microbubble-aided focus ultrasound disruption of the bbb
DESCRIPTION
ultrasoundTRANSCRIPT

Microbubble-Aided Focus Ultrasound Disruption of the
Blood–Brain Barrier in Assisting Drug Delivery for Alzheimer Treatment
Abstract
Blood-brain barrier(BBB) has been considered as a major impediment for drug
delivery for CNS diseases such as Parkinson's and Alzheimer's as well as the tumor
in brain. Many animal studies in the past few years have attempted using
microbubble-aided focus ultrasound to achieve BBB disruption(BBBD) to improve the
drug delivery and the uptake at specific target in brain, such as thalamus,
hippocampus or tumor.
However, even though there is enhancement for the drug delivery at the target,
there also accompanies with minor vasculature damage, extravasations near the
vicinity region, which somewhat indicates that the inertial cavitations of microbubble
within the capillary are difficult to avoid. The purpose of this proposal is to re-examine
and investigate some of the focus ultrasound parameter configurations as well as the
size and dosage of microbubble; thus, to develop an approach that achieves BBBD
for drug delivery for Alzheimer, but induced little damage in vasculature in brain and
along the Focused Ultrasound pathway.
Specific Aims
Ultrasound has been a very common medical imaging modality for decades. Not
only are its non-invasive and non-radiation favorable, but also the time-efficiency and
application diversities make it so popular. Focused Ultrasound is applicable in many
diagnostic and therapeutic areas; however, with different configurations of the sound
field and with the presence of microbubbles, minor or significant bioeffects can occur.
Therefore, the main purpose of this project is to examine how Focused Ultrasound
can be applied securely in assisting drug delivery for Alzheimer treatment.
The idea of using Focus Ultrasound in drug delivery for Alzheimer is by rapidly
oscillating microbubbles in the capillary near the target site, Hippocampus, so that the
vibration softens or loosens the Blood-Brain-Barrier(BBB); thus, allow the drug to
reach the target neuron. However, the most important thing we need to keep in mind
is that if Focus Ultrasound is not operated properly with extreme care, serious
bioeffects and damages such as hemolysis, capillary rupture and extravasations can
occur; especially in such a complex and ingenious organ, brain.
There two basic acoustic mechanisms when using Focus Ultrasound: Thermal
and Non-Thermal. Due to the fact that our goal is to deliver drug in the brain, the
thermal effect should be avoided or minimized as much as possible, which is our first

consideration prior to the treatment success.
Besides, there are different types for microbubbles oscillation such as rectified
diffusion, Stable Cavitations (Non-Inertial Cavitations) and Transient Cavitations
(Inertial Cavitations); whereas, Non-Inertial Cavitations is the appropriate mechanism
for the this drug delivery scenario, which allows microbubble to oscillate around its
equilibrium radius, no greater than twice of its initial radius. Also, one thing that needs
to be aware of is that even though the regular diagnostic ultrasound is used,
hemolysis can still occur when microbubbles are present. Thus, the specific goal of
this project is to determine the significant control parameters for Stable Cavitations,
and in turns to Disrupt the Blood-Brain-Barrier for Alzheimer drug delivery with
minimum temperature change and other bioeffects. The following are aims and
experiments that should be integrated to ensure the drug delivery to the target,
Hippocampus in brain.
Aim 1: Determine appropriate size and material for microbubble and its gas
core. Due to the natural restriction of the capillary size and the drug we want to deliver,
we cannot select a microbubble whose total diameter exceeding the diameter of the
capillary. Also, the initial radius, surface tension, gas core, adiabatic compressibility,
these microbubble's properties that contribute to its resonance frequency need to be
considered. And, the resonance is one of the major factors that determines the
thermal and cavitations mechanism.
