molecular identification of the tca alloantigen as the...
TRANSCRIPT

(CANCER RESEARCH 43, 1914-1920, April 1983|0008-5472/83/0043-0000$02.00
Molecular Identification of the TCA Alloantigen as the Transferrin Receptor onT-Cells of a Leukemic Patient with Serum from a Monozygotic Twin Brother1
Jos P. A. Derks,2 Lilian Hofmans, Hans W. Bruning, and Jon J. van Rood
Department of Immunohaematology, Bloodbank, University Hospital, Ri/nsburgerweg 10, Leiden, The Netherlands
ABSTRACT
The transferrin receptor is encoded by a diallelic locus whichhad been described as the T-cell antigenic system TCA. Using ahuman lymphoblastoid T-cell line (MSB) which reportedly carriesa transferrin receptor and which we showed to be TCA-2 positiveby serology, it appeared that only a TCA-2 but not a TCA-1specific alloantiserum had the capacity to precipitate a proteinwith a molecular weight of 94,000, which comigrated exactlywith the M, 94,000 protein precipitated by the rabbit anti-HSBand rabbit anti-SB antisera, as well as the transferrin receptorwhich was precipitated by a transferrin-antitransferrin complex.The positive sera and the latter complex were shown to cross-react in a binding assay. Conversely, a monospecific TCA-1
alloantiserum was shown to react with the M, 94,000 protein ofTCA-1-positive leukocyte suspensions.
The allelomorphism of the transferrin receptor may be relevantfor the eventual regulatory mechanism controlling cell proliferation, which would be essential at least for those cells that aresupposed to play an immunological role like the TCA-positivecells which are described as T-cells probably involved in the
process of immunosuppression. In addition, we found increasingamounts of autoantibodies with TCA-1 specificity in serum froma healthy individual (referred to as "donor" in this paper), whose
brother at the same time suffered a chronic myeloid leukemia,probably associated with a retrovirus, and whose blood in contrast was shown to contain cytotoxic anti-TCB, from a dialleliclocus expressed on theophylline-insensitive T-cells, and anti-B-
cell activity.
INTRODUCTION
In the course of therapy, a chronic myeloid leukemia patientwas to be treated by BM3 transplantation using cells of a mon-
ozygotic twin brother. BM transplantation is an accepted treatment for severe aplastic anemia, severe combined immunodeficiency, and acute forms of leukemia (12, 34, 40). Unlike the
1This study was supported by the Queen Wilhelmina Foundation, the Dutch
Cancer Research Foundation This article is one of a series of two. For Paper 1,see Ref. 8.
2To whom requests for reprints should be addressed.3The abbreviations used are: BM, bone marrow; GVH. graft versus host; ii2M,
A-microglobulin; p23,30, B-cell-specific protein with M, 23.000 and M, 30,000subunits; SSV, simian sarcoma virus; p30, a viral protein with a molecular weightof 30,000; TCA, diallelic locus expressed on theophylline-sensitive T-cells; TCB,diallelic locus expressed on theophylline-insensitive T-cells; Te, T-cell populationbearing receptors for IgG; T0, T-cell population bearing no receptors for either IgGor IgM; TM, T-cell population bearing receptors for IgM; Ph1, Philadelphia chromo
some; TCF, 2-color fluorescence; ADCC, antibody-dependent cellular cytotoxicity;MSB, a human lymphoblastoid T-cell line; SB, a human lymphoblastoid B-cell line;Con A, concanavalin A; p94, membrane protein with a molecular weight of 94,000;p78, membrane protein with a molecular weight of 78,000; p80, membrane proteinwith a molecular weight of 80.000; p95, membrane protein with a molecular weightof 95,000; gp70, glycoprotein with a molecular weight of 70,000.
Received January 18, 1982; accepted December 30. 1982.
situation with severe combined immunodeficiency patients, HLAbarriers are difficult to overcome with leukemia patients (12), andGVH reaction is a frequent cause of patient death. However,even HLA-matched allogeneic BM transplantation can cause
severe GVH, despite immunosuppression (34), and thereforenon-HLA antigens are also relevant to graft outcome (7, 46).Transplantation with autologous-remission BM often results inrelapse, partly as a result of residual leukemic cells in the graft(10, 34). For these reasons, transplantation with BM of a mon-
ozygotic twin is preferred. However, the mechanism of theimmune response by which GVH or a relapse is controlled stillremains very unclear, since even in isologous BM transplantationacute GVH has been reported as a result of an imbalance ofautoreactive cells (3,30), and functional abnormalities associatedwith imbalance of T-cells have been found in leukemic patients
(6).This report describes the involvement of functional T-cells in a
BM-transplanted leukemia patient and his BM donor, a mono-
zygotic twin. The patient under study, although intensely treated,finally died in relapse. The immunological investigations wereextended onto the molecular level. Products of the major histo-
compatibility complex have been shown to play a major role inimmune phenomena involving specific cell-cell interactions (11),
and qualitative as well as quantitative changes in the expressionof histocompatibility antigens on transformed cells have beendescribed for various tumor systems (5, 16, 32, 33). Therefore,alloantisera routinely used in HLA typing, heterologous rabbitanti-/i2M and rabbit anti-p23,30, were used to study possiblemolecular variation of HLA determinants on the leukemic cells.No alteration could be detected, however, in either the antigenicexpression or molecular weight of the major histocompatibilitycomplex determinants on the patient's cells.
Further attention was paid to antigens that may be associatedwith the leukemic transformation of the cell by using heterologous antisera to SSV and SSV p30, autologous patient serum,and serum from the monozygotic twin brother. A difference inthe antigenic profile of patient versus donor leukocytes wasshown to be at least partly associated with the presence of aretrovirus in some of the leukemic cells of this particular patient(8).
