mohd s case presenation
TRANSCRIPT

Case presentation
Mohammed Al Sakiti

Outlines
• Case presentation
• Discussion
31 Y F referred from privet clinic to neuro OPD with 3 weeks h/o episodes of headache.
• OPD was closed
• Pain score 3/10
• BP 140/80 mmHg, PR 87/min , Spo2 100% in room air , T 36.7 c
• Triage staff ??

History H.A 31 Y Omani F K/D/O HTN on medications,
3/3/2009 Bell’s palsy.
She presented to the ED with 3 weeks H/O frequent episodes of sever throbbing left sided mainly occipital headache associated with blurred vision , reduced visual acuity , photophobia and redness with excessive tearing of the left eye. Disturbing her sleep.
History
No history of fever, nausea , vomiting.
Systematic review was unremarkable.
She denies family history of chronic headache.
.She is a bank cashier, married with two children .No history of travel .she is on OCP.
Examination
• Pain score 3/10
• BP 140/80 mmHg, PR 87/min , Spo2 100% in room air , T 36.7 c
• General examination unremarkable
• GCS 15/15
• Fundoscopy.
• No other neurological deficit could be detected in neurological examination.

Rt & Lt eye
DD

Invx




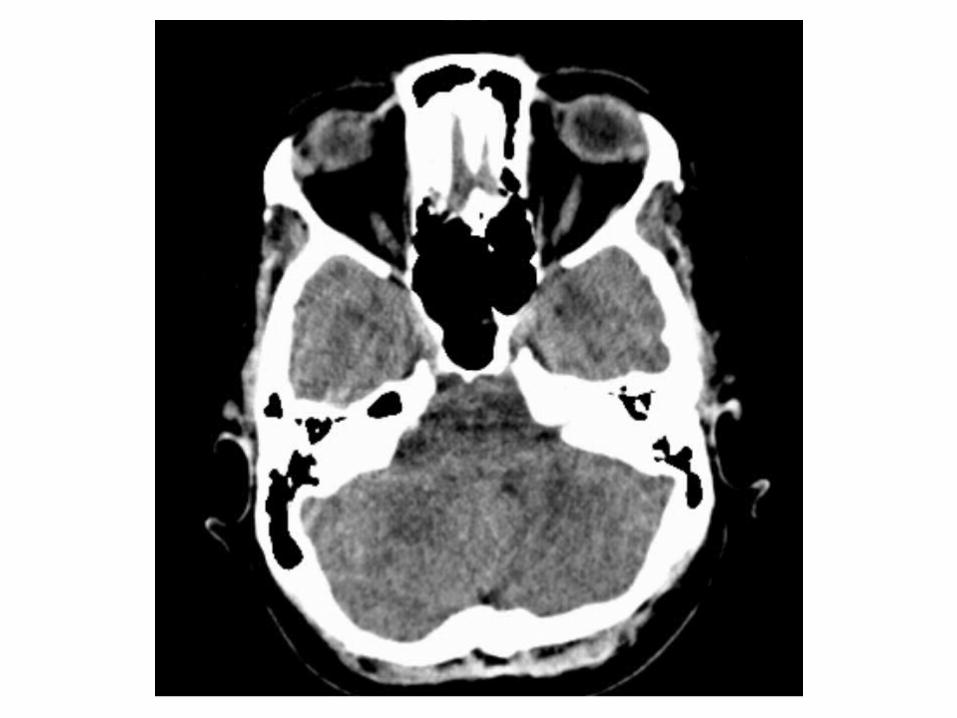

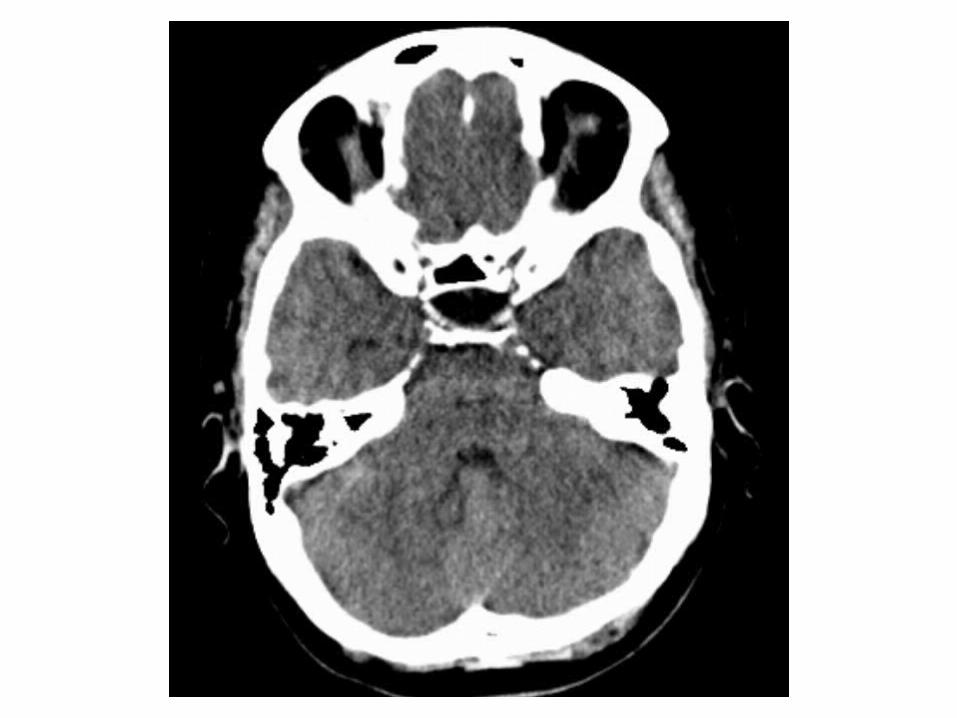
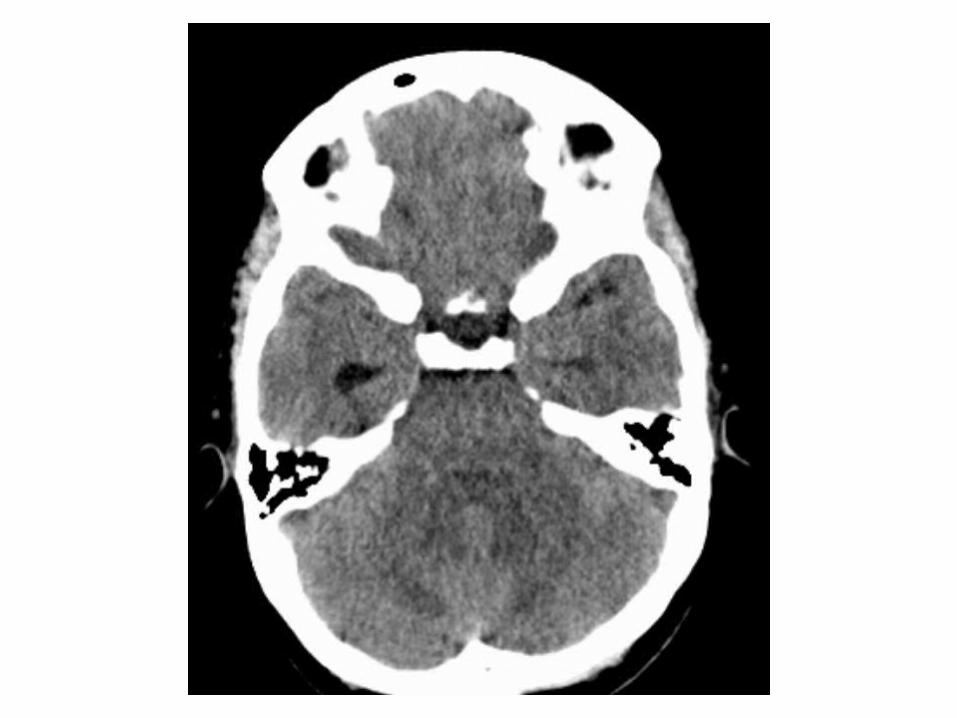