Aim 2: Find out the some restricted indexes, threshold values, pulse width and
PRF. Indexes including Mechanical and Thermal Index, determined by the operating
pressure and frequency, minimize the thermal effects and restrict the selection of
pressure and frequency within a more secure range. Then, we need to find out, by
previous published literatures and graphs, with the pre-determined microbubble, its
radius and the blood's properties, what are the Pressure Threshold for Transient
Cavitations, which we want to keep away while operating Focus Ultrasound
accompanying with microbubbles. Also, we want to determine the maximum Pulse
Width and PRF that can be applied without inducing too much thermal increase.
Aim 3: Experiment for drug delivery. To observe whether Blood-Brain Barrier
Disruption(BBBD) can be achieved by the proposed Microbubble-Focus Ultrasound
(MB-FU) method, MRI contrast agents with large molecule weights can be
intravenous injected into a small animal, e.g. rats or rabbits after transcranial MB-FU
has been applied, where the focal point of the transcranial MB-FU from the head skull
will be aiming at Hippocampus area. Afterwards, the animal needs MR scan to
investigate how the large MRI contrast agents distribute and diffuse into the
Hippocampus region as well as estimate the time efficiency with respect to different
size, molecule weights of the contrast agents. Thus, a roughly estimate of the size of
drug might be obtained for the efficacious delivery.
After repeat Aim 3 in an adequate amount of trials, the molecular weight that can
penetrate BBB after the BBBD is known; thus, we can determine whether the drug for
Alzheimer's disease is capable of crossing the BBB, reaching the Hippocampus and
the surrounding neurons; thus, testify this project of using MB-FU to assist Alzheimer
treatment.
Background & Significance
Alzheimer Disease(AD), one of the most common neurodegenerative diseases
other than Parkinson's Disease and Huntington Disease, leads to high opportunity of
dementia from age 60, and currently affect 15.3 million people worldwide. However,
by this time, 2011, the genesis causes of Alzheimer Disease are still not well known;
not yet its thorough treatment. According to the most recent study, Alzheimer Disease
could be caused by the accumulation of misfolded protein, which penetrates the
neuron membrane and is harmful to partial of neuron's functions, such as growth,
survival and injury repair.
As stated above, AD is a complex disease so currently there is no complete
treatment for it, i.e. there is no active drug to cure AD. Most medication approved by
FDA are to help the patients maintain their mental functions, manage their normal
behaviors and delay the symptoms. Four FDA approved medications to treat
Alzheimer's are Donepezil, Rivastigmine, Galantamine and Memantine, but again,
these medications do not cure the disease; they only help maintain the current state of
the disease or delay the process.
Scientists and researchers have been striving to develop efficacious and efficient
pharmaceutical to regulate or cure Alzheimer's. Several medications such as -
secretase, -secretase, anti -amyloid antibodies, and siRNA have been developed
to be actively stop AD. However, even though these medications are believed to have
active cure for AD, one of the biggest challenge for treatment is the Blood-Brain
Barrier(BBB). Blood-Brain Barrier is a mechanism formulated by the endothelial cells
and tight junctions of capillaries in brain, which selectively allow small molecules such
as oxygen, hormones, carbon dioxide, glucose and molecular weight less than 400
Dalton to cross BBB and diffuse into cerebrospinal fluid; whereas, prevents large
molecules (MW>400) into cerebrospinal fluid. Under such circumstance, most drugs
or medications targeting to treat brain or neurodisease cannot effectively achieve their
efficacy because of the Blood-Brain Barrier.
The following shows diagrams to illustrate Blood-Brain Barrier.

[4] [5]
BBB prevents polar, less water-soluble and large (MW>400) molecules to reach neuron and CSF
In order to open the "door" for drugs, scientists discovered that Focused
Ultrasound accompanying with microbubbles may be used as a key or force to disrupt
the BBB. They claims that by rapidly oscillating the microbubbles in the capillaries, the
oscillation and collision will soften and loosen the BBB, and in turns allow larger
molecules, such as drug (MW>400), to cross or diffuse into the cerebrospinal fluid;
thus, reach the target site.
