minocycline for negative symptoms in...
TRANSCRIPT

Murphy 1
Minocycline for Negative Symptoms in Schizophrenia
Heather Murphy, PharmD PGY-2 Psychiatric Pharmacy Resident
Central Texas Veterans Health Care System Objectives -Review the diagnostic criteria, epidemiology, pathophysiology, and current treatments of schizophrenia -Describe the mechanism of action of minocycline in schizophrenia -Evaluate the current evidence of minocycline in schizophrenia -Formulate an evidence-based conclusion for minocycline use in schizophrenia
Murphy 2
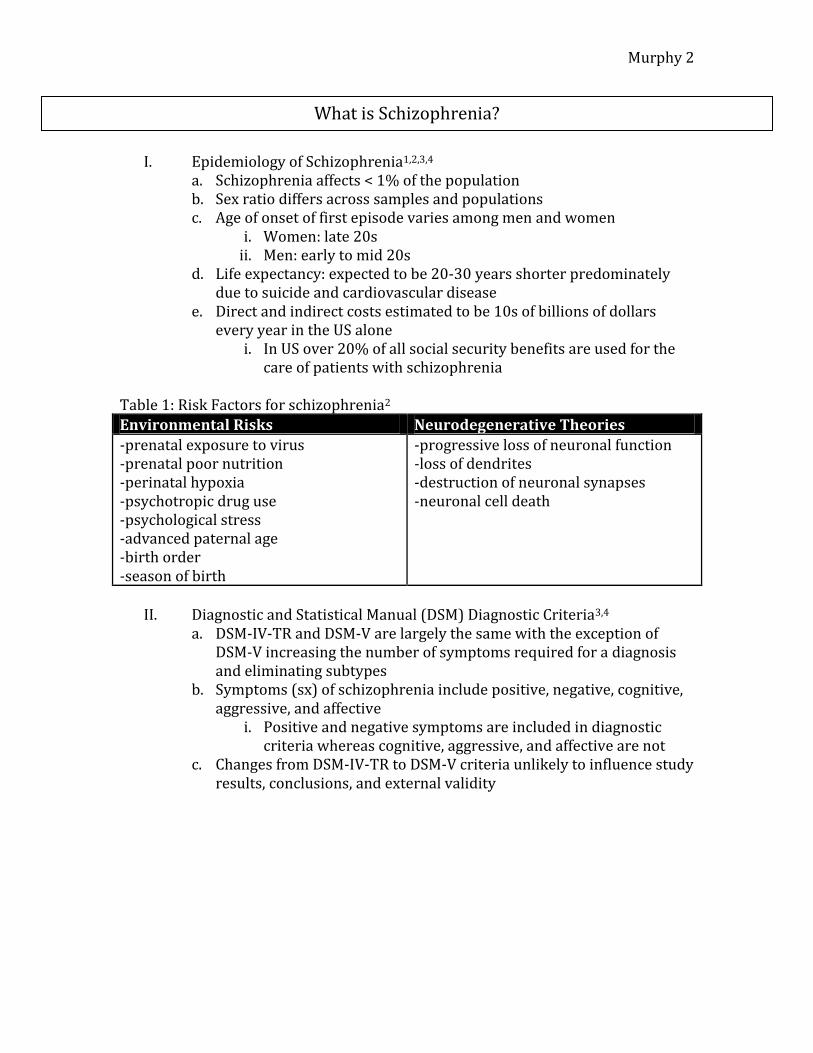
I. Epidemiology of Schizophrenia1,2,3,4
a. Schizophrenia affects < 1% of the population b. Sex ratio differs across samples and populations c. Age of onset of first episode varies among men and women
i. Women: late 20s ii. Men: early to mid 20s
d. Life expectancy: expected to be 20-30 years shorter predominately due to suicide and cardiovascular disease
e. Direct and indirect costs estimated to be 10s of billions of dollars every year in the US alone
i. In US over 20% of all social security benefits are used for the care of patients with schizophrenia
Table 1: Risk Factors for schizophrenia2
Environmental Risks Neurodegenerative Theories
-prenatal exposure to virus -prenatal poor nutrition -perinatal hypoxia -psychotropic drug use -psychological stress -advanced paternal age -birth order -season of birth
-progressive loss of neuronal function -loss of dendrites -destruction of neuronal synapses -neuronal cell death
II. Diagnostic and Statistical Manual (DSM) Diagnostic Criteria3,4
a. DSM-IV-TR and DSM-V are largely the same with the exception of DSM-V increasing the number of symptoms required for a diagnosis and eliminating subtypes
b. Symptoms (sx) of schizophrenia include positive, negative, cognitive, aggressive, and affective
i. Positive and negative symptoms are included in diagnostic criteria whereas cognitive, aggressive, and affective are not
c. Changes from DSM-IV-TR to DSM-V criteria unlikely to influence study results, conclusions, and external validity
What is Schizophrenia?
Murphy 3
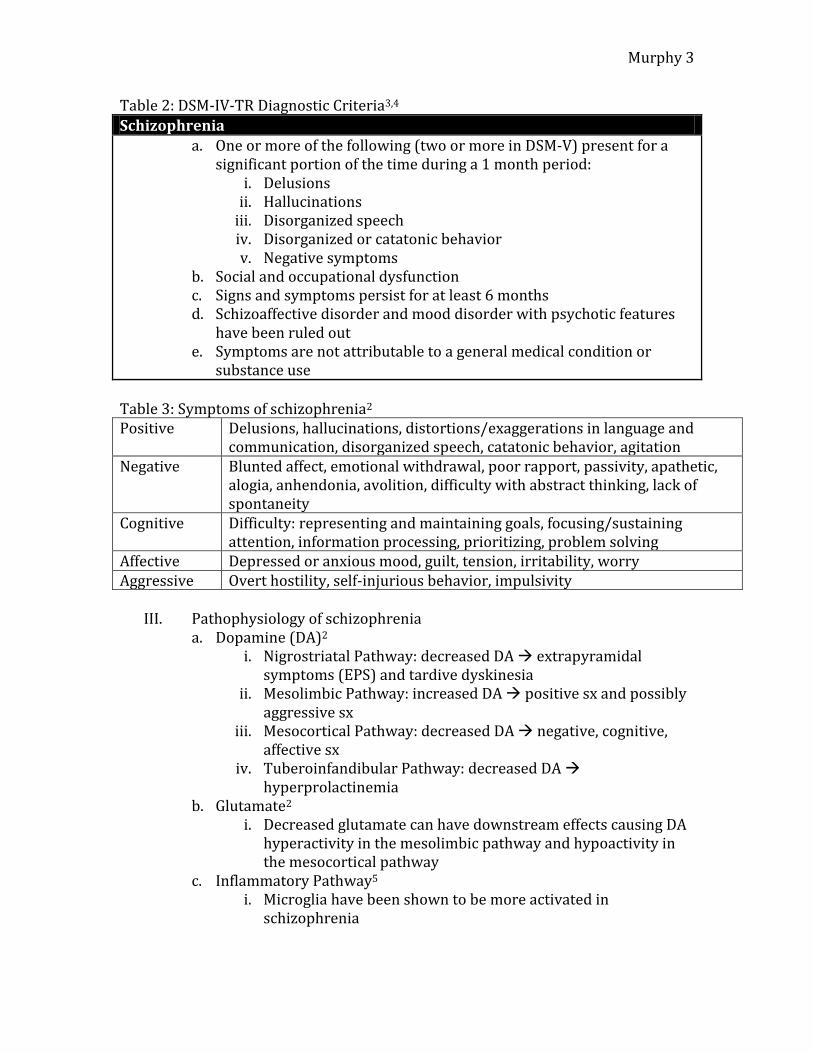
Table 2: DSM-IV-TR Diagnostic Criteria3,4
Schizophrenia a. One or more of the following (two or more in DSM-V) present for a
significant portion of the time during a 1 month period: i. Delusions
ii. Hallucinations iii. Disorganized speech iv. Disorganized or catatonic behavior v. Negative symptoms
b. Social and occupational dysfunction c. Signs and symptoms persist for at least 6 months d. Schizoaffective disorder and mood disorder with psychotic features
have been ruled out e. Symptoms are not attributable to a general medical condition or
substance use
Table 3: Symptoms of schizophrenia2
Positive Delusions, hallucinations, distortions/exaggerations in language and communication, disorganized speech, catatonic behavior, agitation
Negative Blunted affect, emotional withdrawal, poor rapport, passivity, apathetic, alogia, anhendonia, avolition, difficulty with abstract thinking, lack of spontaneity
Cognitive Difficulty: representing and maintaining goals, focusing/sustaining attention, information processing, prioritizing, problem solving
