miniscrew implant-supported maxillary canine retraction ...miniscrew implant-supported maxillary...
TRANSCRIPT

ORIGINAL ARTICLE
Miniscrew implant-supported maxillarycanine retraction with and withoutcorticotomy-facilitated orthodontics
Shadw Mohammed Badr El-Din Aboul-Ela,a Amr Ragab El-Beialy,b Karim Mohamed Fawzy El-Sayed,c
Essam Mohamed Nassef Selim,d Nagwa Helmy EL-Mangoury,e and Yehya Ahmed Mostafad
Cairo, Egypt
aAssoFaculCairo,bAssoFaculcAssoOral adProfeof OraeProfepaediThe aucts oReprintofaciMinaSubm0889-Copyrdoi:10
252
Introduction: The purpose of this study was to clinically evaluate miniscrew implant-supported maxillary canineretraction with corticotomy-facilitated orthodontics.Methods: The sample consisted of 13 adult patients (5 men,8 women; mean age, 19 years) exhibiting Class II Division 1 malocclusion with increased overjet requiring thetherapeutic extraction of the maxillary first premolars, with subsequent retraction of the maxillary canines.Corticotomy-facilitated orthodontics was randomly assigned to 1 side of the maxillary arch at the canine-premolar region, and the other side served as the control. By using miniscrews as anchorage, canineretraction was initiated via closed nickel-titanium coil springs applying 150 g of force per side. The followingvariables were examined over a 4-month follow-up period: rate of tooth movement, molar anchorage loss,plaque index, gingival index, probing depth, attachment loss, and gingival recession.Results: The average dailyrate of canine retraction was significantly higher on the corticotomy than the control side by 2 times during the first2 months after the corticotomy surgery. This rate of tooth movement declined to only 1.6 times higher in the thirdmonth and 1.06 times higher by the end of the fourth month. No molar anchorage loss occurred during canineretraction on either the operated or the nonoperated side. There was no statistically significant differencebetween preoperative and postoperative measurements of plaque index, probing depth, attachment loss, andgingival recession. Conclusions: Corticotomy-facilitated orthodontics can be a feasible treatment modalityfor adults seeking orthodontic treatment with reduced treatment times. (Am J Orthod Dentofacial Orthop2011;139:252-9)
The goal of orthodontic treatment is to improve thepatient’s life adjustment through enhancement ofdentofacial functions and esthetics. Reducing or-
thodontic treatment duration is an issue of importance,particularly for adults. Rapid orthodontic toothmovementwith concomitant reduction in treatment time can be
ciate lecturer, Department of Orthodontics and Dentofacial Orthopaedics,ty of Oral and Dental Medicine, Misr University for Science and Technology,Egypt.ciate lecturer, Department of Orthodontics and Dentofacial Orthopaedics,ty of Oral and Dental Medicine, Cairo University, Cairo, Egypt.ciate lecturer, Department of Oral Medicine and Periodontology, Faculty ofnd Dental Medicine, Cairo University, Cairo, Egypt.ssor, Department of Orthodontics and Dentofacial Orthopaedics, Facultyl and Dental Medicine, Cairo University, Cairo, Egypt.ssor and chairperson, Department of Orthodontics and Dentofacial Ortho-cs, Faculty of Oral and Dental Medicine, Cairo University, Cairo, Egypt.uthors report no commercial, proprietary, or financial interest in the prod-r companies described in this article.t requests to: Yehya Ahmed Mostafa, Department of Orthodontics and Den-al Orthopaedics, Faculty of Oral and Dental Medicine, Cairo University, 60Garden City, 6th of October City, Cairo, Egypt; e-mail, [email protected], January 2009; revised and accepted, April 2009.5406/$36.00ight � 2011 by the American Association of Orthodontists..1016/j.ajodo.2009.04.028
attained through a combination of orthodontic treatmentand surgical alveolar corticotomies.1-5 Corticotomy isdefined as any intentional surgical injury to corticalbone. In adult patients, this technique has beenclaimed to dramatically reduce the treatment timebecause the resistance of the dense cortical bone toorthodontic tooth movement is removed.1,3,6-8 Thealveolar corticotomy technique has been revised andmodified over the years to eliminate its possible risks,such as periodontal damage and devitalization of theteeth and osseous segments because of inadequateblood supply. According to K€ole,1 the tooth embeddedin a bony block of medullary bone served as the handleby which bands of less dense medullary bone sur-rounding the teeth were moved block by block. Onthe other hand, Wilcko et al9 attributed the increasedrate of tooth movement after corticotomy-facilitatedorthodontics (CFO) to a “regional acceleratory phe-nomenon” (RAP), which is characterized by an increasein bone turnover and a drop in mineral content.