Patient and donor sera were screened for leukocyte antibodies. The T-cell-specific alloantisera found thus far using the
theophylline method described by van Leeuwen (43) appearedto be reactive with the products of either one of the diallelic lociTCA and TCB (44). TCA is expressed mainly on TG cells andsome of the T0 cells; TCB is found mainly on TM cells and someof the TG cells. The T-cell allospecificity of the patient and donor
serum was studied because of the alleged functional aspects ofthe 2 T-cell subpopulations, TG, a suppressor cell (15, 27), and
TM, a helper cell (25), which are still subjected to intensiveresearch (14, 43). For a comparison with other published reports
1914 CANCER RESEARCH VOL. 43
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

TCA Alloantigens as Transferrin Receptors
of human T-cell-specific molecules, we refer to Omary ef al. (28),
Pratt ef al. (29), Trowbridge ef al. (41, 42), and Terhorst ef al.(39). The T9, the transferrin receptor, and the TCA alloantigenare shown to be one and the same protein. In this paper, weshow the expression of the transferrin receptor to be the majorantigenic difference between the patient and donor leukocytes,probably resulting from a differential outgrowth of presumed¡mmunoregulatory T-lymphocytes. Our findings suggest that T-
cell antibodies might have been relevant to the final outcome ofthe therapy, in which the patient died in relapse; his brother hasremained medically unaffected up to now, 3 years after thepatient's death.
CASE HISTORY
The patient was a 43-year-old male. Diagnosis of Ph'-positive
chronic myeloid leukemia was made in March 1978 and subsequently treated with chlorambucil. In September 1978, the patient developed a blast crisis, which proved to be unresponsiveto chemotherapy (1-ß-D-arabinofuranosylcytosine, 6-thioguan-
ine, hydroxyurea). On the basis of 21 polymorphic gene markers(RBC antigens, serum proteins, and HLA antigens), it was foundthat the patient's brother was a monozygous twin (p < 0.006).
From October 11, 1978, onwards, the patient was nursed inlaminar-flow isolation and treated daily with 40 mg Adriamycinfrom Days 1 to 4, 180 mg 1-fJ-o-arabinofuranosylcytosine fromDays 1 to 8, and 120 mg 6-thioguanine on Days 1 to 8. On Day
20, the conditioning of the patient for BM transplantation wasstarted with cyclophosphamide (120 mg/kg body weight) andfractionated total-body irradiation (6 treatments, 200 rads each).
On Day 30, the patient was given a transplant of a total of 0.9x 1010 nucleated BM cells, despite severe myelofibrosis. A
complete hematological recovery was observed, and cytogeneticanalysis revealed the absence of the Ph1chromosome. However,
in January 1979, blast cells appeared in the peripheral blood,and the Ph1 chromosome reappeared with other cytogenetic
abnormalities, translocations t(6;12) and t(14;16). The number ofblast cells suddenly increased very rapidly, and after a conventional cytostatic therapy the patient died on January 31, 1979.During the pre- and posttransplantation periods, the patient
received 16 transfusions with RBC concentrates and 31 platelettransfusions, as well as 2 platelet and 5 buffy-coat cell transfu
sions of BM donor origin.
MATERIALS AND METHODS
Serological Techniques. Sera of the patient and donor were testedin the standard NIH microcytotoxicity assay as described by Mittal et al.(24); the indirect immunofluorescence test according to the report of vanLeeuwen ef al. (45); and the TCP test, a complement-dependent cyto-toxicity assay permitting differentiation of B-cells, T-cells, and mono-
cytes, according to the method of van Rood ef al. (47). Patient and donorsera were screened for the presence of alloantibodies against subsetsof T-cells, using the method described by van Leeuwen (43). The ADCCassay, as described by de Rooij-Doyer (9), was performed with a
methodology similar to the one described by Bruning ef al. (4), in whichhe used an automated microfluorometric method to study cell-mediatedlympholysis. Briefly, 4000 carboxyfluorescein-diacetate-labeled target
cells were incubated for 1 hr at room temperature with 5 n\ of antiserum,washed, and incubated again with 100,000 killer cells for 3 hr at 37°.
After a final washing, the percentage of residual fluorescent cells wasassayed with an automatic microfluorometer.
Cellular Techniques. The mixed leukocyte culture test was set upaccording to the technique described by Keuning ef al. (21). The cell-
mediated lympholysis assay was performed according to the techniquedescribed by Goulmy ef al. (17).
Sera. Alloantisera to HLA-A, -B, and -DR antigens, used in routine
HLA typing, were applied in radioimmunoprecipitation experiments. Rabbit anti-p23,30, kindly provided by Dr. J. L. Strominger, had beenprepared by immunizing rabbits with the purified B-cell-specific antigencomplex p23,30. This antiserum recognizes the total B-subset of lymphocytes (37). A rabbit antiserum to MSB cells (a T-cell lymphoblastoidcell line) is a strong anti-T-cell serum, containing only low amounts of B-cell-specific antibodies. A rabbit antiserum to SB cells (allegedly a B-
lymphoblastoid cell line) contained high titers of antibodies reactive withla-like antigens and antigens present on a subpopulation of T-cells. Goatanti-human IgG (Fc)-TRITC (Nordic Co., The Netherlands) was pepsin
treated, absorbed on a Protein A column, and used for direct and indirectimmunofluorescence assays. A potent antiserum to human immunoglob-ulin light chain, rabbit anti-lg(L), was prepared by immunizing a rabbitrepeatedly with serum-free culture supematants of the RPMI 1640 cellline. Rabbit anti-/i2M is a rabbit antiserum to human (J2M(Dako, Copenhagen, Denmark). Goat anti-SSV was obtained from the National CancerInstitute (Bethesda, Md.) (serum identification, 3S-0172). It had been
prepared by immunizing a goat with disrupted SSV particles, propagatedin the NC37-cell line. According to the National Cancer Institute, the
serum showed only one single band when tested in immunodiffusionagainst SSV antigens. It showed 2 bands when tested against NC37cellular antigens. The Sepharose CL-4B-Protein A-binding lgG2 fraction
of the absorbed serum did not contain reactivity towards SSV p30 in aradioimmunoprecipitation. We absorbed the serum twice with cell membranes of 108 uninfected NC37 cells per ml antiserum to remove all
aspecific activity in radioimmunoprecipitation. The unabsorbed serumwas kindly provided by Dr. P. Herbrink, State University of Leiden, Leiden,The Netherlands (19). The monoclonal anti-T-cell antibody mentioned inthis article is R3/41-10 (36). The anti-TCA specificity of the alloantisera
used is fully described by van Leeuwen ef a/. (44). The donor serumcarries the initials R.S. in that article.
