mitral regurgitation with rupture chordae tendinea,
TRANSCRIPT

Brit. Heart J., 1966, 28, 746.
Mitral Regurgitation with Rupture of NormalChordae Tendinea,
PAUL MARCHAND, JOHN B. BARLOW, LOUIS A. DU PLESSIS, ANDIAN WEBSTER
From the Cardio-Vascular Research Unit and Cardio-Pulmonary Research Unit (C.S.I.R.); the Department ofThoracic Surgery and Medicine; the Cardiac Clinic, Johannesburg General Hospital, and University of the
Witwatersrand and the Pneumoconiosis Research Unit (C.S.I.R.)
Surgery for mitral incompetence still presents achallenge despite the great advance made by theintroduction of prosthetic valves. In view of thehigh incidence of late complications of prostheses(Du Plessis et al., 1965), we believe that, wheneverpossible, the natural valve should be preserved.Unfortunately this can be done only in cases of pureor dominant stenosis and in those ofmitral regurgita-tion due to a localized defect or a grossly dilatedannulus. Partial retention of the valve is seldompracticable because of the lack of suitable materialsfor leaflet substitution and the uncertainty of com-petency after a long intricate operation. We have,however, been able to retain the valves of six patientswith severe mitral regurgitation resulting fromruptured chordm tendinee. This paper describesthe anatomical features and surgical management ofthese cases and discusses the probable mechanismof the chordal disruption.
INCIDENCE OF RUPTURED CHORD& TENDINE,Up to January 1965, ruptured chordae were en-
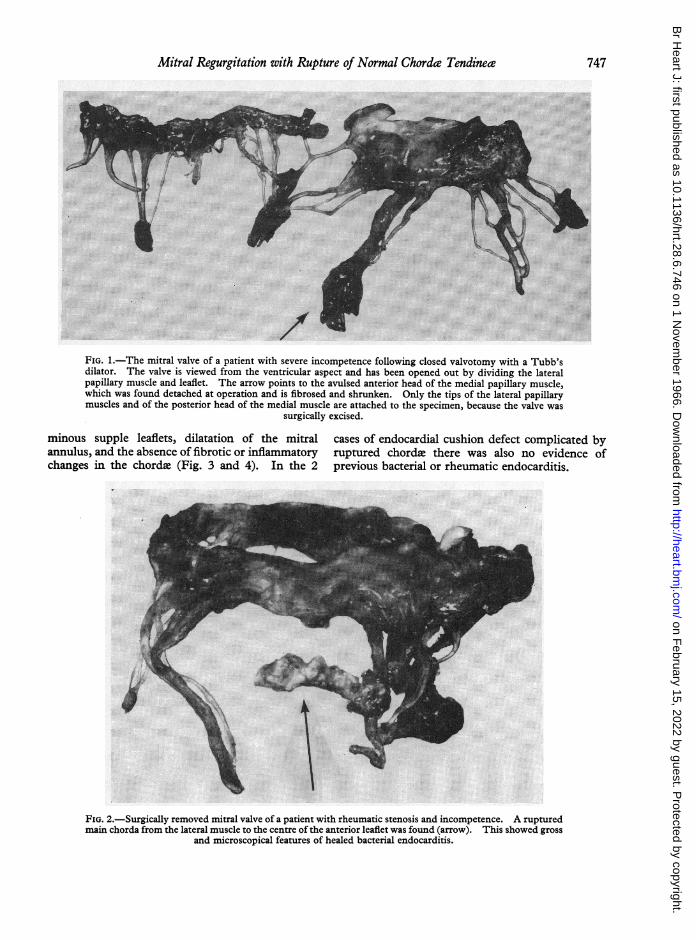
countered in 23 of 126 consecutive mitral valveoperations performed in this unit under cardio-pulmonary bypass (Table I). Of the 23 patients,8 had undergone a previous closed valvotomy, andmitral regurgitation had either been produced orwas aggravated by this procedure. This is oftendue to the production of chordal rupture, and aTubb's dilator may even avulse the medial papillarymuscle if the blades are opened with the instrumentincorrectly placed between this muscle and theventricular septum (Fig. 1). The degree of re-gurgitation following such iatrogenic chordal rup-ture is frequently severe, since, in rheumatic mitral
Received September 6, 1965.
