Trend Source: Workforce BI Dashboard
Fig 87: Trust wide Monthly Registered Nursing Vacancy Trend Source: Workforce BI Dashboard
Background:Trustwide Workforce Data hasremained stable during theCovid-19 period.
What the Charts are TellingUsThe Registered Nursing andNon Registered NursingVacancies are at 26.2% and15.6% respectively at the end ofJune 2020.
Underlying Issues andActions Being Taken:None Noted
Page 111 of 131
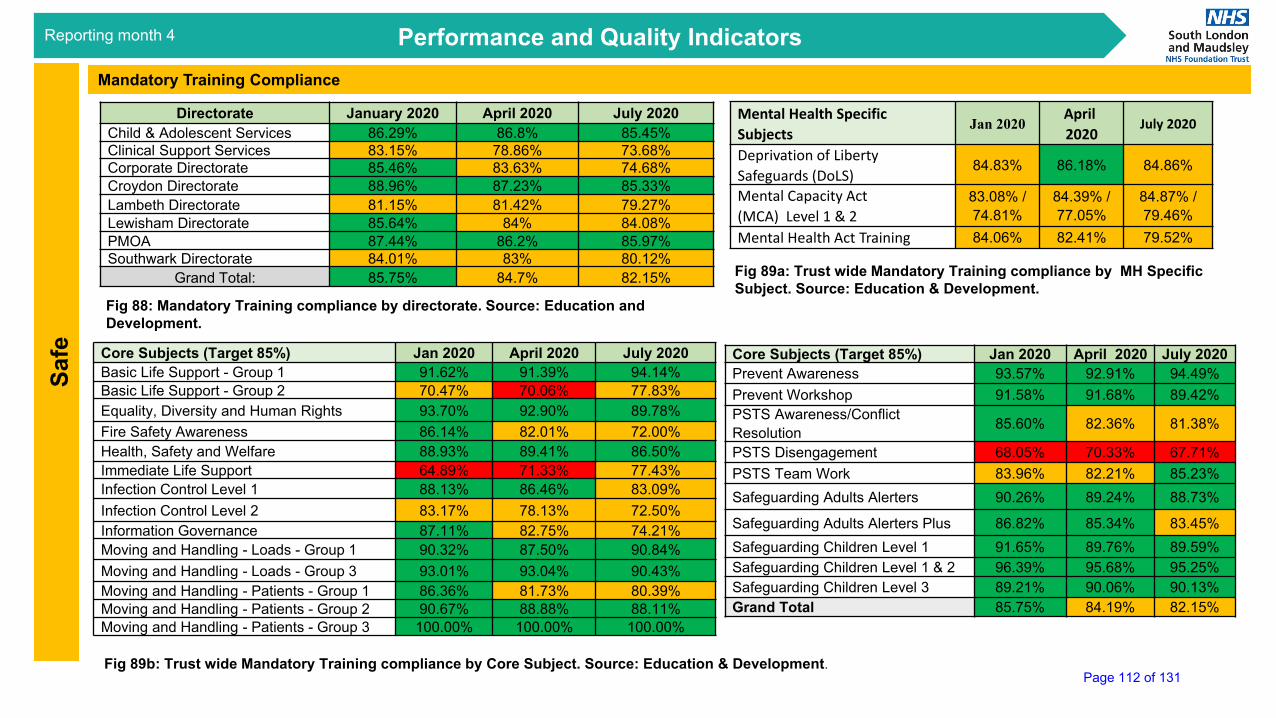
Reporting month: June 2020
Safe
Performance and Quality IndicatorsMandatory Training Compliance
Fig 88: Mandatory Training compliance by directorate. Source: Education and Development.
Fig 89b: Trust wide Mandatory Training compliance by Core Subject. Source: Education & Development.
Directorate January 2020 April 2020 July 2020Child & Adolescent Services 86.29% 86.8% 85.45%Clinical Support Services 83.15% 78.86% 73.68%Corporate Directorate 85.46% 83.63% 74.68%Croydon Directorate 88.96% 87.23% 85.33%Lambeth Directorate 81.15% 81.42% 79.27%Lewisham Directorate 85.64% 84% 84.08%PMOA 87.44% 86.2% 85.97%Southwark Directorate 84.01% 83% 80.12%
Grand Total: 85.75% 84.7% 82.15%
Core Subjects (Target 85%) Jan 2020 April 2020 July 2020Basic Life Support - Group 1 91.62% 91.39% 94.14%Basic Life Support - Group 2 70.47% 70.06% 77.83%Equality, Diversity and Human Rights 93.70% 92.90% 89.78%Fire Safety Awareness 86.14% 82.01% 72.00%Health, Safety and Welfare 88.93% 89.41% 86.50%Immediate Life Support 64.89% 71.33% 77.43%Infection Control Level 1 88.13% 86.46% 83.09%Infection Control Level 2 83.17% 78.13% 72.50%Information Governance 87.11% 82.75% 74.21%Moving and Handling - Loads - Group 1 90.32% 87.50% 90.84%Moving and Handling - Loads - Group 3 93.01% 93.04% 90.43%Moving and Handling - Patients - Group 1 86.36% 81.73% 80.39%Moving and Handling - Patients - Group 2 90.67% 88.88% 88.11%Moving and Handling - Patients - Group 3 100.00% 100.00% 100.00%
Core Subjects (Target 85%) Jan 2020 April 2020 July 2020Prevent Awareness 93.57% 92.91% 94.49%Prevent Workshop 91.58% 91.68% 89.42%PSTS Awareness/Conflict Resolution 85.60% 82.36% 81.38%
PSTS Disengagement 68.05% 70.33% 67.71%PSTS Team Work 83.96% 82.21% 85.23%Safeguarding Adults Alerters 90.26% 89.24% 88.73%
Safeguarding Adults Alerters Plus 86.82% 85.34% 83.45%Safeguarding Children Level 1 91.65% 89.76% 89.59%Safeguarding Children Level 1 & 2 96.39% 95.68% 95.25%Safeguarding Children Level 3 89.21% 90.06% 90.13%Grand Total 85.75% 84.19% 82.15%
Mental Health Specific Subjects
Jan 2020April2020
July 2020
Deprivation of Liberty Safeguards (DoLS)
84.83% 86.18% 84.86%
Mental Capacity Act (MCA) Level 1 & 2
83.08% / 74.81%
84.39% / 77.05%
84.87% / 79.46%
Mental Health Act Training 84.06% 82.41% 79.52%
Fig 89a: Trust wide Mandatory Training compliance by MH Specific Subject. Source: Education & Development.
