microbiology, virology, immunology department. picornaviruses the name is derived from pico meaning...
TRANSCRIPT
Microbiology, virology, Microbiology, virology, immunology department immunology department

Picornaviruses
The name is derived from pico meaning small, and RNA referring to the ribonucleic acid genome,
so "picornavirus" literally means small RNA virus.
Electron Micrograph of Picornaviruses
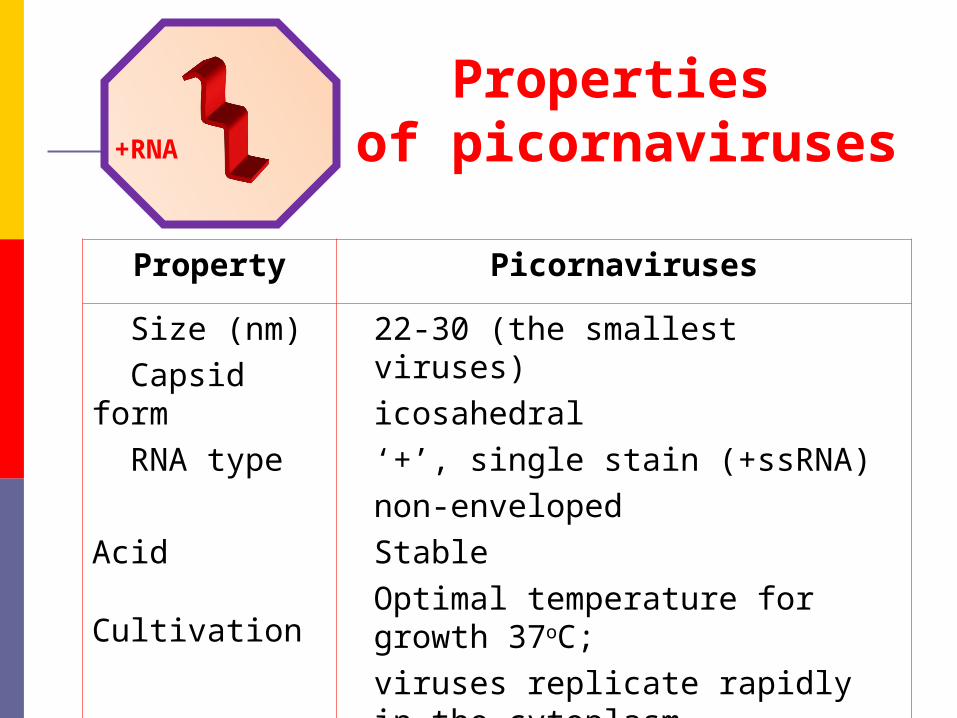
Properties of picornaviruses
Property Picornaviruses
Size (nm) Capsid form RNA type Acid Cultivation
22-30 (the smallest viruses)icosahedral ‘+’, single stain (+ssRNA)non-envelopedStableOptimal temperature for growth 37oC;viruses replicate rapidly in the cytoplasm
+RNA

Picornavirus Classification
o Picornaviruses are separated into nine distinct genera.
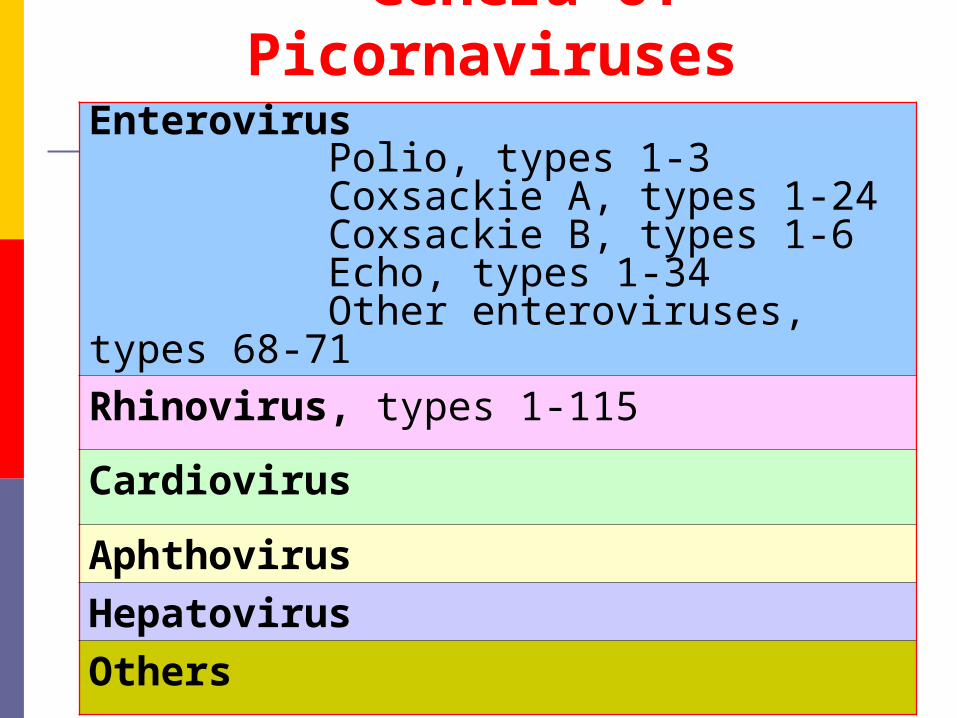
Genera of Picornaviruses
Enterovirus Polio, types 1-3 Coxsackie A, types 1-24 Coxsackie B, types 1-6 Echo, types 1-34 Other enteroviruses, types 68-71
Rhinovirus, types 1-115
Cardiovirus
Aphthovirus
Hepatovirus
Others
Picornavirus Classification
Three important to humans
EnterovirusesRhinovirusesHepatitis A Virus
Clinical manifestation of Enterovirus Infections
Aseptic meningitis Nonspecific febrile
illness Colds Conjunctivitis Pharyngitis Herpangina Hepatitis
Exanthems Encephalitis Paralytic polio Vomiting Diarrhea Pericarditis Myocarditis Hand-foot-mouth
syndrome