Securing appropriate anchorage is an imperativefactor for achieving the objectives of orthodontic
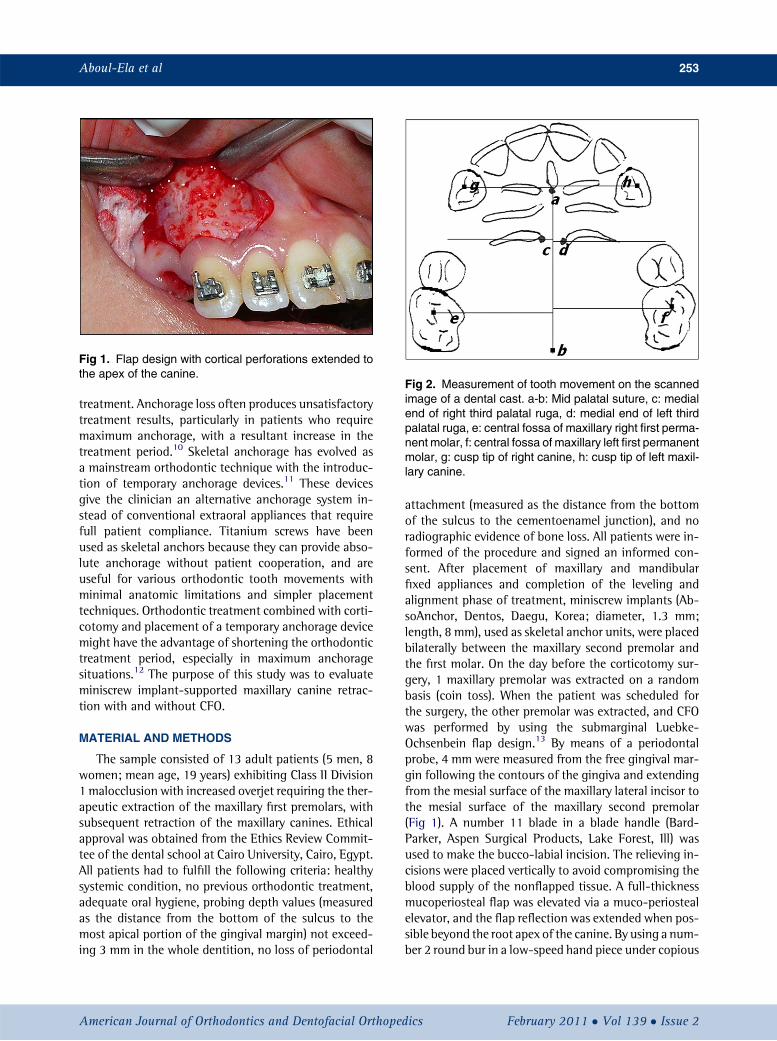
Fig 1. Flap design with cortical perforations extended tothe apex of the canine.
Fig 2. Measurement of tooth movement on the scannedimage of a dental cast. a-b: Mid palatal suture, c: medialend of right third palatal ruga, d: medial end of left thirdpalatal ruga, e: central fossa of maxillary right first perma-nent molar, f: central fossa of maxillary left first permanentmolar, g: cusp tip of right canine, h: cusp tip of left maxil-lary canine.
Aboul-Ela et al 253
treatment. Anchorage loss often produces unsatisfactorytreatment results, particularly in patients who requiremaximum anchorage, with a resultant increase in thetreatment period.10 Skeletal anchorage has evolved asa mainstream orthodontic technique with the introduc-tion of temporary anchorage devices.11 These devicesgive the clinician an alternative anchorage system in-stead of conventional extraoral appliances that requirefull patient compliance. Titanium screws have beenused as skeletal anchors because they can provide abso-lute anchorage without patient cooperation, and areuseful for various orthodontic tooth movements withminimal anatomic limitations and simpler placementtechniques. Orthodontic treatment combined with corti-cotomy and placement of a temporary anchorage devicemight have the advantage of shortening the orthodontictreatment period, especially in maximum anchoragesituations.12 The purpose of this study was to evaluateminiscrew implant-supported maxillary canine retrac-tion with and without CFO.