Reporting month 4
Page 112 of 131
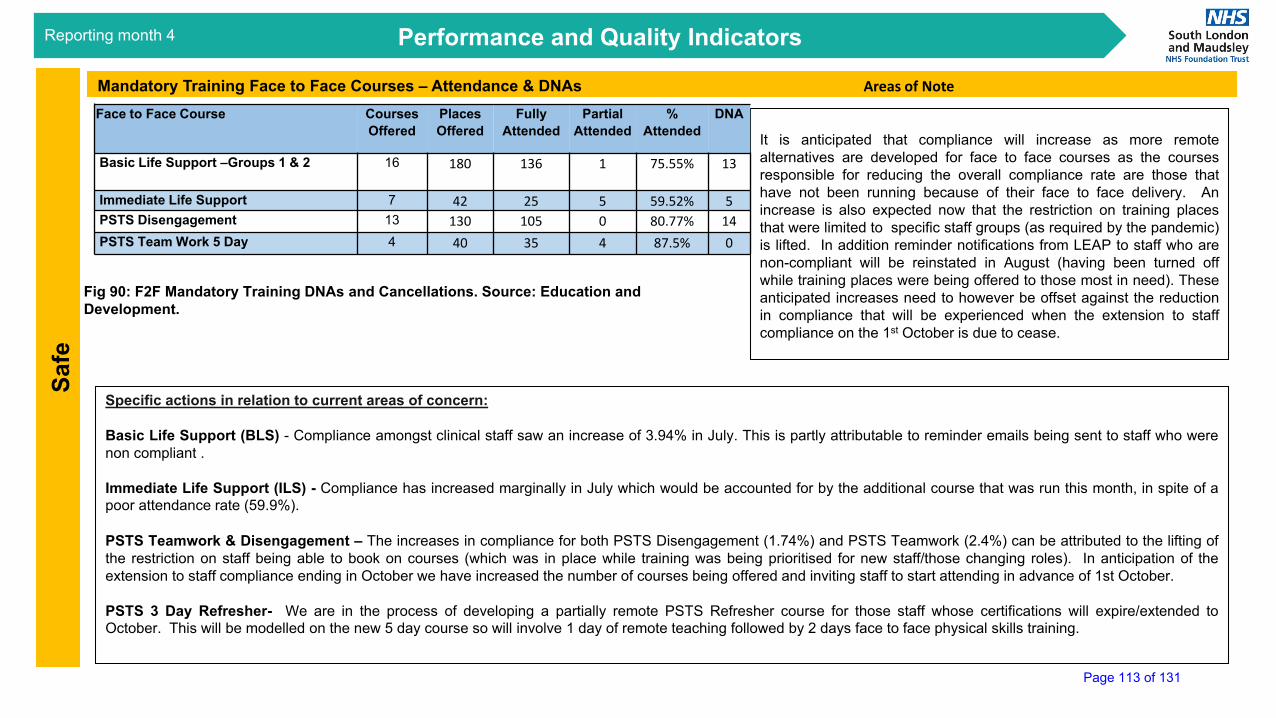
Reporting month 4 Performance and Quality Indicators
Mandatory Training Face to Face Courses – Attendance & DNAs Areas of Note
It is anticipated that compliance will increase as more remotealternatives are developed for face to face courses as the coursesresponsible for reducing the overall compliance rate are those thathave not been running because of their face to face delivery. Anincrease is also expected now that the restriction on training placesthat were limited to specific staff groups (as required by the pandemic)is lifted. In addition reminder notifications from LEAP to staff who arenon-compliant will be reinstated in August (having been turned offwhile training places were being offered to those most in need). Theseanticipated increases need to however be offset against the reductionin compliance that will be experienced when the extension to staffcompliance on the 1st October is due to cease.
Specific actions in relation to current areas of concern:
Basic Life Support (BLS) - Compliance amongst clinical staff saw an increase of 3.94% in July. This is partly attributable to reminder emails being sent to staff who werenon compliant .
Immediate Life Support (ILS) - Compliance has increased marginally in July which would be accounted for by the additional course that was run this month, in spite of apoor attendance rate (59.9%).
PSTS Teamwork & Disengagement – The increases in compliance for both PSTS Disengagement (1.74%) and PSTS Teamwork (2.4%) can be attributed to the lifting ofthe restriction on staff being able to book on courses (which was in place while training was being prioritised for new staff/those changing roles). In anticipation of theextension to staff compliance ending in October we have increased the number of courses being offered and inviting staff to start attending in advance of 1st October.
PSTS 3 Day Refresher- We are in the process of developing a partially remote PSTS Refresher course for those staff whose certifications will expire/extended toOctober. This will be modelled on the new 5 day course so will involve 1 day of remote teaching followed by 2 days face to face physical skills training.
Fig 90: F2F Mandatory Training DNAs and Cancellations. Source: Education and Development.
Face to Face Course Courses Offered
PlacesOffered
Fully Attended
PartialAttended
% Attended
DNA
Basic Life Support –Groups 1 & 2 16 180 136 1 75.55% 13
Immediate Life Support 7 42 25 5 59.52% 5PSTS Disengagement 13 130 105 0 80.77% 14PSTS Team Work 5 Day 4 40 35 4 87.5% 0
Safe
Page 113 of 131

Glossary
Performance and Quality Indicators
Abbreviation Description
AEP Accountable Emergency OfficerAfC Agenda for Change
Ascom Alarm / communications system supplied by Ascom UK, a telecommunications company
ASD / LD Autism Spectrum Disorder / Learning Disability
CAG Clinical Academic Group – bringing together clinical services, research and education and training into a singlemanagement grouping e.g. Psychosis
CAMHS Child and Adolescent Mental Health ServicesCBT Cognitive Behavioural Therapy {CBTp is CBT of psychosis}
CCG Clinical Commissioning Group – an NHS body responsible for the planning and commissioning of health services fortheir local area
CHS Croydon Health Services NHS TrustCIP Cost Improvement ProgrammeCPA Care Programme ApproachCQC Care Quality Commission
CQUIN Commissioning for Quality and Innovation: A fund where payment is contingent on delivery on quality improvementsand meeting milestones agreed with commissioners.