Affective Depressed or anxious mood, guilt, tension, irritability, worry Aggressive Overt hostility, self-injurious behavior, impulsivity
III. Pathophysiology of schizophrenia a. Dopamine (DA)2
i. Nigrostriatal Pathway: decreased DA extrapyramidal symptoms (EPS) and tardive dyskinesia
ii. Mesolimbic Pathway: increased DA positive sx and possibly aggressive sx
iii. Mesocortical Pathway: decreased DA negative, cognitive, affective sx
iv. Tuberoinfandibular Pathway: decreased DA hyperprolactinemia
b. Glutamate2 i. Decreased glutamate can have downstream effects causing DA
hyperactivity in the mesolimbic pathway and hypoactivity in the mesocortical pathway
c. Inflammatory Pathway5 i. Microglia have been shown to be more activated in
schizophrenia
Murphy 4
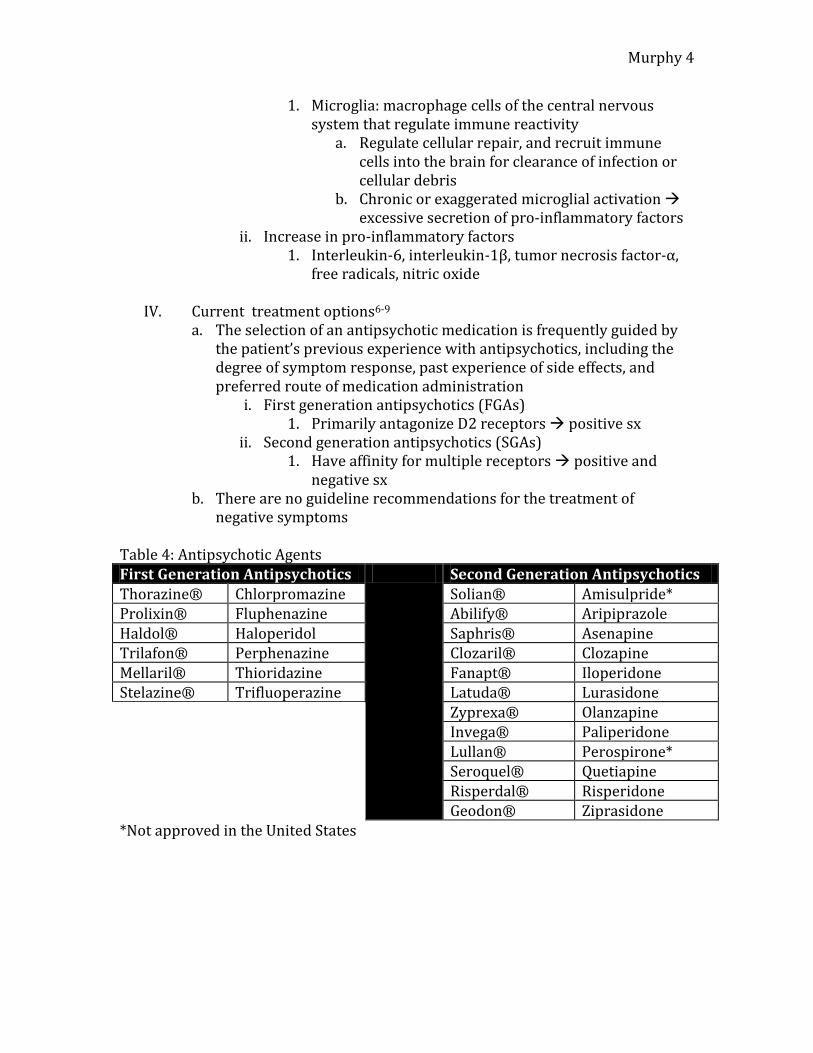
1. Microglia: macrophage cells of the central nervous system that regulate immune reactivity
a. Regulate cellular repair, and recruit immune cells into the brain for clearance of infection or cellular debris
b. Chronic or exaggerated microglial activation excessive secretion of pro-inflammatory factors
ii. Increase in pro-inflammatory factors 1. Interleukin-6, interleukin-1β, tumor necrosis factor-α,
free radicals, nitric oxide
IV. Current treatment options6-9 a. The selection of an antipsychotic medication is frequently guided by
the patient’s previous experience with antipsychotics, including the degree of symptom response, past experience of side effects, and preferred route of medication administration
i. First generation antipsychotics (FGAs) 1. Primarily antagonize D2 receptors positive sx
ii. Second generation antipsychotics (SGAs) 1. Have affinity for multiple receptors positive and
negative sx b. There are no guideline recommendations for the treatment of
negative symptoms Table 4: Antipsychotic Agents First Generation Antipsychotics Second Generation Antipsychotics Thorazine® Chlorpromazine Solian® Amisulpride* Prolixin® Fluphenazine Abilify® Aripiprazole Haldol® Haloperidol Saphris® Asenapine Trilafon® Perphenazine Clozaril® Clozapine Mellaril® Thioridazine Fanapt® Iloperidone Stelazine® Trifluoperazine Latuda® Lurasidone Zyprexa® Olanzapine Invega® Paliperidone
Lullan® Perospirone* Seroquel® Quetiapine Risperdal® Risperidone Geodon® Ziprasidone
*Not approved in the United States
Murphy 5
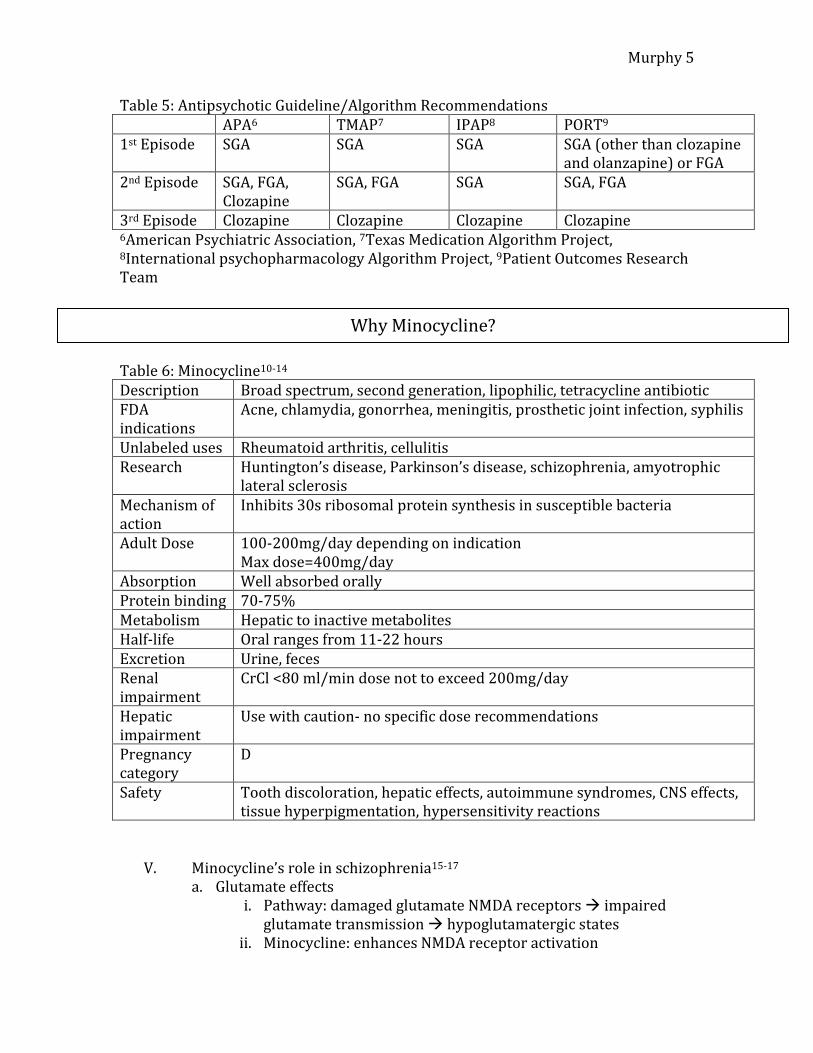
Table 5: Antipsychotic Guideline/Algorithm Recommendations APA6 TMAP7 IPAP8 PORT9
1st Episode SGA SGA SGA SGA (other than clozapine and olanzapine) or FGA
2nd Episode SGA, FGA, Clozapine
SGA, FGA SGA SGA, FGA
3rd Episode Clozapine Clozapine Clozapine Clozapine 6American Psychiatric Association, 7Texas Medication Algorithm Project, 8International psychopharmacology Algorithm Project, 9Patient Outcomes Research Team Table 6: Minocycline10-14
Description Broad spectrum, second generation, lipophilic, tetracycline antibiotic FDA indications
Acne, chlamydia, gonorrhea, meningitis, prosthetic joint infection, syphilis
Unlabeled uses Rheumatoid arthritis, cellulitis Research Huntington’s disease, Parkinson’s disease, schizophrenia, amyotrophic
lateral sclerosis Mechanism of action
Inhibits 30s ribosomal protein synthesis in susceptible bacteria