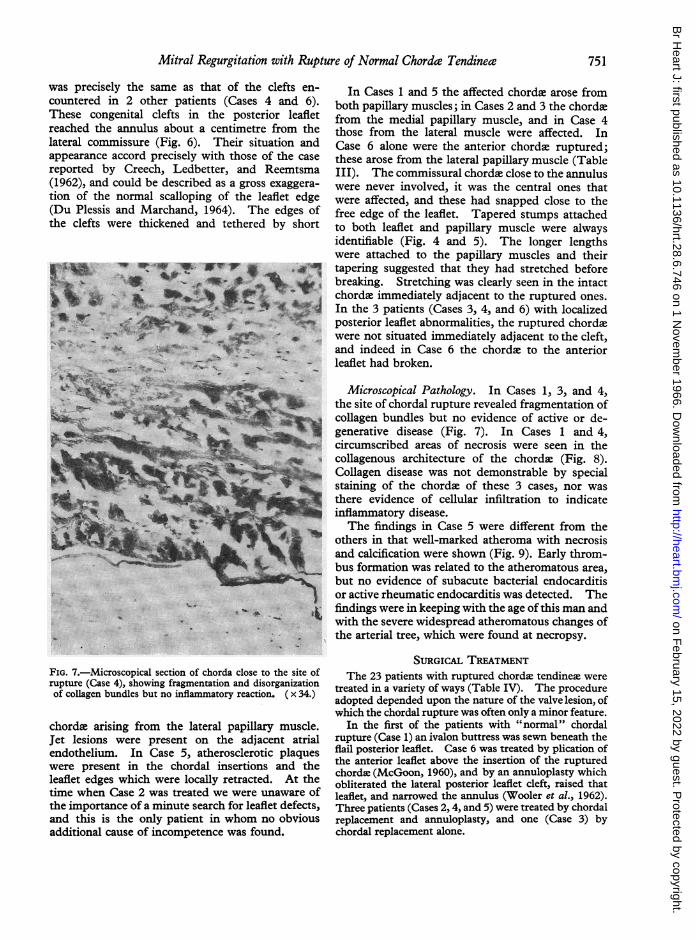
stenosis, the chorde to an extensive length of theleaflet edge are often fused. Many authors (Hepper,Burchell, and Edwards, 1956; Osmundson, Calla-han, and Edwards, 1961; Menges, Ankeney, andHellerstein, 1964) regard bacterial endocarditis asthe commonest cause of ruptured chords, but wewere able to implicate this disease in only 4 of our23 patients. In these 4 instances, areas of calcifica-tion or irregular nodularity were suggestive ofprevious bacterial endocarditis (Fig. 2). In 2 ofthese, the ruptured chordx were considered to bethe major cause of the mitral incompetence. In3 cases of rheumatic mitral incompetence, dueessentially to leaflet retraction, minor commissuralchordae which were irregularly thickened wereruptured, and it is probable that the rheumaticprocess was responsible for both the chordal diseaseand the disruption (Bailey and Hickam, 1944).The 6 patients with pure severe mitral regurgita-
tion due to major chordal rupture form a groupcharacterized by left atrial dilatation, volu-
TABLE IINCIDENCE OF RUPTURED CHORDJ, TENDINENFOUND IN 126 CASES DURING OPEN-HEART
SURGERY FOR MITRAL VALVE DISEASE
Open-heart Ruptured chordaeoperations tendinese
No. No. Previous closedvalvotomy
Pure stenosis 8 0 0Mixed incompetence and 94 15 8
stenosisPure incompetence 10 6 0Endocardial cushion defect 14 2 0
with cleft mitral valve
Total 126 23 8
746
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from
Mitral Regurgitation with Rupture of Normal Chordac Tendinea7
,.
_; ..MA5_'D11-
.''
FIG. 1.-The mitral valve of a patient with severe incompetence following closed valvotomy with a Tubb'sdilator. The valve is viewed from the ventricular aspect and has been opened out by dividing the lateralpapillary muscle and leaflet. The arrow points to the avulsed anterior head of the medial papillary muscle,which was found detached at operation and is fibrosed and shrunken. Only the tips of the lateral papillarymuscles and of the posterior head of the medial muscle are attached to the specimen, because the valve was
surgically excised.
minous supple leaflets, dilatation of the mitralannulus, and the absence of fibrotic or inflammatorychanges in the chordw, (Fig. 3 and 4). In the 2
cases of endocardial cushion defect complicated byruptured chorda there was also no evidence ofprevious bacterial or rheumatic endocarditis.
FIG. 2.-Surgically removed mitral valve of a patient with rheumatic stenosis and incompetence. A rupturedmain chorda from the lateral muscle to the centre of the anterior leaflet was found (arrow). This showed gross
and microscopical features of healed bacterial endocarditis.
747
@E11
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Marchand, Barlow, du Plessis, and WebsterAnterior leatflet
Mitral
annu IusanuluTeflon
buttressingannuloplasty _
'Posteriorleaf let
Cut thick atrial wall
FIG. 3.-Heart of Case 5, a man of 68, viewed from the atrium. The mitral annulus is dilated. Both leafletsare voluminous, the posterior one shows clearly. An annuloplasty was done at the lateral commissure, and theteflon plaque over which sutures were tied is seen in position. The smaller teflon pledgets close to the freeedge at the centre of the posterior leaflet mark the sites where the artificial chordm were fixed to that leaflet.
Base left ventricle Left atrium
Posteriorleaflet
Stumps of
ruptured chordaetendinece
_(§z jLtJ ,~~~~............... A rtfi f i cial N ylonchordae
MedialX papillaryposteriorwall leftventricle
Cut left1E1. s_ IL ~~ventricle
FIG. 4.-Heart of Case 5, viewed through a window cut in the posterior wall of the left ventricle. Theartificial nylon chord: to the medial papillary muscle are visible, those to the lateral disappear to the leftbehind the cut myocardium. The intact chord: tendinese are thin and healthy in appearance. Blunt stumps
of the ruptured chordse can be seen.
