mo1005 effect of weight loss on novel mri quantitative changes in liver and pancreatic fat in...
TRANSCRIPT
AA
SL
DA
bst
ract
s
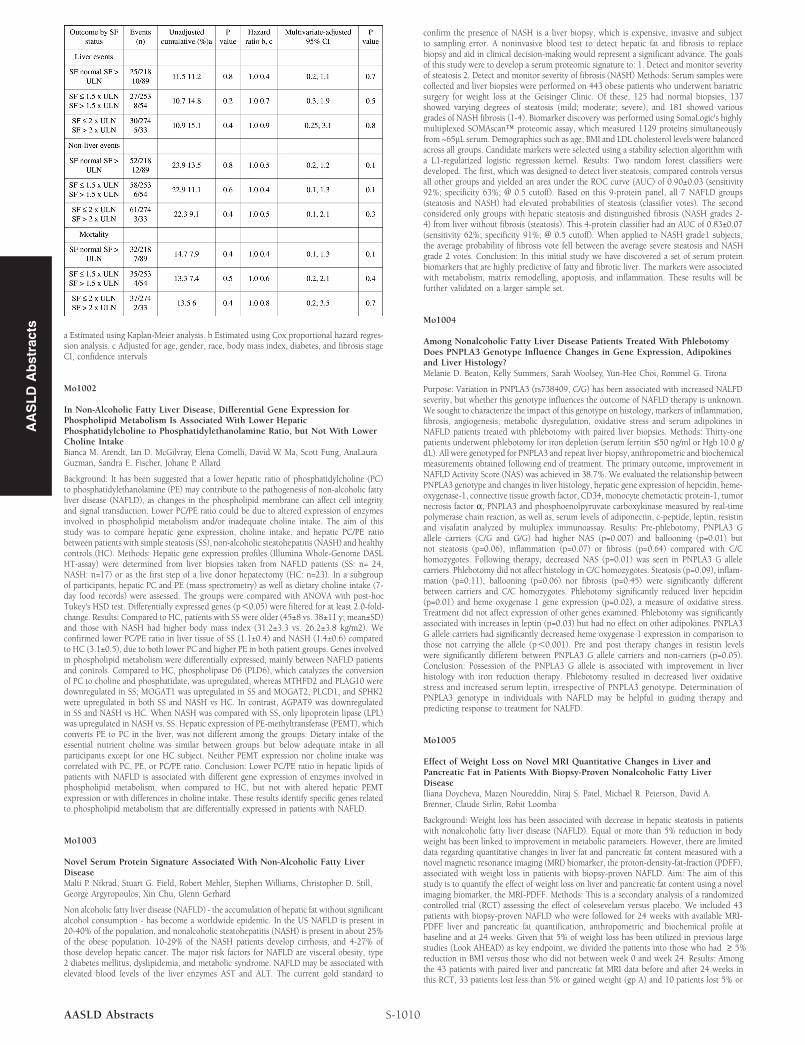
a Estimated using Kaplan-Meier analysis. b Estimated using Cox proportional hazard regres-sion analysis. c Adjusted for age, gender, race, body mass index, diabetes, and fibrosis stageCI, confidence intervals
Mo1002
In Non-Alcoholic Fatty Liver Disease, Differential Gene Expression forPhospholipid Metabolism Is Associated With Lower HepaticPhosphatidylcholine to Phosphatidylethanolamine Ratio, but Not With LowerCholine IntakeBianca M. Arendt, Ian D. McGilvray, Elena Comelli, David W. Ma, Scott Fung, AnaLauraGuzman, Sandra E. Fischer, Johane P. Allard
Background: It has been suggested that a lower hepatic ratio of phosphatidylcholine (PC)to phosphatidylethanolamine (PE) may contribute to the pathogenesis of non-alcoholic fattyliver disease (NAFLD), as changes in the phospholipid membrane can affect cell integrityand signal transduction. Lower PC/PE ratio could be due to altered expression of enzymesinvolved in phospholipid metabolism and/or inadequate choline intake. The aim of thisstudy was to compare hepatic gene expression, choline intake, and hepatic PC/PE ratiobetween patients with simple steatosis (SS), non-alcoholic steatohepatitis (NASH) and healthycontrols (HC). Methods: Hepatic gene expression profiles (Illumina Whole-Genome DASLHT-assay) were determined from liver biopsies taken from NAFLD patients (SS: n= 24,NASH: n=17) or as the first step of a live donor hepatectomy (HC: n=23). In a subgroupof participants, hepatic PC and PE (mass spectrometry) as well as dietary choline intake (7-day food records) were assessed. The groups were compared with ANOVA with post-hocTukey's HSD test. Differentially expressed genes (p,0.05) were filtered for at least 2.0-fold-change. Results: Compared to HC, patients with SS were older (45±8 vs. 38±11 y; mean±SD)and those with NASH had higher body mass index (31.2±3.3 vs. 26.2±3.8 kg/m2). Weconfirmed lower PC/PE ratio in liver tissue of SS (1.1±0.4) and NASH (1.4±0.6) comparedto HC (3.1±0.5), due to both lower PC and higher PE in both patient groups. Genes involvedin phospholipid metabolism were differentially expressed, mainly between NAFLD patientsand controls. Compared to HC, phospholipase D6 (PLD6), which catalyzes the conversionof PC to choline and phosphatidate, was upregulated, whereas MTHFD2 and PLAG10 weredownregulated in SS; MOGAT1 was upregulated in SS and MOGAT2, PLCD1, and SPHK2were upregulated in both SS and NASH vs HC. In contrast, AGPAT9 was downregulatedin SS and NASH vs HC. When NASH was compared with SS, only lipoprotein lipase (LPL)was upregulated in NASH vs. SS. Hepatic expression of PE-methyltransferase (PEMT), whichconverts PE to PC in the liver, was not different among the groups. Dietary intake of theessential nutrient choline was similar between groups but below adequate intake in allparticipants except for one HC subject. Neither PEMT expression nor choline intake wascorrelated with PC, PE, or PC/PE ratio. Conclusion: Lower PC/PE ratio in hepatic lipids ofpatients with NAFLD is associated with different gene expression of enzymes involved inphospholipid metabolism, when compared to HC, but not with altered hepatic PEMTexpression or with differences in choline intake. These results identify specific genes relatedto phospholipid metabolism that are differentially expressed in patients with NAFLD.
