morphine: new findings of an old drug by amnuay thithapandha, ph.d. professor, office of academic...
TRANSCRIPT
MORPHINE: New Findings of an Old Drug
By
Amnuay Thithapandha, Ph.D.
Professor, Office of Academic Affairs
Faculty of Medicine Ramathibodi Hospital
Mahidol University

Among the remedies which it has
pleased Almighty God to give to man
to relieve his sufferings, none is so
universal and so efficacious as opium.
Sydenham (1680)

In 1806, F. Serturner (a German pharmacist) reported the isolation of a pure substance from opium that he named
MORPHINE, after Morpheus (Greek god
of dreams)
CONFUSING TERMINOLOGY
Narcotic ( Greek = stupor ) ---- used only in a legal context
Opioid--- any substance (synthetic or semisynthetic) that has
morphine-like effectsOpiate--- a substance derived from
opium and has morphine-like effects

MAIN USES OF MORPHINEMAIN USES OF MORPHINE
1. SEVERE PAIN
• POST-OPERATIVE
• TRAUMATIC
2. CANCER PAIN (terminal)
3. BURN PAIN
4. TO INTERRUPT THE PAIN CYCLE
Remember : “Severe Pain Can Kill”
(F.J. Brescia et al., J Clinical Oncol 10 : 149, 1992;
G.K. Groulay & D.A. Cherry, Clin J Pain 7:347,1991 )
MORPHINE : KINETICS ORAL BIOAVAILABILITY = 20 %
HALF – LIFE ( PO, IM ,SC , IV ) = 2 – 3 h
CONJUGATED IN LIVER & EXCRETED VIA
KIDNEY ( 90 % OR MORE )
M6G = Active metabolite (9X)
M3G = Toxic metabolite• IN PATIENTS WITH DEHYDRATION, RENAL
FAILURE OR HEPATIC INSUFFICIENCY
REDUCE DOSE
INCREASE DOSING INTERNVAL
USE ONLY PRN IF OLIGURIA OR ANURIA IS PRESENT

