micronutrient deficiencies in the arab · pdf filemicronutrient deficiencies in the arab...
TRANSCRIPT
MICRONUTRIENT DEFICIENCIES IN THE ARAB MIDDLE EAST COUNTRIES
(Proceedings of the workshop on Micronutrient Deficiencies in the Arab Middle East, held in Amman, Jordan 27 - 29 June 1995)
Edited by
Abdulrahman Obaid Musaiger Associate Professor of Human Nutrition
Department of Food Sciences and Nutrition Faculty of Agricultural Sciences
UAE.University, AI-Ain.
Samir Salem Miladi Regional Food and Nutrition Officer
FAO/ RNE Cairo, Egypt.
First Edition, 1996
FAa Regional Office of the Near East (RNEA), Cairo, Egypt United Arab Emirates University, AI-Ain, UAE
Arab Nutrition Society, AI-Ain, UAE
c,

©FAO/RNEA 1996 Musaiger,Abdulrahman Obaid Miladi,Samir Salem
. 1. Arab Middle East Countries 2. Micronutrients 3. Iron,lodine and Vitamin A deficiencies
I. Title II. Musaiger,A.O III. Miladi,S.S.
Requests for additional copies of this publication should be sent:
The FAO 1 RNEA P.O. Box: 2223 Cairo - Egypt Fax: 0202 - 3495981
or
Faculty of Agric. Sciences UAE University AI Ain, UAE P.O. Box: 17555 Fax: 009713 - 632384
or
Arab Nutrition Society P.O. Box : 18062 AI Ain, UAE Fax: 009713 - 511390
M1/1 049E 11/6.96/1000 ISBN 92·855 ·1042·6
Printed with financial support from Nestle
MICRONUTRIENT DEFICIENCIES IN THE ARAB MIDDLE EAST COUNTRIES
Edited by
Abdulrahman O. Musaiger and
Samir S. Miladi

The descriptions employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
M 1/1 049E/1/6.96/1 000 ISBN 92-855-1042-6
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying or otherwise, without the prior permission of the copyright owner. Applications for such permission, with a statement of the purpose and extent of reproduction, should be addressed to the Director, PublicatioQs Division, Food and Agriculture Organization of the United Nations, Via Ie delle Terme di Caracalla, 00100 Rome, Italy.
©FA01996
FOREWORD
Nutritional well-being is a prerequisite for the achievement of the full social, mental and physical potential of the population, so that all people can lead fully productive lives and contribute to the development of their community and the nation. Good nutritional status is dependent upon each person having adequate intake of micronutrients in addition having access to safe drinking water.
During the last three decades, the nutritional status of the population of the Arab Countries have improved, However micronutrient deficiencies have been long standing public health problems, which is widespread among both rich and poor Arab countries and among rural and urban population. The prevalence of a particular deficiency can vary considerably between different geographic locations and socioeconomic groups.
Deficiencies of iron, iodine and vitamin A are especially important because of their serious health consequences, wide geographic distribution, and their implication on economic stagnation.
The main causes of micronutrient malnutrition are inadequate intake of foods containing these micronutrients and their impaired utilization. This is often associated with infections that can reduce their absorption and increase their metabolic consumption. Micronutrient deficiencies have negative impact on the society, they reduce working capacity, cause mental and growth retardation, reduce resistance to disease and can lead to death of women in pregnancy and childbirth.
The International Conference on Nutrition recommendations call upon countries to formulate .and implement programmes to correct micronutrient deficiencies and to prevent their occurrence, through sustainable food-based approaches that encourage dietary diversification, the production and consumption of micronutrient rich foods, the supplementation, food fortification and nutrition education.
In order to increase awareness about the magnitude and extent of this problem and to suggest ways and means to prevent and control this situation, the F AO Regional Office for the Near East is pleased to put this publication at the disposal of its member countries, with the hope it would benefit to all those who are working and interested in this field. This publication is the fruit of cooperation with The United Arab Emirates University, The Arab Nutrition Society private food companies.
ADGlRegional Representative for the Near East
FOREWORD
Micronutrient deficiencies are worldwide problems. Studies in the Arab countries indicate that these deficiencies are widely prevalent, although, their prevalence varies innumerously from country to country, and from disease to disease. The major micronutrient deficiencies reported in this part of the world are iron deficiency anaemia, iodine deficiency disorders, and vitamin A and D deficiencies.
Iron deficiency anaemia is a common nutritional problem'in all Arab countries. Its prevalence ranges from 10% to 80% depending on age, sex and physiological status of the population. Iodine deficiency disorders are reported in many remote and mountain areas in this region. Studies on vitamin D deficiency are scarce. However, several studies from Saudi Arabia showed that even with the abundant sunlight in the country, the prevalence of vitamin D deficiency is relatively high. Indicators from some Arab countries, especially Sudan and Egypt showed that vitamin A deficiency is a problem of concern.
Information on micronutrient deficiencies in the Arab countries are limited. This is the first publication which deals with the prevalence and control of micronutrient deficiencies in these countries. The w<?rk was done in cooperation with FAOIRNEN Cairo, Arab Nutrition Society and Nestle Company.
We hope that this work will be valuable to those interested in micronutrient deficiencies in this part of the world.
Nuhad J.Daghir, Ph.D.
Dean, Faculty of Agricultural ~ciences
CONTENTS
Page
Preface ..
Recommendations .. 2
Micronutrient deficiencies in Arab Countries 5 S.Miladi
Iron deficiency anaemia in women and children in Arabian Gulf Countries.. 11 A. Musaiger
Iron deficiency, causes and prevention.. 16 R. Hurrell
The Role of food fortification in combating micronutrient deficiencies .. 22 K. Nagy
Sodium Iron EDTA as a food fortificanL 35 R. Hurrell
Micronutrient deficiencies in Egypt .. 40 F. EI-Sahn
Prevalence of iron deficiency anaemia in Jordan .. 52 A. Faquih et al
Mapping Saudi Arabia for iodine deficiency . 56 A. AI-Nuaim et al
Micronutrient status in Saudi Arabia. 60 K. Madani & R. Kashoggi
Micronutrient deficiencies in Sudan ...... 67 A. Khattab
Availability of micronutrients in Arab diet, example from Jordan. 73 S. Tukan -
Vitamin A in nutrition and its interaction with other nutrients ... 88 H. Takruri

PREFACE
Micronutrient deficiencies are amongst the most nutritional problems worldwide. The common micronutrient deficiencies of public health significant are iron deficiency anaemia,iodine deficiency disorders and vitamin A deficiency. According to WHO about 149 millions are at risk and affected by iron deficiency anaemia in Eastern Mediterranean region. The corresponding figures for iodine deficiency disorders and vitamin A deficiency are 45 and 14 millions,respectively.
Studies on factors associated with these problems in the Arab Middle East countries are few and limited. In addition, the lack of training of health workers and lack of comprehensive prograrnme to prevent and control of micronutrient deficiencies in these countries made the situation more complicated.
The Arab Nutrition Society in cOllobration with Food and Agriculture Orginization,Regional Office in Cairo and Nestle Company organized this workshop to achieve the following objectives:
1. To asses the current situation of micronutrient deficiencies in the Arab Middle East countries.
2. To review ongoing activities and programmes to combat these problems.
3. To recommend measures to overcome these problems.
We hope that the papers presented in this workshop and measures suggested to overcome micronutrient deficiencies in the Arab Middle East countries are useful for those intrested in these problems.
Abdulrahman O. Musaiger Principal Coordinator, Arab Nutrition Society

RECOMMENDATIONS FOR PREVENTION AND CONTROL OF MICRONUTRIENT DEFICIENCIES
IN THE ARAB COUNTRIES OF THE MIDDLE EAST
MicrQnutrient deficiencies is the term that usually referred to deficiency of vitamins and minerals of public health significant.The main micronutrient deficiencies in the Arab Middle East countries are iron deficiency anaemia, iodine and zinc deficiencies and vitamins A and D deficiencies.
Magnitude and causes of the problems
a. Iron deficiency anaemia: This deficiency is the main nutritional problem in all Arab Middle East countries. It is estimated that about 30%-70% of pregnant women in the region suffered from iron deficiency anaemia. The prevalence ranged from 10% to 50% among pre-school children, and from 20% to 70% among school children. Main causes of this problem are poor dietary intake of iron, low iron absorption, parasitic infection, malaria, vitamin A deficiency, multiparity and early age of m<l.rriage.
b. Iodine deficiency disorders: The prevalence of these disorders is less compared to iron deficiency anaemia. However, the problem is of public health significant in some countries and in mountain areas and Oasis in other cQuntries. The prevalence ranged from 6% to 80% .The main countries reported these disorders are Egypt, Iraq, Jordan, Lebanon, Sudan, Syria, Algeria and Tunisia. Iodine deficiency disorders were also reported in some mountain areas in Saudi Arabia and United Arab Emirates, but these disorders are not common health problems. Low iodine in soil and in most foods commonly consumed are the main causes of iodine deficiency disorders in this region.
c. Zinc deficiency: Data on zinc deficiency in the Arab countries of Middle East are scarce. However, studies on dietary habits of preschool and school children revealed low dietary intake of zinc. It is highly believed that zinc deficiency has an important role in growth retardation of children and adolescents in this part of the world. Low intake of food rich in zinc is the main cause of zinc deficiency, especially among young and school children.
d. Vitamin A deficiency: Few studies were carried out on vitamin A deficiency in this region. Reports from Egypt, Jordan and Sudan show that this problem is exist. Unsound food habits, low intake of foods rich in vitamin A and infection (such as measles) are the main causes of vitamin A deficiency in these countries.
e. Vitamin D deficiency: Despite abundant sunlight in this part of the world, vitamin D deficiency was found to be a public health problem in some countries. Several studies in Saudi Arabia indicate low blood levels of vitamin D in children and adults. Factors responsible for prevalence of vitamin D deficiency are low exposure to sunlight, wrapping of infants for long time, low dietary intake of vitamin ci and unavailability of other nutrients especially calcium.
Actions needed
1. Assessment: In spite of scarity of data on magnitude and factors associated with micronutrient deficiencies, it is highly recommended that each country should start carrying out a national survey to identify these problems. Target group should be clearly defined for each deficiency. Priority must be given to iron deficiency anaemia surveys, with emphasis to use two of the following parameters:Haemoglobin, PCV, serum ferritin, protoporphyrin and blood film.
2
2. Dietary Intervention: Dietary modification is an important approach to reduce the prevalence of micronutrient deficiencies in the communities. Encouragement and support intake of food rich in micronutrientssuch as green leafy vegetables, yellow fruits and vegetables should be done through various mass media and school feeding programmes. Consumption of gOitrogenic foods should be reduced as possible. It is highly recommended that these countries should establish dietary guideline for healthy eating taking into consideration consumption of foods that are rich in micronutrients, and reducing intake of that contain constituents inhibit or interfere with absorption of the micronutrients especially iron, zinc, and calcium.
3. Fortification of Staple Foods: Food fortification is an important method to overcome micronutrient deficiencies. Fortification of salt with iodine and iron has proved in many countries to be one of successful method to control iodine deficiency disorders and iron deficiency anameia.Fortification of sugar with vitamin A has also given an encouraging results. However, it is very essential to study carefully the main food vehichle for fortification in each country. Wheat flours and rice are the main staple foods in the Arab countries of the Middle East.Fortification of these foods, especially wheat flour, with several micronutrients is a major intermediate startegy to control micronutrient deficiencies. Emphasis should also be put on the infant formula, weaning foods and other processed foods which are widely consumed by children. Most of imported whole powdered milk in the region is fortified with Vitamin A and D. This should be extended to other imported dairy products such as butter, margarine and yoghurt.
4. Nutrition Education: One of the main causes of micronutrient deficiencies in this region is the lack of nutrition information on sound dietary habit to prevent these deficiencies. Nutrition education and communication are an important supporting strategy to prevent any nutrient deficiency. Information on causes, consequences and measures to prevent and control these problems should be dessiminated through various mass media. Nutrition education material should be pretested and evaluted. Involvement of target groups in these process is highly recommened.
5. Public Health Measures: Several public health measures should be carried out by health and other related authorities in the region. These measures can be summarized as follows:
a. Supplementation with micronutrients.This can be done through maternal and child health centers and through schools or other local systems. Supplementation of iodized oil for iodine deficiency disorders, capsules (oil) in massive or small dose for vitamin A deficiency and iron folate tablets for iron deficiency anaemia are now carried out in many countries in the region suffered from these micronutrients.
b. Prevention and control of infections through environmental health programmes such as water sa~itation,. immunization, MCH services, control of endemic diseases, oral rehydration theraphy, antiparasitic measures and food hygiene.
c. Food legislation is another public health approach which should be enforced. Legislation regarding food additives, fortification and labelling are essential strategy to prevent these problems. Many countries in the region lack such legislation.
d. Training of health and community workers on management of micronutrient defiCiencies.
e. ,Nutrition surveillance,.system should be established in health sector to provide essential indicators on micronutrient deficiencies.
6. Role of Private Sector: Private sector can play an important role in preventing and control of micronutrient de'ficiencies in the region. Private sector can provide assisstance in equipement, training of staff, laboratory facilities, conducting seminars and studies.
3
7. Role of International Organizations: International Organizations particularly FAO, WHO and UNICEF should provide the following support:
a. Conducting training courses in assessment, planning, implementation and evaluation of programmes related to prevent and control of micronutrient deficiencies.
b. Providing technical assistance in several aspects related to micronutrient deficiencies.
c. Strengthening the national programmes for preventing and control. of micronutrient deficiencies.
d. Supporting research projects to study the magnitude and causes of these problems.
e. Supporting co-operation and co-ordination among countries in the region to overcome micornutrient deficiencis.
4
MICRONUTRIENT DEFICIENCIES IN THE ARAB COUNTRIES
Samir S. Miladi
Food and Agriculture Organization Regional Office, Cairo, Egypt
INTRODUCTION
Micronutrient deficiencies have been long standing public health problems in the Arab Region. It is estimated that over 100 million people in the Arab region are suffering from one or more of micronutrient deficiencies. These nutritional problems are widespread among both rich and poor Arab countries and among the rural and urban population. However, the prevalence of a particular deficiency can vary considerably between differnt geographic locations and socio-economic groups. Most of surveys previously conducted have been of a medical nature and have not been accompanied either by quantitative or qualitative food consumption patterns.
ANAEMIA
Anaemia, especially due to iron deficiency is the most common micronutrient deficiency in the Arab Region, especially among young children and women of reproductive age. Anaemia lead to learning disabilities, an increased risk of infection, diminished work capacity and to death of women during pregnancy and at child birth. Maternal anaemia also contributes to interuterine growth retardation and low birth weight.
The causes of anaemia in the Arab Region are due to low dietary iron intake, poor iron absorption due to dietary constituents such as phytates and iron loss associated with parasitic infections especially in Egypt, Sudan and Iraq. The endemicity of malaria in countries such as Sudan, Somalia and Mauritania is another significant contributory factor.
Data from certain Arab countries have indicated that the phytic (iron-binding) content of wheat which is grown locally is higher than that of imported wheat. It should be also noted that the high consumption of tea (intake of tea in Egypt is more than England) with its binding capacity reduce iron absorption, which is another factor very common through the Arab Countries. ~n Egypt, parasitic infection (Bilharzia and Ankylostoma) are considered important causes of the prevalence of anaemia especially among rural population and among urban low income groups. In most Arab countries anaemia range between 30% to 70% in preschool children and pregnant and lactating women. These findings were reported in several surveys which were carried out in Bahrain, Egypt, Jordan, Sudan, Tunisia, Morocco and Saudi Arabia. It is more prevalent among rural, low income groups and females. A study in Bahrain in 1980 indicated that 34% of pre-school children were anaemic. The' prevalence in rural areas was double that in urban areas in childrran 6-11 years. It was more prevalent among adult females (42.8%) compared to only 21% in males. Later study showed that anaemia decreased with the decrease in the intestinal parastitic infections. A study in Oman indicated that 66% of pre-school children and 38% of school children suffered from anaemia. In Saudi Arabia it was found that 12-50% of the population are suffering from anaemia. In Yemen it
is estimated that 90% of population suffer from anaemia. The rates were 41 % in the West Bank and 67% in the Gaza strip among pregnant women (Osman, 1992).
5

In Egypt, data on anaemia showed that it is most common among child-bearing women, nursing mothers and children between birth and two years of age. Anaemia is more in Upper Egypt than in Lower Egypt. ~Iso 58-73% of school children aged 6-12 years suffered from anaemia. A study in Morocco Indicated that 22% of children (0-2 years) admitted to hospitals had anaemia. It was also prevalent (10-14%) among pregnant women. Similarly the survey in Syria showed that anaemia is wide spread (30%) among women of child bearing age (15-49) years.
Many of the reported studies on anaemia have been carried out on patients admitted to hospital or those vIsiting health centers or school children. Surveys should be carried on children who are not enrolled in schools and on populations who are not visiting health centers.
Actions Needed
The intervention required for the prevention and treatment of anaemia is relatively inexpensive. Iron supplementation for vulnerable groups is essential especially in pregnant and lactating women. Other groups that deserve high priority include premature and low birth-weight infants. For older preschool children and school children in areas of high anaemia prevalence, screening for anaemia and supplementation should be conSidered. Fortification with iron could be undertaken with a variety of food vehicles such as processed cereals, salt, sugar and infant foods.
Attempts to modify dietary intake of iron is also important. There are three ways in Which diet can improve iron absorption: by increasing intake of haem iron (primarily meat sources); by increasing Intake of food rich in ascorbic acid (Vitamin C); and by reducing inhibitors of iron absorption such as wheat and tea.
Programmes for combating iron deficiency are usually cost-effective, since the expenditures are later offset by a better economic performance of the population.
IODINE DEFICIENCY DISORDERS (100)
Iodine deficiency is a major risk factor for both the phYSical and mental development of a large number of the population in the Arab Region who live in iodine deficient environment. More than fifteen Arab Countries which were surveyed indicate the prevalence of iodine deficiencies. .Prevalence have been reported in the mountainous areas in Morocco, Algeria, Tunisia Syria,Lebanon, Yemen and in the Oasis in Egypt.
In pregnancy, iodine deficiency causes spontaneous abortions, stillbirths and infant death. It interferes with braih development, and can result in brain-damage babies. In childhood iodine deficiency can cause mental retardation, delayed motor development, growth failure or st'unding, muscular disorders, paralysis, as well as speech and hearing defects. Data from Egypt indicate a prevalence of 38% in the New Valley and 14% in Upper Egypt. It is also common among school children and females. Goiter has been reported to be endemic in Algeria since 1912. An epidemiological survey included 4500 people indicated a preValence of 51.3% and endemic cretinism of 1.1 % In Lebanon, a stUdy in 1961 indicated a prevalence of iodine deficiency of 49%, mainl~ among population living in mountains areas. 100 in Sudan was reported in 1952 mainly in Darfur areas and Western Sudan reaching up to 86% of school Children. It was also found that iodine content in foods and drinking water was low in most endemic gOitre areas and the presence of goitrogenic substance in millet whiCh constitute the staple cereal in Western Sudan. In Syria, surveys showed the prevalence of 100 among school children(6 - 14 years) were 73%. The rate was higher in high rainfall areas compared to low rainfall areas.
6
Actions needed
The major control methods for IDD are fortification of salt with iodine compounds, and distribution of iodized oil. The cost of iodized salt is about $0.05 per person per year. A possible approach to consider is the supplementation of the diet of domestic animals with iodine, so that livestock products (e.g. milk, meat) contain the necessary nutrient. Another approach would be agricultural research which selects varieties of low goitrogenic grains such as sorghum and millet which contitute the staple of the diet in the rural areas in Sudan and Somalia.
VITAMIN A DEFICIENCY
The extent of vitamin A deficiency in the Arab countries is not clear, though a number of countries such as Djibouti, Sudan and Mauritania, have reported that vitamin A deficiency may be a significant public health problem. A recent study in Iraq indicates that vitamin A deficiency was prevalent as acute and chronic nutritional problems. Vitamin A deficiency, and its sad consequence of blindness, poor growth, increased severity of infections and death is a public health problem especially among the low income groups in some Arab countries. The intake of food which are poor in Vitamin A, or its precursors (Beta- carotene) coupled with increased requirement due to infection particularly measles, lead many children to xerophthalmia and blindness, particularly when the child is suffering from protein energy malnutrition. A survey in Sudan indicated that 14.8% of boys and 11.9% of girls showed signs of xerosis of the eye, while 2.3% of boys and 1.3% of girls showed Bitot's spots and xerosis.
In Egypt, the prevalence was reported among preschool children who are suffering from PEM (22%). In Saudi Arabia, isolated cases of vitamin A deficiency were observed in certain regions. The surveys conducted in Yemen indicated the prevalence of vitamin A deficiencies especially among school children. A study in Jordan on vitamin A deficiency in infant and young children revealed that 1.3% of children under six years of age suffered from night blindness and 0.6% suffered from Bitot's spots.
Actions needed
Vitamin A deficiency may be successfully attacked by relatively simple interventions. Short-term measures to prevent vitamin A deficiency among high-risk groups must be implemented because of the severe consequences of this deficiency. The fortification of commonly consumed f09ds, coupled with targeted distribution of high dose capsules every three to six months, may present the best interim measures. The cost of fortification is estimated to be around $0.5 per person per year. Sugar has been used as the vehicle in central America. Dried Skin milk (DSM) is commonly fortified with vitamin A and D. In Tunisia, reconstituted DSM was fortified with vitamins A and D. This milk was sold at a subsidized price. Unfortunately, this programme Is presently abolished. There is greater coverage through fortification programmes which, however, require some investment and legislation. Health Services can be used for delivering vitamin A supplements, through immunization programmes. It has been estimated that the cost of the high dose of vitamin A supplement is around $0.04 per recipient per year. The long term solution lies in increasing the availability and consumption of vitamin A or Carotene-rich foods, including dark greek leafy vegetables, and deep yellow fruits and vegetables. Agricultural planners and extension field workers must be "aware of the extent and the severity of vital1lin A deficiency among the population, and how the agriculture sector can best address the problems. Nutrition education and social marketing techniques can be employed to improve dietary intakes of good sources of vitamin A.
7

