methodologies for vaccine safety surveillance - · pdf filemain design was a case-control...
TRANSCRIPT
Methodologies for vaccine safety surveillance
Nick Andrews, Statistics Unit
Public Health England October 2015

Some dramas of the past 20 years–which do you think turned out to be real adverse reactions?
MMR Autism
Aseptic Meningitis
Reduced Immunity / allergy
Rotavirus Vaccine
Intussusception
Flu vaccine
H1N1 Pandemic Vaccine Hep B
vaccine HPV vaccine
Narcolepsy
Guillane Barre Syndrome Type 1
Diabetes
Chronic Fatigue
Convulsions
Mercury in vaccines Neurological
problems
Asthma Exacerbation



Talk Overview • The components of vaccine safety surveillance • Epidemiological methods • Example and comparisons • Conclusions

Vaccine Safety Assessment Components
Vaccine Trials reactogenicity
Pharmacovigilance (passive/active): hypothesis generation, RAPID
Signal Strengthening/assessment
Epidemiological studies (hypothesis testing)
Individual causality assessment
Licensure and use
Priority?
Plausibility, other data/methods, experts, other risks, interval from vaccine,….
Passive Surveillance systems
• Often part of Pharmacovigilance by regulatory authorities
• Many countries have a system in place (UK Yellow Card)
• Reports from health professionals / public are monitored. e.g. by comparing rates to historical rates or other vaccines (proportional reporting ratios).
• Some countries (e.g. US VAERS system) have stimulated passive reporting –forms sent to all physicians for return

Active Surveillance example
–! Vaccine safety data link. Using data from US Health Maintenance Organisations
–! Rapid Cycle analysis – e.g .comparing observed convulsions 0-1 days post trivalent influenza vaccine to expected numbers each week based on histyorcial data. on histyorcial data.
Study by TSE et al, Vaccine 2012. Could look at many different outcomes this way
Signal strengthening • Signals may come from many sources – recent
example HPV and Guillane Barre Syndome from a French cohort study
• What can be done to rapidly assess a signal? – Go through the usual causality assessment steps – but
likely lots of missing information. WHO has guidelines. – Look at pharmacovigilance data (if that was not the
source of the signal). – Ecological studies – look in hospital / GP databases at
disease rates over time. – Observed v Expected studies within databases that
contain vaccination data where reporting bias is less likely. Ideally already be looking at possible events of interest in rapid cycle analysis.

Rapid Ecological study
of Guillane Barre Syndome and HPV
vaccine (done in a few days)
Hospitalisations for
GBS by age and period and whether vaccine
scheduled that year (red)
No increased risk seen
Epidemiological studies for Investigating adverse events
• Design issues – Exact question/vaccine/population, case
definition, timing relative to vaccination, confounders, how rare….
• Data sources – For cases, vaccination, confounders (?linkage)
• Methods – Cohort, case-control, case-coverage, case-only
(self controlled case series) – BEST ONE OFTEN DEPENDS ON DATA
SOURCES AND DESIGN ISSUES