Enterovirus can replicate in epithelium of the nasopharynx and regional lymphoid tissue, conjunctiva, intestines, mesenteric nodes, and the reticuloendothelial system. Viremia may cause virus transfer to the spinal cord, brain, meninges, heart, liver, and skin. Some chronic enterovirus infections result in postviral fatigue syndrome.
Rhinoviruses infect and replicate mainly in nasopharyngeal epithelium and regional lymph nodes.
Pathogenesis of infections
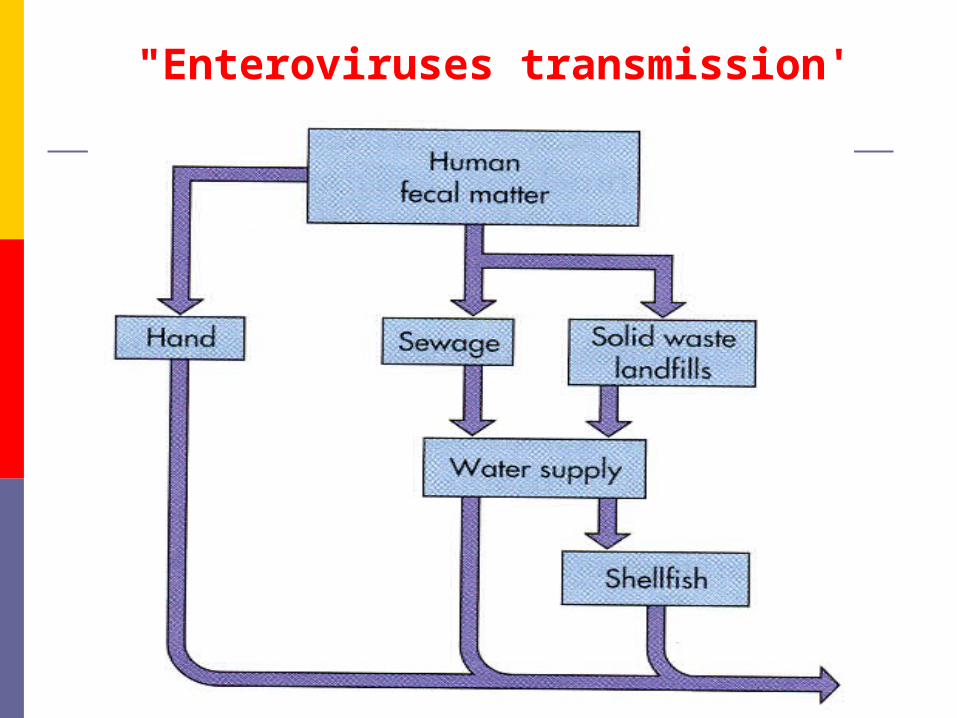
"Enteroviruses transmission'
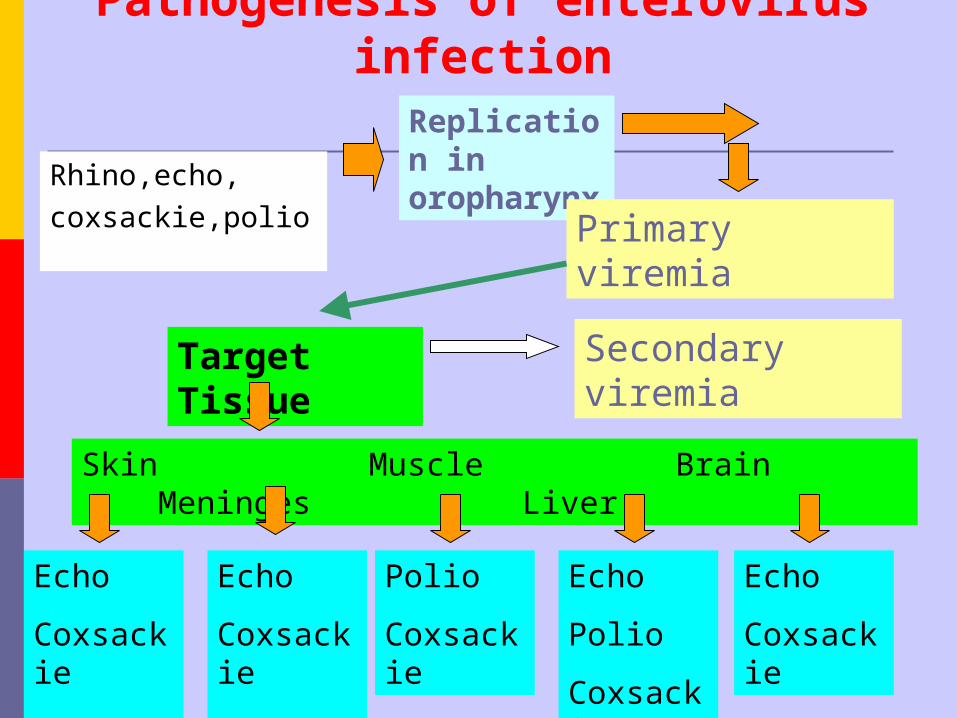
Pathogenesis of enterovirus infection
Rhino,echo,coxsackie,polio
Replication in oropharynx
Primary viremia
Target Tissue Secondary viremia
Skin Muscle Brain Meninges Liver
Echo
Coxsackie
A
Echo
Coxsackie
A, B
Polio
Coxsackie
Echo
Polio
Coxsackie
Echo
Coxsackie
POLIOVIRUS
HISTORICAL ASPECTS
Associated with man since ancient times
Jakob Heine (1840) – first medical report
Karl Oskar Medin (1890) – first epidemic
Karl Landsteiner (1909) – transmission of virus
Jonas Salk (1940s) – inactivated viral vaccine Sabin (1958) – oral vaccine
1949 – three serotypes
The virus is 30 nm in size and forms intranuclear inclusions. The virion is icosahedral and consists of a single sense-strand RNA and a protein capsid containing 32 spherical subunits (capsomeres).
This genome RNA serves as an mRNA and initiates the synthesis of virus macromolecules.
The poliomyelitis virus has neither an outer membrane nor lipids and is therefore not sensitive to the effect of ether and sodium desoxycholate.
Morphology.
Morphology.
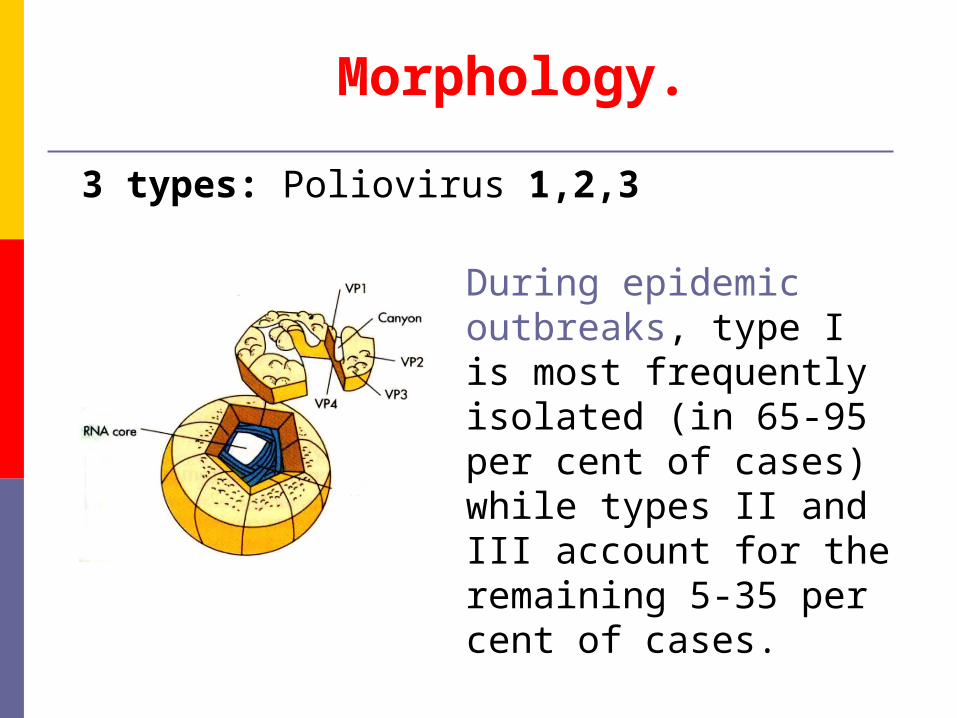
3 types: Poliovirus 1,2,3
During epidemic outbreaks, type I is most frequently isolated (in 65-95 per cent of cases) while types II and III account for the remaining 5-35 per cent of cases.