But, how can we generate the appropriate microbubble oscillation in brain
capillary to achieve BBB disruption (BBBD) without causing many bioeffects or tissue
damage?
Two basic types of microbubble oscillation can occur under a sound field: Stable
(non-inertial) Cavitation and Transient (inertial) Cavitation. The inertial cavitation
usually accompanies with microbubble collapse and generate very high collapse
pressure (10 to 107 MPa) and high temperature (5000 K), which are hazardous and
destructive to the tissues.
Studies[14] show that with presence of microbubble, under 1.15 MHz and 10 MPa
ultrasound sound field, around 4% hemolysis occured. In the same study shows that
the threshold pressure for hemolysis at 1.15 MHz while microbubble presence is
around 1.9 MPa negative pressure and 180 W/cm2 of Isppa.
Petechia is another bioeffect that might be caused by MB-FU. In the same
studies, it shows that with the dosage of 10 mL/kg of Albunex, and continuous wave
sound field of 1.09 MHz, 100s pulse exposure (10 us pulse duration, 1 ms PRP), the
number of Petechia was 30-fold increase compared with controls. Also, in other
experiments show that with the dosage of Optison, the threshold for abdominal
petechia was 0.64 MPa or 0.4 Mechanical Index (MI). Another study shows that with 1
MHz, 0.75 MPa pulsed ultrasound, capillary rupture in skeletal muscle occurred
during MB-FU scan. Thus, from these studies, it should be noticed that the
vasculature and tissue damage are easy to occur during MB-FU while lack of careful
attention of the sound field configurations and microbubble dosage.
Therefore, it is significant that we want to avoid the hemolysis and extravasations
during the BBBD by MB-FU operation. And, in this proposal, our specific focus is to

apply secure Ultrasound field and appropriate size as well as the dosage of
microbubbles to induce stable (non-inertial) cavitations in brain capillary for BBBD,
with minimum or no tissue damage.
Thus, the hypothesis for our experiment is that with the proposed ultrasound field
configurations and microbubble dosage, the BBB can be disrupted securely for
Alzheimer Drug delivery.
Experimental Design
In order to disrupt BBB securely, we want to induce Stable Cavitation in the brain
capillary. However, the sound field that induces any cavitation is highly dependent on
the microbubble's size, dosage and material properties. Therefore, we need to make
a presumption of using Optison® microbubble by GE. Some of the microbubbles'
parameter and manufacture suggested usage are listed below:
• Selection of Optison® by GE: Perflutren gas core.
• Mean Diameter Range: 3.0-4.5μm (max. 32.0μm)
• Recommended Dose: 0.5 mL.
• The injection rate should not exceed 1 mL per second.
• Follow the OPTISON injection with a flush of 0.9% Sodium Chloride Injection,
USP, or 5%, Dextrose Injection, USP.
• The maximum total dose should not exceed 5.0 mL in any 10 minute period
• The maximum total dose should not exceed 8.7 mL in any one patient study.
Once the microbubble is determined, we can start to calculate its resonance with
respect to different sound pressure. However, due to the fact that the microbubble is
injected intravenously, several biological coefficients also need to be considered:
• Ratio of specific heat of Perflurocarbon, _PFC=1.07.
• Surface tension of Blood, _blood = 56*10^-3 N/m.
• Surface tension of Serum Albumin in water, _SA= 50*10^-3 N/m.
• Surface tension of Serum Albumin in blood, _SAB = 53*10^-3 N/m.
• Density of Perflurocarbon = 1350 kg/m3.
• Sound speed in blood@37o = 1590 m/s.
And, by applying the equation proposed by Flynn:
[10]
, where b can be calculated by and , energy loss due

to radiation, viscosity and thermal respectively.
The above equation in adiabatic condition can be reduced to:
Then, we will be able to calculate the resonance of the microbubble, which we
want to keep away to avoid the Transient (inertial) Cavitation.
