msadlier current myths in relation to tobacco and mental ... · • clancy n., zwarn., richmond r....
TRANSCRIPT

Changing attitudes and Culture in relation to
Smoking-Implementing a Tobacco Free
Campus in Mental Health and Social Care
Settings.
Dr. Matthew Sadlier MB; MSc; MRCPI; MICGP; MRCPsych.
Consultant General Adult Psychiatrist
West Blanchardstown Mental Health Service

Mortality and Mental Health
Mental Health Without Mental
Health
P-values
Death during study 463 (26.8%) 15,972 (20.2%) <0.001
Age at death 66.2 74.4 <0.001
Life years lost 11.3 5.9 <0.001
“Un-natural cause 25 (5.4%) 714 (4.7%) 0.5“Un-natural cause
of death”
25 (5.4%) 714 (4.7%) 0.5
Three Factors were identified to explain excess mortality.
• Low Socioeconomic Status
• Adverse Health Behaviours
• Poor Quality of medical care received.
Excess mortality is a result of “medical illness” not Suicide/Traumatic Deaths.
• Druss et al (2011)

Smoking and Mental Health
Smoking is significantly more prevalent in people with Mental Illness.
•21% of General UK population are smokers (Health and Social Care Information Centre 2010)
•40% of those with common mental disorder were identified as smokers (Farrell 2001).
– 64% of those with probable psychosis (Coultard et al 2000)– 64% of those with probable psychosis (Coultard et al 2000)
– Clear relationship between amount of tobacco and numbers of symptoms (Coultard et al 2000)
– 57% of parasuicides within 12 months were smokers.
•Rate of smoking in Australia among those with mental illness is 32% twice the national average (Australian Bureau of Statistics 2006)
•In mental health admission settings 70% of patients smoke with 50% identified as heavy smokers (Jochelson et al).

Smoking and Mental Health
• Estimated in US 44%; 42% in Australia & 42% in England of all tobacco is used by those with a “mental disorder”.
• In US 200,000 of 440,000 annual deaths from tobacco is in people with mental illness (Williams 2004).is in people with mental illness (Williams 2004).
• The decline in smoking seen in the general population between 2004 & 2011 was significantly less then that seen in mental health patients (Le Cook et al 2014).
• Shows that tobacco control policies for the general population were not as effective in mental health populations (Le Cook et al 2014).