Comparing designs: Example1: Rotavirus and Intussusception
• October 1998: an anti-rotavirus vaccine is launched in the USA for use in infants (3 doses).
• May 1999: the vaccination programme is suspended following 9 reports of intussusception temporally associated with vaccination.
• An epidemiological investigation is launched.
Main design was a case-control study
• 382 cases and 1657 controls, matched/controlled for sex, age, hospital of birth, proxies for socio-economic position.
• But control selection difficult – could there be residual confounding.
• So also considered just looking at all the cases (432 could be used) for the timing of any vaccines using self controlled case series.
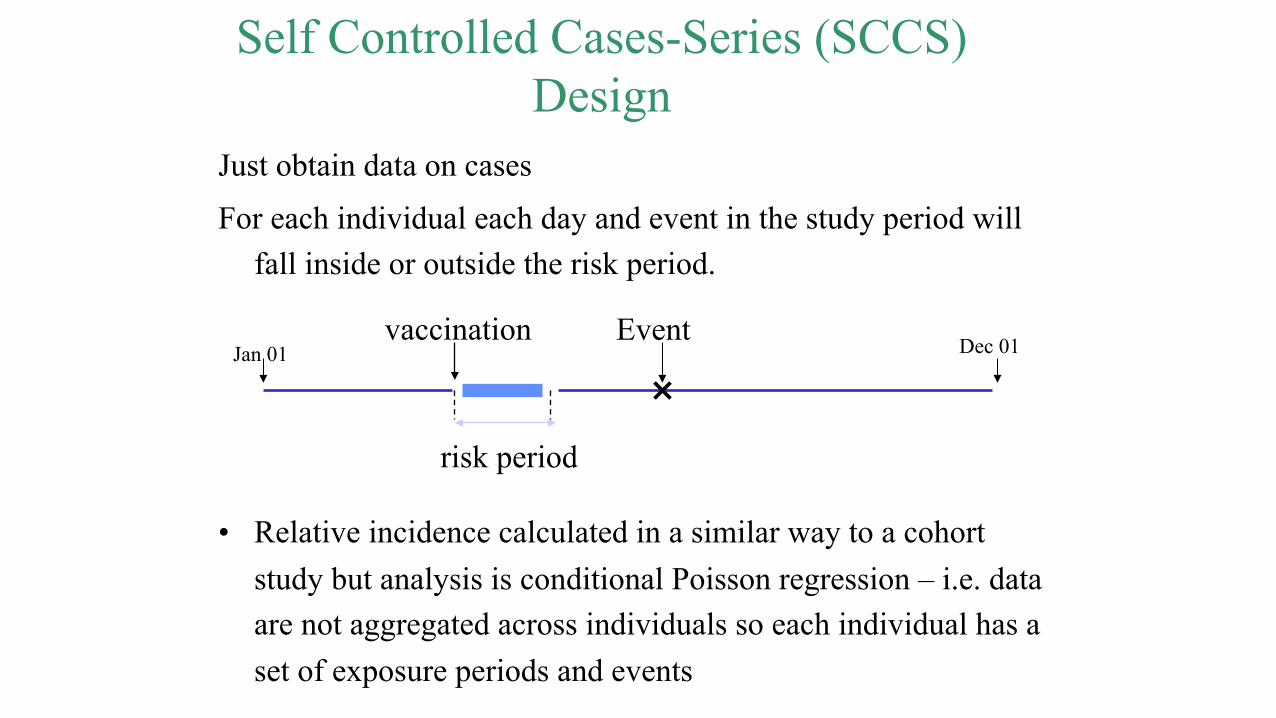
Self Controlled Cases-Series (SCCS) Design
Just obtain data on cases
For each individual each day and event in the study period will fall inside or outside the risk period.
