mobile reminder system for cambodian diabetics -- mopotsyo patient information center
TRANSCRIPT

BRIDGES RESEARCH PROJECT:
MOBILE PHONE DIABETES SELF-MANAGEMENT SUPPORT
MARCH 20, 2014
a 3-country analysis of its implementationin existing Diabetes Self-Management Education Programs in
DR Congo, Cambodia & The Philippines,
Institute for Tropical Medicine (ITM) in Belgium

I. INTRODUCTION OF RESEARCH
• Research Topic: Evaluation of effectiveness of a mobile phone Diabetes Self-Management Support (DSMS) intervention on top of an existing Diabetes Self Management Education (DSME) strategy in 3 countries:
• DR Congo, • Cambodia • Philippines.
• Time period : Sept 2011- Dec 2014
• Beneficiaries: 484 Diabetes patients in MoPoTsyo peer education network (>8000 Diabetes patients are registered in Cambodia,2013)
• Permission from National Ethical Committee

I. 1. DIABETES PEER EDUCATORPROGRAM (MOPOTSYO )
• Cambodian (NGO) for people with chronic
Non Communicable Disease (NCD): 1. Diabetes & associated diseases (kidney,
cholesterol problems, retinopathy etc.)
2. High Blood Pressure (non-diabetic)
• Poor & Remote communities • Not clinic-based, but community-based
• Peer Education Networks provide care and access through Peer Educator to medical services
• National Strategy for Prevention of NCD 2013-2020 recognizes the care system

I. 1. DIABETES PEER EDUCATOR PROGRAM (CONT.)
1. FOLLOW-UP PATIENTS
4
Session group weekly’s and member follow up’s
activities
I. 1. DIABETES PEER EDUCATOR PROGRAM (CONT.)
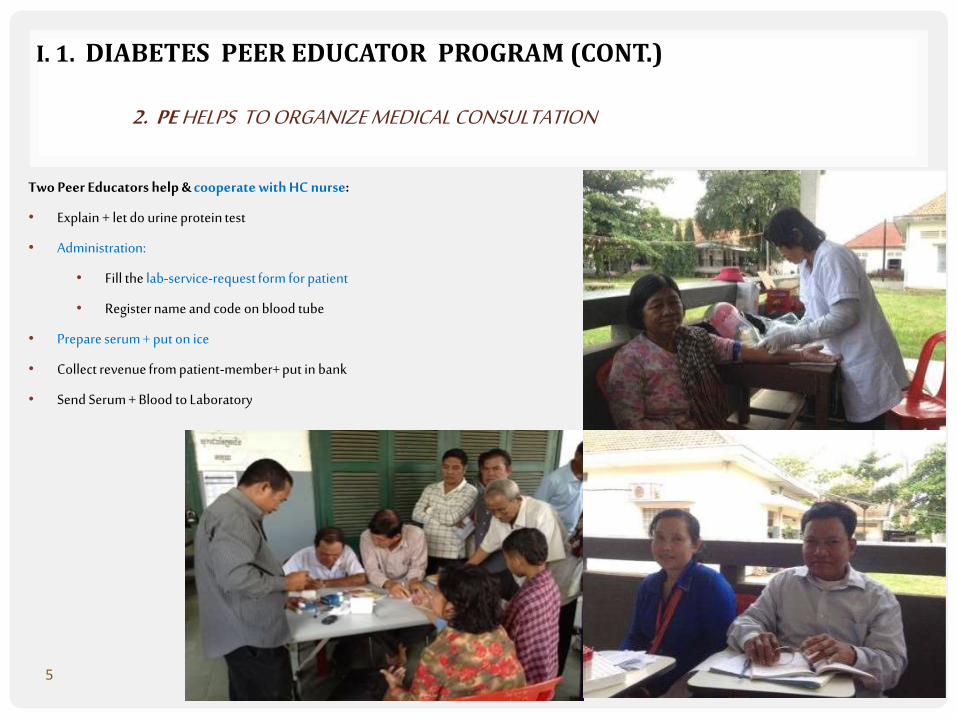
2. PE HELPS TO ORGANIZE MEDICAL CONSULTATION
5
Two Peer Educators help & cooperate with HC nurse:
• Explain + let do urine protein test
• Administration:
• Fill the lab-service-request form for patient
• Register name and code on blood tube
• Prepare serum + put on ice
• Collect revenue from patient-member+ put in bank
• Send Serum + Blood to Laboratory