748
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Mitral Regurgitation with Rupture of Normal Chorde Tendineae
TABLE IIAGE, SEX, AND DETAILS OF HISTORY OF 6 PATIENTS WITH PURE MITRAL
INCOMPETENCE
Case Age Sex Date of History of Time Duration ofNo. (yr.) operation murmur serious
Rheumatic Subacute known symptomsfever bacterial (yr.) (mth.)
endocarditis-|__________ ___________ or trauma
1 46 F 1/6/61 0 25 82 41 M '17/11/61 ? 0 13 33 36 M 4/1/63 0 0 11 64 49 M 21/4/64 0 0 32 215 68 M 15/5/64 0 0 6 66 33 M 15/6/64 0 0 20 3
749
TABLE IIISUMMARY OF GROSS PATHOLOGICAL FEATURES
Case Ruptured chorde| Condition of Annulus Other lesions Anterior leaflet Posterior leafletNo. remaining chordse
1 From lateral and Thick commissural Moderately None Voluminous Voluminous; edge slightlymedial muscles to chordae dilated thickened, rolled andposterior leaflet flail
2 From medial muscle Thin, elongated Moderately None recognized Very voluminous Very voluminous; freeto posterior leaflet dilated edge rolled and flail
3 From medial muscle Long and thin Grossly Lateral perforation Very voluminous Voluminous; thickened,to posterior leaflet dilated in posterior leaf- flail medial leaflet edge
let4 From lateral muscle Elongated and thin, Markedly Deep lateral cleft Voluminous Volumninous; free edge
to posterior leaflet chiefly posterior dilated posterior leaflet rolled and flail5 From lateral and Elongated; some no- Grossly Atheromatous Voluminous; free Voluminous; atheroma in
medial muscles to dular atheroma dilated plaques on leaf- edge thick free edge; flailposterior leaflet lets
6 From lateral muscle Adjacent to cleft Grossly Deep lateral cleft Very voluminous Very voluminousto anterior leaflet thick and stiff; dilated posterior leaflet and flail
others long andthin
CLINICAL FEATURESIt is our intention in a later paper to present the
detailed clinical and investigatory findings in these6 patients. For present purposes the relevantfeatures are summarized in Table II. Of the 6patients, 5 were men: their ages ranged from 33 to68 but only one was older than 50. No patient gavean unequivocal history of rheumatic fever, though2 could recall periodic joint pains during their youth.Every patient had known of the existence of a heartmurmur for years before the development of seriousheart symptoms. In all instances there had been asudden onset of cardiac symptoms within 6 monthsof admission to our wards, and 2 (Cases 1 and 5) hadrapidly developed congestive cardiac failure neces-sitating continuous hospitalization from the time ofdeterioration. Symptoms were pronounced in all,the hearts were radiologically enlarged, and thedegree of incompetence was assessed as severe.Investigations for subacute bacterial endocarditisand rheumatic activity were uniformly negative.
PATHOLOGICAL FINDINGSThe 6 patients were operated upon under direct
vision with the aid ofcardiopulmonary bypass. The
following descriptions are based upon the operativefindings and upon the post-mortem appearances ofCases 1 and 5, the hearts of which were preserved.The ruptured chords of Cases 3 and 4 were excisedduring operation and examined histologically.
Gross Pathology. These findings are summarizedin Table III. All the valves showed annular dilata-tion, free commissures, and mobile voluminousleaflets. The intact chorde, particularly thoseadjacent to the ruptured ones, were elongated andoften thinned. The appearances of the valves wereremarkably similar in all cases, the only differingfeature being the presence of a cause ofincompetenceadditional to the ruptured chordi. The posteriorleaflet edge and the commissural chorda of Case 1were thickened, indicative of rheumatic involvement(Fig. 5). In Case 3, there was a hole 05 cm. indiameter lateral to the centre of the posterior leaflet.The margins of this hole were smooth and flexiblethough slightly thickened, and normal leaflet tissueseparated the defect from the ruptured chordee whicharose from the medial papillary muscle. In theabsence of any evidence of subacute bacterial endo-carditis, it is probable that the defect was congenital,a belief strengthened by the fact that its situation
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Marchand, Barlow, du Plessis, and Webster
M ;r.!:%~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~*.
FIG. 5.-Heart of Case 1 with the left ventricle opened out to display the posterior leaflet. The stumps of theruptured central chordee tendinew are seen to be thin and tapered. Chorde which arose from both the medialpapillary muscle (left) and the lateral papillary muscle have ruptured. The intact chorde are thickened,
suggesting a rheumatic basis.
FIG. 6.-Opened-out normal mitral valve showing deep scallop at site where congenital clefts and the punched-out hole were found in Cases 3, 4, and 6.
750
...... .
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from
Mitral Regurgitation with Rupture of Normal Chorde Tendineae
was precisely the same as that of the clefts en-countered in 2 other patients (Cases 4 and 6).These congenital clefts in the posterior leafletreached the annulus about a centimetre from thelateral commissure (Fig. 6). Their situation andappearance accord precisely with those of the casereported by Creech, Ledbetter, and Reemtsma(1962), and could be described as a gross exaggera-tion of the normal scalloping of the leaflet edge(Du Plessis and Marchand, 1964). The edges ofthe clefts were thickened and tethered by short
rs_w+1t*4:
I .