Transferrin Receptor Binding. The transferrin receptor was boundby incubating antigenic extracts of 106cells with 100 ng human transferrin(AB Kabi, Stockholm, Sweden) for 30 min at 37°and precipitation with
Sepharose CL-4B-Protein A-bound rabbit anti-human transferrin (CatalogNo. A-061; Dako). This ratio has been calculated from the binding
inhibition studies reported by Sutherland et al. (38).Cells. Leukocytes were prepared from fresh heparinized blood by
centrifuging on Ficoll-lsopaque and isolating and washing the interphasecells 3 times with 10% fetal calf serum-RPMI (v/v). The only cell line usedwas CCRF-HSB-2, shortly HSB, a lymphoblastoid T-cell line, kindly
provided by Dr. W. Zeylemaker (Central Laboratory of Blood Transfusions, Amsterdam, The Netherlands).
The preparation of |35S]methionine-labeled antigens, the technique of
immunoprecipitation, gel electrophoresis under reducing conditions of5% 2-mercaptoethanol, and fluorography were as described previously
(8).
RESULTS
Monozygosity was established by phenotyping patient andbrother for 21 polymorphic gene markers (p < 0.006). The HLAphenotype was A2, Aw33, B14, B15.2, Cw3, DR5, DR7. Gran-
ulocyte antigens could be detected only on donor cells.Patient blasts did not form caps when incubated with goat
anti-human immunoglobulin-TRITC and therefore clearly werenot B-cells. A heterologous rabbit anti-p23,30, which specificallyrecognizes HLA-DR, gave a low level of cytotoxicity in the TCP
assay but a positive binding to 90% of patient cells in the indirectfluorescence test.
APRIL 1983 1915
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

J. P. A. Derks et al.
Donor and patient sera were screened for leukocyte antibodieswith 3 techniques (Table 1), the NIH cytotoxicity assay, the TCPassay, and the TCP assay with enriched TM and Te cell suspensions (43, 44). When tested with the NIH technique, no cytotoxicantibody could be shown in either patient or donor serum.However, the patient serum appeared to be cytotoxic for B-cells
of 35 randomly chosen healthy individuals in the TCP assay. Thismay be the result of cytostatic drugs present in the patient'sserum, taken on October 13, 1978 (see "Case History" and"Discussion"), inasmuch as this activity could not be absorbed
by a pool of 5 lymphocyte suspensions. Further, the patientserum appeared to contain cytotoxic activity to the TCB-positive
cells of 22 healthy individuals tested thus far. The donor serumcontained antibodies to TCA-positive cells of those 8 of the same22 individuals who had the TCA-1 specificity. Manifold extension
of these experiments has since given consistent results.Measuring the TCA specificity of the donor serum in an ADCC
assay with 6 days of Con A-stimulated targets, only the TCA-1
target was positive (Chart 1), the percentage of reactive cellsbeing 85%.
Additional leukocyte antibody assays have been performed incross-testings of patient and donor material (Table 2). No NIH
cytotoxic reactivity was found in either direction. In the TCPtechnique, which is more sensitive, the patient serum appearedto react with 10% of the autologous blasts, with donor B-cells,and 25% of donor T-cells, which, based on the TCB reactivity ofthe patient serum, must have included the TCB-positive cells.
The patient serum was positive with 20% of the donor cells inthe indirect fluorescence assay, probably also including the TCB-
positive cells.The donor serum reacted with about 5% of the patient's cells
when tested in the indirect immunofluorescence assay. Thispercentage has been established in routine typing and, assumingthat the positive fraction was a T-cell population, may be esti-
Table 1
Screening lor leukocyte antibodies
Sera of donor and patient were screened on a panel of random healthyindividuals.
TechniqueNIH
cytotoxicityTCP3
T-TCF
TMcellsTo cellsNo.
of individualstested59
3522
22Donor
serum8+,
14-Patient
serum+
3TCF, TCP test on B-cells in a total lymphocyte suspension; T-TCF, TCF test
on enriched T-cell suspensions.
3 S TI 3 5 (Vu"
—»serum dilutionChart 1 ADCC assay carried out with pooled allogeneic 1-day-cultured killer
cells and 6-day-cultured Con A-stimulated targets carrying either the TCA-1 (A) orthe TCA-2 (B) alloantigen. , donor serum; , AB control serum; fluor.,fluorescence.
mated too high. This positive fraction could not be found in theTCF technique, because of the high numbers of blasts. Thepatient's leukocyte suspension actually contained only 3 to 5%E-rosetting T-cells when assayed at 4°.
In the mixed leukocyte culture reaction between fresh leukemicand donor cells, stimulation was found in both directions (Table3) although, because of the high spontaneous thymidine incorporation of patient leukemic cells, donor stimulation of patientblasts could not be properly assessed. When patient cells wereused following chemotherapy, no stimulation was seen in eitherdirection. A cell-mediated lympholysis test in the same combi
nations was negative both ways (Table 4).Chemical investigations were performed by immunoprecipita-
tion and polyacrylamide slab gel electrophoresis of [35S]methio-
nine-labeled antigens. When compared with normal rabbit serum
and normal human serum as negative controls (Chart 2, A to D),rabbit anti-/32M (and anti-HLA-A2, not shown) clearly precipitated
HLA molecules from patient and donor cell extracts (Chart 2, Gand H). The HLA molecules of the patient appeared similar tothose of the donor with regard to molecular weight and intensities. Similarly, the HLA-DR molecules of both individuals ap
peared identical when precipitated by the heterologous antiserarabbit anti-p23,30 (Chart 2, G and H) and rabbit anti-SB (Chart2, C and D) (and alloantisera to HLA-DRw5 and DRw7, not
shown). Donor serum specifically recognized proteins with molecular weights of 80,000 and 94,000, present in autologous, butin much higher amounts also in patient cell extracts (Chart 2, Aand B). In a more detailed study, the latter band appeared to
Table 2Leukocyte antibodies in cross-testing patient and donor
Sera of the donor and patient were reacted with cells of both donor and patient.