I. 2. OBJECTIVES OF RESEARCH PROJECT
To evaluate the effectiveness of a mobile phone DSMS intervention:By assessing the differences before and after the intervention:Between the DSME and the DSME+DSMS groups In each country on:
1. health outcomes:• HemoglobinA1C (HbA1C) • blood pressure• Body Mass Index (BMI) & waist circumference• percentage of people with diabetic foot problems
2. Adequate use of care resources:• failure-to-attend rate • perceived quality of care• health care expenditure
3. Enablement• level of knowledge on diabetes (care)• self-management and ability to cope• adherence to glucose monitoring & control regimes & healthy lifestyle
To understand the differences in effectiveness of the intervention between countries.
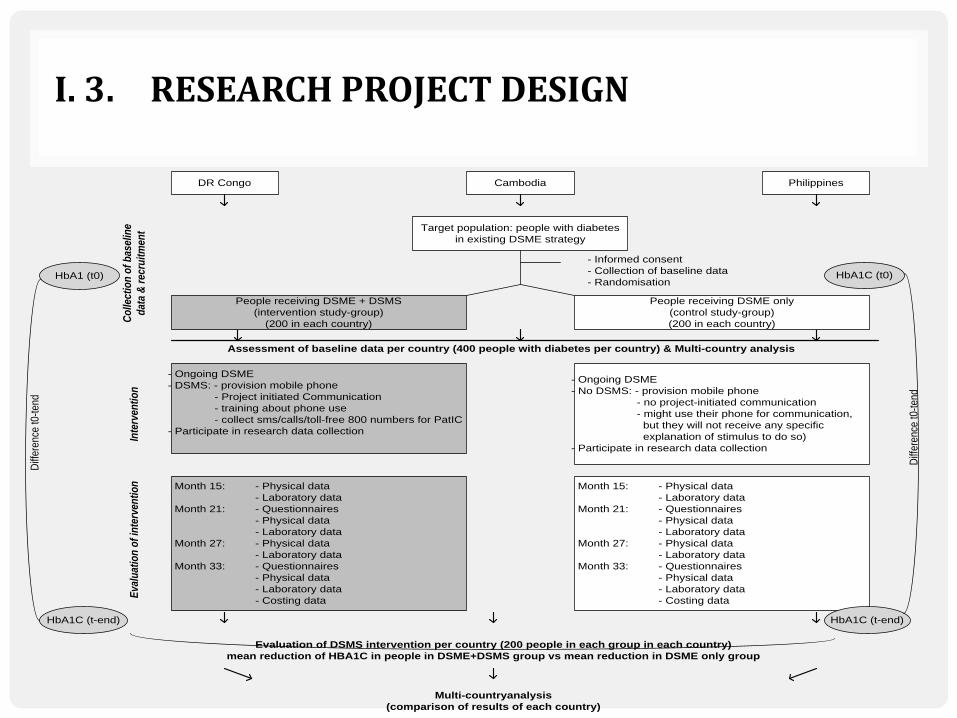
I. 3. RESEARCH PROJECT DESIGN
DR Congo Cambodia Philippines
Month 15: - Physical data
- Laboratory data
Month 21: - Questionnaires
- Physical data
- Laboratory data
Month 27: - Physical data
- Laboratory data
Month 33: - Questionnaires
- Physical data
- Laboratory data
- Costing data
- Informed consent
- Collection of baseline data
- Randomisation
Co
llect
ion
of
bas
elin
e
dat
a &
rec
ruit
men
tIn
terv
enti
on
Eva
luat
ion
of
inte
rven
tio
n
Assessment of baseline data per country (400 people with diabetes per country) & Multi-country analysis
Target population: people with diabetes
in existing DSME strategy
People receiving DSME + DSMS
(intervention study-group)
(200 in each country)
People receiving DSME only
(control study-group)
(200 in each country)
- Ongoing DSME
- DSMS: - provision mobile phone
- Project initiated Communication
- training about phone use
- collect sms/calls/toll-free 800 numbers for PatIC
- Participate in research data collection
Month 15: - Physical data
- Laboratory data
Month 21: - Questionnaires
- Physical data
- Laboratory data
Month 27: - Physical data
- Laboratory data
Month 33: - Questionnaires
- Physical data
- Laboratory data
- Costing data
- Ongoing DSME
- No DSMS: - provision mobile phone
- no project-initiated communication
- might use their phone for communication,
but they will not receive any specific
explanation of stimulus to do so)
- Participate in research data collection
HbA1 (t0)
HbA1C (t-end)
Diff
eren
ce t0
-ten
d
HbA1C (t0)
HbA1C (t-end)
Diff
eren
ce t0
-ten
d
Multi-countryanalysis
(comparison of results of each country)
Evaluation of DSMS intervention per country (200 people in each group in each country)
mean reduction of HBA1C in people in DSME+DSMS group vs mean reduction in DSME only group
I. 4. STUDY INTERVENTION: MOBILE PHONE DSMS
• Provision of phones
• Beeline Phone and SIM• Phone is fill account 1$ per 3month (to keep activate)
• Project initiated communication (SMS)
• General knowledge of Diabetes• Diet & Exercise• Glucose monitoring & medication• Foot care• Smoking & Drinking alcohol • Self-recording• Problem solving and Empowerment

