module 5 osce - uea · pdf filemodule 5 osce document ... questions about your past medical...
TRANSCRIPT

JoshuaChambers
Module5OSCEdocumentConsultationskills:Informationaboutthestation:
• 11-minutestation• Introduction• SSSICERAV–Signpost,summariseandscreen• Ideas,concernsandexpectations• Recognise,acknowledge,validate• HAVEASTRUCTURE!• Havesomekeyphrasesasbackups!
Introduction:• Washhands• Introduce• Highmynameis______.I'ma______medicalstudentfromtheUEA.AndI'vebeen
totalktoyoutodayisthatokay?• NameandDOB• Explainstructure• ‘Thisconsultationwilljustinvolvemeaskingaboutyoursymptomsandthenafew
questionsaboutyourpastmedicalhistory,lifestyleandanymedicationsthatyou’reon,doesthatsoundokay?’
• Areyoucomfortableformetobegin?• Openquestion:‘sowhathasbroughtyouintoday?’
Presentingcomplaint:• Cough-duration,severity,timeoftheday• Wheeze–(askthepatienttoclarifywhattheymeanbywheeze)• Sputum–colour,consistency,volume• Haemoptysis–howmuch,howoften?• Breathlessness–timing,exacerbatingandrelivingfactors,EXERCISETOLERANCE.• Chestpain–SOCRATES
SAWTEM:• “JusttocheckthatIhaven’tmissedanything,I’mjustgoingtoaskyousomegeneral
questionsaboutyourhealth”• AskaboutOrtho/Rhemoquestion:“Haveyougoanyachesorpainsinyour
joints?”PMHx:
• Openquestionaboutanyothermedicalcondition• Askabout:• Atopy• Asthma• Childhoodinfections
FHx:• Anyconditionswhichruninthefamily?• ‘specificallyanylungconditionswhichruninthefamily’• ‘Justaquestionweaskeveryoneisthereahistoryoflungcancer?’

JoshuaChambers
SHx:• Smoking
o 1packyear=20cigaretteso Howmany?o Forhowlong
• Alcoholo Amounto “Whatisyourdrinkofchoice?”
• Occupationo exposuretoasbestoso zookeepero coalminers
• House/Livingarrangementso House/bungalowo Aloneorwithfamily/supporto Adjustmentsathomeo Okaywithstairs?
• Petso chlamydiapsittacio allergenso birdfancierslung
• Anyforeigntravel?o PE/DVT/TB
• Anyuseofrecreationaldrugs• IMPACTONQOL-GOODTORAV
DHx:• ALLERGIES• Iftime,askaboutOTCandherbal• Inhalers?–whatcolour?Howdotheytakeit?• Bronchoconstriction:betablockers,opioids,NSAIDs• DrycoughwithACEinhibitors• Lungfibrosis/parenchymaldiseasewithcytotoxics,DMARDs• ThePILL?–iffemale(DVT/PE)• Amiodaroneandnitrofurantoin(pleuraleffusion,fibrosis)
Commonconditionsthatcouldcomeup?• Asthma• COPDandwithexacerbation• Pneumonia• PE• Lungcancer• Bronchiectasis• Pneumothorax
Respiratoryexamination:Introduction:

JoshuaChambers
• WASHHANDS• Introduceyourself• ConfirmpatientsnameandDOB• ‘I'vebeenaskedbythedoctortodoarespiratoryexaminationonyoutodayisthat
okay?Thisexaminationwillconsistofmehavingageneralinspection,thenhavingalookatyourhandsmouthandchestandthenhavingalistentoyourchest.Isthatokay?’
• Askthepatienttoadequatelyexposethemselves• Positionthepatientat45degrees
Inspection:JVP(Increasedheightorwaveform)/APEXBEAT/oralcandsis/legsperipheraloedema/Practiseeverything/cricosternaldistance/FLAPPINGTREMMOR/havinganydifficultieswithbreathing?Infectioninmouth/CommentonrespiratoryGeneralexamination:
• Commentonthegeneralwell-beingofthepatientandthepresenceofanyaidsaroundthebedsidee.g“oxygen,sputumpots,inhalers”
• Isthispatientinrespiratorydistress?canthepttalkinfullsentences?
• Symptomsofrespiratorydistress:“There’sno…”• nasalflaring,mouthbreathing,subcostal/intercostalmusclerecession,usesof
accessorymuscles(trapeziusandsternocleidomastoid)Hands:
• Lookingatthehandsforanyclubbing,tarstaining,cyanosisandatremor• Cockthewristsback–lookforCO2retentiontremor• Checkpulseandresprate
o Normalrespiratoryrate-12-20o Tachyponoea-greaterthan20o Bradyponoea-lessthan12
• Offertotakeabloodpressure• ‘ifIhadmoretimeIwouldideallytakeabloodpressure’
Eyes:• CouldIjustpulltheskinofyoureyedown?• Anaemia• Jaundice
Mouth:• Oralcandidiasis,centralcyanosis• Pursedlipbreathing
Neck:• Isthetracheacentral?• Cricosternaldistance(3-4fingers)
• Cricosternaldistancejugularnotchtocricoid–ifobstructivelungdiseasethedistancewillbesmallerifhyperinflationispresent3fingerdistance
• JVPandhepatojugularreflux• Askforabdopain–lookupforthis• Lookawayat45degrees