% of positive cells in suspension
TechniqueSF'-CD SD-CP SP-CP SD-CD
NIH cytotoxicityTCP"
B-cellsT-cells
Lymphocyte indirect immunofluorescence
2520
10
NT
a SP, patient serum; CD, donor cells; SD. donor serum; CP, patient cells; NT,
not tested.6 TCF was performed without enriching for T-cells. In the patient cell suspension,
no distinction could be made between B- and T-cells in establishing the percentage
of reactive cells.
Table 3
Lymphocyte activation in mixed leukocyte culture test as measured by uptake of[3H]thymidine
Calculation of relative response (RR):
AB* —AA"RR(patient —donor) = TTZ TTT x 100% = 137%
RR(donor —.patient) =
AX' - AA-
BA- - SB'
BX- - BB' x 100% = 61%
StimulatingcellsA"
B-X*cpm
[3H)thymidine incorporated in following respondercellsAa21
,58737,26633,16320,078B6,067
3019,792
300X17,677
7,986635603-608
215134
a A, patient; B, donor, X, unrelated control differing at HLA-A, -B, and -D;
, irradiated with 2000 rads.
1916 CANCER RESEARCH VOL. 43
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
TCA Alloantigens as Transferrin Receptors
contain 3 molecules with only slightly differing molecular weights.In consecutive donor serum samples, an increase with time ofspecific activity towards these proteins was observed (notshown). Precipitation was performed with several antisera tostudy the nature of these proteins. A heterologous anti-T-cell
Table 4Cell-mediated lympholysis as measured by "Cr release
% kill" with following target cells
EffectorcellsAB'AX'BA*BX'A°-8-8-6-2B-6-7-3+9X-12-5-7+66
a Calculated by
Experimental release -
spontaneous release
Freeze-thaw release (100%) -
spontaneous release
x 100% = % kill
A, patient; B, donor; X, unrelated control differing at HLA-A, -B, and -D; AB*A stimulated against irradiated B (AX', BA', BX* follow same system).
e migration—» ® e migration
PATIENT DONOR— e
Chart 2. Polyacrylamide slab gels (12.5%) which used [35S|methionine-labele<Nonidet P-40 lysates of patient and donor cells and immunoprecipitation witfseveral antisera. Left, radioactive antigen profiles of patient cell membrane extractswhen reacted with several antisera; right, those of donor cell membrane extracts.Both sets of profiles have been put onto same scale by using heterologous rabbit(Ra) anti-f^M and rabbit anti-p23,30 as positive reagents and normal rabbit serum(NRS) as a negative control. Numbers over peaks, molecular weights in units of1000; 72, running front of the gel, containing proteins with molecular weights of12,000 and lower; DOW, donor serum; PAT, patient serum; NHuS. normal humanserum; GaSSV, goat anti-SSV; NGS, normal goat serum.
serum, rabbit anti-HSB, and an allegedly anti-B-cell serum, rabbitanti-SB, recognized the p94 antigen in both patient and donorcell extracts (Chart 2, C and D). A rabbit antiserum to immuno-globulin light chain, rabbit anti-lg(L), did not precipitate a clear
band from patient or donor cell extracts (Chart 2, G and H). Ap78 molecule could be precipitated with a goat anti-SSV anti-
serum only from patient cell extracts (Chart 2, £and F). Althoughit cannot be seen in Chart 2£,the molecular weight of this p78,as seen on the autoradiographic films, appears slightly smallerthan the p80 precipitated by donor serum.
A p30 could be precipitated only from patient cell extracts bypatient serum (Chart 2, A and B). The latter had been shown tocross-react with SSV p30 (8). In another set of experiments, the
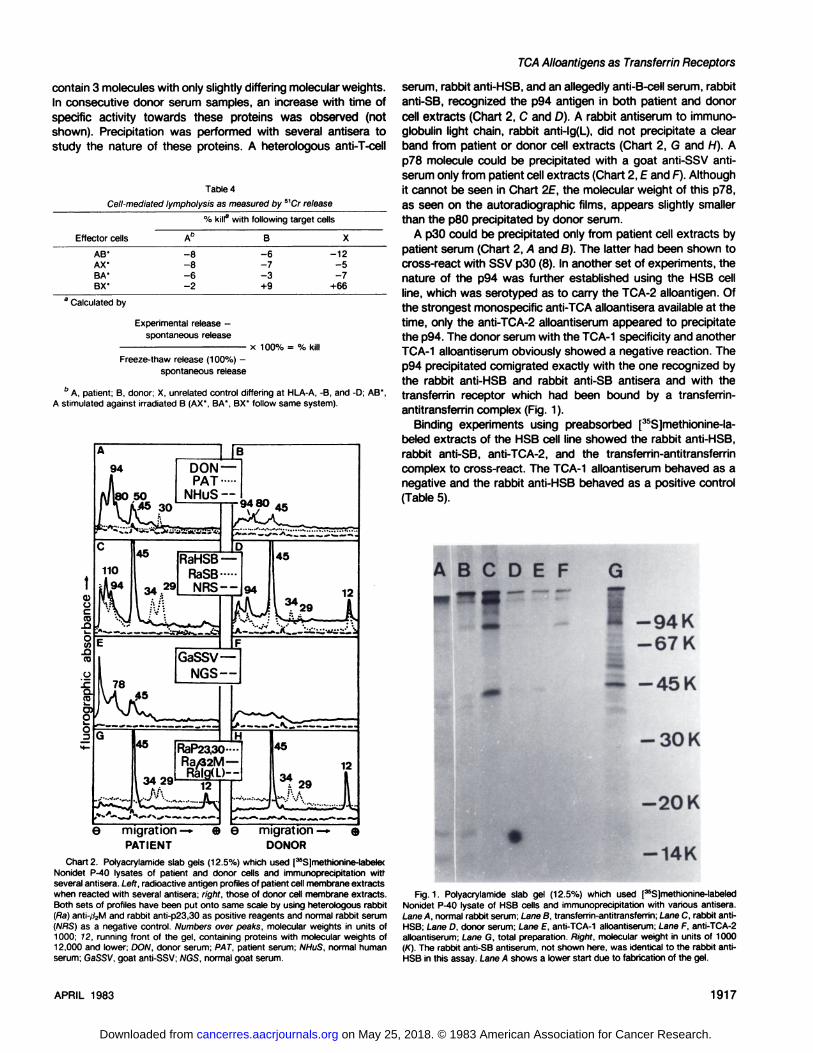
nature of the p94 was further established using the MSB cellline, which was serotyped as to carry the TCA-2 alloantigen. Ofthe strongest monospecific anti-TCA alloantisera available at thetime, only the anti-TCA-2 alloantiserum appeared to precipitatethe p94. The donor serum with the TCA-1 specificity and anotherTCA-1 alloantiserum obviously showed a negative reaction. The
p94 precipitated comigrated exactly with the one recognized bythe rabbit anti-HSB and rabbit anti-SB antisera and with thetransferrin receptor which had been bound by a transferrin-
antitransferrin complex (Fig. 1).Binding experiments using preabsorbed [35S]methionine-la-
beled extracts of the MSB cell line showed the rabbit anti-HSB,rabbit anti-SB, anti-TCA-2, and the transferrin-antitransferrincomplex to cross-react. The TCA-1 alloantiserum behaved as anegative and the rabbit anti-HSB behaved as a positive control
(Table 5).