Poliomielitis virus

17
The Nobel Prize in Physiology or Medicine 1954
"for their discovery of the ability of poliomyelitis viruses to grow in cultures of various types of tissue"
John Franklin Thomas Huckle Frederick Chapman
Enders Weller Robbins
The poliomyelitis virus is cultivated on kidney cells of green African monkeys and on diploid human cells devoid of latent SV40 viruses.
The cytopathic effect (CPE) is attended by destruction and the formation of granules in the infected cells.
Cultivation. CPE.
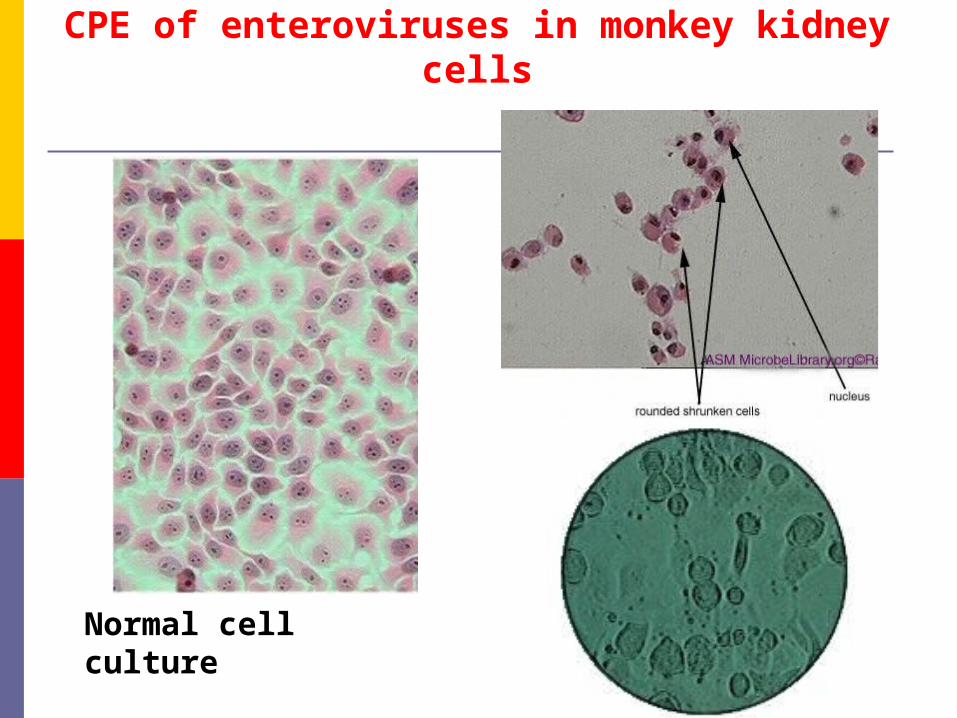
CPE of enteroviruses in monkey kidney cells
Normal cell culture

The virus is extremely resistant to photodynamic inactivation. It survives in sterile water at room temperature for a period of more than 100 days, in milk for 90 days, in faeces in the cold for more than 6 months, and in sewage for several months. It withstands exposure to 0.5-1 per cent phenol solutions and remains viable for several weeks at pH 3.8-8.5.
Resistance.
The poliomyelitis virus is sensitive to calcium chlorate lime, chloramine, formalin, potassium permanganate, and hydrogen peroxide solutions.
It is rapidly killed on boiling.
Resistance.

Poliomyelitis is an acute infectious disease that in its serious form affects the central nervous system. The destruction of motor neurons in the spinal cord results in flaccid paralysis (less than 0.1%). However, most poliovirus infections are subclinical.
Epidemiology
Natural infection occurs only in man.Source of infection: Apparent
and subclinical patientsIncubation: is usually 7-14 days,
but it may range from 3 to 35 days.

Transmission
Fecal – oral route: poor hygiene, dirty diapers (especially in day-care settings)
Ingestion via contaminated food and water Contact with infected hands Inhalation of infectious aerosols
Commoner in areas of poor sanitation
Pathogenesis -1
The mouth is the portal of entry of the virus.
Following ingestion, the virus multiplies in the oropharyngeal and intestinal mucosa.
Pathogenesis-2
The lymphatic system, in particular the tonsils and the Peyer's patches of the ileum, is invaded and the virus enters the blood resulting in a transient viremia.
The virus may be found in the blood of patients with abortive and nonparalytic poliomyelitis.
The central nervous system may then be invaded by way of the circulating blood.

Pathogenesis-3Poliovirus can spread along axons of
peripheral nerves to the central nervous system, and there it continues to progress along the fibers of the lower motor neurons to increasingly involve the spinal cord or the brain:
infects anterior horn cells of motor neurons in spinal cord causing flaccid paralysis.
infects brain causing tissue damage-affects breathing (bulbar polio)
Virus shed in feces
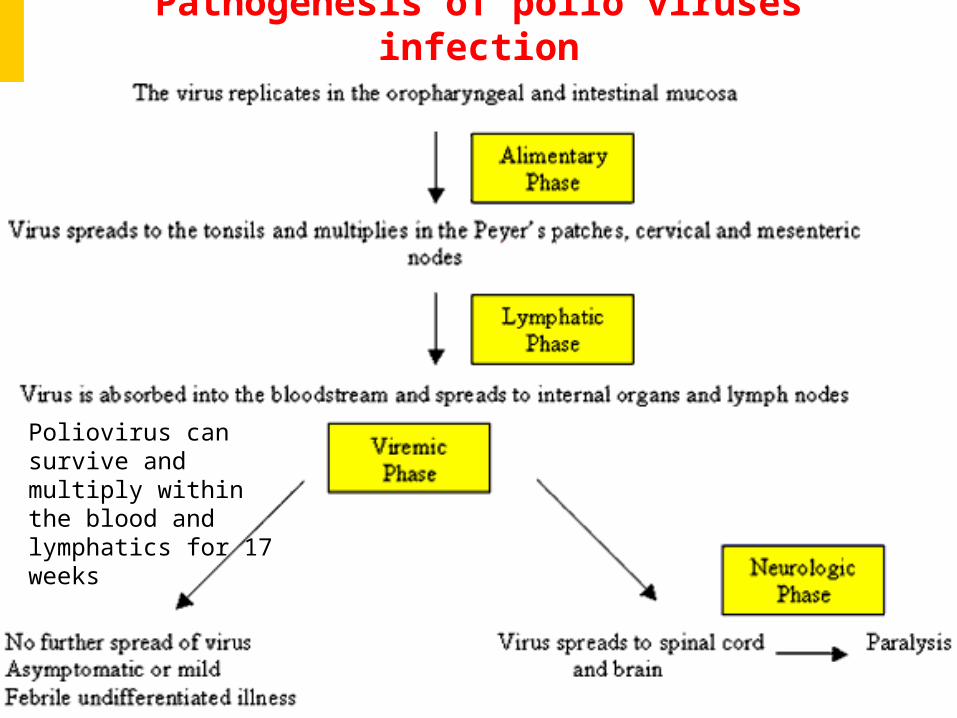
Pathogenesis of polio viruses infection
Poliovirus can survive and multiply within the blood and lymphatics for 17 weeks
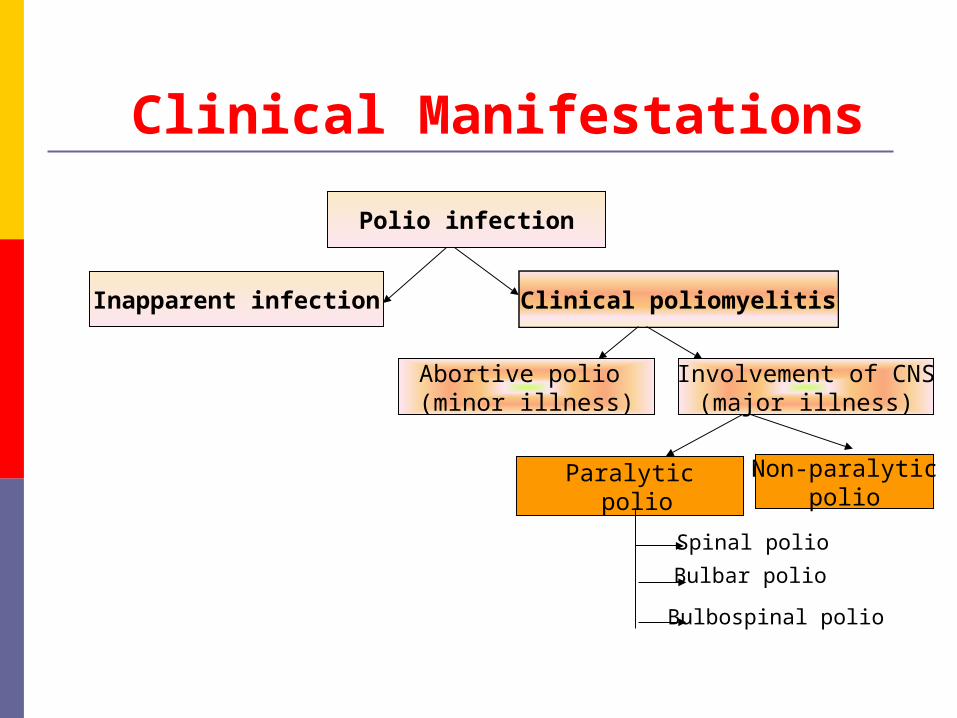
Polio infection
Inapparent infection Clinical poliomyelitis
Abortive polio (minor illness)
Involvement of CNS(major illness)
Paralytic polio
Non-paralyticpolio
Spinal polio
Bulbar polio
Bulbospinal polio
Clinical Manifestations
0 20 40 60 80 100
Percent
Asymptomatic Minor non-CNS illness
Aseptic menigitis Paralytic
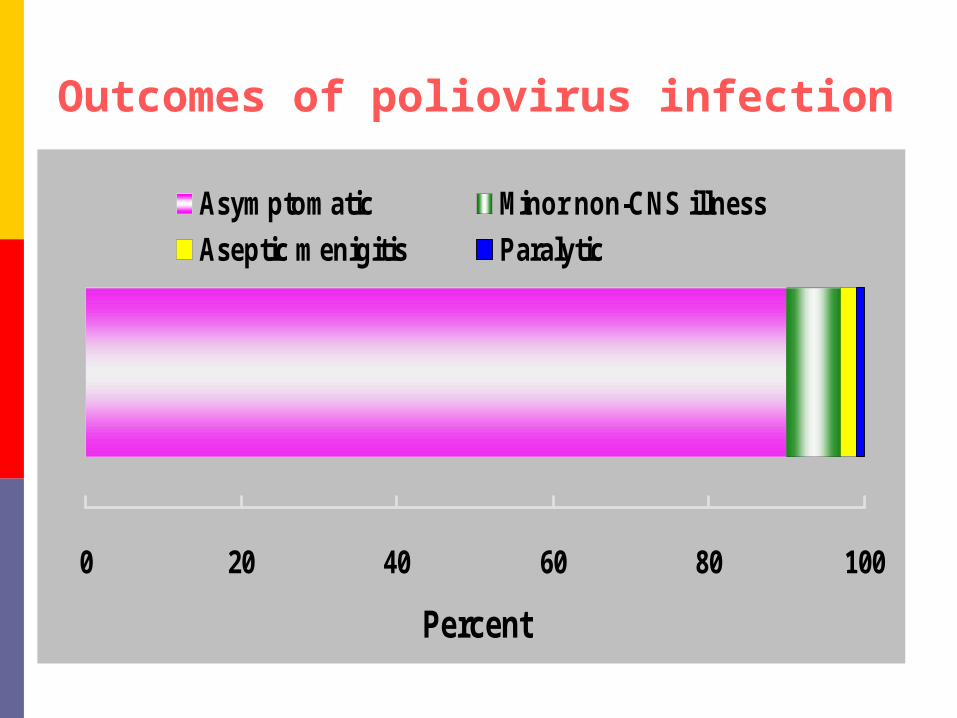
Outcomes of poliovirus infection