I. 5. THE FRONTLINE SOFTWARE
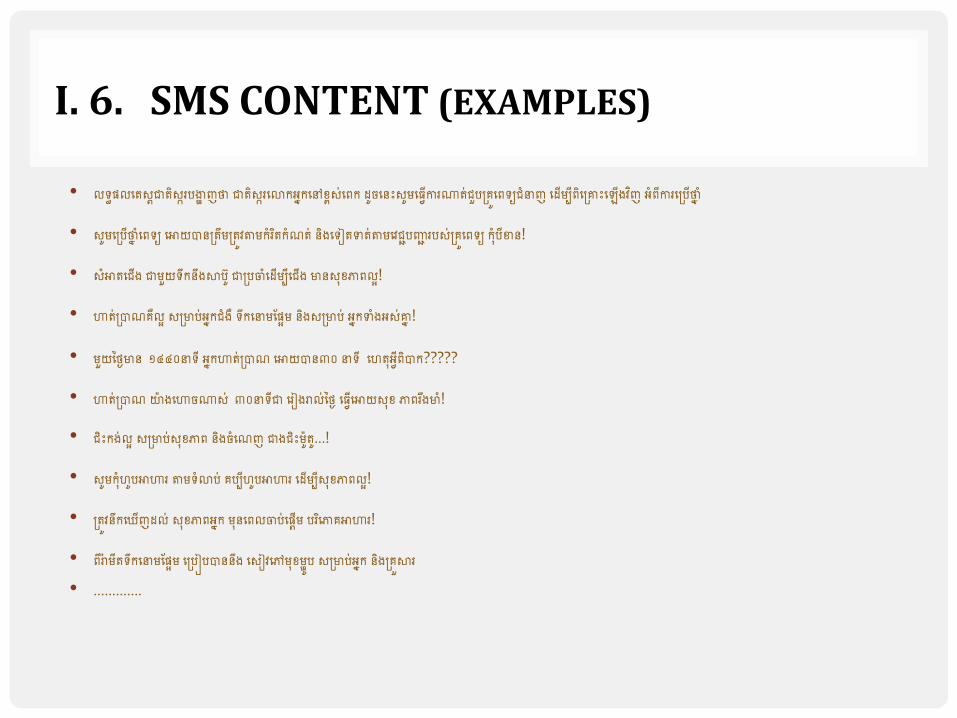
I. 6. SMS CONTENT (EXAMPLES)
• លទ្ធផលតេស្តជាេិស្ករបង្ហា ញថាជាេិស្ករតោកអ្នកតៅខ្ពស្់តេក ដូចត េះស្ូមត្វើការណាេ់ជួបគ្រូតេទ្យជំនាញ តដើមបីេិតគ្រេះត ើងវិញ អ្ំេីការតគ្បើថាន ំ
• ស្ូមតគ្បើថាន ំតេទ្យ តោយបា គ្េឹមគ្េូវតាមកំរិេកំណេ់ ិងតទ្ៀេទាេ់តាមតវជជបញ្ជជ របស្់គ្រូតេទ្យ ក ំបីខា !
• ស្ំោេតជើង ជាមួយទ្ឹក ឹងសាប ូ ជាគ្បចំតដើមបីតជើង មា ស្ ខ្ភាេលអ!
• ហាេ់គ្បាណរឺលអ ស្គ្មាប់អ្នកជំងឺ ទ្ឹកតនាមផ្ផអម ិងស្គ្មាប់ អ្នកទាំងអ្ស្់រន !
• មួយថ្ងៃមា ១៤៤០នាទ្ី អ្នកហាេ់គ្បាណ តោយបា ៣០ នាទ្ី តេេ អ្វីេិបាក?????
• ហាេ់គ្បាណយ៉ា ងតហាចណាស្់៣០នាទ្ីជា តរៀងរាល់ថ្ងៃ ត្វើតោយស្ ខ្ ភាេរឹងមាំ!
• ជិេះកង់លអ ស្គ្មាប់ស្ ខ្ភាេ ិងចំតណញ ជាងជិេះម៉ាូេ.ូ..!
• ស្ូមក ំេូបោហារ តាមទ្ំោប់ របបីេូបោហារ តដើមបីស្ ខ្ភាេលអ!
• គ្េូវ ឹកត ើញដល់ ស្ ខ្ភាេអ្នក ម តេលចប់តផតើម បរិតភារោហារ!
• េីរា៉ា មីេទឹ្កតនាមផ្ផអម តគ្បៀបបា ឹង តស្ៀវតៅម ខ្មាូប ស្គ្មាប់អ្នក ិងគ្រួសារ• ………….

