mr. ankur prabhat kumar - spine wellness expertspinewellnessexpert.com/images/ppt/hemangioma.pdf ·...
TRANSCRIPT

Vertebral Hemangioma

Presenting complaintsPresenting complaints
• 30 year old male30 year old male• Low back pain x 11 years Low back pain x 11 years • Radiating pain to both lower limbs- 6 Radiating pain to both lower limbs- 6
months.months.• Tingling sensation in both lower limbs Tingling sensation in both lower limbs

History of present illness History of present illness • Back Pain: Present through- out the day, less on lying down, Back Pain: Present through- out the day, less on lying down,
aggravated on sitting up and walking.aggravated on sitting up and walking.• Pain is radiating to both lower limbs along the anterior aspect of the Pain is radiating to both lower limbs along the anterior aspect of the
thighsthighs
• Unable to sit up or walk due to the pain in the back since the past 6 Unable to sit up or walk due to the pain in the back since the past 6 monthsmonths
• Associated tingling sensation along the thigh Associated tingling sensation along the thigh
• No weakness in the lower limbsNo weakness in the lower limbs
• No bladder/ bowel symptomsNo bladder/ bowel symptoms
• No constitutional symptomsNo constitutional symptoms

Medical HistoryDiagnosed to be having a hemangioma of the third
lumbar vertebra for which embolisation and posterior decompression by laminectomy of the L3 vertebra was done in 1999
The surgery had to be abandoned due to severe bleeding.
Patients neurological status worsened after immediately after surgery- was unable to walk-but gradually improved- was able to walk independently until six months ago

ExaminationExamination
• Vertical midline scar noted over the lumbar Vertical midline scar noted over the lumbar region extending from L2 to L5 spinous processregion extending from L2 to L5 spinous process
• Kyphotic deformity present at lumbar region L3 Kyphotic deformity present at lumbar region L3 vertebravertebra
• Tenderness present L1-L4 vertebraTenderness present L1-L4 vertebra• ROM of LS Spine could not be assessed due to ROM of LS Spine could not be assessed due to
painpain• No neurological deficitNo neurological deficit

X ray findingsX ray findings
• Collapse of the L3 vertebra
• Lytic lesion in L2 with prominent vertical trabeculae
• Kyphotic deformity at L3 vertebra= 400
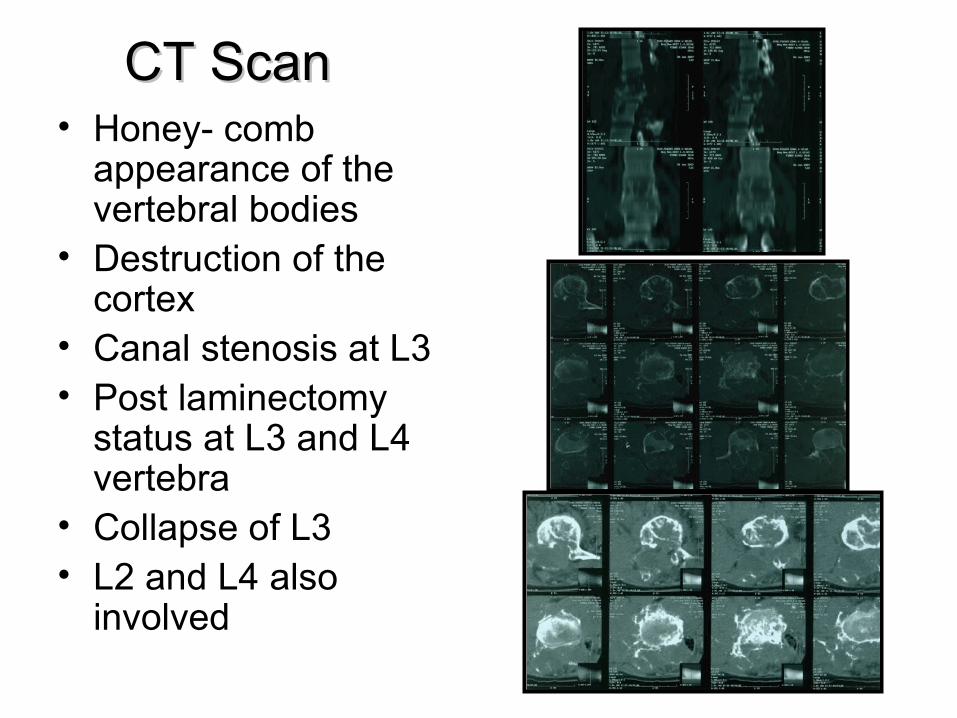
CT ScanCT Scan• Honey- comb
appearance of the vertebral bodies
• Destruction of the cortex
• Canal stenosis at L3• Post laminectomy
status at L3 and L4 vertebra
• Collapse of L3• L2 and L4 also
involved

CT Angiography and embolisation
Markedly hypervascular expansile osseous lesions involving L1 to L4 vertebra with large soft tissue component, suggestive of hemangioma
1. Confirm the diagnosis1. Confirm the diagnosis2. Extent of the lesion, including any 2. Extent of the lesion, including any
extraosseous extensionextraosseous extension3. Relationship between the arterial supply 3. Relationship between the arterial supply
of the tumor and the spinal cord and of the tumor and the spinal cord and thus is crucial in preoperative planning thus is crucial in preoperative planning for resection of osseous hemangiomasfor resection of osseous hemangiomas
Final diagnosis Final diagnosis
Vertebral Hemangioma L2,L3 and L4 Vertebral Hemangioma L2,L3 and L4 vertebrae with extra- vertebral extension vertebrae with extra- vertebral extension into paraspinal and para- vertebral into paraspinal and para- vertebral regions with progressive kyphosis regions with progressive kyphosis without neurological deficitswithout neurological deficits