• Relative incidence calculated in a similar way to a cohort study but analysis is conditional Poisson regression – i.e. data are not aggregated across individuals so each individual has a set of exposure periods and events
risk period
vaccination Jan 01 Dec 01 Event
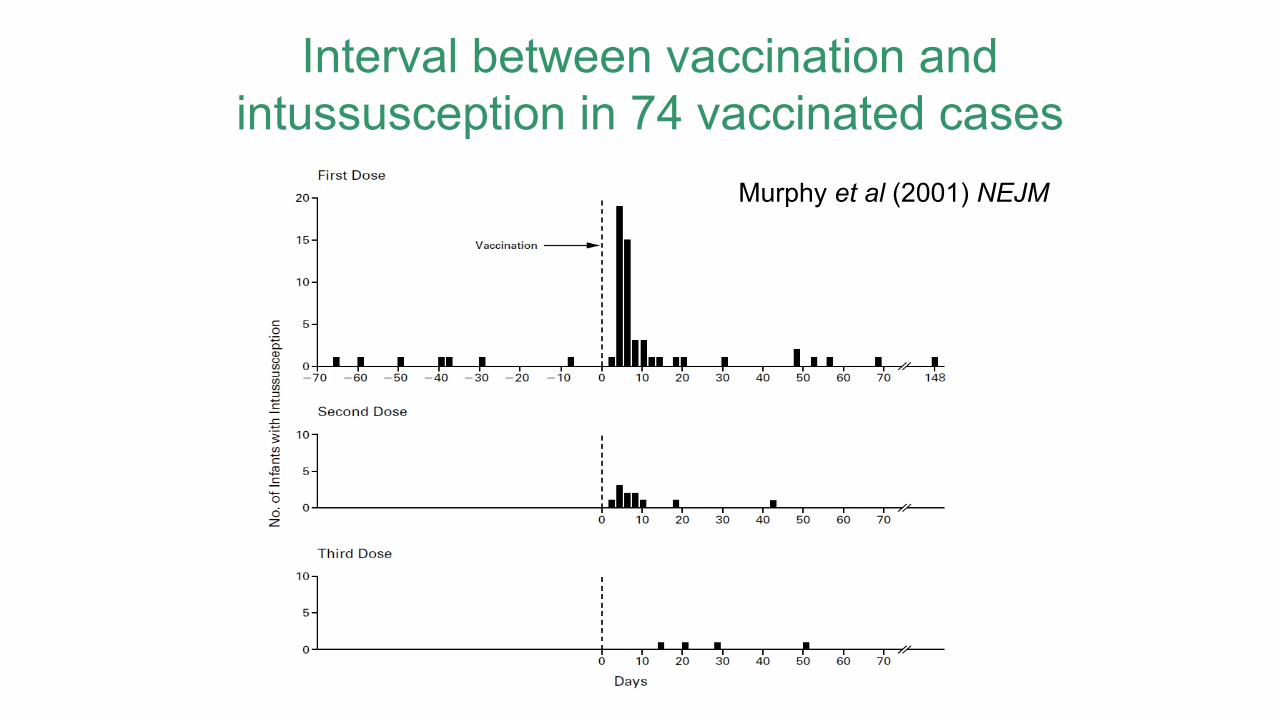
Interval between vaccination and intussusception in 74 vaccinated cases
Murphy et al (2001) NEJM
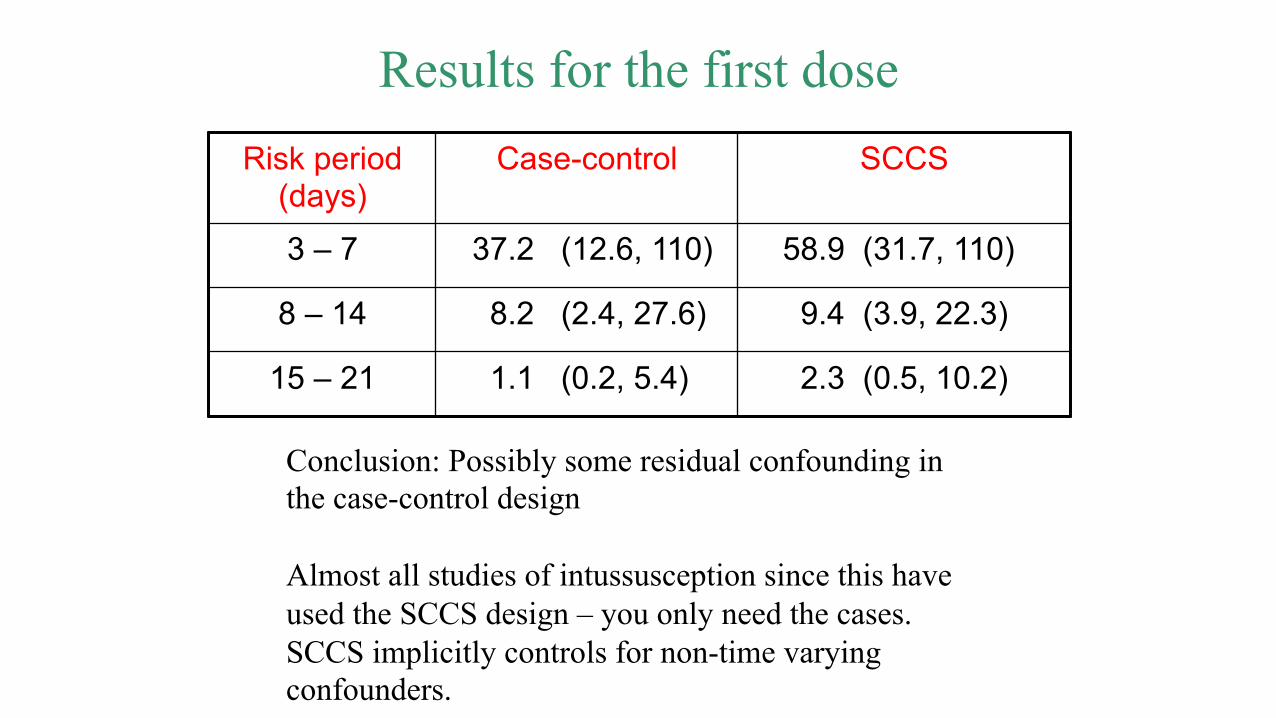
Results for the first dose Risk period
(days) Case-control SCCS
3 – 7 37.2 (12.6, 110) 58.9 (31.7, 110)
8 – 14 8.2 (2.4, 27.6) 9.4 (3.9, 22.3)
15 – 21 1.1 (0.2, 5.4) 2.3 (0.5, 10.2)
Conclusion: Possibly some residual confounding in the case-control design Almost all studies of intussusception since this have used the SCCS design – you only need the cases. SCCS implicitly controls for non-time varying confounders.