Adult Dose 100-200mg/day depending on indication Max dose=400mg/day
Absorption Well absorbed orally Protein binding 70-75% Metabolism Hepatic to inactive metabolites Half-life Oral ranges from 11-22 hours Excretion Urine, feces Renal impairment
CrCl <80 ml/min dose not to exceed 200mg/day
Hepatic impairment
Use with caution- no specific dose recommendations
Pregnancy category
D
Safety Tooth discoloration, hepatic effects, autoimmune syndromes, CNS effects, tissue hyperpigmentation, hypersensitivity reactions
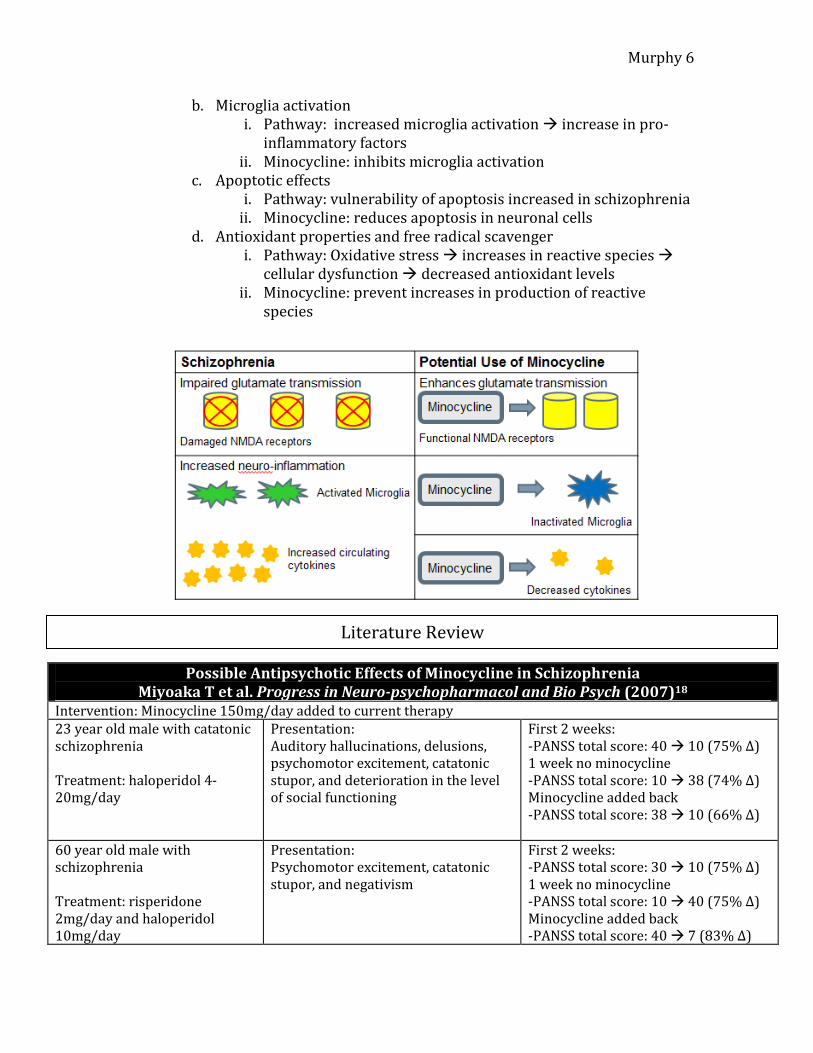
V. Minocycline’s role in schizophrenia15-17 a. Glutamate effects
i. Pathway: damaged glutamate NMDA receptors impaired glutamate transmission hypoglutamatergic states
ii. Minocycline: enhances NMDA receptor activation
Why Minocycline?
Murphy 6
b. Microglia activation i. Pathway: increased microglia activation increase in pro-
inflammatory factors ii. Minocycline: inhibits microglia activation
c. Apoptotic effects i. Pathway: vulnerability of apoptosis increased in schizophrenia
ii. Minocycline: reduces apoptosis in neuronal cells d. Antioxidant properties and free radical scavenger
i. Pathway: Oxidative stress increases in reactive species cellular dysfunction decreased antioxidant levels
ii. Minocycline: prevent increases in production of reactive species
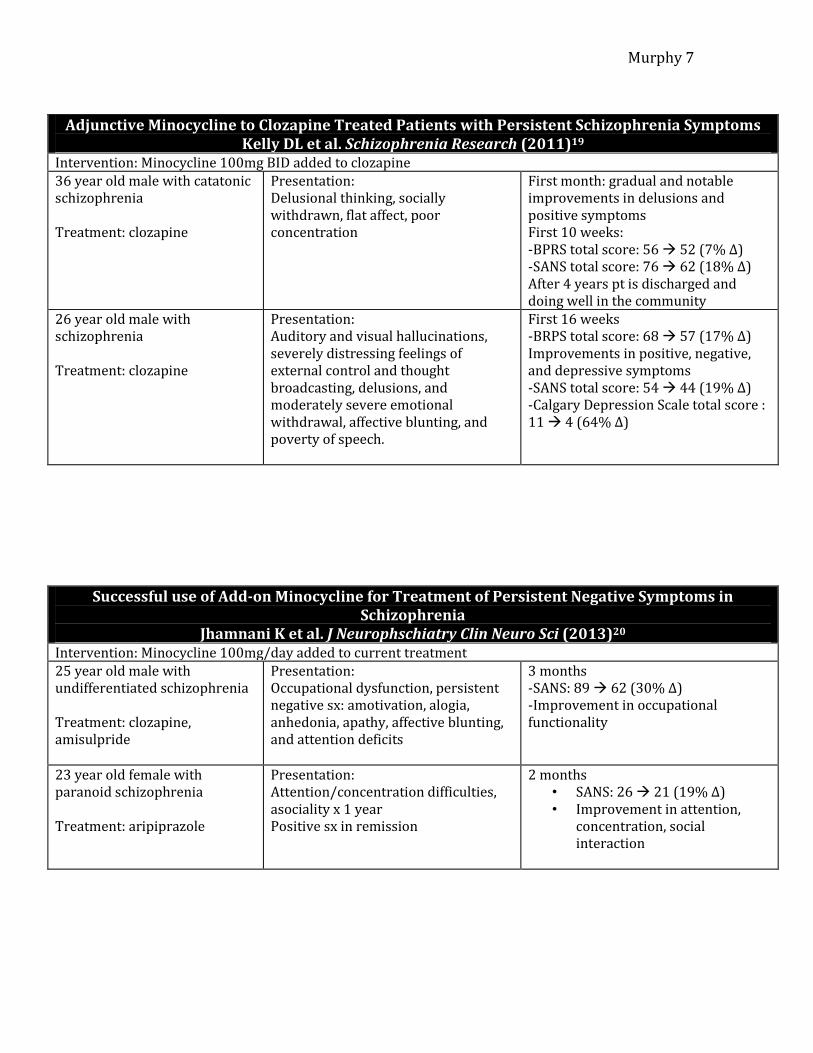
Possible Antipsychotic Effects of Minocycline in Schizophrenia Miyoaka T et al. Progress in Neuro-psychopharmacol and Bio Psych (2007)18
Intervention: Minocycline 150mg/day added to current therapy 23 year old male with catatonic schizophrenia Treatment: haloperidol 4-20mg/day
Presentation: Auditory hallucinations, delusions, psychomotor excitement, catatonic stupor, and deterioration in the level of social functioning
First 2 weeks: -PANSS total score: 40 10 (75% Δ) 1 week no minocycline -PANSS total score: 10 38 (74% Δ) Minocycline added back -PANSS total score: 38 10 (66% Δ)
60 year old male with schizophrenia Treatment: risperidone 2mg/day and haloperidol 10mg/day
Presentation: Psychomotor excitement, catatonic stupor, and negativism
First 2 weeks: -PANSS total score: 30 10 (75% Δ) 1 week no minocycline -PANSS total score: 10 40 (75% Δ) Minocycline added back -PANSS total score: 40 7 (83% Δ)
Literature Review
Murphy 7
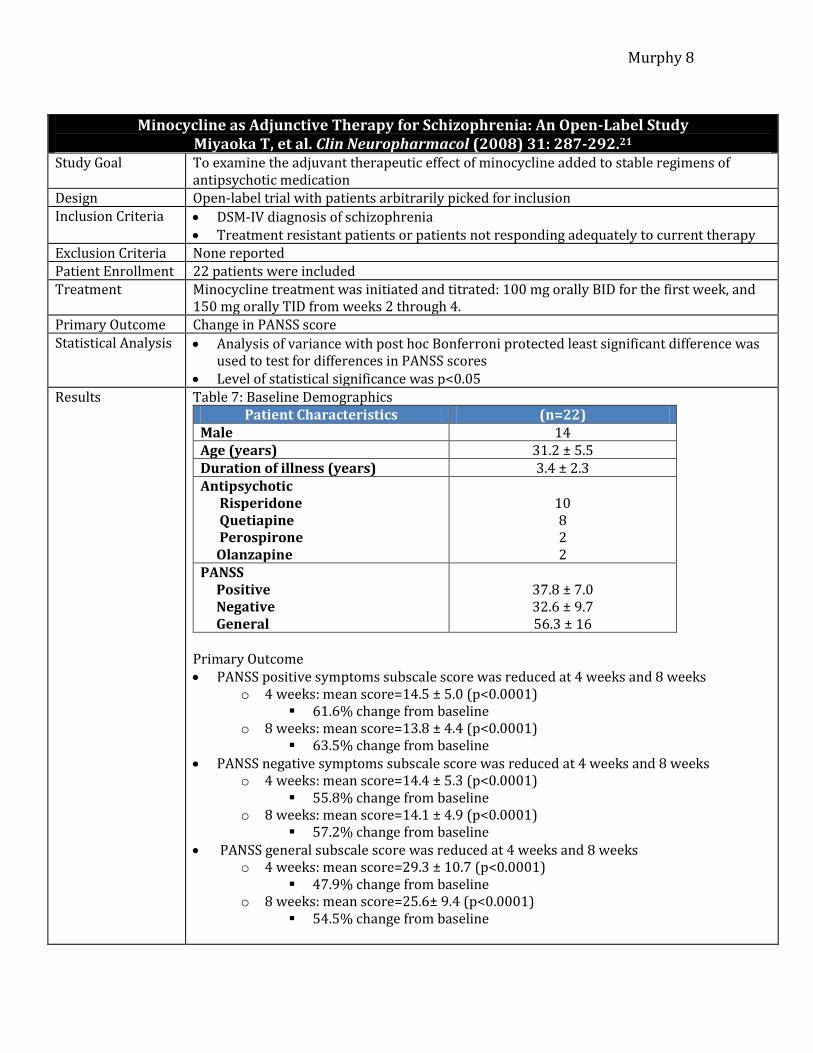
Adjunctive Minocycline to Clozapine Treated Patients with Persistent Schizophrenia Symptoms
Kelly DL et al. Schizophrenia Research (2011)19
Intervention: Minocycline 100mg BID added to clozapine 36 year old male with catatonic schizophrenia Treatment: clozapine
Presentation: Delusional thinking, socially withdrawn, flat affect, poor concentration
First month: gradual and notable improvements in delusions and positive symptoms First 10 weeks: -BPRS total score: 56 52 (7% Δ) -SANS total score: 76 62 (18% Δ) After 4 years pt is discharged and doing well in the community
26 year old male with schizophrenia Treatment: clozapine
Presentation: Auditory and visual hallucinations, severely distressing feelings of external control and thought broadcasting, delusions, and moderately severe emotional withdrawal, affective blunting, and poverty of speech.