But, how do we know which sound field pressure to use for appropriate
resonance frequency and also minimize the bioeffects? As suggested from Duck[11],
to avoid transient cavitation while all range of microbubble present, Mechanical Index
(MI) less than 1 or smaller, less than 0.7, is recommended.
[11]
Also, according to APFEL&HOLLAND (1991), there is a threshold Pressure for
transient cavitation with respect to sound field driving frequency while all size
microbubble are present:
[12]
and, I also generated my own plot for the Pressure Threshold vs. Frequency in blood:
0 1 2 3 4 5 6 7 8 9 10
0
0.2
0.4
0.6
0.8
1
1.2
1.4Optimal Pressure Threshold for Inertia Cavitation for Blood
Frequency (MHz)
Thre
shol
d P
ress
ure
(MP
a)
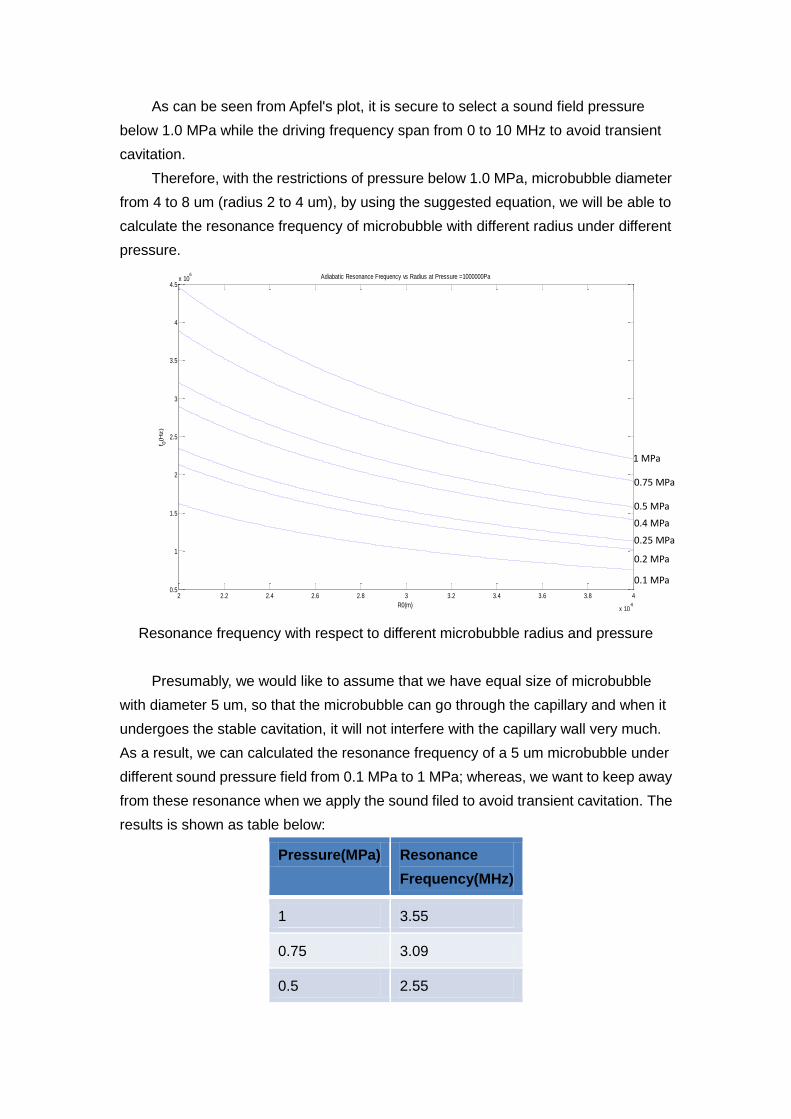
As can be seen from Apfel's plot, it is secure to select a sound field pressure
below 1.0 MPa while the driving frequency span from 0 to 10 MHz to avoid transient
cavitation.