JoshuaChambers
• PressdownonstomachLymphNodes:
• Submental,submandibular,preauricular,postauricular,occipital,anteriorandposteriorcervicalchainandsupraclaviclar
Legs:
• Bilateraloedema–corpulmonale• Unilateraloedema–DVT
Inspection:CHEST:• ‘lookingatthechestanteriorlyandposteriorforanyscars,swelling(sternotomyand
thoracotomy),deformities(e,gpectusexcavatumorpectuscarinatum,kyphosisorscoliosis)’
• Chestwalldeformitieso Pectusexcavatum-sternumisdepressedinrelationtotheribs,o Pectuscarinatum-sternumismoreprominenttotheribso Barrelchest–emphysema/COPD
Palpation:Chestexpansion:
• Anteriorposteriordirection-placebothhandsonthepectoralregionandaskthepatienttotakeadeepbreath-chestshouldexpandsymmetrically
• Laterally-gripthechestbetweenbothhandsandaskthepatienttotakeadeepbreathwhilstobservingmovementofthethumbs
Apexbeat:• shouldbeinthe5thintercostalspaceatthemidclavicularline

JoshuaChambers
• Displacementoftheapexusuallysuggestcardiomegalybutrespiratoryconditionswhichmaycausetheapextobecomedisplacedinclude:Pulmonaryfibrosis,bronchiectasis,pleuraleffusions,pneumothoraxes
Percussion:• Clavicle,midclavicularline,betweentheribs• 4anterioallyand2laterallyEACH
Auscultation:• Askthepatienttobreathinandout–listen4anteriorandposteriorand2laterally
(Midaxillary)FOREACHside.• Listenfordiminishedbreathsounds• Bronchialbreathing• Addedsoundssuchaswheezes,stridororcrackles,orpleuralrubs
Vocalresonance:• Askthepatienttosay99• Increasedinfibrosis,consolidation,collapse
Summary:• Onexaminationofthispatient..• Oninspection..• Onpalpation…• Onauscultation• Clearvesicularbreathsounds• IfIhadmoretimeIwould:
o Doafullcardiovascularexamo LookatCXRo Dothefront/backo BedsidePeakflowo Lookatobschart
Commonconditionsyoumightget:• Chestwalldeformity
o kyphoscoliosis,pectusexcavatum• Post-surgerywithobviousthoracotomyscar• Bronchialbreathingispresentabovetheoedema(Becausethelunghasclumped
together)
SummaryofexaminationfindingsanddiseaseBreathsounds Indicates
Normalvesicularbreathing NormallungsBronchialbreathing Thisisfoundwherelungtissueisreplacedbyuniformlyconducting
tissue.Thisincludes:ConsolidationFibrosisCollapse(withpatentbronchus)
Absentbreathsounds PEPulmonaryeffusionPneumothorax

JoshuaChambers
Whisperingpectoriloquy ConsolidationCollapsewithpatentbronchus
Vocalresonance Consolidation–increasedPE–decreasedPulmonaryeffusion–decreasedPneumothorax–decreased
Crackles Fine–PulmonaryfibrosisandheartfailureCourse–infectionandbronchiectasis
Wheeze AsthmaCOPD
Pleuralrub Inflamedpleura,infection,PE,fracture
ConditionsrelatingtotheirexaminationfindingsCondition General Face/neck Inspection Palpation Percussion AuscultationPneumonia SOB,
fever,tachycardia,cyanosisandhypotension
Flushedorpale
Tachypneic,laboured,reducedexpansion
Tracheanormal
Dull CoursecrackleswithbronchialbreathingandVRandWPincreased.?PleuralrubProminent,mostly,inlowerlobes.
Pleuraleffusion Accessorymuscles,labouredbreathing,looksill
Reducedonside
Tracheaawayiflarge
Stonydull Absentbreathsounds.?Bronchialattopofeffusion.VRreduced
Pneumothorax SOB,pain
?Surgicalemphysema
Reducedexpansiononthatside
Trachealdeviationopposite
Hyper-resonant
Absentornobreathsounds,VRdecreased
Collapse SOB,Tachycardia
Reducedexpansion
Tracheatowardsiflarge
Dull Absentorreduced.?Crackesorwheeze.VFdecreased
ILD ClubbingCyanosis
Clubbing Reducedexpansion
Tracheanormal
Normal Finecrackles?Bronchialbreathing
COPD SOB,oxygen
Accessorymuscles,cyanosisWtloss
Barrelchest Tracheanormal
Normal,hyperresonant
Reducedairentry,(polyphonic)wheeze
Asthma ?SOB Labouredbreathing,shortsentences,accessorymuscles
Hyper-inflationofchest
Tracheanormal
Normal Wheeze

JoshuaChambers
PulmonaryEmbolism
Inpain,cyanosis
SOB,pleuriticpain,signsofDVT,raisedJVP
SOB Normal Normal Absentorreducedbreathingandpleuralrub
Bronchiectasis Reducedexpansion
Reducedpercussion
ReducedairentryCrackleswhichchangewithcoughing
PercussionnoteType Detectedover
Resonant NormallungHyperresonant PneumothoraxDull Pulmonaryconsolidation
PulmonarycollapseSeverepulmonaryfibrosis
Stonydull(Anythingliquid) PleuraleffusionHemothorax
CausesofdiminishedvesicularbreathingReducedconduction
ObesityPluraleffusionorthickeningPneumothorax
ReducedairflowGeneralised.COPDLocalised.Collapsedlungduetooccludinglungcancer
CausesofcracklesPhaseofinspiration Cause
Early Smallairwaydisease,bronchiolitisMiddle PulmonaryoedemaLate Pulmonaryfibrosis(Fine)
Pulmonaryoedema(Medium)BronchialsecretionsinCOPD,pneumonia,lungabscess,tubercularlungcavities(coarse)
Biphasic Bronchiectasis(Also,pulmonaryoedema,ILD,PF,COPD,Pneumonia)
CausesofbronchialbreathsoundsCommon