Example2: MMR and Autism studies
Study Sample size RI / OR
95% CI
SCCS (UK 1999)
357 cases 0.88 (0.40, 1.95)
Cohort (Denmark -2002)
537303 children 316 cases
0.92 (0.68, 1.24)
Case-control (UK 2004)
1294 cases 4469 controls
0.86 (0.68, 1.09)
In this case SCCS worked well, although it is more suited to clearer acute onsets.

Example3: Asthma exacerbation and flu vaccine
Method Sample size RI 95% CI
Cohort, unadjusted 70 753 3.29 (2.55, 4.15)
Cohort, adjusted 70 753 1.39 (1.08, 1.77)
Case series 2075 cases 0.98 (0.76, 1.27)
The cohort results are subject to indication bias. The case series results are unaffected by this bias.
Kramarz et al, Arch. Fam. Med. 2000, 9: 617 – 623
Cohort and case series studies in asthmatic children aged 1 – 6 years in 1995/6. Risk period: 2 weeks after flu vaccine.

Example4: GBS, flu vaccine and flu-like illness
Observation period: all time within GPRD in 1990 – 2005
Two types of exposures: flu vaccination and flu-like illness.
Risk periods: 0-30, 31-60, 61-90 days after vaccine/onset
Pre-exposure risk period: 2 weeks
Age groups: 12 periods over 0 – 115 years
Seasonal groups: calendar month
Repeat episodes: included if > 6 months separation
Stowe et al, Am. J. Epidemiol. 2008, 169: 382 - 388

Results
775 distinct episodes in 690 individuals Flu vaccine: 0 – 30 days: RI = 0.58 (0.18, 1.86) 0 – 90 days: RI = 0.76 (0.41, 1.40) Influenza-like illness: 0 – 30 days: RI = 16.64 (9.37, 29.54) 0 – 90 days: RI = 7.35 (4.36, 12.38)

Interval between influenza-like illness and GBS
From: Stowe et al, Am. J. Epidemiol. 2008, 169: 382 - 388
Example 5: Pandemrix vaccine and
Narcolepsy Miller et al, BMJ 2013
• Pandemrix (AS03 adjuvanted H1N1 vaccine) used widely in Europe
• Signal of possible narcolepsy association from Sweden / Denmark
• Epi studies to date have been cohort, case-control, case-coverage and SCCS.

