mobilizing teams for change: the power of improvement collaboratives in mnch programs youssef...
TRANSCRIPT

Mobilizing Teams for Change: The Power of
Improvement Collaboratives in MNCH Programs
Youssef Tawfik, MBBCH, MPHSr. Quality Improvement Advisor, MNCH University Research Co.,
Reconvening Bangkok: 2007 to 2010 March 6-11, 2010.

What are the quality obstacles?
Resources Processes Results (Outcomes)
Non-compliance with standards
Poor organization of care (inefficiency)
Not sensitive to client needs
Inadequate health services delivered
Negative health outcomes
Poor client satisfaction
Lack updated standards
HR shortage
Poor Providers’ skills
Weak Infrastructure
Weak Health systems
Poor access to care

The Basic Principles of Quality Improvement
• Understand client needs
• Understand the system and processes of care
• Teamwork
• Measure results
• MAKE CHANGES

Definition of an Improvement Collaborative
An Improvement Collaborative is an organized network of a large number of sites (e.g. districts, facilities or communities) that work together for a limited period of time, usually 9 to 24 months, to rapidly achieve significant improvements in a focused topic through shared learning and intentional spread methods.
The system, processes, quality and efficiency of care are to be improved.
Components of Improvement Collaboratives
• Network of participating organizations/sites involved in shared learning
• Quality Improvement (QI) team at each site• Focused on one clinical/public health topic• Work to find better ways to implement best practices and
achieve better results• Regular communication between sites• Common key indicators reported and shared monthly

Two Types of Collaboratives• Demonstration collaborative: 15-60 sites who
work intensively for 9 to 24 months to adapt to their local situation a best model of care.
• Spread collaborative: 40 to 150 sites who work for 12 to 24 months to spread to their sites the best practices and solutions developed in the demonstration collaborative

What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
From: Associates in Process Improvement

Accelerating Improvement for Rapid Results

PharmacistNurse(s) Physican
Lab technician
Manager
Who would be a member of the quality improvement team?
All the people who are involved in the particular
process of care at each site
Midwife

Spread of MNCH interventions through collaboratives
Demonstration
slice
Collaborative = multiple sites working simultaneously and learning together to improve specific MNCH services’ and systems’ indicators.
Regional QI team
District QI team
District 2
District 3
District 1
National QI team

Case example: Russia - Organization of Tula Oblast Intentional Spread Collaborative after
Demonstration Collaborative
Arrows show expansion from initial sites to neighboring spread sites
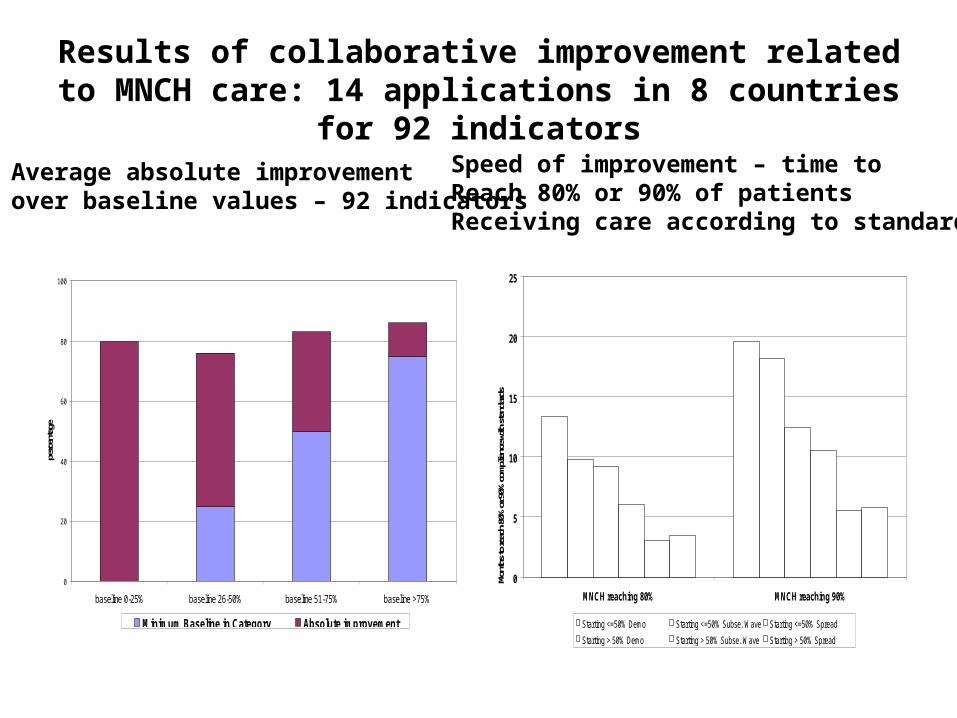
Results of collaborative improvement related to MNCH care: 14 applications in 8 countries for 92 indicators
0
20
40
60
80
100
baseline 0-25% baseline 26-50% baseline 51-75% baseline >75%
perc
enta
ge
Minimum Baseline in Category Absolute improvement
0
5
10
15
20
25
MNCH reaching 80% MNCH reaching 90%
Mont
hs to
reac
h 80%
or 90
% co
mplia
nce w
ith st
anda
rds
Starting <=50% Demo Starting <=50% Subse. Wave Starting <=50% Spread
Starting > 50% Demo Starting > 50% Subse. Wave Starting > 50% Spread
Average absolute improvement over baseline values – 92 indicators
Speed of improvement – time to Reach 80% or 90% of patients Receiving care according to standards

Were gains maintained over time?
Niger MNCH Russia MNCH Ecuador MNCH

Thank You