VITAMIN D DEFICIENCY
Vitamin D deficiency has been reported in some countries. Studies in Yemen indicated that rickets is a major public health problem and Osteomalacia was observed in adult women. In a study in Northern Yemen, it was found that the prevalence of rickets among children under five years of age was 27%. Rickets were common at the end of the first year and had disappeared by the fifth year. In some Arab countries such as Saudi Arabia vitamin D deficiency was observed and was associated with wrapping infants for long periods, dietary factors and limited exposure to sunlight. Surveys in Morocco indicate vitamin D deficiency of 22% in children under four year of age. There has been a systematic preventive programme initiated by the Ministry of Health whiCh may reduce the incidence of rickets.
Actions needed
This particular deficiency is mainly associated with the cultural habits of wrapping the infants for long periods. The actions needed are: education of mothers not to wrap infants for long periods,fortification programme when required and promotion of consumption of food rich in vitamin D.
OTHER MICRONUTRIENT DEFICIENCES
Very limited studies and surveys were carried. in the Arab countries on other micronutrient deficiencies such as zinc. In the later country it was found that 29% of adult population had zinc deficiency. However, this deficiency require further investigation in several countries. Vitamin C deficiency (Scurvey) has been reported among displaced populations in Sudan and Somalia. The food rations which have low in vitamin C and the new environment where wild plants are absent, have lead to the appearance of vitamin C deficiency (Scurvey).
CONCLUSION
The number of people affected by micronutrient deficiences in the Arab Region is large. The consequences of these deficiencies on human health and productivities are serious. The elimination and the control of micronutrient deficiencies in the Arab Countries require the establishment of a system for linking policy action to human need. Micronutrient deficiencies would not be solved by the Ministry of Health alone but require an integrated approach and the involvement of other Ministries such as Agriculture,Supply, Industry, Education and Information as well as the Private sector and NGOS. The World Declaration and Plan of Action on Nutrition which were adopted by the International Conference on Nutrition (ICN) and nutritional goals for children adopted by the World Summit for Children give guidelines of action needed by the international, national and local communities for the monitoring, control and the elimination of these serious defficiencies which impair human development and nutritional well-being. .
8
Table 1 Micronutrient Deficiencies in the Arab Countries
Country Anaemia
Algeria 19 - 42% C
Bahrain 21 -42% a,b
Djibouti * ale
Egypt 20 - 70% b,c,d
Iraq *d
Jordan 34% a
Lebanon *b
Morocco 10 - 40% a,b,c
Oman 38 -66% a,b
Saudi Arabia 21 -50% a,b
Sudan 36% b,c
Syria 30%c
Tunisia 50% b,c
U.A.E. 28 - 43% a,b,c
West Bank/Gaza 25-50% a,c
Yemen NA
a. pre-school children b. school children c.Women of child bearing age d.whole population. • Common health problem. NA : No available data.
Goiter
23 - 71% b,c,d
NA
NA
12 - 43% b
30-80%d
6-16%d
12-70%
18 - 80%
NA
*b
13 - 86% b,c,d
69 -77% b
15 - 51% b,d
NA
NA
NA
9
AVitaminosis
NA
NA
8-14%c
* b,d
*d
06 -1.3% a,b
NA
NA
NA
NA
3 -4%b,d
NA
NA
NA
NA
NA
REFERENCES
FAO/ESN (1994). Nutrition Country Profiles for Arab Countries, Rome, Italy. FAO/RNEA (1993). Summary of the International Conference on Nutrition (ICN) Country Papers of
selected countries in the Near East Region FAO/RNEA, Cairo, Egypt. FAOIWHO (1992). Final Report of the International Conference on Nutrition - Rorne, Italy. Harfouch J.et al (1980).The State of child Health in the Eastern Mediterranean RegionWHOEMRO,
Alexandria, Egypt. M1ladi, S(1992). Food and Nutrition Problerns in the Near East - FAOIWHO Regional Meeting for
the Preparation of the ICN , Cairo, Egypt. Osman, A.K.(1992). A Situation Analysis of Micornutrient Deficiencies in MEMA Countries UNICEF,
Regional Office, Amman, Jordan. Verster, A. (1992). A Regional Nutrition Situation Analysis FAOIWHO Regional meeting for the
preparation of the ION- Cairo April 1992.
10
IRON DEFICIENCY ANAEMIA AMONG CHILDREN AND WOMEN IN THE ARAB COUNTRIES OF THE GULF
INTRODUCTION
Abdulrahman O. Musaiger
Department Food Sciences and Nutrition Faculty of Agricultural Sciences
U. A. E. University, AI Ain, U. A. E.
Despite the significant improvement in economic and health status in the Arab countries of the Gulf, iron deficiency anaemia is the commonest nutritional disorder and affects a high percentage of people, particularly reproductive women and preschool children. This problem, if uncontrolled, leads to anaemia of increasing severity, reduced work capacity, diminished learning ability, increased susceptibility to infection and greater risk of death associated with pregnancy and childbirth (Gilles- pie et al. 1991).
This paper highlights the current pravalence of iron deficiency anaemia in the Arab Countries of the Gulf and discusses factors associated with this problem.
PREVALENCE OF IRON DEFICIENCY ANAEMIA
Pregnant women
Studies in the Gulf countries demonstrated that iron deficency anaemia is one of the main public health problems among pregnant women. Using haemoglobin level less than 11 g/dl the prevalence of anaemia ranged from 30% to 54% in these women (Table 1). The lowest prevalence was reported in Qatar, which is largely due to estimating the anaemia in the first trimester. The reqUirements for iron during the first trimester are relatively small, but rise considerably during the second and third trimester (DeMayer, 1989). A study in Kuwait showed that the prevalence of anaemia was 21 % during the first trimester, increasing to 38% and 45% during the second and third trimester, respectively (Dawood et aI., 1990)
Using other blood parameters, iron deficiency anaemia among pregnant women was also high. In Saudi Arabia, Khoja et (II (1994) reported that 57% of pregnant women were anaemic, using transferrin saturation «16%). When 'serum ferritin «12mg/ml) was determined for the same women, the prevalence of anaemia was very close to that of transferrin saturation (54%).
Adults
Epidemiological studies on iron deficiency anaemia among adults in the Gulf are, at most, scanty. In the United Aral;) Emirates (UAE), Hossain et ai, (1995) found only 16% of non-pregnant women were iron deficient «Hb<12 g/dl). The investigators attributed this low prevalence to the marked increase in the avaiiability and use of antenatal care services in UAE during the last decade. However, this study has several limitations and therefore the results can not be generalised for non pregnant UAE women. The study focused on women who had children 1-22 months and attended immunization centers in one city in UAE (AI Ain).
11
Children and adolescents
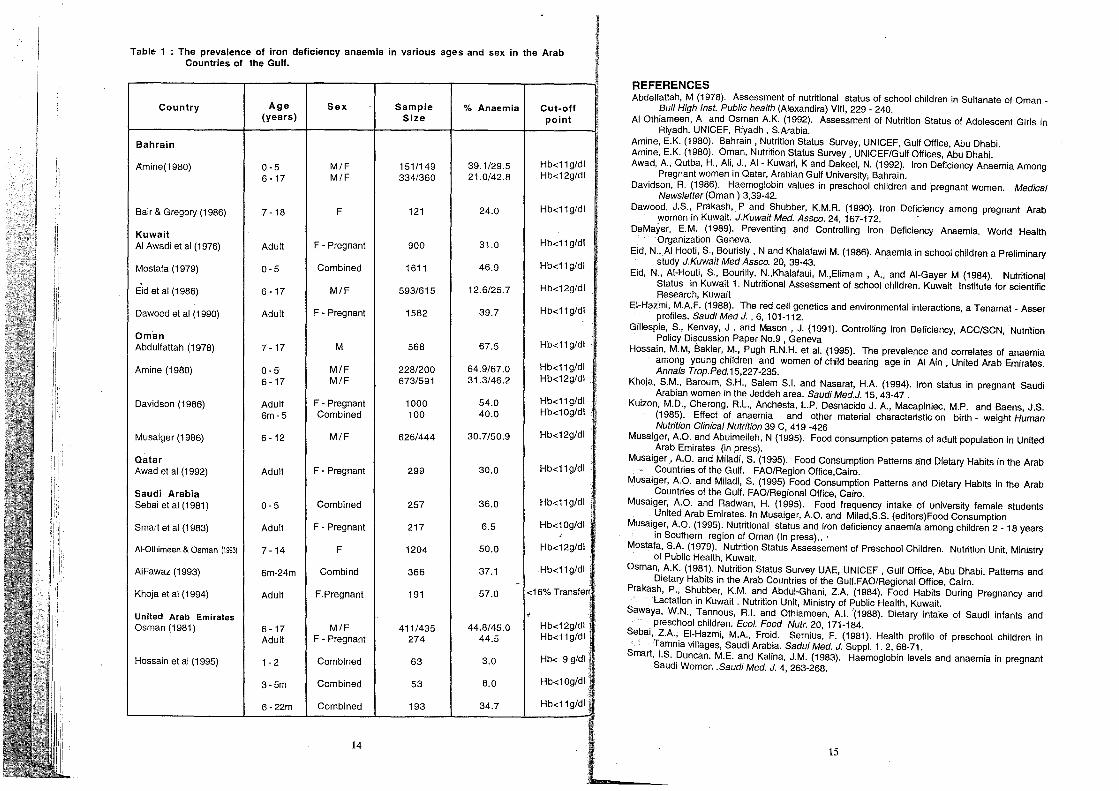
Iron deficiency anaemia is a problem of interest among children in this region; especilly among preschool children and teenage girls. In general, the anaemia is more prevalent among preschool than school age children. From Ta~le 1 we note that the prevalance of anaemia among preschoolers ranged from 29.5% to 67%, while that among school children ranged from 12.6% to 46%.
1n Kuwait a cross-sectional study of 1208 school children aged 6-17 years was carried out to determine the prevalence of iron deficiency anaemia. Data revealed that anaemia was more prevalent among girls (26%) than boys (13%), but it was highly prevalent among younger boys (6-9 years) and adolescent girls compared with other age groups (Eid et al 1986). In Bahrain, Blair and Gregory (1986) demonstrated that 24% of school girls aged 7-18 years had signs of iron deficiency based on transferrin saturation and the anaemia was most prevalent among 15-18 years olds (42%). These findings confirm that teenage girls in the Gulf are among risk groups of anaemia.
FACTORS ASSOCIATED WITH IRON DEFICIENCY ANAEMIA IN GULF
Factors associated with anaemia in this part of the world have not been well investigated. Some factors which are suspected to be responsible for the high prevalence of iron deficiency anaemia in the Arab Countries of the Gulf are briefly discussed.
1. inadequate intake of dietary iron
The intake of food rich in iron was found to be low in the Gulf, particularly by infants, preschoolers and pregnant women. In Saudi Arabia; Sawaya et al (1988) showed that the iron intake of children aged 0-6 years did not exceed 38% of FAOIWHO Recommended Dietary Allowances (RDA). In Kuwait, the intake of iron among school children was also found to be less than the RDA (Eid et al 1984). Another study in Kuwait (Prakash et ai, 1984) demonstrated that the intake of calcium, iron and vitamin C by pregnant women was below 75% of US RDA, while among lactating women, all nutrients (except protein) were below the RDA.
2. Inadequate intake of food enhance iron absorption
Studies, both among children and adults, suggested that foods rich in vitamin C, which enhance iron aborption are poorly consumed in this region. Vitamin C is mostly found in some fresh fruits and vegetables. The daily consumption of fresh fruits and vegetables by university girls aged 18-20 years in UAE was 41% and 59%, respectively (Musaiger and Radwan, 1995). Among adults, only 46% of men and 52% of women aged 20-60 years reported daily consumption of fresh fruits. The corresponding percentages for fresh vegetables were 60% and 65%, respectively (Musaiger and Aburmeileh, 1995).
Among school children and adolescents the situation is worse, as many of them not only consumed fewer fresh fruits and vegetables, but also consumed less meat and fish, which are also enhancers of iron absorption.
3. High intake of foods contained compounds inhibit iron absorption
Many compounds are known to inhibit the absorption of iron, among them; polyphenols (including tannins) which are present in tea and to a lesser extent in coffee; and phytates which are present in wheat and other cereals (DeMayer, 1989). Several studies (Musaiger and Miladi, 1995) demonstrated that the preschool children, adolescents and adults in the Arab countries of the Gulf consumed tea in a high quantity, especially after the heavy midday meal, the lunch. A single
12
cup of tea taken during a meal may cause iron absorption to drop from 11 % to 2%. It would thereforeseem to be essential that health education should focus on reducing the intake of tea, particularly with meal. However, the inhibitory effect of tannins in tea can be counteracted by adding vitamin C to the meal.
4. Infection, especially intestinal parasitic infection
Infections interfer with food intake and the absorption, storage and use of many nutrients (including iron). In some rural areas in Arab countries of the Gulf where the environmental sanitation is poor, morbidity from viral and bact rial infection is high. The repeated episodes of infection may result in the development of anaemia particularly in young children.
Intrestinal parasites were prevalent among young and school children in the Gulf. Sebai et al (1981) showed that 35% of Saudi preschool children had intestional parasitic infection, but no schistosoma eggs were observed. Musaiger and Gregory (1990) found that intestinal paraSites were prevalent among children 6-11 years (14%) although hookworms were not detected. In Saudi Arabia, EI-Hazmi (1985) showed that the incidence of anaemia was significantly higher in parasite - infected individuals (21%) than in parasite-free ones (8%), indicating that paraSitic infections may be one of the causes of anaemia in the region.
5. Other factors
Statistics showed that the fertility ratEl of Gulf women ;s relatively high (4.6 - 7.1 per 1000 women). Multiple deliveries tend to lower the haemoglobin level in women because closely spaced pregnancies deplete the iron stores of the women, especially when there is no iron supplementation during pregnancy (Kuitan et ai, 1985) . In UAE, Hossain et al (1995) found that the prevalence of anaemia was significantly higher in women who had had seven or more pregnanceis then in those who had had 1-3 pregnancies (Odds Ratio = 4.17, 95% CI=1.86 -9.38). Also women whose menstrual periods usually lasted more than 6 days were significantly more likely to be anaemic than were counterparts whose periods usually lasted less than 5 days (Odds Ratio = 4.00, 95% CI=1.17 - 13.67).
There are certain beliefs and attitudes that are negatively associated with the anaemia in the Gulf. Among them is the widely spread belief that iron supplements, which are given to pregnant women, can cause enlargement of fetus or abortion to the women. Consequently, some women do not take these iron supplements.
Malaria which is prevalent in some parts of the Gulf is also another contributing factor. The diagnosis of iron deficiency anaemia in the Gulf becomes more complicated with the high incidence of inherited anaemia such as sickle cell trait and thalassaemia minor (EI-Hazmi, 1985).
CONCLUSION
Iron deficiency anaemia is a serious public health problem in the Arab countries of the Gulf. However epidemiological studies on the prevalence of anaemia in various age groups in the Gulf communities as well as factors associated with anaemia are scarce. Such studies should be given a high priorities in any health research programmes. At the same time measures to prevent and
It control this nutritional disorder should be included in health and nutrition programmes. Iron tablets supplementation for pregnant women, blood screening for women and children, prevention and treatment of intestinal paraSitic infections, iron fortification of some common foods, and dietary modification are among the measures that must be taken into consideration in preventive programmes.
13
.
Table 1 . : The prevalence of iron deficiency anaemia in various ages and sex in the Arab Countries of the Gulf.
Country Age Sex Sample % Anaemia Cut-off (years) Size point
Bahrain
M/F 151/149 39.1/29.5 Hb<11g/dl ~mine(1980) 0-5 6 -17 M/F 334/360 21.0/42.8 Hb<12g/dl
Bair & Gregory (1986) 7 -18 F 121 24.0 Hb<11 g/dl
Kuwait AI Awadi et al (1976) Adult F - Pregnant 900 31.0 Hb<11g/dl
Mostafa (1979) 0-5 Combined 1611 46.9 Hb<11 g/dl
Eid et al (1986) 6 -17 M/F 593/615 12.6/25.7 Hb<12g/dl
Dawood et al (1990) Adult F - Pregnant 1582 39.7 Hb<11g/dl
Oman Abdulfattah (1978) 7 -17 M 568 67.5 Hb<11 g/dl
Amine (1980) 0-5 M/F 228/200 64.9/67.0 Hb<11g/dl
6-17 M/F 673/591 31.3/46.2 Hb<12g/dl
Davidson (1986) Adult F - Pregnant 1000 54.0 Hb<11g/dl
6m-5 Combined 100 40.0 Hb<10g/dl
Musaiger (1986) 6 -12 M/F 626/444 30.7/50.9 Hb<12g/dl
Qatar Hb<11g/dl i Awad et al (1992) Adult F - Pregnant 299 30.0
Saudi Arabia Sebai et al (1981) 0-5 Combined 257 36.0 Hb<11g/dl
Smart et al (1983) Adult F - Pregnant 217 6.5 Hb<10g/dl , F 1204 50.0 Hb<12g/dl I AI-Othimeen & Osman (1993) 7 -14
I Combind 366 37.1 .Hb<11g/dl I. AIFawaz (1993) 6m-24m
-Khoja et al (1994) Adult F.Pregnant 191 57.0 <16% Transferr,
United Arab Emirates i Hb<12g/dl Osman (1981) 6-17 M/F 411/435 44.8/45.0
Adult F - Pregnant 274 44.5 Hb<11g/dl
Hossain et al (1995) 1 - 2 Combined 63 3.0 Hb< 9 g/dl
3-5m Combined 53 8.0 Hb<10g/dl
6-22m Combined 193 34.7 Hb<11g/dl
14
REFER ENCES Abdelfatta h, M (1978). Assessment of nutritional status of school children in Sultanate of Oman _
High Inst. Public health (Alexandira) VIII, 229 - 240. Bull AIOthiam een, A and Osman A.K. (1992). Assessment of Nutrition Status of Adolescent Girls in
adh. UNICEF, Riyadh, S.Arabia. Riy Amine, E. K. (1980). Bahrain, Nutrition Status Survey, UNICEF, Gulf Office, Abu Dhabi.
K. (1980). Oman, Nutrition Status Survey, UNICEF/Gulf Offices, Abu Dhabi. Amine, E. Awad, A, Qutba, H., Ali, J., AI- Kuwari, K and Dakeel, N. (1992). Iron Deficiency Anaemia Among
gnant women in Qatar, Arabian Gulf University, Bahrain. Pre Davidson, R. (1966). Haemoglobin values in preschool children and pregnant women. Medical
wsletter (Oman) 3,39-42. Ne Dawood,
wo J.S., Prakash, P and Shubber, K.M.R. (1990). Iron Deficiency among pregnant Arab
men in Kuwait. J.Kuwait Med. Assco. 24, 167-172. De Mayer, E.M. (1989). Preventing and Controlling Iron Deficiency Anaemia. World Health
anization Geneva. Org Eid, N.,AI Hooti, S., Bourisly, Nand Khalafawi M. (1986). Anaemia in school children a Preliminary
y J.Kuwait Med Assco. 20, 39-43. stud Eid, N., AI -Houti, S., Bourilly, N.,Khalafaui, M.,Elimam , A, and AI-Gayer M (1984). Nutritional
us in Kuwait 1. Nutritional Assessment of school children. Kuwait Institute for scientific earch, Kuwait
Stat Res
EI-Hazini, M.A.F. (1988). The red cell genetics and environmental interactions, a Tenamat - Asser les. SaudiMed J. , 6, 101-112. profi
Gillespie, Poli
S., Kenvay, J . and Mason, J. (1991). Controlling Iron Deficiency, ACC/SCN, Nutrition cy Discussion Paper No.9, Geneva
Hossain, amo
M.M, Bakier, M., Pugh R.N.H. et al. (1995). The prevalence and correlates of anaemia ng young children and women of child bearing age in AI Ain , United Arab Emirates. als Trop.Ped.15,227-235. Ann
Khoja, S. M., Baroum, S.H., Salem S.1. and Nasarat, H.A. (1994). Iron status in pregnant Saudi bian women in the Jeddeh area. Saudi Med.J. 15, 43-47 . Ara
Kuizon, M. D., Cherong, R.L., Anchesta, L.P. Desnacido J. A, Macapinlec, M.P. and Baens, J.S. 5). Effect of anaemia and other material characteristic on birth - weight Human
rition Clinical Nutrition 39 C, 4.19 -426 (198 Nut
Musaiger, Ara
A.a. and Abuimeileh, N (1995). Food consumption paterns of adult population in United b Emirates (in press).
Musaiger, AO. and Miladi, S. (1995). Food Consumption Patterns a:nd Dietary Habits in the Arab ntries of the Gulf. FAa/Region Office,Cairo. Cou
Musaiger, Cou
A.a. and Miladi, S. (1995) Food Consumption Patterns and Dietary Habits in the Arab ntries of the Gulf. FAa/Regional Office, Cairo.
Musaiger, A.a. and Radwan, H. (1995). Food frequency intake of university female students ed Arab Emirates. In Musaiger, A.a. and Milad,S.S. (editors)Food Consumption Unit
Musaiger, AO. (1995). Nutritional status and iron deficiency anaernia among children 2 - 18 years outhern region of Oman (In press) ... in S
Mostafa, S .A. (1979). Nutrition Status Assessement of Preschool Children. Nutrition Unit, Ministry ublic Health, Kuwait. of P
Osman, A. K. (1981). Nutrition Status Survey UAE, UNICEF, Gulf Office, Abu Dhabi. Patterns and ary Habits in the Arab Countries of the Gulf.FAO/Regional Office, Cairo. Diet
Prakash, P., Shubber, K.M. and Abdul-Ghani, Z.A. (1984). Food Habits During Pregnancy and ation in Kuwait. Nutrition Unit, Ministry of Public Health, Kuwait. Lact
Sawaya, W.N., Tannous, R.1. and Othiameen, A.1. '(1988). Dietary intake of Saudi infants and chool children. Ecol. Food Nutr. 20,171-184. pres
Sebai, Z. A., EI-Hazmi, M.A., Froid. Sernius, F. (1981). Health profile of preschool children in mnia villages, Saudi Arabia. Sadui Med. J. Suppl. 1. 2, 68-71. Ta
Smart,I.S . Duncan. M.E. and Kalina, J.M. (1983). Haemoglobin levels and anaemia in pregnant di Women . Saudi Med. J. 4, 263-268. Sau
15

IRON DEFICIENCY CAUSES AND PREVENTION
Richard F. Hurrell
Laboratory for Human Nutrition Swiss Federal Institute of Technology ,Zurich,Switzerland
INTRODUCTION
Of the 87 elements in the earth's crust, iron is number four at 56g/kg (5.6%), only oxygen (464g/kg) (amost 50%), silicon (284g/kg) and aluminium (83g/kg) occur in greater quantities. There is more Fe than Ca, Na or Mg, 1,000 times more than zinc and 100'000 times more than iodine which occurs at 0.5mg/kg. In spite of this, however, 1.3 billion people, that's 24% of the world population, are iron deficient, and iron is the micronutrient with the highest magnitude of deficiency wcrld-wide. In comparison, 217 millon people are iodine deficient (4% of the world population) and 43 millon children under 5 are vitamin A deficient, 7% of the world's children under 5.
The prevalence of anaemia varies in different geographical regions of the world (Table 1) (DeMaeyer and Adiels-Tegman, 1985), being highest in infants (from birth to 4 years), children from 5-12 years and women of child-bearing age (15-49). In South Asia and Africa were some 50% of these population groups are anaemic compared to about 25% in countries of Latin America and 10% in industrialised countries in the West. World-wide, 43% of children from birth to 4 years, 37% of children 5-12 and 35% adult women are anaemic.
Table 1 Prevalence of anaemia in different geographical regions
Estimated percentage of anaemia
Infants Children Women 0-4 years 5-12 years 15-49 years
South Asia 56 50 58 Africa 56 49 44 Latin America 26 26 17 Industrialised Countries 12 7 11 World 43 37 35 ,
FUNCTIONS OF IRON IN THE BODY
In the human body of 75kg, we find 4.8g Fe (Bothwell et a!. 1979). All of it is bound to proteins as under normal circumstances there is no free iron in the body. The~reatest part of the Fe (68%) is found in the haem molecule either as myoglobin in the muscle or haemoglobin in the blood with the function of oxygen transport. A further 5% is as enzymes, haem or non-haem, for electron transfer or oxidation reduction reactions, such as during energy metabolism with cytochromes or in the Krebs cycle, or in the immune system with neutrophiles or lymphocytes. The rest, normally around 27%, is stored as ferritin or as hemosiderin especially in the liver.
16
CONSEQUENCES OF IRON DEFICIENCY
The major consequences of iron deficiency are four-fold: less strength, decreased immune function, increased mortality and morbidity during pregnancy and birth and, probably most importantly reduced psychomotor and mental development in the child (Hercberget a!. 1987). Iron deficient people have less strength because oxygen transport (haemoglobin) and energy metabolism (iron enzymes) are reduced, and work capacity is then decreased which might have increased mortality and morbidity during pregnancy and birth and, probably most importantly reduced psychomotor and mental development in the child (Hercberget a!. 1987). Iron deficient people have less strength because oxygen transport (haemoglobin) and energy metabolism (iron enzymes) are reduced, and work capacity is then decreased which might have serious economic consequences in some Third World Countries (Basta et a!. 1979). Secondly, there is decreased immune function with a possible increase in infection. In addition, there is increased mortality and morbidity during pregnancy and birth; 100'000 pregnant women die each year due to severe anaemia and there are increased numbers of premature infants with all the problems which follow. Finally, iron is essential during the formation of the brain until the age of about 24 months and, if there is not enough iron, there can be reduced psychomotor and mental development in the child. Perhaps more importantly, even if iron is given, the changes appear to be irreversible (Lozoff et a!. 1991).
AETIOLOGY OF IRON DEFICIENCY
The question is: Why there so much Fe deficiency when there is so much iron around? The most probable answer is because of poor iron absorption. Firstly iron oxide in the soil is non-absorbable in addition, iron from plants is poorly absorbed because of absorption inhibitors, and although iron from meat is well-absorbed it is often little consumed (especially in the Third World). Finally, a fact which we often forget, iron absorption is naturally restricted because any free Fe in the body can generate free radicals which can lead to severe health problems.
However, low iron absorption is not the only cause of iron deficiency anaemia (Hercberg et aI.1987). It may be aggravated by intestinal parasites such as hookworm which can cause a steady blood loss (Mahmoud 1966); by malaria where the protozoa ·destroys the red blood cells (Brabin1992); by a low vitamin A status which prevents erythropoesis (Suharno et aI.1993); and finally by protein deficiency, as protein is necessary for the production of haemoglobin and the iron transport protein, transferrin. This review will concentrate on low iron absorption.
FACTORS INFLUENCING THE ABSORPTION OF FOOD IRON
There are two different forms of food Fe: haem Fe (from meats) and non-haem Fe. Haem Fe has a constant absorption of 20-30%. The haem molecule is absorbed intact and the Fe released in the mucosal cell. Its absorption is little influenced by iron status of the individual or by the diet (Bjorn-Rasmussen et al. 1974). Non-haem'Fe on the other hand can vary in absorption from less than 1 % to almost 100% and it is strongly influenced by iron status of the individual (the lower the status, the higher the absorption and vice versa); by solubility in the gastriC juice (especially for fortification iron and contamination Fe) which have to dissolve before they can be absorbed (Hurrell 1992); and by the enhancers and inhibitors of absorption. We will now discuss the enhancers and inhibitors of non-haem Fe absorption.
As long ago as 1973, Layrisse and his group in S.America showed that iron absorption varied greatly between different foods. Iron absorption was lower from vegetable foods such as rice, black beans, corn and wheat, varying between 1 % and 7%, compared to animal foods such as fish and veal Where it varied from 12% to 22% (Martinez-Torres and Layrisse 1973). Many studies using the extrinsic tag radioiron technique (with 55 Fe and 59 Fe) have now confirmed that some foods inhibit Fe absorption, while other foods enhance it. The inhibitory foods include cereals (Hallberg
17

et al. 1987}, legumes such as soy (Hurrell et al. 1992), cow's milk (Hallberg et al1991), beverages such as teas, coffee (Morck et al. 1983) and red wine (Cook et al. 1995) and some vegetables such as spinach (Gillooly et al. 1983). Fruits, other vegetables such as broccoli (Gillooly et al. 1983; Ballot et al. 1987), and meat enhance non haem Fe absorption. The inhibitory component in cereals and legumes is mainly phytic acid (Hurrell et al. 1992). although polyphenols in sorghum and soy protein are also involved (Lynch et al.1994). The inhibitory factor in beverages and spinach is polyphenols and in cow's milk the inhibitory factors are calcium and casein. Ascorbic acid (and other organic acids such as citric acid) are the enhancing factors in fruit and vegetables, whereas the peptides from partially digested muscle protein are the active component in meat (Taylor et al. 1986). The mechanism of action is quite simple. The inhibitors of iron absorption bind Fe in complexes in the duodenum from which Fe is unavailable for absorption. The enhancers reduce Fe from the ferrous to ferric state, and bind it in soluble complexes from which Fe is available for absorption.
INHIBITORS OF IRON ABSORPTION
Polyphenol compounds together with phytic acid are the major inhibitors of Fe absorption in our diet. There are many different phenolic acids and flavonoids, both as individual compounds or combined as polymers such as hydrolysable and condensed tannins. Polyphenol foods include cereals such as sorghum and oats, pulses (in the seed coat), vegetables such as spinach and various spices, but the most important are the beverages such as tea, herb teas, coffee, cocoa and wine. Tea contains mixed polymers of catechin and gallic acid with glucose; herb teas such verveine, and mint contain monomeric flavonoids; coffee contains chlorogenic acid (a combination of the phenolic acid caffeic acid with quinic acid), cocoa and red wine, like sorghum, contain polymerised catechins (condensed tannins).
Th·, first demonstration of the strong inhibitory effect of tea was by Disler and colleagues in South Africa (Disler et al. 1975). This group fed Indi1!n women a meal of rice with potato and onion soup followed by water or tea. Absorption from the meal with water was 10% compared to only 2.5% with tea, a 75% reduction in absorption. In our own extrinsic tag radioiron absorption studies with different beverages (Hurrell, Reddy and Cook, unpublished), when subjects consumed two Fe fortified bread rolls with water, Fe absorption was 10%. When water was replaced by camomile tea this fell to 5%, with cocoa, coffee and red wine to around 3%, with mint tea to 2% and with tea to 1 %. With this more simple meal, tea reduced Fe absorption by 90%. The level of inhibition is dependent, to some extent, on the amount of polyphenols present, but black tea (with or without milk) was the most inhibitory, reducing Fe absorption by 90%.
Phytic acid, myoinositol-6-phosphate, is of widespread occurrence as the Mg, Ca, K salt in cereal grains and legume seeds where it is the source of phosphate and minerals during germination. It accumulates in the aleurone layer (the bran) of cereals but in the protein bodies in the endosperm of legume seeds. Its level in cereal and legume,based foods depends on the processing conditions which can remove or degrade phytic acid. It is a strong inhibitor of Fe and Zn absorption because in the gut it forms peptide-phytatemineral-iron complexes from which Fe is unavailable for' absorption. Phytic acid binds to the amino groups of the partially digested peptides and Fe binds directly to the phosphate groups or via the phosphate groups with the carboxylic acid groups or peptides. It is a very highly bound complex.
Phytic acid occurs at about 1% in most cere,cli grains and legume seeds, in wheat, rice, maize, barley, oats, soybeans, navy beans and peas (Reddy et al. 1982). When flours are manufactured from cereals by taking away the bran, we reduce phytic acid by 50% in high extraction wheat, around 80% in low extraction wheat (white flour) and polished rice and higher still in degermed maize, however when we make protein iSOlates and concentrates from legume seeds, such as soy we can increase the phytic acid content upto 2%.
18
We have studied the influence of phytic acid on iron absorption in man from wheat products (Hurrell, Reddy and Cook, unpublished). In this study, three products were tested; a high extraction wheat porridge with 240 mg phytic acid/100g, a low extraction porridge with 120 mg phytic acid/100g and a bread roll made from the low extraction porridge in which the phytic acid was zero because it had been degraded during fermentation (Svanberg and Sandberg 1988). Mean Fe absorption from the high extraction porridge was 1%, from the low extraction porridge 5% and from the bread roll 14%. In other words, we saw a 14 fold increase in Fe absorption when phytic acid in wheat flour was degraded.
ENHANCERS OF IRON ABSORPTION
There are two enhancers of iron absorption: ascorbic acid and muscle tissue. They both reduce Fe and bind it in a soluble form protected from inhibitors. Ascorbic acid reduces Fe3 to Fe2 and binds it in a soluble chelate. Fe2 is more soluble at alkaline pH; it is less reactive with hydroxyl ions in the gut as well as phytic acid and polyphenols. Muscle protein, on digestion, forms cysteine-containing peptides which similarly reduce Fe3 to Fe2 and form a soluble Fe complex.
To demonstrate that the enhancing effect of meat was due to cysteine-containing peptides, Layrisse fed human subjects a meal of 300mg maize or beans intrinsically labelled with 55 Fe with 100g veal meat or 533 mg glutathione (a tripeptide of glutamic acid, cysteine and glycine) and containing the same amount of cysteine as the meat (Taylor et al.1986). In the maize, study iron absorption from the maize meal alone was 4.1% and it increased to 7.6% with the meat. In a second experiment, absorption from the maize meal alone was 4.0% and with glutathione 6.8%, similar to the effect with meat. With black beans similar results were obtained so that glutathione, the tripeptide containing cysteine, when added to maize meal or black beans had the same enhancing effect as meat.
The enhancing effect of ascorbic acid has been well-studied. As an example, many fruit juices increase iron absorption because they are rich in ascorbic acid (24-30mg/100ml,which is often added as a fortification). In a study from Ballot et al. in 1987, mean iron absorption from a 200g rice meal was 2.5%. With the addition of 100ml apple juice, this increased to 11.1 %, with orange juice to 12.3% and with pear juice 15.0% (6 fold higher). The fruits themselves however are often less rich in ascorbic acid and sometimes do not increase Fe absorption. In the same study, 100g of grapes, peaches and apples with ascorbic acid 4-7mg/100g caused a slight reducation in Fe absorption from the rice meal, may be due to their polyphenol content, and strawberry (60mg ascorbic acid/1 OOg ) had no effect despite its relatively high ascorbic acid level, banana and melon caused a modest increase 2 fold and only the exotic fruits guava and papaya with very high ascorbic acid levels (150-180mg/100g) increased absorption substantially up to 12.6% and 17.3%. It should be emphasised therefore, that many of the fruits which we regularly consume have little or no influence on iron absorption.
Non-haem iron absorption is thus determined as the balance between the 'enhancing and inhibitory factors in a meal. The enhancers of iron absorption, ascorbic acid and muscle tissue, tend to increase absorption and the inhibitors, phytic acid, polyphenols, Ca and some proteins, tend to decrease absorption. Unfortunately, mainly due to the high phytic acid and polyphenol content of cereal and legume-based diets in developing countries, Fe absorption is usually low and iron deficiency results.
SONTROL OF IRON DEFICIENCY
T~ere are three main intervention strategies to correct for nutrient deficiencies. These are food fortification, supplementation (with tablets) and diet modification together with nutrition education. Food fortification is usually considered the best long term approach for prevention. It has moderate
19
capital expenditure, low running costs, can have high population coverage and permanent benefit if continued. Supplementation, on the other hand, is ideal for short-term interventions of highly deficient population groups, such as pregnant women. It is therapeutic. It does, however, have high personnel and administrative costs, requires a high level of supervision and can have side effects, particularly with Fe. It requires a highly effective distribution system which does not always exist. Diet modification likewise has high personnel costs. It also has high community involvement, but is often judged to have only moderate impact.
Finally, the possible intervention strategies to correct for iron deficiencies would include first of all supplementation, where recently it has been shown that a tablet once or twice a week may be as effective as once a day (Schultink et al. 1995). We can add also treatment for intestinal worms which reduces Fe loss. As to diet modification, we can recommend to eat more fruit and vegetables (to increase vitamin C), no coffee or tea with meals and to reduce phytic acid in cereals and legumes by fermentation. Finally food fortification, through careful choice of the food vehicle is needed. Flour, salt, sugar for example, can be used for widespread coverage or chocolate drinks or infant cereals targeted at 'at risk' groups. The iron compound must be of high bioavailability with no organoleptic problems. This is not always easy (Hurrell 1992 ) and may be the reason why iron fortification programmes have not always been successful.
REFERENCES
Ballot, D., Baynes, RD., Bothwell, T.H., Gilooly, M., Macfarlane, B.J.,McPhail,AP.et al (1987). The effects of fruit juices and fruits on the absorption of iron from a rice meal.Brit. J. Nutr. 57, 331-343
Basta, S:S.,Soekirman, M.S.,Karyadi, D. and Scrimshaw, N.S.(1979). Iron deficiency anemia and the productivity of adult males in Indonesia. Am.J. Glin. Nutr. 32,916-25.
Bjorn-Rasmussen, E., Hallberg, L., Isaksson, B. and Arridsson, B. (1974). Food iron absorption in man. Application of the two pool extrinsic tag method to measure haem and nonhaem iron absorption from the whole diet. J. Glin. Invest. 53, 247-255.
Bothwell, T.H., Charlton, R.W.,Cook, J.D.and Finch, C.A. (1979). Iron Metabolism in Man. Blackwell Scientific Publications, Oxford. Brabin, B.J. (1992). The role of malaria in nutritional anaemias. In: Nutritional Anaemias, pp.65-80, (S. Fomon, S.zlotkin, eds.) New York: Raven Press.
Cook J.D., Reddy, M.B. and Hurrell, R.F. (1995). The effect of red and white wine on non-heme iron absorption in humans. Am.J. Clin. Nutr. 61, 800-804.
DeMaeyer, E. & Adiels- Tegman, M. (1985). The prevalence of anaemia in the world. Wid. Hlth. Statist. Quart. 38, 302-316. Disler,P.B.,Lynch, S.R., Charlton, R.W., Torrance, J.D., Bothwell, T.H., Walker, R.B. and Mayet, F (1975). The effect of tea on iron absorption. Gut, 16, 193-200.
Gillooly, M.,Bothwell, T.H., Torrance, J.D.,McPhail, A.P., Derman, D.P., Bezwoda, W.R.et al (1983). The effects of organic acids, phytates and polyphenols on iron absorption from vegetables. Brit.J. Nutr. 49, 331-342.
Hallberg, L., Rossander, L. and Skanberg, A-B.(1987). Phytates and the inhibitory effect of bran on iron absorption in man. Am. J.Glin. Nutr.45,988-996.
Hallberg, L., Rossander-Hulthen, L., Brune, M. and Sandberg A.-S. (1991). Iron absorption from' bread Inhibiting effects of cereal fiber, phytate and inositol phosphates with different numbers of phosphate groups.
Hercberg,S.,Galan, P.i1nd Dupin, H. (1987). Iron Deficiency in Africa. Wid. Rev. Nutr. Diet.5 201-236.
Hurrell, R.F. (1992). Prospects for improving the iron fortification of foods. In Nutritional Anemias, pp. 193-208 (S. Fomon. S.Zlotkin,eds.).New York: Raven Press.
Hurrell, R.F.,Juilierat, M.A., Reddy, M.B., Lynch, S.R., Dassenko, S.A. and Cook, J.D. (1992). Soy protein, phytate and iron absorption an man. Am. J. Glin. Nutr. 56, 573-578.
20
Lozoff, B., Jiminez, E. and Abraham, W.W. (1991). Long term development outcome of infants with iron deficiency. New Eng. J. Med. 325, 687-694.
Lynch, S.R.,Dassenko, S.A., Cook, J.D., Juillerat, M.A. and Hurrell, R.F. (1994). Inhibitory effect of soybean-protein-related moiety on iron absorption in humans. Am. J. Glin. Nutr.60, 567-72.
Mahmoud A (1966). Blood loss caused by helminthic infections. Trans. R. Soc. trap. Med. Hyg. 60,766-769.
Martinez - Torres, C.and Layrisse, M. (1973). Nutritional failors in Iron Deficiency: Food Iron Absorption. In: Clinics in Haematology.Vol.2 (S.T. Callender, ed.), London: W.B. Saumders and
Co., pp.339 - 352. Morek, T.A., Lynch S.R. and Cook, J.D.(1983). Inhibition of food iron absorption by coffee.
Am J.Glin. Nutr. 37, 416-420. Reddy. N.R., Sathe, S.K., and Salunkhe, D.K. (1982).Phytate in legumes and cereals. Adv. Food
Res. 28, 1 - 92. Schultink, W., Gross, R.and Gliwitzki, M., Karyadi, D. and Matulessi, P. (1995) Effects of daily vs
twice weekly iron supplementation in Indonesian preschool children with low iron status. Am. J. Glin. Nutr. 61,111 -115.
Suharno, D., West, C.E., Muhial,Karyadi, D. and Hautvast, J.G.A. (1993). Supplementation with vitamin A and iron for nutritional anaemias in pregnant women in West Java,lndonesia, Lancet 342, 1325 - 28.
Svanberg, U. and Sandberg, A- S. (1988). Improved iron availability in weaning foods using germination and fermentation. IDRC 265 e., eds. Alnwick, D., Moses, S.,
. Schmidt O.G.pp. 366-373. Paper presented at International Workshop on Household Level Technologies for Improving Young Child Feeding in Eastern and Southern Africa,Nairobi, Oct. 1987.
Taylor, P.G., Martinez - Torres, C., Ramano, E.L. and Layrisse, M. (1986). The effect of cyteinecontaining peptides released during meat digestion on iron absorption in humans. Am. J.Glin. Nutr. 43, 68-71.
21