Choice of study design (UK) • SAMPLE SIZE – calculations suggested we needed
to cover a large proportion of cases in England. • Cohort > No national database for vaccinations. • Case-control> Possible but control selection and cost/
ethical permissions issues with getting controls. • SCCS> Yes – although potential problems with
defining risk interval and having enough follow up time for power.
• Case-coverage>Yes – since we have good coverage data in GP databases such as RCGP.

Study Design • Age: 4 to 18 year olds at diagnosis • Period: Onset from Jan 2008 and diagnosed by the time of the
visit. • Case finding: 23 sleep centres • Validation: of cases using ICSD-2 criteria by 3 experts using
notes obtained at centre visits. • Key index date: Onset of excessive daytime sleepiness (EDS) /
cataplexy as reported in case notes or by a GP • Vaccination history: obtained from a letter to the GP. Details
of being in a risk group targeted for vaccination were also obtained from GPs.
• Case - coverage compares odds of vaccination in cases to the age and risk group matched population

RCGP Coverage data for case-coverage design Non risk
group Risk group

Cases by EDS date and vaccination status

Results – vaccine association • OR = 14.4, 95% CI(4.3-48.5) for vaccinated at any time prior to
onset. • Attributable risk: 1.9 per 100,000 doses. Other designs (results here based on first symptoms for children
and Pandemrix): • France – case matched to hospital controls OR = 21.5 (2.8-167) • Finland – retrospective cohort design RI ~ 25 (8-80) • UK SCCS – did not work well because no clear risk window,
lack of control unexposed time and correlation of period effects and vaccine effects as all vaccine given over a few months.

Design Pros and Cons • Case Control
– Pros – can get detailed information on cases and controls – Cons – control selection may lead to bias
• Cohort – Pros – direct estimates of risks, high power – Cons – may be limited data on possible confounders, may be
difficult to construct the cohort (linkage). • Self Controlled Case Series
– Pros – just need cases so cheaper. Automatic adjustment for non-time varying confounders
– Cons – usually need a risk window to be specified, sometimes co-linearity of vaccine and age/time effects.
• Case-Coverage – Pros – simple to use with routine data without linkage. – Cons – usually limited matching to confounders

Conclusions • Post licensure vaccine safety surveillance is an important
component of a vaccine programme
• It is important to be able to perform controlled epidemiological studies rapidly and to be aware of potentially confounding / bias
• Record linkage and the SCCS method has proved an excellent tool for such studies.
• Cohort and other designs such as case-coverage are also required for some events where SCCS is not ideal.
• NEW QUESTIONS KEEP ARISING!

Acknowledgements
•! PHE: Liz Miller, Julia Stowe, Pauline Kaye •! Royal Free: Brent Taylor •! Open University: Paddy Farrington, Heather Whitaker

EXTRA SLIDES: Useful resources
• WHO Global Vaccine Safety Initiative: http://www.who.int/vaccine_safety/en/
• FDA: Guidance for Industry Good Pharmacovigilance Practices and Pharmacoepidemiologic Assessment http://www.fda.gov/cder/guidance/index.htm
• ADVANCE consortium looking at vaccine benefit risk http://www.advance-vaccines.eu/
• SCCS Website: http://statistics.open.ac.uk/sccs Created by Heather Whitaker – to be updated in the next year or so…
• Tutorial paper: Whitaker et al., Statist. Med. 2006, 25: 1768 – 1797 • Useful overview of case-only methods: Farrington, Vaccine 2005,
2064-70. Control without separate controls:…

Comparing designs