Mo1003
Novel Serum Protein Signature Associated With Non-Alcoholic Fatty LiverDiseaseMalti P. Nikrad, Stuart G. Field, Robert Mehler, Stephen Williams, Christopher D. Still,George Argyropoulos, Xin Chu, Glenn Gerhard
Non alcoholic fatty liver disease (NAFLD) - the accumulation of hepatic fat without significantalcohol consumption - has become a worldwide epidemic. In the US NAFLD is present in20-40% of the population, and nonalcoholic steatohepatitis (NASH) is present in about 25%of the obese population. 10-29% of the NASH patients develop cirrhosis, and 4-27% ofthose develop hepatic cancer. The major risk factors for NAFLD are visceral obesity, type2 diabetes mellitus, dyslipidemia, and metabolic syndrome. NAFLD may be associated withelevated blood levels of the liver enzymes AST and ALT. The current gold standard to
S-1010AASLD Abstracts
confirm the presence of NASH is a liver biopsy, which is expensive, invasive and subjectto sampling error. A noninvasive blood test to detect hepatic fat and fibrosis to replacebiopsy and aid in clinical decision-making would represent a significant advance. The goalsof this study were to develop a serum proteomic signature to: 1. Detect and monitor severityof steatosis 2. Detect and monitor severity of fibrosis (NASH) Methods: Serum samples werecollected and liver biopsies were performed on 443 obese patients who underwent bariatricsurgery for weight loss at the Geisinger Clinic. Of these, 125 had normal biopsies, 137showed varying degrees of steatosis (mild; moderate; severe), and 181 showed variousgrades of NASH fibrosis (1-4). Biomarker discovery was performed using SomaLogic's highlymultiplexed SOMAscan™ proteomic assay, which measured 1129 proteins simultaneouslyfrom ~65μL serum. Demographics such as age, BMI and LDL cholesterol levels were balancedacross all groups. Candidate markers were selected using a stability selection algorithm witha L1-regularized logistic regression kernel. Results: Two random forest classifiers weredeveloped. The first, which was designed to detect liver steatosis, compared controls versusall other groups and yielded an area under the ROC curve (AUC) of 0.90±0.03 (sensitivity92%; specificity 63%; @ 0.5 cutoff). Based on this 9-protein panel, all 7 NAFLD groups(steatosis and NASH) had elevated probabilities of steatosis (classifier votes). The secondconsidered only groups with hepatic steatosis and distinguished fibrosis (NASH grades 2-4) from liver without fibrosis (steatosis). This 4-protein classifier had an AUC of 0.83±0.07(sensitivity 62%; specificity 91%; @ 0.5 cutoff). When applied to NASH grade1 subjects,the average probability of fibrosis vote fell between the average severe steatosis and NASHgrade 2 votes. Conclusion: In this initial study we have discovered a set of serum proteinbiomarkers that are highly predictive of fatty and fibrotic liver. The markers were associatedwith metabolism, matrix remodelling, apoptosis, and inflammation. These results will befurther validated on a larger sample set.