First 16 weeks -BRPS total score: 68 57 (17% Δ) Improvements in positive, negative, and depressive symptoms -SANS total score: 54 44 (19% Δ) -Calgary Depression Scale total score : 11 4 (64% Δ)
Successful use of Add-on Minocycline for Treatment of Persistent Negative Symptoms in Schizophrenia
Jhamnani K et al. J Neurophschiatry Clin Neuro Sci (2013)20
Intervention: Minocycline 100mg/day added to current treatment 25 year old male with undifferentiated schizophrenia Treatment: clozapine, amisulpride
Presentation: Occupational dysfunction, persistent negative sx: amotivation, alogia, anhedonia, apathy, affective blunting, and attention deficits
3 months -SANS: 89 62 (30% Δ) -Improvement in occupational functionality
23 year old female with paranoid schizophrenia Treatment: aripiprazole
Presentation: Attention/concentration difficulties, asociality x 1 year Positive sx in remission
2 months • SANS: 26 21 (19% Δ) • Improvement in attention,
concentration, social interaction
Murphy 8
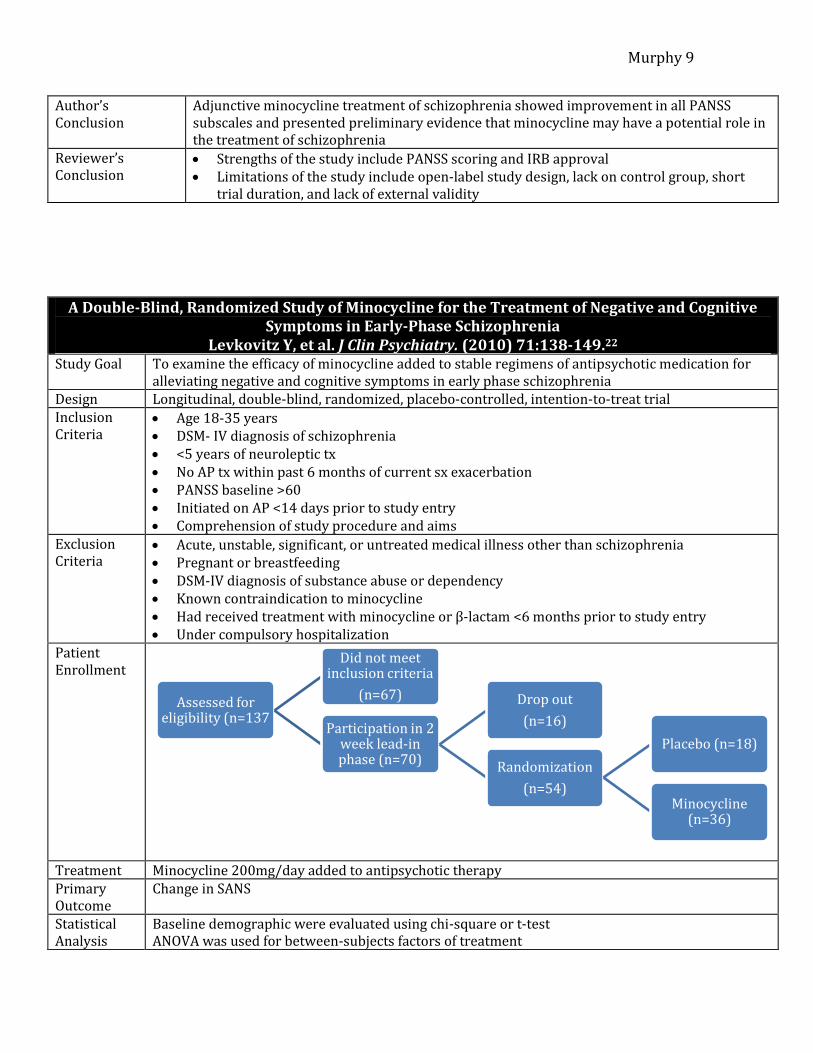
Minocycline as Adjunctive Therapy for Schizophrenia: An Open-Label Study
Miyaoka T, et al. Clin Neuropharmacol (2008) 31: 287-292.21
Study Goal To examine the adjuvant therapeutic effect of minocycline added to stable regimens of antipsychotic medication
Design Open-label trial with patients arbitrarily picked for inclusion Inclusion Criteria DSM-IV diagnosis of schizophrenia
Treatment resistant patients or patients not responding adequately to current therapy Exclusion Criteria None reported Patient Enrollment 22 patients were included Treatment Minocycline treatment was initiated and titrated: 100 mg orally BID for the first week, and
150 mg orally TID from weeks 2 through 4. Primary Outcome Change in PANSS score Statistical Analysis Analysis of variance with post hoc Bonferroni protected least significant difference was
used to test for differences in PANSS scores Level of statistical significance was p<0.05
Results Table 7: Baseline Demographics Patient Characteristics (n=22)
Male 14 Age (years) 31.2 ± 5.5 Duration of illness (years) 3.4 ± 2.3 Antipsychotic Risperidone Quetiapine Perospirone Olanzapine
10 8 2 2
PANSS Positive Negative General
37.8 ± 7.0 32.6 ± 9.7 56.3 ± 16
Primary Outcome PANSS positive symptoms subscale score was reduced at 4 weeks and 8 weeks
o 4 weeks: mean score=14.5 ± 5.0 (p<0.0001) 61.6% change from baseline
o 8 weeks: mean score=13.8 ± 4.4 (p<0.0001) 63.5% change from baseline
PANSS negative symptoms subscale score was reduced at 4 weeks and 8 weeks o 4 weeks: mean score=14.4 ± 5.3 (p<0.0001)
55.8% change from baseline o 8 weeks: mean score=14.1 ± 4.9 (p<0.0001)
57.2% change from baseline PANSS general subscale score was reduced at 4 weeks and 8 weeks
o 4 weeks: mean score=29.3 ± 10.7 (p<0.0001) 47.9% change from baseline
o 8 weeks: mean score=25.6± 9.4 (p<0.0001) 54.5% change from baseline
Murphy 9
Author’s Conclusion
Adjunctive minocycline treatment of schizophrenia showed improvement in all PANSS subscales and presented preliminary evidence that minocycline may have a potential role in the treatment of schizophrenia
Reviewer’s Conclusion
Strengths of the study include PANSS scoring and IRB approval Limitations of the study include open-label study design, lack on control group, short
trial duration, and lack of external validity
A Double-Blind, Randomized Study of Minocycline for the Treatment of Negative and Cognitive Symptoms in Early-Phase Schizophrenia
Levkovitz Y, et al. J Clin Psychiatry. (2010) 71:138-149.22
