modeling the ebola outbreak in west africa, march 10th 2015 update
TRANSCRIPT

DRAFT – Not for a.ribu2on or distribu2on
Modeling the Ebola Outbreak in West Africa, 2014
March 10th Update
Bryan Lewis PhD, MPH ([email protected]) presen2ng on behalf of the Ebola Response Team of
Network Dynamics and Simula2on Science Lab from the Virginia Bioinforma2cs Ins2tute at Virginia Tech
Technical Report #15-‐018

DRAFT – Not for a.ribu2on or distribu2on
NDSSL Ebola Response Team Staff: Abhijin Adiga, Kathy Alexander, Chris Barre., Richard Beckman, Keith Bisset, Jiangzhuo Chen, Youngyoun Chungbaek, Stephen Eubank, Sandeep Gupta, Maleq Khan, Chris Kuhlman, Eric Lofgren, Bryan Lewis, Achla Marathe, Madhav Marathe, Henning Mortveit, Eric Nordberg, Paula Stretz, Samarth Swarup, Meredith Wilson,Mandy Wilson, and Dawen Xie, with support from Ginger Stewart, Maureen Lawrence-‐Kuether, Kayla Tyler, Bill Marmagas Students: S.M. Arifuzzaman, Aditya Agashe, Vivek Akupatni, Caitlin Rivers, Pyrros Telionis, Jessie Gunter, Elizabeth Musser, James Schli., Youssef Jemia, Margaret Carolan, Bryan Kaperick, Warner Rose, Kara Harrison 2

DRAFT – Not for a.ribu2on or distribu2on
Currently Used Data (as of March 10th, 2014)
● Data from WHO, MoH Liberia, and MoH Sierra Leone, available at h.ps://github.com/cmrivers/ebola
● MoH and WHO have reasonable agreement ● Sierra Leone case counts censored up
to 4/30/14. ● Time series was filled in with missing
dates, and case counts were interpolated.
3
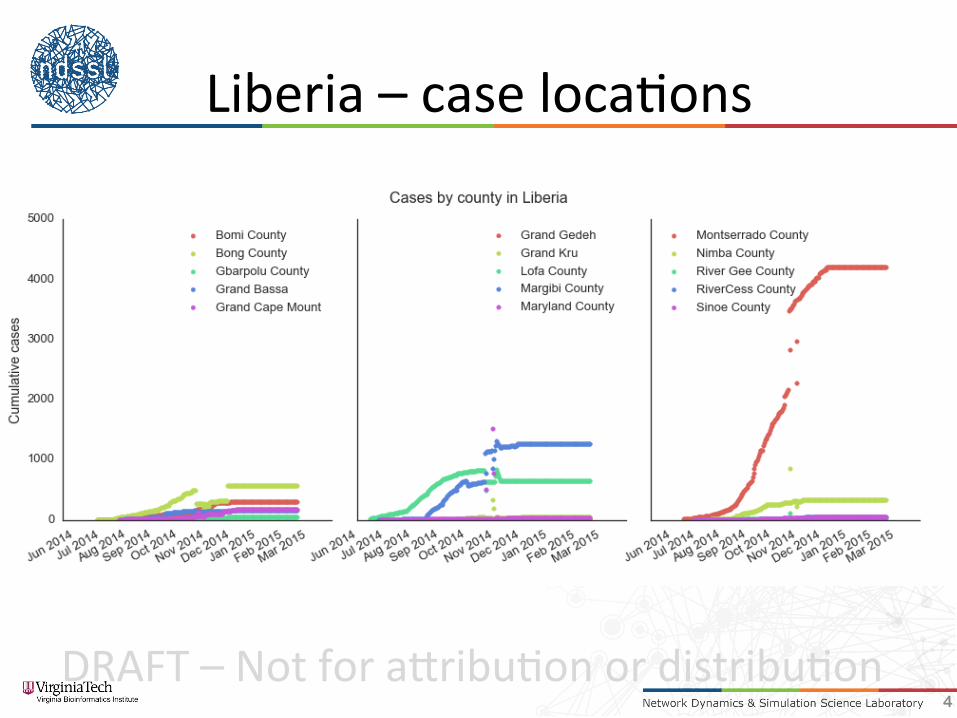
Cases Deaths Guinea 2,871 1,876 Liberia 8,478 3,605 Sierra Leone 10,340 3,145 Total 21,724 8,641
DRAFT – Not for a.ribu2on or distribu2on
Liberia – case loca2ons
4

DRAFT – Not for a.ribu2on or distribu2on
Liberia infec2on rate
5

DRAFT – Not for a.ribu2on or distribu2on
Papers in Submission
• Assessing the Impact of Increased Hospital Capacity on the Ebola Epidemic in Liberia
• Es:ma:ng the Role of Infec:on Control in Containing the Ebola Epidemic in Liberia – First paper looks at the likely effect of the construc2on of ETUs in Liberia in the context of the behavior changes we’ve also seen.
– Second paper compares the rela2ve effect of ETU construc2on with improved infec2on control

DRAFT – Not for a.ribu2on or distribu2on 7
Green line, which models the ETU deployment, a reduc2on in 2me to hospitaliza2on and a change in community behavior is the only combina2on that fits the observed data. No single change accounts for the observed decrease – both ETUs and the behavioral shil were important.