Clinical Manifestations
Asymptomatic (Subclinical) infection (90
- 95%) - inapparent subclinical infection
account for the vast majority of poliovirus
infections.

Clinical Manifestations
Abortive infection (4 - 8%) - a minor influenza-like illness occurs, characterized by fever, malaise, drowsiness, headache, nausea, vomiting, constipation, and sore throat in various combinations. Recovery occurs within a few days and the diagnosis can only be made by the laboratory.
Clinical ManifestationsMajor illness (1 - 2%) - the major illness
may present 2 - 3 days following the
minor illness or without any preceding
minor illness. Signs of aseptic meningitis
are common. Involvement of the anterior
horn cells lead to flaccid paralysis (0.1% to
2% of persons with poliovirus ). Involvement of the
medulla may lead to respiratory paralysis
and death.
resulting from lower motor neuron damage.
Spinal polio - 79% of paralytic cases;
Bulbospinal polio - 19% of paralytic cases;
Bulbar polio - 2% of paralytic cases
The maximal recovery usually occurs within 6 months, with residual paralysis lasting much longer.
Paralytic Poliomyelitis.

Egyptian stele from the 18th dynasty showing a victim of polio with a withered leg

Victims of paralytic polio
Muscle paralysis can sometimes result in skeletal deformities, tightening of the joints and movement disability.

Child with polio sequelae
Franklin D. Roosevelt Born in 1882 at Hyde Park, New York--now a
national historic site--he attended Harvard University and Columbia Law School. On St. Patrick's Day, 1905, he married Eleanor Roosevelt.
Following the example of his fifth cousin, President Theodore Roosevelt, whom he greatly admired, Franklin D. Roosevelt entered public service through politics, but as a Democrat. He won election to the New York Senate in 1910. President Wilson appointed him Assistant Secretary of the Navy, and he was the Democratic nominee for Vice President in 1920.
In the summer of 1921, when he was 39, disaster hit-he was stricken with poliomyelitis. Demonstrating indomitable courage, he fought to regain the use of his legs, particularly through swimming. At the 1924 Democratic Convention he dramatically appeared on crutches to nominate Alfred E. Smith as "the Happy Warrior." In 1928 Roosevelt became Governor of New York.
He was elected President in November 1932, to the first of four terms.

Polio afflicted everyone socially as well as medically Franklin Delano
Roosevelt “Once you’ve
spent two years trying to wiggle one toe, everything is in proportion.”—Franklin D. Roosevelt, 1945
http://americanhistory.si.edu/polio/howpolio/fdr.htm
Active immunity: Life-long, type-specific (is permanent to the type
causing the infection) Mechanism:
Local: sIgA are present in the tonsils and gastrointestinal tract, and are able to block virus replication;
Humoral: IgG and IgM can prevent the spread of the virus to motor neurons of the CNS.
Passive immunity: Maternal antibodies cross the placenta, and protect the infant from polio infection during the first 2-3 months of life.
ImmunityImmunity

Lab DiagnosisLab Diagnosis Definitive diagnosis is made by isolation of
the virus from stool, CFS, oropharyngeal secretions
Cell culture involves fibroblastic MRC-5 cells
CPE is usually evident within 36 hours Serotyping is based on neutralization of
CPE by standardized antisera using intersecting pool followed by specific sera.
ELISA IFA CFT

TreatmentTreatmentThere is no specific treatment. Treatment involves reduction of pain and muscle spasm and maintenance of respiration and hydration. When the fever subsides, early mobilization and active exercise are begun. There is no role for antiserum.
TreatmentTreatmentEarly injections of gamma-globulin, blood transfusion, wide use of vitamins C and B,-, amino acids (leucine, glutamic acid), analgesics (analgine, amidopyrine, pantopon, etc.), mediators, and stimulants (proserine, galanthamine, dibazol, etc.) are recommended.

