modelling the potential economic impact of investment in public health professor malcolm whitfield...
TRANSCRIPT
Modelling the potential economic impact of investment in Public
Health
Professor Malcolm Whitfield Director of The Centre for Health & Social Care Research
Sheffield Hallam University, UK

The Key Problem

“In the most industrialized countries of North America, Europe and the Asian Pacific, at least one-third of all disease burden is caused by tobacco, alcohol, blood pressure, cholesterol and obesity”.
“More than three-quarters of cardiovascular disease (the world’s leading cause of death) results from tobacco use, high blood pressure or cholesterol, or their combination”.
“Overall, cholesterol causes more than 4 million premature deaths a year, tobacco causes almost 5 million, and blood pressure causes around 7 million”
WHO 2002
The health problem

Issue•If we can get people to change their lifestyle i.e. diet, exercise, smoking and alcohol consumption we could reduce the burden of disease in society by up to 33% and reduce the cost of healthcare by over 70%
Questions•How much would we have to change the risk factors to reduce the burden of disease? •What order of savings could we achieve on healthcare costs in the first five years?•How much could we realistically invest in getting lifestyle change?
The model idea
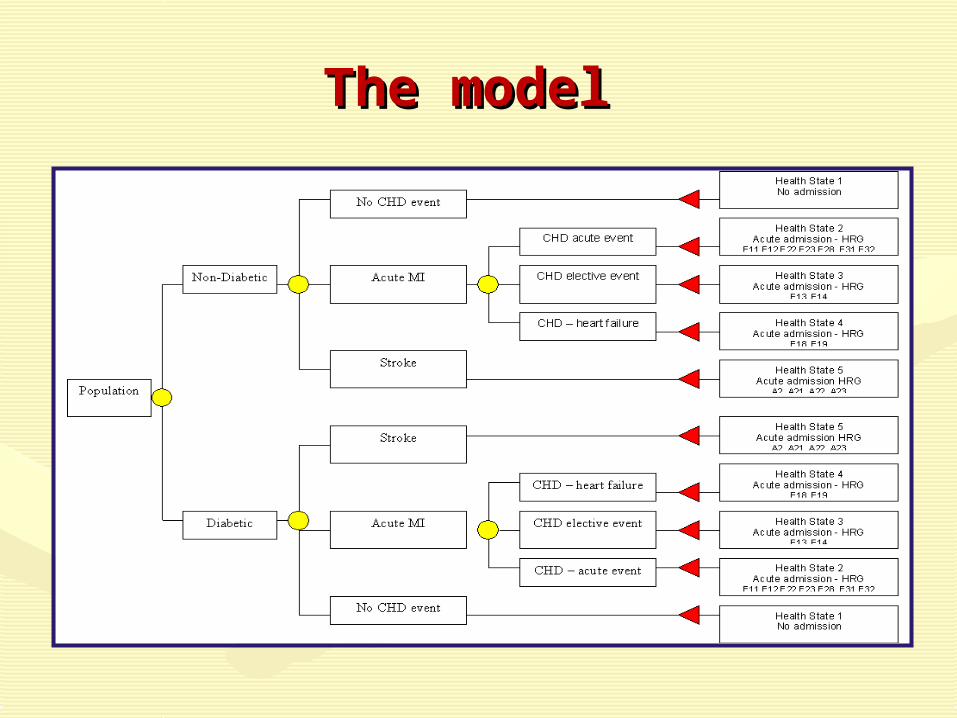
The model The model

The risk factorsThe risk factors
Demographic profile Framingham
Population smoking rates Framingham
Mean total and HDL Cholesterol (mmol/l)
Framingham
Mean systolic blood pressure Framingham
Mean Body Mass Index (BMI) Diabetes / Heart Failure
Mean HBA1c levels UKPDS
Measures of CKD prevalence eGFR etc
Nanes II
Does it work?Does it work?
To validate the model, we estimated how many people in five Primary Care Trusts (n=620,000 population) would have a heart attack, stroke, heart failure, kidney failure and heart surgery.
We then compared the predicted number with the actual number
NB The models has since been tested in 15 PCTs

The validation – S/Yorks
Admission data 2005/06 for 5 PCTs
0500
1000150020002500300035004000
P op. 1 P op. 2 P op. 3 P op. 4 P op. 5 All P ops.
All acute MI events - actual v predicted adjusted (Brindle 2003)
Actual Predicted Adjusted

The validation - Liverpool
0
1000
2000
3000
4000
5000
6000
7000
16-24 25-24 35-44 45-54 55-64 55-74 75+ All events
All acute CHD events - actual v predicted Liverpool PCT (Weighted population)
Actual Predicted

The validation - Birmingham
02000400060008000
1000012000140001600018000
16-24 25-24 35-44 45-54 55-64 55-74 75+ All events
All acute CHD events - actual v predicted Birmingham PCTs
Actual Predicted