CYP Children & Young PeopleDBT Dialectical Behaviour TherapyDSN Data Security NetworkDTOC Delayed Transfers of CareE&D Education & Development DepartmentEI Early Intervention: First Episode PsychosisePJS Electronic Patient Journey System: Clinical records systemEPM Emergency Planning ManagerEPRR Emergency Preparedness, Resilience and ResponseGSTT Guys & ST Thomas’ NHS Foundation TrustHTT Home Treatment TeamIAPT Improving Access to Psychological Therapies
ICD10 Diagnosis coding: International Classification of Diseases (World Health Organisation). Currently iteration ICD10
JOSC Joint Overview and Scrutiny CommitteeKMAU Kent & Medway Adolescent Unit
LoS Length of Stay. The duration of an inpatient stay, usually measured in days. Can include or exclude leave and canfocus on a stay on a particular ward or the full hospital admission.
LSLC Lambeth, Southwark, Lewisham & Croydon (CCGs)LTC Long Term Condition
MHOAD Mental Health of Older Adults and Dementia
MHSDS Mental Health Services Data Set: National dataset submitted to NHS Digital (formerly known asthe Health & Social Care Information Centre)
NHSE NHS EnglandNHSE(L) NHS England (London)
NHSI NHS Improvement: the new regulatory body overseeing all NHS providers as well asindependent providers that provide NHS funded care
NHSP NHS Professionals
NICE National Institute for Health and Care Excellence: provides national guidance and advice toimprove health and social care
OAP Out of Area Placement
OBD Occupied Bed Day – is a unit of currency used to measure the use made of a bed (e.g. 1 obd =1 bed occupied for 1 day by a patient)
PACMAN Performance and Contract Management (meeting)PICU Psychiatric Intensive Care UnitPMF Performance Management FrameworkPMO Programme Management OfficeQIA Quality Impact Assessment
QIPPQuality, Innovation, Productivity and Prevention programme is a series of schemes required bythe CCGs and developed with SLaM to help enhance services and improve their costeffectiveness
QuESTTQuality, Effectiveness and Safety Trigger Tool. An inpatient self-audit which enables pressuresin inpatient wards to be quantified. In 2018 a simple community equivalent is being developedand introduced at SLaM.
SEL South East London
SLP South London Mental Health and Community Partnership. A partnership of SLaM, Oxleas andSWLStG formed in 2015
SOF Single Oversight Framework: NHSI assurance and performance mechanismSPC Statistical Process ControlSTP Sustainability and Transformation PartnershipSWL South West LondonSWLStG South West London and St George’s Mental Health NHS TrustYTD Year to Date
Reporting month 4
Page 114 of 131

Council of Governors 15 September 2020
Name of Report Report from the Lead Governors
Author
Jenny Cobley, Sue Scarsbrook, Brian Lumsden
Presented by
Jenny Cobley and Sue Scarsbrook
Purpose
For information
New governors Following the resignation of two service user governors, one vacancy has been taken up by Torie Robinson, who we welcome to the Council of Governors. Elections for 10 governors will take place this autumn. Governors kept informed Governors receive a weekly newsletter which contains a brief update on coronavirus testing and whether there have been any new positive diagnoses at SLaM. Governors are also provided a recording of the weekly broadcasts by the CEO and Chair; and sent the E-news and update emails to staff. Governor Observers have continued to attend Committee meetings where possible, and their notes are circulated to fellow Governors. However, due to the coronavirus pandemic, we miss our meetings at the Maudsley Hospital and the opportunity to interact with staff and other governors. We are also missing site visits and other opportunities to visit services and to attend events in the community. Governor/NED accountability session Governors met with the Non Executive Directors (NEDs) on 28 July. We discussed physical health checks for patients prescribed antipsychotics, community services, capital programme risks and equity of service for different groups. We continue to be concerned about community services as we have heard that some service users had no contact with SLaM staff during the Lockdown and some waiting lists are long. The lead and deputy lead governors have a quarterly meeting with the Chair and Director of Corporate affairs. Our next meeting is due on 9 September. Council of Governors meeting, 11 June 2020 This meeting, which was held on Microsoft Teams, considered the end of year financial statements, and presented an introduction to the Reshaping our Services programme. A large amount of time was allocated to questions, with discussion around how the organisation could better serve all communities and work in partnership with other providers. The meeting was well attended with 18 governors present.
Page 115 of 131

Informal governors’ meeting, 25 June Seventeen governors joined this meeting on Teams. We discussed personal experiences during the Covid19 pandemic and impressions of governor engagement with SLaM. Working Groups These all met in July using Teams. Other activities Some governors met with Aaron Gains of Social Minds to discuss the revision of the Trust’s strategy. We have also been invited to give feedback on the performance of the NEDs. The lead governors met (on Teams) with the lead governors from GSTT and KCH on 25 August. We would like to thank Charlotte Hudson and her team for keeping us informed of developments and for supporting governors at this difficult time.