Smoking as a Substance Dependency
• ICD-10 Substances Denpendence:
F10. – Mental and behavioural disorders due to use of alcohol
F11. – Mental and behavioural disorders due to use of opioids
F12. – Mental and behavioural disorders due to use of cannabinoids
F13. – Mental and behavioural disorders due to use of sedative hypnoticsF13. – Mental and behavioural disorders due to use of sedative hypnotics
F14. – Mental and behavioural disorders due to use of cocaine
F15. – Mental and behavioural disorders due to use of other stimulants, including caffeine
F16. – Mental and behavioural disorders due to use of hallucinogens
F17. – Mental and behavioural disorders due to use of tobacco
F18. – Mental and behavioural disorders due to use of volatile Solvents
Smoking as a Substance Dependency
• ICD-10: Substance Dependence Syndrome:
• Any Three or more of the following have been experienced together at any time in the past year.
1. A strong desire or sense of compulsion to take the substance;
2. Difficulties in controlling substance-taking behaviour in terms of its onset, termination, or levels of use;
3. A physiological withdrawal state when substance use has ceased or have been reduced, as evidenced by: the characteristic withdrawal syndrome for the reduced, as evidenced by: the characteristic withdrawal syndrome for the substance; or use of the same (or closely related) substance with the intention of relieving or avoiding withdrawal symptoms;
4. Evidence of tolerance, such that increased doses of the psychoactive substance are required in order to achieve effects originally produced by lower doses (clear examples of this are found in alcohol- and opiate-dependent individuals who may take daily doses sufficient to incapacitate or kill nontolerant users);
5. Progressive neglect of alternative pleasures or interests because of psychoactive substance use.
6. Persisting with substance use despite clear evidence of overtly harmful consequences.
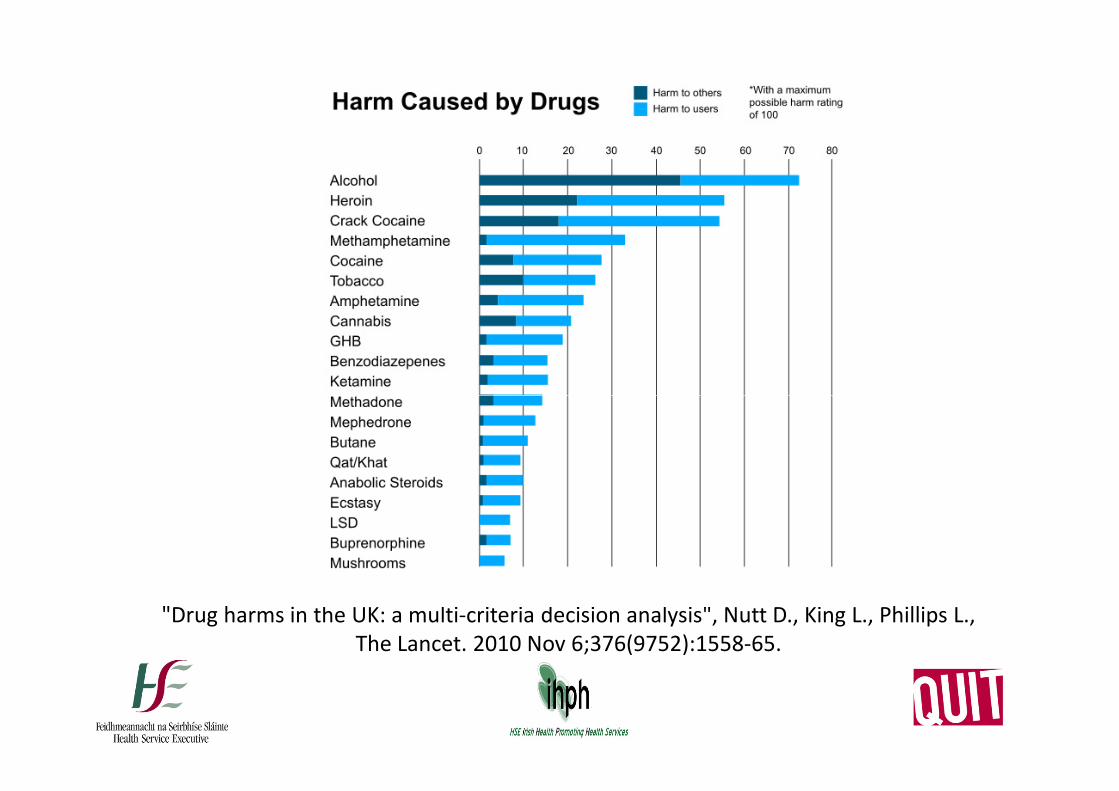
"Drug harms in the UK: a multi-criteria decision analysis", Nutt D., King L., Phillips L.,
The Lancet. 2010 Nov 6;376(9752):1558-65.

Myths about Smoking.
• Smoking can improve your Mental Health.– Belief among regular smokers that smoking can be useful to alleviate
stress symptoms (McEwen et al 2008).
– Smoking was seen as something enjoyable and stress relieving (FidlerJ., West 2009).
• Probable that smoking in fact relieves psychological disturbances that were produced by smoking itself (Taylor et al 2014)that were produced by smoking itself (Taylor et al 2014)– Anger, anxiety, dysphoria , difficulty concentrating, impatience,
insomnia & restlessness are all valid withdrawal symptoms from nicotine (Hughes J 2006).
– Constipation, cough, dizziness, increased dreaming, and mouth ulcers have less evidence supporting but may be abstinence effects (Hughes J 2006).
• Theory that cigarettes don’t improve psychological symptoms but rather treat withdrawal effects induced by Nicotine.
Depression, smoking and smoking cessation:
a qualitative study (Clancy et al 2014)
• Among patients attending a general practice:– Low mood, anxiety and stress were frequently reported as
triggers for smoking.
– Smoking gave them a sense of control over part of their life.
– Strong association between “being bored and smoking”– Strong association between “being bored and smoking”
– Participants were ambivalent about how smoking helped their ongoing symptoms some suggesting it helped and others that it didn’t.
– Some described smoking a form of self harm.
– Strong feeling of hopeless about quitting “I’ve tried before and it didn’t work”.
– Need for psychological support to aid cessation attempts.