ADVERSE EFFECTS OF MORPHINE
COMMON : N+V, DROWSINESS
(initial) DELIRIUM (CONFUSION)
COMMON : CONSTIPATION(on- going) SEDATION
OCCASIONAL : DRY MOUTH
URINARY RETENTION PRURITIS HALLUCINATION RESPIRATORY DEPRESSION
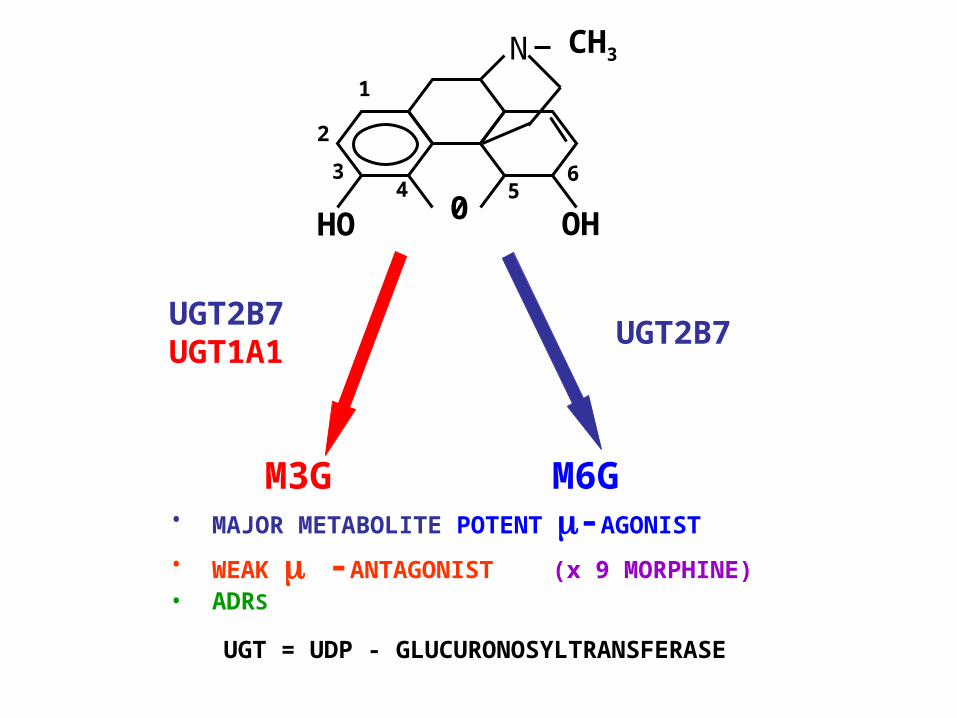
2
1
34
05
6
HO OH
M3G M6G• MAJOR METABOLITE POTENT -AGONIST
• WEAK -ANTAGONIST (x 9 MORPHINE)• ADRS
UGT2B7UGT1A1
UGT2B7
UGT = UDP - GLUCURONOSYLTRANSFERASE
N CH3
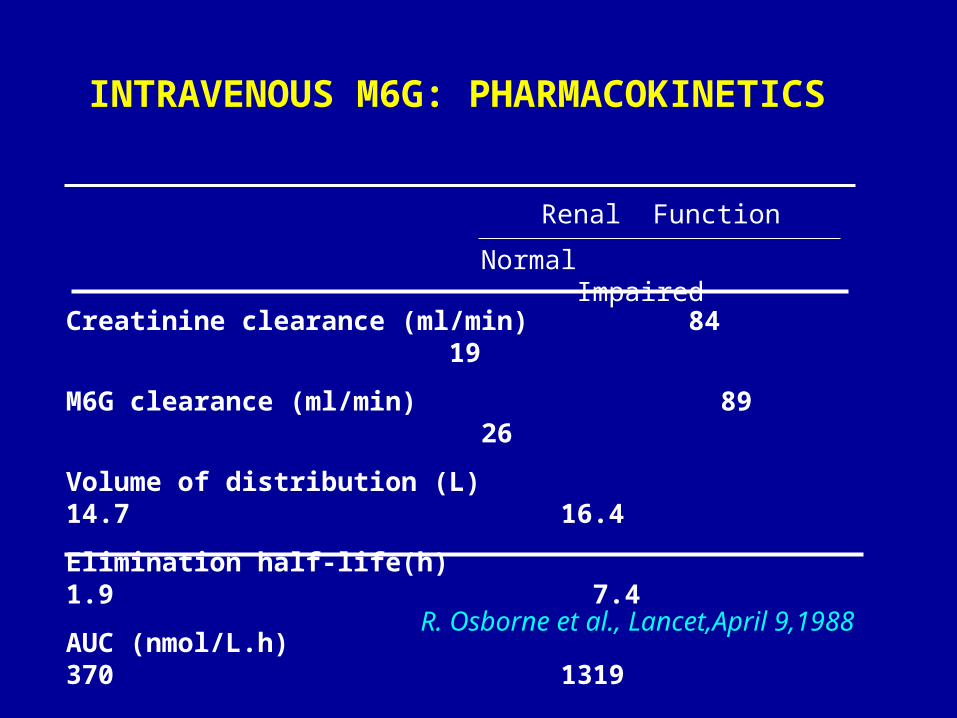
INTRAVENOUS M6G: PHARMACOKINETICS
Renal Function
Normal Impaired
Creatinine clearance (ml/min) 84 19
M6G clearance (ml/min) 89 26
Volume of distribution (L) 14.7 16.4
Elimination half-life(h) 1.9 7.4
AUC (nmol/L.h) 370 1319
BW=70 kg; Dose= 1 mg
AUC from zero to infinity
R. Osborne et al., Lancet,April 9,1988