II. PROJECT PROBLEMS AND SOLUTIONS
• Problems• Patient can’t read the text message. • Text message is limited to 1 sms (as protocol)• Patients lost the phone/phone number (no renew provision)• Patients can’t check inbox/inbox is full• Phone number is cutoff from system (no account >6months)• Phone must support KHMER fonts
• Solution• Other household member can read for patients• Form group discuss to create SMS to ensure SMS is simple and
understandable• We top-up account 1$ per 3months for those use Beeline number provided
by research• We ask PE to help delete sms from inbox about one per 4 or 5months• Patients pay their own money to buy new Beeline SIM, just inform us the
new number.
III. VERBOICE INTERVENTION
• Has starting in January 2014
• We send 6 call flows per week
• We can schedule one per week
• We always get warmly technical support from inSTEDD team in Cambodia

IV. SUCCESSES AND CHALLENGES OF VERBOICE
• Successes: • Patients seem happier with voice message
• It works with all number networks and kind of phones
• Challenges• Higher service cost…sustainability?
• With voice message, patients cannot re-listen
• Still some patients “no answer”. Maybe it takes longer time (than sms) for each transaction.
• Some technical errors????

V. CONCLUSION & SUGGESTIONS
• We appreciate verboice system. It is a good alternative solution to sending text messages . We will use this voice message till the end of the project in December 2014.
• Suggestion:
• Could you design for save number with name???
• Could you extend call log more than 10 displays??
• Could you display history of call log by date??? (normally, I did download as “.csv”, then sort by date, does it have another solution??)

THANKS YOU !