Study Goal To examine the efficacy of minocycline added to stable regimens of antipsychotic medication for alleviating negative and cognitive symptoms in early phase schizophrenia
Design Longitudinal, double-blind, randomized, placebo-controlled, intention-to-treat trial Inclusion Criteria
Age 18-35 years DSM- IV diagnosis of schizophrenia <5 years of neuroleptic tx No AP tx within past 6 months of current sx exacerbation PANSS baseline >60 Initiated on AP <14 days prior to study entry Comprehension of study procedure and aims
Exclusion Criteria
Acute, unstable, significant, or untreated medical illness other than schizophrenia Pregnant or breastfeeding DSM-IV diagnosis of substance abuse or dependency Known contraindication to minocycline Had received treatment with minocycline or β-lactam <6 months prior to study entry Under compulsory hospitalization
Patient Enrollment
Treatment Minocycline 200mg/day added to antipsychotic therapy Primary Outcome
Change in SANS
Statistical Analysis
Baseline demographic were evaluated using chi-square or t-test ANOVA was used for between-subjects factors of treatment
Assessed for eligibility (n=137
Did not meet inclusion criteria
(n=67)
Participation in 2 week lead-in phase (n=70)
Drop out
(n=16)
Randomization
(n=54)
Placebo (n=18)
Minocycline (n=36)
Murphy 10
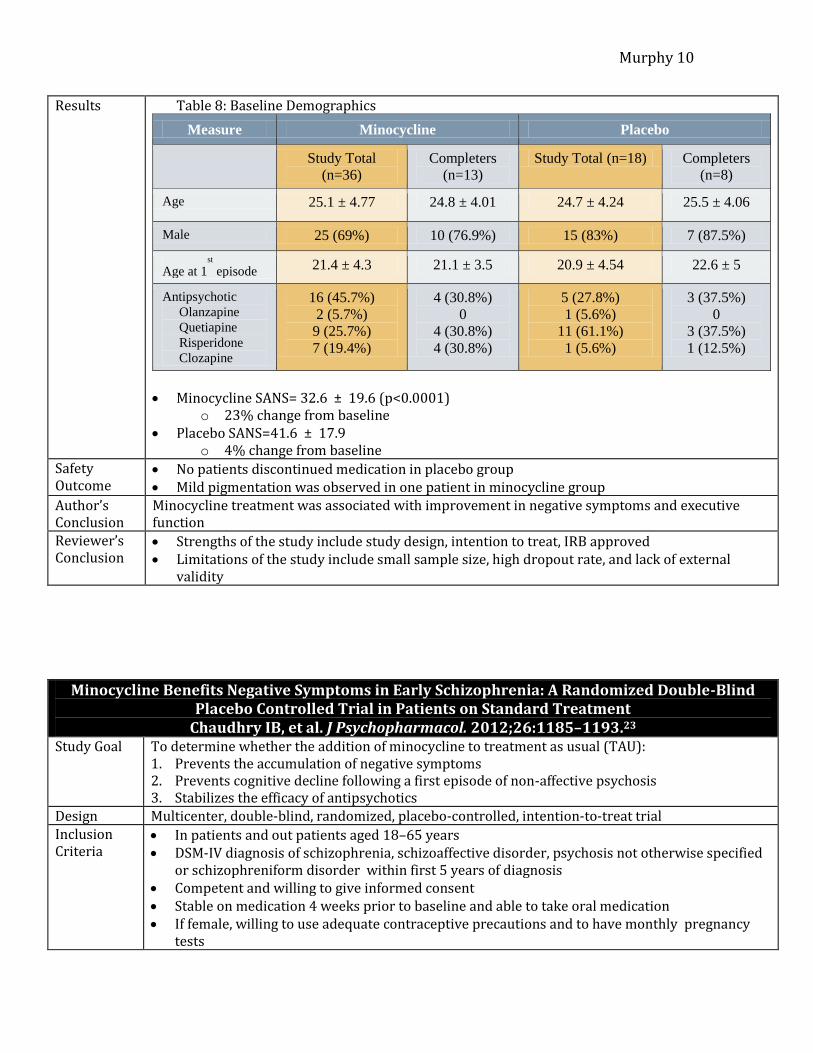
Results Table 8: Baseline Demographics
Measure Minocycline Placebo
Study Total
(n=36)
Completers
(n=13)
Study Total (n=18) Completers
(n=8)
Age 25.1 ± 4.77 24.8 ± 4.01 24.7 ± 4.24 25.5 ± 4.06
Male 25 (69%) 10 (76.9%) 15 (83%) 7 (87.5%)
Age at 1st
episode 21.4 ± 4.3 21.1 ± 3.5 20.9 ± 4.54 22.6 ± 5
Antipsychotic
Olanzapine
Quetiapine
Risperidone
Clozapine
16 (45.7%)
2 (5.7%)
9 (25.7%)
7 (19.4%)
4 (30.8%)
0
4 (30.8%)
4 (30.8%)
5 (27.8%)
1 (5.6%)
11 (61.1%)
1 (5.6%)
3 (37.5%)
0
3 (37.5%)
1 (12.5%)
Minocycline SANS= 32.6 ± 19.6 (p<0.0001)
o 23% change from baseline Placebo SANS=41.6 ± 17.9
o 4% change from baseline Safety Outcome
No patients discontinued medication in placebo group Mild pigmentation was observed in one patient in minocycline group
Author’s Conclusion
Minocycline treatment was associated with improvement in negative symptoms and executive function
Reviewer’s Conclusion
Strengths of the study include study design, intention to treat, IRB approved Limitations of the study include small sample size, high dropout rate, and lack of external
validity
Minocycline Benefits Negative Symptoms in Early Schizophrenia: A Randomized Double-Blind Placebo Controlled Trial in Patients on Standard Treatment
Chaudhry IB, et al. J Psychopharmacol. 2012;26:1185–1193.23
Study Goal To determine whether the addition of minocycline to treatment as usual (TAU): 1. Prevents the accumulation of negative symptoms 2. Prevents cognitive decline following a first episode of non-affective psychosis 3. Stabilizes the efficacy of antipsychotics
Design Multicenter, double-blind, randomized, placebo-controlled, intention-to-treat trial Inclusion Criteria
In patients and out patients aged 18–65 years DSM-IV diagnosis of schizophrenia, schizoaffective disorder, psychosis not otherwise specified
or schizophreniform disorder within first 5 years of diagnosis Competent and willing to give informed consent Stable on medication 4 weeks prior to baseline and able to take oral medication If female, willing to use adequate contraceptive precautions and to have monthly pregnancy
tests
Murphy 11
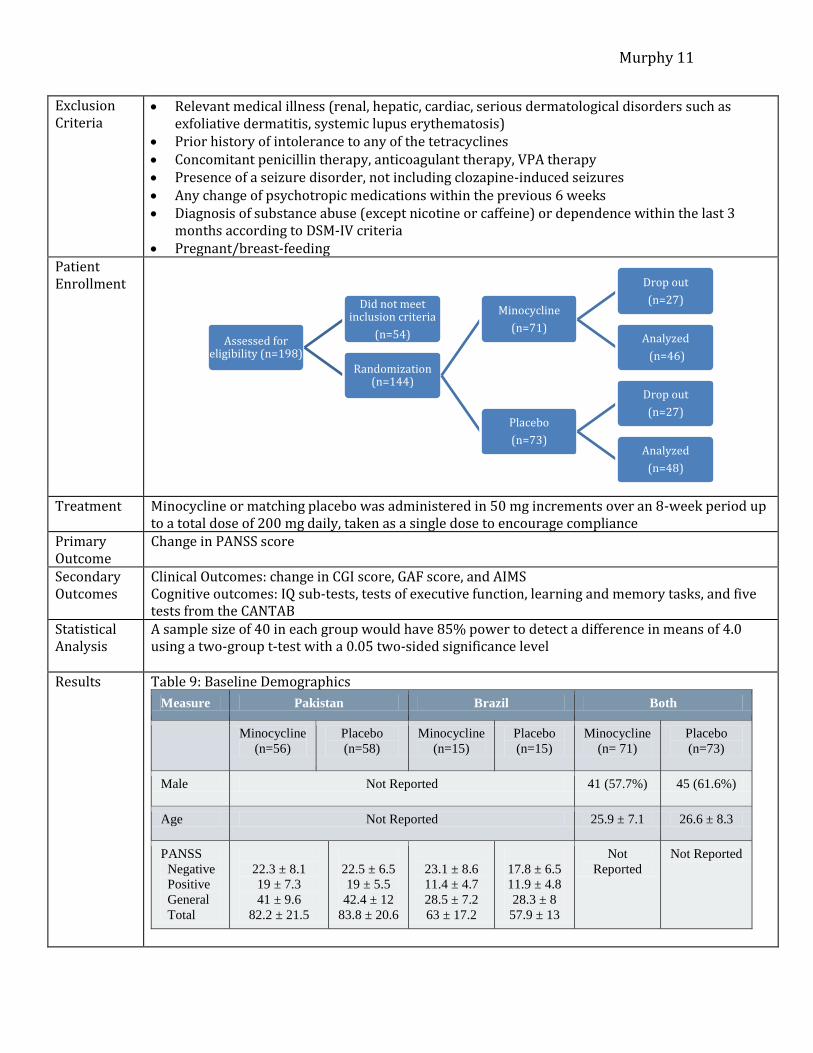
Exclusion Criteria
Relevant medical illness (renal, hepatic, cardiac, serious dermatological disorders such as exfoliative dermatitis, systemic lupus erythematosis)