FIG. 7.-Microscopical section of chorda close to the site ofrupture (Case 4), showing fragmentation and disorganizationof collagen bundles but no inflammatory reaction. ( x 34.)
chordae arising from the lateral papillary muscle.Jet lesions were present on the adjacent atrialendothelium. In Case 5, atherosclerotic plaqueswere present in the chordal insertions and theleaflet edges which were locally retracted. At thetime when Case 2 was treated we were unaware ofthe importance of a minute search for leaflet defects,and this is the only patient in whom no obviousadditional cause of incompetence was found.
In Cases 1 and 5 the affected chords arose fromboth papillary muscles; in Cases 2 and 3 the chordxfrom the medial papillary muscle, and in Case 4those from the lateral muscle were affected. InCase 6 alone were the anterior chordae ruptured;these arose from the lateral papillary muscle (TableIII). The commissural chordqe close to the annuluswere never involved, it was the central ones thatwere affected, and these had snapped close to thefree edge of the leaflet. Tapered stumps attachedto both leaflet and papillary muscle were alwaysidentifiable (Fig. 4 and 5). The longer lengthswere attached to the papillary muscles and theirtapering suggested that they had stretched beforebreaking. Stretching was clearly seen in the intactchordae immediately adjacent to the ruptured ones.In the 3 patients (Cases 3, 4, and 6) with localizedposterior leaflet abnormalities, the ruptured chordxwere not situated immediately adjacent to the cleft,and indeed in Case 6 the chordae to the anteriorleaflet had broken.
Microscopical Pathology. In Cases 1, 3, and 4,the site of chordal rupture revealed fragmentation ofcollagen bundles but no evidence of active or de-generative disease (Fig. 7). In Cases 1 and 4,circumscribed areas of necrosis were seen in thecollagenous architecture of the chorde (Fig. 8).Collagen disease was not demonstrable by specialstaining of the chordee of these 3 cases, nor wasthere evidence of cellular infiltration to indicateinflammatory disease.The findings in Case 5 were different from the
others in that well-marked atheroma with necrosisand calcification were shown (Fig. 9). Early throm-bus formation was related to the atheromatous area,but no evidence of subacute bacterial endocarditisor active rheumatic endocarditis was detected. Thefindings were in keeping with the age of this man andwith the severe widespread atheromatous changes ofthe arterial tree, which were found at necropsy.
SURGICAL TREATMENTThe 23 patients with ruptured chordee tendinem were
treated in a variety of ways (Table IV). The procedureadopted depended upon the nature of the valve lesion, ofwhich the chordal rupture was often only a minor feature.
In the first of the patients with "normal" chordalrupture (Case 1) an ivalon buttress was sewn beneath theflail posterior leaflet. Case 6 was treated by plication ofthe anterior leaflet above the insertion of the rupturedchords (McGoon, 1960), and by an annuloplasty whichobliterated the lateral posterior leaflet cleft, raised thatleaflet, and narrowed the annulus (Wooler et al., 1962).Three patients (Cases 2,4, and 5) were treated by chordalreplacement and annuloplasty, and one (Case 3) bychordal replacement alone.
751
44 on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Marchand, Barlow, du Plessis, and Webster
FIG. 8.-Microscopical section of chorda of Case 3 close to the site of rupture, showing cleft formation withinthe collagen bundles surrounded by a small zone of necrotic collagen. Again there is no cellular infiltration
and complete absence of inflammatory reaction. ( x 160).
Operation for Chordal Replacement. The heart wasexposed through a long left thoracotomy incision.Venous blood was drained through a I in. (1-27 cm.)cannula in the right ventricular outflow tract, andoxygenated blood was returned at a flow rate of 2-2 litres/sq. m./min., through the left femoral artery. The bodytemperature was lowered to 30°C. without altering theperfusion rate.The left atrium was widely opened. The papillary
muscles were defined and their chorda. traced to theleaflet or to the sites of rupture. The leaflets weresearched for areas of thickening, perforations, and con-
genital clefts. Jet lesions on the atrial walls served as
useful guides for the localization of such isolated leafletdefects.
Monofilament 00 nylon was used for chordal replace-ment in ail 4 cases. The needle was passed from theventricular to the atrial aspect of the leaflet close to theremnant of a major chorda. It was then returnedthrough the leaflet 0-25 in. (0-6 cm.) from its entry. Thenylon was buttressed on both aspects of the leaflet withteflon pledgets and was tied firmly with 4 knots, leavingtwo long strands projecting from the ventricular surfaceof the valve. Further similar nylon sutures were theninserted until the whole flail leaflet edge was secured. Inone patient (Case 4), 3 sutures (6 strands) were used,whereas in the others 2 sufficed. The free ends of thenylon were then threaded onto long slim curved skinneedles and passed under vision through the appropriatepapillary muscle close to its apex and about 0-25 in.
TABLE IVTREATMENT OF ALL CASES WITH RUPTURED CHORDJE TENDINEI,
No. Ivalon bung Annuloplasty Artificial Prosthetic Survivalbuttress of and plication chords valveposterior leafletleaflet
Rheumatic mitral stenosis and 7 0 1 1 5 6mitral incompetence
Post-closed valvotomy 8 2 0 0 6 6Endocardial cushion defect 2 0 1 0 1 2Pure mitral incompetence and 6 1 1 4 0 4
ruptured chorda
Total 23 3 3 5 12 18
752
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Mitral Regurgitation with Rupture of Normal Chordee Tendinece
FIG. 9.-Microscopical section through a nodule in a chorda close to the site of rupture (Case 5). This showsan atherosclerotic lesion in which there is well-marked necrosis and calcification but no inflammatory in-
filtration. ( x 14.)