MATERIAL AND METHODS
The sample consisted of 13 adult patients (5 men, 8women; mean age, 19 years) exhibiting Class II Division1 malocclusion with increased overjet requiring the ther-apeutic extraction of the maxillary first premolars, withsubsequent retraction of the maxillary canines. Ethicalapproval was obtained from the Ethics Review Commit-tee of the dental school at Cairo University, Cairo, Egypt.All patients had to fulfill the following criteria: healthysystemic condition, no previous orthodontic treatment,adequate oral hygiene, probing depth values (measuredas the distance from the bottom of the sulcus to themost apical portion of the gingival margin) not exceed-ing 3 mm in the whole dentition, no loss of periodontal
American Journal of Orthodontics and Dentofacial Orthoped
attachment (measured as the distance from the bottomof the sulcus to the cementoenamel junction), and noradiographic evidence of bone loss. All patients were in-formed of the procedure and signed an informed con-sent. After placement of maxillary and mandibularfixed appliances and completion of the leveling andalignment phase of treatment, miniscrew implants (Ab-soAnchor, Dentos, Daegu, Korea; diameter, 1.3 mm;length, 8 mm), used as skeletal anchor units, were placedbilaterally between the maxillary second premolar andthe first molar. On the day before the corticotomy sur-gery, 1 maxillary premolar was extracted on a randombasis (coin toss). When the patient was scheduled forthe surgery, the other premolar was extracted, and CFOwas performed by using the submarginal Luebke-Ochsenbein flap design.13 By means of a periodontalprobe, 4 mm were measured from the free gingival mar-gin following the contours of the gingiva and extendingfrom the mesial surface of the maxillary lateral incisor tothe mesial surface of the maxillary second premolar(Fig 1). A number 11 blade in a blade handle (Bard-Parker, Aspen Surgical Products, Lake Forest, Ill) wasused to make the bucco-labial incision. The relieving in-cisions were placed vertically to avoid compromising theblood supply of the nonflapped tissue. A full-thicknessmucoperiosteal flap was elevated via a muco-periostealelevator, and the flap reflection was extended when pos-sible beyond the root apex of the canine. By using a num-ber 2 round bur in a low-speed hand piece under copious
ics February 2011 � Vol 139 � Issue 2

Table I. Descriptive statistics of molar anchorage lossin operated and nonoperated subjects
Operated NonoperatedMean (preoperative) 13.79 6 1.157 13.62 6 1.062Mean (postoperative) 13.73 6 1.163 13.50 6 1.100
Mean 6 SD (mm).
Table II. Mean rates of anteroposterior position of themaxillary canines in the corticotomy and control sidesper month (mm)
Month 1 Month 2 Month 3 Month 4Operated 1.89 1.83 1.07 0.89Nonoperated 0.75 0.86 0.93 0.85
Fig 3. A, Class I canine relationship achieved 2 monthsafter retraction on the operated side; B, Class I caninerelationship not achieved on the nonoperated side.
254 Aboul-Ela et al
irrigation, corticotomy perforations were made extend-ing from the lateral incisor to the first premolar area.The depth of the holes approximated the width of thebuccal cortical bone. Thereafter, the flap was carefullyrepositioned and sutured with nonresorbable 4-0 blacksilk by using the single interrupted technique. The max-illary archwire (0.0163 0.022-in stainless steel) was thenligated, and nickel-titanium closed-coil springs applying150 g on each side were used for retraction, stretched bi-laterally from the miniscrews to the canine hooks.