Therefore, with the restrictions of pressure below 1.0 MPa, microbubble diameter
from 4 to 8 um (radius 2 to 4 um), by using the suggested equation, we will be able to
calculate the resonance frequency of microbubble with different radius under different
pressure.
Resonance frequency with respect to different microbubble radius and pressure
Presumably, we would like to assume that we have equal size of microbubble
with diameter 5 um, so that the microbubble can go through the capillary and when it
undergoes the stable cavitation, it will not interfere with the capillary wall very much.
As a result, we can calculated the resonance frequency of a 5 um microbubble under
different sound pressure field from 0.1 MPa to 1 MPa; whereas, we want to keep away
from these resonance when we apply the sound filed to avoid transient cavitation. The
results is shown as table below:
Pressure(MPa) Resonance
Frequency(MHz)
1 3.55
0.75 3.09
0.5 2.55
2 2.2 2.4 2.6 2.8 3 3.2 3.4 3.6 3.8 4
x 10-6
0.5
1
1.5
2
2.5
3
3.5
4
4.5x 10
6 Adiabatic Resonance Frequency vs Radius at Pressure =1000000Pa
R0(m)
f 0(H
z)
1 MPa
0.75 MPa
0.5 MPa
0.4 MPa
0.25 MPa
0.2 MPa
0.1 MPa

0.4 2.29
0.25 1.85
0.2 1.67
0.1 (1 bar) 1.25
Resonance Frequency of a 5um microbubble at different sound pressures
After calculated the resonance frequency with a given sound field pressure and
the selected microbubble size, we want to further determine which sound pressure is
appropriate for the BBBD. According to the Duck[11], some studies have shown that
even without the inertial cavitation, some bioeffects can still occur. According to
previous studies, the lowest continuous-wave intensity recorded for a detectable
bioeffect is 4mW/cm2, we would like to minimize our maximum intensity to 4mW/cm2.
And, according to
, we can calculate the maximum pressure for our sound field
to prevent the bioeffects while applying continuous wave to the microbubble in
capillary. Calculation:
As the result shows, the peak negative pressure is fairly low to be able to avoid
any bioeffect, so we would like to select our lowest calculated pressure to be for our
sound field, which is 0.1 MPa, 1 Bar and the corresponding frequency is 1.25 MHz.
According to Flynn's chapter in Physical Acoustic[10], the radius change of
microbubble under a sound field where the driving frequency is not equal to the
resonance frequency can be calculated by:
[10]
By using this equation, it allows us to see the relative radius change under different
frequency sound field with respect to time; thus, in turn to select the driving frequency
for our ultrasound configurations. The following shows several Radius-Time (R-T)
curves as results:
MPap
Pap
m
wp
m
wI
c
p
0116.0
72.11611
15901060240
402
2
2
2
2

The above figures show the relative radius change for a 5 um microbubble at 0.1
MPa with different driving frequency from 0.375MHz, 0.625 MHz, 1 MHz and 1.125
MHz.
Please recall from our resonance frequency look-up table that for a 5 um
microbubble at 0.1 MPa sound field, the resonance is 1.25 MHz. And, as we can see
from these figures, as long as the driving frequency is below 1.125 MHz, which is 0.9
of 1.25 MHz, the relative radius change is less than 2, which is in a secure stable
cavitation range. However, once the driving frequency rises and approach the
resonance frequency, 1.25 MHz, the relative radius change exceeds twice of its initial
radius, which certainly cross the threshold for the inertial cavitation.
Therefore, in our ultrasound configuration, we would like to select a driving
frequency equal or under 1 MHz for a 5 um microbubble and 0.1 MPa negative peak
pressure.
To summarize our assumption of microbubble and ultrasound configurations, we
assume that with a 5 um microbubble under a continuous wave sound field of 0.1
MPa at 1 MHz driving frequency, it will induce a quite secure stable cavitation in the
capillary for the BBBD.