TreatmentTreatmentAn orthopaedic regimen is set up from the first day that paralysis develops to prevent contractures and deformations, and exercise therapy is carried out during the rehabilitation period.
An apparatus for artificial respiration is employed when there are respiration disturbances.
PreventionNo specific antiviral therapy is available. However the disease may be prevented through
vaccination. There are two vaccines available.
oral polio vaccine (OPV live, attenuated , Sabin, 1957)
consists of live attenuated virus of all 3 serotypes
inactivated poliovirus vaccine (IPV, Salk, 1954)
consists of formalin inactivated virus of
all 3 poliovirus serotypes

Albert Sabin (1906-1993)
1958

Most countries use OPV because of its ability to induce local immunity and also it is much cheaper to produce than IPV.
OPV is used for the WHO poliovirus eradication campaign

Advantages and disadvantages of OPV
Advantages Effectiveness (The normal response rate to OPV is
close to 100%) Lifelong immunity Induces both systemic (IgG) and local (IgA)
immunity Induction of secretory antibody response
similar to that of natural infection Ease of administration Lack of need for repeated boosters Possibility of attenuated virus circulating in
community by spread to contacts (indirect immunization) (herd immunity)

Advantages and disadvantages of OPV
Disadvantages Can mutate to more virulent strain Unsafe administration for immunodeficient
patients Risk of vaccine-associated poliomyelites in
vaccine recipients or contacts Spread of vaccine to contacts without their
consent May be blocked if another enterovirus is
infecting a cells
Rarely causes paralytic poliomyelitis, around 1 in 3 million doses
Jonas Salk
1952

Advantages and disadvantages of IPV
AdvantagesAdvantages Cannot undergo genetic virulence.
Good stability during transport and in storage
Safe administration in immunodeficient patients
No risk of vaccine-related disease

Advantages and disadvantages of IPV
Disadvantages Lack of induction of local (gut) immunity Some lots had poor antigenic potency Need for booster vaccine for lifelong
immunity. Confers immunity only after 4 boosters
Requires parenteral administration. Fact that injection is more painful than oral administration
Expensive
Prevention Intramuscular Poliovirus Vaccine (IPV)
consists of formalin inactivated virus of all 3 poliovirus serotypes.
Produces serum antibodies (IgG) only: does not induce local immunity (IgA) and thus will not prevent local infection of the gut.
However, it will prevent paralytic poliomyelitis since viremia is essential for the pathogenesis of the disease.
Oral Poliovirus Vaccine (OPV) Consists of live attenuated virus of all 3 serotypes. Produces local immunity through the induction of
an IgA response as well as systemic immunity. Rarely causes paralytic poliomyelitis, around 1 in
3 million doses.

Polio cases have decreased by over 99% since 1988, from an estimated 350 000 cases then, to 1 349 reported cases in 2010. The reduction is the result of the global effort to eradicate the disease.
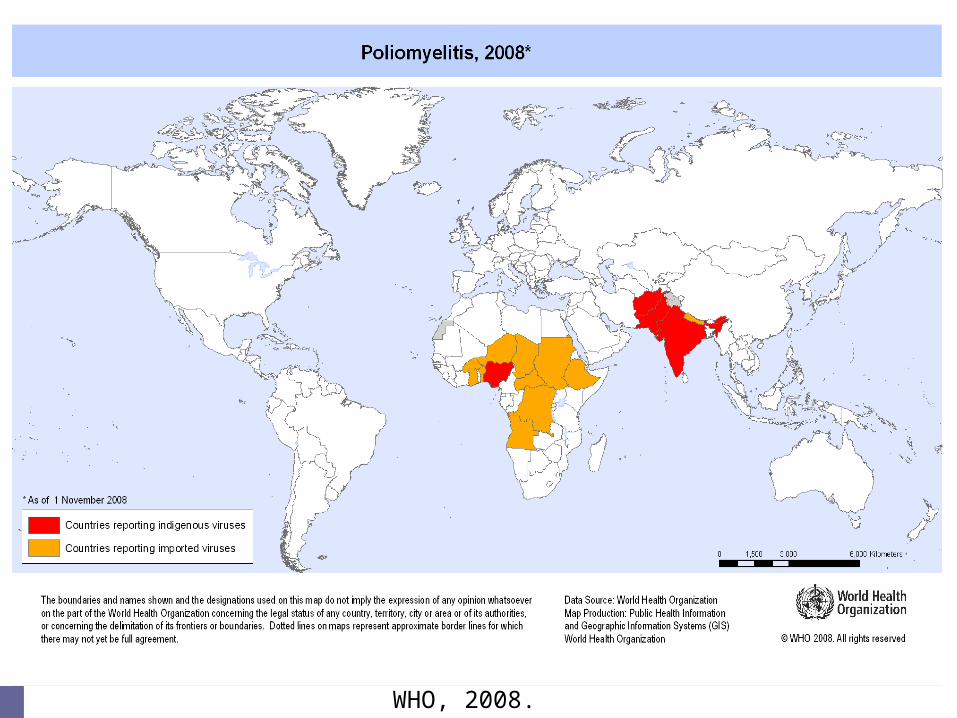
WHO, 2008.
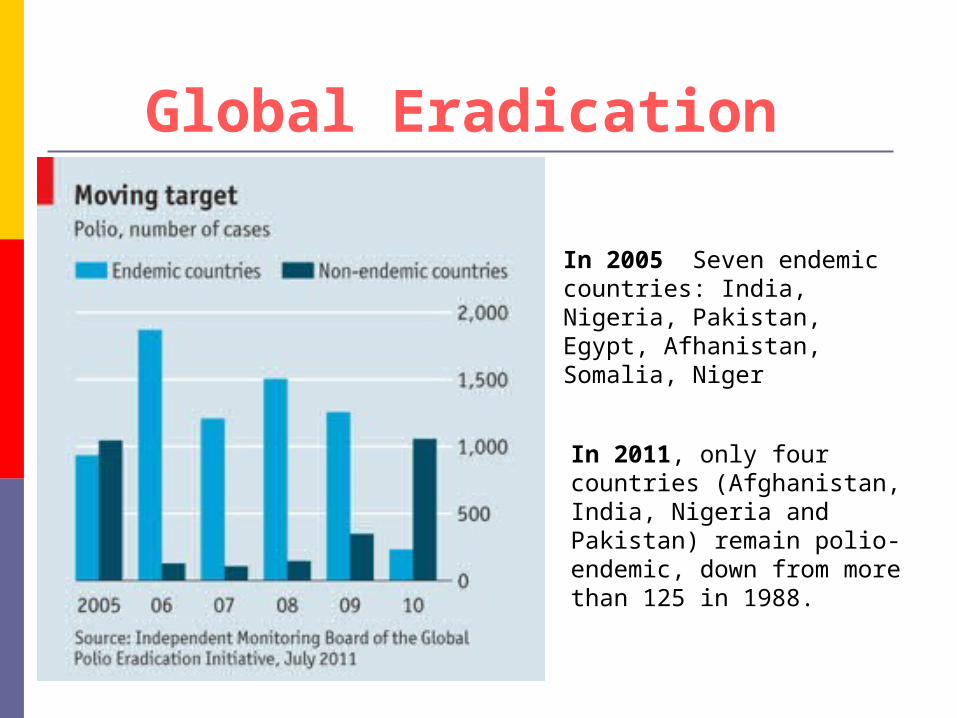
In 2005 Seven endemic countries: India, Nigeria, Pakistan, Egypt, Afhanistan, Somalia, Niger
In 2011, only four countries (Afghanistan, India, Nigeria and Pakistan) remain polio-endemic, down from more than 125 in 1988.
Global Eradication
Global Eradication in 2011
To the end of 2011 649 cases globally have been reported (wild poliovirus type 1 and type 3) from 16 countries (Pakistan, Afghanistan, Nigeria, Democratic Republic of Congo, Chad, Angola, Mali, Cote d'Ivoire, Burkina Faso, Niger and Gabon).
The WHO reported that in 2011 India had its first polio-free year and is therefore no longer considered polio-endemic.
The report of the 30 January - 01 February 2012 meeting of the Independent Monitoring Board (IMB) has been published. The IMB congratulates the Indian government. IMB is extremely concerned at the increase in polio transmission in Nigeria and Pakistan.
COXSACKIEVIRUSESCOXSACKIEVIRUSES
The coxsackieviruses comprise a large subgroup of the enteroviruses. They produce a variety of illnesses in human beings, including aseptic meningitis, herpangina, pleurodynia, hand, foot, and mouth disease, myo- and pericarditis, common colds, and possibly diabetes. Coxsackieviruses have been divided into 2 groups, A and B, having different pathogenic potentials for mice.