A B C D E F G
J I -94K-67 K
45 K
-30 K
-20 K
-14K
Fig. 1. Polyacrylamide slab gel (12.5%) which used [35S]methionine-labeled
Nonidet P-40 lysate of MSB cells and immunoprecipitation with various antisera.Lane A, normal rabbit serum; Lane B, transferrin-antitransferrin; Lane C, rabbit anti-HSB; Lane D, donor serum; Lane E. anti-TCA-1 alloantiserum; Lane F. anti-TCA-2alloantiserum; Lane G, total preparation. Right, molecular weight in units of 1000(K). The rabbit anti-SB antiserum, not shown here, was identical to the rabbit anti-
HSB in this assay. Lane A shows a lower start due to fabrication of the gel.
APRIL 1983 1917
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

J. P. A. Derks et al.
Table 5Cross-reactivity measured by precipitation ol 3sS-labeled MSB antigenic extracts
Immunoprecipitation was performed by using Sepharose CL-4B-Protein A-boundIgG of 20 pi of various antisera and 100 */l of the antigenic extract. The antigenicextract was prepared as described previously (8), including preabsorption of theextract with Sepharose CL-4B-Protein A-bound IgG of 150 ¡Anormal rabbit serum.Sequential precipitations using Sepharose CL-4B-Protein A-bound IgG of 20 /jl ofeither normal rabbit serum or rabbit anti-HSB for preabsorption, and SepharoseCL-4B-Protein A-bound IgG of 10 j/l of various antisera in the second phase werethen performed without intervening freezing.
cpm |35S]methionine precipitated
after sera were preabsorbedwith
SeraRabbit
anti-HSBRabbitanti-SBAnti-TCA-1Anti-TCA-2Transferrin-antitransferrinNormal
rabbit serumNormal
rabbitserum7982652213412312059119Rabbit
anti-HSB127813059611019665
DISCUSSION
Identical State of the TCA Alloantigen to the TransferrinReceptor Described as T-Cell Antigen T9 (39, 42). This investigation was undertaken to study the T-cell allospecificity of both
sera from a chronic myeloid leukemia patient and an identicaltwin brother. Screening of the donor serum on randomly selectedhealthy donors indicated the presence of specific antibodies tothe alloantigen TCA-1, which is present mainly on the TG cells
and some of the T0 cells (44). This antigen is an alloantigen,since a polymorphism is detectable by testing various alloantiserain the TCP assay on enriched TG fractions (44), and the donorserum accordingly was reactive with only a part of the test panel(Table 1) and because donor serum activity was found to beincluded in that of a monoclonal anti-T-cell antibody R3/41-10,
showing allospecificity (36).By indirect immunofluorescence, it was shown that the donor
serum did not react with leukemic blasts but with only 5% of thepatient cells (Table 2). It is very likely that this fraction wasactually T-cells. The TCA alloantigen is identical to the transferrin
receptor because a molecule with identical molecular weight wasprecipitated by rabbit anti-HSB and rabbit anti-SB (Chart 2, Cand D; Fig. 1) and a transferrin-antitransferrin complex (Fig. 1),all of which were shown to cross-react with one another in a
binding assay using the MSB cell line (Table 5). The TCA alloantigen therewith is identical to the p95, described by Trowbridgeto react with rabbit anti-HSB and rabbit anti-SB (41) and alsoidentical to the T-cell antigen T9, reported by Terhorst ef al. (39),
which had been described as the transferrin receptor recently(38, 42).
The TCA specificity can also be detected in the ADCC assayon Con A-stimulated targets (Chart 1), which is a very sensitive
assay. Con A reportedly enhances TG expression (26), which inour experiments is seen in the high percentage of cells reactivein this assay with the undiluted donor serum (about 80%). Wehave as yet no experimental evidence as to the mechanism ofthis increase of TCA expression, but a similar increase of expression upon Con A stimulation is reported for the T9 antigen (39),which undoubtedly is related to the proliferative aspects of thetransferrin receptor.
The allelomorphism of the transferrin receptor may be relevantfor the eventual regulatory mechanism controlling cell prolifera
tion, which would be essential at least for those cells which aresupposed to play an immunological role like the TCA-positivecells which are mainly TGcells.
Our p94 is not equivalent to the tumor-associated cell surface
antigen p95, called CALLA, reported by Ritz ef al. (31), becausethe CALLA antigen does not occur on healthy human lymphocytes and because the antiserum recognizing our p94 wasderived from a healthy twin donor, who never had a transfusionand whose blood did not show any leukemic cells even yearsafter the patient's death.
Nature of the p80 Component in the Immunoprecipitates ofthe Donor Serum. As with T9 (42), we found coprecipitation ofa p80 molecule under certain conditions (Chart 2, A and B).When we used heteroantisera to precipitate the p94, we foundno coprecipitation of this p80 (Chart 2, C and D), which suggeststhat the heteroantisera might recognize a different epitope onthe p94, therewith prohibiting binding of the p80. According tothe suggestions of Trowbridge ef al. (42), p80 might be transferrin, which as a serum protein, however, was not expected tobecome metabolically radiolabeled. Here, we might have a firstindication that at least some of the leukocytes are capable ofsynthesizing transferrin. The HSB cell line as a homogeneouspopulation did not show any metabolically radiolabeled p80.