(0-6 cm.) apart. The needles emerged externallythrough the posterior ventricular wall, care being takento avoid transfixing or straddling major coronary vessels.Each pair of filaments was brought through a square ofteflon extemally.The first time this technique was used the heart was
defibrillated and the length of the artificial chordle,necessary to prevent eversion of the leaflet duringventricular systole, was adjusted. It was found thatslight traction upon the exteriorized nylon pulled theposterior leaflet against the ventricular wall and causedincompetence. Adjustment was difficult as the tendencywas to tie the strands too tightly, and the knots had to beloosened several times before a satisfactory result wasobtained. Subsequently, chordal length was adjustedbefore the heart was closed. This was achieved by graspingthe leaflet edge with forceps and flapping it towards theatrium until the remaining natural chordee were tense.When the nylon restrained the leaflet to the same extentas the natural chordae, a mosquito clamp was applied tothe threads externally and flush with the ventricular wall.Leaflet competence was later confirmed in the beating3c
heart by digital exploration, and the nylon was then tiedover the teflon patch. A correctly adjusted loop ofnylon did not dig deeply into the ventricle when thepatient's own circulation was restored.
In addition to the chordal replacement, any other lesionthat could cause incompetence must be corrected. Thehole in the posterior leaflet of Case 3 was covered with along strip of pericardium which was sewn to the atrialsurface of the leaflet from the annulus to its free edges.The pericardial strip was left long enough to reach theapex of the papillary muscle to which it was fixed withsilk sutures after the nylon threads had been adjusted forlength. Despite the dilated mitral ring, annuloplastywas not-done, and this proved to be a mistake sincemoderate regurgitation remained. In Cases 4 and 6, thedeep clefts of the posterior leaflet were obliterated byincluding their inner edges in the lateral annuloplasties.
RESULTS
Cases 1 and 5 died in hospital; the remaining 4survived (Table V). Minimal mitral regurgitation
753
-P
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Marchand, Barlow, du Plessis, and Webster
TABLE VSUMMARY OF OPERATIVE RESULTS
Case Hospital Course Post-operativeNo. _
Murmur of mitral incompetence Time in hospital Symptoms Auscultation
1 Nil until 1 week before death; then Died at 6 weeksgross
2 Nil 23 days Asymptomatic 4 years later Grade 1/6 late systolic murmur; mid-late systolic click
3 Grade 2 late systolic murmur 23 days Marked improvement 3 years Grade 2-3/6 late systolic murmur;later mid-late systolic click
4 Nil 20 days Asymptomatic 2 years later Grade 1/6 pan-systolic murmur; mid-late systolic click
5 Nil Died at 14 days6 Grade 1 pan-systolic murmur 22 days Marked improvement 1 years Grade 3/6 pan-systolic murmur
later
remained in Cases 2 and 4 as shown by a grade 1late systolic murmur (Barlow et al., 1963; Segal andLikoff, 1964; Tavel, Campbell, and Zimmer, 1965;Barlow, 1965; Barlow and Pocock, 1965; Ronan,Perloff, and Harvey, 1965; Barlow et al., 1966), andpansystolic murmur, respectively. Case 3 also hada late systolic murmur, but this was loud (grade 3)and probably denoted a more significant degree ofincompetence. Case 6 had a grade 3 pansystolicmurmur and moderate residual mitral regurgitation,though this was considerably less than beforeoperation. In all 4 survivors the symptoms im-proved or disappeared. Systolic clicks were presentin the 3 patients (Cases 2, 3, and 4) with artificialchord:. This finding was compatible with thepostulate that non-ejection clicks are usually ofintracardiac origin (Barlow et al., 1963; Barlow,1965; Ronan et al., 1965; Barlow et al., 1966).