THE ROLE OF FOOD FORTIFICATION IN COMBATING MICRONUTRIENT DEFICIENCIES
INTRODUCTION
K. Nagy
F.Hoffmann - La Roche Ltd Basel - Switzerland
The fortification of food which is the enrichment of commonly consumed foodstuff with micronutrients in order to improve the nutritional quality of the diet offers considerable nutritional benefits to the population. Food fortification can be used to prevent micronutrient deficiencies in populations where nutritional problems are prevalent. The idea of food fortification is not new. The addition of iodine to table salt to prevent development of goiter was already suggested in France about 150 years ago. This practical and inexpensive way to prevent a nutritional disease is widely practiced today. Also other types of food fortification are carried out regularly in many countries. The focus is on both staple foods, as well as on any other food item produced and processed industrially. In the United States, for example, fortification of margarine with vitamin A, milk with vitamin D, the addition of vitamin B1, B2, niacin and iron to cereal products has been carried out for over 50 years and is practiced in many other countries too. The fortification of food becomes especially important in case of novel types of food products which are marketed to replace traditional foods. The increasing use of refined foods, introduction of engineered foods that are formulated from highly purified ingredients, may contribute to dietary micronutrient deficiency if not upgraded adequately.
There are about 50 chemically well defined substances which must be present in the diet of a healthy human being. However, the daily requirement for the different compounds vary widely. Macronutrients like carbohydrates, fats and proteins are needed in higher quantities than micronutrients such as minerals, vitamins and trace elements.
The food we consume should contain sUfficient amounts of the nutritional compounds to meet all our requirements for normal metabolism. However, with the eXQeption of mothers' milk no other food appears in nature for the sole purpose of feeding human beings. Our diet has to be balanced in order to provide a satisfactory combination of nutrients. Unfortunately this physiological demand for a balanced diet is not always satisfied. The quantity or the quality of the food intake may often be insufficient. There are several reasons for this phenomenon. The causes for inadequate nutrition can be attributed to different factors for example, primary food deficiency due to crop failure and heavy storage losses. Dental problems, infections, and other diseases may further impair'nutrition. There exist groups or single persons in the population who for economic, cultural or misconceived health reasons and occasionally just out of carelessness and ignorance have adopted eating habits which are unreasonable from a physiological point of view. The social and economical development in our society favours the growth of urban settlements and causes crowded living conditions. The large amount of food required to feed urban populations have to be kept in stock and distributed through existing sales channels. The distance from producer to consumer coupled with treatments to prevent deterioration inevitably causes losses in nutritive
, value and often decreases the dietary value of foods significantly. Another factor is the increase in the use of refined processed convenience foods which are tasty and easy to prepare but may be poor or incomplete in essential micronutrients. The average daily diet may therefore be constantly lacking in certain essential nutritional compounds. The population in rural areas, on the other hand, often depends only on foods produced locally. Climatic conditions and economic aspects may considerably limit the variety of foods available. The daily diet of the rural population may therefore
22
be Similarly inadequate. The most important dietary components which have a marked tendency to fall below requirement levels belong to the group of micronutrients namely vitamins, minerals and trace elements (Thomas, 1968 and FAO,1970).
Vitamins are active substances which are essential for life. There is a well-defined need for vitamins, and the daily requirement for vitamins has been established by national and international authorities. It is worth noting that the the Recommended Daily Allowances for nutrients (RDAs) are recommendations established for healthy persons. Special needs for nutrients arising from inherited metabolic disorders, infections, chronic diseases, etc. are not covered by the RDA. The need for certain vitamins which playa role in the prevention of degenerative diseases also exceeds the quantities defined by the RDAs (Brubacher, 1988).
Unlike macronutrients which serve as building material and energy source for the organism, the vitamins exercise catalytic functions. The metabolic functions of the vitamins have been extensively studied. Vitamin B1, B2, B6, B12, Folic Acid, Niacin, Pantothenic Acid and Biotin are incorporated in the enzymes systems which are indispensable for normal metabolism of protein, carbohydrates and fats. In these metabolic processes the vitamins do not participate as cell building material and this explains why the daily requirement remains small compared to that of the macronutrients. Soluble vitamins play their role in metabolism either directly or in the form of metabolities. The biological efficacy, for example of vitamin D, is due to its metabolities and is comparable to that of hormones. Nevertheless, the human organism is dependent on an external supply of vitamin D or at least of its precursors.
If one or more vitamins are either not available at all or only in insufficient quantities certain metabolic processes are impaired leading to disturbances in metabolism growth inhibition and disease. The functions of the single vitamins in metabolism are very specific so that in case of deficiency one or more defined by chemical reactions in certain organs will be affected. (Schotach, C.J. 1988; Czeizel and Dudas,1992 and Czeizel, 1993). The disturbances of metabolism can show up in very characteristic deficiency symptoms, however, the pattern of disturbed health is frequently confused for example when the vitamin is required for several metabolic reactions or when other nutrients or other active substances are lacking simulianeously. (Brubacher, 1988 ; Bendich and Cohen, 1988; Chandra 1992).
FOOD FORTIFICATION
Food fortification is the addition of micronutrients to food in order to upgrade its nutritive value. Food fortification is recognized as being the most effective way to eliminate dietary micronutrient defiCiencies. Food fortification is SOCially acceptable, does not change the characteristics of the food, it requires no changes in food habits, has readily visible benefits and can legally be enforced for a nationwide action. It is the least expensive nutrition intervention and its effect can easily be mOnitored and is sustainable. ,
The need for the addition (restoration) of micronutrients becomes especially evident in case of processed and reformed staple food e.g. white and semi-white flour. The removal of the germ and br~n from wheat results in a flour which is very low in vitamins and minerals (figures 1 and 2). Since white and semi-white flour are widely used for staple food such as bread and pasta products, the fortification of flour has to be implemented to improve the otherwise poor micronutrient intake.
History of Food Fortification ~
The .. concept of fortifying food with nutrients had its beginning in the 19th century when the ~ddltlon of iodine to table salt was recommended to prevent goiter. This practice was adopted first In EUrope after 1900 and then in the United States. The best known example of fortification apart
23
from iodized salt is the vitaminization of flour, by the addition of vitamin B1 (thiamin), vitamin B2 (riboflavin), vitamin PP (niacin) and iron. This practice was introduced in the USA in 1941 as a programme to prevent beriberi, ariboflavinosis, pellagra and iron-deficiency anaemia. Compulsory wheat flour fortification was implemented in many other countries too. A great number of countries followed the practice of flour fortification on optional basis (Table 1). Enrichment of maize, maize grits, rice and pasta products followed thereafter.
The last epidemic outbreak of manifest vitamin A deficiency in Europe, which led even to blindness and enhanced mortality, occurred in the early years of this century, when margarine was intorduced in Denmark as cheap replacement for butter. The disease disappeared with the mandatory vitaminization of margarine (Bloch 1931). The successful intervention in Denmark prompted many other countries to make the fortification of margarine with vitamins A and D mandatory.
Selection of Foods for Fortification
In order to make fortification programmes viable and implemented successfully nationwide certain conditions must be met.
The following characteristics of a food item to be used for fortification are considered necessary:
1. Widely consumed by the population. 2. The consumption per capita varies little from person to person and from day to day. 3. The fortification results in no change of organoleptic characteristics. 4. The cost and nature of the food make the process of fortification economically feasible on an industrial scale.
By this definition, it is obvious that staple foods should be given priority in fortification projects .. The significance of food items in the daily diet differs considerably and one has to be pragmatic In
selecting foods for fortification. In Table 2, some samples of fortified foods are given. In addition to the food items, the micronutrients and their quantities which are generally added are also mentioned.
Implementation of Food Fortification
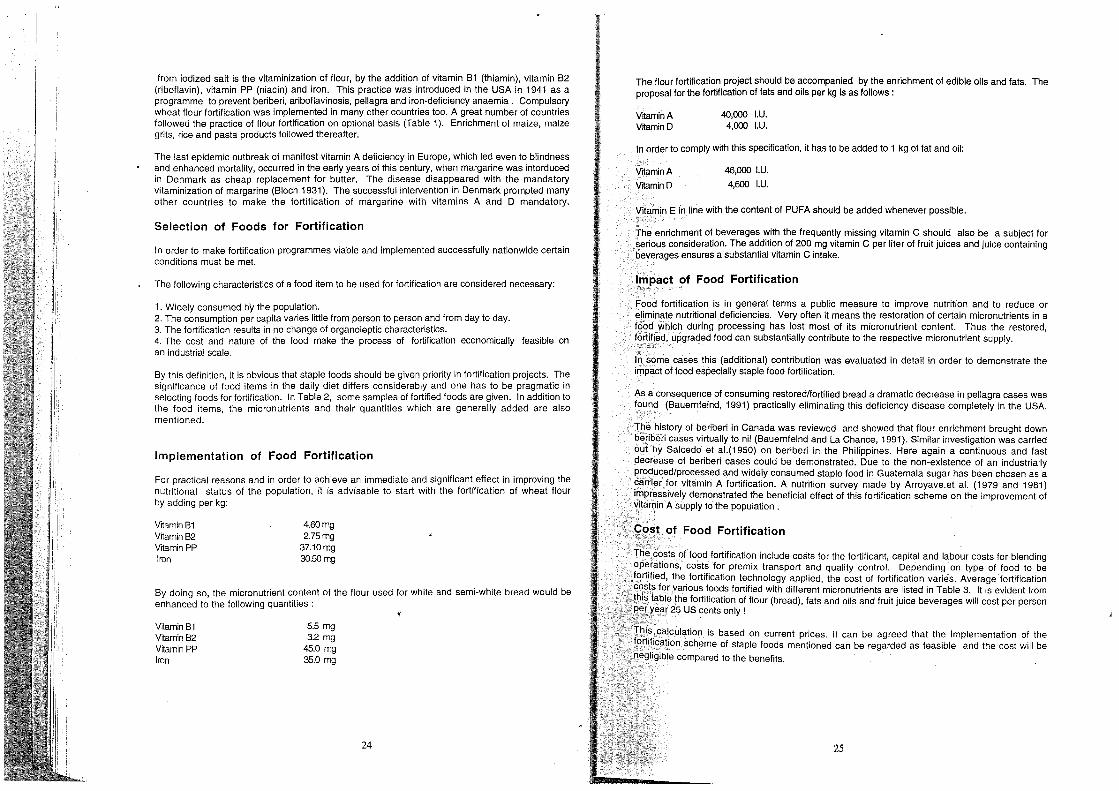
For practical reasons and in order to achieve an immediate and significant effect in improving the nutritional status of the population, it is advisable to start with the fortification of wheat flour by adding per kg:
VitaminB1 VitaminB2 Vitamin PP lIOn
4.60mg 2.75mg
37.10mg 3O.50mg
By doing so, the micronutrient content of the flour used for white and semi-white bread would be enhanced to the following quantities:
VitaminB1 Vitamin B2 VitaminPP lIOn
5.5 mg 3.2 mg
45.0 mg 35.0 mg
24
The flour fortification project should be accompanied by the enrichment of edible oils and fats. The proposal for the fortification of fats and oils per kg is as follows:
VrtaminA VitaminD
40,000 I.U. 4,000 I.U.
In order to comply with this specification, it has to be added to 1 kg of fat and oil:
VrtaminA
Vrtamin D
46,000 I.U.
4,600 I.U.
Vitamin E in line with the content of PUFA should be added whenever possible.
The enrichment of beverages with the frequently missing vitamin C should also be a subject for serious consideration. The addition of 200 mg vitamin C per liter of fruit juices and juice containing beverages ensures a substantial vitamin C intake.
Impact of Food Fortification f,>~>
Food fortification is in general terms a public measure to improve nutrition and to reduce or eliminate nutritional deficiencies. Very often it means the restoration of certain micronutrients in a food which during processing has lost most of its micronutrient content. Thus the restored, f?rtified, upgraded food can substantially contribute to the respective micronutrient supply.
In some 'cases this (additional) contribution was evaluated in detail in order to demonstrate the impaCt of food especially staple food fortification.
As a consequence of consuming restored/fortified bread a dramatic decrease in pellagra cases was found (Bauemfeind, 1991) practically eliminating this deficiency disease completely in the USA.
The history of beriberi in Canada was reviewed and showed that flour enrichment brought down beniberi cases virtually to nil (Bauernfeind and La Chance, 1991). Similar investigation was carried out by Salcedo et al.(1950) on beriberi in the Philippines. Here again a continuous and fast decrease of beriberi cases could be demonstrated. Due to the non-existence of an industrially produced/processed and widely consumed staple food in Guatemala sugar has been chosen as a carrier for vitamin A fortification. A nutrition survey made by Arroyave.et al. (1979 and 1981) impressively demonstrated the beneficial effect of this fortification scheme on the improvement of vitamin A supply to the population.
<:,()st of Food Fortification
The, costs of food fortification include costs for the fortificant, capital and labour costs for blending operations, costs for premix transport and quality control. Depending on type of food to be
,ff)rtified, the fortification technology applied, the cost of fortification varies. Average fortification cos1s for various foods fortified with different micro nutrients are listed in Table 3. It is evident from this 'iable' the fortification of flour (bread), fats and oils and fruit juice beverages will cost per person ,p_:~ ye;:tr 25 US cents only!
Ih,i,s "calculation is based on current prices. It can be agreed that the implementation of the ,ff)rti!ication scheme of staple foods mentioned can be regarded as feasible and the cost will be negligible compared to the benefits.
25

Cost of Malnutrition
The costs of malnutrition in general, and micronutrient malnutrition in particular are difficult to quantify. Only in recent years have some more sophisticated mathematical models for quantifying economic losses due to premature disability and death have been developed (The World Bank, 1993).
In order to quantify the total economic loss caused by malnutrition, the term disability-adjusted life years (DALY's) has been defined (The World Bank, 1994). DALY is an index of productive life years lost due to premature disability or death caused by malnutrition and preventable disease.
According to such calculations the average cost of malnutrition which is partly caused by micronutrient malnutrition can be assumed in the range of hundreds or even thousands of dollars per person per year (Table 4).
Safety of Food Fortification
More than 50 years of experience in food fortification in industrialized and developing countries confirm that food fortification is safe and efficacious. Vitamin levels applied in food fortification are typically in the range from 15% of the RDA to 25% of RDA per serving.
Generally fortification levels are designed such as not to exceed one RDA per day even in case the fortified food would be consumed inexcessive amounts. For safety reasons, fortification levels should be monitored on a regular basis. In order to avoid mixing errors or potency variations criteria for quality control should be defined and implemented. Fortification should be monitored by a qualified laboratory equipped with modern analytical technology and manned by experienced staff.
CONCLUSIONS
Micronutrient deficiencies remain an important health problem in many parts of the world. Four key strategies to solve micronutrient defiCiencies, namely die)ary diversification, supplementation, food fortification and nutrition education have been recommended. Each strategy has its strength and should be prioritized in the context of cultural factors, economics and maximum impact (FAO I WHO,1992).
Experience gained both in developing and industrialized countries has shown, that food fortification is safe, efficacious, inexpensive and sustainable. Suitable technologies for fortification of flour, vegetable fats and oils, fruit juice beverages, sugar and dairy products have been developed and are transferable to local food industries in developing countries.
Food fortification does not require active p~rticipation of the consumer and only minimally affects taste and appearance of foods. Economic studies by The World Bank and other institutions active in public health research have documented that food fortification is cost effective and can be maintained over decades if needed.
In order to improve the nutritional status of the population immediately it is suggested that flour and edible fats and oils (Figures 3 and 4) be fortified as proposed. As these food items are produced locally, the fortification has'to be carried out in the flour mills, margarine plants and oil mills.
The cost of Vitaminization outlined in details is reasonable and will be compensated by the improved nutritional situation in the country. Enrichment of staple foods can be regarded as one of the most effective measures in basic health service and preventative medicine.
26
,,'
Table 1 : Enrichment of flour - Legal Status in Various Countries
Australia: Bahrain: Brazil : Canada: Chile: Costa Rica: Denmark: EI Salvador: Dominican Republic: Finland: Guatemala: Honduras: Japan: Jordan:
Nicaragua: Nigeria:
Oman: Panama: Peru: Philippines: Portugal: Puerto Rico: Saudi Arabia:
Sweden:
Switzerland: United Kingdom: U,S.A. :
Venezuela: Yemen:
flour enrichment optional flour enrichment optional flour enrichment optional flour enrichment compulsory flour enrichment compulsory flour enrichment compulsory flour enrichment compulsory flour enrichment compulsory flour enrichment optional flour enrichment optional flour enrichment compulsory flour enrichment compulsory flour enrichment optional flour enrichment approved by the government flour enrichment compulsory specific standard exists; flour enrichment optional flour enrichment optional flour enrichment compulsory flour enrichment optional flour enrichment optional flour enrichment optional flour enrichment optional specific standard exists; flour enrichment optiona specific standard exists; flour enrichment optional flour enrichment optional flour enrichment compulsory specific standard exists; flour enrichment compulsory in most states flour enrichment compulsory flour enrichment optional
27
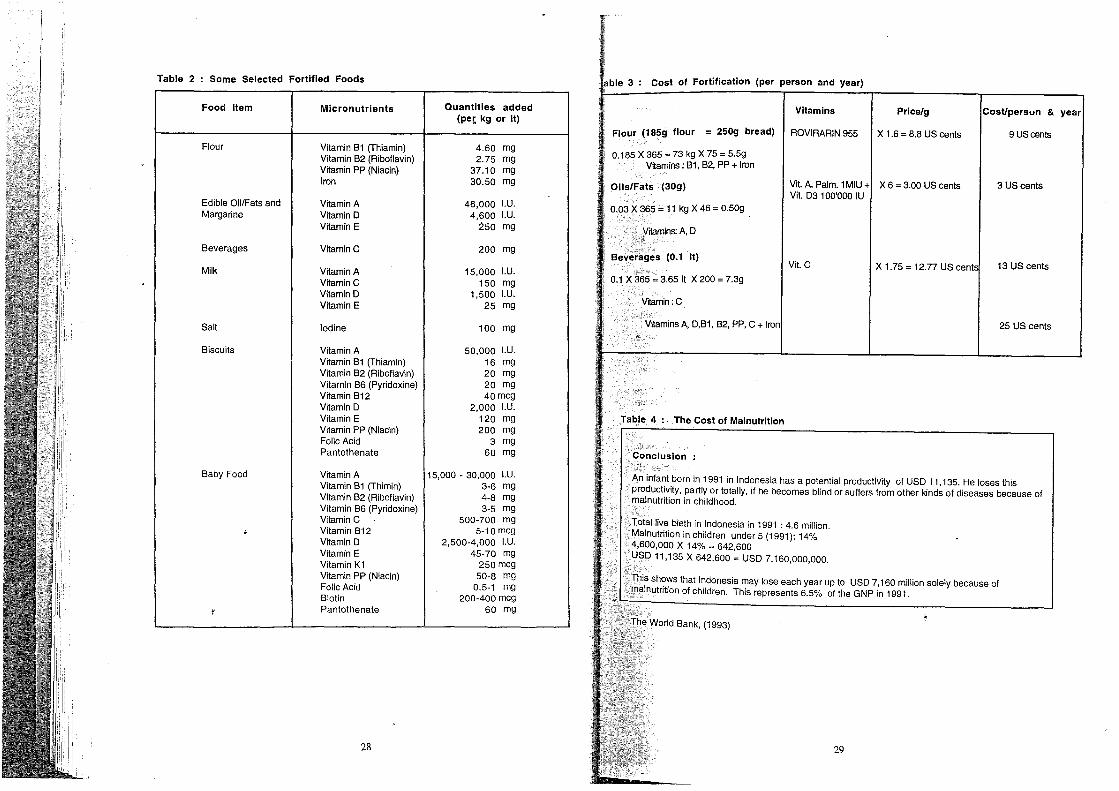
Table 2 Some Selected Fortified Foods
Food Item Micronutrients Quantities added (pet kg or It)
Flour Vitamin Bl (Thiamin) 4.60 mg Vitamin B2 (Riboflavin) 2.75 mg Vitamin PP (Niacin) 37.10 mg Iron 30.50 mg
Edible OillFats and Vitamin A 46,000 I.U. Margarine Vitamin D 4,600 I.U.
Vitamin E 250 mg
Beverages VitaminC 200 mg
Milk Vitamin A 15,000 I.U. VitaminC 150 mg Vitamin D 1,500 I.U. Vitamin E 25 mg
Salt Iodine 100 mg
Biscuits Vitamin A 50,000 I.U. Vitamin Bl (Thiamin) 16 mg Vitamin B2 (Riboflavin) 20 mg Vitamin B6 (Pyridoxine) 20 mg Vitamin 812 40mcg Vitamin D 2,000 LU. Vitamin E 120 mg Vitamin PP (Niacin) 200 mg Folic Acid 3 mg Pantothenate 60 mg
Baby Food Vitamin A 15,000 • 30,000 I.U. Vitamin Bl (Thimin) 3·6 mg Vitamin 82 (Riboflavin) 4·8 mg Vitamin 86 (Pyridoxine) 3·5 mg Vitamin C 500·700 mg
, Vitamin 812 5·10 mcg Vitamin D 2,500·4,000 I.U. Vitamin E 45·70 mg Vitamin Kl 250 mcg Vitamin PP (Niacin) 50·8 mg Folic Acid 0.5·1 mg Biotin 200·400 mcg
,. Pantothenate 60 mg
28
3 cost of Fortification (per person and year)
Vitamins Price/g &
Flour (185g flour = 250g bread) ROVIRARIN 955 X 1.6 = 8.8 US cents 9UScenls
0.185 X 365 = 73 kg X 75 = 5.5g Vftamins: 81, 82, PP + Iron
Oils/Fats (30g) ViI. A. Palm. 1 MIU ViI. D3 100'000 IU
X 6 = 3.00 US cents 3 US cents
0.03 X 365 = 11 kg X 46 = 0.50g
Vftamins: A, D ~n~
BeVe~~ges (0.1 It) Vil.C X 1.75 = 12.77 US 13 US cents
0.1 X 365 = 3.65 It X 200 = 7.3g
Vrtamin: C
,!itaminsA, D,Bl, B2, PP,C+ 25 US cents
Table 4 The Cost of Malnutrition
Conclusion
An infant born in 1991 in Indonesia has a potential productivity of USD 11,135. He loses this productivity, partly or totally, if he becomes blind or suffers from other kinds of diseases because of malnutrition in childhood.
Total live bieth in Indonesia in 1991 : 4.6 million. Malnutrition in children under 5 (1991): 14% 4,600,000 X 14% = 642,600 USD 11,135 X 642,600 = USD 7,160,000,000.
. This shows that Indonesia may lose each year up to USD 7,160 million solely because of malnutrition of children. This represents 6.5% of the GNP in 1991.
The World Bank, (1993)
29
year

REFERENCES
Arroyave, G et al (1979), Evaluation of sugar fortification with vitamin A at the national level. Pan American Health Organization, scientific publication No. 384, 1979
Arroyave,G et al (1981), The effect of vitamin A fortification of sugar on the serum vitamin A levels of preschool Guatemalan children: a longitudinal evaluation. Am J Clin Nutr 34: 41-49.
Aykroyd, W.R et al (1949), Medical survey of nutrition in Newfoundland 1948. The Canadian Medical Association Journal 60, April 1949.
Bauernfeind, J.C. and P.A. LaChance (1991). Concepts and Practices of Nutrifying Foods, pp 19-86 in: Nutrient Additions to Food, edited by J.C. Bauernfeind and P.A. LaChance, Food & Nutrition Press, Inc. Trumbull, Connecticut 06611, USA.
Bendich, A. and M. Cohen (1988). B Vitamins: Effects 'on Specific and Nonspecific Immune Responses pp 101 - 123 in: Nutrition and Immunology, Alan R Liss, Inc. 1988.
Bloch, C.E.(1931. Effects of deficiency in vitamins in infancy. Am J. Dis Child 42: 236-278. Brubacher, G.B. (1988}.Scientific Basis for the Estimation of The Daily Requirements for
Requirements of Vitamins.ln Elevated Dosages of Vitamins Benefits and Hazards. Hans Huber Publishers, Toronto.
Chandra, RK. (1992) Effect of vitamin and trace-element supplementation on immUne responses and infection in elderly subjects. Lancet 340: 1124-1127.
Czeizel, A. and 1 Dudas (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation N. ""Engl. J. Med 327: 1832 - 1835.
Czeizel, A. (1993). Prevention of congenital abnormalities by periconceptional multivitamin supplementation BMJ 306: 1645-1648.
FAa and WHO (1992). International Conference on Nutrition - Final report of the Conference, Rome Dec. 1992 FAa and WHO (1992).
Food and Agriculture Organization (FAa) (1970). Wheat in Human Nutrition. FAa, Rome. Salcedo, J. et al (1950) Artificial enrichment of white rice as a solution to endemic beriberi.
The Journal of Nutrition 42 (4) : 501-523. Schorach C.J. (1988). Importance of Adequate Folate Nutrition in Embryonic and Early Fetal
Development. In : Berger H. (ed}.vitamins and Minerals in Pregnancy and Lactation. Raven Press, New York: 167-176.
The World Bank (1993). World Development Report 1993 - Investing in Health-World Development Indicators. The World Bank, Oxfprd University Press 1993.
The World Bank (1994). Enriching Lives - Overcoming Vitamin and Mineral Malnutrition in Developing Countries. The World Bank, Washington D.C. 1994.
Thomas, B.(1968) Nutritional-Physiological views in processing cereal products.Vegetables 15, 360.
30
Figure 1
Changes in vitamin content of wheat grain with milling
40
30
20
10
Vitamin E
--"'=:::::::=--------- Riboflavin
Folic acid
Nicotinic acid Biotin
Vitamin B1
o,~----~----_,,_----._----~----~----__ 100 90 80 70 60 50 40
Extraction rate ('10)
Wheat in Human Nutrition: FAO, Ro:ne (1970)
31

Mineral retention (om) () ::r
IV w ... U> 0- '" 5 Il>
0 5 0 0 0 0 0 a 0 a 0 t:l
:1 I I I I I
~ OQ
;l C1I In
0 5-3 e; 3 :0 5-0-
~ C1I ... ~ n 0 g C1I
~1 ///// / g 0 ..., ~
'T1
~ J 7 / ::r C1I cO--..., e! c
;;J a Cil
L OQ ... '" w Il>
N 5-§-
.e,o 3::'" .", ;<1Q '" S-" 0
0 8. '!l " g £ o. c- § " c :J: c- 53 3 c- 3 ~ 5-3 OQ
figure 3
Minerals Contained in 200g Bread
Vitamins/Minerals I Daily 200g unenriched 200g whole wheat 200g enriched white Requirements white bread (70% ER) bread (95% ER) bread (70% ER + BOg
ROVlFARIN 955/ ton
Percentage of daily Percentage of daily Percentage of daily requirements supplied requirements supplied requirements supplied
81 1.2mg G,~ 50%
w
8" w
G14% 82 1.8mg "-- IIIII'IIIIJI" 25%
pp 15.0 mg G,· \ 40%
Iron 15.0 mg G12% CiI~. CiI-