Mo1004
Among Nonalcoholic Fatty Liver Disease Patients Treated With PhlebotomyDoes PNPLA3 Genotype Influence Changes in Gene Expression, Adipokinesand Liver Histology?Melanie D. Beaton, Kelly Summers, Sarah Woolsey, Yun-Hee Choi, Rommel G. Tirona
Purpose: Variation in PNPLA3 (rs738409, C/G) has been associated with increased NALFDseverity, but whether this genotype influences the outcome of NAFLD therapy is unknown.We sought to characterize the impact of this genotype on histology, markers of inflammation,fibrosis, angiogenesis, metabolic dysregulation, oxidative stress and serum adipokines inNAFLD patients treated with phlebotomy with paired liver biopsies. Methods: Thirty-onepatients underwent phlebotomy for iron depletion (serum ferritin ≤50 ng/ml or Hgb 10.0 g/dL). All were genotyped for PNPLA3 and repeat liver biopsy, anthropometric and biochemicalmeasurements obtained following end of treatment. The primary outcome, improvement inNAFLD Activity Score (NAS) was achieved in 38.7%. We evaluated the relationship betweenPNPLA3 genotype and changes in liver histology, hepatic gene expression of hepcidin, heme-oxygenase-1, connective tissue growth factor, CD34, monocyte chemotactic protein-1, tumornecrosis factor α, PNPLA3 and phosphoenolpyruvate carboxykinase measured by real-timepolymerase chain reaction, as well as, serum levels of adiponectin, c-peptide, leptin, resistinand visafatin analyzed by multiplex immunoassay. Results: Pre-phlebotomy, PNPLA3 Gallele carriers (C/G and G/G) had higher NAS (p=0.007) and ballooning (p=0.01) butnot steatosis (p=0.06), inflammation (p=0.07) or fibrosis (p=0.64) compared with C/Chomozygotes. Following therapy, decreased NAS (p=0.01) was seen in PNPLA3 G allelecarriers. Phlebotomy did not affect histology in C/C homozygotes. Steatosis (p=0.09), inflam-mation (p=0.11), ballooning (p=0.06) nor fibrosis (p=0.45) were significantly differentbetween carriers and C/C homozygotes. Phlebotomy significantly reduced liver hepcidin(p=0.01) and heme oxygenase 1 gene expression (p=0.02), a measure of oxidative stress.Treatment did not affect expression of other genes examined. Phlebotomy was significantlyassociated with increases in leptin (p=0.03) but had no effect on other adipokines. PNPLA3G allele carriers had significantly decreased heme oxygenase 1 expression in comparison tothose not carrying the allele (p,0.001). Pre and post therapy changes in resistin levelswere significantly different between PNPLA3 G allele carriers and non-carriers (p=0.05).Conclusion: Possession of the PNPLA3 G allele is associated with improvement in liverhistology with iron reduction therapy. Phlebotomy resulted in decreased liver oxidativestress and increased serum leptin, irrespective of PNPLA3 genotype. Determination ofPNPLA3 genotype in individuals with NAFLD may be helpful in guiding therapy andpredicting response to treatment for NALFD.