Page 116 of 131
Council of Governors 15 September 2020
Name of Report Working Group reports
Author
Working Group Chairs Carol Stevenson, Membership Officer
Presented by
Working Group Chairs: Gill Sharpe, Angela Flood, Ermias Alemu, Simon Darnley
Purpose
For information
Quality Working Group (QWG) report (Gill Sharpe) The digital meetings held by the QWG have been very well attended, and involvement and discussion have been animated. Among the large number of questions submitted to the NEDs during this period has been the concern of service users who have received inconsistent levels of contact from community mental health services during the lockdown, an experience which has proved very distressing for them. This has been one of the many occasions when directly reported evidence from our Service User Governors has been of great value in the constant vigilance to ensure the high quality of SLaM services, thus underscoring the importance of Service User involvement. Governors received presentations on the Performance & Quality report: a key duty of the Group being to ‘review and comment’ on information updates throughout the year. This report continues to be refined and further sessions explaining the data and how it is presented will be held. We hope that the Governors will be able to make a significant contribution to the discussion. We have been interested to hear about the new Reshaping our Services programme which is taking place and the renewed commitment to improving quality in all areas of SLaM. Governors will be informed of, and involved in, this programme. At the last meeting of the QWG the agenda item on the Service User Involvement Strategy received a warm welcome and provoked much discussion. Tim Dee has been appointed to the working party. We wish him well in the post as he contributes to the consideration of an issue which has long been of interest to SU Governors, and has too often, in the Chair’s experience, been somewhat side-lined. One of the compelling issues of our day – how the Trust can play its part in answering the issues raised by the Black Lives Matter Campaign – has found its focus in QWG meetings as elsewhere in Governors’ discussions. We look forward with interest to see how greater future diversity in SLaM staffing and management brings about – as it usually does – general all-
Page 117 of 131

round improvement. We add our warm congratulations to Mike Franklin on his appointment as Joint Director of Equality and Inclusion at NHS England. Finally, we are seeking offers of interest from present Governors in standing as Chair, or Deputy Chair, of the QWG to replace the present Chair whose term of office reaches its conclusion in November; and Kathryn Grant, whose elevation to the Recovery College we rejoice in, even as we feel her loss. This is a committee which deals with issues of central importance to the running of the Trust: how to identify problems in the Trust’s services; how to encourage improvement; and how to ensure that we are constantly looking ahead to future progress. We hope someone will be prepared and willing to take up this challenging and rewarding position. Date of next meeting: 15 October 2020, 13.30 to 15.30 via Teams. Planning and Strategy Working Group (PSWG) report (Angela Flood) The Planning and Strategy Working Group last met (virtually) on 9 July 2020. This enabled excellent attendance including Governors representing the different constituencies, a recently appointed Non-Executive Director, a NeXT Director and members of the Executive and Senior Management Team. There were two main items for presentation and discussion. Adult and Social Care Strategy/Carla Fourie (CF), Director of Social Care CF gave a comprehensive presentation on the significant challenges facing adult and social care - including those resulting from the Covid-19 pandemic - and actions to address them. Key to this would include: delivering outcomes from the Mental Health Law Quality Improvement Programme; ensuring the integration of social care models across care pathways; developing a Quality Assurance Framework and ensuring that social care is a fully involved partner in strategic population health and in the development of Alliances and other partnerships. Strengthening partnerships and governance arrangements with Local Authorities is essential in ensuring that Care Act duties are embedded and delivered in integrated services and that better collaboration leads to improved discharge pathways. An exercise to map the location of all social workers within the Trust was also being undertaken. Governors were pleased to hear about plans for the development of the social care workforce - a key essential to delivering cohesive and improved services and outcomes for our service users. In collaboration with Trust HR, this will include: developing and agreeing specification of the social work skill set for inclusion in job descriptions; establishing career pathways and the introduction of a SLaM Social Work Forum to ensure that social work is recognised as a core profession within the Trust. It was felt that recent years had seen a dilution of the social care skill set, especially in roles such as Care Co-ordinators, and a balanced approach was required between re-professionalising certain areas and introducing innovation through more community-facing models of practice. CF recognised that there was inconsistency in its application and that both training and developing community partnerships would help to address this. Social and racial inequalities in the delivery of mental health services at community level were a Governor concern. CF acknowledged this and believed that integrating social care improvements within the Patient and Carers’ Race Equality Framework, the work of the Mental
Page 118 of 131
Health Law Committee looking at the disproportionate use of Trust services by Black males and the development of a Workforce Race Equality Framework for social care would help to address these ongoing challenges. Lambeth Hospital proposals/Lucy Canning (LC), Associate Director of Strategy and Commercial; Matthew Longmate (ML), Programme Director for the Lambeth Hospital changes ML provided a recap on the process resulting in the preferred option – moving the Lambeth Hospital acute wards to a new build facility on the Maudsley Hospital site. A consultation process led by SEL CCG in conjunction with SLaM sought to gather feedback from the local community including community representatives, voluntary organisations, hard-to-reach groups, service users and carers. A majority recognised the need for change and supported the proposal to move the wards to a new build facility. Recommendations included the need to engage with Black communities to develop a culturally appropriate inpatient care model – SLaM will be working with Black Thrive on this. Due to the impact of Covid-19, it was decided to extend the consultation process using a range of communication methods including Facebook, the local press and networks. Governors asked if engagement had taken place with LGBT+ representative groups. In response, LC said the intention to do so was outlined in the Equality Impact Assessment but she would check that this had taken place. In terms of governance and decision making, the preferred option had received support from the Lambeth and Southwark Joint Health Overview and Scrutiny Committee, the Living Well Network Alliance Leadership Team and the Lambeth Together Strategic Board. A Decision Making Business Case would be presented to the SEL CCG Governing Body for a formal decision on whether to proceed to the implementation stage. Any decision will need to be recognised by the SLaM Board (July), with a Full Business Case submitted to it (September). Should the proposal be accepted, Governors asked about any plans for the future use of the Lambeth site, for example, affordable housing. They were advised that, in this eventuality, a detailed and robust planning consultation on the future of the site would be held with a range of stakeholders. Governors wish to be updated on the Lambeth Hospital developments and, accordingly, this item will be added to the PSWG forward workplan. Date of next meeting: 27 October 2020, 17:00 to 18:30 via Microsoft Teams and via telephone (TBC). Membership and Involvement working Group (MIWG) report (Ermias Alemu) The Governors’ Membership and Involvement Working Group received reports on SLaM’s Mental Health Prevention agenda and the Patient & Carers Race Equality Framework (PCREF). The presentation on SLaM’s Mental Health Prevention initiative was made by Ranjeet Kaile, Interim director of Communication and covered the following points: • The origins of the urgent mental health summit and the establishment of the Prevention
Working Group; its underpinning workstreams to take the prevention programme forward and how these are progressing.