Periodontal health was assessed by evaluating thefollowing parameters: plaque index, gingival index,probing depth, attachment level, and gingival recessionaccording to the method of Silness and Loe.14 Dentalcasts were used for the quantification of the anteropos-terior movement of the canines and the first molars(Fig 2) every 30 days with the method described byZiegler and Ingervall.15
Statistical analysis
Descriptive statistics were computed for the variablesof tooth movement (canine retraction and molar an-chorage loss) and periodontal indices before and aftercanine retraction, and the results were graphically repre-sented (Tables I and II; Figs 3-10). A paired t test wasused to determine the statistical significance of thedifference between the operated and nonoperatedsides for preoperative and postoperative measurements.
RESULTS
There were statistically significant differences(P #0.01) in the rates of anteroposterior movement ofthe canines between the operated and nonoperated sidesat all measurement times, and the rates of canine retrac-tion were consistently higher in the operated than in thenonoperated side. There was no statistically significant
February 2011 � Vol 139 � Issue 2 American
difference (P.0.05) in plaque index scores, attachmentloss, gingival recession, and probing depth valuesbetween the operated and nonoperated sides measuredpreoperatively and at 4 months postoperatively. On theother hand, gingival index scores were significantlyhigher (P \0.05) on the operated side compared withthe nonoperated side by the end of the study.
DISCUSSION
The subjects selected for this study all had a Class IIDivision 1 malocclusion. The treatment plan requiredthe extraction of the maxillary first premolars and thesubsequent retraction of the maxillary canines. Westarted with 15 patients, but 2 patients were excludedfrom the study—1 because of multiple missed appoint-ments and the other because of poor oral hygiene.A considerable amount of patient cooperation wasnecessary; the patients were expected to comply withthe instructions regarding strict attention to oral hygienemeasures and keeping the follow-up visits.
Journal of Orthodontics and Dentofacial Orthopedics

Fig 4. Cumulative mean changes of anteroposterior position of the canines in the corticotomy andcontrol sides.
Fig 5. Mean changes of anteroposterior position of the canines in the corticotomy and control sides permonth.
Aboul-Ela et al 255
In this study, it was hypothesized that the cortico-tomy technique could be used to reduce treatmenttime by facilitating tooth movement. CFO has beenclaimed to dramatically reduce the treatment timebecause the resistance of the dense cortical bone to or-thodontic tooth movement is removed.3,6,16,17 In thisstudy, cortical perforations were made in the buccalcortical plate of bone only without vertical orsubapical cuts and without the reflection of a palatalflap. The justification of this is the assumption that theRAP induced by the buccal corticotomy would readilyinvolve the noncorticotomized palatal side. Moreover,the main purposes of adopting this conservative techniquewere to reduce operation time and postoperativepatient discomfort by eliminating exposure of thepatient to the risks of an additional palatal surgery. Thesubmarginal Luebke-Ochsenbein flap was used insteadof the conventional flap design of the corticotomy
American Journal of Orthodontics and Dentofacial Orthoped
surgery, which uses an intrasulcular incision. In thisflap design, 2mmof attached gingivamust remain apicalto the depth of the gingival sulcus, and there must beenough tissue remaining to allow suture placement.The relieving incisions were placed vertically to preventcompromising the blood supply of the nonflappedtissue.13 These modifications attempted to optimize thetreatment outcome of the surgical procedure withminimal if any effects on the periodontium.
It is well known that, in most orthodontic extractionpatients, anchorage reinforcement is of prime impor-tance. Effective and reliable anchorage will dramaticallyimprove the results of treatment.18 In this study, mini-screw implants were used as skeletal anchorage duringcanine retraction because of their simpler placementtechnique and the possibility of eliminating the relianceon patient compliance. Assessment of miniscrew mobil-ity after loading showed no mobility during canine
ics February 2011 � Vol 139 � Issue 2

Fig 6. Preoperative and postoperative changes of the plaque index scores in the corticotomy andcontrol sides.
Fig 7. Preoperative and postoperative changes of the gingival index scores in the corticotomy andcontrol sides.