Prior history of intolerance to any of the tetracyclines Concomitant penicillin therapy, anticoagulant therapy, VPA therapy Presence of a seizure disorder, not including clozapine-induced seizures Any change of psychotropic medications within the previous 6 weeks Diagnosis of substance abuse (except nicotine or caffeine) or dependence within the last 3
months according to DSM-IV criteria Pregnant/breast-feeding
Patient Enrollment
Treatment Minocycline or matching placebo was administered in 50 mg increments over an 8-week period up to a total dose of 200 mg daily, taken as a single dose to encourage compliance
Primary Outcome
Change in PANSS score
Secondary Outcomes
Clinical Outcomes: change in CGI score, GAF score, and AIMS Cognitive outcomes: IQ sub-tests, tests of executive function, learning and memory tasks, and five tests from the CANTAB
Statistical Analysis
A sample size of 40 in each group would have 85% power to detect a difference in means of 4.0 using a two-group t-test with a 0.05 two-sided significance level
Results Table 9: Baseline Demographics
Measure Pakistan Brazil Both
Minocycline
(n=56)
Placebo
(n=58)
Minocycline
(n=15)
Placebo
(n=15)
Minocycline
(n= 71)
Placebo
(n=73)
Male Not Reported 41 (57.7%) 45 (61.6%)
Age Not Reported 25.9 ± 7.1 26.6 ± 8.3
PANSS
Negative
Positive
General
Total
22.3 ± 8.1
19 ± 7.3
41 ± 9.6
82.2 ± 21.5
22.5 ± 6.5
19 ± 5.5
42.4 ± 12
83.8 ± 20.6
23.1 ± 8.6
11.4 ± 4.7
28.5 ± 7.2
63 ± 17.2
17.8 ± 6.5
11.9 ± 4.8
28.3 ± 8
57.9 ± 13
Not
Reported
Not Reported
Assessed for eligibility (n=198)
Did not meet inclusion criteria
(n=54)
Randomization (n=144)
Minocycline
(n=71)
Drop out
(n=27)
Analyzed
(n=46)
Placebo
(n=73)
Drop out
(n=27)
Analyzed
(n=48)
Murphy 12
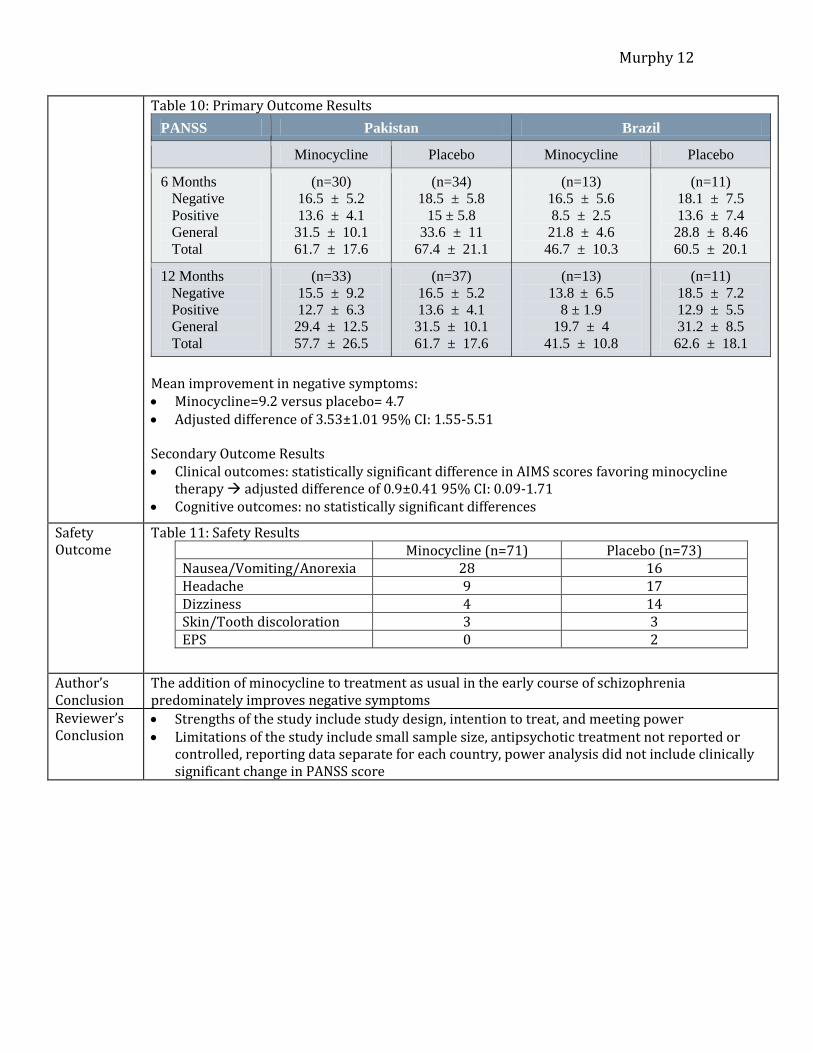
Table 10: Primary Outcome Results
PANSS Pakistan Brazil
Minocycline Placebo Minocycline Placebo
6 Months
Negative
Positive
General
Total
(n=30)
16.5 ± 5.2
13.6 ± 4.1
31.5 ± 10.1
61.7 ± 17.6
(n=34)
18.5 ± 5.8
15 ± 5.8
33.6 ± 11
67.4 ± 21.1
(n=13)
16.5 ± 5.6
8.5 ± 2.5
21.8 ± 4.6
46.7 ± 10.3
(n=11)
18.1 ± 7.5
13.6 ± 7.4
28.8 ± 8.46
60.5 ± 20.1
12 Months
Negative
Positive
General
Total
(n=33)
15.5 ± 9.2
12.7 ± 6.3
29.4 ± 12.5
57.7 ± 26.5
(n=37)
16.5 ± 5.2
13.6 ± 4.1
31.5 ± 10.1
61.7 ± 17.6
(n=13)
13.8 ± 6.5
8 ± 1.9
19.7 ± 4
41.5 ± 10.8
(n=11)
18.5 ± 7.2
12.9 ± 5.5
31.2 ± 8.5
62.6 ± 18.1
Mean improvement in negative symptoms: Minocycline=9.2 versus placebo= 4.7 Adjusted difference of 3.53±1.01 95% CI: 1.55-5.51 Secondary Outcome Results Clinical outcomes: statistically significant difference in AIMS scores favoring minocycline
therapy adjusted difference of 0.9±0.41 95% CI: 0.09-1.71 Cognitive outcomes: no statistically significant differences
Safety Outcome
Table 11: Safety Results Minocycline (n=71) Placebo (n=73) Nausea/Vomiting/Anorexia 28 16 Headache 9 17 Dizziness 4 14 Skin/Tooth discoloration 3 3 EPS 0 2
Author’s Conclusion
The addition of minocycline to treatment as usual in the early course of schizophrenia predominately improves negative symptoms
Reviewer’s Conclusion
Strengths of the study include study design, intention to treat, and meeting power Limitations of the study include small sample size, antipsychotic treatment not reported or
controlled, reporting data separate for each country, power analysis did not include clinically significant change in PANSS score
Murphy 13
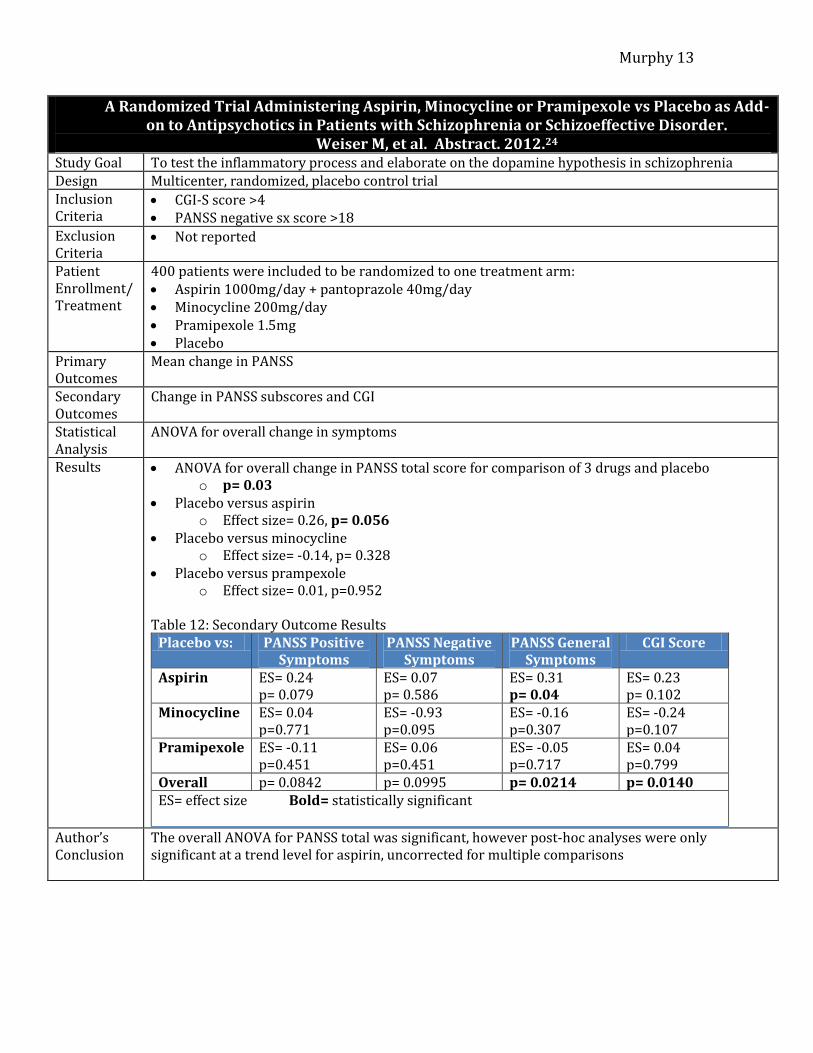
A Randomized Trial Administering Aspirin, Minocycline or Pramipexole vs Placebo as Add-on to Antipsychotics in Patients with Schizophrenia or Schizoeffective Disorder.