(/)
0 --(/)
ca LL en
0 (1)
C '<t (I) ""'0 :; en CD ii: C
·co +-' C 0 0 (/) c E CO +-'
>-
VI c: .~
5
""C Ol
~'O. '1ij g. ~ VI
°2 Ol c: OlOl 19 E c: Q)
8 °s ~ cOl Ol a.. ~
o o o I.{)
« c E C\:l ....... :>
34
::5 o o ..;r
NaFeEDTA AS A FOOD FORTIFICANT
Richard F. Hurrell
Laboratory for Human Nutrition Swiss Federal Institute of Technology, Zurich, Switzerland
INTRODUCTION
Much of the information in this report is based on a recent monograph prepared by the International Nutritional Anemia Consultative Group (INAGG 1993) entitled 'Iron EDTA for Food Fortification'. This organisation believes that NaFeEDTA is the most suitable iron fortificant for iron fortification programmes in developing countries because it protects iron from the inhibitory ligand phytic acid. While it is at the moment about 6 times more expensive than ferrous sulphate per unit of Fe, it is 2-3 fold better absorbed and avoids the use of ascorbic acid addition. In relation to elemental Fe, which
. is often used to fortify wheat flour, NaFeEDTA is 6 times more expensive but at least 6 times better absorbed (see Hurrell (1992) for discussion of elemental Fe). In addition, using NaFeEDTA guarantees that a useful amount of Fe will be absorbed. It is not possible to guarantee that a useful
: amount of Fe will be absorbed when using some forms of elemental Fe.
REGULATORY ISSUES
In relation to the regulatory issues, JECFA (Joint WHO/FAO Expert Committee on Food Additives) in 1974 permitted the use of CaNa2EDTA and Na2EDTA at up to 2.5mg/kg body weight/day with a max. ADI (acceptable daily intake) at 150mg/person/day. The ADI was extrapolated from the rat study by Oser (1963) as the highest no-effect level (250mg/kg) and applying a safety factor of 100. Unfortunately this study did not include higher levels of EDTA. These EDTA compounds are now permitted by the local FDA's for use in many countries world wide in Asia, Africa, Middle East, Europe and America as a sequestering agent for metals to prevent offlavour, rancidity, discoloration, etc. It is most often added to foods such as mayonnaise, fish and beer and, in the USA for instance, it is permitted in 34 different foods although the estimated daily intake is only 25mg/person/ day, 10 times less than the ADI/JECFA. In 1993, at the request of the International Life Science Institute (ILSI), INAGG gave provisional approval for the use of NaFeEDTA in monitored national fortific~tion programmes but, as yet, not one has begun.
. T~ble 1 gives examples of some of the foods to which Na2CaEDTA is added in the United States for colour, texture, flavour retention or as a·preservative. There is a whole range of foods (beans,
. soft drinks, egg products, mushrooms) with beans (800mg/kg) and crab meat (250-340mg/kg) containing the highest amounts. Soft drinks, however, probably provide the highest daily intake be
of their higher consumption .
35
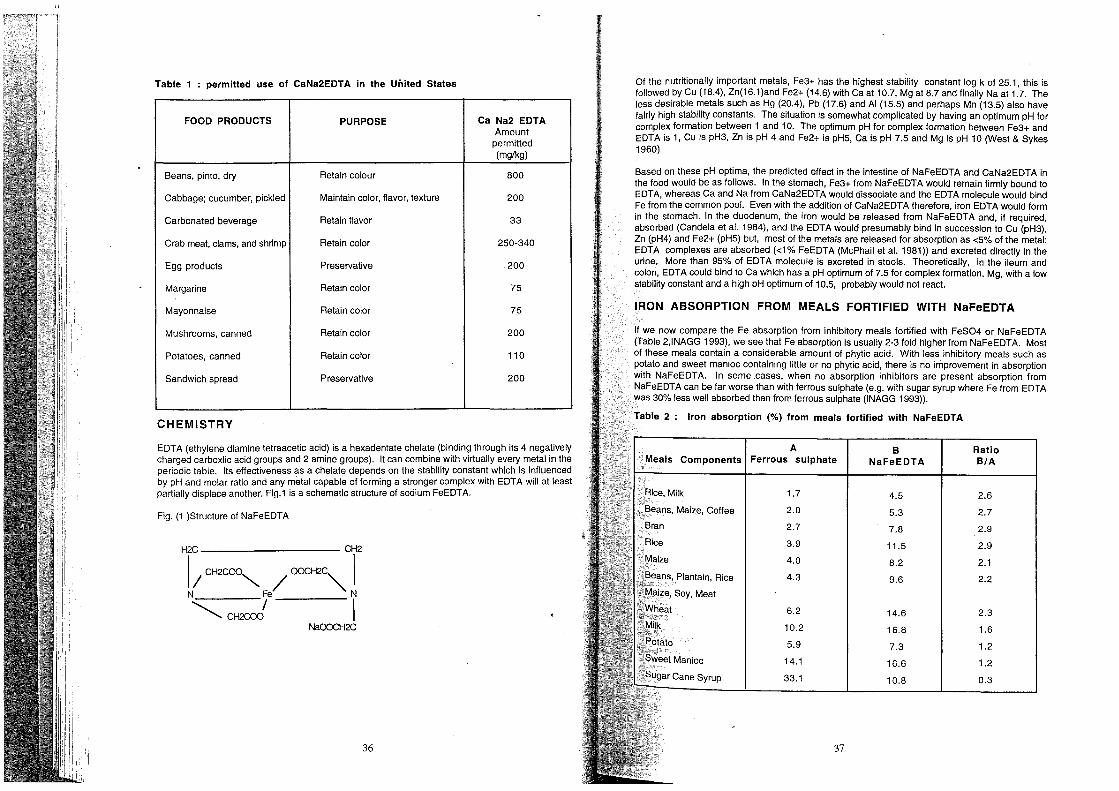
Table 1 permitted use of CaNa2EDTA in the United States
FOOD PRODUCTS PURPOSE Ca Na2 EDTA Amount
permitted (mg/kg)
Beans, pinto, dry Retain colour 800
Cabbage; cucumber, pickled Maintain color, flavor, texture 200
Carbonated beverage Retain flavor 33
Crab meat, clams, and shrimp Retain color 250-340
Egg products Preservative ·200
Margarine Retain color 75
Mayonnaise Retain color 75
Mushrooms, canned Retain color 200
Potatoes, canned Retain color 110
Sandwich spread Preservative 200
CHEMISTRY
EDTA (ethylene diamine tetraacetic acid) is a hexadentate chelate (binding through its 4 negatively charged carboxlic acid groups and 2 amine groups). It can combine with virtually every metal in the periodic table. Its effectiveness as a chelate depends on the stability constant which is influenced by pH and molar ratio and any metal capable of forming a stronger complex with EDTA will at least partially displace another. Fig.1 is a schematic structure of sodium FeEDTA.
Fig. (1 )Structure of NaFeEDTA
H~ C~
I / CH2COO"" OOCH2C, I N Fe/ 'N
~C~crx! I NaOOCH~
36
Of the nutritionally important metals, Fe3+ has the highest stability constant log k of 25.1, this is followed by Cu (18.4), Zn(16.1)and Fe2+ (14.6) with Ca at 10.7, Mg at 8.7 and finally Na at 1.7. The less desirable metals such as Hg (20.4), Pb (17.6) and AI (15.5) and perhaps Mn (13.5) also have fairly high stabil!ty constants. The situaHon is somewhat complicated by having an optimum pH for complex formation between 1 and 10. The optimum pH for complex formation between Fe3+ and EDTA is 1, Cu is pH3, Zn is pH 4 and Fe2+ is pH5, Ca is pH 7.5 and Mg is pH 10 (West & Sykes 1960)
Based on these pH optima, the predicted effect in the intestine of NaFeEDTA and CaNa2EDTA in the food would be as follows. In the stomach, Fe3+ from NaFeEDTA would remain firmly bound to EDT A, whereas Ca and Na from CaNa2EDT A would dissociate and the EDT A molecule would bind Fe from the common pool. Even with the addition of CaNa2EDTA therefore, iron EDTA would form in the stomach. In the duodenum, the iron would be released from NaFeEDT A and, if required, absorbed (Candela et al. 1984), and the EDTA would presumably bind in succession to Cu (pH3), Zn (pH4) and Fe2+ (pH5) but, most of the metals are released for absorption as <5% of the metal: EDTA complexes are absorbed «1% FeEDTA (McPhail et al. 1981)) and excreted directly in the urine. More than 95% of EDTA molecule is excreted in stools. Theoretically, in the ileum and colon, EDT A could bind to Ca which has a pH optimum of 7.5 for complex formation. Mg, with a low stability constant and a high pH optimum of 10.5, probably would not react.
IRON ABSORPTION FROM MEALS FORTIFIED WITH NaFeEDTA
If we now compare the Fe absorption from inhibitory meals fortified with FeS04 or NaFeEDTA (Table 2,INAGG 1993), we see that Fe absorption is usually 2-3 fold higher from NaFeEDTA. Most of these meals contain a considerable amount of phytic acid. With less inhibitory meals such as potato and sweet manioc containing little or no phytic acid, there is no improvement in absorption with NaFeEDTA. In some cases, when no absorption inhibitors are present absorption from NaFeEDTA can be far worse than with ferrous sulphate (e.g. with sugar syrup where Fe from EDTA was 30% less well absorbed than from ferrous sulphate (INAGG 1993)).
Table 2: Iron absorption (%) from meals fortified with NaFeEDTA
A B Ferrous sulphate NaFeEDTA
1.7 4.5
2.0 5.3
2.7 7.8
3.9 11.5
4.0 8.2
4.3 9.6
6.2 14.6
10.2 16.8
5.9 7.3
14.1 16.6
33.1 10.8
37
Ratio B/A
2.6
2.7
2.9
2.9
2.1
2.2
2.3
1.6
1.2
1.2
0.3

POSSIBLE REACTIONS OF EDTA WITH OTHER DIETARY MINERALS
If we now look at the possible impact of EDTA from NaFeEDTA (10mg fortification Fe/Day) with nutritional status of other minerals assumed to be in the diet at a level equivalent to their RDA, 2mg Cu, 15mg Zn, 350mg Mg and 800mg CA, we can calculate that on a molar basis there is 50 times more Mg and 80 times more calcium in the diet than EDTA, so there would be no likely impact of NaFeEDTA on Mg or Ca metabolism. With Cu and Zn, however, there could be a possible effect since on a molar basis there is 8 times more EDTA than Cu and equivalent amounts of EDTA and Zn. We have investigated this effect in both rats and adult women. In rats, increasing the level of EDT A in the diet increased zinc absorption and to a lesser extent copper absorption, but had no effect on calcium (Hurrel et al. 1994). In adult women fed bread rolls fortified with either NaFeEDTA or ferrous sulphate, zinc absorption was increased from 20% to 34% by adding NaFeEDTA with no effect on calcium. Zn excretion was also increased from 0.3 to 0.6% but this had little negative effect on zinc metabolism. The EDTA molecule, from added NaFeEDTA, can therefore increase both iron and zinc absorpotion from meals containing phytic acid.
INTERVENTION STUDIES
Intervention studies have been made with NaFeEDTA by Garby and Areekul (1974) in Thailand, Viteri et al. (1983) in Guatemala and Ballot et al. (1989) in South Africa. All were controlled studies, although only the Ballot et al. study was a double blind. The number of subjects varied from 600-1000 and the study time from 12-24 months. None of the vehicles themselves contained phytic acid. They were fish sauce, sugllr and curry powder. The amounts of iron provided per day ranged from 4.3mg with sugar,7.7mg with curry powder to 10-15mg with fish sauce. All intervention produced an improvement of iron status. In the fish sauce study, packed cell volume (PCV) increased in men, women and children. In the sugar study, Hb increased in children and there was an increase in serum ferritin (iron stores) in adults. In the curry powder study, there was an increase in Hb and serum ferritin in all subjects and the prevalence of anaemia in women fell dramatically from 22% to 5%.
ORGANOLEPTIC PROPERTIES
Many soluble iron compounds cause unacceptable colour and flavour changes when added to foods and/or promote fat oxidation reactions (Hurrell, 1992) The organoleptic properties of NaFeEDT A have not been well-studied. It has been shown not to promote fat oxidation in stored wheat flour, although sodium EDTA plus ferrous sulphate added seperately do promote fat oxidation Similarly to ferrous sulphate alone. NaFeEDTA, however, offers little protection against adverse colour reactions. Bananas and chocolate will turn blue as they do with all soluble iron compounds.
CONCLUSIONS
In conclusion, NaFeEDTA increases Fe absorption 2-3 fold compared to FeS04 in phytic acid containing meals. It has improved Fe status in pilot studies and has been accepted as a food additive by the JECFA. Zn absorption is probably also increased especially from low bioavailability foods, but is has no effect on Ca balance. There is still some contern over the influence of NaFeEDTA on Mn, AI, Pb and Ca absorption and this should be evaluated. It can be added without organoleptic problems to wheat flour, but needs a more systematic evaluation in respect to other foods, particularly in relation to adverse colour reactions. NaFeEDTA would appear a very useful iron compound for wheat flour fortification.
38
REFERENCES
Ballot, D.E., McPhail, A.P., Bothwell, T.H., Gilooly, M. and Mayet F.G. (1989). Fortification of curry powder with NaFe (III) EDTA: Report of a controlled iron fortifiction triaI.Am.J.Clin. Nutr. 49,162-169.
Candela,E.,Camacho M.V., Matinez-Torres,C.,Perdomo,J., Mazzarri,G.,Acurero,G.and Layrisse, M.(1984). Iron absorption by humans and swine from J.Nutr. 114, 2204-2211.
Garby, L. and AreekuI.S.(1974).lron supplementation in Thai fish sause. Ann.Trop.Med. Parasitol. 68,467-76.
International Nutritional Anemia Consultative Group (INACG) (1993).IRON EDTA for Food Fortification. The Nutrition Foundation/ILSI:Washington DC.
Hurrel,R.F.(1992).Prospects for improving the iron fortification of foods. In Nutritional Anemias, pp.193-208 (S.Fomon, S.Zlotkin, eds.). New York: Raven Press.
Hurell, R.F.,Ribas,S. and Davidsson, L.(1994).NaFe3+EDTA as a food fortificant:influence on zinc, calcium and copper metabolism in the rat. Brit.J.Nutr.71 ,85-93.
McPhail,A.P.,Bothwell, T.H.,Torrance, J.D.,Deyman, D.P.,Bezwoda, W.R. and Charlton, R.W. ", (1981). Factors affecting the absorption of iron from Fe (III) EDTA Brit.J. Nutr. 45, 215-227.
Oser.B.L.,Oser, M. and Spencer, H.C. (1963).Safety evalution studies of calcium EDTA.Tox AppJ. " " Pharmacal. 5,142-162. .
Vile ri , F.E., Alvares, E. and Torun, B. (1983). Prevention of iron deficiency by means of iron fortification of sugar. In: Nutrition intervention strategies in national development, pp. 287-314, (B.Underwood, ed.),New York: Academic Press.
West,T.S. and Sykes, Aa.S. (1960). Diamino-ethane-tetra-acetic acid. In: Analytical applications of diamino-ethane-tetra-acetic acid. Poole, UK : The British Drug Houses Ltd, pp.9-22.
39
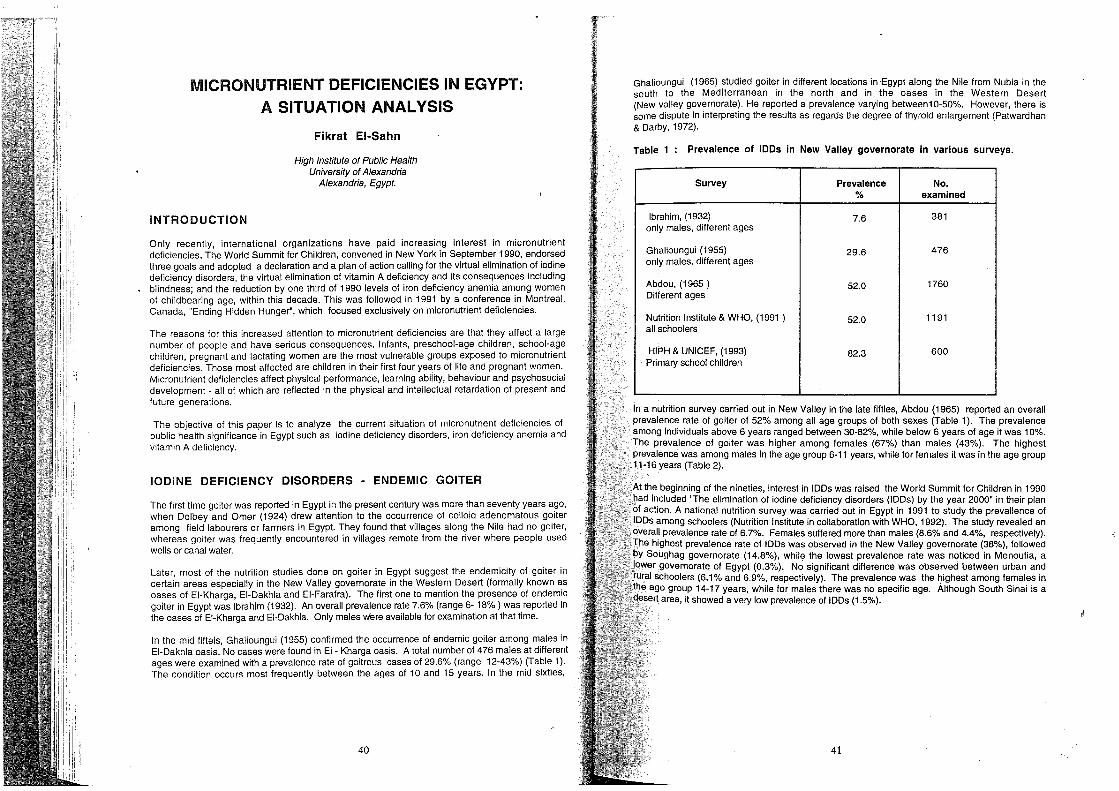
MICRONUTRIENT DEFICIENCIES IN EGYPT:
INTRODUCTION
A SITUATION ANALYSIS
Fikrat EI-Sahn
High Institute of Public Health University of Alexandria
Alexandria, E!JYPt.
Only recently, international organizations have paid increasing interest in micronutrient deficiencies. The World Summit for Children, convened in New York in September 1990, endorsed three goals and adopted a declaration and a plan of action calling for the virtual elimination of iodine deficiency disorders, the virtual elimination of vitamin A deficiency and its consequences including blindness; and the reduction by one third of 1990 levels of iron deficiency anemia among women of childbearing age, within this decade. This was followed in 1991 by a conference in Montreal, Canada, "Ending Hidden Hunger", which focused exclusively on micronutrient deficiencies.
The reasons for this increased attention to micronutrient deficiencies are that they affect a large number of people and have serious consequences. Infants, preschool-age children, school-age children, pregnant and lactating women are the most vulnerable groups exposed to micronutrient deficiencies. Those most affected are children in their first four years of life and pregnant women. Micronutrient deficiencies affect physical performance, learning abiiity, behaviour and psychosocial development - all of which are reflected in the physical and intellectual retardation of present and future generations.
The objective of this paper is to analyze the current situation of micronutrient deficiencies of public health significance in Egypt such as iodine deficiency disorders, iron deficiency anemia and vitamin A deficiency.
IODINE DEFICIENCY DISORDERS - ENDEMIC GOITER
The first time gOiter was reported in Egypt in the present century was more than seventy years ago, when Dolbey and Omer (1924) drew attention to the occurrence of colloid adenomatous goiter among field labourers or farmers in Egypt. They found that villages along the Nile had no gOiter, whereas goiter was frequently encountered in villages remote from the river where people used wells or canal water.
Later, most of the nutrition studies done on goiter in Egypt suggest the endemicity of gOiter in certain areas especially in the New Valley governorate in the Western Desert (formally known as oases of EI-Kharga, EI-Dakhla and EI-Farafra). The first one to mention the presence of endemic goiter in Egypt was Ibrahirn (1932). An overall prevalence rate 7.6% (range 6-18%) was reported in the oases of EI-Kharga and EI-Dakhla. Only males were available for examination at that tirne.
In the mid fifteis, Ghalioungui (1955) confirmed the occurrence of endemic goiter arnong males in EI-Dakhla oasis. No cases were found in EI - Kharga oasis. A total number of 476 males at different ages were examined with a prevalence rate of goitrous cases of 29.6% (range 12-43%) (Table 1). The condition occurs most frequently between the ages of 10 and 15 years. In the mid sixties,
40
Ghalioungui (1965) studied goiter in different locations in ,Egypt along the Nile from Nubia in the south to the Mediterranean in the north and in the oases in the Western Desert (New valley governorate). He reported a prevalence varying between10-50%. However, there is some dispute in interpreting the results as regards the degree of thyroid enlargement (Patwardhan & Darby, 1972).
Table 1: Prevalence of IDDs in New Valley governorate in various surveys.
Survey Prevalence No. % examined
Ibrahim, (1932) 7.6 381 only males, different ages
Ghalioungui (1955) 29.6 476 only males. different ages
Abdou, (1965 ) 52.0 1760 Different ages
Nutrition Institute & WHO, (1991 ) 52,0 1191 all schoolers
HIPH & UNICEF, (1993) 82.3 600 Primary school children
In a nutrition survey carried out in New Valley in the late fifties, Abdou (1965) reported an overall prevale~c~ ~ate of gOiter of 52% among all age groups of both sexes (Table 1). The prevalence among indiViduals above 6 years ranged between 30-82%, while below 6 years of age it was 10%. The prevalence of gOiter was higher among females (67%) than males (43%). The highest prevalence was among males in the age group 6-11 years, while for females it was in the age group 11-16 years (Table 2).
At the beginning of the nineties, interest in IDDs was raised the World Summit for Children in 1990 had i~cluded "The elimination of iodine deficiency disorders (IDDs) by the year 2000" in their plan of action, A national nutrition survey was carried out in Egypt in 1991 to study the prevallence of IDDs among schoolers (Nutrition Institute in collaboration with WHO, 1992). The stUdy revealed an overal! prevalence rate of 6.7%. Females suffered more than males (8.6% and 4.4%, respectively). The highest prevalence rate of IDDs was observed in the New Valley governorate (38%), followed by Soughag governorate (14.8%), while the lowest prevalence rate was noticed in Menoufia, a
"lower governorate of Egypt (0.3%). No significant difference was observed between urban and ,rural schoolers (6.1% and 6,9%, respectively). The prevalence was the highest among females in "the age group 14-17 years, while for males there was no specific age. Although South Sinai is a desert area, it showed a very low prevalence of IDDs (1.5%).
41

Table 2 : Prevalence of IDDs given by various surveys in Egypt according to sex and age groups.
Survey Thyroid Enlargement
Sex Grade I Grade II, 111 Total No. % % Examined
New Valley Oases, 1959 (Abdou, 1965)
0-6y M 7 28 F 6 4 29
6-11 Y M 34 17 463 F 50 16 364
11-16y M 30 14 378 F 49 30 168
More than 16 M 23 12 252 F 26 29 78
Cairo school children, 1962 M 1.4 0.3 1657 (Abdou et ai., 1967) F 15.9 1.9 1219
Follow-up survey, 197 M 6.8 0.4 1612 (Said et ai., 1980) F 10.6 2.7 1848
Cairo school children, 1991 M 10.8 843 (EI-sayed et ai., 1995) F 16.2 0.1 805
IDDs among schoolers, 1991 (NI & WHO, 1992) Primary 6-11 y M 4.4 0.1 5262
F 6.0 0.1 4276
Preparatory 11-14 y M 4.5 0.1 5705 t F 7.5 0.7 5761
Secondry 14-17 y M 3.9 0.3 4947 F 10.7 0.7 4907
100 among primary school children New valley, 1993 (HIPH & UNICEF, 1993) M 73.9 8.7 299
F 70.1 12.0 301
42
The most recent study in New Valley governorate was carried out in 1993, to study the prevalence of IDDs among primary school children 6-12 years (HIPH in collaboration with UNICEF, 1993). The overall prevalence rate of goiter was 82.3%. No significant difference by sex was found. IDDs prevalence rate was higher in rural areas (85.2%) than in urban areas (72.9%). A fertilized pie enriched with iodine is distributed to school children in New Valley. The study revealved a relatively lower prevalence rate of IDDs (81.7%) among students taking the iodine enriched pie compared with those not taking this pie (86.2%).
Despite the difference in the prevalence rates between different surveys carried out in Egypt, it is apparent that IDDs is a public health problem in some areas in Egypt especially in the New Valley governorate. Lack of sufficient iodine in soil, water, salt and agricultural products is the cause of goiter edemicity in New Valley (Ghalioungui and Shawarby, 1959; HIPH / UNICEF, 1993). The situation is aggravated by the nature of drinking water. In New Valley, water supply is from artesian wells often 200-300 meters deep, with only traces of iodine but high calcium, magnesium sulfate, sodium and potassium contents. These minerals interfere with the availability of iodine in the human body. This hardness of drinking water was regarded E;!arlier by Ibrahim (1932) to be the chief causative factor of goiter endemicity in New Valley. Contaminated drinking water was excluded as a causative factor (Ibrahim, 1932; Ghalioungui and Shawarby, 1956).
Although iodine deficiency is the primary etiological factor in causation of endemic goiter in New Valley, other factors may interplay a role. Among these are deficiency of vitamin A, vitamin C and riboflavin, low protein diet, or an excess of salt and onion intake (Abdou, 1965; Abdou and Awadallah, 1959, 1970). A hereditary predispostion was suggested as a high prevalence of gOiter was noticed among several members of the same faniily (Abdou, 1965).
Action plans for iodine deficiency disorders
The situation analysis indicated that iodine deficiency is a major public health problem in some areas in Egypt. Data available indicated that gOiter is endemic in New Valley governorate. Irrespective of whether the cause of IDDs is environmental deficiency or due to other factors,the most efficient and easiest way of eliminating the problem is by adding iodine to the diet. This can be done through the addition of iodine to salt, water, various sauces or in an oily form (WHO, 1993). However, prophylaxis with iodized salt has been mostly used. i
Successful iodized salt programmes date from 1920s in the United States, Switzerland and ",,;;anrlln~I\I'"' are good examples of the effectiveness of iodized salt (Hetzal ,1993). Yet, the
of iodized salt depends on several factors. The concentration used depends on the level consumption of table salt, the Climate, handling and distribution (Lamberg, 1993). Egypt, The EI-Nasr Salt Company, a governmental company, started the process of salt
loalln"tinn by dry mixing refined table salt with 1 00 ppm potassium iodine. Small quantities are the private sector. The average salt consumption in Egypt is 10 gm/day Hi.nge
Although iodination of salt is a Simple process, consistent monitoring of the iodine salt at the .production, storage, sale, consumption levels and prevention of sale of salt are vital components of salt iodination programmes which should be adjusted to conditions and requirements. Recently, experiments on iodized salt produced by
Company revealed that using potassium iodate instead of potassium iodine is as it is more stable (Ism ii, personal communication). Also, iodized salt should be under cool conditions, used post-cooking and used within one year of prQduction.
Committee for "Eradication of IDDs" was founded in Egypt in late 1993. The committee reores;enIIMi'lies from the Ministry of Health, Nutrition Institute (Cairo), High Institute of
(Alexand.ria), UNICEF, WHO, Ministry of Industry and EI-Nasr Salt Company. In 995 the committee started an intervention iodine programme in New Valley governorate goiter is endemic - by distributing iodized oil (oriodol) given orally. A dose of 308 mg
43

iodine is given to children below six years and pregnant women, while a dose of 616 mg iodine is given to lactating women, women at child bearing age, males and females between 6-18 years (EI-Sayed, personal communication). Also, a training course for medical and paramedical personnel working at health centers was carried out in order to explain the problem, ways of examination and treatment.
One still has to stress that the surveillance system for IDDs must be strengthened in order to eliminate the IDDs. Continuous assessment of 100 prevalence, identification of high risk areas/groups, evaluation of programmes and social mobilization is needed in order to be able to aChieve the goal of elimination of IDDs by the year 2000 in Egypt.
IRON DEFICIENCY ANAEMIA
Anaemia prevalence among preschool children
Anaemia is an important public health problem in preschool age in Egypt. In 1978, the National Nutrition Survey on preschoolers (6-72 months) revealed a prevalence rate of 38.4% of the total representative sample (Nutrition Institute and Central Disease Control, 1979). It is more prevalent among rural (39.2-44.6%) than urban populations (23.3-30.5%). A higher prevalence of anemia was shown among children of the underprivileged districts in Cairo and Alexandria (35.5 and 42.1 % respectively). This is due to increased urbanization in these cities as result of the demand for employment.
According to geographic distribution, the highest prevalence of anaemia among preschool children was detected in Beheira governorate, EI-Giza , EI-Fayoum Beni-Suef and EI-Menia (54%).The prevalence of severe anaemia «9.5 gm/dl) was 12.2% of the total representative sample. It ranged from 3.3% in small cities to 15.7% in rural regions (Table 3).
Table 3 : Percentage distribution of preschool children by anemic status and geographic areas.
Geographic Area Hb Level <9.5 gm/dl Anaemic Total No. % % Examined
Lower Egypt, rural 14.9 44.6 715
Upper Egypt, rural 16.5 43.4 358
Large villages 11.9 39.2 176
Small towns 8.3 30.5 180
Small cities 3.3 23.3 180
Total representive sample 12.2 38.4 1609,
Cario-Giza 5.6 35.5 177
Alexandria 11.8 42.1 178
Advantaged group 1.9 16.9 359
44
According to age, anaemia prevalence was hi h t diminishes till 12.8% at 60-71 months. This is e;pe~~e:~~;~23 months (59.4% ) and gradually women. Chronic undernutrition was more common among :~;~~sCPhrleldvale(nt among pregnant anaemic (17.4%). ren 31.4%) than non
A follow uP. nutrition survey was conducted in 1980 (NI and CD . Villages Originally surveyed in 1978 National Nutrition Surve Th C, 1980) In two of the six rural the prevalence of anemia and the mean hemo I b' Y'. e results of the study showed that survey. go In concentration were closely similar to the 1978
In .1 986, another follow up survey was conducted in order to children after a nine-years lapse from that of 1978 N r I S compare the status of preschool in 34 sites previously surveyed in 1978 wer . la ~o~a u;:ey. A total of 1020 school children increase in the prevalence of anaemia amon :1I
1:c
u e In t e survey. The results revealed an severe anaemia (26.8% versus 14.8% in 19i8) (C;,~~~~:~~!:~le 4). The difference is mostly in
Table 4 : Prevalence of anaemia among preschool children by age group in 34 sites and NS 1978
Age National Survey 34 Sites
in months 1978 1978 1986
6-11 57.3 77.8 74.4
12-23 59.4 57.8 60.4
24-35 41.1 44.8 56.0
36-47 39.9 40.7 48.3
48-59 16.6 27.2 38.5
60-71 12.8 33.3 35.1
Total 38.4 48.0 51.6
lence of anaemia among school children
studies have been carried out 0 h I h is a prevalent nutritional probl;ms~~~n~r~~h~O~~~~dr~~eslen s1t9u6d2ies have revealed that
(6 19 ) h . a survey among Cano ". . n level-wa~~~~9~d~7edb a prevalence rate of 13% for boys and 11 % for girls. The mean
Cario sch : . or oys and 12.5 g/dl for girls (Abdou et ai, 1967). A follow u 45~ in 001
1 c~~dr~n In 1975 revealed an increased prevalence of anaemia to reach 390j,
studY:h glr.~ al etal, 1980). The mean hemoglobin concentration was lower than th; i ere I was estimated to be 11.6 gm% for boys and 11.4 gm% for girls (Table 5
the tw~ blood hemoglobin concentration and the increase in the prevalence of anaemi~ et ai, 1980). surveys was attributed to the increased prices of animal food during this period
45
r £ g¥§