Nevertheless, some considerations concerning the nature ofp80 must be made. We cannot exclude that it is an idiotypic T-
cell receptor, because that could not be tested due to lack ofknowledge of the specific antigen that should be recognized.Idiotypic receptors have been shown to have a molecular weightof 70,000 (22). They occur on at least some tumor cells (18). Areceptor structure with a molecular weight of 70,000 and idiotypic to murine leukemia viruses has been shown in virus-
induced lymphomas (1). Thus far, we have excluded, however,that p80 is an idiotypic surface membrane IgM molecule byshowing that rabbit anti-IgM did not stain patient cells in indirectimmunofluorescence and that a rabbit antiserum to immunoglob-ulin light chain [rabbit anti-lg(L)] did not precipitate the p80
antigen (Chart 2, G and H). Furthermore, we have excluded thatp80 is idiotypic for viral p30, because donor serum is not antiidi-otypic to idiotypic anti-virus p30 patient antibodies (8).
We can exclude that p80 is an Fc receptor, since then it shouldalso have reacted with patient serum, but it failed to do so (Chart2, A and B).
Although a viral association of the patient's disease has been
substantiated (8) and although a p78 was recognized by a goatanti-SSV antiserum, which is close to p80 (Chart 2E), it is unlikely
that the p80 recognized by donor serum is of viral origin. Thearguments for this are: (a) although this is not clearly seen inChart 2, p78, precipitated by goat anti-SSV, was clearly distin
guishable on the gel from the p80, precipitated by donor serum.We do not think that the small difference in molecular weightwas caused by artifacts, because the experimental conditions ofprecipitation were identical and there was no overloading of thegel by serum immunoglobulin whatsoever; (b) we were able toprecipitate p80 from patient as well as from healthy donor cellextracts, using donor serum (Chart 2, A and B), whereas p78,which might be the equivalent of viral gp70, could be precipitatedonly from patient cell extracts, using goat anti-SSV (Chart 2, £
and F); (c) Snyder and Fleissner (35) and Barbacid ef al. (2),resolving conflicting evidence reported earlier by several authors,recently reported that human sera do not recognize viral gp70produced in human cells; (d) if the donor really had been sensi-
1918 CANCER RESEARCH VOL. 43
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

TCA Alloantigens as Transieran Receptors
tized towards viral gp70, one would have expected not only theblastogenic T-cell response of the donor against patient cells
that we found (Table 3) but also a strong cytotoxic cellularresponse (23). This cytotoxic response, however, could not bedemonstrated (Table 4), a finding which is in line with those ofZier ef a/. (48).
Possible Involvement of TCA and TCB Loci in the Processof Immunoregulation. Our evidence for a viral association withthe disease pattern of the particular patient under study is ofinterest. SSV p30-cross-reacting p30 proteins were actively syn
thesized in patient cells (8). A p30 could also be precipitated bypatient serum from autologous cell extracts (Chart 2A). In addition, patient serum was shown to contain anti-TCB and anti-B
cell activity to all randomly selected healthy individuals testedthus far (Table 1). The determinants recognized are mono-
morphic, assuming that these serum activities are antibody mediated. The indirect fluorescence assay of patient serum on donorcells shows that at least part of the activity is indeed antibodymediated (Table 2). The aspecific anti-B-cell activity, however,
may also result from cytostatic drugs in patient serum that wastaken on October 13, 1978 (see "Case History"), because no
la-like proteins could be precipitated with patient serum, because
the percentage of donor cells reactive with the patient serum inthe indirect fluorescence assay is lower than that in the TCPassay (Table 2), and finally because the cytotoxic anti-B-cell
effect appeared to be not absorbable by a pool of lymphocytes.Considering the differential in vivo synthesis of T-cell-specific
alloantibodies in this monozygotic twin couple and the cell prolif-
erative aspects of the transferrin receptor (42), which is identicalto the TCA alloantigen, and finally assuming that TCA and TCBare somehow markers for the allegedly immunoregulatory TGand TM subsets of T-cells (19, 25, 44), showing a disease
association (20), the antibodies found in the patient and donorsera may be involved in the regulation of the immune responseto an infectious agent associated with the patient's disease. The
finding of Gallery ef a/. (6) that chronic lymphocytic leukemiapatients showed a deficiency in functional T-cells, probably helperT-cells, is in line with ours. The high concentration of p94 in the
extracts of patient leukocyte membranes is suggestive for thepresence of a metabolically very active TCA-positive cell, whichis a T-cell probably involved in the process of immunosuppres-
sion.Assuming that the immune system is involved in the defense
mechanism against leukemia, it may be reasonable to suggestthat transplantation with bone marrow from an isologous immu-
nocompetent donor should be performed in a stage of thedisease early enough to counterbalance an eventual viral or otherinfectious pressure, by immunocompetent cells and immunoregulatory anti-T-cell antibodies. It may be of interest that none of
the 4 chronic myeloid leukemia patients transplanted with isologous BM in the chronic and not in the blast phase of the diseasehas relapsed thus far (13).
ACKNOWLEDGMENTS
We gratefully thank Dr. S. O. Warnaar and Dr. P. Herbrink, Department ofPathology, for providing the viral antisera; Dr. F. Zwaan. Department of Haematol-ogy. for providing patient material and the case history; R. P. Schuitemaker fordonating so much blood; A. Naipal. Department of Haematology, for performingthe ADCC assay; Dr. P. L. Pearson, Department of Human Genetics, and Dr. A.van Leeuwen and Dr. J. J. van Rood, Department of Haematology, for reading themanuscript; and in particular the latter for establishing the essential contacts andfor stimulating discussions. All departments are located in Leiden. Further, we
thank Dr. H. G. van Eijk. Department of Chemical Pathology. Erasmus University,Rotterdam. The Netherlands, for providing the transferrin and antitransferrin.
REFERENCES
1. Baird. S. M. Antigenic properties and molecular weights of murine leukemiavirus-binding proteins. J. Immunol.. 122: 1389-1396, 1979.