JoshuaChambers
Lungconsolidation(Pneumonia)Uncommon
LocalisedpulmonaryfibrosisPleuraleffusionCollapsedlungwheretheunderlyingmajorbronchussoundsareobvious(Oftenpartialcollapse)
Spirometryprocedureandinterpretation:• GooverPFTquizlet• Gooverthepaperdocumentinfolderwiththison
Whatismeasured?• Totalvolumeofairforciblyexpiredafterafullinspiration.(FVC)• Volumeofairthepatientisabletoexpireinthefirstsecondofaforcedexpiration.
(FEV1)• FEV1/FVCratioexpressedasapercentage• Maximumflowachievedfromaforcedexpiration.(PEF)
Indications:
• Abnormalitypresent?• Assessmentofseverity• Serialmeasurements• OccupationalMedicineorEpidemiologicalstudies• Research
Normalvaluesdependupon:
• Age• Sex• Height• Ethnicorigin
Limitationstoflowvolumeloop
• Notspecific• Sensitivity
Whattocheckbeforewedospirometrywithpatients:
• Height,sex,age• Inhalers,whendidyoulastusethem• Shouldn’tbedoingitonpeoplewhohavehadanMIinthepastweek• Thoracicsurgeryinthepast12weeks• Haven’thadapneumothoraxinthepast2weeks• ‘Haveyoubeenaninpatient’• ‘Haveyouhadanyoperationsinthepastfewmonths?’• Otherconditions• Smoker?

JoshuaChambers
• ExplainthenatureandpurposeofthetestMeasurements:
• RVC’s(Relaxedvitalcapacity)–x3• FEV1/FCV–3withgoodtechnique
o 2withina100mlofeachotherBadtechnique:
• Co-ordination• Noleakage• Nocoughing• Nottakingfullbreathin• Gentle–givingaslowblow(misdiagnosedfalsepositiveslookslikeCOPD)• Earlytermination(Lessthan6sec)underestimateFVC,sofalsenegatives
FEV1%predicted:• >80mild• 50-79moderate• 30-49severe• <30verysevere
Obstruction:• ‘Scooping’onthegraph
CalculatingspirometryintheOSCE?
• Youwillbegivensomedatafromapatient(FEV1,FVC,possiblyacoupleofFlow/volumeloopsorvolume/timecurves)
• Youwillneedtocalculatethepatient’sFEV1/FVCratiousingacalculator(calculatorprovided!)
• Youwillneedtofindthepatient’spredictedFEV1onatable• Youwillthenneedtocalculatethepatient’spredictedFEV1%• FEV1/PredictedFEV1• Thensuggestadiagnosis–probablyCOPD• DescribeseveritybasedonNICEguidelines

JoshuaChambers
LearnCOPDseverity:
Describingspirometry:PRACTISETHIS
• Demographic–e.g.age• Quality–e.g.slowstart,takinganextrabreath• Numberofblows• FEV1(%predicted)• FVC(%predicted)• FEV1/FVC• Preandpostdilator• Commentoncurves–e.g.shape,anyanomalies• Diagnosis–e.g.restrictiveorobstructive• Lookatquality
o Ifpatienttooslowblowingout–scooponinspirationo Ortakinganextrabreath

JoshuaChambers
• DEFINEFEV1andFVC• Asthma
o Diurnal–morethan20%differenceatdifferenttimeso Peakflow
Flowvolumeloops:
• Thesearegraphsconstructedfrommaximalexpiratoryandinspiratorymanoeuvresperformedonaspirometer.
• Theloopismadeupoftwohalves,aboveistheflowoutofairfromthemouthandbelowistheflowofairintothemouth.
• Theshapeoftheloopcanidentifythetypeanddistributionofairwayobstruction.• Whenlookingatthese,lookforthenormalflowvolumeloop–withthetriangle
expiratorycurve,slowingdownoncetotalrespiratoryvolumeisreached.There’sasemi-circularinspiratorycurve
• AnydeviationfromtheshapeofA=pathology• TheFEV1=*• ReducedFEV1anywayindicatesobstructiveairwaysdisease.
Inrestrictivedisease:
• Maximumflowrateisreduced• Totalvolumeexhaledisreduced• Becauseofincreasedlungrecoil–flowrateishighduringthelaterpartofexpiration
Extraphysiologicaldetail:• Inrestrictivedisease(suchaspulmonaryfibrosis,ILD,neuromuscularproblemsor
chestandspinedeformities)there’sarestrictiontolungexpansion.Thereforethere’sareductioninthevitalcapacityinthelungs,resultinginareductioninFVC