Group A viruses
produce widespread myositis in the skeletal muscles of newborn mice, resulting in flaccid paralysis without other observable lesions.
Group B viruses
may produce spasticity effect in sucking mice, focal myositis, encephalitis, and, most typically, necrotizing steatitis involving mainly fetal fat lobules.
Some B strains also produce pancreatitis, myocarditis, endocarditis, and hepatitis in both suckling and adult mice.
Normal adult mice tolerate infections with group B coxsackieviruses.

There is an abrupt onset of fever, sore throat, anorexia, dysphagia, vomiting, or abdominal pain.
Herpangina:
The pharynx is usually hyperaemic, and characteristic discrete vesicles occur on the anterior pillars of the fauces, the palate, uvula, tonsils, or tongue. The illness is self-limited and most frequent in small children.

Pleurodynia (Bornholm disease) Acute febrile illness Intense pleuritic pain Upper abdominal muscular pain CXR: Normal WBC: Normal or elevated myeloid cell
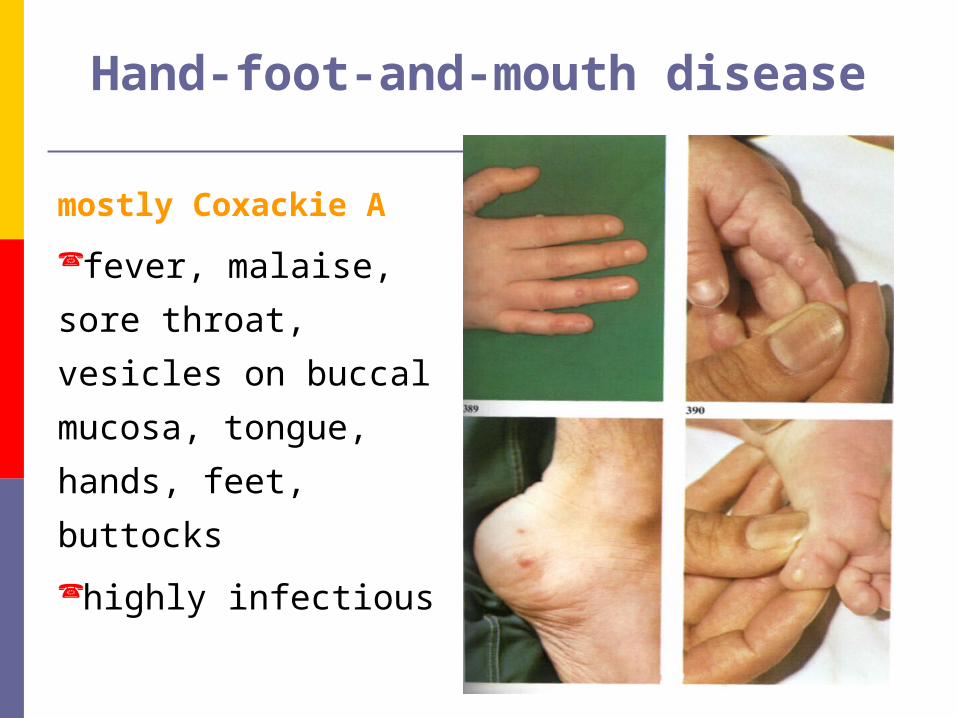
mostly Coxackie A
fever, malaise, sore
throat, vesicles on
bucсal mucosa,
tongue, hands, feet,
buttocks
highly infectious
Hand-foot-and-mouth disease

Hand-foot-and-mouth disease
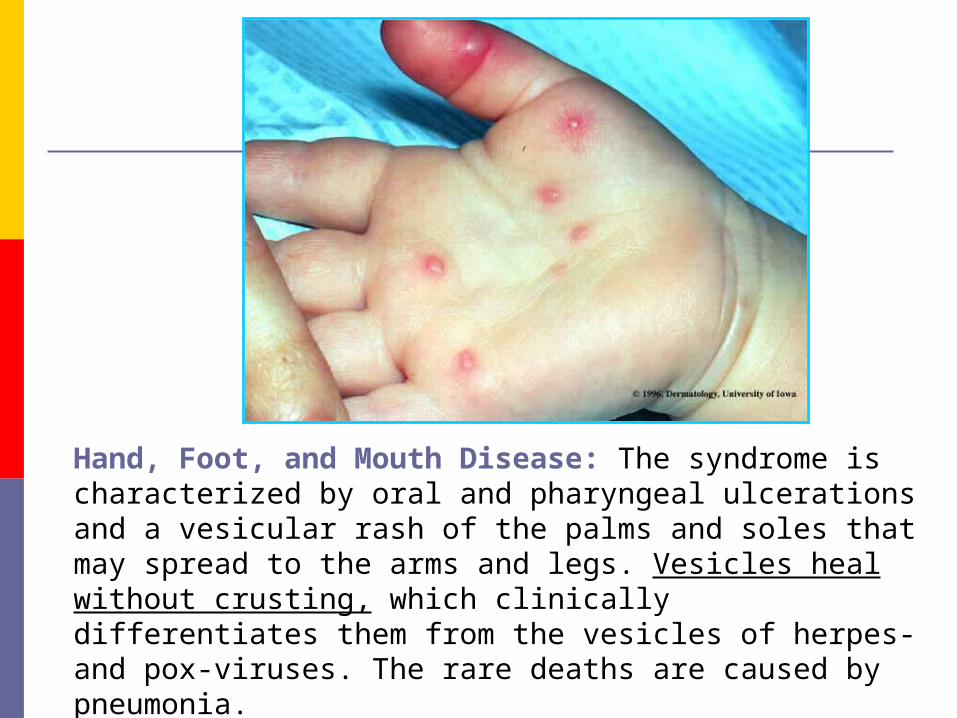
Hand, Foot, and Mouth Disease: The syndrome is characterized by oral and pharyngeal ulcerations and a vesicular rash of the palms and soles that may spread to the arms and legs. Vesicles heal without crusting, which clinically differentiates them from the vesicles of herpes- and pox-viruses. The rare deaths are caused by pneumonia.
The ECHOviruses (enteric cytopathogenic human orphan viruses) are grouped together because they infect the human enteric tract and because they can be recovered from humans only by inoculation of certain tissue cultures. Over 30 serotypes are known, but not all cause human illness.
Properties of the Viruses
General Properties. Echoviruses are typical enteroviruses measuring 24-30 nm.
ECHOVIRUSES

Important Characteristics Not produce diseases in sucking mice,
rabbits, or monkeys; Cause aseptic meningitis, infantile
diarrhea, febrile illnesses with or without rash, common colds, and acute hemorrhagic conjunctivitis
Monkey kidney and human embryonated kidney cell culture
Some also multiply in human amnion cells and cell lines such as HeLa.
Certain echoviruses agglutinate human group O erythrocytes. The hemagglutinins are associated with the infectious virus particle but are not affected by neuraminidase.
Initially, ECHOviruses were distinguished from Coxsackieviruses by their failure to produce pathologic changes in new-born mice.
Lab DiagnosisLab Diagnosis
but ECHOvirus-9 can produce paralysis in new-born mice. Conversely, strains of some Coxsackievirus types (especially A9) lack mouse pathogenicity and thus resemble echoviruses. This variability in biologic properties is the chief reason why new enteroviruses are no longer being subclassified as ECHO- or Coxsackieviruses,
Lab DiagnosisLab Diagnosis
The epidemiology of echoviruses is similar to that of other enteroviruses. They occur in all parts of the globe. Unlike the enterobacteria, which are constantly present in the intestinal tract, the enteroviruses produce only transitory infections.
They are more apt to be found in the young than in the old. In the temperate zone, infections occur chiefly in summer and autumn and are about 5 times more prevalent in children of lower income families than in those living in more favourable circumstances.
Epidemiology.
The pathogenesis of the alimentary infection is similar to that of the other enteroviruses.
Virus may be recovered from the throat and stools: in certain types (4, 5. 6, 9, 14) associated with aseptic meningitis, the virus has been recovered from the cerebrospinal fluid.
Pathogenesis & Pathology.