2. Barbacid. M.. Bolognesi. D., and Aaronson. S. A. Humans have antibodiescapable of recognizing oncoviral proteins: demonstration that these antibodiesare formed in response to cellular modification of glycoproteins rather than asconsequence of exposure to virus. Proc Nati. Acad. Sei. U. S. A., 77: 1617-
1621, 1980.3. Barnes. D. W. H., and Loutit, J. F. Letter to the editor: acute graft-versus-host
disease in recipients of bone-marrow transplants from identical twin donors.Lancet, 1: 905-906, 1979.
4. Bruning. J. W.. Kardol, M. J.. and Arentzen. R. Carboxyfluorescein fluorochro-masia assays. I. Non-radioactively labeled cell mediated lympholysis. J. Immunol. Methods. 33: 33-44. 1980.
5. Callahan, G. N., Pellegrino, M. A., McCabe, R. P., Frugis. L., Allison, J. P., andFerrane. S. Histocompatibility antigens on tumor cells: spatial and structuralrelationship with tumor associated antigens. Behring Inst. Mitt., 62: 115-128,1978.
6. Gallery. R. T.. Strelkauskas, A. J., Yanovich. S., Marks, S.. Rosenthal. D., andSchlossman, S. F. Functional abnormalities associated with T-lymphocytesfrom patients with chronic lymphocytic leukemia. Clin. Immunol. Immuno-pathol., 77:451-458, 1980.
7. Claas, F. H. J., van Rood. J. J.. Warren. R. P., Weiden. P. L., Su. P. J., andStorb, R. The detection of non-HLA antibodies and their possible role in bonemarrow graft rejection. Transplant. Proc.. 11: 423-426. 1979.
8. Derks, J. P. A.. Hofmans, L.. Bruning, J. W.. and van Rood, J. J. Synthesis ofa viral protein with molecular weight of 30.000 (p30) by leukemic cells andantibodies cross-reacting with simian sarcoma virus p30 in serum of a chronicmyeloid leukemia patient. Cancer Res.. 42: 681-686. 1982.
9. de Rooij-Doyer, E., Bruning. J. W., and van Rood, J. J. Inhibition of respondercell activity in mixed leukocyte culture reactions. Tissue Antigens, 18: 154-166. 1981
10. Dicke. K. A.. Spitzer. G.. Peters. L.. McCredie. K. B.. Zander, A., Verma. D.S., Vellekoop, L., and Hester. J. Autologous bone marrow transplantation inrelapsed adult leukemia. Lancet 7: 514-517. 1979.
11. Doherty. P. C., and Zinkernagel, R. M. A biological role for the major histocom-patibility antigens. Lancet, 1: 1406-1409. 1975.
12. Dupont, B.. O'Reilly, R. J., Pollack, M. S., and Good, R. A. Use of HLA-
genotypically different donors in bone marrow transplantation. Transplant.Proc.. 11: 219-224, 1979.
13. Fefer, A., Cheever, M A., Thomas, E.. Boyd. C . Ramberg, R.. Glucksberg.H., Buckner, C. D., and Storb, R. Disappearance of Ph'-positive cells in four
patients with chronic granulocytic leukemia after chemotherapy, irradiation andmarrow transplantation from an identical twin. N. Engl. J. Med., 300: 300-
333, 1979.14. Ferrara. G. B. Identification of new cell surface markers in man: the problem
of ¡mmunogenicity. Transplant. Proc., 11: 715-718. 1979.15. Ferrarini. M.. Moretta, L., Abrile, R., and Durante. M. L.. Receptors for IgG
molecules on human lymphocytes forming spontaneous rosettes with sheepred cells. Eur. J. Immunol.. 5: 70-72. 1975.
16. Festenstein. H., Schmidt. W., Testorelli. C.. De Giorgi, L.. Morelli. O.. Matos-sian-Rogers. A., and Atfield, G. Immunogenetic and immunochemical studiesof H-2 antigens of foreign haplotypes on tumour cells. J. Immunogenet. (Oxf),6:263-270. 1979.
17. Goulmy. E.. Termijtelen. A., Bradley. B. A., and van Rood. J. J. HLA-restrictionof non-HLA-A, -B and -D cell mediated lympholysis (CML). Tissue Antigens. 8:317-326. 1976.
18. Haughton, G.. Lanier, L. L.. Babcock, G. F., and Lynes. M. A. Antigen-inducedmurine B cell lymphomas. II. Exploitation of the surface idiotype as tumorspecific antigen. J. Immunol., 727: 2358-2362. 1978.
19. Herbrink, P.. Moen. J. E. T., Brouwer, J., and Warnaar, S. O. Detection ofantibodies cross-reactive with type C RNA tumor viral p30 protein in humansera and exúdate fluids. Cancer Res., 40: 166-173,1980.
20. Huddlestone. J. R., and Oldstone, M. B. A. T suppressor (T9) lymphocytesfluctuate in parallel with changes in the clinical course of patients with multiplesclerosis. J. Immunol., 723: 1615-1618.1979.
21. Keuning. J. J.. Termijtelen, A., Blussévan Oud Alblas, A., Gabb, B., D'Amaro,
J.. and van Rood. J. J. LD (MLC) population and family studies in a Dutchpopulation. In: Kissmeyer (ed.), Hisotcompatibility Testing 1976. pp. 533-543.Copenhagen: Munksgaard A/S, 1976.
22. Lea, T.. Forre. O. T.. Michaelsen, T. E.,and Natvig. J. B. Shared idiotypes onhuman peripheral blood B and T lymphocytes. J. Immunol., 722: 2413-2417,1979.
23. Lee, J. C., and Ihle, J. N. Characterization of the blastogenic and cytotoxicresponses of normal mice to ecotropic C-type viral gp71. J. Immunol., 778:928-934, 1977.
24. Mittal. K. K.. Mickey. M. R., Singal, D. P.. and Teresaki. P. l. Serotyping forhomotransplantation. XVIII. Refinement of microdroplet lymphocyte cytotox-
APRIL 1983 1919
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

J. P. A. Derks et al.
¡citytest. Transplantation (Baltimore), 6: 913-927, 1968.
25. Moretta, L., Ferrarini, M., Durante, M. L., and Mingari, M. C. Expression of areceptor for IgM by human T-cells in vitro. Eur. J. Immunol., 5: 565-569,1975.