JoshuaChambers
• Moreover,asthere’sreducedcomplianceandelasticitythere’sALSOareductionintheFEV1
Inobstructivedisease:• Flowrateislowinrelationtolungvolume• Expirationendsprematurelybecauseofearlyairwaysclosure“Scoopedout
appearance”afterthepoint.Extraphysiologicaldetail:
• Inobstructivedisease(COPD,Asthma,CF,bronchiectasis)there’saresistancetoexpiratoryflow.ThismakesitdifficulttoachieveagoodFEV1
• Thismakestheratiolower,commoninrespiratorydiseaseThegraphsshow:
• A=Normal• B=Restrictivedefect(Phrenicpalsy)• C=Volumedependantobstruction(Asthma)• D=Dependantobstruction(Severeemphysema)• E=Rigidobstruction(Trachealstenosis)
Volumetimegraphs:
• Inanobstructivepicture,thecurvedoesn’tplateau.Youhavetothinkaboutratios–
ifitdoesn’tplateauthenFEV1willbemuchlowerthanFCV,givingarestrictive<70%picture.
• However,withrestrictive,thecurveisjustasmallerversionthannormal.That’swhytheratioremainsthesame.
• Rememberrestrictivedefectsincludeintrathoracicandextrathoracicrestrictions
Peakflowprocedureandinterpretation:Peakflow:Intro:
• Washhands• Introduceself• ConfirmpatientsnameandDOB
JoshuaChambers
• ‘I’vebeenaskedtoassessyourpeakflowisthatokaywithyou?Explanation:
• Checkpatientsunderstandingofthecondition• ExplainwhymeasuringtheirPEFRisimportantasaguidetohowwell-controlled
theirasthmais• ExplaintothepatientthattheyshouldbecheckingtheirPEFRregularly,particularly
iftheirasthmaisworsethanusual• Thepeakflowmeasuresthemaximumspeedofexpiration(howfastyoucanblow
outalltheairinyourlungs)• Todothisyouwillhavetoblowashardandasfastasyoucanintoatube.
Demographicstoreceive:
• Weight• Height• Ethnicity
Thingstoconsider?
• Havetheyjusttakenaninhaler?• Havetheyjustsmoked?• Havetheyjustdonestrenuousexercise?• Havetheyjusthasabigmeal?
StepsofthePEFRmeasurement:
• DescribethestepsinPEFRmeasurement• Connectacleanmouthpiece• Ensurethemarkerissetto0• Standorsitupright• Holdthemeterhorizontallyandensuretheyarenottouchingthedial• Takeasdeepabreathinasyoucanandholdit• Placethemouthpieceinyourmouthandformastightasealaspossiblearoundit
withyourlips• Breathoutashardandasfastasyoucan(measuresthefirstpuffsotheydonot
needtoexpirefully)• Observeandrecordthereading• Repeat3-4timesandrecordthehighestreading• Notedowntherecordinginadiaryforcomparison• Afterdescribingtheprocesstothepatient,youshouldshowthepatienthowto
performthemeasurement–dothisbymeasuringyourownPEFR• ASKTHEPATIENT,ISTHISALLCLEAR,DOYOUHAVEANYQUESTIONS?REPEATTO
MEBACK• Oncethetechniquehasbeendemonstratedasthepatienttoshowyouhowthey
wouldperformthemeasurementbythemselves.• Makesuretheyaredoingitcorrectlyandresolveanymistakestheymaybemaking
Postprocedure:
JoshuaChambers
• Askthepatientiftheyhaveanyquestionsorconcerns• Disposeofthemouthpiece• Thankthepatient
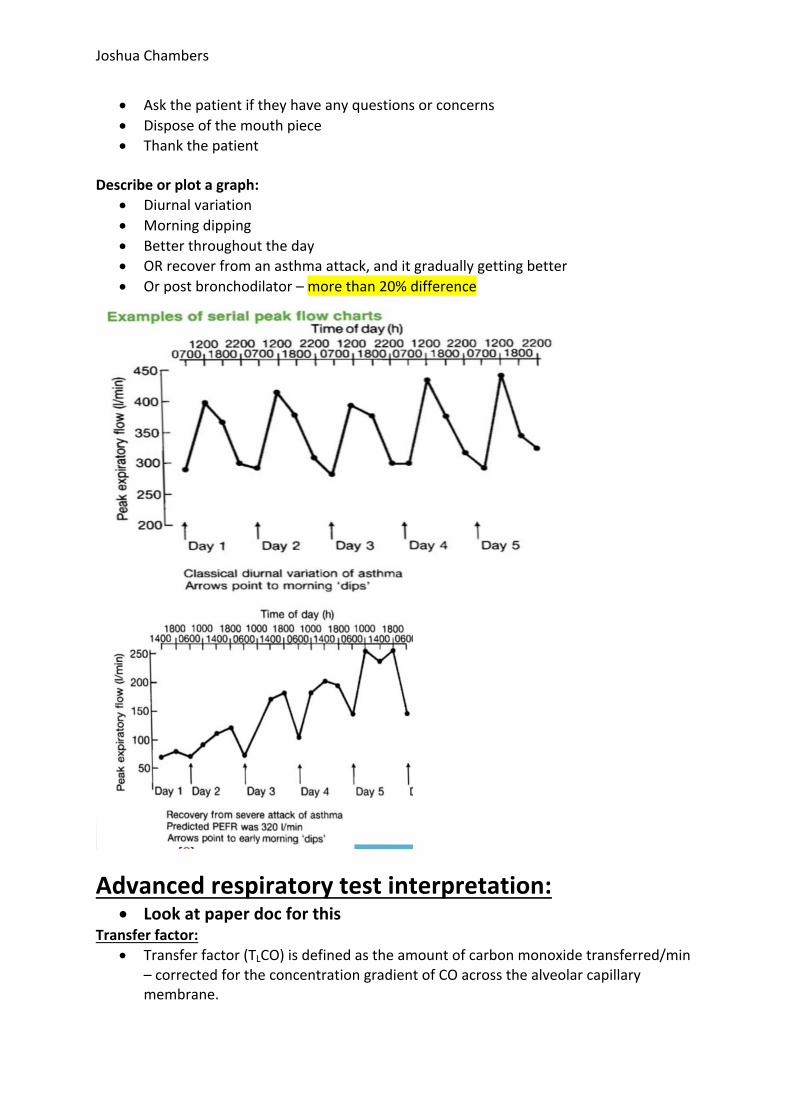
Describeorplotagraph:
• Diurnalvariation• Morningdipping• Betterthroughouttheday• ORrecoverfromanasthmaattack,anditgraduallygettingbetter• Orpostbronchodilator–morethan20%difference
Advancedrespiratorytestinterpretation:• Lookatpaperdocforthis
Transferfactor:• Transferfactor(TLCO)isdefinedastheamountofcarbonmonoxidetransferred/min
–correctedfortheconcentrationgradientofCOacrossthealveolarcapillarymembrane.