In Alexandria governorate a study of 2685 students aged 6-18 years representing the three educational levels in rural and urban areas revealed a prevalence rate of anaemia of 22.01% (Wasty, 1979). The highest prevallence rates were among primary school children with a prevalence of 27.7%. The distribution of anaemia by age showed that the highest anaemia prevalence (36.4%) was seen in children aged 6-8 years. Anaemia was more prevalent among students from rural areas (70.2%) compared to urban school children (25.8%). The mean blood hemoglobin concentration was 10.16 gm% in rural areas, while in urban areas it was 10.79 gm%.
Parasitic infections were significantly higher in prevalence among anaemic students than among non anaemic group (Wasfy, 1979). Anaemia had its impact on physical growth as demonstrated in the heights and weights of anaemic children compared to non anaemic Ones (Fahmy, 1979). More than 70% if anaemic students at the primary school level were below 50th percentile of Egyptian standards for weight and height.
Table 5 : Mean hemoglobin concentrations and percent anaemics among School Children from various surveys
Mean Hb % Anaemic Concentration
Survey B9Ys Girls Boys Girls
Cairo school children (1962) 6-19 years 12.7 12.5 13.0 11.0
(Abdou et aI., 1967)
Follow up Cairo school children (1975) 11.6 11.4 39.0 45.0
6-19 years (Said et al , 1980)
Alexandria school children (1978), 6-18 years 22.2 21.8
0Nasty, 1979}
Prevalence of anaemia in women
Early studies carried out during the fifties and sixties indicated that anaemia was a major nutrition disorder during pregnancy (Mohi EI-Oin, 1954; Abdou et aI., 1965). These studies demonstrated too that anaemia associated with pregnancy in Egypt was mostly due to iron deficiency.
The results of the National Nutrition Survey in 1978 (NI and CDC, 1979) revealed that the prevalence of anaemia among women was high in rural populations (24.3-35%), being highest in large villages followed by Lower Egypt rural and Upper Egypt rural (Table 6). The prevalence was generally lowest in urban populations (20.5-25.6%). The highest prevalence of anaemia (35.2%) was seen in women in lower socioeconomic population of Alexandria. It is worthwhile to note that the women included in this survey were not representative of Egyptian women since only those with at least one child 6-71 months of age were included in the survey.
46
Table 6 Percentage distribtion of hemoglobin among mothers of presch I h'ld and prevalence of ana 00 C I ren by geographic area. emla
Hb Level<9.5 g/dl Anaemic Total No. Geographic Area
% % Examined
Lower Egypt rural 5.2 29.8 642
Upper Egypt rural 2.4 24.3 334
Large villages 8.6 35.0 163
SmaIl towns 4.2 25.6 168
SmaIl cities 0.6 20.5 171
Total representative sample 4.3 27.5 1478
Cairo-Giza 1.8 28.7 164
Alexandria 6.1 35.2 165
Taking hemoglobin cut off levels as defined b . different physiological status is presented i~ ~~~ ~i~72C ana~mla amo!1g surveyed mothers at
of anaemia (25.3%), followed by pre an e t . actatln~ wom~n showed the highest pre'on'~nr"l on the mother's iron stores and g an women (22: 1 Yo). This may reflect the stress
,"ggrElvated by low intake of iron enriched fOOdt: e concomitant Increased requirements of iron, . adequate dietary iron replacement leads t (OeMaeyer, 1989). Prologned breast feeding . 0 serve maternal anaemia (Oakroury, 1979).
stUdies in Alexandria revealed a hi her I women attenting MCH centers fr~e an~~~~~rence hrate of Ian aemi a among lactating and
, ance osplta s (Table 7).
available data indicated that iron deflci . factors interact in causation of ana:~~~ :naemla was a crucial health problem in Egypt.
Women. The National Nutrition Surv . mong preschoolers, schoolers, pregnant and . Yet, a major contributing factor in cau:~~od~do~~~~e~l~e .the individual contributions of these Iron in the Egptian diet. This was due to the fa t -he IClency anaemia was low availabllty of
. of energy as well as protein intake per day (~a~s~tr ~~r~al~ :;:) le.f~mes were the main I of animal protein in Egyptian diet 0 ,." . IS was coupled With
changes all affected food . ,Ietary habits, economic considerations, as well a role in causation of anaemia lI~onsumptlon patterns In, Egypt which in turn may have are determinats that Increase th~ ri~t:~~cl~a~~~graVldlty, history of abortion and short birth
47
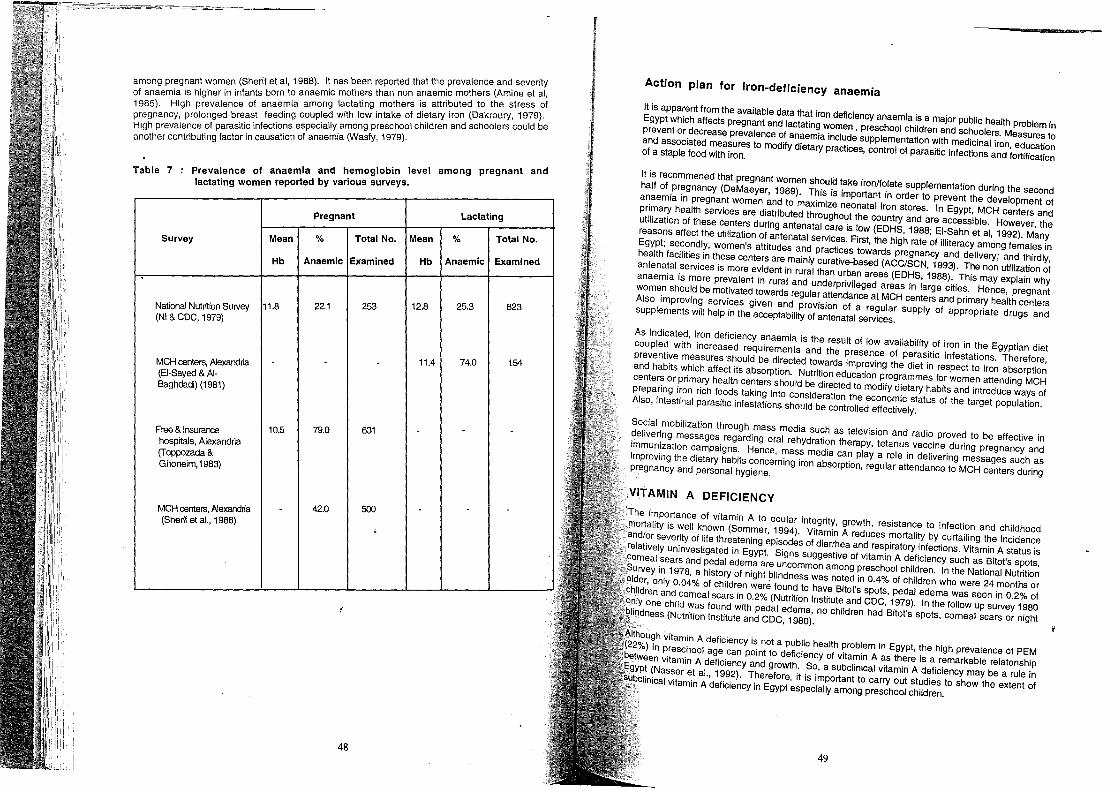
. t has been reported that the prevalence and severity among pregnant women (Shenf et ai, 1988). I. the s than non anaemic mothers (Amine et ai, of anaemia is higher in infants born to anaemic ~~tati~g mothers is attributed to the stress of 1985). High prevalence of anaemia am~n~ ith low intake of dietary iron (Dakroury, 1979). pregnancy, prolonged breast feeding coup.ell Wong preschool children and schoolers could be High prevalence of parasitic infectlO~s especla ya~M f 1979) another contributing factor in causation of anaemia \"as y, .
Table 7 . I I among pregnant and Prevalence of anaemia and ~emoglobln eve lactating women reported by various surveys.
Pregnant Lactating
Survey Mean % Total No. Mean % Total No.
Hb Anaemic Examined Hb Anaemic Examined
National Nutrition Survey 11.8 22.1 253 12.8 25.3 823 (NI & CDC, 1979)
MCH centers, Alexandria - - 11.4 74.0 154 (EI-Sayed & AI-Baghdadi) (1981)
Free & Insurance 10.5 79.0 631 - -hospnals, Alexandria (Toppozada & Ghoneim,1983)
MCH centers, Alexandria 42.0 500 - - -(Sherif et aI., 1988)
48
Action plan for iron-deficiency anaemia
It is apparent from the available data that iron deficiency anaemia is a major public health problem in Egypt which affects pregnant and lactating women, preschool children and Schoolers. Measures to prevent or decrease prevalence of anaemia include supplementation with medicinal iron, education and associated measures to modify dietary practices, control of parasitic infections and fortification of a staple food with iron.
It is recommened that pregnant women should take iron/folate supplementation during the second half of pregnancy (DeMaeyer, 1989). This is important in order to prevent the development of anaemia in pregnant women and to maximize neonatal iron stores. In Egypt, MCH centers and primary health services are distributed throughout the country and are accessible. However, the utilization of these centers during antenatal care is low (EDHS, 1988; EI-Sahn et ai, 1992). Many reasons affect the utilization of antenatal services. First, the high rate of illiteracy among females in Egypt; secondly, women's attitudes and practices towards pregnancy and delivery; and thirdly, health facilities in these centers are mainly curative-based (ACC/SCN, 1993). The non utilization of antenatal services is more evident in rural than urban areas (EDHS, 1988). This may explain why anaemia is more prevalent in rural and underprivileged areas in large cities. Hence, pregnant women should be motivated towards regular attendance at MCH centers and primary health centers Also improVing services given and provision of a regular supply of appropriate drugs and supplements will help in the acceptability of antenatal services.
As indicated, iron deficiency anaemia is the result of low availability of iron in the Egyptian diet coupled with increased requirements and the presence of paraSitic infestations. Therefore, preventive measures Should be directed towards improving the diet in respect to iron absorption and habits which affect its absorption. Nutrition education programmes for women attending MCH centers or primary health centers should be directed to mOdify dietary habits and introduce ways of preparing iron rich foods taking into consideration the economic status of the target population. Also, intestinal parasitic infestations should be controlled effectively.
Social mobilization through mass media such as television and radio proved to be effective in delivering messages regarding oral rehydration therapy, tetanus vaccine during pregnancy and immunization campaigns. Hence, mass media can playa role in delivering messages such as improving the dietary habits concerning iron absorption, regular attendance to MCH centers during pregnancy and personal hygiene.
VITAMIN A DEFICIENCY
'The importance of vitamin A to ocular integrity, growth, resistance to infection and childhood .mortality is well known (Sommer, 1994). Vitamin A reduces mortality by curtailing the incidence and/or severity of life threatening episodes of diarrhea and respiratory infections. Vitamin A status is relatively uninvestigated in Egypt. Signs suggestive of Vitamin A deficiency such as Bitot's spots, corneal sears and pedal edema are uncommon among preschool children. In the National Nutrition
. Survey in 1978, a history of night blindness was noted in 0.4% of children who were 24 months or r, only 0.04% of children were found to have Bitot's spots, pedal edema was seen in 0.2% of
and comeal scars in 0.2% (Nutrition Institute and CDC, 1979). In the follow up survey 1980 child was found with pedal edema, no Children had Bitot's spots, corneal scars or night (Nutrition Institute and CDC, 1980).
vitamin A deficiency is not a public health problem in Egypt, the high prevalence of PEM preschool age can point to deficiency of vitamin A as there is a remarkable relatonship vitamin A deficiency and growth. So, a subclinical vitamin A deficiency may be a rule in
r et aI., 1992). Therefore, it is important to carry out studies to show the extent of Vitamin A deficiency in Egypt especially among preschool children.
49