1 2 43 5 6 7 8
60
100
20
80
40
TIME (h)
M6G (0.5 mg, IV)V
AS
Cancer pain N = 5 x ± SE IV OVER 5 MIN
R. Osborne et al Lancet, April 9, 1988
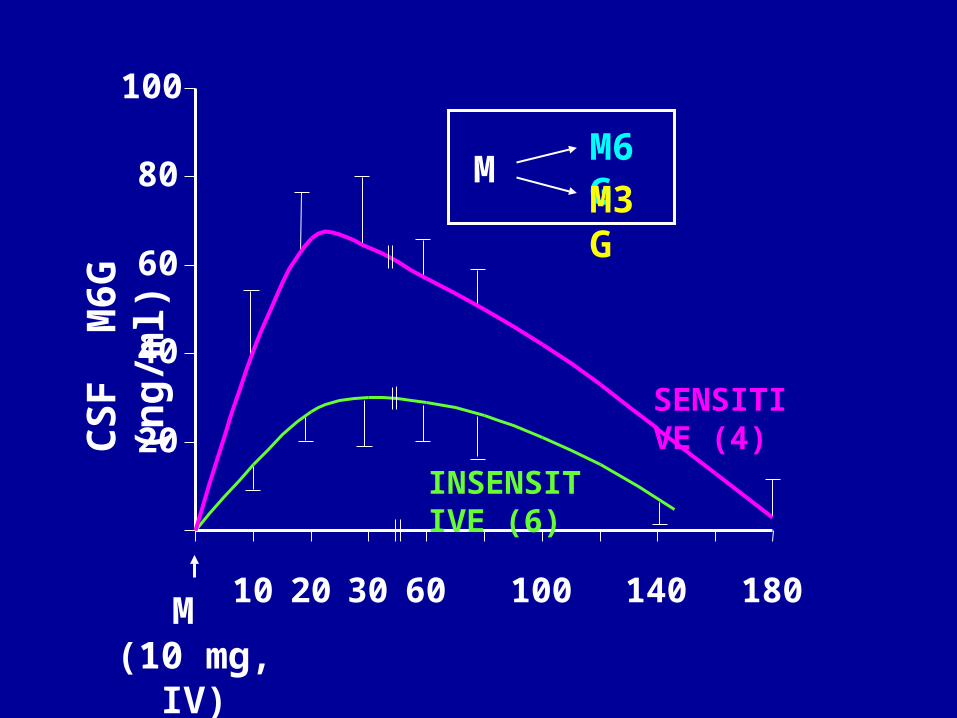
20
40
60
80
100
10 20 30 60 100 140 180M (10 mg,
IV)
INSENSITIVE (6)
SENSITIVE (4)
MM6GM3G
CS
F M
6G
(n
g/m
l)
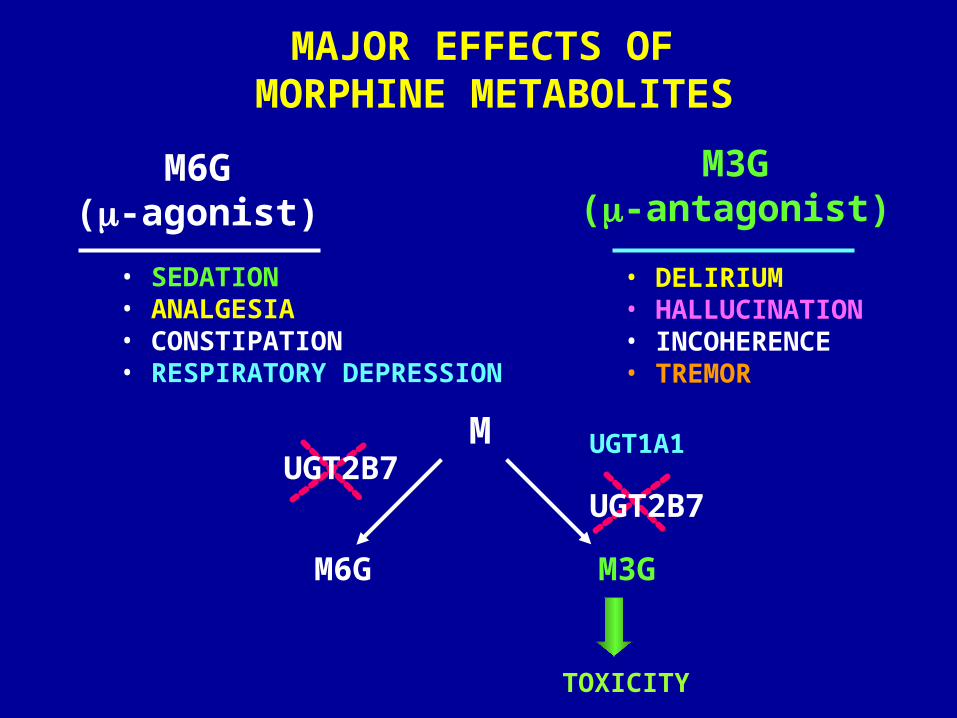
MAJOR EFFECTS OF MORPHINE METABOLITES
M6G(-agonist)
M3G(-antagonist)
• SEDATION• ANALGESIA• CONSTIPATION• RESPIRATORY DEPRESSION
• DELIRIUM• HALLUCINATION• INCOHERENCE• TREMOR
M
M6G M3G
TOXICITY
UGT2B7UGT1A1
UGT2B7