JoshuaChambers
Whenistransferfactorreduced?• Feweralveolarcapillaries• V/Qmismatches• Reducedaccessiblelungvolumes
Testing:• Gastransferisarelativelysensitivebutnon-specifictest• Itisusefulfordetectingearlydiseaseinlungparenchyma• Transfercoefficient,therefore,isabettertest.• Transfercoefficient(KCO)iscorrectedforlungvolumesandisusefulat
distinguishingcausesoflowTLCOduetolossoflungvolume.• TLCOandKCOarealwayslowinemphysemaandfibrosingalveolitis• TLCOislowbutKCOisnormalinpleuraleffusionsandconsolidation.
Conditionsthataffectthetransferfactor
DecreasedTF IncreasedTFPulmonarycauses Emphysema,lossoflung
tissueanddiffuseinfiltration
PulmonaryHaemorrhage
Cardiovascularcauses Lowcardiacoutput,pulmonaryoedema
Thyrotoxicosis
Othercauses Anaemia Polycythaemia
ABGprocedure:Introduction:
• Washhands• Introduceyourself• ConfirmpatientsnameandDOB• ‘I'vebeenaskedbythedoctortotakeabloodsamplefromyourarteriestodayis
thatokay?’• Explainprocedure• ‘Theprocedurewillinvolvemeputtingasmallneedleintoanarteryintoyourwrist
togetabloodsample.Itshouldn’tbetoouncomfortablebutifyou’dlikemetostopatanypointpleaseletmeknow’
Tocheckfor:• Contraindications
o Clottingdisorders“Anyproblemsinthepast?”o Onanyanticoagulants/warfarin
• Isthepatientonair?o Inspiredair-oxygensats/pao2-aretheyonconstantoxygen?
• Temperatureo canaffectdissociationcurve
• Alan’stesto Tocheckforulnaarteryperfusiono Toensureadequatebloodsupplytothehand
Preparation:

JoshuaChambers
Getequipment:• Gloves• Syringepack• Alcohol• Cottonwool• Sharpsbin
Questionstoask:• Whichisthepreferredarm?• Placethewristinhyperextension• Locatetheradialartery• Offeranaesthetic(2%lidocainesubcut)
Procedure:• Palpateradialartery• Cleanskin• Letthepatientknowyouareabouttoproceedandtoexpectasharpscratch.• Pullbackplungerto0.7(1.5ml)toallowroomforthebloodtofillit• Inserttheneedleat30degreestotheskinatthepointofmaximumpulsationof
theradialartery.• Advancetheneedleuntilarterialbloodflushesintothesyringe.Thearterialpressure
willcausethebloodtofillthesyringe.• Removetheneedle/syringeplacingtheneedleintothebung.Pressfirmlyoverthe
puncturesitewiththegauzetohaltthebleeding.(5secondsthenletthepatientdoit)
• PushoutanyairwithinitandShaketomixanticoagulantsPostprocedure:
• Labelthesamplewiththepatient’sname,DOB,hospitalnumberandinspiredoxygenandsendforanalysis
• Removeyourglovesanddisposethemintheclinicalwastebin.• Disposeofallofthestuffintherelevantbins• Washyourhandsandthankthepatient.
ABGinterpretation:
1. Onairoronoxygen2. Lookatoxygen–type1/2respiratoryfailure?Below8kPa3. LookatthepH,AcidemiaorAlkalemia?4. LookatthePCO2,Isithigh?Thatwouldbeanacidosis.Isitlow?Alkalosis?Ifit
correspondstowhatisinstepone–youknowitsduetorespiratoryabnormality,ifitdoesn’tcorrespond–iepHof7.47andaCO2innormalranges–it’sprobablymetabolic
5. Lookatthebicarb.Isthebicarbhighorlow?Highbicarb–alkalosis.Low–acidosis.6. THINKwhatisoppositetothepH?IftheCO2agreeswiththepHandthebicarbis
opposingthepHitsuggestscompensation7. Ifyouhaveconflictingresultsbetweenametabolicorrespiratoryprimary–lookat
theO2.IftheO2islowitdoesindicatethatthere’srespiratoryfailure…Therefore..leadingyoutobelieveit’sarespiratoryprimary.

JoshuaChambers
Noteoncompensation:
• Compensationisanopposingmechanism• Thebodyneverovercompensates,topushittheotherside• Compensationmaybecompleteorincomplete.Thus,ifit’scompleteitthepHmay
stillbeinnormalranges.Ifit’sincompletethepHwillbeoutsidenormalranges.Type1RespiratoryFailure=paO2<8kPawithnormal/lowpaCO2Type2RespiratoryFailure=paO2<8kPawithhighpaCO2>6.5kPaSteps ResultsFirstlookatthepH <7.35=Acidosis
>7.45=Alkalosis
NextlookatpaCO2-Isitinkeepingwithabove?
pH<7.35andpaCO2>6.0=RespiratoryacidosispH>7.45andpaCO2<4.5=Respiratoryalkalosis
IfpaCO2notinkeepingwithpHthenlikelyitsgoingtobemetabolic
pH<7.35andHCO3-<22=Metabolicacidosis
pH>7.45andHCO3->28=Metabolicalkalosis
Lookforcompensation Respiratorycompensationmayoccurearlywhereasmetaboliccompensationoccursinchronicdisease
InterpretationofABGs–valuestobearinmind
HC03 <21mmoles 21–29mmoles >29mmolesPaC02>6kPa
Respiratory+metabolicacidosis
Respiratoryacidosis Metabolicalkalosis+respiratoryacidosis
PaC024.5–6kPa
Metabolicacidosis Normal Metabolicalkalosis
PaC02<4.4kPa
Metabolicacidosis+respiratoryalkalosis
Respiratoryalkalosis Metabolic+respiratoryalkalosis
Pastandsfor“Pressureintheartery”