Weiser M, et al. Abstract. 2012.24 Study Goal To test the inflammatory process and elaborate on the dopamine hypothesis in schizophrenia Design Multicenter, randomized, placebo control trial Inclusion Criteria
CGI-S score >4 PANSS negative sx score >18
Exclusion Criteria
Not reported
Patient Enrollment/ Treatment
400 patients were included to be randomized to one treatment arm: Aspirin 1000mg/day + pantoprazole 40mg/day Minocycline 200mg/day Pramipexole 1.5mg Placebo
Primary Outcomes
Mean change in PANSS
Secondary Outcomes
Change in PANSS subscores and CGI
Statistical Analysis
ANOVA for overall change in symptoms
Results ANOVA for overall change in PANSS total score for comparison of 3 drugs and placebo o p= 0.03
Placebo versus aspirin o Effect size= 0.26, p= 0.056
Placebo versus minocycline o Effect size= -0.14, p= 0.328
Placebo versus prampexole o Effect size= 0.01, p=0.952
Table 12: Secondary Outcome Results
Placebo vs: PANSS Positive Symptoms
PANSS Negative Symptoms
PANSS General Symptoms
CGI Score
Aspirin ES= 0.24 p= 0.079
ES= 0.07 p= 0.586
ES= 0.31 p= 0.04
ES= 0.23 p= 0.102
Minocycline ES= 0.04 p=0.771
ES= -0.93 p=0.095
ES= -0.16 p=0.307
ES= -0.24 p=0.107
Pramipexole ES= -0.11 p=0.451
ES= 0.06 p=0.451
ES= -0.05 p=0.717
ES= 0.04 p=0.799
Overall p= 0.0842 p= 0.0995 p= 0.0214 p= 0.0140 ES= effect size Bold= statistically significant
Author’s Conclusion
The overall ANOVA for PANSS total was significant, however post-hoc analyses were only significant at a trend level for aspirin, uncorrected for multiple comparisons
Murphy 14
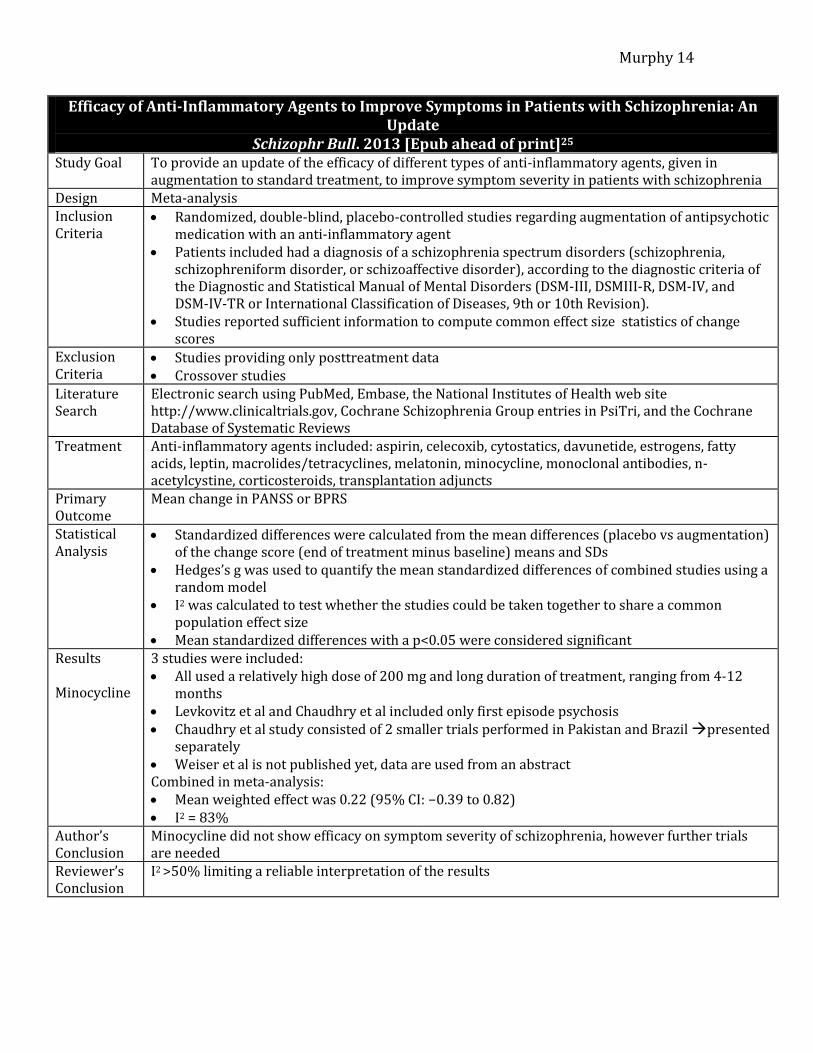
Efficacy of Anti-Inflammatory Agents to Improve Symptoms in Patients with Schizophrenia: An Update
Schizophr Bull. 2013 [Epub ahead of print]25
Study Goal To provide an update of the efficacy of different types of anti-inflammatory agents, given in augmentation to standard treatment, to improve symptom severity in patients with schizophrenia
Design Meta-analysis Inclusion Criteria
Randomized, double-blind, placebo-controlled studies regarding augmentation of antipsychotic medication with an anti-inflammatory agent
Patients included had a diagnosis of a schizophrenia spectrum disorders (schizophrenia, schizophreniform disorder, or schizoaffective disorder), according to the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III, DSMIII-R, DSM-IV, and DSM-IV-TR or International Classification of Diseases, 9th or 10th Revision).
Studies reported sufficient information to compute common effect size statistics of change scores
Exclusion Criteria
Studies providing only posttreatment data Crossover studies
Literature Search
Electronic search using PubMed, Embase, the National Institutes of Health web site http://www.clinicaltrials.gov, Cochrane Schizophrenia Group entries in PsiTri, and the Cochrane Database of Systematic Reviews
Treatment Anti-inflammatory agents included: aspirin, celecoxib, cytostatics, davunetide, estrogens, fatty acids, leptin, macrolides/tetracyclines, melatonin, minocycline, monoclonal antibodies, n-acetylcystine, corticosteroids, transplantation adjuncts
Primary Outcome
Mean change in PANSS or BPRS
Statistical Analysis
Standardized differences were calculated from the mean differences (placebo vs augmentation) of the change score (end of treatment minus baseline) means and SDs
Hedges’s g was used to quantify the mean standardized differences of combined studies using a random model
I2 was calculated to test whether the studies could be taken together to share a common population effect size
Mean standardized differences with a p<0.05 were considered significant Results Minocycline
3 studies were included: All used a relatively high dose of 200 mg and long duration of treatment, ranging from 4-12
months Levkovitz et al and Chaudhry et al included only first episode psychosis Chaudhry et al study consisted of 2 smaller trials performed in Pakistan and Brazil presented
separately Weiser et al is not published yet, data are used from an abstract Combined in meta-analysis: Mean weighted effect was 0.22 (95% CI: −0.39 to 0.82) I2 = 83%
Author’s Conclusion
Minocycline did not show efficacy on symptom severity of schizophrenia, however further trials are needed
Reviewer’s Conclusion
I2 >50% limiting a reliable interpretation of the results

Murphy 15
Schizophrenia is a complex disease state with many potential pathophysiological causes
Current treatments are more effective at reducing positive symptoms compared to negative symptoms
Preliminary evidence suggests minocycline may have a role in the treatment of schizophrenia
Further research is needed to determine minocycline’s place in therapy
Content Critique: Lisa Mican, PharmD
Style Critique: TBD
Primary Reviewer: Mina Mehvar, PharmD
Addition Reviewers: Emily Czeck, PharmD Katerine Getchell, PharmD
Conclusions
Acknowledgments
Murphy 16
1. World Health Organization. Schizophrenia Statistics (2013). 2. Stahl, SM. Essential Pharmacology, 4th edition. (2013) 3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
Disorders (Revised 4th ed. Text Revision). Washington, DC: American Psychiatric Publishing;2000.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. (5th ed.). Arlington, VA: American Psychiatric Publishing;2013.