256 Aboul-Ela et al
retraction except for 2 miniscrews. One screw becameloose 1 month after loading and the other 1.5 monthsafter loading. These miniscrews were immediately repo-sitioned between the maxillary first and second molars,and canine retraction was resumed. These findingsshowed that the success rate of miniscrews in this studywas approximately 93%, which is in accordance withprevious reports.18-20
The miniscrews selected had a diameter of 1.3 mmand a length of 8 mm. This was based on the recommen-dations of Kuroda et al.11 The rationale was to optimizethe mechanical retention of the screws and eliminate anyrisks of root proximity or contact that might contributeto failure during treatment. The placement site of the
February 2011 � Vol 139 � Issue 2 American
miniscrews, between the maxillary second premolarand the first molar buccally, was selected based on therecommendations of Schnelle et al,21 who advocatedthis site as bone stock for safe miniscrew placement inthe maxillary arch. Placement of the miniscrews was per-formed in the attached gingiva rather than the nonker-atinized mucosa because we expected that the successrates would be higher, placement and retrieval wouldbe simpler, and the likelihood of tissue proliferationaround the miniscrews would be eliminated. The factthat the miniscrews were placed in tight soft tissue,where no incisions were required, might have contrib-uted to the relatively high stability of the screws withbetter patient acceptance to the overall procedure. These
Journal of Orthodontics and Dentofacial Orthopedics

Fig 8. Preoperative and postoperative changes of the probing depth values in the corticotomy andcontrol sides.
Fig 9. Preoperative and postoperative changes of the attachment loss values in the corticotomy andcontrol sides.
Aboul-Ela et al 257
findings are in accordance with the report of Kurodaet al,22 who reported that miniscrews implanted withoutflap surgery have higher success rates with less painand discomfort than those placed with flap surgery.
Nickel-titanium springs were used for retraction topermit constant force application. The medial end ofthe third palatal rugae was used as the reference pointto construct reference planes for measurement of toothmovement and quantification of changes in toothposition on the dental casts.14,23-26
The results in this study have demonstrated that it ispossible to rapidly retract the canines by using CFO. Theanteroposterior changes in the position of the canineswere significantly higher on the corticotomy side thanon the control side during the first and second months
American Journal of Orthodontics and Dentofacial Orthoped
of the follow-up period (Fig 3). During the first 2 monthsafter the corticotomy surgery, the average monthly rateof canine retraction was significantly higher: approxi-mately 2 times faster on the corticotomy side comparedwith the control side. On the other hand, during the thirdand fourth months, this mean monthly rate, though stillhigher on the corticotomy than the control side, declinedto only 1.6 times higher in the third month and 1.06times higher by the end of the fourth month (Fig 5).This information is consistent with the transient natureof the RAP.
In 6 patients (approximately 45%), a Class I caninerelationship was achieved in 4 patients after 2 monthsand in 2 patients after 3 months of retraction. On theother hand, no canine on the control side was retracted
ics February 2011 � Vol 139 � Issue 2

Fig 10. Preoperative and postoperative changes of the gingival recession values in the corticotomyand control sides.
258 Aboul-Ela et al
to a Class I canine relationship until the end of thestudy.
The findings in this study agree with those of Wilckoet al,9 Iino et al,17 Ren et al,27 and Mostafa et al,5 whoreported that tooth movement velocity on the cortico-tomy side was 2 to 3 times faster than that on the controlside. On the other hand, the reason for the rapid canineretraction can only be speculated, since no histologicstudy was carried out. Because the lingual corticalbone was left intact and bone blocks surrounding theteeth were not made, the rapid rate of tooth movementseemed to depend mostly on a RAP rather than bonyblock movement. However, further histologic studieswith longer follow-up periods are required to investigatethe underlying biologic background of the corticotomyprocedure.
No significant molar anchorage loss occurred duringcanine retraction on either the corticotomy or thecontrol side (Table I). These results showed that titaniummicroimplants can function as simple and efficient an-chors for canine retraction especially when moderateto maximum anchorage is desired. These results agreewith the findings of Thiruvenkatachari et al,18,28 whoadvocated the use of implants as anchorage during theretraction of canines as a viable alternative toconventional molar anchorage.