Myths about Smoking and Mental
Health
• Smokers suffering mental health problems don’t want to and can’t quit.– Smokers within mental health populations are just as
interested in quitting as those in general population (Siru 2009)
– 47% of psychiatric in-patients in Australia made an – 47% of psychiatric in-patients in Australia made an attempt to quit in previous 12 months (Stockings et al 2013)
– NICE Guidelines:• Evidence based smoking cessation interventions are
effective for smokers with mental disorder.
• Smokers with Mental Disorder require additional monitoring for medication dosage adjustment when ceasing smoking.
Mental Health Implications of Quitting
Smoking
– Quitting smoking was associated with.
• Significant decrease in anxiety, mixed anxiety and
depression, depression symptoms, decrease in stress &
Increase in Psychological quality of life.
• Strength of association is similar for the general and clinical • Strength of association is similar for the general and clinical
populations.
• Meta-analysis of the effect size for SSRI antidepressants in
mild to severe depression is less than that seen for stopping
smoking.
• “This should reassure doctors treating patients with mental
illness that cessation is unlikely to have negative effects”
(Taylor et al 2014)
Smoking Cessation in Mental Health
Settings.
• General Principles in Treating Smoking Cessation in Mental Health:– Similar in principal to smoking cessation in other
populations (Hall et al 2006)
– Has been noted that patient’s within mental health service may need more support especially one-to-one
– Has been noted that patient’s within mental health service may need more support especially one-to-one support (Clancy et al 2013)
– Need to be aware of effects of quitting smoking on medication and adjust dosages if necessary.
– Smoking cessation in mental health services needs a multipronged approach across a continuum of care (Lawn et al 2013)

Smoking Cessation in Mental Health
Settings.• Efficacy of Initiating Tobacco Dependence Treatment in
Inpatient Psychiatry: A Randomized Controlled Trial
Prochaska J, Hall SE, Delucchi K, Hall SM
• American Journal of Public Health: August 2014, Vol. 104, No. 8, pp. 1557-1565.– Study run in an Acute locked psychiatric ward.– Study run in an Acute locked psychiatric ward.
– motivational tobacco cessation treatment combined with nicotine replacement
– Psychiatric measures did not predict abstinence; measures of motivation and tobacco dependence did
– cessation treatment appeared to decrease the risk of rehospitalisation risk.
– Did smoking cessation provide a broader therapeutic benefit?

Smoking Cessation in Mental Health
– Nicotine replacement therapy (NRT):• May require combination of patch and faster acting form
and may require higher doses (Piper et al 2009).
• Longer term use of NRT may be needed compared to general population (Horst et al 2005).
– Bupropion:– Bupropion:• Triples rates of non-smoking in those with schizophrenia
with no adverse effects (Tsoi et al 2010)
– Varenicline:• Evidence to support use in Depression more so than in
Schizophrenia (RCP/RCPsych 2013; NICE 2013).
• No evidence that Varenicline is associated with adverse neuropsychiatric events (Gibbons 2013).

