module #3 - lesson 25 super nutrition academy mdule 3 lesson 2 b u Ç x } u we have triglycerides,...
TRANSCRIPT

Cell Membranes and the Cholesterol Myth (Part 1)
MODULE #3 - Lesson 2

2Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Module 3 - Lesson 2Cell Membranes and the Cholesterol Myth (Part 1)
Welcome to Module 3, Lesson 2. Today we will talk about cell membranes, how fats work in the body, and the cholesterol myth. This will be a very in-depth look at fats, cholesterol, heart disease, cell membranes. I have broken up this lesson into two parts.
The first part we’ll talk about now and the second part in Lesson 3. This is really important stuff so I’m going to try to do my best to make a very complicated subject easy to understand.
What We’ll Be Covering TodayToday we will cover fats in the cell membrane; how fat is digested, transported, and stored in your body; the role of triglycerides in heart disease; how to measure your blood lipid levels; and more.

3Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
In The Body…
In the body, fat is stored and used for transport as 3 different molecules but we’ll start off with two. The first one is called a triglyceride, which as the picture on the right shows, is three fatty acid chains and a glycerol head. So, we have three fatty acids chains.
Remember, if they have a kink, they might have one double bond; so, it might be an unsaturated fat. If they’re straight, then they’ll most likely be a saturated fat.

4Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Next we’ve got our glycerol head, so that is what a triglyceride is. When we eat fat, it is broken down in our small intestine then it is rebuilt into a triglyceride before it goes anywhere else.
Now, we also have cholesteryl esters. When we eat a food that contains cholesterol, we don’t actually absorb cholesterol as cholesterol, it has to combine with another molecule, and a cholesteryl ester is cholesterol plus a fatty acid.
Just to the right of the triglyceride picture, we have a cholesteryl ester, which is, essentially, an unsaturated fatty acid. On the bottom right here, we have the cholesterol molecule. It looks more dense, and at the bottom you can see what a cholesterol molecule looks like; it’s a lot more dense and packed. Cholesteryl esters are what we absorb through the small intestine.
Cholesterol and fat are not water-soluble, so they can clog the capillaries if they’re not packaged correctly.
The reason that the body goes through all this trouble to repackage the way the fats we eat is to prevent a buildup of fats in our capillaries. If fat got stuck in them we’d have a stroke all throughout our body. The body’s amazing at repackaging these fat molecules in a way that that’s all prevented.
PhospholipidsPhospholipids are another type of fat, and these really make up the major component of our cell membranes. We’re going to look at cell membranes and cells, which are really the fundamental building block, if you will, of the human body and why it’s so important to have a healthy cell membrane.
Phospholipids are comprised of two fatty acid chains. In this case we have a saturated fat and an unsaturated fatty acid plus a glycerol molecule at the top, plus phosphates, and choline…usually.
Choline, phosphates, and glycerol form up the head group. The nature of choline, phosphate, and glycerol make the phospholipid have a hydrophobic head, so a head that repels water. The tail is hydrophilic, so it likes water. And this is important because it will lead to a natural lipid alignment.

5Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
We have triglycerides, which are three fatty acids and a glycerol molecule, we have cholesteryl esters, which are cholesterol, plus a fatty acid, and we have phospholipids, which are two fatty acids, a glycerol, phosphate, and choline head.
Cell MembraneAs we learn more about health on a microscopic level, we realize that our entire body’s health starts with cellular health. It’s really important that we take care of our cells and give them the nutrients and the support that they require.
A cell membrane is the outer layer of a cell. It’s a semi permeable membrane meaning it allows certain things to come in and certain things to go out. It separates the interior of the cell from the outside environment. It allows for diffusion or the transport of certain substances like oxygen and carbon dioxide. For instance, when you’re exercising, your body produces a lot of waste from cellular metabolism. The CO2 produced can leave the cell through diffusion.
When the red blood cells come to your cells and they’re ready to give off their

6Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com

7Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
oxygen. , That oxygen diffuses right into the cells. Water can be transported across the membrane by osmosis. It’s basically just water molecules going from an area of high concentration to low concentration. Then we have mediated or active transport. We have special transport proteins that help sugars. For instance, we have proteins called GLUT4 transporters in our muscle cells that help take sugar out of the bloodstream and into the cells. We also have amino acids. These transport proteins also allow amino acids into the cell and waste to leave the cell. So, we’ve got active transport as well as passive transport.
Endocytosis is a process in which cells absorb molecules, if you look at the picture on the bottom right, by engulfing them. It’s almost like Pac-Man. A couple molecules come toward the cell membrane and then you’ve got Pac-Man engulfing them right into the cell. This requires energy, ATP. Then on the flipside, we have exocytosis.
This is a way for the cell to eject waste from the plasma inside the cell. These two pictures on the bottom right depict that. It is almost like a balloon that feels like it’s going to float away. That’s the same type of thing that’s happening with exocytosis.
There’s a natural bilipid setup with these phospholipids. This picture here shows phospholipids. If we look at the circular head, this would be our phosphate, choline, and glycerol head group, and that is what repels water. Inside we have our fatty acid chains, the two fatty acid chains for each phospholipid. Notice how they’ve arranged themselves so that the fatty acid chains are kind of toe-to-toe.
The head of the phospholipid bilayer is hydrophilic. It actually attracts water. We know fat repels water; it naturally flips around and will associate with the other fatty acid chains because they are hydrophobic. The outside of the bilayer is friendly to water, the inside is unfriendly to water, and that’s why we get this natural configuration.
Phospholipids allow for fluidity. If you look at this picture, you can see wavy fatty acid chains. This allows for this fluidity of the cells. The other important components to the phospholipid bilayer, are rigidity and structure. This is provided by cholesterol. So, this is where we start talking about the importance of cholesterol. Remember the picture of it being really kind of compact and a

8Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
really kind of solid-looking structure? That’s what it gives the cell membrane. Here’s an important thing: More essential fatty acids in a cell membrane means more cholesterol will be held in the membrane, which means there will be lower cholesterol in the blood.
If we have a lot of essential fatty acids, which are very fluid, in the cell membrane, the cell knows it needs more structure and rigidity, so it actually calls cholesterol into action, to give more rigidity. Therefore, less cholesterol is circulating in the blood because more of it is in the cell membrane.
Now, the opposite is true if there’re too many saturated fatty acids in the cell membrane. This is where we start to look at the importance of the notion of “you are what you eat.” If you eat a diet of high-saturated fatty acids, a lot of rancid fats, a lot of polyunsaturated fats that are of really bad quality, if you eat too many, for instance, animal fats, a lot of these will be stored in

9Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
the cell membrane. Because the cell membrane is more structured due to saturated fats, then the cell membrane won’t need as much cholesterol. It’ll already be structured and rigid; therefore, you will naturally have higher levels of cholesterol in the blood.
Here’s just another image of the cell membrane. We have our phospholipid bilayer here. If we just look at the round heads, which are water-friendly; inside the fatty acid chains are not water friendly; that’s why they align like this. We have the fluid structure, and then we have cholesterol placed throughout these white hexagons. We have different receptors, binding sites, protein molecules that allow transport of certain things. This is what it looks like from a very microscopic level.
Again, it separates the extracellular fluid, the outside of the cell from the inside of the cell. And then it’s just a matter of moving things in, moving things out. It’s kind of like breathing and exhaling at a very microscopic level.

10Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Delicate Cell MembranesOur cell membranes incorporate the fats that we eat, so quality really matters. That’s what we talked about in the first lesson, the importance of omega-3 fatty acids. They’re very, very important. It doesn’t matter which cell we’re talking about. It could be a brain cell, it could be a cell in your muscle; every single one of those cells will incorporate the fats that you are eating. Omega-3 and omega-6 are important components of cell membranes.
So, we talked about the action potentials in the first lesson, the first module. They also help with that and allow it to kind of work more effectively. They hold oxygen in the cell membrane, where it acts as a barrier to viruses, fungi, and bacteria. This is a really important concept because omega-3s are such an interesting molecule. They’re very, very highly reactive, and just the nature of their chemical structure holds oxygen inside or beside them. That’s a great thing for the cell membrane because we want to be oxygenated, we want our cells to be oxygenated, and that allows for that.
And they also hold proteins in the membranes via electrostatic forces. These similar forces that hold oxygen into the cell also allow for electrostatic forces to hold proteins into the cell. Because, again, we’ve seen that omega-3s have unpaired electrons and are very kind of unstable molecules, so they kind of hold on to other things to help stabilize them, and this improves active transport. This improves things like moving sugar from the blood into the cell, moving amino acids into the cell through active transport. So, omega-3s—especially omega-3s; omega-6s obviously to a lesser extent—are very, very, very important. This is just another example of why they are.
Healthy Cells Resist DiseaseWe have a couple pictures here. On the left-hand side the really nice-looking, shiny car is the healthy cell. It’s infused with essential fatty acids, lots of oxygen inside it, and it’s got a good amount of cholesterol, so it naturally resists disease and degeneration. On the flipside, this broken down car is the unhealthy cell. So, it doesn’t have a lot of fatty acids, its low on oxygen, and prone to disease and degeneration.

11Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Now, these diagrams on the right show the same thing, just more from a cellular perspective. The sick cell is asking for help. It’s very porous; it doesn’t have good structure, so it’s not able to fend off bad things and keep them out, whereas the healthy cell, you can just see these little things bouncing off and it’s kind of got this natural glow and that’s because the cell is healthy, it’s infused with the right structures for the cell membrane, good amounts of essential fatty acids, cholesterol, good, healthy fats and it’s holding on to oxygen and, therefore, it’s just deflecting different foreign substances that do not belong inside the cell. Very important.
When we’re talking about health, we are talking about these two images right here. Healthy cell, healthy body. Sick cell, sick body.
EFAs, Cell Membranes, and CancerTo be functional, the cell membrane must maintain its integrity and fluidity. Cells without a healthy membrane lose their ability to hold water, vital nutrients, oxygen, and their ability to communicate with other cells. We’ve seen these different protein molecules on the cell membranes. These are also used in communication.
When a cell loses these things, it is one of the physiological events that leads to the growth of cancerous tumors. The integrity and fluidity of our cell membranes is determined in large part by the type of fat. Diets containing

12Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
large amounts of saturated or hydrogenated fats will lead to cell membranes that are hard and lack fluidity.
Evidence suggests that when omega-3 fatty acids are incorporated into cell membranes, they can help protect against cancer, notably by inhibiting a proinflammatory enzyme called COX-2, which is an enzyme that promotes breast cancer. It also activates a type of receptor called peroxisome proliferator-activated receptors, so PPAR, which can shut down a number of variety of cells in breast cancer and breast cancer tumors, and it increases the expression of different tumor suppressor genes.
Essentially, omega-3 fatty acids inhibit certain enzymes, certain genes that can lead to tumor growth and then, follow to the development of cancer while promoting other receptors and genes and enzymes to work to keep the cell healthy.
In 2005 the International Journal of Cancer that looked at EPA and DHA and showed that they protect against cancer by affecting cell growth by activating an enzyme called sphingomyelinase, which then generates the release of ceramide, which is a compound that activates the human tumor suppressor gene 21. It inhibits these genes that are causing our cells to mutate into cancerous genes.
An animal experiment was conducted where mice were fed diets rich in either omega-3 or omega-6 after which breast cancer cells were implanted. Three weeks later tumor volume and weight were significantly lower in mice on the omega-3-rich diet. In the lab culture experiments, when cells were treated with DHA or EPA—which, again, are derivatives of omega-3s—sphingomyelinase activity the enzyme we just looked at in the previous slide increased by 30 to 40 percent, and breast cancer cell growth dropped by 20 to 25 percent. The more omega-3s you bring into your body, the better quality the cell membranes. It’s also affecting, literally, cancer-suppressing genes at the cellular level.
In Sum…High-quality cell membranes are very important to all aspects of your health. Think of them as trillions of little houses within your body. What if the foundation of your house was sinking or your roof had holes in it?
13Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Would you just want strangers coming into your house? These are all things that kind of lessen the value, if you will, and the security of your home and what’s inside of it. The same thing happens with the cells. We need them to be strong, a good combination of fluidity and structure to give you the ultimate health that you need.

14Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
How Fat is Digested
Fats begin their digestion absorption in the small intestine, the duodenum. If you look at the diagram here on the right-hand side, which is out of the picture, that would be the stomach. The stomach is now kind of bringing stuff in, kind of allowing, ejecting what is known as chyme into the small intestine. When you eat food and it’s in the stomach, when it leaves the stomach, it becomes this mushy thing called chyme.
So, this chyme comes into the small intestine. The first part of the small intestine is called the duodenum. Now, when these little fat globules are in the duodenum, they cannot be absorbed or broken down.
If you’ve ever gotten fat on your hands from handling, bacon or fish you’ll notice that the fat doesn’t go away with just water, and that’s because water and fat don’t mix.
So we need to use soap to emulsify the fat, which means that the soap renders the fat more water-soluble so that we can get it off our hands.
Bile is like the soap; it emulsifies fat. And lecithin, which is a component of bile, increases the surface area for enzyme exposure. Bile kind of surrounds the fat globules and allows that to improve the surface exposure of these fat molecules so that enzymes can then act on them and break down.
So, once that happens, lipase from the pancreas begins to digest fats into individual components, fatty acids and monoglycerides.
If you ever use digestive enzymes, lipase would be an enzyme in digestive enzymes that help break down fats. Lipase is produced and secreted from the pancreas then it enters the digestive tract and breaks down those emulsified fat molecules.
These components then diffuse into the epithelial cells of the small intestine that are lining the lumen, then fats are reassembled and form chylomicrons and these chylomicrons then diffuse into the lymph and then are dumped into

15Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
the bloodstream and distributed throughout the body. When you have steak, butter, any kind of fat, omega-3s, this is exactly what happens from start to finish.
The small intestine can digest about 10 grams of fat per hour, so if you have a meal that’s really in fat, with more than 10 grams of fat, you’re going to be suffering for a little bit of time.

16Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
How Fat Gets Digested
On the left we have the lumen inside of the small intestine, where we have these fats, and these three blocks are fatty acids. The dark block is the glycerol molecule. Notice how, with digestion, it’s all broken apart? And then inside they’re diffused, they kind of get into the cells, the epithelial cells lining the small intestine; that’s what these are here, these cells, these blocks. And these individual components are then reassembled into triglycerides.
So, we eat triglycerides but in order for it to get across these epithelial cells, it needs to be broken down first and then we reassemble. Sometimes you think of it as a little bit inefficient, but at the same time, it’s necessary for our body to absorb it. So, a triglyceride is broken down, and then we form it again into triglycerides eventually.
These chylomicrons, don’t actually reach our cells. They go through a number of different steps. And that’s where lipoproteins come in. If you’ve ever heard of lipoproteins like LDL, HDL, that’s where we’re going.

17Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
How Fat is Transported
Fat is insoluble, as we’ve seen so it must be packaged and transported somehow throughout the blood without clogging the capillaries. That’s why we use lipoprotein particles, LDL, HDL, a couple others as well.
Think of them as a moving truck, like a FedEx truck or UPS truck. Essentially, it’s an outer layer that is comprised of lipids that are oxygen-rich and a type of protein known as apoproteins, inside the cell, a hydrophobic core; so, a cell inside that is scared of water, and this allows the compacting of fat.
We know that fat doesn’t like water, so it’s all able to kind of hide together, away from the watery exterior, and they’re able to really pack in nice and densely, and they’re surrounded by this hydrophilic phospholipid shell. So, the phospholipid bilayer—again, this lipoprotein particle has this phospholipid bilayer just like any cell in our body does. The outside of the cell we know is water-friendly, and that allows this lipoprotein to be transported throughout the blood. Pretty cool stuff.

18Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
The 4 Types of Lipoproteins
We have four types of lipoproteins that we’re going to be talking about. On the left we have a chylomicron, and the chylomicron is the first molecule that leaves the small intestine.
Before we go any further, the orange inside any of these lipoproteins represents triglycerides, the yellow represents cholesteryl esters. As we go from a chylomicron to VLDL, there’s a huge decrease in the amount of triglycerides inside the lipoprotein.
As we go from VLDL to LDL, there are no more triglycerides. It’s only cholesteryl esters inside the LDL. As we go further to HDL, now we have a small, compact, less cholesterol-intense, if you want to call it that, lipoprotein. So, we’ve moved from a big chylomicron molecule, which carries triglycerides, to an HDL lipoprotein, which carries cholesteryl esters. And, as you look, the more we move to the right, the more protein it has, and the protein will be denoted by these different receptors, these different kind of triangles and squares and rectangles on the cell membranes. It would be more protein relative to the size, so it’s relative protein.
On the left side here there’s more fat as we’re toward the chylomicron and LDL. As we move back toward the HDL, it’s obviously more compact, more

19Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
dense, and that is what we want. And that’s why HDL is the ultimate lipoprotein that we want more of in the body, okay? We’re going to look at this a lot more in depth starting on the next slide and moving into the next lesson.
Just to clarify, chylomicrons and VLDL, they carry primarily triglycerides. LDL and HDL carry primarily cholesteryl esters.
In General…In general, cholesterol isn’t bad it’s the packaging that can be the problem, especially if they are rancid or oxidized LDL. And the reason this happens is that if LDL circulates in the blood too much, it can then become exposed to free radical damage and oxidative stress and that’s a problem.
So, if the packaging is damaged, it will do damage. Imagine you have a FedEx truck and it has a flat tire. It’s not going to be able to steer properly; it could literally just kind of drive off the road and hit a house. That’s the same type of thing that’s happening here.
VLDL is reversely proportional to HDL levels. The higher the HDL levels, the lower the VLDL levels and vice versa. We don’t want a lot of VLDL in the blood, but we do want a lot of HDL in the blood.
We hear a lot about cholesterol, but triglycerides are a huge risk factor for cardiovascular disease. Hopefully you’ve heard of this stuff from your doctor. If you haven’t, then you need to pay attention to triglycerides, and that’s where we’re going. Before we look at how these lipoproteins are formed, we need to look at triglycerides.
Quick Note on TriglyceridesTriglycerides are fat in the blood. If you’ve ever left chicken soup in the fridge overnight in the fridge, the layer of fat on top is essentially, triglycerides.
If blood is left on the counter for a while the fat will rise to the top, leaving the water at the bottom.
Triglycerides are often overlooked, but they’re a very important contributor to atherosclerosis and cardiovascular disease. A study in 1994 by Hodis and

20Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
his colleagues reported that bad cholesterol, LDLs, appeared to be masking arterial damage caused by triglyceride-rich lipoproteins called VLDLs, very low-density lipoproteins, and intermediate-density lipoproteins.
They were masking the damage that was actually being caused by triglyceride-rich protein. The study found that despite aggressive treatment of the bad cholesterol with medication, patients with high triglycerides continued to suffer damage to their arterial walls. VLDL and IDL, because both of them are triglyceride-rich molecules, one step down from the chylomicrons—they were the culprits in this case.
TGs and Insulin ResistanceThis is a very interesting relationship. I think this will really illuminate some stuff for you. Approximately 50 percent of people with high blood pressure—hypertensive patients—have an insulin-resistance syndrome or problem. Insulin resistance is a risk factor for atherosclerosis and cardiac hypertrophy; it’s essentially growth and size of the heart. So, insulin resistance, in Module 1 we looked at the dangers of sugar, the problem that it creates with diabetes and spiking insulin and all this stuff. This is just another reason why it’s really, really bad to be eating a refined sugar, if you have a lot of refined sugar in your diet.
Insulin ResistanceWhat we have here is the liver as a whole with fat cells or adipose tissue.
Let’s say over time you’ve eaten a lot of sugar and your body continues to pump out insulin; over time what happens is, your cells will no longer respond to the high amounts of insulin in your blood, and that’s known as insulin resistance.
Eventually, we have a problem called dyslipidemia, or high levels of lipids in the blood. This is caused by high levels of insulin, increased production of glucose in the liver, and a decreased disposal of glucose. There are three factors involved here: increased sugar production in the liver, glucose; its inability to get rid of it; and high levels of insulin in the blood.

21Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
When you’re insulin-resistant, it activates an enzyme known as HSL, hormone-sensitive lipase, inside your fat cells to break down triglycerides into free fatty acids and then, obviously, the glycerol backbone. Because, remember, your cells no longer respond to insulin.
If insulin was working properly with your cells if your insulin levels were higher, it would indicate, “Store this in here,” or “Store sugar in here.” But because your cells no longer respond to insulin, now your fat cells are like there literally is no insulin, so we need to break down fat, and what happens is, when we break down triglycerides, we get free fatty acid chains and the glycerol molecule.
These free fatty acid chains are secreted out into the blood, and they move to the liver. When this happens, free fatty acids are then worked upon by the different enzymes and different pathways in the liver, and they are produced or they turn into triglycerides for storage or they are sent to the mitochondria—remember, the workhorse—to produce energy inside the liver.

22Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Hyperinsulinemia, so high levels of insulin, induces a specific gene inside the liver to activate literally all what are called lipogenic genes. So, high levels of insulin in the blood tells the liver, “Hey, activate lipogenic genes,” which are genes that, essentially, convert stuff into fat. That’s not a good thing. And that is denoted as SREBP-1c. That little thing there, that expression, insulin kind of tells that gene in there to express all the lipogenic genes to start converting stuff into fat.
What ends up happening is that the excess glucose that is produced in the liver is converted into fatty acids. Increased fatty acid production increases the production of malonyl-CoA, right in the middle of this little pathway, which inhibits CPT1, which is the protein that is responsible for fatty acid transport into the mitochondria.
Essentially, what happens is because this malonyl-CoA inhibits this protein from being fatty acids into the mitochondria, now fatty acids are literally all being converted into triglycerides, and that’s why when you have high levels of insulin and you are insulin resistant, there is a preferential conversion of free fatty acids and glucose into triglycerides. And when we have high triglycerides in the liver, those will eventually be packaged as VLDL in the blood.
So, over the years you’ve had a lot of sugar, and at one point there’s too much insulin in your blood because insulin’s released in response to sugar, and now your cells don’t know how to respond to insulin; that’s called insulin resistance. Hormone-sensitive lipase is activated inside the fat cells to break down fatty acids; more fat is produced inside the liver; more triglycerides are produced inside the liver as a result of this, and all of that spews out more VLDL, which is not a good lipoprotein that we want in the blood.
Insulin Resistance EffectsIf we look at this, VLDL, can actually give triglycerides to HDL, which is the good lipoprotein that we want more of, but, again, we don’t want HDL to be carrying triglycerides, because if that happens, if HDL starts to take on triglycerides from VLDL—very low-density lipoprotein to HDL it naturally should not be carrying triglycerides. But if it does, this apoA, this protein will dissociate from this HDL molecule.

23Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
The problem with that is when this happens, this apoA is then excreted in the kidneys, and what happens when that happens is that it reduces the availability of HDL for reverse cholesterol transport, as we’re going to look at in Lesson 3.
The reason HDL is so good is because it takes cholesterol from the cells and brings it back to the liver. That’s known as reverse cholesterol transport. However, if VLDL gives triglycerides to HDL, apoA will dissociate from it, go into the kidneys, and then HDL will be less readily available to move cholesterol from the cells to the liver.
So, VLDL can go that way. The other thing that can happen is, it can actually give more triglycerides to LDL, and we obviously don’t want more LDL in the blood, regardless of whether it contains triglycerides or not. It can go one of two ways.
All of this comes back to the original problem of insulin resistance.
TG Guidelines for AdultsBlood triglycerides are measured using a lipid profile after a 12-hour fast. Generally, you go to the doctor in the morning after sleeping or not having anything to eat for 10 or 12 hours. And this should be done by everyone who’s over the age of 20 every 5 years.
24Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Normal levels for triglycerides are under 115 mg/dl of blood. Borderline high, 151–200. At this point, at about 190 mg/dl, blood begins to thicken, so that’s not a good thing, because if you have thick blood, then you have more strain on your heart. If you have thick blood, you have higher blood pressure, and your heart has to work a lot harder to pump. High triglycerides, 201–499; that’s not where we want to be. Very high, 500 mg/dl or higher. And levels about 500 mg/dl are a potential precursor to pancreatitis, inflammation of the pancreas.
If you think about it, high levels of triglycerides are an indication that there is, first of all, potentially a huge amount of fat coming into your digestive system. And that means that the pancreas is having to pump out a huge amount of lipase, which is one of the enzymes that’s responsible for fat digestion. So, it’s stressing out the pancreas from that level, but it’s also stressing out the pancreas because high levels of triglycerides are also an indication of insulin resistance, and if you have insulin resistance, then the pancreas is continually pumping out more insulin because your cells are not responding to insulin. Therefore, the pancreas secretes more insulin and is overworked and overworked and overworked, so it literally grows in size.
These are American numbers, the mg/dl. If you want to go to Canadian numbers, just divide those numbers by 90 to get mmol/L. Depending on where you are, you might be using either of those numbers, but those guidelines will be the same in mmol/L; just, obviously, they won’t be 150; they might be whatever they are, one-point-something. If you’re in Canada, that’s what you want to be using if your doctor uses mmol/L.
Food Sources of TGsOkay, so food sources of triglycerides. Obviously, fat in food, especially saturated fat, is a source of triglycerides, ’cause we mentioned that triglycerides are broken down and then repackaged as triglycerides. When we eat meat we eat triglycerides. If you think about it, if we were cannibals and we ate humans and if we ate the fat in humans, what would we be eating? We would be eating triglycerides, because our cells store fat as triglycerides.

25Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Refined carbohydrates are bad for triglycerides because they spike insulin levels, which leads to the formation of triglycerides in the liver. Remember, when we eat sugar, it spikes insulin, and if we’re not insulin resistant at that point, the liver and fat cells and muscle cells will store that sugar, and if it’s obviously more than our glycogen storage can handle, then it’ll be converted to fat. A high sugar intake also decreases the removal of triglycerides from the liver, so we’ve got more triglycerides forming in the liver and we have fewer being removed, as we saw in that earlier picture.
Many studies say that carbs as a blanket statement are bad, but the problem with these studies is that, first of all, they’re really giving people straight-up sugar—it’s just like sugar water—or very, very simple forms of sugar, and they’re force-feeding participants.
It’s not a natural kind of ad libitum way of consuming food. They’re force-feeding these individuals high amounts of carbohydrates—usually refined carbohydrates—so, obviously, the results are going to show that carbohydrates are bad, and when people see that, they think, Okay, carbohydrates are making me fat, but that’s not necessarily the case.
If you eat normally to the point of satiation and you’re eating foods high in complex carbohydrates like starchy vegetables, pseudo grains like quinoa, amaranth, millet, buckwheat, there’s not a problem with that. Fruit, there’s a little bit of controversy whether fruit has an impact on triglycerides. Some of the research says it does, so if you are sensitive to triglyceride levels and cholesterol levels in the blood, you may want to tone down the fruit a little bit, but, again, if you’re eating whole fruit, you’re getting the fiber and all the other stuff, so it’s not really that big of an issue.
Be wary of some of the science that’s coming out, saying that all carbs are bad for triglycerides or heart health. But at the end of the day, sugar is deadly. The two food sources of triglycerides are fat and sugar.

26Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
In Sum…In sum, simple sugars from the diet cause the liver to desynthesize fat through de novo lipogenesis. Essentially, fructose, 30 percent of sugar, is converted into fat because of this cool phenomenon.
The more bad fat you eat, the more resistant your cells become to insulin. This has been shown in the research quite extensively, where if there’s more fat inside the cells, eventually, the cells will become resistant to insulin, all other things being equal. You don’t want bad fat; you want good fat. Omega-3s, get that stuff in there; monounsaturated fats. A decent amount of good saturated fats but not too much.
Okay, so all this contributes to insulin resistance, and then from there we have just a whole slew of bad stuff that happens.

27Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Fat Transport after Feeding
On the left here we have the small intestine, we’ve got triglycerides, which are broken down and then reformed in the chylomicrons and stuff. They go to the tissues, they’re stored in there, or they can go to the liver. This just kind of shows the pathway. TG, triglycerides, C, cholesteryl esters, and how they move from the tissues back to the liver.
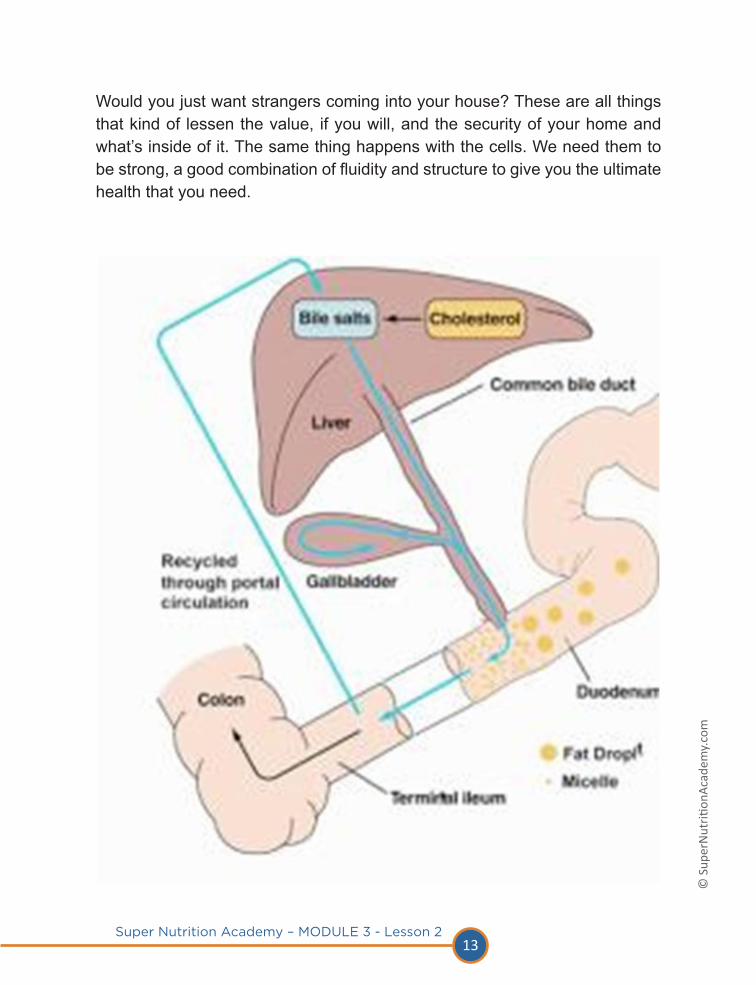
Cholesterol can move from the liver to the tissues. For instance, if cholesterol moves from the liver to the tissues, it’s going to get transported using LDL, which is why we don’t want too much LDL in the blood, because if we have too much LDL, it’s going to be moving a lot of cholesterol to the tissues, where we don’t want it. We want HDL, which is reverse cholesterol transport, where it takes the cholesterol from the tissues, moves it to the liver, and then the liver can say, “Okay, we have too much cholesterol. We can get rid of that cholesterol through the common bile duct and out into our poop, or we will reuse that cholesterol, turning it into bile, and then we’ll use that bile to emulsify fats further in the small intestine.”

28Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Lipoprotein Formation
Let’s say you have the fat in the steak; it’s a triglyceride. It’s then broken down into fatty acids and a monoglycerides or a glycerol molecule.
Again, they’re broken down; they’re then repackaged into a chylomicron. At the same time cholesterol from the food that you eat is broken down into a fatty acid, plus cholesterol. The cholesterol will then combine with the fatty acid that is kind of circulating in the lumen of the small intestine to form a chylomicron. And this is an epithelial cell; this is the cell kind of adjoining right beside the small intestine. Once chylomicron is formed, it will then move into the lymph, which is like the drainage system of the body, and it will then be dumped out into the blood. That’s the first part.

29Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
We’ve got the intestines. We have a chylomicron. This chylomicron, now that it’s in the blood after it’s been dumped out of the lymph, it will be given two proteins, apoE and apoC-II. These are just two examples; there are many other different apoproteins, but we’ll just, for this example, use these two.
They’re donated by HDL, so HDL, through its recycling process, will give off two of these different proteins. And then this chylomicron will then go to the tissues; so, it might go to the fat cells, for instance. It will then bind with a receptor, basically lipoprotein lipase, which is an enzyme, at the fat tissue here. What will happen next is that will allow the tissues to kind of vacuum in the triglycerides. Remember, the orange part is the triglycerides; the yellow is the cholesteryl ester.
This chylomicron is now smaller because the tissues have now taken up these triglycerides, or more of the triglycerides, into the tissue, and what happens next is, we have a smaller molecule. Then, as this chylomicron remnant will leave the tissue, leave the fat cell, it will give back this apoC-II or a different apoprotein to HDL, so say, “Thank you very much for giving this to me. I’m going to give it back to you,” because it needed that protein to bind to the fat cell. It needed that, as you can see how the receptor, the lipoprotein lipase and the apoC-II kind of combine nicely, so now it can give back that protein to the HDL ’cause it doesn’t need it anymore.
It then leaves the fat tissue, and it’s now become a chylomicron remnant, so it’s a remnant of whatever it was before, and it still has this particular kind of triangle protein on it, which will then combine with an LDL receptor at the liver. Okay, so this is the liver down here, this brown triangle. And the liver will then take in this chylomicron remnant. So, it’s kind of like this protein has bound to the receptor on the liver; the liver says, “Come on in.” It takes the chylomicron in, which now has a smaller amount of triglycerides but still has a good amount of cholesteryl ester, as you can see in the yellow, and takes it into the liver. That’s the first part of this cycle.
We see the chylomicron from the small intestine. We’ve had some food. Now it needs to get rid of; it needs to move this fat. So, it’s like this big moving truck. It takes all of this stuff from your house, it brings it over to a storage facility,
30Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
which is your fat, and it drops off a bunch of the furniture. It still has some furniture in the truck ’cause it can’t get rid of all of it, and then it moves over to the liver for further processing.
VDL Formation
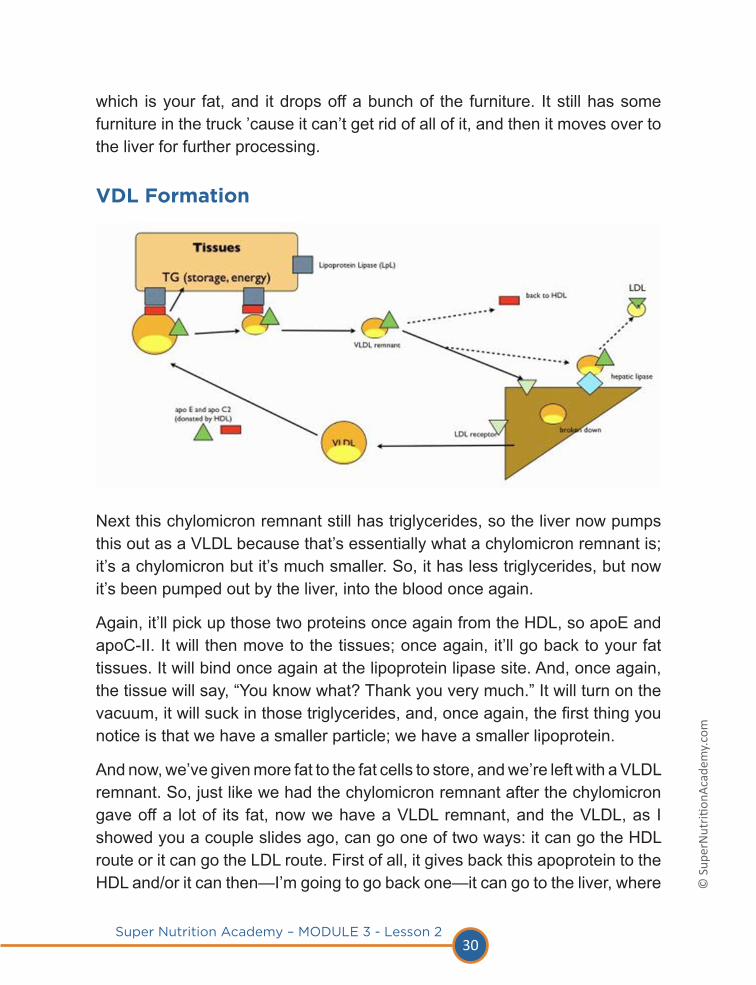
Next this chylomicron remnant still has triglycerides, so the liver now pumps this out as a VLDL because that’s essentially what a chylomicron remnant is; it’s a chylomicron but it’s much smaller. So, it has less triglycerides, but now it’s been pumped out by the liver, into the blood once again.
Again, it’ll pick up those two proteins once again from the HDL, so apoE and apoC-II. It will then move to the tissues; once again, it’ll go back to your fat tissues. It will bind once again at the lipoprotein lipase site. And, once again, the tissue will say, “You know what? Thank you very much.” It will turn on the vacuum, it will suck in those triglycerides, and, once again, the first thing you notice is that we have a smaller particle; we have a smaller lipoprotein.
And now, we’ve given more fat to the fat cells to store, and we’re left with a VLDL remnant. So, just like we had the chylomicron remnant after the chylomicron gave off a lot of its fat, now we have a VLDL remnant, and the VLDL, as I showed you a couple slides ago, can go one of two ways: it can go the HDL route or it can go the LDL route. First of all, it gives back this apoprotein to the HDL and/or it can then—I’m going to go back one—it can go to the liver, where

31Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
it will then bind to the LDL receptor site for further breaking down. So, at this point it can go to the liver to be broken down or it can go to hepatic lipase, which is another enzyme on the liver where the hepatic lipase will take in the extra triglycerides into the liver and then give off LDL as the final by-product.
This is happening all the time. What we don’t want to have happen is, we don’t want to have too much VLDL floating around; we don’t want to have too much LDL floating around, and we’re going to look at why specifically in the next lesson we don’t want too much of this. Essentially, these are the two molecules; these are two very big, problematic molecules, VLDL and LDL. We want more of the HDL for ultimate heart health.
Blood Fat MeasurementsA lipid profile should be done after about a 10- or 12-hour fast. We’re looking at total serum triglyceride. When a doctor says your triglycerides are 120, what that means is that is your triglycerides in VLDL. Not in the chylomicron; we’re looking at the actual triglycerides in the very low-density lipoprotein. That’s what the measurement is. Total cholesterol is the cholesterol contained in HDL and LDL.
It’s not the total cholesterol you should be worried about, but these are two indicators that you want to be looking at. You want to know your total cholesterol so you can work from that. First indicator you want to look at is your HDL-to-total cholesterol ratio; it should be 25 percent. And this is more important than your basic LDL levels. So, we’re looking at of your total cholesterol, how much of your total cholesterol is HDL? We want at least 25 percent of it to be HDL. That’s the first indicator we want to look at.
The second indictor is the triglyceride-to-HDL level, where the ratio should be below two. We’ll look at an example of this. And, again, for our Canadians, divide by 90 for the triglycerides level and divide by 40 for the cholesterol level.
32Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
comDesirable Blood Cholesterol Levels
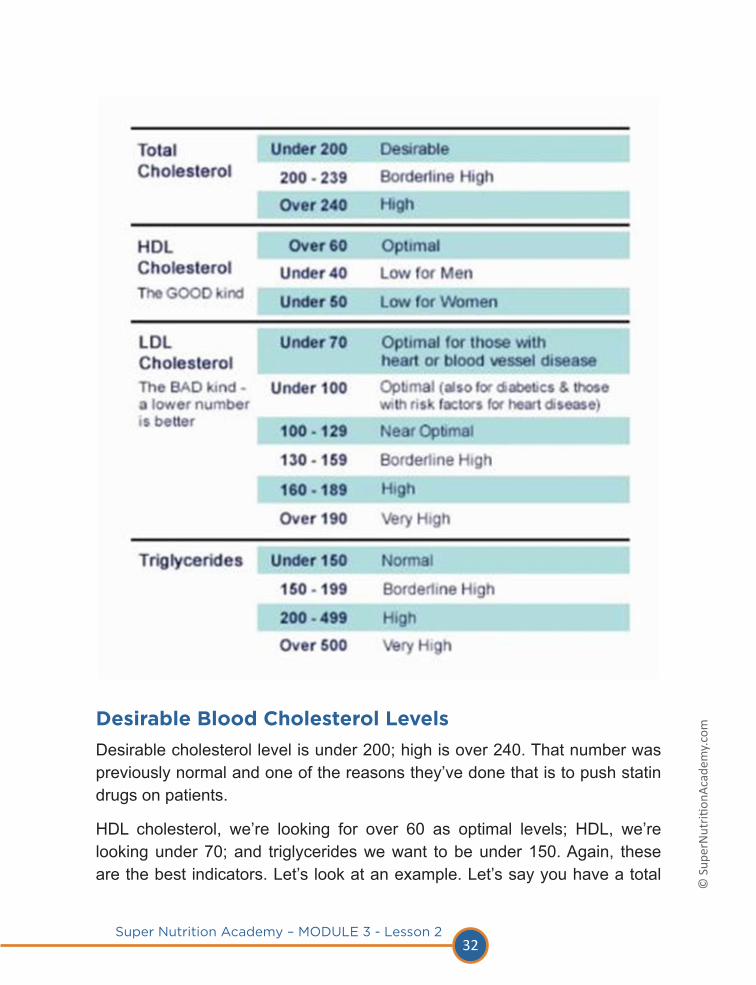
Desirable cholesterol level is under 200; high is over 240. That number was previously normal and one of the reasons they’ve done that is to push statin drugs on patients.
HDL cholesterol, we’re looking for over 60 as optimal levels; HDL, we’re looking under 70; and triglycerides we want to be under 150. Again, these are the best indicators. Let’s look at an example. Let’s say you have a total

33Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
cholesterol of 220. Your HDL is 50, which is a little bit lower than optimal. Your LDL is 50. That obviously doesn’t really add up to 220, but there are obviously a couple other little lipoproteins in there that would make up the difference, so let’s just say that it equals what it does, about 200. Generally, it should be 220, but, again, that doesn’t account for those different lipoproteins that might be in there.
So, your LDL’s 150, which, again, is borderline high; and triglycerides are 160 mg/dl. Over the gamut of these different measurements, we’ve noticed that you’re kind of borderline, borderline high for total cholesterol, under optimal for HDL, borderline high for LDL, and borderline high for triglycerides. That’s great and all, but we want to look specifically at the relationships here.
HDL to total cholesterol. What is the percentage of HDL to your total cholesterol? It’s 23 percent. So, again, it’s a little bit low. We want it to be 25 percent or higher. All I did there is I did 50 ÷ by 220 X 100, and that gives me 23 percent. If it was 60, the optimal range, 60 ÷ 220 would give me 27 percent. So, that’s where I’d like to be, or that’s where you’d like to be, at least 25 percent or higher.
The second one we’re looking at is, triglycerides to HDL should be two or lower. In this case we’re at 3.2, which is obviously high, and we don’t want to be there. All I did there in this example, I did 160 (that’s the triglycerides) divided my HDL, which is 50; it gives me 3.2.
If you know your numbers, if you’ve done a lipid profile with your doctor and you know your numbers, you can just plug those numbers in to this equation, and you’ll know where you stand. Cool? Awesome.
TG in Blood Determined By…Okay, so triglycerides in blood determined by—we’ve seen that it’s the measurement of the triglycerides in the VLDL, in that lipoprotein. There are a couple determinants. How much triglycerides you have coming in is determined by your diet. Drugs, for instance, alcohol, and estrogen can increase VLDL. And, also, if you have a high-estrogenic diet, so if you eat a lot of soy, stuff like that, can increase VLDL. Genetics, obviously, genetics isn’t always great. For instance, the ability to absorb triglycerides and synthesize apoproteins is

34Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
a limiting factor depending on your genes. And then how easily your body can get rid of triglycerides is determined by genetics, metabolism, and specifically with respect to insulin resistance or low insulin.
If you have low lipoprotein lipase—remember that enzyme on the fat cells, at the tissues—if you have low amounts of that lipase, well then, you’re not going to be able to take up as much triglyceride into your cells for storage; therefore, you’re going to have higher triglycerides and higher VLDL in your blood. And insulin resistance or low insulin will negatively impact that lipoprotein lipase enzyme. So, just another reason you don’t want to become insulin resistant. Therefore, you don’t want to eat sugar. It’s all coming back to sugar to a great extent.
Summing UpWe’ve looked at how the quality of your cells membranes really determines your health. Cholesterol and high-quality fats, EFAs, monounsaturated fats are integral components. Triglycerides are problematic and greatly enhanced by a high-sugar and high-saturated fat diet. And the two most important ratios to look for in a lipid profile are: HDL-to-total cholesterol should be 25 percent or higher; and triglycerides to HDL should be 2 percent and lower.

35Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Your Assignment
Your assignment for this lesson is very simple. If you haven’t done so already, schedule an appointment with your doctor or blood clinic to run a lipid profile. Now, it might take a couple days or a couple weeks to get the information back, but once you do, use the simple equations we just looked at to see where you are. Just take your numbers, plug ’em in to those two equations we just looked at, and then you’ll kind of know where you stand.

36Super Nutrition Academy – MODULE 3 - Lesson 2
© S
uper
Nut
rition
Acad
emy.
com
Coming in Part 2 (Lesson 3)In Lesson 3, we’re going to be taking a kind of deeper look at cholesterol. We’re going to take those processed maps, where I showed you how VLDL and HDL were formed and how it kind of gives off LDL and all that kind of stuff; I’m going to make sense of all that for you. We’ll touch upon that at the beginning of the lesson so we kind of get a little refresher, and then we’ll move right into that stuff. We’ll look at the difference between HDL and LDL cholesterol; the truth about cholesterol-lowering drugs; how doctors have been influenced by drug companies and the shocking new trend that’s putting an end to all of it; and eight ways to manage your cholesterol naturally.
That’s what we’ll be discussing in the next lesson. I hope this lesson has made sense of the importance of cell membranes, the importance of the quality of fats you’re eating, and how fats are digested and transported throughout your body and how all of that relates to triglyceride and cholesterol levels that you see on your blood profile or your lipid profiles when you go to your doctor.