Page 119 of 131
• The tremendous range of prominent external stakeholders who have been engaged (including the input of the CEO and Chair) to support both the delivery of the summit and the wider work of the 12-month prevention programme. Including with the four borough authorities and within the ICS.
• The six specific actions that were identified at the summit to facilitate mental health prevention and how these will be progressed.
• Focus on initiatives such as the establishment of a taskforce of representatives across SLaM and key partner stakeholders and the schedule of monthly public broadcast events concentrating on key themes emerging from the summit.
• The potential for authentic, appropriate Governor involvement and support for current and emerging initiatives.
The presentation on Patient & Carers Race Equality Framework (PCREF) initiative was given by Zoe Reed, Director of Organisation and communities. With regards future involvement of the following plan has been outlined: • The Governors will be invited to nominate a Governor from the Public constituency to join
the Programme Board – called the PCREF Partnership Group and could feed views through their representative
• The Trust’s Service User structures will similarly be invited to nominate a Service User to join the PCREF Partnership Group
• The Trust’s Carer structures will similarly be invited to nominate a Carer to join the PCREF Partnership Group.
• Ideally both Carer and Service User representatives should be identified from the Black community.
Date of next meeting: 3 November 2020, 16:00 to 17:30 via Microsoft Teams Bids Steering Group (BSG) report (Simon Darnley and Carol Stevenson) The Bids Steering Group met via Teams on 2 July and we were pleased to be joined by Alice Casey, Director of Programmes at Maudsley Charity. She replaces David Blazey, who had been involved with the Smile Bids Schemes since their inception. There are two Bids Schemes currently running. Time to Smile started in 2019 and the bid projects are currently running. Covid-19 has hit the scheme hard as many of the projects were for groups and outings so we are working with the bidders to agree changes to their bids to make them suitable for the changed circumstances. We have also gained the agreement of Maudsley Charity to extend the finish date to the end of March 2021. Smile with Us was launched on 27 July 2020 (though sadly we were not able to hold a Launch Event) and is open for bids. The application process has been moved on-line (using Microsoft Forms) which makes the process easier to manage with the administrator working from home. At the beginning of September we had received 6 completed application forms, compared to
Page 120 of 131

ten at the equivalent date last year. So far nobody has reported that they are unable to use Microsoft Forms. We will be assessing the Smile with Us bids in late January / early February 2021 and all governors are invited to join us. Even without Gabrielle’s famous courgette cake it will be an enjoyable day. Date of next meeting: 22 October 2020, 15.30 to 16.30 via Microsoft Teams.
Page 121 of 131

Audit Committee report (Sep 2020): appointment of external auditor Page 1 of 7
Council of Governors Tuesday 15 September 2020
Name of Report Audit Committee report: appointment of external auditor Author Steven Thomas (Audit Committee Secretary) Presented by Duncan Hames (Audit Committee Chair) Purpose
The Council of Governors (‘the Council’) is asked: • to consider this report and its recommendation about the
appointment of the Trust’s external audit provider; and • taking account of that recommendation to make a decision as to
appointment of the Trust’s external audit provider Background The Audit Committee (‘the Committee’) is required under its terms of reference to make recommendations to the Council as to the appointment, reappointment, termination of appointment and fees of the external auditor. This is met through the content of this paper.
Recommendation The Audit Committee recommends to the Council of Governors that the current external audit provider’s (Grant Thornton’s) contract be extended to cover the 2020/21 audit, and that in June 2021 the Audit Committee considers whether to recommend a similar extension for the 2021/22 audit.
Background and current position 1. The Trust’s current external audit provider is Grant Thornton UK LLP. They were appointed as a result of a collaborative procurement exercise with Oxleas NHS Foundation Trust (‘Oxleas’) from the London Procurement Partnership (‘LPP’) framework. Bids were received from three firms: Deloitte & Touche LLP; Grant Thornton UK LLP; and Mazars LLP (alphabetical order). The bid review panel included representatives from the governing bodies and senior management teams of both the Trust and Oxleas, the Trust Audit Committee Chair, the Trust Chief Financial Officer and the Trust’s procurement team. 2. The signed letter of engagement with Grant Thornton states that, as approved by the Council of Governors at its meeting on 29 September 2017, Grant Thornton’s appointment as the Trust’s external auditor is ‘for the [audit of accounts for the] three financial years from 2017/18 [that is, 2017/18. 2018/19 and 2019/20] with the option to extend for a further two years’ – that is, to extend for 2020/21 and 2021/22. 3. Therefore the Trust now needs to take action to appoint/reappoint external auditors at least for 2020/21. 4. The Audit Committee’s terms of reference require it to make recommendations to the Council of Governors as to the appointment, reappointment, termination of appointment and fees of the external auditor. However it is the Council of Governors that makes the final decision on this, taking account of the recommendation from the Audit Committee. There are provisions covering what to do if the Council of Governors were to disagree with the Audit Committee’s recommendation.
Page 122 of 131

Audit Committee report (Sep 2020): appointment of external auditor Page 2 of 7
5. External audit fees for 2019/20 were as noted in the table below. Item 2019/20 external audit
fee £
Original Contract Fee (excluding VAT) 68,650 Raising the Bar 2,500 PPE Valuations – Work of Experts 2,000 Impact of Covid-19 on Audit Procedures 7,600 Work on Maudsley Commercial 4,000
Total: revised fee for 2019-20 (excluding VAT) £84,750 Source: External Audit Findings Report dated 16 June 2020 (considered by the Audit Committee at its June 2020 meeting) Assessment process in outline 6. In addition to the formal process outlined below, note that the Audit Committee has already informally assessed the external auditor’s performance annually for 2017/18, 2018/19 and 2019/20. These informal assessments took account of the reports received from external audit, and other parties, considered at each Committee meeting. Based on this, the Committee has been satisfied with the performance of the Trust’s external auditors, the quality and value of their work, the timeliness of their reporting and the external audit fee. 7. The Director of Corporate Affairs agreed with the Lead Governors and Deputy Lead Governor the process for this year’s re-appointment: • a timely Audit Committee to be held, Grant Thornton not attending, to review their
performance, consider the market, current restrictions (such as the Covid-19 pandemic), pricing, and other risks or benefits. The Governor Observer should attend this meeting; and
• the Audit Committee’s recommendations to be put to the Council of Governors at the Council’s meeting on 15 September 2020.