Case: MORPHINE REACTIONS
Sirima Triamruktakul, a 45-year-old woman
weighing 56 Kg, was admitted to the emergency room
because of low back pain. The pain intensity was such
that she could not mobilize and felt desperate. She was
given a small dose of morphine (5 mg, IM) but did not
obtain any pain relief even at 1 hour after the drug
administration. In fact, she manifested signs of tremor
and hallucination which became apparent at only half
an hour after the opioid. Diazepam (5 mg, IV) was needed
to ameliorate these adverse reactions.
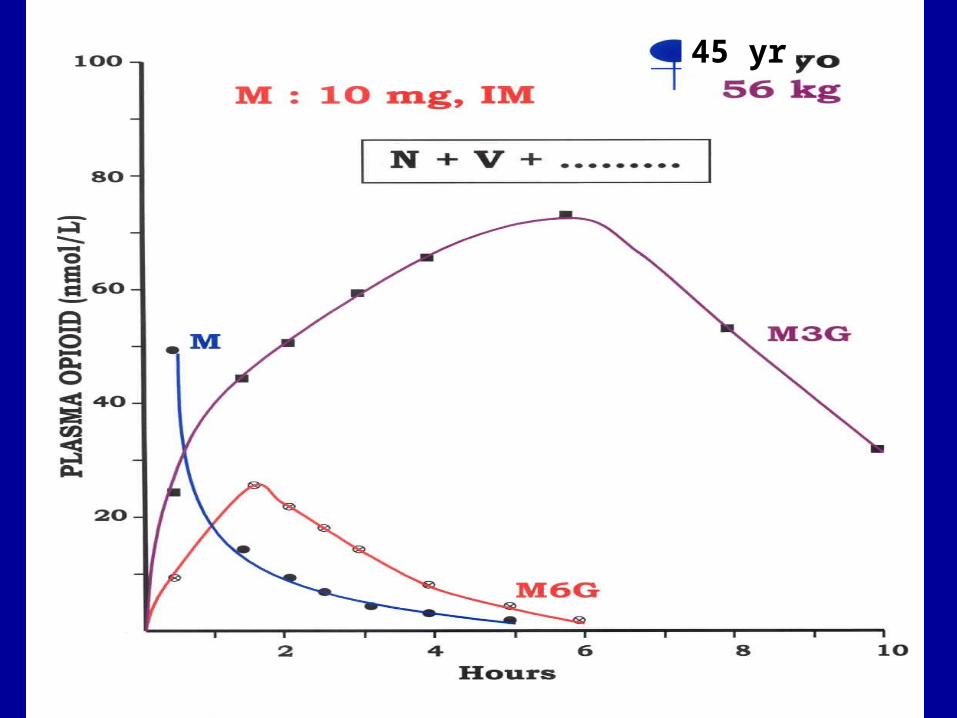
Case: MORPHINE REACTIONS (CONT)
Three months later she was readmitted with the same
complaint. Morphine (5 mg, IM) was tried on her again
with the same signs of its adverse reactions. Blood
samples were taken serially from 0.5,1,2,3,4,6 and 8 hours.
When morphine and its metabolites were analyzed, it was
found that she could make little M6G but an unusually large
M3G profile was noted.
45 yr
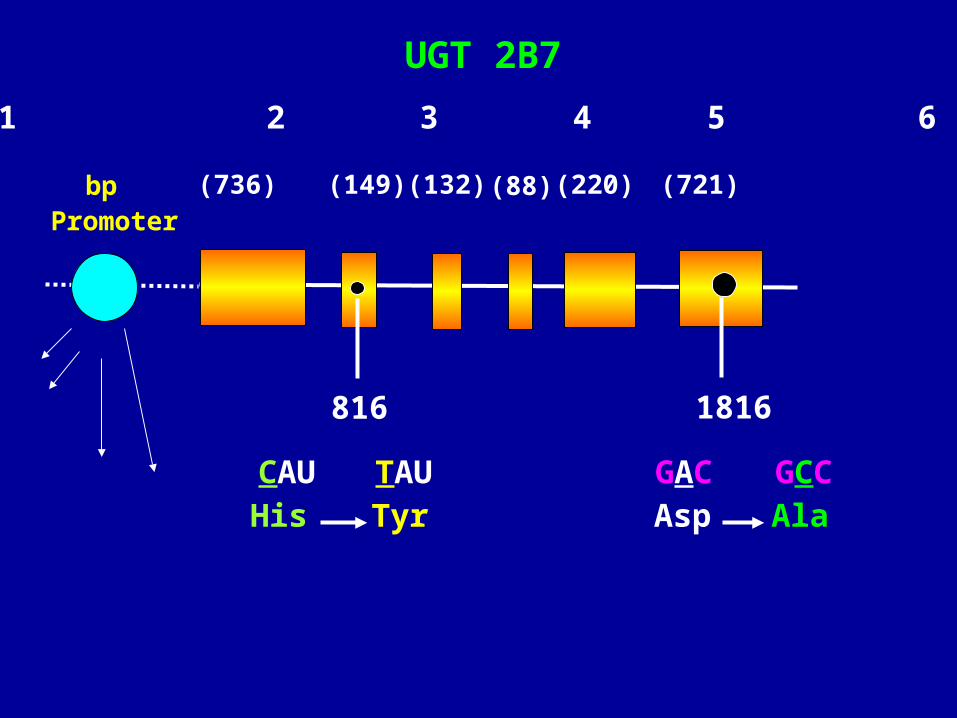
UGT 2B7
CAU TAUHis Tyr
1 2 3 4 5 6
1816
(736) (149) (132) (88) (220) (721)
GAC GCCAsp Ala
816
bpPromoter