Several reports have been published regarding theadverse effects to the periodontium after CFO. Thesereports range from no problems to slight interdentalbone loss, decrease of attached gingiva, and periodontaldefects observed in some cases with short interdentaldistances.6,9,12 Bell and Levy2 reported a damagingeffect to the periodontium around the incisors aftercorticotomy cuts at the premolar and incisor regions in4 rhesus monkeys. According to the authors, alterationof the circulation could reduce the viability of the
February 2011 � Vol 139 � Issue 2 American
bone and teeth, affect the healing capacity of the mobi-lized bone, and have a destructive effect on the perio-dontium. On the other hand, Dǘker,4 Gantes et al,6
and Suya8 speculated that, by keeping the vertical corti-cotomies 1.5 mm shy of the crest of the marginal bone,there would be less chances of damaging the marginalperiodontium. In this study, we observed no hazardousside effects from the corticotomy surgery on the perio-dontium. Assessment of probing depths, attachmentloss, and gingival recession in particular showed no sig-nificant differences between the operated and nonoper-ated sides (Figs 8-10). These results agree with thefindings of Anholm et al,29 Gantes et al,6 Suya,8 Wilckoet al,9 and Iino et al,12 who reported rapid tooth move-ment and reduced treatment times without clinicallynoticeable adverse periodontal effects from the CFO.
In our study, the conventional flap design of the cor-ticotomy surgery, with an intrasulcular incision, wasreplaced with the submarginal Luebke-Ochsenbeinflap.13 The fact that the marginal bone was not incisedduring the surgery and an intrasulcular incision wasnot made could have resulted in optimization of theperiodontal condition after the surgery. The reason forthe absence of any effects on the periodontium afterthe corticotomy procedure could be attributed to themanner of bone removal, because the corticotomy wasnot done as a true osteotomy, with a block of bone re-moved. The procedure only perforated the bone, leavingthe original bony architecture intact. This allowed theresorption-deposition cellular process to proceed in theexisting bony architecture. On the other hand, Yaffeet al30 reported that RAP begins a few days after the sur-gery, peaks between 1 and 2 months, and takes from 6 to24 months to resolve completely. These findings mightexplain the higher gingival index scores on the cortico-tomy side compared with the control side in this study,
Journal of Orthodontics and Dentofacial Orthopedics

Aboul-Ela et al 259
when the longer times required for complete resolution ofthe RAP after the corticotomy surgical procedure mighthave contributed to elevated gingival index scores.
CONCLUSIONS
On the basis of the results obtained from this study,the following conclusions can be drawn.
1. CFO can be an effective method for patients whodesire shortened orthodontic treatment durations.
2. The Luebke-Ochsenbein flap design is a feasible andan applicable modification to the original cortico-tomy flap design.
3. Miniscrew implants can function as viable alterna-tives to conventional molar anchorage. They aresimple and efficient anchors for canine retraction,especially in moderate to maximum anchoragesituations.
REFERENCES
1. K}ole H. Surgical operations on the alveolar ridge to correct occlusalabnormalities. Oral Surg 1959;12:515-29.
2. Bell WH, Levy BM. Revascularization and bone healing after max-illary corticotomies. J Oral Surg 1972;30:640-8.
3. Chung KR, Oh MY, Ko SJ. Corticotomy-assisted orthodontics.J Clin Orthod 2001;35:331-8.
4. Dǘker J. Experimental animal research into segmental alveolarmovement after corticotomy. J Maxillofac Surg 1975;3:81-4.
5. Mostafa YA, Fayed MS, Mehanni S, ElBokle NN, Heider AM. Com-parison of corticotomy-facilitated vs standard tooth-movementtechniques in dogs with miniscrews as anchor units. Am J OrthodDentofacial Orthop 2009;136:570-7.
6. Gantes B, Rathbun E, Anholm M. Effects on the periodontiumfollowing corticotomy-facilitated orthodontics. Case reports.J Periodontol 1990;61:234-8.
7. Generson RM, Porter JM, Zell A. Combined surgical andorthodontic management of anterior open bite using corticotomy.J Oral Surg 1978;36:216-9.
8. Suya H. Corticotomy in orthodontics. In: H}osl E, Baldauf A, editors.Mechanical and biological basics in orthodontic therapy. Heidel-berg, Germany: Huthig Buch Verlag; 1991. p. 207-26.
9. Wilcko W, Wilcko T, Bouquot E. Rapid orthodontics with alveolarreshaping: two case reports of crowding. Int J Periodontics Restor-ative Dent 2001;21:9-19.