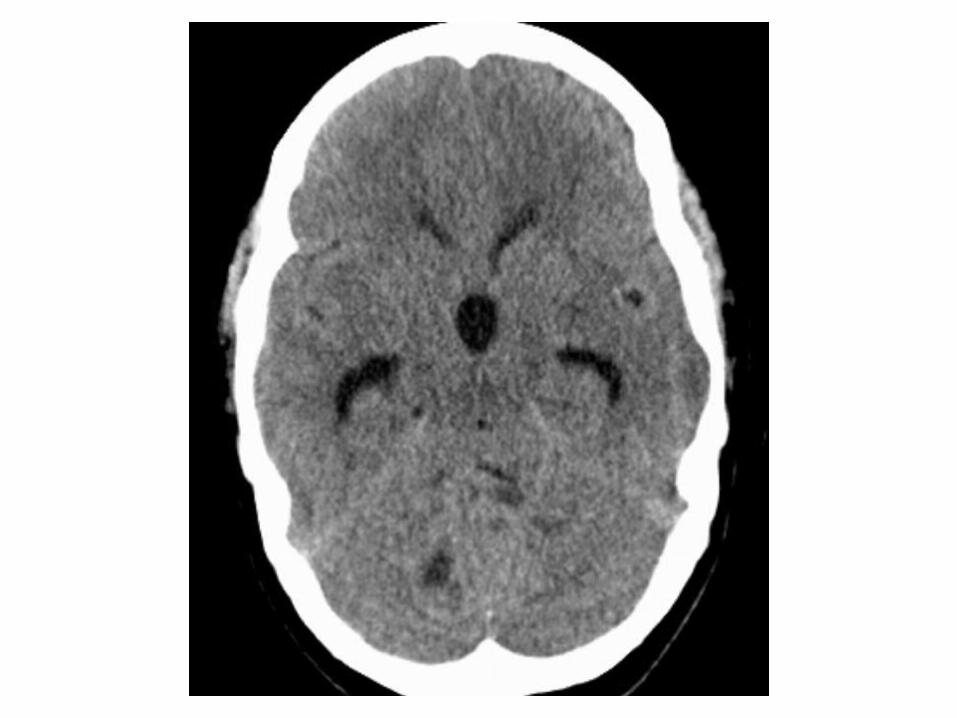
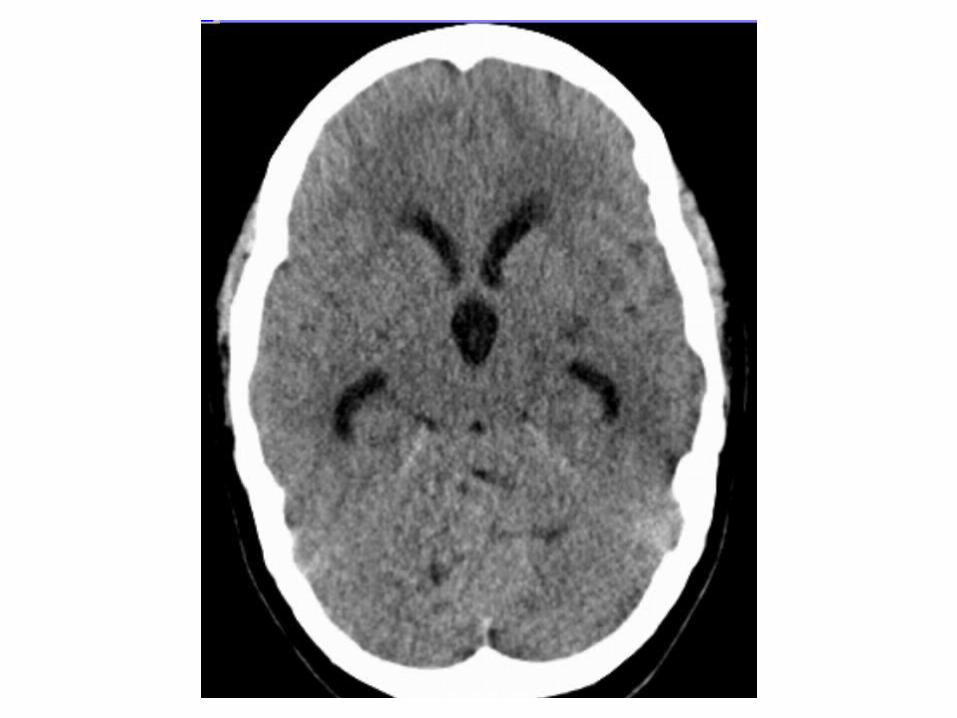