GENETIC ANOMALIES UNDERLINE THE CAUSE OF SEVERE ADVERSE REACTIONS TO MORPHINE
PATIENT DISEASE M3G ADRS GENETIC CAUSE
M6G
Appendicitis 10:1 N + V Point mutation in exon 2,6
Burn 25:1 Delirium Point mutation in + Tremor exon 2,6
Renal stone 30:1 Tremor Insertion of an extra
+ Hallucination TA in the promoter;
Point mutation in exon 6
Low back pain 40:1 N + V Gene deletion + Hallucination
+ Seizure
The M3G:M6G ratio was obtained from AUC 0.5-8h after morphine (5 mg, IM).
UGT2BT
40.4 3.4 9.2 12.8 15.6
35.2Xanthopsia
10.0 8.4
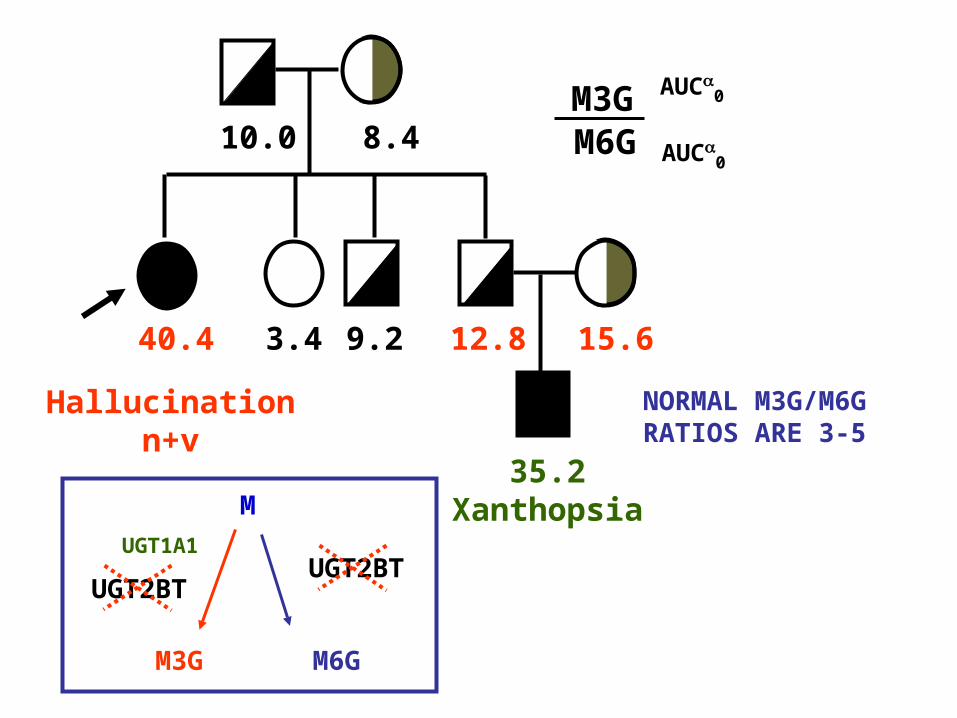
Hallucinationn+v
NORMAL M3G/M6G RATIOS ARE 3-5
M3G AUC0
M6G AUC
0
M
M3G M6G
UGT1A1UGT2BT
Nose itching and pruritis caused by
morphine are due to histamine release
and are antagonized by hydroxyzine
or naloxone. In the presence of the
antagonist, however, plasma histamine level in the sensitive individuals remains elevated.
A.Thithapandha, Toxicol. Appl. Pharmacol., 2007(in press)

MORPHINE-INDUCEDHISTAMINE RELEASE IN SENSITIVE PATIENTS
* P < 0.05
PLA
SM
A
CO
NC
(n
g/m
l)
20
10
*
*
8
0
1
2
3
4
5
CONTROL INSENSITIVE SENSITIVE

MORPHINE
(Base, pKa = 7.9)
NALOXONE
M – OPIOIDRECEPTOR
MASTCELL
ANALGESIA
HISTAMINE
HYDROXYZINE
ITCHING
No patient should ever wish for death because of a physician’s reluctance to use adequate amounts of effective opioids.
Gutstein and Akil (Goodman & Gilman, 11th edition, 2006)