10. El Beialy AR. Clinical and radiographic assessment of self-drillingsurgical screws used for anchorage reinforcement [thesis]. Cairo,Egypt: Cairo University; 2007.
11. Kuroda S, Yamada K, Deguchi T, Hashimoto T. Root proximity isa major factor for screw failure in orthodontic anchorage. Am J Or-thod Dentofacial Orthop 2007;131(Suppl):S68-73.
12. Iino S, Sakoda S, Miyawaki S. An adult bimaxillary protrusiontreated with corticotomy-facilitated orthodontics and titaniumminiplates. Angle Orthod 2006;76:1074-82.
American Journal of Orthodontics and Dentofacial Orthoped
13. Heasman P. Master dentistry: restorative dentistry, paediatricdentistry and orthodontics. 1st ed. Oxford: Churchill Livingstone;2003.
14. Silness J, Loe H. Periodontal disease in pregnancy. II. Correlationbetween oral hygiene and periodontal condition. Acta OdontolScand 1964;22:112-35.
15. Zigler P, Ingervall B. A clinical study of maxillary canine retractionwith a retraction spring and with sliding mechanics. Am J OrthodDentofacial Orthop 1989;95:99-106.
16. Frost HM. The regional acceleratory phenomenon. Orthop ClinNorth Am 1981;12:725-6.
17. Iino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Miyawaki S. Acceler-ation of orthodontic tooth movement by alveolar corticotomy inthe dog. Am J Orthod Dentofacial Orthop 2007;131:448.e1-8.
18. Thiruvenkatachari B, Pavithranand A, Rajasigamani K, Kyung HM.Comparison and measurement of the amount of anchorage loss ofthe molars with and without the use of implant anchorage duringcanine retraction. Am J Orthod Dentofacial Orthop 2006;129:551-4.
19. Owens SE, Buschang PH, Cope JB, Franco PF, Rossouw PE. Exper-imental evaluation of tooth movement in the beagle dog with themini-screw implant for orthodontic anchorage. Am J OrthodDentofacial Orthop 2007;132:639-46.
20. Park HS, Jeong SH, Kwon OW. Factors affecting the clinical successof screw implants used as orthodontic anchorage. Am J OrthodDentofacial Orthop 2006;130:18-25.
21. Schnelle MA, Beck FM, Jaynes RM, Huja SS. A radiographicevaluation of the availability of bone for placement of mini-screws. Angle Orthod 2004;74:832-7.
22. Kuroda S, Sugawara Y, Deguchi T, Kyung HM. Clinical use of mini-screw implants as orthodontic anchorage: success rates and post-operative discomfort. Am J Orthod Dentofacial Orthop 2007;131:9-15.
23. Almeida M, Phillips C, Kula K, Tulloch C. Stability of the palatal ru-gae as landmarks for analysis of dental casts. Angle Orthod 1995;65:43-8.
24. Bailey L, Esmailnejad A, AlmeidaM. Stability of the palatal rugae aslandmarks for analysis of dental casts in extraction and non-extraction cases. Angle Orthod 1996;66:73-8.
25. Christou P, Killiaridis S. Vertical growth-related changes in thepositions of palatal rugae and maxillary incisors. Am J OrthodDentofacial Orthop 2008;133:81-6.
26. Hoggan B, Sadowsky C. The use of palatal rugae for the assessmentof anteroposterior tooth movements. Am J Orthod DentofacialOrthop 2001;119:482-8.
27. Ren A, Lv T, Kang N, Zhao B, Chen Y, Bai D. Rapid orthodontictooth movement aided by alveolar surgery in beagles. Am J OrthodDentofacial Orthop 2007;131:160.e1-10.
28. Thiruvenkatachari B, Ammayappan P, Kandaswamy R. Compari-son of rate of canine retraction with conventional molar anchorageand titanium implant anchorage. Am J Orthod Dentofacial Orthop2008;134:30-5.
29. Anholm JM, Crites DA, Hoff R, Rathbun WE. Corticotomy-facili-tated orthodontics. Calif Dent Assoc J 1986;14:7-11.
30. Yaffe A, Fine N, Binderman I. Regional accelerated phenomenon inthe mandible following mucoperiosteal flap surgery. J Periodontol1994;65:79-83.
ics February 2011 � Vol 139 � Issue 2