CONCLUSION
Iodine deficiency and iron deficiency anaemia are the two major micronutrient deficiencies of public health significance in Egypt. IDDs can be controlled through salt iodination. On the other hand, because the causes of iron deficiency anaemia are multifactorial, programmes aimed at reducing the prevalence of iron deficicncy anaemia should be delivered in an integrated package of interv.entions. Long term measures which may have direct or indirect impact on nutrition such as fortification of a staple diet with iron, improvement of sanitation, provision of safe water and education must be implemented at a national level. The surveillance system must be organized for continuous monitoring and evaluation of programmes aimed at controlling micronutrient malnutrition.
REFERENCES
Abdou, LA and Awadalla, M.Z. (1959). A study of the effect of some dietary factors, weight, function of the thyroid gland of experimental animals. J.Egypt. Publ. Hlth. Assoc.34, 245-58.
Abdou, LA. (1965). Nutritional status in The New Valley (in Arabic). Cairo, Egypt: In National Information and Documentation Center, pp. 238-51.
Abdou, LA., Aly, H.E. and Lebshtein, AK. (1965). Study of the nutritional status of mothers, infants and children attending maternal and child health centers in Cairo.Buli. Nutr.lnst.1, 9-20.
Abdou, LA. et al. (1967). Incidence of nutritional deficiencies, gOiter and dental caries among school children in Cairo. J. Egypt. Hlth. Assoc. 42,175-84.
Abdou, LA. and Awadalla, M.Z. (1970). A biochemical and histopathological study of the effect of some dietary factors on the thyroid gland of experimental animals. IBID 41, 45-56.
ACC/SCN (1993). Second report on the world nutrition situation. Vol. II, Chapter 1, Country trends, pp.45-50.
Amine, E.K., EI-Syed, H. and Shaheen, F.(1985). Epidemiological study of anemia in pregnancy in a rural community. Part II : The impact of mate mal anemia on the development of anemia in infancy and early childhood. Bull. H.I.P.H. 15, 185-203.
CAP MAS and UNICEF (1988). The state of Egyptian children. Chapter III : Nutrition status of Egyptian children and women. pp.76-97.
Dakroury, AM. (1979). Prevalence of anemia among pre-school children and their mothers: Relationship to child growth. In proceedings of workshop on Nutrition and Health in Egypt. Cairo, October 20 -22
DeMaeyer, E.M. (1989): Preventing and controlling iron deficiency anemia through primary health care: A guide for health administrators and program managers. World Health Organization, Geneva.
Dolby, R.V. and Omar, M. (1924). 1>. rate concerning the incidence of goiter in Egypt: An analysis of 216 cases. Lancet ii, 549. .
EDHS (1988).Egypt demographic health survey. Egypt National Population Council, Cairo. EI-Sahn, f., Darwish; O. and Soliman, N. (1992). Sociocultural and nutritional risk factors of
adolescents and young pregnant women in an endemic area of schistosomiasis. J. Egypt. Publ. Hlth. Assoc. 67, 311-340.
EI-Sayed, N.A. and AI-Baghdadi, B.S. (1981). Present nutritional status of lactating mothers in Alexandria. J. Egypf. Publ. Hlth. Assoc. 56, 122-34.
EI-Sayed, N.A., Hussein M.A.A., Ismail, H. and Kamal, A. (1995). Assessment of the prevalence of iodine deficiency disorders among primary school children in Cario,EMHT (In press).
Fahmy, s. (1979). Malnutrition among school children in Egypt. In proceedings of workshop on Nutrition and Health in Egypt, Cairo. October 20-22
Ghalioungui, P. (1955). A short medical survey of the Kharga and Dakhla oases. Bull. Clin. Sci. Soc. Abhassiah, Faculty of Medicine, Cario, 6:1
Ghalioungi, P. and Shawarby, K. (1956). Endemic goiter in Egypt. Soc. Endocrinol. Metab. 2,33-9.'
50
Ghalioungui, P. (1965). Thyroid en/ar em . .
Hetzel,N:.t~~~191~~0)r~~on and Doc~m~nta~~~~~~;~~. with reference to the Nile Basin. Egypt: The H' hi' e control of Iodine defi .
Ig nstltute of Public Health In col/abor I' cl.ency. Am. J. Publ. Hlth. 83 494-5 prevalence of . d' a Ion with UNICEF (1993) R ' . Ibr h 10 Ine deficiency disorders in N ,eport on : Assessment of the
Lamberg,aB~~: ~'9~~~~~d~~d~~!C gOiter ~n Dakhal oasis i~~~:~~~j.g~;;~~o~t~ ~lexandna,Egypt. Lozoff, B.; Jimenez, E. and WOlfl,C~.':.Z: 1~~~~d)ert and endemic goiter. Eur;p. ~ CIi:tZ~'t; 54¢~~8
Iron defiCiency N E I J . ong-term developmental t ',. Mohi EI-Din 0 (1954) . ng. . Med. 325, 687-94. ou come of infants with N ,. . Studies on anemia of r
assar, H.;Moussa, W.; Kamel A and M' p egnancy. J. Egypt. Med. Assoc 37 6138 progr If ,. InlaWI A (1992) R . " -.
Nutrition In~~~ea aencdtlncg nuttrition and health in Egypt'(1970_1990)evlews of trends, policies and en re for Disease C t I .
N USAID and Washington mimeo on ro (1978). Nutntion Status Survey I R utrltlon Institute and Centre f~r D' . , eport to
N " Washington, mimeo.. Isease Control (1980). Nutntlon status II, Report to USAID utntlon Institute in collaboration with WHO 19 and
patwa~~~~d~sNamodngDsChOOI children in Egy~t. ~~;o REe9Pyop7 on : prevalence of iodine 'deficiency . '.' . an abry, W.J. (1972) T ' ...
S 'd ~nlverslty Press. Nashville. pp. 86-91 he state of nutrition in the Arab Middle East. Vande b'lt ai, .K., MOussa, W.H., Demain . r I
nutritional defi" ' H.G., Aref, N.M. and Aly HE (19 Sherif, A.A., Mortada ~e~cle:b~m~ng Cairo school children. J.Egypt.· PUbl ~~h' :Ollow up study of
~~~.e~lt~tt~~d~~~_~~H Ueni;sKi~d~~~;~na;r~ ~~~o~;id~~~I~~i~~i:~~~~:i.~~~~~~~~;~~~t Sommer, A.(1994). Vitamin A' It. . Ig nst, Toppozada, H.K. and Ghonei~, ~~~~c~s9~~ childhood sight and life. Nutr. Re·v. 52, S60-6
wasf/~~sl.~.u(~~~~) hO~Pital ~oPulatio~s. I~~//~;~!~~o~~:;e~t~df ~~~r:gnant wom~n in free Ph 0 Th . '. naemla, a health hazard amon AI . .' - 5.
WHO (1972). N~~:i~io~~1~ Insti!ute of PU~lic Health, univ~rsi~x~fn~;:x:~~~OI children. Unpublished WHO (1991). National stra~:;~~sio:echnlcal Report Series, 503. na.
WHO ~1993). Report on the WHO/U~~~~~~;gl~~ronutrient mal~utrition, Geneva,WHO[EP89/27 In support of 100 control programs. EMRO. regional meeting on the role of communication
51
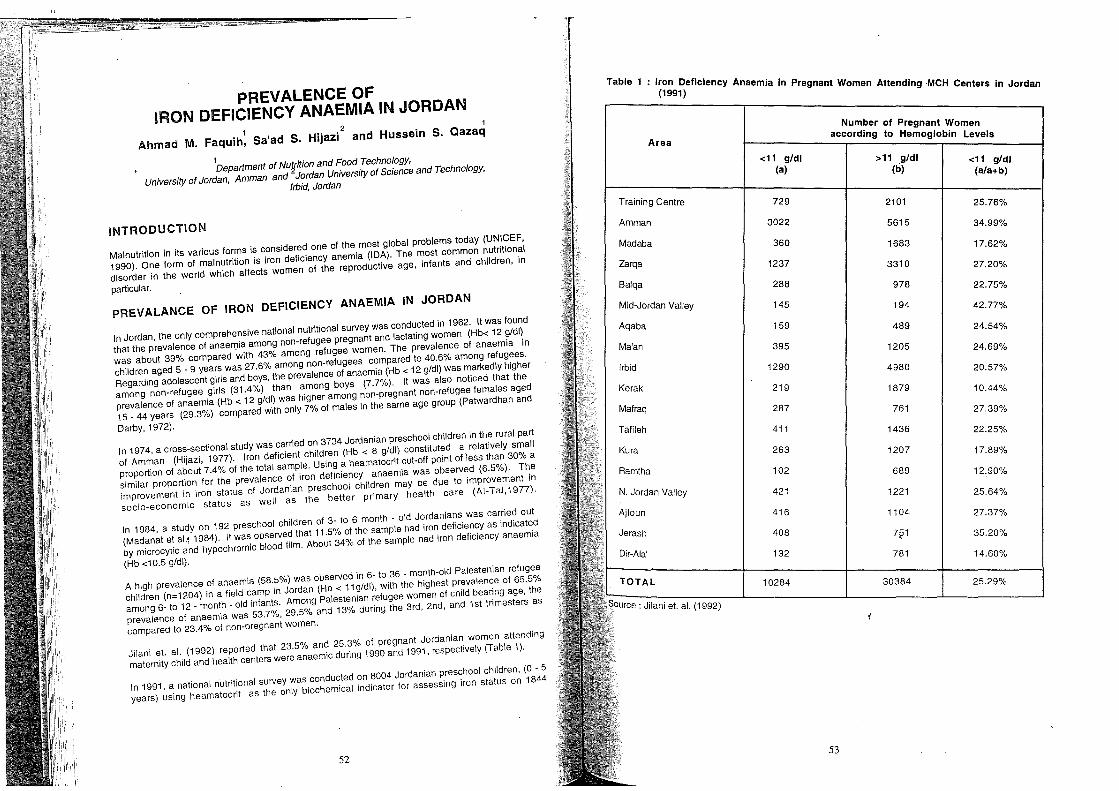
PREVALENCE OF IRON DEFICIENCY ANAEMIA IN JORDAN
1 2 1
Ahmad M. Faquih, Sa'ad S. Hijazi and Hussein S. Qazaq
1 Department of NUifition and Food Technology, University of Jordan, Amman and Jordan University of Science and Technology,
Irbid, Jordan
INTRODUCTION
Malnutrition in its various forms is considered one of the most global problems today (UNICEF, 1990). One form of malnutrition is iron deficiency anemia (IDA). The most common nutritional disorder in the world which affects women of the reproductive age, infants and children, in
particular.
PREVAlANCE OF IRON DEFICIENCY ANAEMIA IN JORDAN
In Jordan, the only comprehensive national nutritional survey was conducted in 1962. It was found that the prevalence of anaen)ia among non-refugee pregnant and lactating women (Hb< 12 g/dl) was about 39% compared with 43% among refugee women. The prevalence of anaemia in ch'lldren aged 5 _ 9 years was 27.6% among non-refugees compared to 40.6% among refugees. Regarding adolescent girls and boys, the prevalence of anaemia (Hb < 12 g/dl) was markedly higher among non-refugee girls (31.4%) than among boys (7.7%). It was also noticed that the prevalence of anaemia (Hb < 12 g/dl) was higher among non-pregnant non-refugee females aged 15 _ 44 years (29.3%) compared with only 7% of males in the same age group (Patwardhan and
Darby, 1972).
In 1974, a cross-sectional study was carried on 3734 Jordanian preschool children in the rural part of Amman (Hijazi, 1977). Iron deficient children (Hb < 8 g/dl) constituted a relatively small proportion of about 7.4% of the total sample. Using a heamatocrit cut-off point ofiess than 30% a similar proportion for the prevalence of iron deficiency anaemia was observed (6.5%). The improvement in iron status of Jordanian preschool children may be due to improvement in socio-economic status as well as the better primary health care (AI-Ta.I,1977).
In 1984, a study on 192 preschool children of 3- to 6 month - old Jordanians was carried out (Madanat et al.j 1984). It was observed that 11.5% of the sample had iron deficiency as indicated by microcy1ic and hypochromic blood film. About 34% of the sample had iron deficiencY anaemia
(Hb <10.5 g/dl).
A high prevalence of anaemia (58.5%) was observed 'In 6- to 36 - month-old Palestenian refugee children (n=1204) in a field camp in Jordan (Hb < 11 g/dl), with the highest prevalence of 65.5% among 6- to 12 _ month _ old infants. Among Palestenian refugee women of child bearing age, the prevalence of anaem'la was 53.7%,29.5% and 13% during the 3rd, 2nd, and 1st trimesters as
compared to 23.4% of non-pregnant women.
Jilani et. al. (1992) reported that 23.5% and 25.3% of pregnant Jordanian women attending maternity child and health centers were anaemic during 1990 and 1991, respectively (Table 1).
In 1991, a national nutritional survey was conducted on 8004 Jordanian preschool children, (0 - 5 years) using heamatocrit as the only biochemical indicator for assessing iron status on 1844
52
Table 1 Iron Deficiency Anaemi . (1991) a In Pregnant Women Attending MCH C . enters in Jordan
Area
Training Centre
Amman
Madaba
Zarqa
Balqa
Mid-Jordan Valley
Aqaba
Ma'an
Irbid
Kerak
Mafraq
Tafileh
Kura
Ramtha
N. Jordan Valley
: Jilani et. al. (1992)
<11 g/dl (a)
729
3022
360
1237
288
145
159
395
1290
219
287
411
263
102
421
416
408
132
10284
Num~er of Pregnant Women according to Hemoglobin Levels
53
>11 g/dl (tI)
2101
5615
1683
3310
978
194
489
1205
4980
1879
761
1436
1207
689
1221
1104
7§1
781
30384
<11 gldl (a/a+b)
25.76%
34.99%
17.62%
27.20%
22.75%
42.77%
24.54%
24.69%
20.57%
10.44%
27.39%
22.25%
17.89%
12.90%
25.64%
27.37%
35.20%
14.60%
25.29%
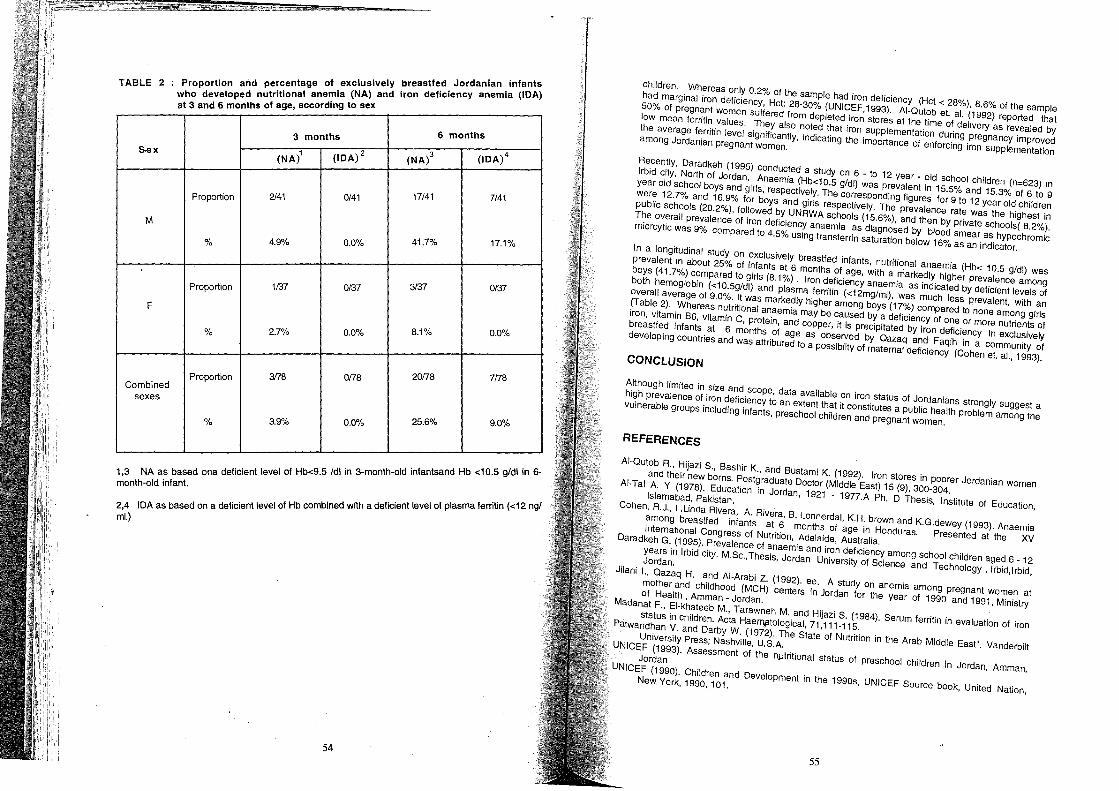
TABLE 2 breastfed Jordanian. infants . ntage of exclusively a (IDA) : Proportion and pe~~e I emia (NA) and iron deficiency aneml who developed nutntlona an d. to sex at 3 and 6 months of age, accor 109
3 months 6 months
&ex (NA)1 (IDA)2 (NA)3 (IDA)4
Proportion 2/41 0/41 17/41 7141
M
% 4.9% 0.0% 41.7% 17.1%
Proportion 1137 0/37 3/37 0/37
F
% 2.7% 0.0% 8.1% 0.0%
Proportion 3178 Combined
0178 20178 7178
sexes
% 3.9% 0.0% 25.6% 9.0%
I f Hb 9 5 Idl 10 3-month-old mfants 1 ,3 NA as based ona deficient leve 0 <. and Hb <10.5 gldl in 6-
month-old infant. b' d with a deficient level of plasma ferritin «12 ngl IDA as based on a deficient level of Hb com me 2,4
mI.)
54
Children. Whereas only 0.2% of the sample had iron deficiency (Hct < 28%), 8.6% of the sample had marginal iron deficiency, Hct: 28-30% (UNICEF,1993). AI-Qutob et. al. (1992) reported that 50% of pregnant women suffered from depleted iron stores at the time of delivery as revealed by low mean ferritin values. They also noted that iron supplementation during pregnancy improved the average ferritin level significantly, indicating the importance of enforcing iron supplementation among Jordanian pregnant women.
Recently, Daradkeh (1995) conducted a study on 6 - to 12 year _ old school children (n=623) in Irbid city, North of Jordan. Anaemia (Hb<10.5 g/dl) was prevalent in 15.5% and 15.3% of 6 to 9 year old school boys and girls, respectively. The corresponding figures for 9 to 12 year old children were 12.7% and 16.9% for boys and girls respectively. The prevalence rate was the highest in public schools (20.2%), followed by UNRWA schools (15.6%), and then by private schools( 8.2%). The overall prevalence of iron deficiency anaemia as diagnosed by blood smear as hypochromic micrcytic was 9% compared to 4.5% using transferrin saturation below 16% as an indicator.
In a longitudinal study on exclusively breastfed infants, nutritional anaemia (Hb< 10.5 g/dl) was prevalent in about 25% of infants at 6 months of age, with a markedly higher prevalence among boys (41.7%) compared to girls (8.1%). Iron deficiency anaemia as indicated by deficient levels of both hemoglobin «10.5g/dl) and plasma ferritin «12mg/ml), was much less prevalent, with an overall average of 9.0%. It was markedly higher among boys (17%) compared to none among girls (Table 2). Whereas nutritional anaemia may be caused by a deficiency of one or more nutrients of iron, vitamin B6, vitamin C, protein, and cOPper, it is preCipitated by iron deficiency in exclusively breastfed infants at 6 months of age as observed by Qazaq and Faqih in a community of developing countries and was attributed to a possibilty of maternal deficiency (Cohen et. aI., 1993).
CONCLUSION
Although limited in size and scope, data available on iron status of Jordanians strongly suggest a high prevalence of iron deficiency to an extent that it constitutes a public health problem among the vulnerable groups including infants, preschool children and pregnant women.
REFERENCES
AI-Qutob R., Hijazi S., Bashir K., and Bustami K. (1992). Iron stores in poorer Jordanian Women and their new borns. Postgraduate Doctor (Middle East) 15 (9), 300-304.
AI-Tal A. Y (1978). Education in Jordan, 1921 - 1977.A Ph. D Thesis, Institute of EdUcation, Islamabad, Pakistan.
Cohen, R.J., l.Unda Rivera, A. Rivera, B. Lonnerdal, K.H. brown and K.G.dewey (1993). Anaemia among breastfed infants at 6 months of age in Honduras. Presented at the XV international Congress of Nutrition, Adelaide, Australia.
Daradkeh G. (1995). Prevalence of anaemia and iron deficiency among school children aged 6 _ 12 years in Irbid city. M.Sc.,TheSis, Jordan University of SCience and Technology, Irbid,lrbid, Jordan.
Jilani I., Qazaq H. and AI-Arabi Z. (1992). ee. A stUdy on anemia among pregnant women at mother and childhood (MCH) centers in Jordan for the year of 1990 and 1991, Ministry of Health, Amman - Jordan.
Madanat F., EI-khateeb M., Tarawneh M. and Hijazi S. (1984). Serum ferritin in evaluation of iron status in Children. Acta Haerl'\iltological, 71,111-115.
Patwandhan V. and Darby W. (1972). The State of Nutrition in the Arab Middle East". Vanderbilt University Press; Nashville, U.S.A.
UNICEF (1993). Assessment of the n!.ltritional status of preschool children in Jordan, Amman, Jordan
UNICEF (1990). Children and Development in the 1990s, UNICEF Source book, United Nation, New York, 1990, 101.
55

MAPPING SAUDJ ARABIA FOR IODINE DEFICIENCY
1 Abdulrahman AI-Nua~m,
Yagoub AI-Mazr~u, Orner AI-Attas, 3
Nasser AI-Daghari'2 Mohammed Kamel,
3 1 . ' 2.. of Health, King Saud University, King Khalid University HOSP~~;d::~~S~~ Arabia
INTRODUCTION . ..' dine deficient areas, many suffer from the
It is estimated that 1000 million subjects IiV~ I~ ~ clinical manifestation, which basic~Uy, relates sequalae of iodine deficiency. There IS at~~~i~~ deficiency. Therefore, mild iodine deflclednc~ ~~~ to the severity and duration of exposure 0 I evalence of smaU goiter. On the other en o. be asymptometic or present wIth a low p~ present with high prevalence of severe gOiter, spectrum, severe iodine deficiency ~a:and~cape for newborn and children. hypothyroidism and mental and physlca . . d'
iodization has been shown to eradicate 10 In.e Iodine supplement, commonest thrOught ~~I;ted successful experience in iodine supplement IS deficiency and related sequelae, the mos
switzerland. . . d' e . . his can be done through unnary 10 In
There is a need to map the country for iodine def~~:cih~ age of 8 to 10 years old. Twenty four measurements of school children, pre~er~b~o~~ver for epidemiological purposes, casu~1 un~e hour urine collection is the ideal met / ' without dreatinine measurement, have been s ~wn 't~ samples assayed for iodine concentra lon, re is a need to supplement the iodine estlma e WI be practical cost effective and meaningful. T~e the modified WHO criterial (grade 1, palpable and
, t f esence of gOiter uSing ., ) clinical assess men or pr . 'bl when neck at resting position. visible only on deglutation; grade 2, VISI e d'
. 'demilogical household survey among ·Sau I We have conducted a national cross-~e~~I~~~~d~~~9 the iodine status in Saudi Arabia, through school children, aged 8 to 10 years 0 . urinary iodine estimate and clinical assessment.
METHODS Id were randomly selected from
'Id aged 8 to 10 years 0 . A total sample of 4638 Saudi school ~h~a~nie was adjusted for gender and regional population different regions of the country. Th p distribution.
Chemical Measurement . . ube from the studied population. Upon
Casual urine samples of 10 ml were collected In :a~ryl~s were sent to the central laboratory at
completion of the target sam~l~for e~:~~ ~i~~~h, for ~nalysis. Iodine determination ;t~S ~o~~::. College of Science, King Sau . nlV was digested with chloric acid under mild c?n I ~o~phate in Colorimetric Meth?d , where un~e its catalitic rule and reduction of Cenc Ammonium iodine was determined man~allY y the presence of Arsenios aCid.
56
Clinical Assessment
After completion of the urinary iodine determination, random samples of 1357 school children, aged 8 to 10 were selected from areas with different geographical nature i.e. coastal, high altitude and deserts. Clinical neck examination was done and goiter was ascertained and classified according to modified WHO criteria for goiter assessment. The neck examination was done by the first author for all the students.
RESULTS
There were 4638 school children, 2365 (51%) male and 2273 (49%) female subjects. The national median and mean (SD) of urinary iodine concentration was 18, 17(8) Ug/dl, respectively.
There were 3154 (68%) subjects living in urban communities and 1484 (32%) subjects living in rural communities. Their median and mean (SD) of urinary iodine concentration were 17 and 16(7), and 20 and 18(8) Ug/dl for urban and rural subjects, respectively (p=0.0001) (Table1).
The sample size, median urinary iodine concentration and percentage of subjects with urinary iodine concentration <10 Ug/dl in different provinces is shown in Figure, 1, at national level, 1020 (22%) of SUbjects had urinary iodine concentration <10Ug/dl.
About 1357 students from different geographical areas had their neck examined for the presence of goiter. The prevalence, degree of gOiter and their corresponding median urinary iodine concentration in different geographical areas is shown in Table 2.
DISCUSSION
There was a provincial variation with respect to median urinary iodine concentration with the lowest found in the Southern province (11 Ugldl) and the highest in the Western province (24 U/dl). The difference can be attributed to the special character of provinces, where the Southern province is characterized as being at high altitude, with low to medium income, compared with the Western province which of low altitude and medium to high income.
Subjects living in rural communities have significantly higher median urinary iodine concentration, When compared with subjects living in urban communities. This is probably attributed to the crowded is nature pf urban communities but be affected by other factors such as the type of food consumed.
The clinical assesment showed significant correlation between the prevalence of goiter and the median of urinary iodine concentration in different geographical areas, where the highest prevalence and advanced grade of goiter was found in the area with the lowest median urinary iodine. In general, the prevalence of gOiter was 28%, the majority were of mild degree (grade 1).
., FinaUy, it appears that the Southern province is the only province which had mild degree of iodine deficiency as detected by urinary iodine measurement and clinical assessment. There is a need to ensure that only iodized salt is used in the Southern province. This can be achieved through strict Control on the imported and 10caUy produced salt.
57
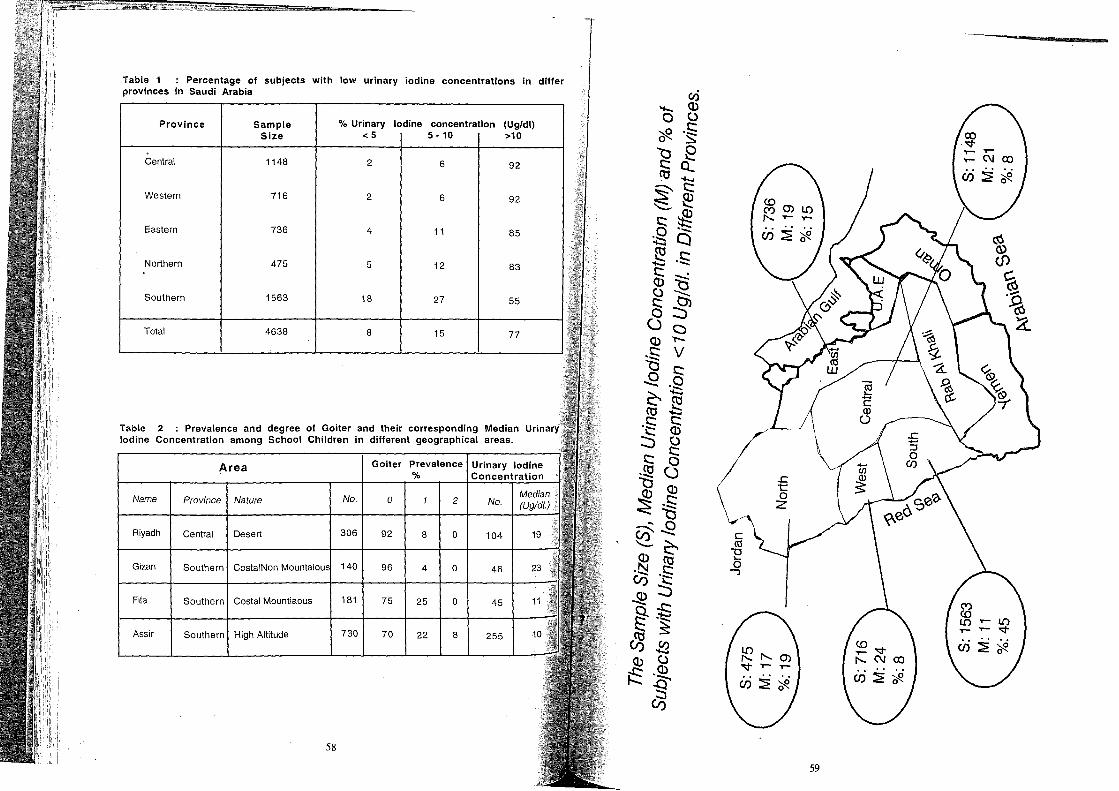
Table 1 : Percentage of subjects with low urinary iodine concentrations in differ provinces in Saudi Arabia
Province Sample % Urinary Iodine concentration (Ug/dl) Size <5 5·10 >10
Central 1148 2 6 92
Western 716 2 6 92
Eastern 736 4 11 85
Northern 475 5 12 83
Southern 1563 18 27 55
Total 4638 8 15 77
Table 2 : Prevalence and degree of Goiter and their corresponding Median Urinary Iodine Concentration among School Children in different geographical areas.
Area Goiter Prevalence Urinary Iodine % Concentration
Name Province Nature No. 0 2 No.
Riyadh Central Desert 306 92 8 0 104 19
Gizan Southern CostalNon 140 96 4 0 46
Fila Southern Costal Mountiaous 181 75 25 0 45
Assir Southern High Altitude 730 70 22 8 255
58
.c t o
Z
59

MICRONUTRIENT STATUS IN SAUDI ARABIA 1 2
Khalid A. Madani and Rufaida H. Khashog9i
1 2 Ministry of Health, King Abdulaziz University, Jeddah, Saudi Arabia
INTRODUCTION In Saudi Arabia, development has advanced markedly in the last three decades, with major improvements in the health, agriculture, education, and social services. The effects of such development, however, on the nutritional status, particularly on the micronutrients status of Saudis, has not been well studied. Little is known about the prevalence of some forms of malnutrition of micronutrients present in the Kingdom. The purpose of this paper is to highlight the micronutrients
statu.s in Saudi Arabia, namely vitamin A, vitamin D, iodine, zinc and iron deficiencies.
IRON DEFICIENCY ANAEMIA McNeil (1968) studied the infants and children in a well baby clinic of Aramco Hospital in the Eastern region of Saudi Arabia. OiJt of 500 children examined, 39.6% were anaemic. The prevalence of iron deficiency anaemia among infants aged 6 to 24 months was studied. They were attending the well baby cliniC at King Khalid University Hospital in Riyadh for routine vaccinations (AI Fawaz, 1993). Of the 366 screened infants, 37.2% were anaemic (Hb<11 g/dl). In another study using the same criteria to define iron deficiency anaemia for 84 Saudi 9 month old infants attending the baby clinic in King Khalid Hospital in Jeddah, the prevalence of anaemia was 35.7% (Stevens et aI., 1989). In view of the high prevalence of iron deficiency in infants studied, the investigators recommended that all infants should be screened for iron defic'lency during their routine visits for
immunizations. The Turaba study in western Saudi Arabia (Sebai, 1985) found that the level of haemoglobin of the Bedouin children under five years of age ranged from 6 to 10 g/100 dl in 34% of them. Another study, in the region of Tamnia, showed 36% of the pre-school children had haemoglobin levels
below the normal level (Sebai, 1981).
In Saudi Arabia iron deficiency anaemia is more prevalent among preschool children than school children. EI-Hazm'l (1982) indicated that there were statistically significant differences in.the
average haemoglobin level of pre-school and school children. •
Rasheed et al. (1989) reported that 26.4% of primary school girls had anaemia (Hb< 11 g/dl) and 9.2% were infested with one parasite or more. Anaemia was common in those harboring infestations. This finding was also confirmed by Hammouda and Lebshtcin (1987) who found that anaemia was more prevalent among primary school children with parasitic infection compared to
those with no infection. Iron deficiency anaemia in pregnancy is still a health problem in Saudi Arabia (Hartley, 1980, smart et ai, 1983 Ghaznawi et aI., 1988 Khoja et a1.1994 and Madani et aI., 1995). From Table (1) we note that the prevalence of iron deficiency anaemia among pregnant women ranges from 4.6% to 26.5%. The reason for this wide range is due to the different in the cut-off points used for
haemoglobin.
60
Table 1 Iron deficiency anaemia in Saudi pregnant women
-Study Sample size % Anaemia Cut-off
L- -Hartley (1980) 436 4.6 Hb<10g/dl
Smart et. al. (1983) 217 6.5 Hb<10g/dl
Ghaznawi et. al. (1988) 272 25.6 Hb<11g/dl
Khoja et. al. (1994) 119 10.1 Hb<10.3g/dl
Madani et. al. (1995) 952 22.9 Hb<11g/dl
AI-Amoudi (1995) 710 26.5 Hb<11g/dl
Several studies (EI-Hazmi et al 1982 Nazi, 1994) have tried to ' .' Bacchus et ai, 1986 Ghafouri et al 1 population. In one study (Nestabllsh a haematological reference va! 9~7 Khan et ai, 1989 and males and 1202 f aZI, 1994), haematological anal s ue or the Saudi Arabian
Fahd National Gu:~a~~~~;~i~allynOrmal cons~cutive Sau~i ~~:e;~r~:~o~med on 2433 (1213
:::~O~:~b~; ;::;':~~;~O"ot "h=:~91':~;:, h:=;~~~;~':';:;;,,::"" d'~::::;::::':':':~: results revealed no st~i~:~t~:et c?unt, red cell distribut'ion width ~~:~:tmOFlobin, mean cell haematological values (p 02) a ~ slgmfflcant differences betwee th ICU ocyte count. The sexes. These observatio:' an consequently a single reference v
n e male and female
reference values for Saudi ~~:bvlde detailed haematological parameter:I~~ bCrtahn
be used for both oms. I and can serve as
The normal reference ranges of hae . specimens of volunt matologlcal parameters were obt . Saudi University in ~~~~~ur~~~s (226 females and 578 males aged 2~~e2d9 by the analysis of blood
~:::~~,~:' '" "'"~ ,~'pl f:;:~~; ':i';;:;:;" ~:~::~~~ ~th,' re,"'':f~;~~:~d;:~gf:~~':; . Ig er for the Saudi males than for
Bacchus et ai, (1986) tried to es . . representative Saudi 0 . tabllsh normal reference ranges of h . the capital city of RiY~d~ul~tlon selected from the AI-Kharji district a aematologlcal parameters in a males and 110 f . aematologlcal analysis were erl ,n agricultural area 80 Km from
had SignifiCantl:~i~I~!~, i~~h ag~ ranging from 18 to 60 y~ars~~~:~t~~; 3~6 he:lthY
Saudis (1266 than females The au Ices or haemoglobin red blood count s owe that male subjects haematologic'al values t~~r~h cO;c1uded that their findings could be auns!:ean corpuscular volume stUdy, when compared with ~alaudl population. However, the number otf~ a r~ference range lor
eS,and may not represent the lemal ma es was low in this Since a large Ire population In the country.
st d rac Ion 01 the Saudi popul r' . T~ Y to determine the haemoglobin no a Ion lives at high altitudes, Khan et al (1989) c d e study was done in Abha City, WhiC~~Ss s~t~~t~~~~ ~~O~~:u~1 th~ people livtng at a hi~~ ~~:~~ea e 0 2500 to 3000 meters above sea
61

were obtained from healthy individuals coming for level. Haemoglobin levels and blood groups It showed that males had higher haemoglobin family registration In the primary health centre. Redsu
b s e These findings may help physicians to
f th e of 15 years an a ov . . ' f levels than females rom e ag , 'h In des and help administrators responsible or assess anaemia in patients liVing at hlg a I u procurement of specific blood groups for hospitals.
" uch as sickle cell traits and thalassaemias affect the The high incidences of heamoglobln dlsordersss d' EI Hazm'l et al 1985 1990) showed that
' , d f' ' anaemia tu les ( - " , determination of Iron e IClency "d' A ' b' The high incidences of haemoglobin
'h' 'despread In Sau I ra la. , haemogloblnopat les are WI , I t' tural selection and inbreeding for generations. disorders have been related to ISO a lon, na
CAUSES OF IRON DEFICIENCY ANAEMIA
Although factors responsible for the incidences of iron .deficiency anaemia in Saudi Arabia have not been well investigated, possible factors are as follows.
. ' and Ahmed et aI., 1989) reported that parasit~s were 1, Several studies (AI-Madam et aI., 19S: d' A abia The incidence of anaemia was higher In prevalent among children and adults In ~u_i e: one~ indicating that parasitic infections may be
arasitic-infected individuals than In parasl e r , , ~ne of the causes of iron deficiency anaemia In Saudi Arabia.
, ' 'arit are at risk for the development of iron deficiency 2, Mothers with high number of gravida and p Yd ultiparity the births of 5 more viable Infants, IS anaemia (Khoja et ai, 1994), In Saudi Arabia gr:n ,~ I 1994) common (Cochran and Faqeera , 1982 and Ma am e a, .
3, Low dietary intake of iron (AI-Othiameen et ai, 1992) is also an important factor in infancy,
4. Low daily dietary intake of vitamin C, which can improve iron absorption.
t' n of tea and coffee by adults during the day, especially with meals. It is known 5. Heavy consump 10 "
that tea and coffee inhibit the absorptIOn of Iron.
., 'b' lis for an in-depth study for the determination of The high prevalence of anaemia In Saudi ~~~~~f: Intervention programmes to combat iron factors associated ~Ith Iron defl~lency d be i;en a high priority. Several measures ~ust be deficiency anaemia In Saudi Arabia shoul g, These include supplementation of Iron and taken into consideration w~en. dealing With ~~~~~~rs to attend pre-natal clinics regularly, and folic acid to mothers, motivation of pregna , Sufficient spacing between subsequent assessment of haemoglobin concentr~.lons"th weaning foods fortified with iron after the first pregnancies, supplementation of breast fee ~~~t:n and treatment of intestinal parasitic infections, six months, blood screemng for children, preD'ff t nutrition education prbgrammes should be iron fortification of some common foods. I ert~~ intake of iron rich foods and vitamin C, and to conducted especially for the mothers to ~n~ea~e bit iron absorption such as phytates, tannins and reducing intake of other substances w IC In a other polyphenols.
VITAMIN D DEFICIENCY
.. .. nc in Saudi Arabia is a public health problem The available data indicate that vitamin ID 1~~~)le s~verai studies in Saudi Arabia (Elidrissy et a!, (Serenius et ai, 1984 and Abana~y at a d low I~vels of vitamin D in mother's plasma and In th~lr 1981 and Abanamy et ai, 1991) indicate h . of rickets in infants born to mothers With infants. This indicates the rOle
d ~e t~:::s~ ~~:~t~S~~igin in the prenatal period.
inadequate vitamin D status, an
62
Sedrani et al (1992 ) studied the prevalence of clinical and subclinical rickets in SaUdi children admitted to Sulimania Childrens' Hospital in Riyadh. Among the total admissions (16125) the annual prevalence of clinical and subclinical rickets was 1.3% and 3.1 % , respectively. The majority of the Children with rickets (88%) were breast fed compared with 42.1 % in the cbntrol children. Five percent of the children under 6 years of age were vitamin D deficient. There is a continuing presence of radiologically proven rickets in Saudi infants. This situation can be improved by changes in public health policy.
Another survey (Sedrani et ai, 1992 b) was carried out on 4078 subjects to stUdy the effect of regional and environmental location on vitamin D status of Saudis. The studied population was divided into five groups on the basis of their geographical location and lifestyle. The lowest 25-0HD plasma concentrations were observed in the population living in the northern province. The highest levels were found in the western province. Rural children have higher concentrations than rural adults. In the same geographical location, rural adult males and females had significantly higher 25-0HD than urban adult males and females. The concentration of 25-0HD in rural adult females is much greater than that of urban females. This study suggested several inter-regional, gender, and age differences, revealing that even in a country like Saudi Arabia, with an abundance of ultraviolet light, deficiency of vitamin D is frequently seen.
Sedrani et ai, (1992 c) studied the prevalence of vitamin D in the Saudi population. The study included 4078 Saudi males and females living in different regions in Saudi Arabia. Volunteers were from <6 years up to 90 years of age. Male children and children less than 6 years of age have a significantly higher plasma level than older SUbjects. Whereas the female adolescents (age 13-18 years) and preschool children have the lowest plasma 25-0HD levels in comparison with the other groups. No significant association was detected between plasma 25-0HD and age. Saudi males have significantly higher 25-0HD than females. Regarding the house type, occupants of tents have significantly higher 25-0HD than those occupying mud houses, villas or brick houses.
In some parts of the world such as in United States of America (Frager,1980). the peak incidences of vitamin D deficiency occurs in the winter and early spring when exposure to sunlight is at a minimum. This is not always the case in Saudi Arabia, as Sed rani et al (1992 d) found that there was no significant difference between the plasma concentration of 25-0HD in January and August for adult females and males. These results may suggest that as the temperature increase during the summer, the exposure of the Saudi population to solar ultraviolet radition is decreased, and hence, the concentration of plasma 25-0HD decreases.
CAUSES OF VITAMIN D DEFICIENCY
By reviewing the literature, the existence of a vitamin D deficiency in Saudi Arabia can be supported by the following clinical results:
1. Overdressing ·of the babies with limited exposure to sunlight, and keeping them in badly illuminated houses (Sed rani et ai, 1992 a).
2. The low level of vitamin D in plasma of mother and infants with rickets indicates that mother's milk is already depleted and deficient in vitamin D (Elidrissy 1986 and Abanamy et ai, 1991).
3. Dietary vitamin D intake has been calculated at approximately one-tenth of the daily intake of that in the United States of America (Woodhouse and Norton, 1982)
4. An increase in ultraviolet light insulation due to atmosphere dust particles could be one of the factors responsible for vitamin D deficiency in Saudi Arabia (Hannar et ai, 1984).
63

· .' Iso exists in Saudi Arabia, either as familial vitamin D 5 Genetic factors associated with rickets at in D dependent rickets (Degheishem et ai, 1991) r~sistance rickets (AI-Ageel et ai, 1B~3)t ~I ~~91) and other forms of inborn errors of metabolism congenital hypoparathyroldlsrn (Sanja e a, (Moharnmed et ai, 1993).
.' . . xists in the Saudi population at a high frequency and has In conclusion, vitamin D deflclency.e. b sunlight yet maintained privacy houses, vigorous highlighted the need for betl~r Illuminating Y d unnec~ssary wrapping up of babies, benefits of
• d' igns against excessive an . d' t d . e mass me la campa ..' d f' cy Nutrition educaton, including Ie ary a VIC sunshine for protecting against vitamin ~e~~~::~on' with vitamin D, or a diet adequate in calcium should be given to the cornmunlty. supp. t A concerted effort must be made to screen and phosphorus, effectively controlls ~I~ke s. f rickets and to educate the public about the breast-fed children to detect subcllnlca orms 0 .
importance of sunlight exposure and divesified nutrients.
VITAMIN (A) DEFICIENCY · he revalence of vitamin A deficiency. A recent National
In Saudi Arabia, there IS no data on ~ST P1993) indicates that 1.2% of Saudi subjects had serum Nutritional Survey of Saudi Arabia (KA , vitamin A levels lower than 10 ug/dl.
IODINE DEFICIENCY . . intake and the consequence of its deficiency, there is
Despite the importance of adequate Iodine oiter in Saudi Arabia. Recently, AI-Atlas and Sullmanl no data about the prevalence of endemiC '~>ns in Saudi Arabia staple foods. Bread and cereal, (1993) detemined the Iodine concentr~\ It dr'lnks and some composite meals were analyzed products, milk, eggs, vegetables, fruits, I~ ,s~ealed that iodine concentrations are comparable to for their iodine concentrations. The resu sd
re monly consumed by Saudis appears to have an
those of Britain and the United States. Foo s com adequate iodine concentration.
· ' . documented low iodine levels in samples of tap water and On the other hand, Sullmanl et al (1991) f S udi Arabia. There is no data on the prevalence of drinking mineral water from different regions 0 a mend the routine use of iodized salt In the endemic gOiter, therefore it may be Wise, to recom
Kingdorn. tl encountered endocrine diseases in childhood. Early
Hypothyroidism is one of the most frequedn Y prevents developmental retardation and other detection and proper treatment of the 981~ea~~ Saudi Arabia, there is no precise data on the sequelae of the conditIOn (Malvanx, 1 ): 'mpression fostered by clinical experience and
f h d· se however there IS an I d' prevalence 0 t e Isea , ' s for con enital hypothyroidism that this is not a rare Isease local nenonatal screenmg progr~~~~89 and ~-Jurayyan et ai, 1992). (Bacchus et al,1988; AI-Nualm e a,
CONCLUSION . e revalence and causes of iodine, zinc and vitamin A
It can be concluded that studies on th ~ er studies showed that iron deficiency aneamla deficiencies in the Kingdom are lackmg
d. ~w~~ ~nd further ameliorative measures are needed to and vitamin D deficiency do eXist In Sau I ra prevent and control these public health problems.
64
REFERENCE
Abanamy, A., Salman, H., Cheriyan, M., Shuja, M. and Siddrani, S. (1991). Vitarnin D deficiency rickets in Riyadh. Ann. Saudi Med. 11, 35 - 39.
Ahmed, M. M, and Hady, H.M.(1989). A preliminary survey of parasitic infectors and nutritional status among school children in Riyadh, Saudi Arabia.J.Egypt. Soci.Parasitology 19,101-106.
AI - Ageel, A., Ozand, P., Sobki, S., Sewairi, W. and Marx, S. (1993). The combined use of intravenous and oral calcium for the treatment of vitamin D dependent ricket type II. Clin. Endocrinol Ex!. 39, 229 - 237.
AI - Amoudi,S.M. (1995). Anaemia in pregnancy is Bisha region. SaUdi Med.J.(in press) AI - Atlas, O.S. and Sulimani, R.A. (1993) Iodine concentration in Saudi staple foods. Saudi Med. J.
14, 322 - 324. AI Fawaz, I. (1993) Surveillance for iron deficiency anaemia at a well baby clinic in Riyadh, Saudi
Arabia. Saudi Med. J. 14, 27 - 31. AI - Jurayyan, N., Abdullah, M.A., EI - Desouki, M. I., AI-Habib,S.A. and AI-Nuaim, AA (1992).
Childhood hypothyroidism in SaUdi Arabia: A retrospective study. Saudi Med. J.9,182 - 185. AI Madani, A.A., Omar, M.S., Abu-Zeid, H.A. and Abdulla, S.A. (1989) Intestinal Parasites in urban
and rural communities of Abha, Saudi Arabia. Ann. Saudi Med. 9, 182 - 185. AI- Nuaim, AR., Sulimani, R, EI-Desouki M. and Abdullah M. (1989). Thyroid gland dyshormon
ogenesis:A report of five cases with a review of the literature. Ann.Saudi Med. 9, 287 - 290. AI - Othaimeen, A.I., Kipps, M., Thomson, J. and Villanueva, B.P. (1992). Nutrition intake and
weight / height of Saudi patients at King Faisal Specialist Hospital in Riyadh, Saudi Arabia. Nutr. Health. 8,195 - 206.
Bacchus, R., Garner, E., Madkour, M.M., Haque, S. and Hurdle, A. (1986). The haematology reference range for Saudi Arabians. Saudi Med. J. 7, 46 - 52.
Bacchus, R., Williams, S, Joyce, B., Sabagh, T.O., Khan, M. and Paterson W. (1988) Neonatal Screening for congenital hypothyroidism in Riyadh. Saudi Med. J. 9, 588 - 595.
Cochran, T.E. and Faqeera.F. (1982) Demograph data: Saudi obstetric patients. Saudi Med. J.3, 3,25 - 30.
Degheishem, S.M., Sedrani, S.H., Van-Baelem, H., Bouillon, R. and Duhaiman, AS. (1991). Distribution of group - specific component / Vitamin D binding protein subtypes in Saudi Arabia. Hum. Hered. 41, 53 - 56.
EI-Hazmi, M. A. (1985) Survey of laboratory variables in Qassim children, In: Community health in Saudi Arabia, a profile of two villages in Qassim region. Saudi Med. J. (Monograph No.1), 19 - 23
EI-Hazmi, M.A. (1990). Frequency of glucose -6 phosphate dehydrogenase variants and deficiecy in Arabia. Gene. Geogr. 4, 15 - 19
EI-Hazmi, M.A., AI- Faleh, F.Z. and AI-Mofles, A.S. (1982). Establishment of normal reference for hematological parameters for healthy Saudi Arabs.Trop. Geogr. Med. 34,333-339.
EI-Hazmi, M.A., Jabbar, F.A., AI- Faleh, F.Z., AI- Swailem, AR. and Warsy, A.S. (1991). Patlerns of sickle cell, thalassemia and glucose - 6 phosphate dehydropgenase deficiency gene in north-western Saudi Arabia. Hum. Hered. 4, 26 - 34.
Elidrissy, AT. and Sedrani, S.H. (1981). Infantile vitamin D deficiency rickets in Riyadh. Is maternal vitamin D deficiency a possible factor? Calcified Tissue Intern. 33, 47 - 53.
Elidrissy, A.T. (1986). Protein-calorie nutritional status of infants with deficiency rickets in Riyadh. Ann. Saudi Med. 6,101 - 104.
Fraser, D.R. (1980). Regulation of the metabolism of vitamin D. Physiol. Rev. 60, 551 - 613. Ghafouri, H., AI Fores, A., Islam, S., Ahmed, A. and Jan, M. (1987). Haematological reference
values assessed from birth to adolescence in Saudi subjects in the area of Jeddeh.Saudi Med. J. 8, 585 - 582
Ghaznawi, H. I., E.E. and Hussein, M.M. (1988). Anaemia in pregnancy in Jeddah, Saudi Arabia. An epidemiological study. Bull. High Inst. Publ. Health. 18, 541 - 553.
Hammouda, A and Lebshtein, A (1987). Effect of Parasitic Infection on the Nutritional Status of School Children in Jeddeh and Wadi Fatma. King Abdul Aziz City for Science and Technology. Final Report, 174 - 176.
65

Hannar, M.a., EI - Yazigi. A., AI - Watban. F.a. and Fateih N. (1984). Measurement of solar ultraviolet B in Riyadh: Its significance in studies on vitamin 0 deficiency in Saudi Arabia. King Faisal Specialist Hasp. Med. J. 4, 307 - 312.
Hartley, O.R. (1980). One thousand obstetric deliveries in the asir province, Kingdom of Saudi Arabia: A review. Saudi Med. J. 1, 87 - 196. KACST (1993). Evaluation of the nutritional status of the people of Saudi Arabia. King Abdulaziz City for Science and Technology. Riyadh, Saudi Arabia.
Khan, M.U., Amir, S.E. and Aggerwal, S.(1989). Haemoglobin levels and blood groups in living at a high altitude. Ann. Saudi Med. 9, 458 - 462.
Khoja, S.M., Baroum, S.H., Salem, S.1. and Nasrat, H.A. (1994). Iron status in pregnant Saudi Arabian women in Jeddeh area. Saudi Med. J. 15,43 - 47.
Madani, K.A., Khashoggi, R.H., AI-Nowaisser, A.A., Nasrat, H.A. and Khalil, M.H.(1994). Lactation amenorrhea among Saudian Women. J. Epi. Community Health. 48, 286 - 289.
Madani, K.A., Nasrat, H.A., AI-Nowaisser, A.A., Khashoggi, R.H. and Abalkhail, B.A. (1995). Low birth weight in Taif Region, Saudi Arabia. East. Mediter. Health J. April issue.
Malvaux, P. (1983) Hypothyroidism. In: Brook C.G. (editor). Clinical Paediatric Endocrinology. Oxford: Blackwell Scientific Publications, 329 - 339.
McNiel, J.R. (1968). Variations in the response of childhood iron-deficiency anaemia to oral iron. Blood. 31, 641 - 646.
Mohammed, S., Addae, S., suleiman, S., Adzaku, F., Annobil, S., Kaddoumi, O. and Richards, J. (1993). Serum calcium parathyroid hormone, and Vitamin 0 status in children and young adults with sickle cell disease. Ann. Clin. Biochem. 30, 45-51.
Nazi, G. A. (1994). Hematological profile of Saudi newborn. saudi Med. J. 15, 243 - 249. Rasheed, P., AI-Yousef, N. and AI-Oabal, B. (1989). Nutritional profile of Saudi primary school girls
in an urban region. Ann. Saudi Med. 9, 371. - 377. Sanjad, S.A., Sakati, N.A., Abu-Osba, Y.K., Kaddoura, R. and Milner, R.O. (1991).A new syndrome
of congenital nypoparathyroidism, severe growth failure, and dysmorphic features. Arch. Dis. chgi/d. 66, 193 - 196.
Sebi, Z. A. (1985). Health in Saudi arabia, Vol. 1. Riyadh, Tihama Publications, 39 -72. Sebi, Z.A., EI-Hazmi, M.A. and Serenius F. (1981). Health profile of pre-school Children in Tamnia
villages, Saudi Arabia. In: Priorities in child care. Saudi Med. J. (Supple.1 ),68 - 71. Sedrani, S.H., Abanmy, A., Salman, H., AI-Arabie, K. and Elidrissy. A. (1992 a). Vitamin 0
status of studies: are Saudi children at risk of developing vitamin 0 deficiency rickets? Saudi Med. J. 13, 430 - 433.
Sed rani, S.H., AI Arabi. K., Abanmy, K., AI-Arabi. K., Abanmy,K. and Elidrissy, A. (1992 b). Vitamin o status of Saudi. Il.effect of regional and environmentallocation.Saudi Med. J.13, 206 - 213.
Sedrani, S.H., AI-Arabie:, K., Abanmy, and Elidrissy, A. (1992 c).vitamin 0 status of Saudies: I. effect of age, sex and living accommodation. Saudi Med. J. 13, 151 - 158.
Sedrani, S.H., AI-Arabie, K., Abanmy, A., and Elidrissy, A. (1992 d). Vitamin 0 status of Saudi: IV. seasonal variations. Saudi Med. J. 13, 423 - 429.
Serenius, F., Elidrissy, A.T. and Oandona, P. (1994). vitamin 0 nutrition in pregnant women at term and in newly born babies in Saudi Arabia. J. Clin. Pathol.37, 444 - 447.
Smart, I. S., Duncan, M.E. and Kalina, J. M. (1983). Haemoglobin levels and anaemia in pregnant Saudi women. Saudi Med. J. 4, 263 -268.
Stevens, O. W., Wainscoat, J. S., Ketley, N., Timms, P., Ayoub, o. and Shah, R. (1989). The pathogenesis of hypochromic anaemia in Saudi infants.J. Trap. Pedi. 35,301-305.
Sulaimani, R.A., AI-Atlas, 0., EI-Oesouki. M., Eissa, M., AI-Nuaim, A.A. and AI-Sekai, M. (1991). Iodine concentrations in saudi waters: A cause for concern. Ann. Saudi. Med. 2, 655 - 657.
Woodhouse, N.J. and Norton, W.l. Low vitamin 0 level in Saudi Arabians. King Faisal Specialist Hospital Med. J. 3,127 - 131.
66
MICRONUTRIENT DEFICIENCIES IN SUDAN
A SITUATION ANALYSIS
INTRODUCTION
Abdel-Gadir H. Khattab
Faculty of Agriculture University of Khartou;'
Shambat, Sudan. '
Sudan is a large country of about 2 5 millio .
~~~:~~;~~~e~~~~~ t~~~oa~~~~~~;~i:e~~~~onh~~~~:r~h~~or~~~~sir;~St~~a~~~:~S~nd t~ d~~e~~itroi~~ts f;o~uced under different farming systerIs. ~~i~e~~~t;ld ~n at~ide range of food crops and livestoc~
a consumption patterns and dietary practices. e WI a diverSity In the population to varied
The SUdanese dietary patterns are based 0 .
~~~~~~yto mlcronutrients. Therefore, there ar~ ~~tr~t~~~~I~~~i~~e~f unbablalnced diets particularly with . cy pro ems In vanous parts of the
The prevalence of micronutrient deficiencies .
~~~~~~~!t~~~ed\~e~t~~~~YdeHence their tr.ea~:~~,u~~~~~~~~~ ~~~ ~o~;~~~~~eA~~on and iodine are more difficult because of the c;easte Protein Energy Malnutrition (PEM) The sitU:;i~echelvlnbg equal refu XIS ence of a large numb f . n as ecome cou~ees resulting from the civil conflicts within theer; dcamps for displaced communities and
nes. u an and some of the ne· hb . Ig ounng
The prevalence of· . differ mlcronutnent deficiences in the Suda h
~i~!edet~:i~~~s o~ot~:u~oe~n~~;i~ul~~~~: ~~:I~~~~~rted ~n ~~!:~~ ;~~o~:~i~: i~~~:~:~ Wa~~k:r:ni~ . t;;ln ,nboflavln and vitamin C. A nutritional ' pregnancy and lactation were low in calcium In e same area found that the d· t survey conducted by Khatlab and EI H d· ' reported by. Culwick (1951), in sPit~eo~ t~~nsumed. were still defiCient in the same mi~roa~~;:i:69) :n;; Managlls ?rop rotations and the introl~~~~i~flca:l~n and diverSification policies in the Gez~:: c eme. ThiS IS an obvious case of d . . . n 0 airy farms and poultry producti .
~i~:h~E~~~l~{~:~:a~~~s:~~~ ~:~~~e1:c~:~:~~~~1~~~~~~:~~~~u~~~~t~~~:~~~~oif:~~0~;:i~: proper nutrition education in th~~r~~~ducts In the region. This situationPagain i~~i~:~~a~~~k ~: ,sUbsequently, several nutritional surv Ministry of Health, Khartoum and SO:~sN~~; undertaken by the National Nutrition Department i;evalence of defiCiencies in vitamin A iron and s I~. different parts of the country indicated that th~
e country. ,10 Ine are the most common n t ·t· I· u n lona disorders in
67
VITAMIN A DEFICIENCY . blem in the Sudan. In 1980/81 a survey was conduct~d
Vitamin A deficiency is a long standing pro. f Health Khartoum in collaboration with WHO In by the National Nutrition department, MII~~~~4~ childre~ were seen. About 1559 were in the 0-6 Kassala and Red Sea provinces. A tota
ears Of the 1559 children (0-6 years old) 814 wem males
years age group and 589 were over 6 Y . . d uffered from various degrees of vltamm A and 745 were females. All the children ex.amt~nel sros'ls to dryness of the conjectiva and Bltot's
. f om simple conJuc Iva xe h h'ld en deficiet'icy problems ranging r 't' The diet of the families of t ose c I r spots. Some exhibited corneal scars and opa~1 les'nted sorghum flour) eaten with mulah (stew consisted of kisra (a thin pan cake made frlor:tt:~~:as most common: Breakfast in the morning made of meat and vegetables). A two mea P'I nd tea Lunch is the major meal of the day
h t b d fava beans or lentl es a , There consisting of w ea rea, f f fresh fruits and vegetables was rare. consisting of "kisra" and "mulah". The consumf. Ion ~others apart from the use of "nash a" (a thin were no special diets for pregnant and lacta Ing porridge made of sorghum flour).
t in North darfur (1988) Vitamin A deficiency assessmen
• d b the National Nutrition Department, Minist~. of Health, Five districts in North Dartur were surveye Y Th erall prevalence of vitamin A defiCiency was Khartoum in collaboration with H~I In 1988iecte~ ~v night blindness, 0.1 % had Bitot's spots and found to be 0.73% of which 0.52 Yo were ea~ted that ~ctive vitamin A deficiency did not consltute a 0.1 % had corneal scars. T.halt hdata hSUg~ertain areas children were at risk. major public health problem, at oug In
Double Blind Randomized vitamin A Trial (1988-1990)
. or international Development (HIID) and the National A joint programme between Harvard Institute f
rt was undertaken during the period 1988-1990.
Nutrition Department, Ministry of Health, Kha 9 0~1m months was selected from four rural areas In
A sample of 30,000 children aged between -. two-thirds of the children were from Khartoum an.d Khartoum and one rural area In Gezlra ~r~vln~ed that symptoms of vitamin A deficiency was high In 1/3 from the Gezira. Preliminary results In Ica e all children from both locations.
Vitamin A survey in the Red sea Province . . nducted by the National Nutrition Department, .~inistry of
A survey on vitamin A defiCiency was co d 2001 children all of whom showed P?sltlve slgn~ Health Khartoum in 1989. The data ~~CIUtdg 70/. had night blindness, 0.3% had Bltot s spots an s mptoms of vitamin A deficiency. ou . 0
OY1% had both night blindness and Bitot's spots. . . Th . . . was therefore 1.1 % which exceed the WHO cntena. e
The overall prevalence of night blindness . nificant public health problem In the Red Sea results showed that vitamin A defiCiency was a slg
province. . . I Sinkat (6.1%) North Toker (6.2%), rural Vitamin A deficiency was identified in f~~~ ~~X;c~~en;::t~ree districts V:ere rural and treg fo~erall Port Sudan (2.1 %) and Hillat EI Shan 2 5% ~hile the prevalence in urban areas was on y . o. prevalence of vitamin A defiCiency was . ,
IODIN DEFICIENCY DISORDERS (100) . h incidence of endemic goitre in the region was due
Dietary studies in Dartur suggested that the hlg factors such as PEM, low Vitamin A I~take, high not only to iodine deficiency, but due ;~h~~~~nking water coupled with high consumptIOn of mllle~ sodium, potassium and Iron contents 0 t I ereal in the region, was further investigated an (pennistem typhoids). Millet, which IS the s ap e c
68
found to cause histological changes in the thyroid of millet fed rats which were similar to those that happen in humans.
During the period November 1981-January 1984 EI Tom conducted gOitre surveys in Dartur region, Kosti town and the cities of Khartoum and Port Sudan. A total of 27,830 school children of age 7-15 years were examined for goitre. In addition 1,249 inhabitants ( of all age groups) of the Shakshako villages in Tawila on the northern foot of Jabal Marra (Dartur State) were also examined for goitre.
The goitre prevalence was high among school children in both rural and urban Dartur (87.7% and 86.7% respectively) and Kosti Town (74.9%), while it was low in Khartoum (17.5%) and Port Sudan (13.5%). About 78% of the inhibitants of Shakshako villages suffered from goitre. All age groups were affected, but the most affected were those between 7 and 19 years of age with a peak among women 15-19 years old. There was no gender prevalence of goitre until puberty. After puberty the rate of thyroid gland enlargement declined in both sexes. The iodine content in the food and drinking water was low in most endemic goitre areas and was inversely proportional to the prevalence of goitre. In most locations studied the iodine content of water was low.
Due to their inland location, iodine-rich marine foods were rarely eaten in Dartur and KostL Moreover, iodine was known to be poor in soils of Dartur region.
In November 1981, a goitre survey was conducted in Darfur region. The sample included 5,885 school children aged 7-15 years from the junior classes of 33 schools in the villages of rural Darfur and the town of Nyala. They were divided randomly into three groups which received either oral or intramuscular-iodized oil and the third group remained as control. Results showed that both oral and intramuscular iodized oil were effective in goitre prophylaxis and in providing adequate iodine supply for at least two years ..
The two forms of iodized oil had an equal capacity to replenish the intrathyrodial iodine store and maintain adequate supply for hormone biosynthesis for at least two years. Thus oral iodized oil, being cheaper and simple to use, was suggested as the best altlernative for goitre prophylaxis in areas where iodization of salt was not feasible. As an alternative to the use of iodized salt, iodization of sugar was suggested. Sugar was suggested as a suitable vehicle for iodine supplementation in the Sudan based on the following reasons:
1) High consumption of sugar. 2) Central and systematic distribution of sugar to all families. 3) No appreciable change in the phYSical characteristics of sugar. 4) The additional of iodine is technically simple and economically feasible.
A national programme of endemic goitre control (EGCP) was launced in1989. In a mass prophylaxis campaign in Darfur region, 85% of the population received iodized oil treatment orally within a period of less than two years. The positive impact of iodine treatment was clearly demonstrated by examining randomly selected subjects from among those who received the iodine treatment about 72% of the goitrous resolution or definite repression of the goitre size. Ongoing studies using iOdinated sugar showed encouraging results.
IRON DEFICIENCY ANAEMIA
Attempts to control iron deficiency aneamia among pregnant and lactating mothers had been practised through Melt centres for a long time. These centres continue to distribute iron and folic acid tablets for pregnant and lactating mothers together with health and nutrition education. Therefore, available records on this problem originate from hospital records. It was reported that nutritional aneamia is one of the ten major causes for hospital admission.
69