ECHOviruses 4, 6, 9, 11, 14, 16, 18, and others have been associated with aseptic meningitis.
Rashes are common in types 9, 16 ("Boston exanthem disease"), 18, and 4. Rashes are commonest in young children.
Occasionally, there is conjunctivitis, muscle weakness, and spasm (types 6,9, and others).
Infantile diarrhea may be associated with some types (e.g., 18, 20).
Clinical Findings.

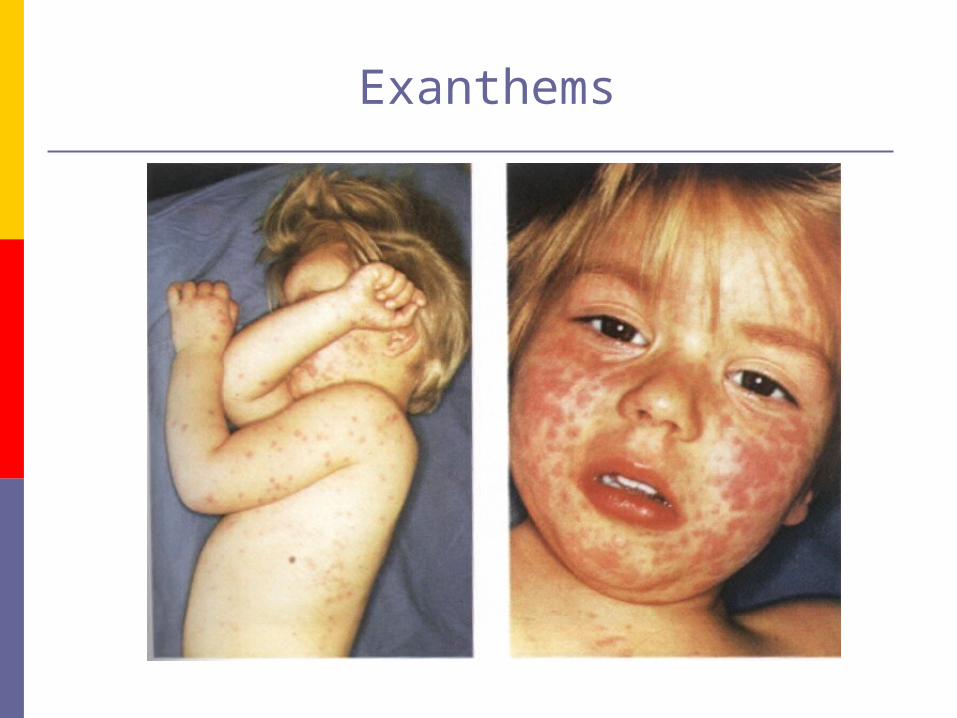
Exanthems

It is impossible in an individual case to diagnose an echovirus infection on clinical grounds. The diagnosis is dependent upon laboratory tests.
The procedure of choice is isolation of virus from throat swabs, stools, rectal swabs, and, in aseptic meningitis, cerebrospinal fluid.
If an agent is isolated in tissue culture, it is tested against different pools of antisera against enteroviruses. Determination of the type of virus present depends upon neutralization by a single serum. Infection with 2 or more enteroviruses may occur simultaneously.
Laboratory Diagnosis

Serologic tests are impractical — because of the many different virus types — unless a virus has been isolated from a patient or during an outbreak, of typical clinical illness. Nt and HI antibodies are type-specific and may persist for years. CF antibodies give many heterotypic responses.
Laboratory Diagnosis
Avoidance of contact with patients exhibiting acute febrile illness, especially those with a rash, is advisable for very young children.
Members of institutional staffs responsible for caring for infants should be tested to determine whether they are carriers of enteroviruses. This is particularly important during out breaks of diarrheal disease among infants.
Control.
Enterovirus 68 was isolated from the respiratory tracts of children with bronchiolitis or pneumonia.
Enterovirus 70 is the chief cause of acute hemorrhagic conjunctivitis. Acute hemorrhagic conjunctivitis has a sudden onset of subconjunctival hemorrhage ranging from small petechiae to large blotches covering the bulbar conjunctiva. There may also be epithelial keratitis and occasionally lumbar radiculomyelopathy. The disease is commonest in adults, with an incubation period of 1 day and a duration of 8-10 days. Complete recovery is the rule. The virus is highly communicable and spreads rapidly under crowded or unhygienic conditions. There is no effective treatment.
Other enterovirus types
Enterovirus 71 was isolated from patients with meningitis, encephalitis, and paralysis resembling poliomyelitis. It continues to be one of the main causes of central nervous system disease, sometimes fatal, around the world. In some areas, particularly in Japan and Sweden, the virus has caused outbreaks of hand, foot, and mouth disease.
Other enterovirus types
Rhinovirus most frequent cause of the common cold. In contrast to the other picornaviruses, the
rhinoviruses produce localized infections. Each serotype (>115) is distinct
not cross-reactive little cross-protection
more heat and acid labile than the enteroviruses.
Rhinovirus Pathogenesis
Transmission mainly by respiratory droplets; hand to hand transmission (via nasal
and ocular secretions). localized infections of the nose responsible for most cases of the
common cold. Symptoms occur 2 to 4 days after
exposure and last about one week. There is no fever.
The incubation period is brief,
from 2 to 4 days, the acute illness usually lasts for 7 days although a non-productive cough may persist for 2-3 weeks.
The average adult has 1-2 attacks each year.
Usual symptoms in adults include irritation in the upper respiratory tract, nasal discharge, headache, mild cough, malaise, and a chilly sensation. There is little or no fever.
Clinical Findings.
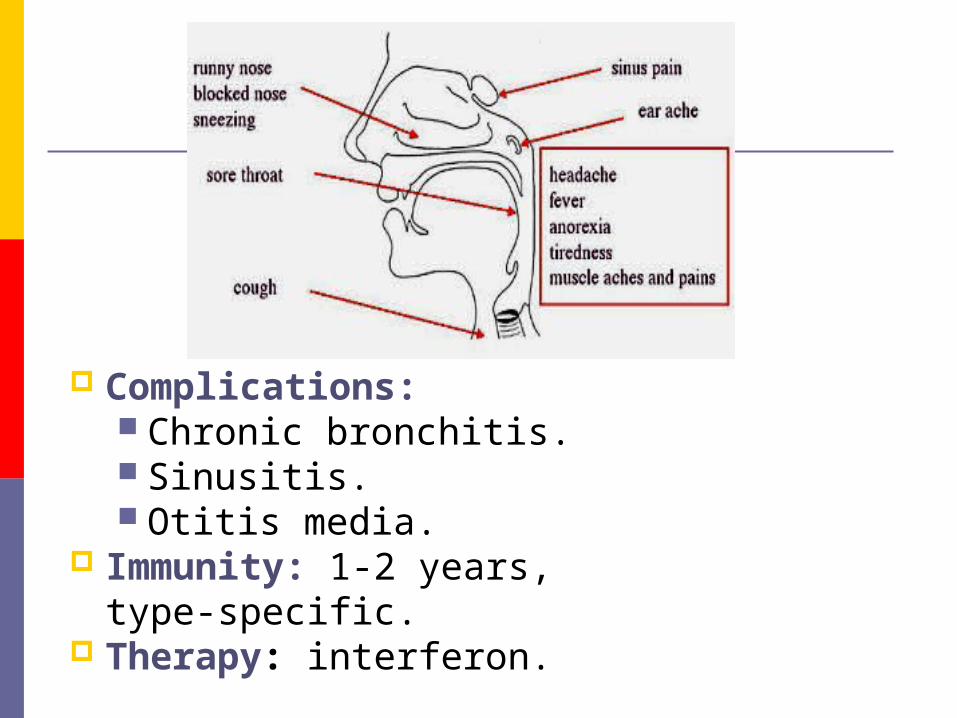
Complications: Chronic bronchitis. Sinusitis. Otitis media.
Immunity: 1-2 years, type-specific.
Therapy: interferon.
Laboratory diagnosis
Virus Isolation from nasopharyngeal secretions in cell culture Identification: NT, IF.
Serology: NT.