JoshuaChambers
Generalcausesofrespiratoryfailure:Type1:
• It’scausedbyaloworhighV/Qmismatch• LowV/Qcauses:whereareasoflungareperfusedwithdeoxygenatedbloodbynot
ventilatedwithoxygen• HighV/Qcauses:Whereareasofthelungareperfusedwithdeoxygenatedbloodbut
arenitbeingventilated.• ThereasonCO2isnormal,isbecausethenormalpartsofthelungarefreetoblood
offmoreCO2thannormalType2:
• Causedbyalveolarhyperventilation• Thismeansthatoxygencannotgetintothealveoliandcarbondioxidecannotget
out• COPD,restrictivelungdiseaseorneuromusculardiseasecausethis
Oxygentherapy,practicalstuff,prescribingandtypesofmask:FiO2:
• FiO2=fractionofinspiredoxygen• Roomairis21%FiO2• Highflowmaskscangive60%FiO2• CanbehardtotellifPO2isappropriatelyhighforFiO2andwhetheroxygenationis
impaired• Ruleofthumb:ExpectedPO2=FiO2%-10• Example:patientonFiO240%(facemask).ABGshowsPO2of18.8kPa(normal
>10kPa)• IMPAIREDOXYGENATION
TargetsatsforCOPDandnormalpatient:TargetsaturationsforT1/T2respiratoryfailure?
• TypeIIRespiratoryFailure:o 88-92%targetsats.o VenturiessentialinTypeII
• TypeIRespiratoryFailure:o 94-98%targetsatso Assesssatsatleast6hourly
Uncontrolled(variable)performancesystems:Theoxygensuppliedtothepatientwillbeofvariableconcentrationdependingontheflowofoxygenandthepatient’sbreathingpattern.
• ThisiswhenO2requiredtoraisetheSaO2above92%• NoconcernsthehighO2willsupresstheventilatorydrive.
Device Image Flowrates(FiO2)
ConcofOxygenthatcan
bedelivered
Examplesofuse

JoshuaChambers
Nasalcannulae
1-6L/min
approx24-50%
SimpleFaceMaskAlsoreferredtoas:• MCMask• MediumConcentration
Mask• MaryCatterallMask• HudsonMask
6-10L/min
Flowratemust
beatleast5
L/mintoavoidCO2re-
breathing
approx40-60%
ReservoirMask(NonRe-breathingMask)
• Deliverthehighestflowoxygentosomeoneinhospital
• Reallysickpatients• 15L–MAXoxygen
10-15LminReservoir
mustbefilledcorrectlybefore
administration
approx60-90%
Short-termuseTraumaEmergencyCriticalillnessPostcardiac/respiratoryarrest
Controlled(fixed)performancesystemsWillgiveanaccurateconcentrationofoxygentothepatientregardlessofthepatientsbreathingpatternandflowofoxygen(providingtheminimumsuggestedflowrateasshownontheVenturivalveisused)
• ControlledusewithextraO2isrequired.• However,it’sCONTROLLEDasventilationrequiresthehypoxicdrive• ThereforePaO2mustnotgoabove8kpa(BasicallyoutofT2respiratoryfailure)
VenturiMasks• O2isdirectedthrough
anarrownozzleandexitsatspeed.
• Thisdrawsinairanddilutestheoxygen
• ItmixesairandO2atthesameratioregardlessofflow
Asper
instructiononVenturivalve
24-60%
Patientsatriskofhypercapnicrespiratoryfailure(egCOPD)
TracheostomyMask
OxygenMUSTbehumidified
24-70%
Patientswithtracheostomyorlaryngectomy
Oxygentherapy:

JoshuaChambers
OxygentherapyreviewTypeofoxygentherapy Aims IndicationsLTOT–Longtermoxygentherapy PatientNEEDSoxygen
LongtermhypoxiaAtleast15hoursIdeally18-20Toreducelongtermcomplicationsofchronichypoxiasuchascorpulmonale(LTOT)
PaO2lessthen7.3(Hypoxicinastablestate)Lessthan7.3Kpaon2occasions,3weeksapartwhenstableOR7.3-8IF…Secondarypolycythaemia,nocturnalhypoxemiaandcorpulmonaleNOTinacuteexacerbationABGinoutpatients,lessthan7.3–doagainin2weeks,confirmandthenstartLTOT
Ambulatoryoxygentherapy AllpatientsonLTOTExercisedesaturation
ExercisedesaturationIeatrest–O294-95%...butifyoudoa6minwalktestitdropssuddenlyNEEDtodemonstratethepatientsgetbenefitwithoxygenMakethepatientwalk,without,withplaceboandwithoxygen–supposedtogiveambulatoryoxygen
SBOT:Shortburstoxygentherapy SevereSOBandunresponsivetoothermeasuresThus,theirPaO2isfineallthetimebuttheyfeelREALLYbreathlessPlaceboornot–itkeepspeopleawayfromhospital
Oxygenalertcard:
• ThisshouldbegiventoallpatientswithapreviousHxofhypercapnia/respiratoryfailure

JoshuaChambers
Prescription:• Oxygenshouldbeprescribedonthedesignatedsectionofthedrugcharttoachievea
targetoxygensaturationof94-98%formostacutelyillpatientsor88-92%forthoseatriskofhypercapnicrespiratoryfailure.
• Forsomepatientsitmaybeappropriatetospecifyadifferenttargetrange.• Alloxygenshouldbeprescribedexceptinanemergency(peri-arrestorcriticallyill)when
itshouldbestartedimmediatelyusingamaskwithreservoirbagat15L/minanddocumentedlaterinthepatientsrecord.
CXRandCTreportsChestX-ray:
• First–READTHESCENARIO.Thiswillgiveyouclues• Demographics:–Name–DOB–DateTaken–View(AP/PA/lateral)–“Thisisa
plainfilmchestradiograph,PAview,takenof………..,DOB10/06/1941.Itwastakenon15/11/2014…”
• BrieflyrunthroughqualityofCXR(RIPE)o Inclusion/Exposure–bothcostophrenicangles,bothapiceso Rotation–symmetryofclavicleso Inspiration–5-7anteriorribso Penetration–seethoracicvertebraethroughheart
• WorkthroughrestoftheCXR:o A-Airwaysincludingthehilao B-Bonesandsofttissueo C-Cardiacsilhouette,sizeandmediastinumo D-Diaphragm,costophrenicanglesandhemidiaphragmso E-Effusionsandpleurao F-Lung'fields‘
• Checkpleuraandlungedgeforpleuraleffusionandpneumothorax• Lines,drainsetc..E.g.chestdrain,centralline• KerleyBlines=Pulmonaryoedema
o Usuallyfoundatthelungbases• Anyforeignbodies,ECGleads,endotrachealtubes,pacemakers• STATETHEOBVIOUSFINDINGS
Extras:• Opacity=white