Surgical Planning• Pre- operative embolisation
1.1. Reduce tumor sizeReduce tumor size2.2. Relieve spinal blockRelieve spinal block3.3. It is the procedure of choice in reducing It is the procedure of choice in reducing
intraoperative bleedingintraoperative bleeding

Aim of our surgery
• adequate decompression
• mechanical stability of the spine
• Pain elimination

Proposed procedure
Posterior decompression L2, L3 and L4 level, Corpectomy of L2 and bone grafting with correction of kyphosis and posterior stabilisation with pedicle screw construct
• Arranged enough Blood and Blood substitutes
• Prepare for a staged procedure in case of excessive bleeding
Surgery DoneSurgery DonePosterior midline exposure was donePosterior midline exposure was done
There was torrential bleeding from the hemangioma There was torrential bleeding from the hemangioma which had infiltrated the paraspinal muscles= 6 units of which had infiltrated the paraspinal muscles= 6 units of blood transfused during surgery.blood transfused during surgery.
Surgical wound had to be temporarily closed to provide Surgical wound had to be temporarily closed to provide compression and control bleedingcompression and control bleeding
Surgical time had to be cut short. As a result a Surgical time had to be cut short. As a result a Pedicle screw fixation at D12, L1 and L5 vertebrae Pedicle screw fixation at D12, L1 and L5 vertebrae only could be achievedonly could be achieved

Pedicle screws between D12, L1 and L5
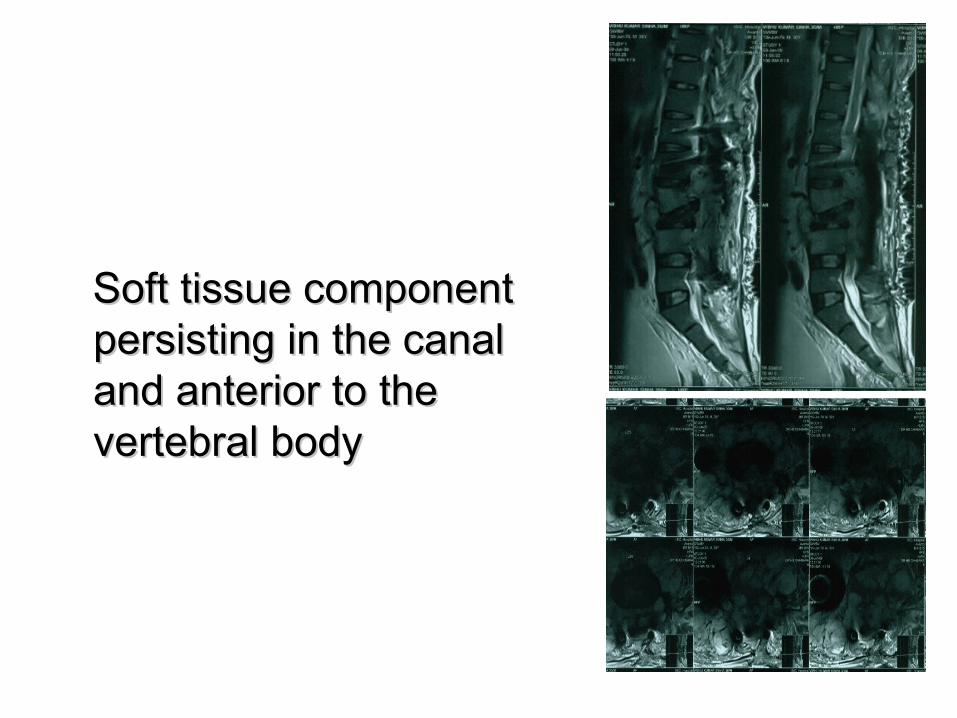
Soft tissue component Soft tissue component persisting in the canal persisting in the canal and anterior to the and anterior to the vertebral bodyvertebral body

CT Scan showing accurate screw placement

Post OperativePost Operative• Immediately after surgery the patient was stable and the Immediately after surgery the patient was stable and the
neurological status was normalneurological status was normal
• On second day post surgery he developed numbness and loss of On second day post surgery he developed numbness and loss of power in both lower limbs. power in both lower limbs.
L.L - R L L2 1 1 L3 3 3 L4 0 2 L5 0 2 S1 0 2
PAS : Absent PAS : Absent VAC : AbsentVAC : Absent

• He was reviewed by a neurologist and was He was reviewed by a neurologist and was diagnosed as cauda equina syndrome diagnosed as cauda equina syndrome secondary to bleeding in extradural space. secondary to bleeding in extradural space.
• He under went a repeat embolisation in an He under went a repeat embolisation in an effort to bring down the tumor size and effort to bring down the tumor size and relieve the canal stenosisrelieve the canal stenosis
• Subsequently he regained motor power Subsequently he regained motor power but only partiallybut only partially

Second Operative procedure • Done 2 weeks following the primary surgery• Pre- operative embolisation was repeated• Anterior trans- peritoneal approach was done• 8 feeder vessels arising from the aorta were ligated• L 2 and L3 corpectomy done with discectomy of L1-2
and L3-4 levels.• Complete decompression of the canal was achieved • Strut graft from iliac crest was placed anteriorly in the
corpectomy defect.• Blood loss- 700 ml

Iliac strut graft noted between L2 and L4


NEUROLOGICAL STATUS• Hypotonia in right lower limb• Power – 5/5 in B/L U.L , • L.L - R L• L2 1 2• L3 3 3• L4 1 4• L5 1 3• S1 1 3 • SENSORY – INTACT• PAS- Present • VAC- Present

Take Home message
Hemangioma rarely presents with deficits
Have to be well prepared before surgery
Reduce the risk of bleeding by embolisation
Expect bleeding in spite of a well done embolisation procedure