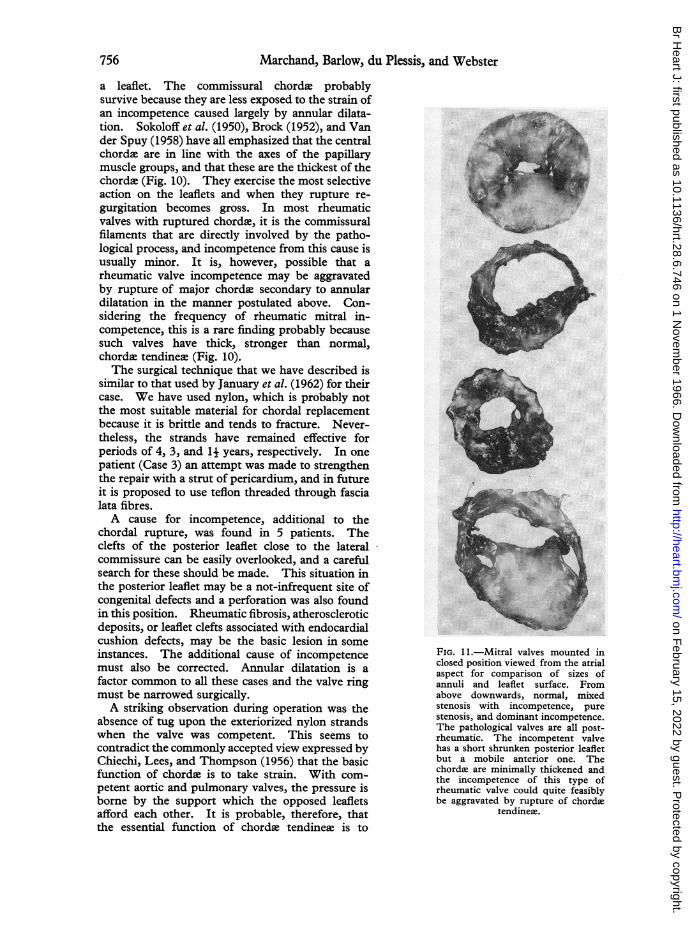
DISCUSSIONIt is rare to find pure severe rheumatic in-
competence with minimal leaflet or chordal thicken-ing, and in most cases a degree of stenosis coexists(Saphir, 1953) (Fig. 10 and 11). Hepper et al.(1956) considered that bacterial endocarditis was themain cause of chordal rupture, and Osmundsonet al. (1961) found evidence of active or healedbacterial endocarditis in 16 of 20 rheumatic valveswith ruptured chords. These latter authors con-sidered that rheumatic activity could producechordal disruption but that the incompetence wasthen seldom severe since the commissural filamentswere usually involved. Bailey and Hickam (1944)described 7 cases of ruptured chordee which theyattributed to rheumatic disease. Barber (1944) hasshown that a crush injury or blow to the chest wallcan rupture chordw tendine-.
Several workers (Frothingham and Hass, 1934;Shapiro and Weiss, 1959; January, Fisher, andEhrenhaft, 1962) have claimed that normal chordscan rupture, and our 6 cases fall into this category.
It is possible that the posterior leaflet perforation ofCase 3 was a legacy of bacterial endocarditis, but theabsence of history, the otherwise unscarred leaflet,and the fact that the defect was remote from thechordal ruptures, makes this most unlikely. Saphir(1953) maintained that, with bacterial endocarditis,the chord.e were affected by direct extension of theinfective process.Our only specific histological finding was the
atherosclerosis present in the chordae of Case 5.Features of rheumatic disease were not seen in the3 patients (Cases 1, 3, and 4) examined, butadmittedly this was a difficult histological diagnosisto make. Rokitansky (1852) and Coombs (1924)differ in their interpretation of the pathogenesis ofrheumatic valve thickening but agree that the lesionis a dense nodular fibrosis associated with thickeningand fusion of the chordae. Gross and Kugel (1931)described a non-rheumatic deposition of lipid in thechorde close to their leaflet insertion. Sokoloff,Elster, and Righthand (1950) reported degenerativechordal changes at the insertional sites in elderlypeople, and they described local chordal thickeningcharacterized histologically by a loss of cellularityand increased hyalinization. They also mentionedtapering of these thickened chord. at the insertioninto the leaflet. Certainly, in our cases, the chord;ruptured close to the leaflet edge and the stumpswere tapered. However, adjacent intact chordewere thin and stretched, and did not show thedegenerative histology described by these authors.There was, therefore, in our patients, scant
evidence of rheumatic endocarditis or subacutebacterial endocarditis, and we believe that normalchordte ruptured as a result of pre-existing and un-related valve incompetence. This view is basedupon the known presence of cardiac murmurs manyyears before the onset of disabling heart symptoms,the finding in 3 cases of non-rheumatic leafletpathology, and the generally non-specific histologicalappearances of the ruptured chordae. Of the 6
754
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Mitral Regurgitation with Rupture of Normal Chordee Tendinea7
FIG. 10.-Series of mitral valves opened out to display the chordse and annuli.From above downwards, normal, pure stenosis, mixed stenosis and incompe-tence, and dominant incompetence. Note the discrepancy in the diameters ofthe valves and the different chordal appearances. The pathological valves are
all post-rheumatic and surgically excised.