5. Fineberg AM, Ellman LM. Inflammatory cytokines and neurological and neurocognitive alterations in the course of schizophrenia. Biol Psychiatry. 2013;73:951–966.
6. American Psychiatric Association. Practice guideline for the treatment of patients with schizophrenia. 2nd ed. Arlington (VA): American Psychiatric Association; 2004.
7. Moore TA, Buchanan RW, Buckley PF, et al. The Texas Medication Algorithm Project Antipsychotic Algorithm for Schizophrenia: 2006 Update. J Clin Psychiatry 2007;68:1751-1762.
8. World Federation of Societies of Biological Psychiatry Guidelines of Biological Treatment of Schizophrenia. World J of Biol Psychiatry. 2005; 6(3): 132-191.
9. Kreyenbuhl J, Buchanan RW, Dickerson FB, et al. The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2009. Schizophr Bull. 2010;36(1):94-103.
10. Solodyn [package insert]. Scottsdale, AZ: Medicis; August 2012. 11. Dynacin [package insert]. Spring Valley, NY: Par Pharmaceuticals;
November 2011. 12. Ximino [package insert]. Jacksonville, FL: Ranbaxy Labs; July 2012. 13. Minocin [package insert]. Cranford, NJ: Triax Pharmaceuticals; August 2010. 14. Minocin Kit [package insert]. Cranford, NJ: Triax Pharmaceuticals; August
2010. 15. Dean OM, Data-Franco J, Giorlando F, et al. Minocycline Therapuetic Potential
in Psychiatry. CNS Drugs. 2012;26(5):391-401. 16. Miyaoka T. Minocycline for Schizophrenia: A Critical Review. OJ Psych.
(2012) 399-406. 17. Garrido-Mesa N, Zarsuelo A, Galvez J. What is Behind the Non-Antibiotic
Properties of Minocycline? Pharmacological Research. 2013;67:18-30. 18. Miyaoka T, Yasukawa R, Yasuda H, et al. Possible antipsychotic effects of
minocycline in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry 2007;31:304-307.
19. Kelly DL et al. Adjunct minocycline to clozapine treated patients with persistent schizophrenia symptoms. Schizophrenia Research. 2011;133:257-258.
20. Jhamnani K, et al. Successful Use of Add-on Minocycline for Treatment of Persistent Negative Symptoms in Schizophrenia. J Neuropsychiatry Clin Neuro Sci. 2013; 25(1):E06-7.
References
Murphy 17
21. Miyaoka T, Yasukawa R, Yasuda H, et al. Minocycline as Adjunctive Therapy for Schizophrenia: An Open-Label Study. Clin Neuropharmacol. 2008;31:287-292.
22. Levkovitz Y, Mendlovich S, Riwkes S, et al. A double-blind, randomized study of minocycline for the treatment of negative and cognitive symptoms in early-phase schizophrenia. J Clin Psychiatry. 2010;71:138–149.
23. Chaudhry IB, Hallak J, Husain N, et al Minocycline benefits negative symptoms in early schizophrenia: a randomized double-blind placebo-controlled clinical trial in patients on standard treatment. J Psychopharmacol. 2012;26:1185–1193.
24. Weiser M, Burstein S, Fodoreanu L, et al. A Randomized Trial Administering Aspirin, Minocycline or Pramipexole vs Placebo as Add-on to Antipsychotics in Patients with Schizophrenia or Schizoeffective Disorder. Abstract. 2012.
25. Sommer IE, van Westrhenen R, Begemann MJ, et al. Efficacy of Anti-inflammatory Agents to Improve Symptoms in Patients With Schizophrenia: An Update. Schizophr Bull. 2013 Oct 8. [Epub ahead of print]
26. Andreasen NC: Scale for the Assessment of Negative Symptoms (SANS). Iowa City, University of Iowa, 1984
27. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull 1987;13(2):261–276.
28. Guy W: ECDEU Assessment Manual for Psychopharmacology-Revised. Rockville, MD, U.S. Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, NIMH Psychopharmacology Research Branch, Division of Extramural Research Programs (1976) 218–222
29. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychological Reports 1962;10:799-812.
30. Muller MJ, Brening H, Gensch C, et al. The Calgary Depression Rating Scale for schizophrenia in a healthy control group: Psychometric properties and reference values. Journal of Affective Disorders. 2005; 88: 69-74.
31. ECDEU Assessment Manual for Psychopharmacology, Guy W, ed, Washington DC: U.S. Department of Health, Education and Welfare, 1976.
32. Robbins TW, James M, Owen AM, et al. A study of performance on tests from the CANTAB battery sensitive to frontal lobe dysfunction in a large sample of normal volunteers: Implications for theories of executive functioning and cognitive aging. Journal of the International Neuropsychological Society 1998;4: 474-490.
33. Goldman HH, Skodol AE, Lave TR. Revising Axis X for DSM-IV: A review of measures of social functioning. American Journal of Psychiatry. 1992; 149: 1148-1156.

Murphy 18
Scale for Assessment of Negative Symptoms (SANS)26 o Used to measure negative symptoms in schizophrenia split into 5
domains, and within each domain separate symptoms are rated from 0 (absent) to 5 (severe)
o Response is variable however a percentage improvement has not been consistently used in the literature to define a response
Positive and Negative Syndrome Scale (PANSS)27 o Validated 30-item clinician administered rating scale used to assess the
effects of drug treatment in schizophrenia o Assess positive, negative, and general psychopathology symptoms rated
on a scale of 1 to 7: “not present” to “extremely severe” o Response is variable: generally 20-30% reduction
Clinical Global Impression (CGI)27 o Provides an overall clinician-determined summary measure that takes
into account all available information, including a knowledge of the patient's history, psychosocial circumstances, symptoms, behavior, and the impact of the symptoms on the patient's ability to function.
o Response is variable but generally much improved to very much improved indicates response
Brief Psychiatric Rating Scale (BPRS)28 o One of the oldest, widely used clinician administered scales to measure
psychotic symptoms rated on a scale of 1 to 7: “not present” to “most severe”
o Response is variable: generally 20-40% reduction Global Assessment of Functioning (GAF)29
o Clinician rated, functional assessment scale rated 1 (most impaired) to 100 (healthiest)
o Response is variable Calgary Depression Scale for Schizophrenia30
o Clinician rated assessment scale for depressive symptoms o Assesses depressive symptoms in schizophrenia separate from that
related to positive, negative, and EPS o Score above 6 has an 82% specificity and 85% sensitivity for predicting
presence of major depressive episode Abnormal Involuntary Movement Scale (AIMS)31
o Clinician rated scale used to assess for dyskinesias such as tardive dyskinesia
o Not a diagnostic tool but provides ratings that can be used in diagnostic criteria
o 12 item scale rated on a continuum of 0 (none) to 4 (severe) o Response is not defined
Appendix A- Rating Scales
Murphy 19
Cambridge Neuropsychological Test Automated Battery (CANTAB)32 o Computer-based cognitive assessment system consisting of a battery of
neuropsychological tests, administered to subjects using a touch screen computer.
o Consists of 22 tests that examine various areas of cognitive function including:
General memory and learning Working memory and executive function Visual memory Attention and reaction time Semantic/verbal memory Decision making and response control
o Response is variable Social and Occupational Functioning Assessment Scale (SOFAS)33
o Clinician rated scale that considers social and occupational functioning on a continuum from excellent functioning to grossly impaired functioning
o Includes impairments in functioning due to physical limitations, as well as those due to mental impairments
o Impairment must be a direct consequence of mental and physical health problems
o Response is variable
AIMS= Abnormal Involuntary Movement Scale AP=antipsychotic APA= American Psychiatric Association CGI=Clinical Global Impression Scale DA=dopamine DSM=Diagnostic and Statistical Manual EPS=extrapyramidal symptoms ES=effect size FGA=first generation antipsychotic GAF=Global Assessment of Functioning I2=homogeneity statistic IPAP= International psychopharmacology Algorithm Project PANSS=Positive and Negative Syndrome Scale PORT=Patient Outcomes Research Team SANS=Scale for Assessment of Negative Symptoms SGA=second generation antipsychotic SOFAS= Social and Occupational Functioning Assessment Scale Sx=symptoms TAU=treatment as usual TMAP=Texas Medication Algorithm Project
Appendix B- Abbreviations