Admissions avoided (364,912
pop)
Estimated reduction in annual acute events/admissions over a five year period assuming 20% move toward risk factor reduction target per annum
0
1,000
2,000
3,000
4,000
5,000
6,000
Baseline Year 1 Year 2 Year 3 Year 4 Year 5
Scenario 1 Scenario 2
Scenario Annual acute admission events avoided after 5 years
5 year cumulative acute admission events avoided
Current risk 0
0
Scenario 1 1,707
5,120
Scenario 2 1,075
3,225

Deaths avoided (364,912 pop)
Estimated reduction annual premature deaths over a five year period assuming 20% move toward risk factor reduction target per annum
0
500
1,000
1,500
2,000
2,500
Baseline Year 1 Year 2 Year 3 Year 4 Year 5
Scenario 1 Scenario 2
Scenario Annual premature deaths avoided after 5 years
5 year cumulative premature deaths avoided
Current risk 0
0
Scenario 1 490
1,470
Scenario 2 326
979
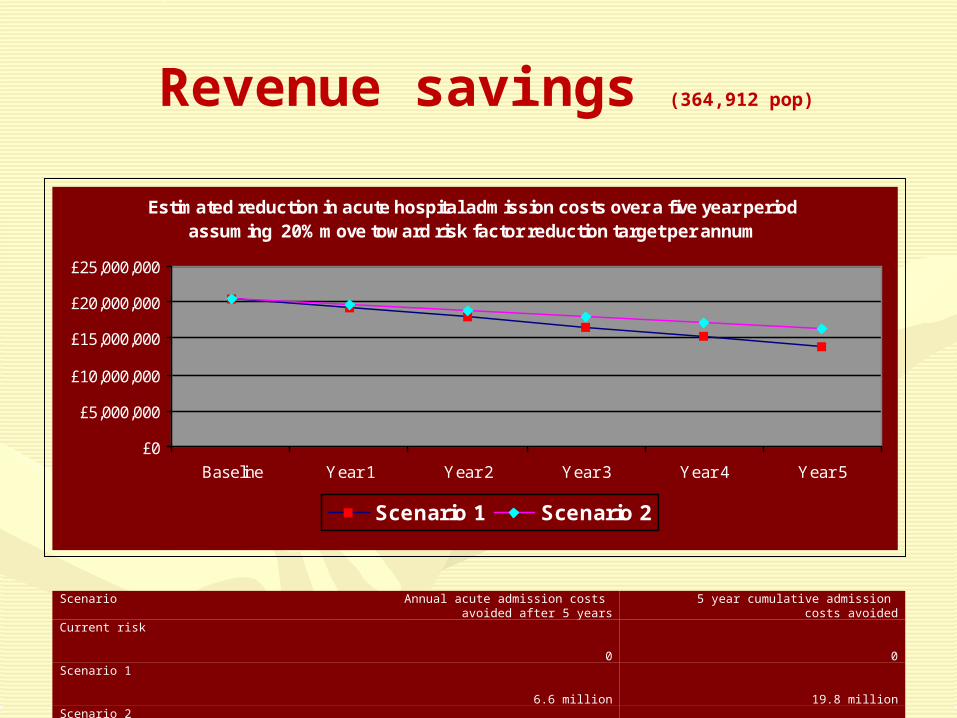
Revenue savings (364,912 pop)
Estimated reduction in acute hospital admission costs over a five year period assuming 20% move toward risk factor reduction target per annum
£0
£5,000,000
£10,000,000
£15,000,000
£20,000,000
£25,000,000
Baseline Year 1 Year 2 Year 3 Year 4 Year 5
Scenario 1 Scenario 2
Scenario Annual acute admission costs avoided after 5 years
5 year cumulative admission costs avoided
Current risk 0
0
Scenario 1 6.6 million
19.8 million
Scenario 2 4.1 million
12.5 million

Estimated impact of health determinants on Estimated impact of health determinants on population healthpopulation health
Key
10% Physical Environment15% Genetic endowment25% Health System50% Socio-economic environment

Linkage to Decipher model
Original model

North Karelia
Main risk factors in North Karelia between 1972 and 2007 among men and women aged 30-59 years
DeathsRate in 1969-1971
Rate in 2006 Change from 1969-1971 to 2006
All causes 1509 572 -62%
All cardiovascular 855 182 -79%
Coronary heart disease
672 103 -85%
All cancers 271 96 -65%
Lung cancers 147 30 -80%
Age-adjusted mortality rates of coronary heart disease in North Karelia and the whole of Finland among males aged 35–64 years from 1969 to 2006.

Nuffield Bio-Ethical
http://www.nuffieldbioethics.org/news/council-cited-white-paper-public-health

Public health intelligence (case finding)
Pathway to equality Pathway to equality
EPHP'sEngagem
ent
Social marketing Health- literacy Informed choiceEnvironmental initiatives
Lifestyle change: Health Trainers Smoking Cessation Five a day Healthy schools meals Housing Green spaces Etc…
Primary care: StatinsHypotensivesObesity treatments
PH Intelligence Public Health Interventions Primary care
TE TETETE TE
AE
(Example) - CVD
Cardiac risk checks Disease registers
TE

http://www.sportseng.org/sheftool//
Decipher model