In order to compare our sound field with some standard or concern of thermal
effect, Mechanical Index and Thermal Increase are calculated:
Given:
Optison® , 5.0-8.0x108/mL, 0.1 MPa (1 bar), f<=1MHz
Mechanical Inedx(MI)= = 0.1
1
1.0

And, the thermal increase:
where we can see that with MI as low as 0.1 and thermal increase per bubble equal to
5.59oC/s, our purpose seems to be in a very secure region to induce Stable Cavitation
with a little bioeffect or damage.
Once the microbubble and ultrasound configurations are determined, MRI
contrast agents can be used to testify our BBBD hypothesis.
First, one of the following MRI contrast agents may be chosen to intravenous
inject to a small animal after our MB-FU operation.
• MAGNEVIST – MW 469.01
• acid gadolinium - MW 547.57
• Gadodiamide – MW 591.672
The reason to choose MRI contrast agents for the first trial is that these agents
have molecular weight just right above the maximum molecular weight that can cross
the BBB. Therefore, if the BBB is not disrupted, these agents will not cross the BBB;
whereas, if the BBBD is achieved by our MB-FU, these agents will cross the BBB and
reach to our target, Hippocampus, and can be observed on the MRI T1-weighted
image; thus, in turns to prove our BBBD hypothesis.
Discussion
As mentioned in the end of the previous section, our BBBD can either be
success, which allow the contrast agents to reach the target site, or it can be fail so
that the contrast agents are still blocked out from the BBB and retained in the
capillary.
Case 1, Success:
If penetration of MRI contrast agents takes place successfully, that means the
BBBD by MB-FU is feasible and allow large molecule (MW>500) to cross the BBB.
However, we still don't know if our Alzheimer drugs such as - secretase, -
secretase, anti -amyloid antibodies or siRNA could also cross BBB. Thus, we would
slightly increase the injected molecule size to test what the up limit is for the
sCqkR
T
Rpq
RNRNNS
o
thvis
/5868.54
1
1012.9)(2
1890.0
105.210
1590107
2
22
.
5
0
2.
66
8

molecules to cross BBB once BBB has been disrupted. Then, we would know what
drug size will be suitable for this MB-FU treatment.
Case 2, Fail:
Fail means that we don't see any MRI contrast agents cross the BBB and reach
to the target site. This might indicate the energy or vibration of our stable cavitation is
not high enough to disrupt BBB. So, a suggestion is to increase the Mechanical Index
gradually, which means either increase the negative peak pressure or decrease the
driving frequency; however, the resonance frequency should always be kept away to
avoid the transient cavitation.
Besides, it is also very important to follow the threshold rule that the MI should
never exceed 0.5, which tremendously increases the chance for inertial cavitation.
Also, as long as the MI is increased in the case that negative peak pressure is
increased, one should be highly aware that the local intensity at the focus is increased
even more. Therefore, one the MI is increased, it is necessary to have a low PRF to
keep the Ispta as low as possible to avoid any excessive heating or bioeffects.
Comparison with Literature and Conclusion
My proposed MB-FU method and configuration is compared with one of the
literature that performs the in-vivo MB-FU BBBD experiments by N. MCDANNOLD et
al. [13], where it shows to disrupt BBB at a 2.04 MHz sound field, with just very low
negative peak pressure, the chance for BBBD to occur exceeds 50%. As shown in the
figure below:
[13]
This figure states that at 2.04 MHz, the threshold pressure for BBBD to occur is
around 0.69 MPa or roughly around 0.55 to 0.87 MPa. This means the minimum
Mechanical Index that can induce BBBD is around 0.21 and with MI=0.53 is definitely
sufficient for BBBD.
In fact, as one of their investigation shows, the BBBD threshold can be
represented in pressure and frequency dependant curve or represented in a MI but

frequency independent curve. The following figures illustrate the results:
[13]
The left figure indicates that to have BBBD occurred, the pressure is increased
as the US frequency increased. As we can compare from out proposal, if we select 1
MHz frequency with 0.1 MPa, the BBBD may have less chance to occur, but it should
be within a secure region. The right figure indicates that the BBBD's MI threshold is
independent from frequency, which means that as long as the MI reaches around
0.46, the BBBD can occur. This may reflect my suggestion of gradually increase the
MI of sound field for BBBD.