8. Accordingly the Audit Committee held a meeting on 26 August 2020, attended also by the Chief Financial Officer, Deputy Director of Corporate Affairs, a representative from the Council of Governors and the Audit Committee Secretary. The meeting was quorate. The views of another NED Committee member, who could not be present, were taken into account by the Committee Chair. At the meeting, the Audit Committee, taking into account views from Trust senior Finance management: • considered a paper analogous to this report to the Council of Governors, setting out the
relevant background. Appendix 1 to this report is an extract from the minutes of the Audit Committee’s meeting, summarising factors discussed and considered;
• formally assessed the performance of Grant Thornton. Audit Committee members had regard to a checklist of relevant factors for consideration (reproduced in Appendix 2 to this report);
• considered feedback already received from the Lead Governors and Deputy Lead Governor during their discussions with the Director of Corporate Affairs;
• considered comments from the Trust’s Head of Internal Audit and Internal Audit Manager; and
• based on these considerations, formulated the recommendation above for the Council of Governors as to appointment of external auditors.
Page 123 of 131
Audit Committee report (Sep 2020): appointment of external auditor Page 3 of 7
APPENDIX 1: EXTRACT FROM AUDIT COMMITTEE MINUTES – 26 AUGUST 2020 Noted below is an extract from the detailed minutes of the Audit Committee’s meeting on 26 August 2020 (paragraph numbers amended for consistency). 1. The Committee Chair opened discussions, noting that the agenda paper includes a detailed and comprehensive checklist of factors relevant when assessing external auditors, and attendees confirmed they had taken this into consideration [Appendix 2 to this report refers]. 2. Committee members considered the paper was very helpful. It was noted that in Australia external auditors cannot serve for more than three consecutive years. The Committee queried the position in the UK, and: • the Chief Financial Officer (‘CFO’) responded that there is no such requirement in NHS
regulation. This allows for judgment calls to be made about longer periods of service, balancing the threats to external audit objectivity and independence against the benefits of increased efficiency and effectiveness; and
• the CFO advised he had no concerns about the current external auditors (Grant Thornton) as regards objectivity, independence or otherwise. They had been appointed from the LPP’s framework list (that is, a list of external auditors pre-vetted by the London Procurement Partnership) and in their three years’ service to the Trust they have adopted a rigorous, challenging approach and have coped well with logistical and other issues arising from the Covid-19 pandemic.
3. The Audit Committee Secretary advised that he had contacted the Trust’s Head of Internal Audit and Internal Audit Manager requesting any comments from them about the external auditors, Grant Thornton. The Audit Committee Secretary advised that they had no specific comments. The Head of Internal Audit had advised his view that generally, if there are no issues with the service, it would be sensible to re-appoint from a continuity perspective particularly given the current levels of uncertainty in the system. 4. Further to the Committee Chair’s query, the CFO advised that Oxleas NHS Foundation Trust (‘Oxleas’) had appointed Grant Thornton in 2017/18 in line with the procurement, and the CFO’s understanding was that Oxleas’ management and their Audit Committee were satisfied with Grant Thornton’s performance. The CFO advised that discussions with other Directors of Finance around the NHS (including Oxleas) had identified no significant issues as to the service provided by Grant Thornton, who act as external auditors for a number of local NHS Trusts. The CFO advised that other firms of external auditors had received adverse comments in such discussions, for instance as regards handling of issues due to the Covid-19 pandemic. 5. The CFO advised his own experience and views of the Trust’s external auditors, Grant Thornton: • the CFO is pleased with Grant Thornton’s approach and professionalism. They are open
and transparent in their communication. In particular the working relationship with the external audit partner and manager is very good. They are helpful, facilitative and challenging;
• external audit has provided good advice on various issues, and has provided a robust challenge where appropriate;
• the CFO had some questions about additional fees charged by external audit for 2019/20, but these were not significant and overall the fees are acceptable;
• likewise there have been some understandable temporary difficulties in working arrangements between external audit and the Finance team arising from the requirements of audit during the lockdown when staff were working remotely, but nothing significant; and
Page 124 of 131

Audit Committee report (Sep 2020): appointment of external auditor Page 4 of 7
• the CFO has no concerns about independence, objectivity and robust challenge, and is confident that external audit would raise any concerns directly with the Committee Chair where that need was indicated.
6. The Governor Observer gave his views based on his experience as a Governor and as an observer at Quality Committee meetings, and: • advised that he was very impressed with how the external audit partner engaged with him
and other Governors and responded to their questions, and how the external audit partner engaged with the Quality Committee; and
• flagged that the Governors are interested in the Trust’s policies and practice around Diversity and Inclusion, and would be interested to know how external audit relates to this.
7. The Committee Chair concluded as follows: • audit firms have been withdrawing from NHS audits in recent years, giving a reducing field
from which to select. For example, only one of the ‘Big Four’ firms participated in the most recent tender exercise;
• comments shared in this discussion about the current external auditors, Grant Thornton, have been favourable, with no significant concerns raised; and
• the Committee Chair proposed that the Committee recommends to the Council that Grant Thornton’s contract be extended to cover the 2020/21 audit, and that in June 2021 the Committee considers whether to recommend a similar extension for the 2021/22 audit.
8. After due discussion the Committee noted the agenda item, agreed with the Committee Chair’s proposal and authorised the Committee Chair on its behalf to approve the report to the Council on this matter.