Mo1005
Effect of Weight Loss on Novel MRI Quantitative Changes in Liver andPancreatic Fat in Patients With Biopsy-Proven Nonalcoholic Fatty LiverDiseaseIliana Doycheva, Mazen Noureddin, Niraj S. Patel, Michael R. Peterson, David A.Brenner, Claude Sirlin, Rohit Loomba
Background: Weight loss has been associated with decrease in hepatic steatosis in patientswith nonalcoholic fatty liver disease (NAFLD). Equal or more than 5% reduction in bodyweight has been linked to improvement in metabolic parameters. However, there are limiteddata regarding quantitative changes in liver fat and pancreatic fat content measured with anovel magnetic resonance imaging (MRI) biomarker, the proton-density-fat-fraction (PDFF),associated with weight loss in patients with biopsy-proven NAFLD. Aim: The aim of thisstudy is to quantify the effect of weight loss on liver and pancreatic fat content using a novelimaging biomarker, the MRI-PDFF. Methods: This is a secondary analysis of a randomizedcontrolled trial (RCT) assessing the effect of colesevelam versus placebo. We included 43patients with biopsy-proven NAFLD who were followed for 24 weeks with available MRI-PDFF liver and pancreatic fat quantification, anthropometric and biochemical profile atbaseline and at 24 weeks. Given that 5% of weight loss has been utilized in previous largestudies (Look AHEAD) as key endpoint, we divided the patients into those who had ≥ 5%reduction in BMI versus those who did not between week 0 and week 24. Results: Amongthe 43 patients with paired liver and pancreatic fat MRI data before and after 24 weeks inthis RCT, 33 patients lost less than 5% or gained weight (gp A) and 10 patients lost 5% or

more (gp B). The average BMI (kg/m2) in gp A and B was 31.1±4.6 and 33.7±4.9, respectively.The average weight change in gp A over the 24-week period was + 0.6 kg, while in gp B itwas -5.1 kg (p,0.0001). There was no difference between groups at baseline in demographic,anthropometric and biochemical characteristics. In gp B, hepatic MRI-PDFF decreased from18.3% to 13.6% (p=0.037) or 25.7% reduction, while pancreatic MRI-PDFF decreased from9% to 8.2% (p=0.16). MRI-PDFF showed no difference between baseline and week 24 inboth liver (15.9% vs. 16.6%, p=0.33) and pancreas (8.3% vs. 8.5%, p=0.89) in group A.Compared to no weight loss (gp A), patients who lost weight (gp B) showed significantdecrease in both liver (p=0.025) and pancreatic (0.028) fat as well as significant reductionin waist circumference (p=0.017), ALT (p=0.016), and hemoglobin A1C (p=0.043). Conclu-sions: Weight loss by ≥5% reduction in BMI in patients with biopsy-proven NAFLD led toa significant decrease in both liver and pancreatic fat that can now be quantified using anaccurate and novel MRI method. These data have significant implications in clinical trialsin NASH for dissecting the relative contributions of weight loss versus pharmacologicalintervention in reducing liver fat content.
Quantitative changes in liver and pancreatic fat with or without weight loss in patients withNAFLD: A secondary analysis of RCT
Mo1006
Alanine Aminotransferase (ALT) to Triglyceride (TG) Ratio As a Marker ofNonalcoholic Fatty Liver Disease (NAFLD) in Obese ChildrenShrinidi Mani, Katharine Eng, Rocio Lopez, Jonathan Moses, Naim Alkhouri
Introduction: The incidence of non-alcoholic fatty liver disease (NAFLD) has increaseddramatically in association with the childhood obesity epidemic. Therefore, it is extremelyimportant to develop an easy and non-invasive tool to detect patients with fatty liver. It hasbecome clear that liver enzymes (ALT and AST) perform poorly for diagnosing NAFLD.Hepatic ultrasonography is the most commonly used imaging modality for NAFLD screening;however, it not always readily available and requires expert interpretation. More recentlythe ALT/triglyceride (TG) ratio has been identified as a simple, non-invasive means ofaccurately identifying NAFLD in asymptomatic obese women. The goal of this study wasto evaluate the ALT/TG ratio as a non-invasive marker for identifying NAFLD in obesechildren. Methods: Obese children between the ages of 6 and 18 with ALT and TG measure-ments were included in the study. All subjects underwent a hepatic ultrasound to evaluatefor the presence of NAFLD. Univariable analysis was performed to assess for differences indemographic and clinical characteristics between subjects with and without NAFLD. TheALT/TG ratio was calculated as follows: ALT (U/L) / [Ln fasting TG (mg/dL)]. Multivariablelogistic regression was then used to evaluate the ability of the ALT/ TG ratio to distinguishbetween the presence or absence of NAFLD. A p value of ,0.05 was considered to bestatistically significant. Results: Data was collected from 59 obese children, average age of14.1 ± 2.8 years; 36 (61%) of whom had NAFLD and 23 (39%) without NAFLD. Patientswith NAFLD were more likely to be Caucasian, have higher AST and ALT and lower alkalinephosphatase. The ALT/TG ratio was found to be significantly elevated in subjects withNAFLD compared to those without (6.9 [4.6, 12.6] and 3.8 [3, 4.6] respectively; p ,0.001)even after adjusting for the presence of the metabolic syndrome. The ALT/TG ratio was alsofound to have excellent accuracy for distinguishing between patients with and withoutNAFLD (AUC = 0.83) (Figure). For every 1 unit increase in the ratio the odds of havingNAFLD increase by a factor of 1.8 (95% CI: 1.2, 2.7; p = 0.004). Conclusion: The ALT/TG ratio is significantly higher in obese children with NAFLD compared to those without.This ratio has excellent accuracy in distinguishing between patients with and without NAFLD.If validated externally, the ALT/TG ratio could be utilized as a non-invasive method tostratify the risk of NAFLD in obese children.