WISH WISH
UU
GREATGREAT
WEEKWEEK
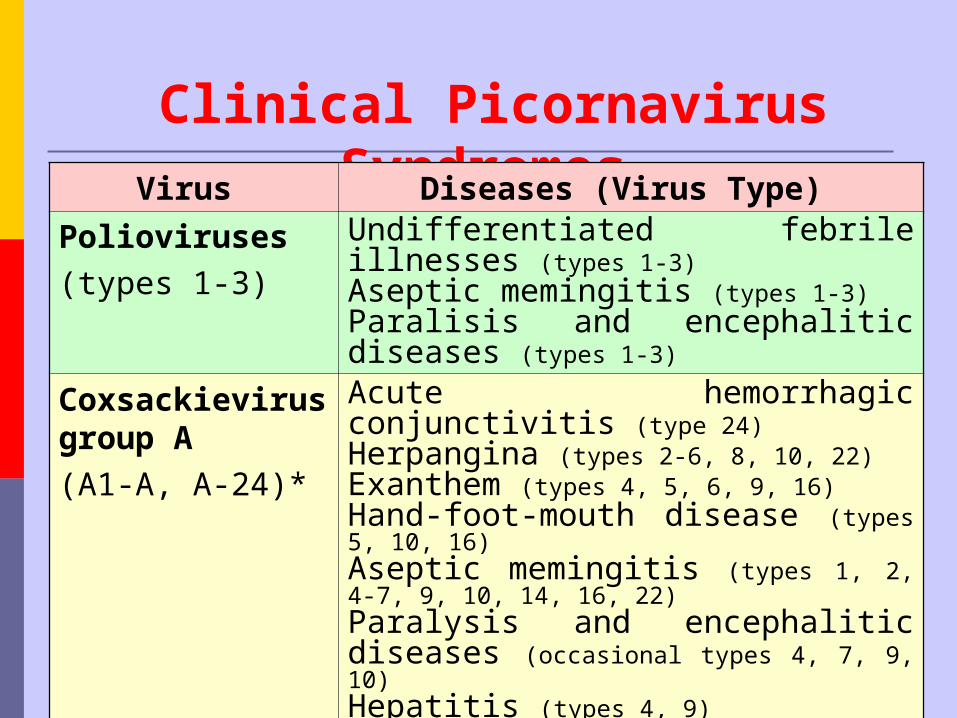
Clinical Picornavirus Syndromes Virus Diseases (Virus Type)
Polioviruses
(types 1-3)
Undifferentiated febrile illnesses (types 1-3)Aseptic memingitis (types 1-3)Paralisis and encephalitic diseases (types 1-3)
Coxsackievirus group A
(A1-A, A-24)*
Acute hemorrhagic conjunctivitis (type 24)Herpangina (types 2-6, 8, 10, 22)Exanthem (types 4, 5, 6, 9, 16)Hand-foot-mouth disease (types 5, 10, 16)Aseptic memingitis (types 1, 2, 4-7, 9, 10, 14, 16, 22)Paralysis and encephalitic diseases (occasional types 4, 7, 9, 10)Hepatitis (types 4, 9)

Virus Diseases (Virus Type)
Coxsackievirus group A (A1-A, A-24)*
Upper and lower respiratory illnesses (types 9, 10, 16, 21, 24) Lymphonodular pharyngitis (10)Infantile diarrhea (types 18, 20, 21, 22, 24 variant)Undifferentiated febrile illnesses (types 1-6)Pleurodinia (types 1-5)Pericarditis, myocarditis (types 1-5) Aseptic meningitis types (1-6)Paralysis and encephalitic diseases (occasional types 1-5)Severe systemic infection in infants, meningoencephalitis and myocarditis (types 1-5)Upper and lower respiratory illnesses (types 4, 5) Exanthem, hepatitis, diarrhea (types 5)

Virus Diseases (Virus Type)
Echoviruses (1-7, 9, 11, 29-33)*
Aseptic meningitis (many seroypes ) Paralysis and encephalitic diseases (occasional types 1, 2, 4, 6, 7, 9, 11, 14-16, 18, 22, 30)
Exanthem (types 1-9, 11, 14, 16, 18, 19, 25, 30, 32)
Hand-foot-mouth disease (19)
Pericarditis, myocarditis (types 1, 6, 9, 19, 22)
Upper and lower respiratory illnesses (types 4, 9, 11, 20, 22, 25)
Neanatal diarrhea (types 11, 14, 18, 20, 32)
Epidemic mialgia (types 1, 6, 9)
Hepatitis (types 4, 9)
Virus Diseases (Virus Type)
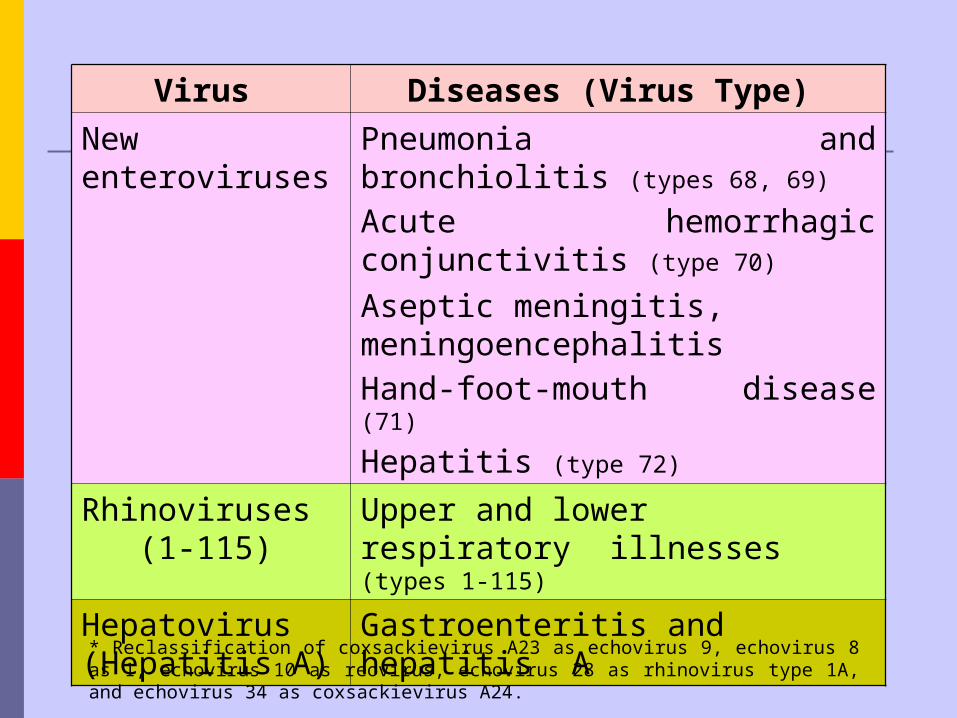
New enteroviruses
Pneumonia and bronchiolitis (types 68, 69)
Acute hemorrhagic conjunctivitis (type 70)
Aseptic meningitis, meningoencephalitisHand-foot-mouth disease (71)
Hepatitis (type 72)
Rhinoviruses (1-115)
Upper and lower respiratory illnesses (types 1-115)
Hepatovirus (Hepatitis A)
Gastroenteritis and hepatitis A
* Reclassification of coxsackievirus A23 as echovirus 9, echovirus 8 as 1, echovirus 10 as reovirus, echovirus 28 as rhinovirus type 1A, and echovirus 34 as coxsackievirus A24.