Smoking and Psychotropic Medication
• Interactions are caused by polycyclic aromatic hydrocarbons which are components of tobacco smoke and induce hepatic CYP1A1, 1A2, and possibly 2E1 isoenzymes.
• It is not Nicotine and nicotine replacement therapy will not affect changes in medication levels caused by smoking cessation.
• As well as prescribed medications smoking can increase caffeine metabolism and clearance.metabolism and clearance.
• For example:– When a patient stops smoking, clozapine and olanzapine dosages may
need to be reduced by 30% to 40% to avoid elevated serum concentrations and risk of toxicity (Fankhauser 2013).
• Number of lists of how different medications may be affected by smoking cessation available on-line or in medication guidebooks/handbooks.
Conclusions
• Smoking is a significant problem among those with mental health.
• Smoking cessation can have physical and mental health benefits.
• Smoking cessation interventions are successful in • Smoking cessation interventions are successful in mental health settings.
• Need for adequate staff training across all mental health settings (Community; Day hospital and In-patient) to initiate smoking cessation.
• Need to consider smoking cessation method and effect on medication.
References
• Druss BG,. Zhao L., Von Esenwein S et al Understanding excess mortality in Persons with mental illness. Medical Care 49:6
• Lawn S, Campion J. (2013) Achieving smoke free mental health services; lessons from the past decade of implementation research. Int J Environ Res Public Health 10:4224-44.
• McEwen A., West R., McRobbie H. Motives for smoking and their correlates in clients attending a Stop Smoking treatment services. correlates in clients attending a Stop Smoking treatment services. Nicotine Tob Res 2008;10:843-50.
• Australian Bureau of Statistics. National Health Survey 2004–05: Summary of Results. Cat. No. 4364.0. Canberra, Australia: ABS, 2006.
• Clancy N., Zwar N., Richmond R. (2014). Depression, smoking and smoking cessation: a qualitative study. Family Practice
• Fidler J., West R. (2009) Self Perceived smoking motives and their correlates in a general population sample Nicoteine Tob Res.
References
• Hughes J. (2007) Effects of abstinence from tobacco: Valid symptoms and time course. Nicoteine and Tobacco Research 9; 3 315-27.
• Lê Cook B, Ferris Wayne G, Kafali EN, Liu Z, Shu C, Flores M (2014) Trends in Smoking Among Adults With Mental Illness and Association Between Mental Health Treatment and Smoking Cessation. JAMA 311(2).
• Hall SM, Tsoh JY, Prochaska JJ, Eisendrath S, Rossi JS, Redding CA, Rosen AB, Meisner M, Humfleet GL, Gorecki JA (2006) Treatment for cigarette smoking among depressed mental health outpatients: a randomized AB, Meisner M, Humfleet GL, Gorecki JA (2006) Treatment for cigarette smoking among depressed mental health outpatients: a randomized clinical trial.Am J Public Health; 96(10):1808-14.
• Prochaska J, Hall SE, Delucchi K, Hall SM (2014) Efficacy of Initiating Tobacco Dependence Treatment in Inpatient Psychiatry: A Randomized Controlled Trial. Am J Public Health; 104(8), 1557-1565.
• Tsoi DT, Porwal M, Webster AC (2010) Interventions for smoking cessation and reduction in individuals with schizophrenia (Review). Cochrane Database Syst Rev
References
• Fankhauser MP (2013) Drug interactions with tobacco smoke: Implications for patient care. Current Psychiatry; 12(1).
• Siru R, Hulse GK, Tait RJ (2009) Assessing motivation to quit smoking in people with mental illness: A review. Addiction; 104: 719–733.
• Stockings E, Bowman J, McElwaine K, Baker A, Terry M, Bartlem K, Wye P,Bridge P, Knight J, Wiggers J (2013) Readiness to quit smoking and quit attempts among Australian mental health inpatients. Nicotine Tob. Res; 15: 942–949.attempts among Australian mental health inpatients. Nicotine Tob. Res; 15: 942–949.
• Piper ME, (2009) A randomised placebo-controlled clinical trial of 5 smoking cessation pharmacotherapies. Arch Gen Psych 66(11)
• Horst W, Klein MW, Williams D, Werder SF (2005) Extended use of nicotine replacement therapy to maintain smoking cessation in persons with schizophrenia. Neuropsychiatr Dis Treat; 1(4): 349–355.
• Gibbons RD, Mann JJ (2013) Varenicline, Smoking Cessation and Neuropsychiatric adverse events. Am J Psych 170(12).