Page 125 of 131

Audit Committee report (Sep 2020): appointment of external auditor Page 5 of 7
APPENDIX 2: EXTERNAL AUDIT ASSESSMENT CHECKLIST This appendix formed the appendix to the paper considered by the Audit Committee at its meeting on 26 August 2020 The following is an extract from ‘NHS Briefing: Selection and assessment of external auditors’ (Deloitte, April 2016) selected because it is detailed and comprehensive. For the purposes of assessing the Trust’s current external auditor for re-appointment, it is suggested that the 10 main factors below are considered, and the supporting detailed ‘bullet points’ are used simply as indications of the type of factors to consider when assessing against the 10 main headings. 1. The audit engagement lead • Does the audit engagement lead demonstrate a strong understanding of your organisation, your values and
culture, as well as the wider NHS sector in which you operate and the challenges you face? • Is the audit engagement lead demonstrably committed to audit quality? Does he/she have a robust and
professional working relationship with management, and demonstrate strong technical knowledge and professional scepticism in the challenge of our key judgements?
• Does the audit engagement lead inspire confidence, and do you value their opinion, not just because you need their signature?
• Is the audit engagement lead a strong leader, able to marshal audit professionals and, where required, specialists and ensure that quality is maintained to and beyond your expectations?
2. The audit team • Do the audit engagement lead, managers and professional staff demonstrate a strong understanding of your
organisation, and the wider NHS environment in which you operate and the challenges you face? • Does the audit team have sufficient experience, technical and industry knowledge and are they appropriately
directed and supervised by the audit engagement lead and managers? • Does the audit team appear to be well resourced in terms of team structure and time available? 3. The audit approach – planning, scope and risk identification • Do the engagement lead and managers actively and visibly lead the audit planning process? • Has the planning process involved early discussion with management and the audit committee to identify
significant issues at the earliest opportunity and to develop an appropriate audit response? • Has the planning process involved assessment of accounting policies, feedback on prior year disclosure
deficiencies or misstatements and relevant accounting/governance developments? • Does the audit approach provide a framework and procedures to obtain sufficient appropriate audit evidence
effectively and efficiently? • Does the audit approach reflect a clear understanding of your organisation, and the NHS sector and the
significant risks, with appropriate focus on the right financial reporting, value for money, and quality accounts (if applicable) risks?
• Have the auditors demonstrated a good understanding of your internal control systems? • Have the level of quantitative materiality adopted for the audit (including error reporting thresholds and,
where relevant, component/subsidiary materiality) and qualitative materiality considerations been explained satisfactorily?
4. The audit approach – execution • Have all requests or queries raised with the auditors, at any level, been dealt with promptly and effectively? • Do audit quality control procedures appear effective, understood and applied? • Are key accounting judgements, including significant estimates, identified and addressed in advance where
possible? Have they received appropriate resource, including any necessary specialist involvement and were they challenged robustly, demonstrating professional scepticism?
• Have key judgements around the quality accounts (if applicable) been identified and addressed in advance where possible? Have they received appropriate resource, including any necessary specialist
• involvement and were they challenged robustly, demonstrating professional scepticism? • Do audit team professionals exhibit scepticism in their work and are they robust in dealing with issues
identified during the audit?
Page 126 of 131

Audit Committee report (Sep 2020): appointment of external auditor Page 6 of 7
• Were discussions between the auditors and management on fraud risk, prevention and detection led at the appropriate level and were they challenging and comprehensive during the planning, execution and concluding of the audit process?
5. The role of management in an effective audit process • Is the information provided by management for the audit timely, clear, complete and presented with a culture
of “right first time”? • Are management papers presented to the auditors and the audit committee analysing key judgements of
good quality and depth and make use of independent experts/advisers and independent data where this would enhance quality and reliability and are they balanced in presenting alternative treatments in reaching conclusions?
• Do the accounting systems produce reliable information and audit trail, with particular emphasis on control over material judgements, adjustments and journal entries?
• Do the systems used to monitor quality performance produce reliable information and audit trail, with particular emphasis on control over adjustments made to records?
• Does management maintain up-to-date process and controls documentation, particularly over financial reporting and quality performance, and is the documentation subject to regular review?
• Is the audit committee kept informed about development of the control environment by management (and by internal audit)?
• Is the management team involved in the audit and Quality Accounts assurance process well organised, efficient and committed to the value of independent audit and the development of professional relationships with the auditors?
• Does management examine proposed audit adjustments seriously and do they prefer to book audit adjustments?
6. Communications by the auditor to the audit committee • Are communications with the audit committee appropriately positioned in the annual reporting cycle? • Are significant audit and accounting issues, including adverse unexpected findings, raised on a timely basis
with the audit committee? • Are significant issues in relation to the quality accounts (where applicable), including adverse or unexpected
findings, raised on a timely basis with the audit committee? • Are any significant matters outstanding at the time of the final audit committee meeting to discuss the annual
report, quality accounts and financial statements followed up, resolved and reported to the audit committee in a supplementary final written report on or before approval of the financial statements?
• Does the audit committee approve the auditor’s requests for reasonable audit fees, which take account of developments in the business and changes in regulatory requirements?
7. Supporting the work of the audit committee • Does the audit engagement lead promote excellence in governance and financial reporting and endeavour to
guide the audit committee as to best practice including in relation to the audit committee Report in the annual report?
• Does the audit engagement lead provide support to the audit committee between meetings, in the form of briefings and updates on governance developments to the extent the audit committee requires?
• Does the audit committee welcome the candour of the audit engagement lead’s observations in private sessions with them?
8. Insights and adding value • Have the audit process and the audit team challenged your thinking and contributed to improved standards
at your organisation? • Has the audit firm contributed to improvements in the financial reporting at your organisation? • Has the audit firm contributed to improvements in the quality accounts (where applicable) at your
organisation? • Has the audit firm contributed to improvements in governance, including quality governance, at your
organisation? 9. Independence, objectivity and the firm • Is it clear from the communications (both written and oral) received from the auditors that the objectives of
the FRC’s Ethical Standards regarding independence and objectivity have been achieved? • Is the relationship between the auditors and management appropriate such that there is no perception that
the auditors may lack, or appear to lack, the required degree of objectivity?