patients with ruptured chorde reported by Mengeset al. (1964), 5 had also been known to have heartmurmurs for many years before decompensationoccurred, and though 3 of their cases had clearhistories of rheumatic fever, no gross evidence ofleaflet vegetation or ulceration to indicate precedingbacterial endocarditis was found at operation. Inthe presence of supple mitral valve components,"incompetence begets more incompetence", be-cause of progressive annular dilatation (Edwards andBurchell, 1958; Levy and Edwards, 1962). We
believe that leaflet apposition becomes progressivelyless extensive as the annulus dilates, and that anincreased strain is then thrown upon the chorde,which consequently stretch and may eventuallysnap. When a chorda breaks the situation issuddenly aggravated, greater strain has to be borneby the adjacent intact chords, and serial rupture ofthese may then result. Our cases include ruptureof the chorde from one papillary muscle, unilateralchordal rupture with stretching of those from theopposite muscle, and central rupture of all chorda to
755
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from
Marchand, Barlow, du Plessis, and Webster
a leaflet. The commissural chorde probablysurvive because they are less exposed to the strain ofan incompetence caused largely by annular dilata-tion. Sokoloff et al. (1950), Brock (1952), and Vander Spuy (1958) have all emphasized that the centralchords are in line with the axes of the papillarymuscle groups, and that these are the thickest of thechordae (Fig. 10). They exercise the most selectiveaction on the leaflets and when they rupture re-gurgitation becomes gross. In most rheumaticvalves with ruptured chordae, it is the commissuralfilaments that are directly involved by the patho-logical process, and incompetence from this cause isusually minor. It is, however, possible that arheumatic valve incompetence may be aggravatedby rupture of major chordae secondary to annulardilatation in the manner postulated above. Con-sidering the frequency of rheumatic mitral in-competence, this is a rare finding probably becausesuch valves have thick, stronger than normal,chordae tendineee (Fig. 10).The surgical technique that we have described is
similar to that used by January et al. (1962) for theircase. We have used nylon, which is probably notthe most suitable material for chordal replacementbecause it is brittle and tends to fracture. Never-theless, the strands have remained effective forperiods of 4, 3, and 11 years, respectively. In onepatient (Case 3) an attempt was made to strengthenthe repair with a strut of pericardium, and in futureit is proposed to use teflon threaded through fascialata fibres.A cause for incompetence, additional to the
chordal rupture, was found in 5 patients. Theclefts of the posterior leaflet close to the lateralcommissure can be easily overlooked, and a carefulsearch for these should be made. This situation inthe posterior leaflet may be a not-infrequent site ofcongenital defects and a perforation was also foundin this position. Rheumatic fibrosis, atheroscleroticdeposits, or leaflet clefts associated with endocardialcushion defects, may be the basic lesion in someinstances. The additional cause of incompetencemust also be corrected. Annular dilatation is afactor common to all these cases and the valve ringmust be narrowed surgically.A striking observation during operation was the
absence of tug upon the exteriorized nylon strandswhen the valve was competent. This seems tocontradict the commonly accepted view expressed byChiechi, Lees, and Thompson (1956) that the basicfunction of chorde is to take strain. With com-petent aortic and pulmonary valves, the pressure isborne by the support which the opposed leafletsafford each other. It is probable, therefore, thatthe essential function of chorde tendineee is to
FIG. 11.-Mitral valves mounted inclosed position viewed from the atrialaspect for comparison of sizes ofannuli and leaflet surface. Fromabove downwards, normal, mixedstenosis with incompetence, purestenosis, and dominant incompetence.The pathological valves are all post-rheumatic. The incompetent valvehas a short shrunken posterior leafletbut a mobile anterior one. Thechordae are minimally thickened andthe incompetence of this type ofrheumatic valve could quite feasiblybe aggravated by rupture of chorde
tendinee.
756
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Mitral Regurgitation with Rupture of Normal Chorde Tendinece
restrain the leaflet edge early in ventricular systoleso that the leaflet can "catch" the blood and billowin the same way as the sails of a boat catch the wind.The filled leaflets make surface contact and by theirmutual support resist the rising ventricular pressure.We have used no refined techniques to measure thequantitative pull on the artificial chords, butSalisbury, Cross, and Rieben (1963), working withdogs, have shown by replacing a segment of chordawith a transverse displacement transducer, that theshape of its tension curve follows the contour of theintraventricular pressure curve until the aortic valveopens. Thereafter, chordal tension falls sharply,while the left ventricular pressure continues to rise.When all other chorde were cut, however, theydemonstrated that the tension on the intact oneincreased and continued to rise after aortic valveopening. Despite the use of nylon, our patientshave survived up to 4 years without recurrence ofserious incompetence, and presumably withoutfracture of the strands. This would indeed beremarkable if the threads had to bend and straightenmany millions of times while resisting the full leftventricular pressure.
A description is given of 6 patients in whom therewas severe mitral incompetence associated withsupple voluminous leaflets, annular dilatation, andrupture of histologically normal chorde tendinew.All were subjected to operation, and 4 have sur-vived. The chorda were replaced in 4.
It is believed that in these cases, and possibly in2 others with endocardial cushion defects, rupturewas not due to local chordal disease. Thehypothesis is advanced that the chorde rupturedbecause they were not adapted to resist the pressuresthrown upon them by progressive mitral regurgita-tion caused by dilatation of the annulus of the valve.A cause ofmitral regurgitation preceding the chordalrupture must, therefore, be present to account forthe annular dilatation. The original, minor in-competence may be due to any congenital or acquiredlesion, and such were found in five of the casespresented. All the patients were known to have hadheart murmurs many years before the onset ofserious cardiac symptoms. Only after the annulushas dilated sufficiently to impair wide surfaceapposition of the leaflets, do the chords come underpathological strain. Chordal rupture results insudden aggravation of the incompetence, and serialrupture may then occur.Our experience with the insertion of artificial
chord. indicates that they resist little strain duringventricular systole. It is suggested that the functionof chorde tendinete is to restrain the leaflet edges
early in ventricular systole, so converting them tocup-shaped structures, the surfaces of which canoppose. As a result of the wide support which theleaflets then provide for each other, the chorde of acompetent valve are relieved of the burden ofresisting the full left ventricular pressure.
REFERENCESBailey, 0. T., and Hickam, J. B. (1944). Rupture of mitral
chorde tendineae. Clinical and pathologic observationson seven cases in which there was no bacterial endo-carditis. Amer. Heart J., 28, 578.