S-1011 AASLD Abstracts
Figure: ALT to TG ratio as a marker for NAFLD in pediatric patients: Receiver OperatingCharacteristics Analysis
Mo1007
Curcumin, Anti-Oxidant, and Pioglitazone Therapy With Inclusion of VitaminE in Non Alcoholic Fatty Liver Disease-a Randomized Open Label PlaceboControlled Clinical Prospective Trial (CAPTIVE)Patrick Basu, Niraj J. Shah, Ravi Siriki, Kavya Mittimani, Srilakshmi Atluri, A. Rahaman,Sakina Farhat, Robert S. Brown
Objectives: NAFLD is a global clinical challenge which progresses to cirrhosis and livercancer. Defective transport of free fatty acids and mitochondrial dysfunction lead to explosionof a series of free radicals, apoptosis, up regulated cytokines and fibrogenesis ultimatelycausing cirrhosis and cancer. Curcumin is a pan-antioxidant with anti-inflammatory, anti-apoptotic, anti-microbial, and anti-fibrogenic properties. This study evaluates the role ofcurcumin in NAFLD to progression of NASH. Methods: Eighty patients (n=80) with meanBMI 29% were recruited, NAFLD score 0.66, NASH fibrotic score 0.33, HOMA IR 3.8, ALT58, LDLc 143, HDLc 29, Triglyceride 186 and Adipokines ( Leptin, Adiponectin, RetinalBinding Proteins ) were divided into Group A- (n=20) Pioglitazone 15mg, Group B- (n=20) vitamin E, Group C- (n=20) curcumin (all the three above groups received placebo),and Group D (n=20) vitamin E plus curcumin. Pre and post values (Triglycerides, LDLc,HDLc, ALT, HOMA-IR, TNF-alfa, Leptin, Adiponectin, Retinol Binding Protein, HBA1c,Serum necro-inflammatory NAFLD and NASH fibrotic score were analyzed at 3, 6, and 12months. Diet and exercise were left unchanged. Daily alcohol content was less than 30 grams.Exclusion; HIV, Medications causing fatty liver including herbal supplements, Lipodystropy,Overt diabetes mellitus, Pregnancy. hypersensitivity to study medications. Results: GroupA- Minimal changes on ALT, HbA1c, HOMA, lipids, no changes in TNF-alfa, adipokines,lipid profile and necro-inflammatory score and/or NASH fibrosis score. Group B and GroupC had modest changes in ALT, lipid profile, HbA1c and HOMA; while no changes inadipokines, necro-inflammatory score and fibrotic score. Group D had significant changesin all scores particularly the adipokines and small improvements in fibrotic score. All patientstolerated the medications well. Conclusion: This study postulates the positive effects ofCurcumin added to vitamin E in NAFLD subgroups; even preventing NASH with a modestanti-fibrotic effect and improved necroinflammatory score; and impressive changes in adipok-ines levels. Additive effects of Curcumin with vitamin E has significant effects on serumlipids and insulin sensitivity. Unavailability of Pre and post liver biopsy was the limitationof this study. A large control trial needs to validate.
Mo1008
Role of TWEAK in the Pathogenesis of Nonalcoholic Fatty Liver DiseaseZulfikar Polat, Ahmet Uygun, A.Melih Ozel, Metin Basaranoglu, Fatih Aslan, MustafaGulsen, Sait Bagci
Background and Aim: Tumor necrosis factor-like weak inducer of apoptosis (TWEAK) hasrecently been introduced as a potential mediator of cardiovascular disease. We aimed toevaluate the associations between TWEAK, chemerin and adipokines in patients with NAFLD.Subjects and Methods: Sixty patients with NAFLD and twenty healthy controls were includedin this prospective study. BMI, waist circumference, plasma lipids, glucose, aminotransferasesand adipokines were evaluated for each patient, and TWEAK (by ELISA) and chemerinlevels were measured. TWEAK, chemerin, IFN, IL-6, MCP-1 and adiponectin levels wereexamined and compared in patient and control groups. Results: TWEAK levels were signifi-cantly higher (504.56 [76.47-1098.20] pg/ml vs. 308.64 [92.12-274.11] pg/ml, p , 0.001)in patients with NAFLD than controls. There was no difference in chemerin levels betweenpatients and controls. IL-6 levels (2.92 [1.18-25.60] pg/ml vs. 1.68 [1-4.05] pg/ml, p,0.001)and MCP-1 levels (190.73 [91-471] pg/ml vs. 165.75 [126-267] pg/ml, p= 0.026) weresignificantly higher in the patient group. Finally, adiponectin levels in patients with NAFLD
AA
SL
DA
bst
ract
s