JoshuaChambers
• Hypo(dark)/hyper(white)density• LateralCXR–drawthehorizontalandtransversefissuresofthelung–knowthe
surfacemanagementHowtodescribealesion?
• Whereisit• Howbigisit?(Tennisball,5pcoin,10pcoin)• Whatisit’sshape?• Boarderwellorpoorlydemarcated?• DESCRIBEwhatitlookslike–fluffy,homogenous,heterogenous?)• Presenceofanairfluidlevel?• Awhitefluffyzonearoundalesionisoftensclerotic
Howtodescribeanopacity:
• Whereisit?• Whatzoneisit?• Doesitcoveranyboarders?(Indicatingalobe)• DESCRIBEWHATYOUSEE,fluffy,homogenous,hetrogenous…etc..
Commonpathologiestocomeup(Knowthemanagementofthese!)
• Pneumonia:consolidation,airbronchograms,identifylobes,parapneumoniaeffusion
• PleuralEffusions:bluntingofcostophrenicangle,homogenouswhiteout,mediastinalshiftaway
• Pneumothorax:mediastinalshifttowards(unlesstension),pleuralline,lossoflungmarkings
• Pulmonaryoedema:batwingappearance,septallines,venoushypertension,smallbilateralpleuraleffusions
• Collapse:mediastinalshifttowards,increaseddensitywithoutairbronchograms,identifylobes
• Fibrosis–thisisclassifiedasupper,middleorlowerzones–andcanbespreadoutallaround…Itgivesthoseweirdlinedappearances..
• KNOWWHERETHEFISSURESAREBOTHONAPANDLATERALThingstoconsiderfortheOSCE:
• Atfirst,untiltoldto,don’tbespecific!Say“Opacity”insteadofconsolidation• Insteadof“Cavity”say“Lesion”,asthisislessspecific.• USEZONESinsteadoflobes• ALWAYScheckifit’sAP/PA• AlwaysrelateCXRtotheclinicalpicture…• InbonesREALLYLOOKFOR#orchunkmissing-becauseoftentheremaybea
pneumothorax!• Forany?consolidation-look
Specificsforcollapse:(+generalcollapsefindings)

JoshuaChambers
• Upperlobecollapse–subtlebecausethelowerlobecompensateso Oftendemarcatedbythehorizontalfissureo Thelungbecomessmallero Mediastinalshiftoccurso Diaphragmgoesupo Tofindoutwherethecollapseis–lookforshady/hazyshadowingandthisindicatesasto
whereitis.o Canyouseethroughtheheart?Ifnot?Leftlowerlobecollapseo Looktoseeifthehilahasmovedupordowno Veillikeappearancehereiscommon
• Leftlowerlobecollapseo Tocardiacleftboarders‘Sailsign’o Canlooklikecardiomegaly
• Leftupperlobecollapseo Vaillikeopacityo Also,retentionoftheheartboarder
• Rightupperlobecollapseo Somethingdodgeisgoingonupinthatcornerasthelungfoldsinonitselfo AlthoughthisCANlooklikeabronchogeniccarcinoma
• Rightmiddlelobecollapse:o Oftenamassorevenaverywelldefined,sharptrianglejuttingoutofthemediastinum
• Rightlowerlobecollapse:o Quiteaclearsailsortontherightsidecoveringthecosto-diaphragmaticangle.

JoshuaChambers

JoshuaChambers
Prescribing(oxygen),inhalersandnebulisers:Inhalers:Typesofinhaler:
• Nebulisero Drivinggaso Forathomeuseo Onlyforuseinpatientswho’sbreathingissolabouredthatcoordination
wouldbeimpossibleo Mostclinicalscenariosuseaspacerinstead.
• Metereddoseinhalero Pressurisedincanister
• Drypowderinhalero Inspirationo Notgoodwithpeoplewhoworkinwetdampenvironments
Techniquedependingontype:
• DPI=quickanddeepfromthestart• MDI/aerosol=Breatheinslowlyandsteadily• Mostinhalersarequickanddeep.
TakinganMDI:
• Checktheexp.Date• Checkthecapsoff• Checkforanyforeignbodies• Shake• Breathout• Sealaroundcap• Pressdownonce• Slowandsteady• Holdbreathandwaitfor10seconds
MDIwithspacer:• Same• Breatheout• Pressit• 4-5tidalbreaths–slowandgentle• (Reducesoralthrushasitdoesn’thitthemouthasfast)
Whyarespacerssogood?
• Co-ordinationo Delayininspirationo Itgivesusalittletimetogetitallin
• Lessoropharyngealdeposition• Improvedlungdelivery

JoshuaChambers
CPAPandBiPAP:TypeofpatientwithCPAP:Type1
• OSAo Stentingopentheupperairways
• Pulmonaryoedemao Shorttermthingtoenablethemedicalmanagementtokickin(Ie
diuretics/nitrites)• Pneumonias
o Affectingpressuregradiento Can’tventilateo HIGHFLOW(oxygen)ratherthansomethingtosplintthemopen
TypeofpatientonBIPAP:Type2
• COPD• Patientsintype1thatgettired,andunderventilate• Bronchiectasis• Chestwallissues
o Abnormalventilation• Obesity
o Fat• Neuromuscularconditions• Headinjuries/opiates/postsurgery
Inhalertechniqueandinformationgiving:Introduction:
• Introduceyourself.• Washhands.• Confirmpatientdetails–name/DOB• Checkpatient’sunderstandingoftheirinhaler–allowingyoutotailoryour
explanationtothepatient’slevelofknowledge.Explanation:
• Explainwhattheinhalerdeviceis• Youhavebeenstartedon….(nameofinhaler)…foryourasthma/COPD“–Showthe
patienttheinhalerdeviceExplainingdifferenttypesofinhaler:Preventer:
• Forexample,ICSbeclomethasone(Brown)• (Name of inhaler) is a preventer – it helps to reduce the swelling in the airways and
stopping them from being so sensitive. You use this to lower the risk of severe attacks. I would like you to inhale …(x puff(s))…(x time(s) a day)…everyday. It’s really important that you don’t miss doses, as regular use is key to keeping your asthma/COPD under control” – Remind the patient to rinse mouth after use if the inhaler contains a steroid due to risk of oral candidiasis.
Reliever:• Forexample,Salbutamol(Blue)