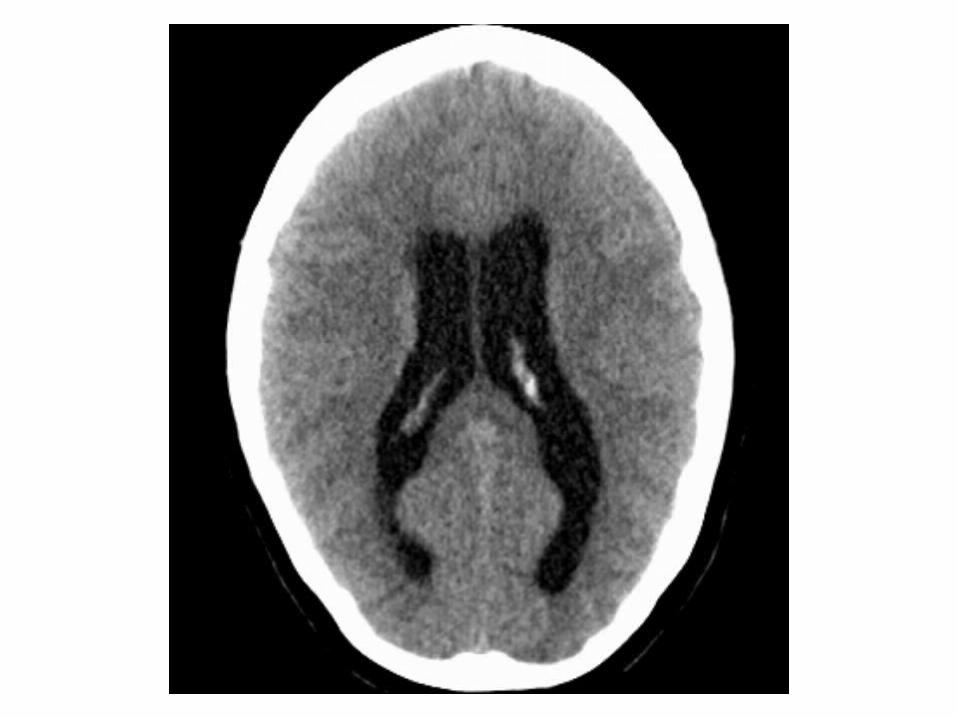

CT with out contrast
• 3 cm hyperdense mass in the midline cerebellum with focal oval shaped cystic area.
• Mass effect on 4th ventricle resulting in acute obstructive hydrocephalous.
• DD : cystic medulloblastoma , density astrocytoma.
MRI


Disposition
• Neurosurgery KH .

Principles of Disease
“Headache is the most common
presenting complaint with brain tumor, being reported by approximately 50% of the patients.”
Forsyth PA, Posner JB: Headaches in patients with brain tumors: A study of 111 patients. Neurology 1993; 43:1678.
“The pain patterns produced are highly variable, depending on the location of the mass and the structures involved”
Newman LC, Lipton RB: Emergency department evaluation of headache. Neurol Clin 1998; 16:285

Clinical Presentation
The classic triad of brain tumor headache: sleep disturbances, severe pain, and nausea and vomiting—is seen in only one third of patients
Patchell RA, Posner JB: Neurologic complications of systemic cancer. Neurol Clin 1985; 3:729.

Diagnostic Evaluation
• Contrast enhancement on CT often improves the identification of the underlying mass lesion
• MRI

Treatment
• urgent referral to neurosurgery • acute complications: symptoms suggestive of increased
ICP →10 mg IV, followed by 4 mg every 6hs. seizures → anticonvulsant therapy
Empirical or prophylactic treatment .
Newton HB, et al: Clinical presentation, diagnosis, and pharmacotherapy of patients with primary brain tumors. Ann Pharmacother 1999; 33:816.

Thank you