However, let's exam more about the safety issue, which is still out top priority
since we are operating the MB-FU in the brain capillary.
Undoubtedly, my proposal could be much safer than the literature because of my
low MI as 0.1. According to N. MCDANNOLD et al., even though the BBBD was
achieved by MI at 0.46, some damage such as extravasations and hemorrhage also
occurred. The following figures illustrate the number and the density of extravasations
which depends on the US frequency as soon as BBBD occurred.
[13]
As shown, in the figure at left, the number of extravasations decreases as US
frequency increases; whereas, the density of extravasations increases as the
frequency increases.
This indicates that once the BBBD occurred at low frequency sound field, many
extravasations can occur but spread out locally in the surrounding region; however, if
the BBBD occurs at high frequency field, even though less extravasations occur, but
they all accumulate or cluster together in a local area. Any bio or physiological effects
caused by either type of extravasations should be carefully examined and
investigated or further reduced or prevented before MB-FU BBBD can be applied in
clinical settings.

Reference
[1] NIH Senior Health: Alzheimer's Disease.
http://nihseniorhealth.gov/alzheimersdisease March 30th 2010
[2] Understanding Alzheimer's Disease. U.S Department of Health and Human
Services. National Institutes of Health. National Institute on Aging.
[3] Alzheimer's Disease Fact Sheet. Alzheimer's Disease Education &
Referral(ADEAR) Center. NIA. NIH. February 2010.
[4] Ben Best, “The Anatomical Basis of Mind “
[5] N. Joan Abbott, Lars Ronnback and Elisabeth Hansson. “Astrocyte–endothelial
interactions at the blood–brain barrier.” Nature Reviews. Neuroscience, Vol. 7,
January 2006.
[6] http://www.rxlist.com/optison-drug.htm
[7] E. HRNCIR, J. ROSINA. “Surface Tension of Blood”, Physiol. Res. 46 (4): 319-321,
1997
[8] D. R. Absoloma, b, c, C. J. Van Ossb, W. Zinggc, d and A. W. Neumann.
“Determination of surface tensions of proteins II. Surface tension of serum albumin,
altered at the protein-air interface .” Biochimica et Biophysica Acta (BBA) - Protein
Structure, Volume 670, Issue 1, 28 August 1981, Pages 74-78
[9] http://www.medsafe.govt.nz/profs/datasheet/d/Definityinj.htm
[10] H.G. FLYNN “Physics of Acoustic Cavitation in Liquids” Physical Acoustics,
MASON Vol. I PART B
[11] F A Duck, A C Baker and H C Starritt. “Ultrasound in Medicine.” p230-p231
[12] Robert E. Apfel, Christy K. Holland. “Gauging The Likelihood of Cavitation From
Short-Pulse, Low-Duty Cycle Diagnostic Ultrasound.” Ultrasound in Med. & Biol. Vol.
17, No. 2, pp. 179-185,1991
[13] NATHAN MCDANNOLD, NATALIA VYKHODTSEVA, and KULLERVO HYNYNEN
" BLOOD-BRAIN BARRIER DISRUPTION INDUCED BY FOCUSED ULTRASOUND
AND CIRCULATING PREFORMED MICROBUBBLES APPEARS TO BE
CHARACTERIZED BY THE MECHANICAL INDEX " Ultrasound in Med. & Biol., Vol.
34, No. 5, pp. 834–840, 2008
[14] Diane Dalecki. "WFUMB SAFETY SYMPOSIUM ON ECHO-CONTRAST
AGENTS: BIOEFFECTS OF ULTRASOUND CONTRAST AGENTS IN VIVO"
Ultrasound in Med. & Biol., Vol. 33, No. 2, pp. 205-213, 2007