JoshuaChambers
• (Name of inhaler) is a reliever. This is useful to help relieve immediate wheezing/asthma attacks. It works by relaxing the airways so that you can breathe more easily. You shouldn’t need this more than 3 times a week if your asthma is well controlled. Ask your GP for a review if you are using this more frequently. I would like you to inhale (x puff(s)) when you feel short of breath.
SMART/MARTtherapy:• (Symbicort Maintenance and Reliever Therapy)regime
“Symbicort is used as both a preventer and a reliever. You need to use this regularly …(x puff(s))…twice a day to prevent symptoms and …(x puff(s))…each time you have an attack.” – Remind the patient to rinse mouth after use due to risk of oral candidiasis.
ASKTHEPATIENTTOSUMMARISEKEYPOINTSBACKTOYOUDemonstration:1.Preparetheinhaler–Takeoffthelid/ShakeifMDI/Insertcapsuleifhandihaler2.Loadthedose–pressbuttontopuncturecapsuleifhandihaler/pressleveronceifaccuhaler/twistbottomifturbohaler3.Breatheoutgentlyasfarasiscomfortable.4.Tightlyseallipsaroundthemouthpiece.5.Breathein:
• Drypowderinhalers(DPI)needstobebreathedinquickanddeep• Metereddoseinhalers(MDI)needstobebreathedinslowanddeep• Softmistinhalers(SMI)needstobebreathedinslowanddeep
6.Removeinhalerfrommouth,holdbreathforaslongasiscomfortable.7.Repeatprocedureasdirected.Observeandassess:
• Askthepatienttocarryouttheprocedurethemselveswhilstyouobserve• Mostpatientswillrequiretweaking.• Pointoutthepositives…“youaredoingX&Yverywell“…thenintroduceroomfor
improvement…”butdoingA&Bmayhelpyourinhalersworkmoreeffectivelyforyou“
• DEMONSTRATE>OBSERVE>FINETUNE>REPEATASNECESSARYSpacerdevises:
• Spacersareusedtoimprovedrugdepositiontothelungsinpatientswhocannotmastertheiraerosolinhalertechnique.Theyareusefulinreducingsideeffectsofhighdoseinhaledcorticosteroidsbyreducingtheamountofdrugswallowedandabsorbedintothebody.CommonlyusedspacersareVolumaticandAeroChamber.
1.Prepareinhaler(shakeaerosolinhaler).2.Attachinhalermouthpiecetothespacerdevice.3.Breatheoutgentlyasfarasiscomfortable.4.Lipssealaroundthespacermouthpiece.5.Release1doseintothespacerdevice.6.Breatheinandoutthroughthespacermouthpieceseveraltimes.7.Administerseconddoseifneededandfinish.

JoshuaChambers
• Thespacerdeviceshouldbewashedwithdetergent(washingupliquidisfine)onceamonthandleavetoair-dry.Itshouldneverbewipeddryasthiscancausestaticwithinthedeviceanddrugparticleswillsticktosidesofthespacerasaresult.Spacersshouldbereplacedatleastonceayear.
Closingtheconsultation:
• Askifthepatienthasanyquestionsorconcerns–ensureyouaddressthese• Provideinformationleafletifavailable.• Advisethepatienttogetintouchshouldtheyhaveanymorequestionsorconcerns.• Thankpatient.• Washhands.
SleepstudiesTypes:
• Overnightpulseoximetry• Limitedpolysomnography• Fullpolysomnography• Actigraphy
CXR:
• Lookforairbronchograms• Lookforonething,lookforsomethingelse• Bilaterallymphadenopathycausedbylymphoma• Pleuralplaques–asbestosis• Multiplelungmetsinbothlungs
o Renalo Melanomao Ovarian
• FULLWHITEOUT:pleuraleffusion(butlookfortrachea)pneumonectomyandfulllongcollapse(Inacavity–fillswithfluid)
• Surgicalemphysema–lookup–looksstreakfromtheoutside• Leftlowerlobecollapse–CTindicatedasit’smostcommonlycausedbyatuourof
theleftlowerbronchus• Pneuothorax• COLLAPSE:CTindiated,orbronchoscopylookforcause(Mucousplug,tumouretc..)• Tumourinlungapex–candamagephrenicnerveandcausediaphragmisraised• Welldefinedpneumoniawithinalobe–lobar/roundpneumonia• Smallandfairlywelldefined–CANCER–goforCTand/orbiopsy• TRAUMA–Pneumohaemothorax(Orhydropneumothorax)becausetheairpushes
downtheeffusion• Ifwhiteopacitywithnomeniscus–think,infectionconsolidation• Middlewhiteopacitythatlookslikemiddlelobeconsolidationisacavitywith
infectionandairfluidlevel• CANgetsailsignwithrightlowerlobecollapse–lookforheartboarderunderthe
effusion!!Ifwelldefined

JoshuaChambers
• LOOKFORNGtubegoingintotheleftlung• Don’tcommentoncardiomegaly–AP• IFTRIAGNLEOPACITYFROMRIGHTHEARTBOARDER–middlelobeconsolidationor
collapse• Theringshadowsinbronchiectasisarebronchioles