26. Moretta, L., Ferrarini, M., Mingari, M. C., Moretta, A., and Webb, S. R.Subpopulations of human T cells identified by receptors for immunoglobulinsand mitogen responsiveness. J. Immunol., 777: 2171-2174, 1976.
27. Moretta, L., Mingari, M. C., Moretta, A., and Cooper, M. D. Human T-lymphocyte subpopulations: studies of the mechanism by which T-cells bearingFc-receptors for IgG suppress T-dependent B-cell differentiation induced bypokeweed mitogen. J. Immunol., 722: 984-990,1979.
28. Omary, M. B., Trowbridge, I. S., and Minowada, J. Human cell surfaceglycoprotein with unusual properties. Nature (Lond.), 286: 888-891, 1980.
29. Pratt, D. M., Schlossman, S. F., and Strominger, J. L. Human T-lymphocytesurface antigens: partial purification and characterization utilizing a high titreheteroantiserum. J. Immunol., 724: 1449-1461,1980.
30. Rappeport, J., Reinherz, E., Mihmn, M., Lopansri, S., and Parkman, R. Acutegraft-versus-host disease in recipients of bone-marrow transplants from identical twin donors. Lancet, 7: 717-720,1979.
31. Ritz, J.. Pesando, J., Notis-McConarty, J., Lazarus, H. L., and Schlossman, S.F. A monoclonal antibody to human acute lymphoblastic leukemia antigen.Nature (Lond.), 283: 583-585, 1980.
32. Robinson, P. J., and Schirrmacher, V. Differences in the expression of histo-compatibility antigens on mouse lymphocytes and tumor cells: immunochemi-cal studies. Eur. J. Immunol., 9: 61-66, 1979.
33. Russell, J. H., Ginns, L. C., Terres, G., and Eisen, H. N. Tumor antigens asinappropriately expressed normal alloantigens. J. Immunol., 722: 912-919,
1979.34. Santos, G. W., Elfenbein, G. J., and Tutschka, P. J. Bone marrow transplan
tation, present status. Transplant. Proc., 77: 182-188, 1979.35. Snyder, H. W., Jr., and Fleissner, E. Specificity of human antibodies to
oncovirus glycoproteins: recognition of antigen by natural antibodies directedagainst carbohydrate structures. Proc. Nati. Acad. Sei. U. S. A., 77: 1622-
1626. 1980.36. Spitz, M., Fainbain, L., and van Leeuwen, A. A new genetic marker of human
T-lymphoid cells detected by a xenogeneic monoclonal antibody. J. Immuno-genet., (Oxf.), 7: 307-313, 1980.
37. Springer, T. A., Kaufman, J. F., Giphart, M. J., Man, D. L., Terhorst, C., andStrominger, J. L. Origins of lymphocyte diversity. Cold Spring Harbor Symp.
Quant. Biol., 41: 387-396, 1976.38. Sutherland, R., Delia, D., Schneider, C., Newman, R., Kemshead, J., and
Greaves, M. Ubiquitous cell-surface glycoprotein on tumor cells is proliferationassociated receptor for transferrin. Proc. Nati. Acad. Sei. U. S. A., 78: 4515-4519, 1981.
39. Terhorst, C., van Agthoven, A., LeClair, K., Snow, P.. Reinherz, E., andSchlossman, S. Biochemical studies of the human thymocyte cell-surfaceantigens T6, T9 and T10. Cell, 23: 771-780, 1981.
40. Thomas, E. D., Buckner, C. D., Banaji, M., ¿lift,R. A., Fefer, A., Flournoy, N.,Goodell, B. W., Hickman, R. O., Lerner, K. G., Neiman, P. E., Sale, G. E.,Sanders, J. E., Singer, J., Stevens, M., Storb, R., and Weiden, P. L. Onehundred patients with acute leukemia, treated by chemotherapy, total bodyirradiation, and allogeneic bone marrow transplantation. Blood, 49: 511-533,1977.
41. Trowbridge, I. S., Hyman, R., and Mazauskas, C. Surface molecules of culturedhuman lymphoid cells. Eur. J. Immunol., 6: 777-782, 1976.
42. Trowbridge, I. S.. and Omary, M. B. Human cell surface glycoprotein relatedto cell proliferation is the receptor for transferrin. Proc. Nati. Acad. Sei U SA., 78:3039-3043, 1981.
43. van Leeuwen, A. Alloantibodies that react with subsets of human T cells.Tissue Antigens, 74: 437-443, 1979.
44. van Leeuwen, A., Festenstein, H., and van Rood, J. J. Di-allelic alloantigenicsystems on subsets of T-cells. Human Immunol., 4: 109-121, 1982.
45. van Leeuwen, A., Schuit, H. R. E., and van Rood, J. J. Typing for MLC. II. Theselection of non stimulator cells by MLC inhibition tests using SD identicalstimulator cells (MISIS) and fluorescent antibody studies. Transplant Proc 5-1539-1542.1973.
46. van Rood, J. J., van Leeuwen, A., Goulmy, E., Termijtelen, A., Bradley, B. A.,Brand, A., and Eernisse, J. C. The importance of non-HLA-systems and thefeasibility of the use of unrelated donors in bone marrow transplantation.Transplant. Proc., 77: 47-51, 1978.
47. van Rood, J. J., van Leeuwen, A., and Ploem, J. S. Simultaneous detection oftwo cell populations by two colour fluorescence and application of the recognition of B-cell determinants. Nature (Lond.), 262: 795-797, 1976.
48 Zier, K. S., Huber, C., Albert, E., and Braunsteiner, H. Cell mediated immuneresponses between HLA-identical siblings: recognition of antigenic changesassociated with acute myelogenous leukaemia. Clin. Exp. Immunol., 40: 136-146,1980.
1920 CANCER RESEARCH VOL. 43
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1983;43:1914-1920. Cancer Res Jos P. A. Derks, Lilian Hofmans, Hans W. Bruning, et al. Serum from a Monozygotic Twin BrotherTransferrin Receptor on T-Cells of a Leukemic Patient with Molecular Identification of the TCA Alloantigen as the
Updated version
http://cancerres.aacrjournals.org/content/43/4/1914
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/43/4/1914To request permission to re-use all or part of this article, use this link
on May 25, 2018. © 1983 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from