One of the ad hoc studies conducted at EI Shagara Health Centre (Khartoum) showed that 37% of the pregnant mothers attending the heaith centre suffered from nutritional aneamia.The causitive factors behind the widespread prevalence of iron deficiency aneamia in the Sudan may be summarized as follows:
1) dietary insufficiency. 2) poverty and low purchasing power. 3) illiteracy in general and lack of food and nutrition education in particular. 4) socio-cultural factors particularly food habits and taboos. 5) prevalence of infectious and parasitic diseases. 6) loss of iron due to excessive menstruation or postpartum haemorrhage. 7) depletion of iron stores as result of repeated pregnancies. 8) problems related to malabsorption.
In spite of the absence of enough information about the prevalence of iron deficiency anaemia in the Sudan, control measures have been going on for a long time through MCH centres as mentioned previously.
VITAMIN C DEFFICIENCY IN CAMPS FOR DISPLACED PEOPLE
Cases of scurvy were reported by an NGO (Medicine Sans Frontier MSF) from Belguim in camps of displaced people in South Darfur in May 1989. The patients were complaining from swollen and painful joints and of swollen gums which bled easily. All the cases were children and adult females. They were all from camps and more were reported from the neighboring villages.
A total of 26 cases were identified in Abu Karenka camp and 10 in Muhageria camp. Most of the cases were children and adult females. All were from the poorest families and showed signs of aneamia.Treatment started immediately with vitamin C tablets 250 mg/day for 10 days. The symptoms disappeared rapidly with treatment. The treatment was accompained by nutrition education.
The problem was caused by the fact that most displaced people in the camps were dependent on food distribution for all their nutritional needs. They were separated from their usual environment and lost their assets upon which the local population could rely. The only item in the food ration containing vitamin C was groundnuts (provided they were eaten fresh). Foodstuffs rich in vitamin C were scarce in the market during that period, and hence their price made them inaccessible to most displaced families.
Wild foods which could have replaced the cultivated ones were not known to the displaced persons as they came from parts of the country with different plant life.
CURRENT PROGRAMMES UNDERTAKEN BY THE MINISTRY OF HEALTH TO COMBAT MICRONUTRIENT DEFFICIENCIES IN SUDAN
The existing programmes for the elimination of the micronutrient deficiencies include: ~
1. Iodine supplementation in endemic areas by the administration of iodinated oil injections and tablets.
2. lodization of common salt which has now been adopted as a Government policy and will be available in all parts of the country.
70
3. Fortification of sugar with iodine is bei consumed by virtually everyone in lhe Su:~ttesmpted at all the experimental level since sugar is exceptions were security does not prevail H' ugar reaches the whole population with very few
. ence sugar provides a very suitable vehicle for iodine.
4. Supplementation of vitamin A capsules in most affected areas.
5.Programmes of intensive nutrition and health . . consumption of locally available foods rich in vl'tam' eAdu~atlon are. bemg condUcted to enhance
In ,Iron and Iodine.
6. Conduction of regular surveys at the state level to d . deflclences in different geographical locations and edtfefct signs symptoms of micronutrient
among I erent population groups.
FUTURE STRATEGIES AND PLANS TO PREVENT MICRONUTRIENT DEFICIENCIES IN THE SUDAN AND CONTROL
Vitamin A
Supplementation of vitamin A capsules will co r under two years living in areas with inad ~ Inue to ens~re that at least 80% of the children combination of promotion of breast f d' equa e vitamin A Intake receive vitamin A through a fortification and Supplementation Plan ee lng, tlmprovement of supplementary feeding and food
IDD . s are se to eliminate vitamin A deficiency by the year 2000.
Iodized salt for human and animal consum tion' I . will be made available in 'all parts f ih ,inC udlng salt for food processing and preservation Supplementation with oral or injected iO~ize; o~~.~t~y wdhere IDD is a public health problem. possible. I e a mlnstered where full salt iodization is not
Research on the use of sugar as a vehicl f . d' and iron will continue to achieve a practica~ a~dlo Ine and the double fortification of salt with iodine that by the year 2000 elimination of IDD . h' eadsy ways of dlstrrbutlon and storage. It is planned , IS ac leve .
Iron Deficiency Anaemia
Programmes for the reduction of iron deficienc a' . gOing on through determination of the h I Y naemla among Infants and children are now of ferrious sulphate tablets or injection ~:~~~~b~~ level and the admlnstration of iron in the form Iron deficiency anaemia will be r d d b 0 need It. It IS planned that by the year 2000
e uce ,y one third compared to its level in 1990.
Future strategies for the prevention a d t I . . . include the continuation of regular nut~r co~ ro of mlcronutrrent deficiencies in the Sudan also and the causes behind the prevale~~oenaOfsurveys forthe detection, .geographical distribution Intervention and preventive measures can be tak~~~ronutrrent defiCienCies so that appropriate
In collaboration with the Ministries of A ri It . Production and consumption of fruits a;d ~~ ure, Education and Health it is planned to promote the green fOOds and domesticated and wild ani~et~~I~r an~ anrmal produ~ts (both cultivated and wild health education through nutrition and he Ith as. .IS a so planned to Intensify food, nutrition and Ministry of Education with the ob' r a
f agencies, the agricultural extension services and the
diets. Jec Ives 0 promoting the consumption of adequate and balanced
71

REFERENCES S d Khartoum Survey Dept. Report
Culwick, G.M. (1951). Diets in the Gezira Irrigated Area, u an.
No. 304. I ICN 1992 FAOIWHO (1992). Nutrition, the GIOba(~ ~~~}I a~~~r;tiona; evalu'ation of diets in Gezira and Managil. Khattab, A.G.H. and EI Hadan, A.M. . .
Sudan Notes and Records. 50, 161-1}9~. t'f al evaluation of diets in the Nuba Mountains, Khattab. A.G.H. and EI Hadan,A.M. (1972. u n 1~~3
Sudan. Sudan Notes and Records. 53, 119~ Khartoum (1988-1992). Nutritional assessment National Nutrition Department, MInistry of Hea t 88-1992. . .
reports in different states of the Sudan, ~~I 1990-1991). MSF (Belgium) report on vitamin C Nutritional Anaemia Records, Khartoum Hosg (1989 National Plan of Action for Nutrition -
as deficiency, South Darfur, Nyala amp . Sudan, Khartoum, 1995.
72
AVAILABILITY OF MICRONUTRIENTS
IN JORDANIAN DIET
INTRODUCTION
Salma K. Tukan
Department of Nutrition and Food Technology Faculty of Agriculture, University of Jordan
Amman - Jordan
mw
Deficiency of micronutrients is common in many parts of the world. It has been estimated that between 5-10 million children die every year as a result of xerophthalmia due to vitamin A deficiency; it has also been reported that mild deficiency of this vitamin can lead to an increase in child mortality rate for those between 6 months and 6 years (UNICEF, 1993).
In the Near East region, anaemia, vitamin A deficiency and iodine deficiency disorders are reported to be common in many countries (Osman, 1992). However, little information is available on the prevalence or the etiology of such deficiencies.
Studies on nutrients deficiencies mainly focused on the clinical and lor biochemical signs of the diseases or disorders, which means studies took place at an advanced stage of the deficiency. This could lead to irreversible damage, and make intervention costly and slow. Recently, attention to hidden malnutrition is being focused upon as the number of those who suffer from it greatly exceeds that of those who suffer from severe deficiency. This is evident regarding energy malnutrition; whereas only 1-2% of children under 5 in developing countries suffer from severe malnutrition in which deficiency symptoms and signs appear, however, about 190 million were estimated to be undernourished and suffer from poor health and slow growth rate but without deficiency signs (UNICEF, 1994). Such persons are often considered healthy since it is difficult to detect hidden malnutrition.
Although the body can adjust to the low intake of micro nutrients, this might be accompanied with physical, mental and behavioral changes that are usually neglected by health workers, the parents or the individual himself, or attributed to other factors. Studies have shown that iron deficiency with or without anaemia is associated with abnormalities in mental performance and unhapiness behaviour which improve with treatment with iron (Addy, 1986). Further more, low blood level of micronutrients attibuted to low intake of some foods was related to increased incidence of cancer. The people of Linxian Country in China have one of the world's highest rates of esophageal/gastric cancer and at the same time they are known to have a low intake of several micronutrients (Blot et. al. 1993).
Information on the quantities of food available and the food pattern of the country as well as the adequacy of the food supply to meet the needs of the population, is necessary for food and ~ nutrition planning. It is especially useful for assessing energy and nutrients levels of the diet and their relationships with health. Such information may help in identifying nutritional problems and population groups at risk at an early stage, and guides in means of combating them.
This paper presents the supply and adequacy of energy, macro- and micronutrients in the diets of households in the various governorates of Jordan.
73
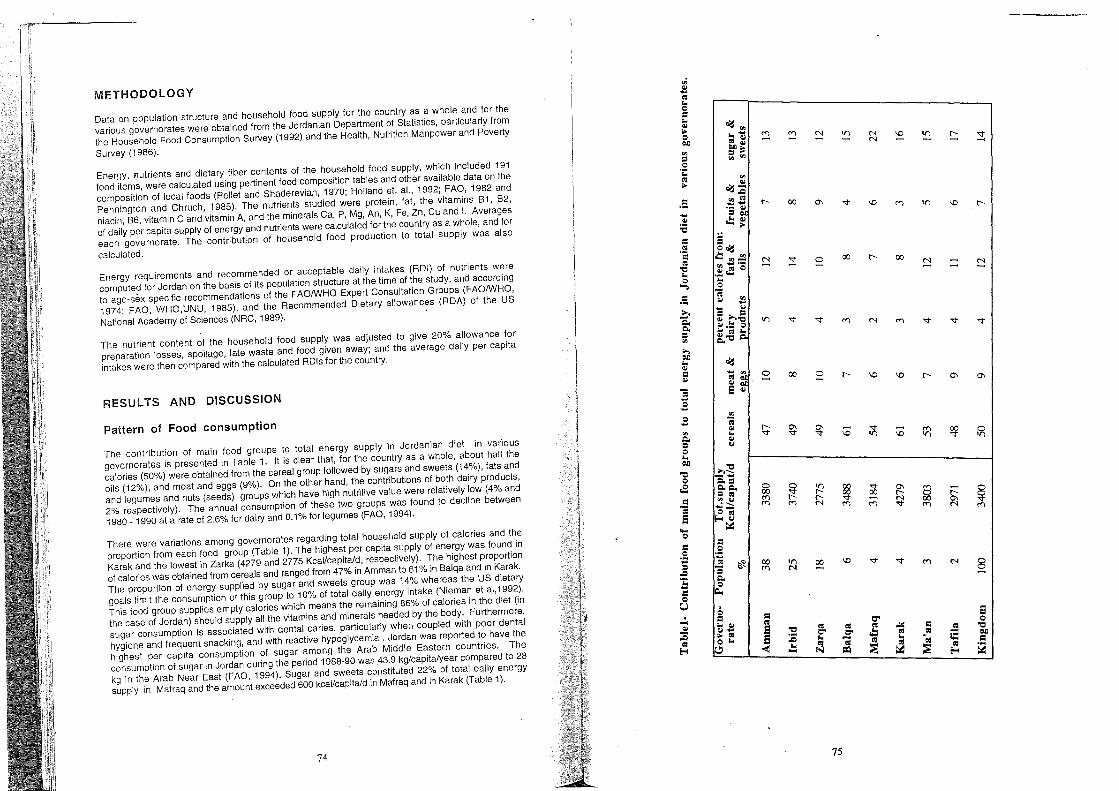
METHODOLOGY
Data on population structure and household food supply for the country as a whole and for the various governorates were obtained from the Jordanian Department of Statistics, particularly frqm the Household Food Consumption Survey (1992) and the Health, Nutrition Manpower and Poverty
Survey (1986).
Energy, nutrients and dietary fiber contents of the household food supply, which included 191 food items, were calculated using pertinent food composition tables and other available data on the composition of local foods (Pellet and Shaderevian, 1970; Holland et. aI., 1992; FAO, 1982 and Pennington and Chruch, 1985). The nutrients studied were protein, fat, the vitamins B1, B2, niacin, B6, vitamin C and vitamin A, and the minerals Ca, P, Mg, An, K, Fe, Zn, Cu and I. Averages of daily per capita supply of energy and nutrients were calculated for the country as a whole, and for each governorate. The contribution of household food production to total supply was also
calculated.
Energy requirements and recommended or acceptable daily intakes (RDI) of nutrients were computed for Jordan on the basis of its population structure at the time of the study, and according to age-sex specific recommendations of the FAOIWHO Expert Consultation Groups (FAOIWHO, 1974; FAO, WHO,UNU, 1985), and the Recommended Dietary allowances (RDA) of the US
National Academy of Sciences (NRC, 1989).
The nutrient content of the household food supply was adjusted to give 20% allowance for preparation losses, spoilage, late waste and food given away; and the average daily per capita intakes were then compared with the calculated RDls for the country.
RESULTS AND DISCUSSION
Pattern of Food consumption
I"he contribution of main food groups to total energy supply ·In Jordanian diet in various governorates is presented in Table 1. It is clear that, for the country as a whole, about half the calories (50%) were obtained from the cereal group followed by sugars and sweets (14%), fats and oils (12%), and meat and eggs (9%). On the other hand, the contributions of both dairy products, and legumes and nuts (seeds) groups which have high nutritive value were relatively low (4% and 2% respectively). The annual consumption of these two groups was found to decline between 1980 _ 1990 at a rate of 2.6% for dairy and 0.1% for legumes (FAO, 1994).
There were var"lations among governorates regarding total household supply of calories and the proportion from each food group (Table 1). The highest per capita supply of energy was found in Karak and the lowest in Zarka (4279 and 2775 Kcal/capitald, respectively). The highest proportion of calories was obtained from cereals and ranged from 47% in Amman to 61 % in Balqa and in Karak. The proportion of energy supplied by sugar and sweets group was 14% whereas the US dietary goals limit the consumption of this group to 10% of total daily energy intake (Nieman et al,1992). This food group supplies empty calories which means the remaining 86% of calories in the diet (in the case of Jordan) should supply all the vitamins and minerals needed by the body. Furthermore, sugar consumption is associated with dental caries, particularly when coupled with poor dental hygiene and frequent snacking, and with reactive hypoglycemia. Jordan was reported to have the highest per capita consumption of sugar among the Arab Middle Eastern countries. The consumption of sugar in Jordan during the period 1988-90 was 43.9 kg/capita/year compared to 28 kg in the Arab Near East (FAO, 1994). Sugar and sweets constituted 22% of total daily energy supply in Mafraq and the amount exceeded 600 kcallcapitald in Mafraq and in Karak (Table 1).
74
en .. -; .. c =: .. .. ;. c C/l
_5
;., C/l .. .. =: .. ] .B c .... '" c.. ::I C .. C/l
't:I C
oS =:
.OJ S .... c =: .s -= :5 b =: c U
=: .s -= "3 c.. c ~
Q =:
'" -; .. .. .. ...
.. .. ..... ;. CIS C ..
"
If"1
o -
00
'"
00
00
't:I :c .. -
N -
o 00
-\0
00 -
75
N N
N
00
-\0
If"1
If"1
N - N - - -
N

Contribution of food groups to nutrients and dietary fiber
Protein, fat and dietary fiber: The average daily per capita supply of protein for the country as a whole and in the different governorates is shown in Table 2. It ranged from 80 g/caput/d in Mafraq to 124 g in Karak, and the highest proportion came from cereals, followed by meat; while the contribution of dairy products was low for most regions especially in Tafila (47%).
Meat and eggs group supplied 52% of the fat, and the group of fats and oils supplied another 29% the average daily suply was 150g/capita/d for the country as a whole, and ranged from 107g in Mafraq to 170 g in Irbid.
The supply of dietary fiber was 34 g/capita/d for the kingdom, ranging from 29g in Zarka to 44 in Karak. Cereals supplied 63-84%, while vegetables supplied 8-22% of the total dietary fiber in the household supply.
Vitamins: The contribution of food groups to vitamins is shown in Tables 3 and 4. The average daily per capita supply of vitamin A (Table 3) ranged from 342 mg RE in Mafraq to 1009 in Irbid. Vegetables contributed over half of the vitamin (55% of the total) followed by meat and dairy products' groups (23% and 12% respectively). Over half of the vitamin contribution of dairy products came from Whole powdered milk. All brands of this type of milk available on the local market, are fortified with the vitamin. However, the contribution of vegetables to vitamin A is probably higher than the obtained value since data on the consumption of wild edible plants were not available, this was also reported by Takruri and Hamdan (1989).
Vitamin C supply ranged from 172 mg/capita/d in Irbid to 86 mg in Karak, and for the country as a whole, it was 150g. About two thirds of the vitamin was obtained from vegetables and one third from fruits.
The average daily per capita supply for thiamine (81) was 1.5 mg (Table 4) ranging from 1.3 mg in Zarka to 2.1 mg in Karak. Cereals, vegetables, and meat and eggs groups constituted 47%, 23% and 11 % of the total supply respectively. The average supply of riboflavin (82) for the country was similar to 81 (1.5 mg/capita/d) but lower in many regions. Meat, cereals, dairy products and vegetables groups supplied 28%, 21 %, 21 % and 17% of the total supply respectively. Niacin per capita supply ranged from 38 mg Niacin Equivalent (NE) in Zarqa to 67 mg NE in Karak, and the average for the country was 47 mg NE; most of the vitamin (44-67%) is derived from cereals. The supply of 81 in Amman and Irbid obtained in this study (1.5 and 1.7 mg, respectively) is much lower than what was obtained from a Similar previous study (2.3 mg and 3.0 mg, respectively) conducted in 1982. Average daily per capita supply for 86 was 2.9 mg with a large proportion de"rived from cereals (44-66%).
Minerals: The levels of the macrominerals Ca, P, Mg and K in the Jordanian diet are shown in •. Table 5. Average Ca supply was 797 mg/caput/d for the whole country with a range from 506 mg in Mafraq to 929 mg in Irbid. Ca supply obtained in this study for Amman and Irbid (831 and 929 mg/caput/day, respectively) are much higher than those obtained earlier by Tarkruri and Hamdan 1989 (about 647 and 547 mg/capita/d respectively). Most of the supply of Ca in this study came from plant origin indicating possible low absorption of this nutrient. The cereal group provided 31 %, dairy products 32%, and fruits and 24% vegetables of the total supply. Cereals were also the main source of P and Mg in the Jordanian diet (41% and 59%, respectively). Cere~ls and vegetables groups each supplied about one third of the supply of K (31% and 30% respectively), whereas fruits which are rich in this nutrient contributed only 9%. Consumption of fruits declined at a rate of 2.9% per year during the period 1980-1990 (FAO,1994).
76
Table 2- Contribution of food groups to protein, and fat in Jordanian diet governerates .
protein % from: Governo- Nutrient supply cereals meat & rate g/caput/d dairy fats &
eggs products oils
Amman protein 99 44 32 11 * fat 157 5 51 7 29
Irbid protein 105 48 28 9 fat 170 5 49 5 34
Zarqa protein 83 46 32 8 fat 128 5 55 5 25
Balqa protein 99 62 23 6 fat 114 7 56 5 26
Mafraq protein 80 60 25 5 fat 107 7 60 4 24
Karak protein 124 64 22 7 fat 143 8 56 6 26
Ma'an protein 108 53 26 11 fat 156 6 51 6 31
Tafila protein 90 47 34 9 fat 156 5 64 4 24
Kingdom protein 98 49 29 9 fat 150 6 52 4 29
* amount is negligible
77
according to
Total Calories
12
42
11
41
12
41
11
29
10
30
12
30
11
37
12
47
12
40