Page 127 of 131

Audit Committee report (Sep 2020): appointment of external auditor Page 7 of 7
• Has your policy on non-audit services been complied with and, for non-audit related services, were threats and safeguards communicated to you? Are any matters of contention arising in relation to the provision of non-audit services discussed and resolved at the earliest opportunity?
10. Formal reporting by the auditors • Does the report to the audit committee contain those matters that in your view had the greatest effect on the
overall audit strategy, the allocation of resources in the audit and directing the efforts of the • audit team? • Do you consider the reports presented to management and the audit committee to be of an appropriate
length and quality? • Has the audit engagement lead given an informed view in the audit committee on whether the annual report
is fair, balanced and understandable? • Where applicable, does the report to the audit committee on the quality accounts (where applicable) present
clearly the findings and recommendations arising from the work performed?
Page 128 of 131

Council of Governors
15 September 2020 Name of Report NED/Governor meeting minutes, 28 July 2020
Author
Ian Rothwell, Interim Deputy Director of Corporate Affairs
Presented by
Sir Norman Lamb, Trust Chair
Purpose
To note
Present (Governors) Jenny Cobley (Joint Lead Governor) Ermias Alemu Abraham Blay Janet Campbell Rhoda Dakar Bert Johnson Michael Kopelman Brian Lumsden Present (Non-Executive Directors) Norman Lamb (Chair) Béatrice Butsana-Sita Helen Edwards Mike Franklin June Mulroy Geraldine Strathdee Anna Walker Renuka Jeyarajah-Dent, NExT Director Present (in attendance) Ian Rothwell, Deputy Director of Corporate Affairs (Interim) 1. Physical health checks for patients
Are NEDs assured that patients, particularly those prescribed antipsychotics, are having appropriate physical health checks? Do you know if this has been audited and if not, should it be? Anna Walker reported the physical healthcare team are currently reviewing data to ensure that all those who are actively prescribed antipsychotic medication have physical health screening captured in records. An audit had been carried out, which had raised some issues about the accuracy of recording physical health checks and action is being taken. Data is being presented on a monthly basis for services to review. The intention is to move to capturing physical health screening for all active patients at the Trust.
Page 129 of 131
Geraldine Strathdee confirmed that NEDs were not fully assured in regard to the question, but processes were in place to improve assurance. The Mind and Body programme, hosted by King’s Health Partners, was also assisting with the physical health needs of mental health service users. This programme was presented to Governors at the joint meeting with Governors from across King’s Health Partners in May 2019. Oxleas are developing an internal GP service. This is of interest to the Board, and progress would be reported. Helen Edwards affirmed that the Trust has a responsibility to patients being treated with anti-psychotics, not least because the medications lead directly to excess weight gain. It is a side-effect of the treatment provided, so should be managed as part of the treatment. Michael Kopelman highlighted that all doctors should be able to provide a basic physical health check. Outpatient areas should have couches to provide the appropriate environment for carrying out checks. 2. Community provision Are the NEDs assured that all community services have adequate facilities or plans for such facilities, and that the services being provided are of sufficient quality with appropriately frequent follow-up of service users? Béatrice Butsana-Sita was acutely aware that not all the Trust estate is not fit for purpose – the situation is true both for the community and inpatient estate. Previous plans need updating both for Alliance based delivery and for the ‘new normal’ post Covid. The Trust would be setting out to do this now that Neil Jackson, the new Director of Capital Estates and Facilities, had been appointed. Improving the existing estate does face capital constraints. Helen Edwards felt that there was in increased focus on the community provision, including estate. If the Trust provides effective and proactive community services it could address other problems in the system. The Reshaping our Services programme included an emphasis on community, and developing work with partners through One Croydon and the Lambeth Living Well Alliance. Norman Lamb added that some of the work currently occurring was to set a vision for the organisation. There is concern among the Board regarding the levels of sectioning, and whether this could be reduced by earlier treatment in the community. The ratio of staff distributed between inpatient and community services also needed a thorough review. The Trust is also working collaboratively with partners to develop a public mental health response to Covid-19 and associated factors. The next Quality Committee agenda would contain an update on the estates programmes and a discussion regarding community indicators. 3. Capital programme risks Does the current economic situation put capital programmes at risk and how are NEDs assured that risks are being appropriately managed. Béatrice Butsana-Sita detailed the current assurance and reporting mechanisms: the overall programme is overseen by the Capital Review Group which reports to the Executive Leadership Team; any specific material risks have then been raised through the Business Development and Investment Committee (BDIC) and the Finance and Performance
Page 130 of 131

Committee. Douglas Bennett House and the Centre for Children and Young People are standing items at every BDIC. The current funding of the schemes depends on a significant contribution from sale of surplus space. Advisers have indicated that there could be a reduction in value compared with the value prior to the pandemic if sites were disposed of in the current environment. A particular difficulty throughout this process is that each Integrated Care System (ICS) has been allocated a capital spend ‘envelope’ or limit. The South East London ICS contains King’s College Hospital and Guy’s and St Thomas’: both large acute trusts with significant capital plans of their own. 4. Equity of service for different groups How are NEDs assuring themselves regarding equity and quality of service provision for service users of all ages, ethnicities and cultures? Norman Lamb reported that work had commenced to improve ethnicity data; this vital work would allow the Trust to more accurately measure service user’s experiences and treatment by various protected characteristics. Ethnicity data is being simplified to aid in the recording – the 42 ethnicity categories being reduced to 16. Mike Franklin reported that ethnicity data is regularly discussed at the Equalities and Workforce Committee. The emphasis had been in improving staff experiences at work, but there was now an increasing focus on the experiences of services users. There were gaps in assurance due to the incomplete data. Progress on the three-year Integrated Equalities Action Plan is being reported at the Board this month. Geraldine Strathdee added that ethnicity was just one element of the dataset that needed to be recorded to assess service user experience. Others, such as language; age; employment status would also be beneficial.
Page 131 of 131