Barber, H. (1944). The effects of trauma, direct and indirect,on the heart. Quart. J3. Med., n.s. 13, 137.
Barlow, J. B. (1965). Conjoint clinic on the clinical signifi-cance of late systolic murmurs and non-ejection systolicclicks. J. chron. Dis., 18, 665.
, Bosman, C. K., Pocock, W. A., and Marchand, P. (1966).Late systolic murmurs and non-ejection (mid-late)systolic clicks. In preparation.
, and Pocock, W. A. (1965). The isolated systolicmurmur. S. Afr. med. J7., 39, 909.
, Marchand, P., and Denny, M. (1963). Thesignificance of late systolic murmurs. Amer. Heart J.,66, 443.
Brock, R. C. (1952). The surgical and pathological anatomyof the mitral valve. Brit. Heart J., 14, 489.
Chiechi, M. A., Lees, W. M., and Thompson, R. (1956).Functional anatomy of the normal mitral valve.J. thorac.Surg., 32, 378.
Coombs, C. F. (1924). Rheumatic Heart Disease. Wood, NewYork.
Creech, O., Ledbetter, M. K., and Reemtsma, K. (1962).Congenital mitral insufficiency with cleft posteriorleaflet. Circulation, 25, 390.
Du Plessis, L. A., and Marchand, P. (1964). The anatomy ofthe mitral valve and its associated structures. Thorax,19, 221.-- , Fuller, D., Joubert, E., Gale, G., and Chesler, E.
(1965). Experience in 100 patients with Starr-Edwardsprosthetic valves in the mitral and aortic positions.S. Afr. med. J., 39, 944.
Edwards, J. E., and Burchell, H. B. (1958). Pathologicanatomy of mitral insufficiency. Proc. Mayo Clin.,33, 497.
Frothingham, C., and Hass, G. M. (1934). Rupture ofnormalchordae tendinee of the mitral valve. Amer. Heart J.,9, 492.
Gross, L., and Kugel, M. A. (1931). Topographic anatomyand histology of the valves in the human heart. Amer.J. Path., 7, 445.
Hepper, N. G. G., Burchell, H. B., and Edwards, J. E. (1956).Mitral insufficiency in healed, unrecognized bacterialendocarditis. Proc. Mayo Clin., 31, 659.
January, L. E., Fisher, J. M., and Ehrenhaft, J. L. (1962).Mitral insufficiency resulting from rupture of normalchordae tendinex. Report of a surgically corrected case.Circulation, 26, 1329.
Levy, M. J., and Edwards, J. E. (1962). Anatomy of mitralinsufficiency. Progr. cardiovasc. Dis., 5, 119.
McGoon, D. C. (1960). Repair of mitral insufficiency due toruptured chordm tendineae. J. thorac. cardiovasc. Surg.,39, 357.
Menges, H., Ankeney, J. L., and Hellerstein, H. K. (1964).The clinical diagnosis and surgical management ofruptured mitral chordse tendinem. Circulation, 30, 8.
Osmundson, P. J., Callahan, J. A., and Edwards, J. E. (1961).Ruptured mitral chorde tendines. Circulation, 23, 42.
757
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from

Marchand, Barlow, du Plessis, and Webster
Rokitansky, C. (1852). A Manual of Pathological Anatomy,Vol. IV. Sydenham Society, London.
Ronan, J. A., Perloff, J. K., and Harvey, W. P. (1965).Systolic clicks and the late systolic murmur. Amer.Heart J., 70, 319.
Salisbury, P. F., Cross, C. E., and Rieben, P. A. (1963).Chorde tendines tension. Amer.3J. Physiol., 205,385.
Saphir, 0. (1953). Nonrheumatic inflammatory diseases ofthe heart. B. Endocarditis. In Pathology of the Heart, ed.S. E. Gould, p. 707. Charles C. Thomas, Springfield,Illinois.
Segal, B. L., and Likoff, W. (1964). Late systolic murmur ofmitral regurgitation. Amer. Heart J., 67, 757.
Shapiro, H. A., and Weiss, D. R. (1959). Mitral insufficiencydue to ruptured chord2e tendineae simulating aorticstenosis. New Engl. j. Med., 261, 272.
Sokoloff, L., Elster, S. K., and Righthand, N. (1950).Sclerosis of the chorda tendineae of the mitral valve.Circulation, 1, 782.
Tavel, M. E., Campbell, R. W., and Zimmer, J. F. (1965).Late systolic murmurs and mitral regurgitation. Amer.J. Cardiol., 15, 719.
Van der Spuy, J. C. (1958). The functional and clinicalanatomy of the mitral valve. Brit. Heart J., 20, 471.
Wooler, G. H., Nixon, P. G. F., Grimshaw, V. A., and Watson,D. A. (1962). Experiences with the repair of the mitralvalve in mitral incompetence. Thorax, 17, 49.
ADDENDUMSince preparing this paper we have operated upon a
further case of pure mitral incompetence in whichruptured chorde were associated with a congenital cleftof the lateral junctional tissue of the anterior leaflet.This cleft stopped a centimeter from the annulus, and a
small perforation was present in the intervening bridge ofleaflet. The patient had a history very suggestive ofsubacute bacterial endocarditis.
758
on February 15, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.28.6.746 on 1 Novem
ber 1966. Dow
nloaded from