Table J - Contribution of main food groups to vitamin A in Jordanian diet according to governerates •
Governorate vitamin A % from:
J.Lg REI meat dairy fats fruits vegetables caput/d
&oils Amman 931 23 14 3 4 53
Irbed 1009 21 10 2 3 59
Zarqa 930 29 9 3 55
Balqa 520 12 16 2 3 62
Mafraq 342 16 16 4 5 53
Karak 549 29 21 4 3 37
Ma'an 939 32 13 7 2 41
Tafila 679 29 12 6 4 45
Kingdom 882 23 12 2 3 55
78
Table 4 - M.a~ foo~ groups contributing to daily per capita supply of Bl, B2, maclD eqUIvalent (NE) and B6 according to governorate in Jordan.
Governorate Vitamin Supply Cereals Meat Dairy Fruits Vegetables mg % % % % % Amman BI(mg) 1.5 44 13 5 6 4 B2 (mg) 1.6 19 30 17 6 20 NE(mg) 47.3 44 35 4 I 11 B6 (mg) 2.7 44 19 3 7 25 Irbid Bl(mg) 1.7 45 10 5 6 4 B2(mg) 1.7 20 26 23 6 17 NE(mg) 49.3 47 17 5 2 17 B6 (mg) 3.2 44 17 4 7 9 Zarqa Bl(mg) 1.3 41 12 4 6 28 B2 (mg) 1.3 20 30 17 6 20 NE(mg) 38.1 41 37 4 2 11 B6(mg) 2.5 40 20 3 7 25 Balqa Bl(mg) 1.6 65 8 3 3 15 B2 (mg) 1.2 30 26 21 4 15 NE(mg) 47.9 62 26 3 3 6 B6 (mg) 2.8 60 15 3 4 16 Mafrq Bl(mg) 1.2 58 9 3 4 19 B2 (mg) 1.0 29 24 18 5 17 NE(mg) 47.9 63 23 2 1 8 B6(mg) 2.7 54 15 2 4 22 Karak Bl(mg) 2.1 73 7 4 3 9 B2(mg) 1.4 32 27 23 3 10 NE(mg) 66.7 63 22 4 ..... * 4 B6(mg) 2.7 54 14 3 3 12 Ma'an Bl(mg) 1.6 52 II 6 5 17 B2 (mg) 1.5 23 26 25 5 14 NE(mg) 61.9 61 25 5 1 5 B6(mg) 3.0 51 18 4 5 17 Tafila B l(mg) 1.4 52 12 5 4 20 B2(mg) 1.3 21 31 22 5 16 NE(mg) 47.0 46 37 5 1 8 B6(mg 2.7 44 22 3 5 23 Kingdom Bl(mg) 1.5 47 11 5 5 23 B2(mg) 1.5 21 28 21 7 17 NE(mg) 47.3 48 33 5 1 8 B6(mg) 2.9 46 18 3 6 21
* amount is negligible
79

Table 5: Main food groups contributing to daily ° per capita supply of Ca, P, Mg and K according to governorate In Jordal!0
Governo- nutrient mg cereals meat dairy fruits vegetables rate % % % % % Amman Ca 797 31 5 32 4 20
P 1527 41 22 15 2 8 Mg 487 55 8 5 4 10 K 3129 29 17 5 10 30
Irbid Ca 929 30 5 32 4 23 P 1641 41 21 16 2 9
Mg 543 58 7 5 4 10 K 29 14 8 10 30
Zarqa Ca 703 32 5 26 4 24 P 1288 38 23 13 2 10
Mg 416 57 8 4 4 12 K 2870 28 15 4 9 34
Balqa Ca 650 40 5 30 3 16 P 1442 56 18 12 1 6
Mg 527 72 5 3 2 6 K 2528 40 15 5 7 27
Mafraq Ca 506 40 5 28 4 15 P 1222 53 18 10 1 8
Mg 424 69 6 3 3 9 K 2640 36 13 4 7 32
Karak Ca 661 35 6 37 3 11 P 1911 61 16 12 1 4
Mg 622 74 5 4 2 4 K 2900 47 15 4 6 21
Ma'an Ca 779 28 6 37 4 16 P 16% 46 19 17 I 6
Mg 552 63 7 5 3 7 K 3031 36 15 5 8 25
Tafila Ca 637 28 7 35 4 18 P 1431 43 24 15 I 8
Mg 423 59 9 5 3 10 K 2895 31 18 6 7 32
Kingdom Ca 797 31 5 32 4 20 P 1527 41 ~ 22 15 2 8
Mg 494 59 7 5 3 9 K 3104 31 15 6 9 30
80
Table 6 shows the levels of the micro minerals Fe, Zn, Cu and I in the Jordanian diet. The average daily per capita supply of Fe was 19 mg for the country as a whole, ranging from 14 mg in Mafraq to 21 mg in Irbid and in Karak. The proportions from cereals, meat and vegetables groups were 35%, 19% and 27%, respectively; and as the case of Ca, most of the sources of this mineral in the diet were from plant origin implying reduced absorption. As for Zn, the average daily per capita supply for the country as a whole was 15 mg. Values obtained for Amman and Irbid in this study (15 and 16 mg, respectively are higher than those obtained by Takruri and Hamdan (1989) (12.6 and 12.8 mg, respectively). More than half of the zinc supply (52-70%) came from cereals with a moderate contribution (14-24%) from meat and eggs. Similarly a large Proportion of Cu supply was provided from cereals-77%. As for iodine, table salt in Jordan was found to contain traces of the element (HKJ, Minstry of Health,1993), therefore, the contribution of this commodity was negligible. The average daily supply of iodine from food sources was 145 mg/capita/day for the country as a whole, ranging from 110 mg in Mafraq to 175 in Irbid. Cereals, meat and dairy products groups provided 40%,24% and 26% of the total supply respectively.
In general, the cereal group has been the most important in the Jordanian diet as in other countries of the region. It provided about half of the energy, protein, B1, niacin, B6, P, Mg, Zn and Cu. Vegetables provided more than half of vitamins A and C, and meat provided more than half of the fat supply. On the other hand, the contribution of dairy products, legumes and nuts can be generally considered low.
Geographical location did not seem to influence the pattern of food consumption, however, Karak which is located in the southern uplands had the highest supply of energy from cereals, while Irbid which is located in the northern uplands had the highest supply of energy from fats and oils, and fruits and vegetables. On the other hand, Amman governorate which is predominantly an urban area had the highest supply of energy from meat and dairy products. Ma'an which is in the arid region had the highest energy supply from dairy products
THE CONTRIBUTION OF HOUSEHOLD FOOD PRODUCTION TO TOTAL SUPPLY
Household food production is important for family food security and for improving the nutritional intake of household members. The contribution of household food production to total daily per capita energy and nutrients supply was generally very low for the country as a whole and in the various governorates. The highest contribution for the kingdom was 8% for fat and 7% for calcium. The contribution of household food production slightly exceeded 10% of the total supply for Ca and vitamin A in Balqa (10% and 12% respectively) and Mafraq (14% and 13% respectively, and for fat and Ca in Tafila (10% and 15% respectively). Dairy products were the main source of supply of these nutrients.
ADEQUACY OF ENERGY AND NUTRIENTS IN THE JORDANIAN DIET
The daily per capita energy and nutrients consumption were compared with the average calculated recommended daily intake (RDI) for Jordan (Table 7). The level of energy consumption usually reflects the adequacy of food intake while nutrient intake reflects the quality of the diet.
Energy: The diet covered 121 % of the daily needs of energy for the country as a whole, The consumption in Zarka was the lowest (99%) among the various governorates; the deficit could be even higher due to maldistribution of food within the household and the governorate. Energy intake in Tafila considered marginal and a deficit due to maldistribution is also suggested.
Government subsidization of foods, particularly of some cereals and sugar, has undoubtedly contributed to adequate energy intake, it could also contribute to overconsumption.
81

<Xl ...,
<Xl
'"
Table 6: Main food groups contributing to daily per capita supply of iron, zinc, copper and iodine in according to governorate in Jordan.
Fe* C M F V S Zn C M D V S Cu C M FIV S I C M Governo mg % % % % % mg % % % % % mg % % % % flg % % rate
Amman 19 33 21 5 27 9 15 52 24 8 6 5 2.4 60 14 10 9 145 38 27
Irbed 21 32 17 4 31 10 16 56 19 7 7 6 2.6 62 12 10 10 175 36 21
Zarqa 17 28 20 5 33 9 13 53 23 6 7 4 2.0 59 23 10 10 120 40 27
Balqa 16 52 16 3 18 7 15 70 15 5 4 3 2.5 76 9 5 5 132 53 21
Mafraq 14 53 14 3 20 5 12 65 15 5 7 3 2.0 71 10 8 5 110 52 19
Karak 21 62 15 2 10 5 18 72 14 6 3 3 3.1 77 9 4 5 148 54 23
Ma'an 19 45 19 4 17 9 14 57 19 9 5 6 2.5 63 13 7 9 149 43 25
Tafila 16 42 21 4 21 6 12 57 21 7 6 4 2.0 62 17 9 6 128 37 26
Kingdon 19 35 19 4 27 9 15 56 21 7 6 5 2.4 63 13 9 9 145 40 24
* C= cereals, M= meat, D= dairy products, F= fruits, V= vegetables, S= legumes & nuts
Table 7: Adequacy of energy and nutrients intakes for the kingdom and according to governorate.
Nutrient RDI kingdom Amman Irbid Zarka BaJqa Mafraq Karak Ma an Tafila ref.*
% energy 121 121 134 99 125 114 140 136 106 protein 145 147 156 123 146 118 183 160 133 fat 2 133 140 151 114 102 95 127 139 139 BI 1 102 99 114 87 107 82 143 104 94 B2 1,2 85 88 95 75 68 57 80 84 75 Niacin 1,2 253 252 263 203 255 255 355 330 251 B6 2 145 143 159 123 142 134 178 148 137 Vito A 1 132 142 153 141 79 52 83 143 103
2 88 93 101 93 52 34 55 94 68 Vito C 2 219 299 250 221 143 151 126 185 188 Ca lI8 123 137 104 96 75 98 115 94 2 67 69 78 59 54 42 55 65 53 P 2 137 140 147 116 129 110 247 152 128
lV!g 2 154 152 170 130 165 133 194 173 132 Na 3 154 163 179 119 155 102 137 154 137 K 2 ,_ 44 45 50 41 36 38 41 43 41 Fe 1 122 122 138 108 103 94 138 126 105 Zn 2 90 91 98 78 94 71 113 87 76 Cu 2 191 190 207 162 197 160 244 196 163 91 91 109 75 8.B 70 93 93 80
* Recommended dietary intake references are: I for FAO expert groups, 2 for RDA or other American recommendations.
--=-=--~- --~-~~-=-~~-=--~;::---'=:-=-=::.-~:~.~-==-- -~~~---
D %
24
32
20
20
20
16
24
26
26

Protien, fat, cholesterol and dietary fiber: The per capita protein consumption was generally adequate in all governorates, it ranged from 118% in Mafraq to 183% of RDI in Karak. As in the case of energy, governrnent subsidization of foods contributed to the adequacy of protein. In addition, the percent energy from protein (Table 2) was between 10-12% which is within the acceptable range (20).
As for fat, the Nutrition Cornmittee of the American Heart Association (Nieman,1992) has recommended that total fat intake should be less than 30% of total energy intake and cholesterol less than 1'00 mg/1000 kilocalories. Accordingly, fat intake in Jordanian diet exceeded RDI by more than 10% in all governorates except Balqa and Mafraq (102 and95% respectively). The proportion of calories frorn fat FCal% (Table 2) was higher than the recornmended one for the country as a whole (40%) and in all governorates except Balqa, Mafraq and Karak in which the proportion was within the acceptable range. High FCal% in the major three governorates (Amrnan, Irbld and Zarka) is probably linked with urbanization and vegetable oil production (In Irbid), whereas in Ma'an and Tafila it could be attributed to prevalence of a nomadic lifestyle. Cholesterol intake, on the other hand: was acceptable, it ranged from 42 mg/1000 Kcal/d in Mafrak to 80 rng in Amman.
The consumption of dietary fiber was adequate and higher than what had been rcommended by Williams (1993). The daily per capita consumption was 151% of RDI for the country as a whole. Dietary fiber is known to interfere with mineral absorption (Hazell, 1985), but data on maxirnum safe level of intake has not been established yet.
Vitamins: Regarding B1, the intake ranged from 82% in Mafraq to 143% of the RDI in Karak. The intake can be considered adequate in Irbid and Karak, and marginal or inadequate in the remaining regions. As for B2, the deficit is even higher as the intake constituted 95-75% of RD!. Low intake of dairy products contributed to the deficit Which could be even higher for household members who have poor preference to rnilk, or lactose intolerance. Cases of ariboflavinosis were reported among preschool children (UNICEF, 1992). On the other hand the consumption of niacin, B6 and vitamin C were adequate and exceeded the RD!.
On the basis of RDA, there was a deficit in the intake of vitamin A (34-101%) in all governorates, but on the basis of the FAO recommendations, there was a deficit in the intake of this nutrient in Balqa, Mafraq and Karak (79%, 52% and 83%, respectively), and marginal intake (103%) in Tafila. The intake of this vitamin is probably higher than what was obtained, as several edible plants rich In the vitamin such as vine leaves, mallow, garden rocket, garden cress, gundelia and other various Wild plants are consumed but information on supply was not available. Although vitamin A deficiency was not reported as a public health problem, it is possible that mild deficiency exists in some areas but it might not be detected nor documented.
Minerals: The RDI for P, Mg and Cu were adequate in all governorates (Table 7). Na consumptiol'}, on the other hand, exceeded the recommended intake by 10-80% except in Mafraq (102%). On the other hand, a deficit in the intakes of Ca, K, Fe and I were obtained In some governorates. Calcium intake for the country as a whole was 67% of RDI when compar~d With RDA, with a range from 53-78%, but it was 118% based on FAOIWHO values With a defiCit In Mafraq, Balqa and Karak (96%, 75% and 98% of RDI, respectively). and amarginal intake in Zarka (104%). Although drinking water in Jordan contributes to Ca Intake, the defiCit probably stili eXists as most of dietary calcium is derived from plant sources. Furthermore, Ca/P ratio was very low and did not exceed 0.6 implying adverse effects on the absorption of this mineral.
Studies on Ca status in Jordan are few, they mainly dealt with intake in Amman. In a recent study on a group of 39 obese female students aged 16-22 years, mean daily Ca intake was found to be 443 mg, it dropped to 369 mg after a weight reduction programme even though It was coupled With nutrition education (Qadri, 1995, unpublished). A stUdy on 80 pregnant women dUring the third trimester of pregnancy showed that their mean total daily intake of Ca was 717.5 mg of which 594
84
from dietary sources and the remaining amount was s~pplemental Ca (Shalbak,1993,unpublished).
Inadequate Ca intake is a risk factor for osteoporosis, which is more common in females than in. males. This disease is common in women after menopause,and it was reported to affect half of all the women over the. age of 45, and 90% of all the women over the age of 75 years (Thomson, 19~0). Modern techniques for early diagnosis of this disease, however, are still not widely used, while conventional X-ray method detects only severe bone loss (Thomson, 1990).
Regarding Na and K, no recommended intake has been established for these two minerals, however, the American Food and Nutrition Board (FNB) suggested 500 mg Na and 2,000 mg K as minimum requirements, and 3600 mg as desirable intake of K for healthy individuals aged 10 years and over (NRC, 1989). Accordingly the consumption of Na in Jordan which mainly comes from table salt, was more than 10 times higher than the minimum requirements, however the minimum recommended intake of Na for Jordanians is probably higher than the FNB recommendations due to prevalence of hot uncontrolled climatic conditions for the majority of the population for several months of the year. On the other hand, K intake was just above the minimum requirement in Balqa and Mafraq governorates (101 % and 106% respectively). The intake of K was much below the desirable level, it was 124% of the minimum requirement for the country as a whole, and was highest (140%) in Irbid governorate which also has the highest energy supply from fruits and vegetables. A Na/K ratio of 0.6 has been recommended to maintain normal blood pressure (Nieman, 1992). In thiS study the Na/K ratio obtained was much higher than the recommended on~, it was 2.0 for the country as a whole, and ranged from 1.6 in Mafraq to 2.5 in Balqa. These ratios are much higher than what was found in diets of adult Americans (less than 1.1) (Pennington 1986). '
The intake of Fe was 122% of RDI for the country as a whole, but it was low or marginal in Mafraq, Balqa, Tafila and Zarka governorates (Table 7). Some reports and studies, which were mostly conducted in Amman, have revealed the occurrence of deficiency of this micronutrient in Jordan among children, pregnant and non-pregnant women (Osman, 1992; UNICEF, 1992; FAO, 1994, Yip, 1990). The mean daily intake of dietary Fe of a group of 80 Jordanian pregnant women 16.2 mg and the total intake including supplements was 33.7 mg . Data also showed that 14% of the sample had low hemoglobin «10g/dl) and 18% were at marginal level (10.0-10.9g/dl)(Shalbak, 1993, unpublished). In this study, about 20% of Fe came from animal sources implying poor absorption. Poor Intake IS not the only factor contributing to Fe deficiency in Jordan, poor food habits and parasitic infections could also be contributing factors.
As for zinc, there was a deficit in the intake in all governorates except in Karak (113%), the average Intake for the country as a whole, was 90% of RDI. Data on the status of this micronutrient in Jordan are scarce, however, cases of acrodermatitis enteropathica have been reported in Jordanian hospitals, which responded to zinc supplementation. In two studies on Jordanian pregnant women, both Zn intake and serum level were low. In one. study mean daily consumption of Zinc of a group of 290 pregnant women was 7.3 mg and the meari serum zinc level was 66.9 mg/dl(Takruri, 1982, unpublished). In a more recent study on 80 pregnant Jordanian women, mean daily intake of Zn during the third trimester was 9.6 mg (65% of the RDA for that group) and mean serum Zinc was 60.7 mg/dl at the end of pregnancy (Shalbak, 1993. unpublished). Values below 68 mg/dl were considered low (Tuttle et. al. 1985). Poor absorption of this micronutrient is also expected as a large proportion (about 70% ) of it came from plant sources.
Similarly, the average intake of iodine was 91% O/RDI with a deficit in all governorates except in Irbid (109%). Iodine is considered a public health problem in Jordan; a recent report has shown the prevalence of goitre in school children aged 8-10 years to be about 38% (HKJ, Ministrty of Health, 1993).
85

THE NUTRIENT DENSITY OF THE JORDANIAN DIET
The nutrient, as percent of RDI, divided by energy, as percent of requirement,is the index of nutritional quality (INQ) (Hansen et. aI., 1979). This index is a good indicator of the quality of the diet in relation to both its energy content and the recommended intake. The diet is adequate if the index is 1 or more since, in this case, it supplies nutrients in the same proportion as energy needs; but if the index is below 1, the diet has a low nutrient density as it provides less nutrients than energy. Such diets, although adequate in energy, they can lead to deficiency diseases. Figure 1 gives the profile of Jordanian diet expressed as 100 INQ in comparison with the percent adequacy for selected nutrients. The index for Ca is below 1 although it is adequate when compared with RDI. This implies a decline in Ca intake is expected upon reducing food intake.
CONCLUSION AND RECOMMENDATIONS
The Jordanian diet was generally adequate in energy, protein, fat and dietary fiber. Fat intake was above the recommended level, it was 124% for the country as a whole, but cholesterol was within the suggested limits. The levels of fat and dietary fiber in the diet did not seem to have adverse effects on micronutrients availability. However, the diet was inadequate in B2, Zn, and iodine. Mafrak, Balqa and Tafila governorates had the highest nutrient deficits, while Amman and Irbid had the lowest. Low micronutrient intake is mainly attributed to the quality of diet rather than to total food intake which was generally adequate.
Food subsidisation is necessary for adequate energy supply, however, it should be modified to include more of the high nutrient density foods particularly from the dairy products group (to provide Ca, B2 and vitamin A) and legumes, but less of the low nutrient density foods, namely sugar. Furthermore, household production of fruits, vegetables and dairy products should be encouraged to supply these nutrients as well as potassium.
There is a need to increase awareness of policy makers regarding food and nutrition matters. Also, there is a need for well defined food and nutrition policies to ensure adequate food supply and subsequent balanced nutrition for all population groups and to avoid over consumption of food.
Nutrition intervention to improve the nutritional status of infants, children and women particularly from low socio-eonomic and low food availability areas, should be stressed and given priority. Increase in food availability for areas of deficient or low supply is required, particularly in Mafraq, Balqa, Zarka and Tafila governorates.
Foods rich in B2, Ca, Fe and Zn and vitamin A should be made available in all regions of the country, and their consumption should be encouraged particularly by children and women through nutrition education and feeding programmes. Iodized salt, should also be made available in all parts of the country.
Household food consumption data should be linked with clinical and / or biochemical data on nutrients for monitoring the nutritional status of Jordanians.
ACKNOWLEDGEMENTS
The author wishes to thank Mr.M Shunnak, Mr. Y.Hamdan and Mrs.M.Alkhas from the Jordanian Department of Statistics for their help in supplying the data, and Mr. S. Farhan from the Computer Center in the University of Jordan for data analysis.
86
REFERENCES
Addy, D.P. (1986). Happiness is : iron. British Medical Journal 292, 6526, 969-970. Blot W.J. et. al.(1983). Nutrition intervention trials in Linxian, China. Supplementation with specific
vitamin/minerai combinations, cancer incidence and disease-specific mortality in the general population, J. National Cancer Institute, 85, 1483 - 1492.
FAO (1982). Food Composition Tables for the Near East. Food and Nutrition paper no. 26. FAO, Rome.
FAO (1994). Changes in Food Consumption patterns in the Arab Middle East Countries. FAO Regional Office of the Near East, Cario. 1994.
FAOIWHO (1974). Handbook on Human Nutritional Requirements.FAO, Rome. FAOIWHO (1988). Requirements of vitamin A, Iron, Folate and Vitamin B12. Report of the jOint
FAOIWHO expert Consultation, Food and Nutrition Series No. 23, FAO, Rome. FAOIWHO/UNU(1985).Energy and Protein Requirements. Report of a joint FAOIWHO/UNU Expert
Consultation. WHO Tech. Rep.Ser. No.724, WHO, GeneVa. Hansen R., Wyse B.W. and Sorenson A.W (1979). Nutritional Quality Index of Foods. AVI
publishing Co., Westport. Hashemite Kingdom of Jordan, Ministry of Health, WHO and UNICEF(1993). Study on Iodine
Deficiency in Jordan (Preliminary Report), Amman. Hazel, T (1985). Minerals in Foods: Dietary sources, chemical forms, interactions, bioavailability.
Wid. Rev.Nutr.Diet. 46, 1 - 123. Holland, A.A. et. al.(1992). McCance and Widdowson's The Composition of Foods. 5th edition. The
. Royal SOciety of Chemistry and Ministry of Agriculture, Fisheries and Food. Cambridge, U.K National Research Council (1989). Recommended Dietary allowances. 10th edition, National
Academy Press, Washington, D.C. Nieman D.C., Butterworth D.E., and Nieman C.N (1992). Nutrition. Wm C. Brown Publishers,
Dubuque, USA. Osman, A.K (1992). Situation Analysis of Micronutrient Deficiencies (Vitamin A, Iodine, Iron) in
MENA Countries. Regional Over view 1. UNICEF Regional Office for the Middle East and North Africa Programme section, Amman.
Pellet, P.L. and Shadarevian, S (1970). Food Composition Tables for Use in the Middle East. American University of Beirut, Lebanon.
Pennington, JAT and Church, H.N (1985). Food values of Portions Commonly Used. 14th edition, Harper and Row, USA.
Pennington J.A.T. et.al.(1986). Mineral content of foods and total diets: The selected minerals in foods surveys. Journal of the American Dietetic Association, 876-891.
Takruri H.R. and Hamdan, M.R (1989). Food consumption pattern in the city of Arnman and Irbid District: vitamin and mineral intakes. UAE Journal of Agricultural Sciences. 1, 1-13.
Thomson, A.R (1990).Promoting the health of adults. In Kaufman, M. ed., Nutrition in Public Health. Aspen Publishers, Gaithersburg. 1990, pp. 192-193.
Tuttle S., aggett P.J., Campell D. and MacGillivray I. (1985). Zinc and copper nutrition in human pregnancy: a longitudinal study in normal primigravidae and in primigravidae at risk of delivering a growth retarded oaby. Am. J.Clin.Nutr.41, 1032-1041.
UNICEF (1992). Preliminary Report on the Assessment of the Nutritional Status of Preschool Children in Jordan. Amman.
UNICEF (1993). The State of the World's Children. New York. UNICEF (1993). The State of the World's Children, New York, 1994 Williams S.R.(1993) "Nutrition and Diet Therapy". Mosby, St. Louis, USA.YipR. el. al. (1990).
Report of the UNRWA Nutrition Survey of Palestinian Refugees in Gaza, Jordan, Lebanon, Syria, and the West Bank. UNRWA and EMROIWHO.
87
III b. Imnrovinn vit~min A ~t!=ltt I~ rQC:;lllt~ in r,:r.rlllr.inn th~ ric:;k" nf rT1nri.o.lit" hll 103;AoL
VITAMIN A IN NUTRITION AND ITS INTERACTION WITH OTHER NUTRIENTS
Hamed R. Takruri
Department of Nutrition and Food Technology, Faculty of Agriculture, University of Jordan, Amman, Jordan.
INTRODUCTION
Vitamin A is a fat-soluble vitamin which was the first to be identified early in this century (Moore, 1957). Although ocular symptoms of its deficiency, particularly night blindness, have known since antiquity, it is in this century that consequences of its deficiency in animals and humans were understood; poor growth, persistant infection, immune incompetence and dry eye (xerophthalmia) are known symptoms of vitamin A deficiel)cy (VAD) (Sommer, 1995).
The term vitamin A applies to several biologically active compounds which are of the preformed vitamin (retinol, dehydoretinol and many chemically related derivatives) and the provitamin A or carotenoids. Of over than 100 carotenoids, only 9 compounds have been found to have vitamin A activity, with B - carotene being the most potent of them (Moore, 1957; Pike and Brown, 1984).
Vitamin A deficiency was eliminated in wealthier countries through dietary intervention in the fourties, however, it is still one of the main health problems in developing countries, particularly in Africa, Asia, Western Pacific, the Caribbean countries, Central and South America and the Eastern Mediterranean (WHO / UNICEF, 1994). It is estimated that 118-190 million young children, 1-5 years old, live in areas of VAD (WHO /IVACG, 1992). It is estimated that 5-10 million will develop xerophthalmia annually with 250-500 thousand becoming blind. (Humphrey et aI., 1992; Sommer, 1995).
The rich food sources of preformed vitamin A are of animal origin and include liver (particularly fish liver), kidney, butter and egg yolk. The carotenoids, on the other hand, are obtained from foods of plant origin most important of which are dark green leafy vegetables, red palm oil, carrots and certain colored fruits.
PHYSIOLOGIC FUNCTIONS OF VITAMIN A
Carotenoids are absorbed and coverted to retinal then to retinol and esterified esters in the mucosal cells of small intestines.
The efficiency of conversion of B-carotene to retinol is 1/6 and that of other carotenids is 1/12. On the other hand, the absorption of retinol and its derivatives is much more complete and may reach 90%. However the bioavailability of both retinol and cartenoids depends on many factors and on interactions with other nutrients (Wise, 1980; Takruri, 1982).
Vitamin A, regardless of its sources, is transported after absorption and conversion to retinyl ester (mainly palmitate) via the lymphatic system and stored in the liver in the ester form to be mobilized from there upon need by peripheral tissues. It is mobilized from the liver as retinol attached to a protein synthesized in the liver named retinol-binding protein (RBP), which is further bound to another protein called transthyretin.
88
The most important functions of vitamin A are as follows:
1. Vitamin A is necessary for normal vision. Retinol and retinal prevent night blindness while retinoic acid does not (De Luca, 1978).
2. Vitamin A is necessary for reproductive functions. It is involved as retinol but not retinoic acid in reproductive actvities in the male where it is needed for spermatogenesis in males and in placental development and embryo development in females (Marks, 1980).
3. Cell membrane integration and cell differentiation. It seems that vitamin A is needed for the synthesis of specific glycoproteins which in turn act on RNA syhthesis and cell differentiation. It was found that vitamin A is needed for carrying mono-and oligo-saccharide units to an accepter site for the biosynthesis of glycoproteins situated in the cell membranes (De Luca and Wolf, 1970). It has also been postulated that vitamin A may be involved in electron transfer reactions in membranes (Sundaresan, 1972). Vitamin A deficiency is reflected in poor integration of epithelial tissues which renders them exposed to infection.
4. Normal growth: Since vitamin A has a role in cell integrity and membrane stability, its deficiency affects cell division and growth of growing animals.
5. Vitamin A seems to be necessary for the stability of membranes of mitochondria and Iysosomes.
6. There is quite good evidence that vitamin A, and particularly carotenoids, provide protection against cancer (Madani, 1995; Rohan et aI., 1993).
DEFICIENCY SYMPTOMS
Normal vitamin A status implies that an individual is free of symptoms and has sufficient stores to provide protection against metabolic demands in infection and stress. A normal well-nourished child has a serum level of 1.0-1.4 ~mol/liter (30-40 ~g/dl). Because vitamin A is stored, any vitamin A intake over needs is stored in the liver and thus it takes some time before hepatic stores of vitamin A are depleted (Sommer, 1995).
With continued VAD and/or low bioavailability of the vitamin, its hepatic stores become subnormal followed by reduced serum levels. Then a series of changes continue ending up with xeropthalmia and blindness which are accompanied by high mortalily anaemia, and reduced growth.
If the intake of vitamin A is so low that vitamin starts being depleted, the plasma level decreases. When the plasma level is <0.7 ~mol/L «20 ~g/dl) symptoms start to appear (Sommer, 1995). Severe symptoms, particularly frank ocular symptoms, may be manifested at levels of < 0.35 ~mol/L «10~g/dl) (Sommer, 1982).
The following are ciinical symptoms which develop in severely deficient persons (usually children 1-5 years old):
1. fletarded growth : The period needed depends on the stores in the liver and the rate of utilization of the vitamin and the dietary vitamin A ingested.
2. Abnormal spematogenesis in males and increased risk for abortion and still births in females with poor outcome of pregnancy including teratogenic developments.
89