DRAFT – Not for a.ribu2on or distribu2on 8
Similar to the previous plot – very high levels of infec2on preven2on within the constructed ETUs, along with behavioral changes, fit the epidemic. Minor decreases in the quality of infec2on preven2on (supply shortages, lack of training, errors etc.) cause a substan2al increase in the number of cases.

DRAFT – Not for a.ribu2on or distribu2on 9
Comparing ETU deployment to improving infec2on control: • Changes in infec2on control
(going from ideal to less-‐than-‐ideal scenarios for preven2ng within hospital transmission) have a bigger impact on cases than halving or doubling the number of ETUs.
• Appropriate training and supplies to respond to an outbreak are essen2al.
• However, ETUs also have a substan2al impact on the outbreak.
• If possible, do both, but supplies and training can occur very early in a response.
Comparing ETU deployment to improving infec2on control

DRAFT – Not for a.ribu2on or distribu2on
Vaccine Stockpile Study ObjecAve: Assuming that early deployment of vaccine interven2ons, what vaccine stockpile is necessary to control a reasonably stressful outbreak like the 2014 West African outbreak?
10

DRAFT – Not for a.ribu2on or distribu2on
Vaccine Stockpile Study
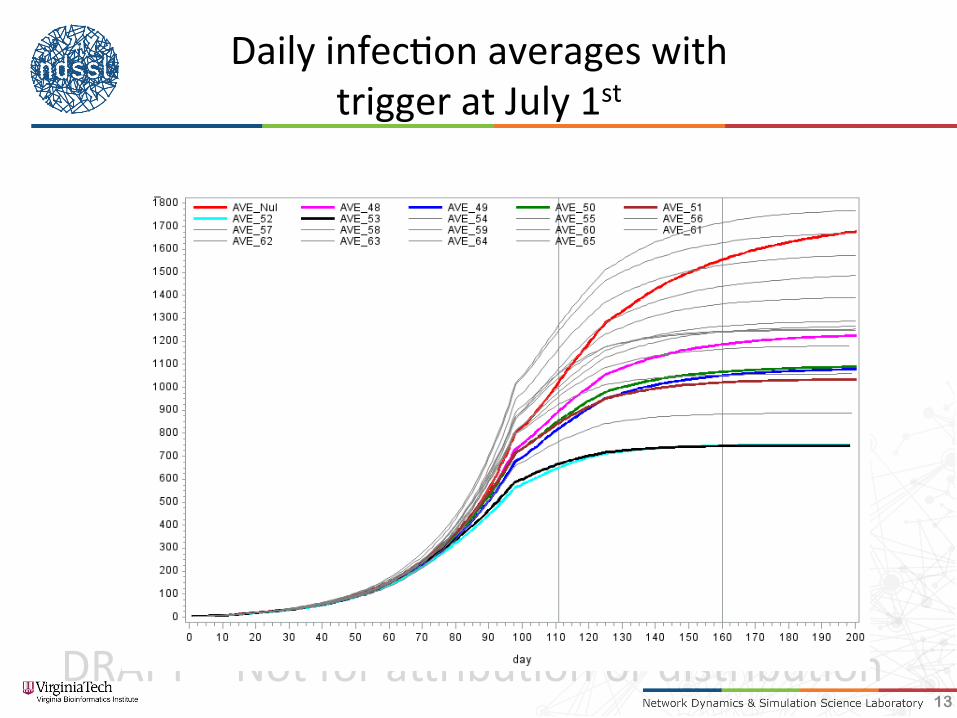
Intervened PopulaAons: school-‐aged and older IntervenAon sweep: July 1st, July 16th, Aug 1st Doses: 3k, 5k, 10k Compliance: 25%, 50%, 75% Efficacy: 50%, 80%
11

DRAFT – Not for a.ribu2on or distribu2on
Vaccine Stockpile Study
• Ini2al seeds in Lofa County • At designated 2mes, vaccine campaigns start • Ring vaccina2on with compliance levels • Addi2onal vaccine provided to others in vaccina2on area (Lofa county) ~100
• Campaign con2nues 2ll stockpile exhausted
12
DRAFT – Not for a.ribu2on or distribu2on
Daily infec2on averages with trigger at July 1st
13

DRAFT – Not for a.ribu2on or distribu2on
Daily infec2on averages with trigger at July 16th
14

DRAFT – Not for a.ribu2on or distribu2on
Daily infec2on averages with trigger at August 1st
15

DRAFT – Not for a.ribu2on or distribu2on
Comparison – 10k doses
16
6 weeks aler start of campaign 3 months aler start of campaign
DRAFT – Not for a.ribu2on or distribu2on
Vaccine Stockpile Study
• To be assessed: – Across mul2ple doses – Number of replicates where epidemic dies out – Number of replicates where epidemic is sufficiently reduced that other “classic” measures can maintain and complete control
– Number of cases that escape Lofa county
17